

Abstract
Objective:
To synthesize currently existing data and investigate the prevalence of tooth transposition as well as its relation to gender, dental arch, and quadrant occurrence.
Materials and Methods:
Several electronic databases were searched in order to identify the potentially relevant studies. Initially, 591 papers were retrieved. After applying specific inclusion and exclusion criteria, nine studies were eligible for inclusion in this evaluation. Meta-analysis was performed by determining the event rate and the 95% confidence intervals estimated by the random effect model.
Results:
Analysis of the data of the primary studies revealed that tooth transposition has a mean prevalence of 0.33%. This prevalence seems to be the same between the two genders. However, tooth transposition appears more frequently in the maxilla than in the mandible and more unilaterally than bilaterally.
Conclusion:
Tooth transposition is a rare phenomenon that affects various populations, including across genders, in a similar manner. Some maxillary predisposition exists, and its unilateral occurrence is higher than that of bilateral.
Keywords: Tooth transposition, Prevalence, Meta-analysis
INTRODUCTION
Tooth transposition is considered a rare condition and is usually related to eruption disturbances of the teeth and to the subsequent abnormal occlusal relationships.1 More specifically, tooth transposition is defined as the positional interchange of two neighboring teeth and especially of their roots, or the development or eruption of a tooth in a position normally occupied by a non-neighboring tooth.2 Therefore, tooth transposition is a peculiar type of ectopic eruption in which each ectopic tooth changes the normal order of the tooth sequence in the dental arch.3
The prevalence of tooth transposition varies considerably in the existing literature—from 0.09% to 1.4%1,4—and has not been analyzed by an integrated approach. Systematic reviews and meta-analyses can summarize the results of other studies and provide the readers with some indication of where the weight of the evidence lies. These study designs may, therefore, produce and defend conclusions based on the best available evidence or in some cases may conclude that the evidence currently available does not allow for any conclusions.5
Therefore, the aim of this study was to perform a systematic evaluation in an evidence-based manner to increase the insight into the prevalence of tooth transposition through a meta-analytic procedure in order to identify any possible associations between the prevalence of tooth transposition and the type of population and gender in which it occurred, as well as its dental arch and quadrant localization.
MATERIALS AND METHODS
Detailed search strategies were developed5 to identify potentially relevant studies reporting data from patients presenting tooth transposition. Every effort to minimize any possible bias in the location of studies was made, and citations to potentially relevant studies from journal articles, dissertations, or conference proceedings were located by searching the appropriate electronic databases. In addition, to identify potentially relevant unpublished or ongoing studies, the databases of research registers were researched. Table 1 presents the databases searched and outlines the search strategy used. This electronic search was conducted on December 17, 2008, after appropriate changes in vocabulary and the syntax rules of each database.
Table 1.
The Electronic Databases Searched and the Search Strategy Used in the Meta-Analysis (as of December 17, 2008)
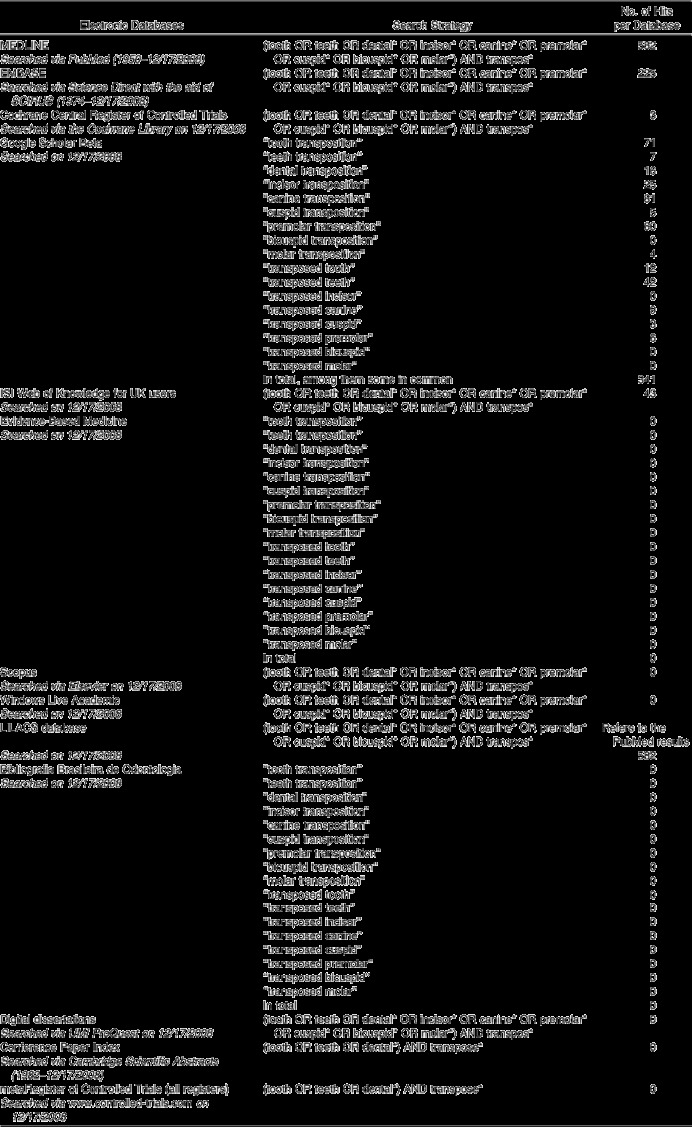
In addition to the electronic searches, manual searching was also performed by checking the references of the initially retrieved articles. When abstracts or full-text articles provided insufficient evidence, the corresponding authors were contacted. No restrictions were applied during the identification procedure concerning the years considered, the publication status, or the language of the studies.
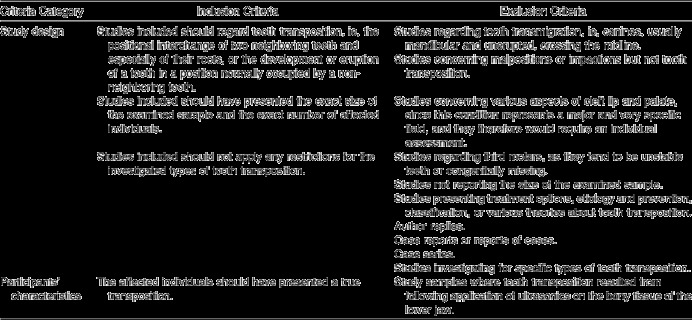
Studies appropriate for inclusion in the meta-analysis fulfilled specific criteria with regard to study design, participants' characteristics, intervention characteristics, and principal outcome measures. The detailed inclusion and exclusion criteria are listed in Table 2.
Table 2.
Criteria for Selecting Studies to be Included in the Meta-Analysis
Initially, the titles and abstracts of identified studies were reviewed. Any retrieved article was checked for data from patients presenting tooth transposition. Any investigation not fulfilling this criterion was excluded from further evaluation. If the reviewer could not decide on the eligibility of a study by examining the title and the abstract, the full text of the article was retrieved. Furthermore, duplicate citations, such as dissertations that formed the basis of published trials, conference abstracts of published trials, case reports, reports of cases, case series, or review articles, were discarded. For the remaining articles, the corresponding full text was retrieved for further evaluation. These were evaluated in duplicate by two reviewers working independently (Dr Papadopoulos and Dr Chatzoudi). Evaluation of the interreviewer agreement during the selection procedure was assessed by kappa score. All the above-mentioned processes were not performed blinded, because scientific evidence does not strongly recommend masked assessment.6 Any remaining differences were resolved through mutual agreement.
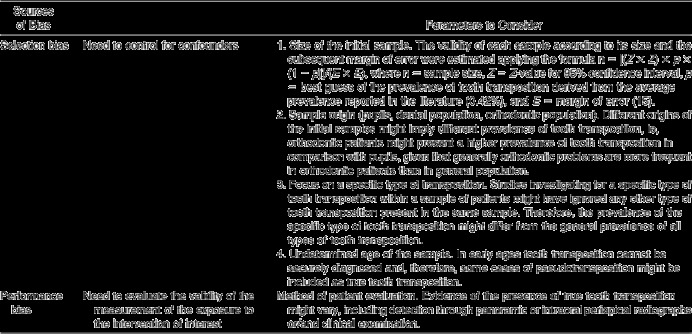
The quality of nonrandomized trials cannot be evaluated in the same way as for randomized controlled trials.7–9 Various criteria have been suggested to critically appraise their validity, which can be applied to other types of studies; however, a great deal of judgment is necessary.10 The possible sources of bias and the parameters to consider in nonrandomized trials, as discussed in Higgins and Green,10 were considered in this investigation and presented in Table 3.
Table 3.
Possible Sources of Bias According to Higgins and Green7 and Parameters to Consider for the Present Meta-Analysis
The retrieved data was analyzed by means of specially designed software, the Comprehensive Meta-Analysis (Biostat Inc, Englewood, NJ).
The random effects method for meta-analysis, which takes into consideration the heterogeneity of the data, was used to combine the prevalence of transposition according to the approach of Borenstein et al.9 The choice of this model was based on the assumption that the variability in the studies retrieved could influence the effects under investigation. Nevertheless, to further identify the extent of heterogeneity, the Cochran test for homogeneity and the I2 test were calculated to check for heterogeneity and inconsistency, respectively. Subgroup analyses were performed implementing the approach of Deeks et al.11
Publication bias was assessed by preparing a funnel plot. Funnel plot asymmetry was inspected graphically and measured numerically using the approach proposed by Egger et al12 and Sterne et al.13,14 Evidence of asymmetry was based on P < .10.
RESULTS
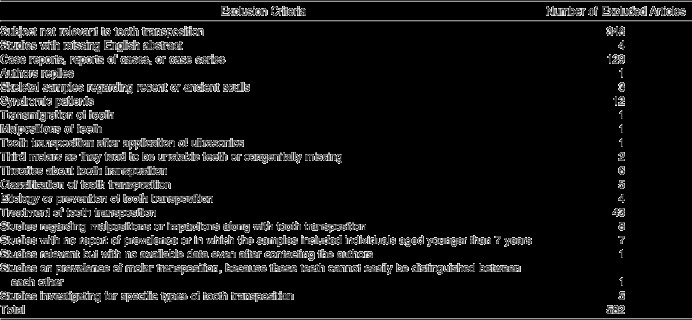
The flow diagram of the retrieved studies is presented in Figure 1. Following utilization of the above-mentioned search strategy, 591 studies were initially identified (582 through electronic searching and nine through manual searching). After applying the specific inclusion and exclusion criteria, 582 articles were excluded for various reasons, and only nine studies were considered as appropriate to be included in the meta-analysis. The exclusion criteria and the number of excluded articles are listed in detail in Table 4. The kappa score for the overall agreement between the two investigators before reconciliation was 0.851 (asymptotic standard error 0.085).
Figure 1.
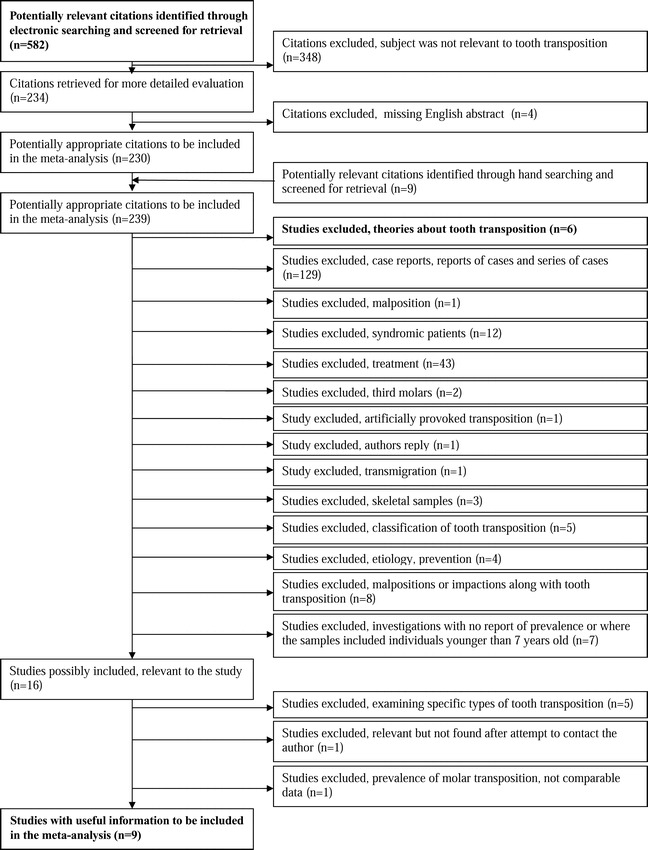
Flow diagram of the retrieved studies through the selection process.
Table 4.
Exclusion Criteria and Number of Excluded Articles in This Meta-Analysis
The exact types of tooth transposition investigated in the studies included in this meta-analysis are presented in detail in Table 5, and their characteristics in Table 6.
Table 5.
Types of Tooth Transposition Investigated in the Source Studies Included in the Meta-Analysis
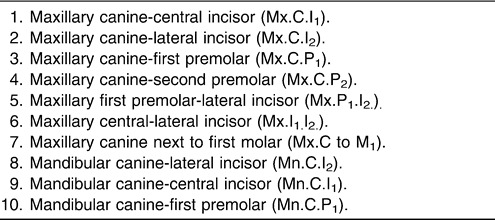
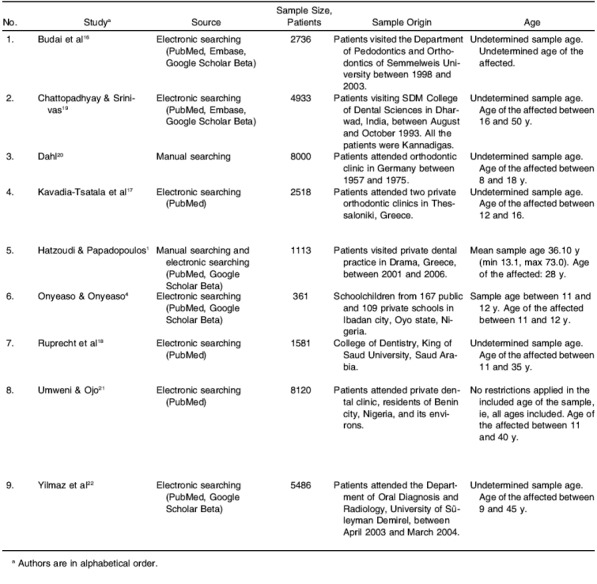
Table 6.
Characteristics of Studies Included in the Meta-Analysis
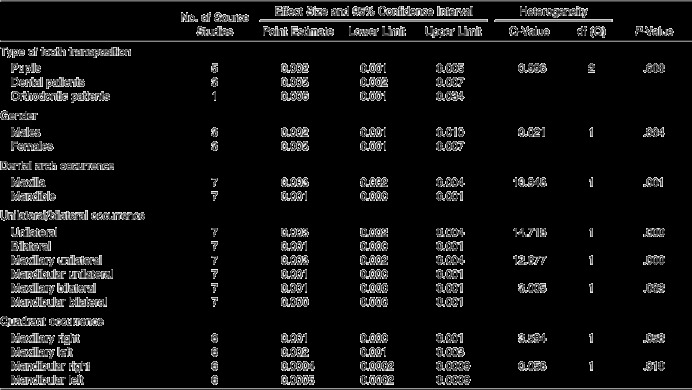
Table 6.
Extended
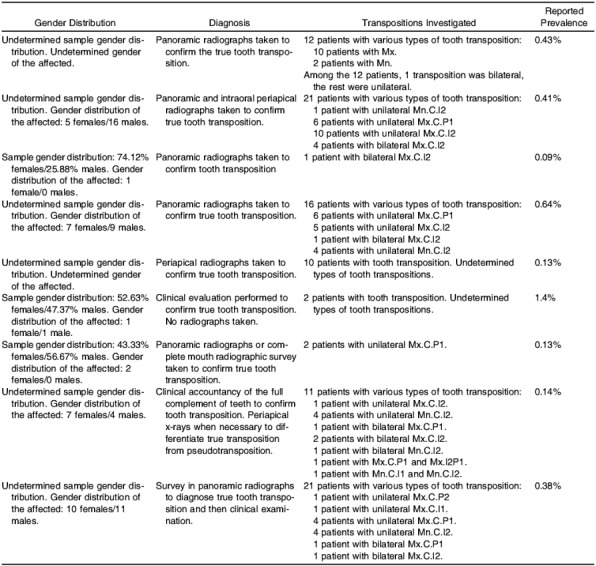
In only one4 out of the nine studies under evaluation, the sample included was relatively small (under 500 patients) and allowed for a margin of error approximately 0.051.15 In four studies1,16–18 the sample was quite adequate, consisting of 1000 to 4500 patients and allowing for a margin of error between 0.018 and 0.029.15 In the remaining four studies,19–22 the samples were relatively big, including more than 4500 patients and allowing for a margin of error between 0.011 and 0.014.15
In one study4 the samples were selected from school populations (pupils), in three studies16,17,20 the samples were retrieved from university orthodontic departments or private orthodontic practices (orthodontic patients), and in the remaining five studies1,18,19,21,22 the samples were derived from dental schools or private dental practices (dental patients). The inclusion of studies investigating tooth transposition on dental or orthodontic patients represents selection bias, since these samples may not be representative of the underlying population.
In one study4 the diagnosis of tooth transposition was based solely upon clinical examination, whereas in the remaining eight studies1,16–22 there was a radiographic confirmation of the transposition. These different methods of diagnosis might imply a detection bias as well.
In six studies16–20,22 the ages of the individuals in the sample were undetermined, whereas in one study21 all ages were included in the sample under investigation. However, tooth transposition cannot be securely diagnosed in individuals aged younger than 7 years. Thus, the inclusion in the analysis of studies that have possibly investigated individuals aged younger than 7 years might imply a kind of selection bias.
Publication bias was first assessed visually with a funnel plot analysis (Figure 2). Because studies of varying sample sizes were included in the meta-analysis, the Egger linear regression method was also used (intercept = −1.857, 95% CI = −5.727 to 2.012; t = 1.134; df = 7; 2-tailed P = .293).13 Although an indication of asymmetry was observed in the funnel plot, no evidence of publication bias was found.
Figure 2.
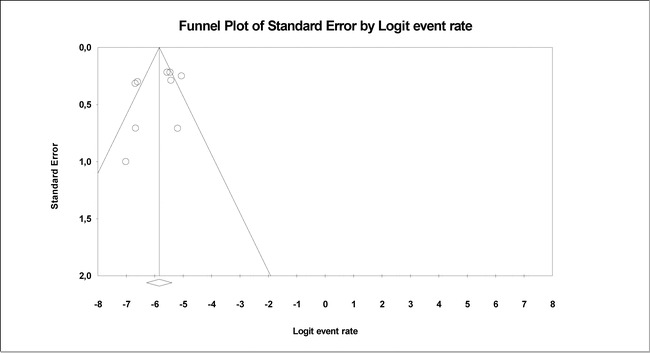
Funnel plot analysis.
The results of the meta-analysis concerning the general prevalence of tooth transposition, as well as for the various subgroups, are presented in Table 7. The general prevalence of tooth transposition following evaluation of the nine studies included in the meta-analysis was 0.33% (Figure 3).
Figure 3.
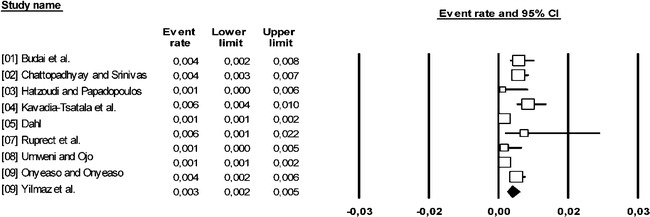
Forest plot for the prevalence of tooth transposition (Q-value = 31.96, I2 = 74.975).
Table 7.
Results of the Meta-Analysis (Random Effects Model) for the Prevalence of Tooth Transposition with Regard to the Various Subgroups, Including the Number of the Source Studies, the Effect Sizes with the 95% Confidence Intervals, the Assessment of Heterogeneity, and the Statistical Significance
The prevalence of tooth transposition in pupils and dental and orthodontic patients was found to be 0.20%, 0.30%, and 0.60%, respectively, and presented no statistically significant differences among these three different subgroups (P = .608).
Further, the prevalence of tooth transposition did not differ statistically between males (0.20%) and females (0.30%) (P = .884), is more pronounced in the maxilla (0.003) than in the mandible (0.001) (P = .001), and takes place more frequently unilaterally (0.30%) than bilaterally (0.10%) (P = .000). Furthermore, this unilateral occurrence is more pronounced in the maxilla (0.30%) than in the mandible (0.10%) (P = .000). However, the maxillary bilateral occurrence of tooth transposition (0.10%) was not significantly higher than the mandibular bilateral one (0.00%) (P = .083).
Finally, the prevalence of tooth transposition did not differ statistically between the maxillary left (0.20%) and right quadrant (0.10%) (P = .058) or between the mandibular left (0.05%) and right quadrant (0.04%) (P = .810).
DISCUSSION
In the present study, every effort to minimize any possible selection bias was made by developing a precise protocol that was followed during the study.5 In detail, the search strategy was performed for the time period 1951–2008, including electronic searching of the most important electronic databases of the medical literature as well as manual searching. Efforts to identify potentially relevant unpublished or ongoing studies were made by searching the databases of research registers. In addition, when abstracts or full-text articles provided insufficient information, the corresponding authors were contacted. In fact, in two cases the authors were contacted about providing us with detailed data of their investigations.17,23 The authors of the first study17 sent all the necessary information; however, no reply was received from the authors of the second study,23 and consequently this article was excluded from the current meta-analysis. No restrictions were applied during the identification process for the years considered, the publication status, or the language of the studies. However, studies in non-English languages with missing English abstracts were excluded (four studies in total). Several inclusion and exclusion criteria have been applied in order to select the appropriate studies to be included in the analysis. The selection procedure was accomplished independently by two authors, and the outcomes were analyzed to address any methodological inconsistencies. Potential biases concerning the eligibility and quality of the original studies to be included in the analysis were resolved through mutual agreement. Evaluation of the interreviewer agreement before reconciliation was assessed by kappa score and proved to be excellent.
Evidence of true tooth transposition of the affected individuals was considered as an essential issue for a study to be included in this meta-analysis. Consequently, the method used for the diagnosis and evaluation of tooth transposition was taken into consideration. In most of the studies included in the meta-analysis, a radiographic examination by means of panoramic or intraoral periapical radiographs was undertaken to diagnose tooth transposition, whereas in only one of them4 the diagnosis was based mainly upon clinical evaluation. Although true tooth transposition can be detected quite easily even by means of clinical examination and palpation of the area of the roots of the corresponding teeth, an additional radiographic examination is desirable and usually recommended when conducting an evidence-based study. However, the possible selection bias that may have been inferred by including the above-mentioned study,4 where only clinical evaluation was performed to diagnose tooth transposition, was not considered as significant and therefore this study was included in the current evaluation.
Following critical appraisal of the inclusion and exclusion criteria applied in this investigation, every effort was done to select only the appropriate data of the primary studies. When these studies did not present adequate data for all variables under investigation, they were partly included in the analysis using only the corresponding data. Consequently, the number of the original studies included in the analysis was different for each variable under investigation.
The consistency of the initial samples is another issue that needs to be taken into consideration because in some of the samples the clear multi-ethnic background of the population investigated was not adequately assessed. In addition, the different sources of the selected samples (from schools, university departments, and/or private dental clinics) might involve a form of selection bias, suggesting that some caution when interpreting the results of this study. In addition, selection bias might also have been introduced through the inclusion of studies with no information concerning the ages of the individuals under investigation, because tooth transposition cannot be securely diagnosed earlier than age 7.
According to the results of this investigation, the average prevalence of tooth transposition was found to be 0.33%. This percentage is lower compared with the corresponding ones found in other published reports in the existing literature concerning various ethnic groups (eg, 0.38% in Turkey,22 0.40% in India,19 and 1.4% in Nigeria4), and higher than those found in reports from Greece (0.09%)1 and Germany (0.13%).20 All these figures suggest that tooth transposition might be considered a rare phenomenon.
There seem to be no statistically significant differences in the prevalence of tooth transposition between pupils and dental and orthodontic patients or between males and females. The latter is in contrast to the observations of some authors,2,21,24 who found that tooth transposition was more frequent in females than in males. Some of these authors proposed a hypothesis that gender-related genes may be responsible for tooth transposition.25,26 However, according to our evaluation this hypothesis could not be confirmed.
Further, maxillary occurrence of tooth transposition was found to be higher than the mandibular. The high bone density of the mandible might be responsible for a prohibition of the phenomenon of tooth transposition, and thus the higher incidence of maxillary occurrence. It is remarkable that the most common type of tooth transposition in the mandible takes place between the canines and lateral incisors, where the bone is more porous than in the posterior area. In contrast, the lower density of bone in the maxilla may enhance the incidence of tooth transposition as well as the variety of types of transposition (eg, between canines and first premolars, between canines and lateral incisors, between central and lateral incisors).26–30
In addition, it was also observed that the unilateral occurrence of tooth transposition is more frequent than the bilateral, and this agrees with previous reports in the literature.3,30–32 Although there is a genetic basis for tooth transposition (evidence for this might be the symmetrical occurrence of bilateral transposition19,26), the expression of the corresponding genome usually follows the rule of asymmetry that applies for the whole body as well as for the orofacial structures. However, specific local factors, such as mechanical disturbances of the normal eruption path of the permanent teeth or trauma, may also lead to a unilateral expression of the genome,33 whereas early extraction of deciduous teeth may also create a developmental disharmony in the dental arch and, at times, tooth transposition.34
Regarding the side quadrant localization of tooth transposition, no left- or right-side predilection in the maxilla or mandible was evident. In contrast, other authors found that tooth transposition occurred more frequently in the maxillary left side2,28 without, however, presenting any explanation that could justify this observation.
CONCLUSIONS
Tooth transposition is a rare phenomenon (0.33%) with various—sometimes inexplicable—forms of manifestation.
Its occurrence seems to have no specific gender predilection, but some maxillary predisposition exists. Its unilateral occurrence is considerably higher than the bilateral.
REFERENCES
- 1.Hatzoudi M, Papadopoulos M. A. Prevalence of tooth transposition in Greek population. Hell Orthod Rev. 2006;9:11–22. [Google Scholar]
- 2.Peck L, Peck S, Attia Y. Maxillary canine-first premolar transposition, associated dental anomalies and genetic basis. Angle Orthod. 1993;63:99–109. doi: 10.1043/0003-3219(1993)063<0099:MCFPTA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.Peck L, Peck S. Classification of maxillary tooth transpositions. Am J Orthod Dentofacial Orthop. 1995;107:505–517. doi: 10.1016/s0889-5406(95)70118-4. [DOI] [PubMed] [Google Scholar]
- 4.Onyeaso C. O, Onyeaso A. O. Occlusal/dental anomalies found in a random sample of Nigerian schoolchildren. Oral Health Prev Dent. 2006;4:181–186. [PubMed] [Google Scholar]
- 5.Papadopoulos M. A. Meta-analysis in evidence-based orthodontics. Orthod Craniofac Res. 2003;6:12–26. [PubMed] [Google Scholar]
- 6.Moher D, Cook D. J, Jadad A. R, Tugwell P, Moher M, Jones A, Pham B, Klassen T. P. Assessing the quality of reports of randomized trials: implication for the conduct of meta-analyses. Health Technol Assess. 1999;3:i–iv. 1–98. [PubMed] [Google Scholar]
- 7.Altman D. G, Schulz K. F, Moher D, Egger M, Davidoff F, Elbourne D. The revised CONSORT statement for reporting randomized trials: explanation and elaboration. Ann Intern Med. 2001;134:663–694. doi: 10.7326/0003-4819-134-8-200104170-00012. [DOI] [PubMed] [Google Scholar]
- 8.Pildal J, Chan A. W, Hróbjartsoon A, Forfang E, Altman D. G, Gøtzche P. C. Comparison of descriptions of allocation concealment in trial protocols and the published reports: cohort study. BMJ. 2005;330:1049. doi: 10.1136/bmj.38414.422650.8F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Borenstein M, Hedges L. V, Rothstein H. Fixed-effect versus random-effects models. In: Borenstein M, Hedges L. V, Higgins J. P. T, Rothstein H, editors. Introduction to MetaAnalysis. Hoboken, NJ: Wiley; 2009. [Google Scholar]
- 10.Higgins J. P. T, Green S, eds . Cochrane Handbook for Systematic Reviews of Interventions Version 426 [updated September 2006] Chichester, UK: John Wiley & Sons; [Google Scholar]
- 11.Deeks J. J, Altman D. G, Bradburn M. J. Statistical methods for examining heterogeneity and combining results from several studies in meta-analysis. In: Egger M, Davey Smith G, Altman D. G, editors. Systematic Reviews in Health Care MetaAnalysis in Context. London, UK: BMJ Publication Group; 2001. [Google Scholar]
- 12.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sterne J. A, Egger M, Davey Smith G. Systematic reviews in health care: investigating and dealing with publication and other biases in meta-analysis. BMJ. 2001;323:101–105. doi: 10.1136/bmj.323.7304.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sterne J. A. C, Gavaghan D, Egger M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol. 2000;53:1119–1129. doi: 10.1016/s0895-4356(00)00242-0. [DOI] [PubMed] [Google Scholar]
- 15.Adcock C. J. Sample size determination: a review. Statistician. 1997;46:261–283. [Google Scholar]
- 16.Budai M, Ficzere I, Gábris K, Tarjan I. Frequency of transposition and its treatment at the Department of Pedodontics and Orthodontics of Semmelweis University in the last five years. Fogorv Sz. 2003;96:21–24. [PubMed] [Google Scholar]
- 17.Kavadia-Tsatala S, Sidiropoulou S, Kaklamanos E. G, Chatziyanni A. Tooth transpositions associated with dental anomalies and treatment management in a sample of orthodontic patients. J Clin Pediatr Dent. 2003;28:19–25. doi: 10.17796/jcpd.28.1.c320v565x8413n7g. [DOI] [PubMed] [Google Scholar]
- 18.Ruprecht A, Batniji S, El-Neweihi E. The incidence of transposition of teeth in dental patients. J Pedod. 1985;9:244–249. [PubMed] [Google Scholar]
- 19.Chattopadhyay A, Srinivas K. Transposition of teeth and genetic etiology. Angle Orthod. 1996;66:147–152. doi: 10.1043/0003-3219(1996)066<0147:TOTAGE>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 20.Dahl T. The transposition of teeth [in German] Zahn Mund Kieferheilkd Zentralbl. 1976;64:267–270. [PubMed] [Google Scholar]
- 21.Umweni A. A, Ojo M. A. The frequency of tooth transposition in Nigerians, its possible aetiologic factors and clinical implications. J Dent Assoc S Afr. 1997;52:551–554. [PubMed] [Google Scholar]
- 22.Yilmaz H. H, Turkkahraman H, Sayin M. O. Prevalence of tooth transpositions and associated dental anomalies in a Turkish population. Dentomaxillofac Radiol. 2005;34:32–35. doi: 10.1259/dmfr/57695636. [DOI] [PubMed] [Google Scholar]
- 23.Ionescu E, Duduca I, Preoteasa E, Suciu I, Dragoi C. Canine tooth transposition study on a group of patients orthodontically treated [in Rumanian] Rev Med Chir Soc Med Nat Iasi. 2006;110:978–981. [PubMed] [Google Scholar]
- 24.Shapira Y. Transposition of canines. J Am Dent Assoc. 1980;100:710–712. doi: 10.14219/jada.archive.1980.0217. [DOI] [PubMed] [Google Scholar]
- 25.Gholston I. R, Williams P. R. Bilateral transposition of maxillary canines and lateral incisors: a rare condition. ASDC J Dent Child. 1984;51:58–63. [PubMed] [Google Scholar]
- 26.Peck S, Peck L, Kataja M. Mandibular lateral incisor-canine transposition, concomitant dental anomalies, and genetic control. Angle Orthod. 1998;68:455–466. doi: 10.1043/0003-3219(1998)068<0455:MLICTC>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 27.Sandham A, Harvie H. Ectopic eruption of the maxillary canine resulting in transposition with adjacent teeth. Tandlaegebladet. 1985;89:9–11. [PubMed] [Google Scholar]
- 28.Shapira Y, Kuftinec M. M. Maxillary tooth transpositions: characteristic features and accompanying dental anomalies. Am J Orthod Dentofacial Orthop. 2001;119:127–134. doi: 10.1067/mod.2001.111223. [DOI] [PubMed] [Google Scholar]
- 29.Thilander B, Jakobsson S. O. Local factors in impaction of maxillary canines. Acta Odontol Scand. 1968;26:145–168. doi: 10.3109/00016356809004587. [DOI] [PubMed] [Google Scholar]
- 30.Plunkett D. J, Dysart P. S, Kadros T. B, Herbison G. P. A study of transposed canines in a sample of orthodontic patients. Br J Orthod. 1998;25:203–208. doi: 10.1093/ortho/25.3.203. [DOI] [PubMed] [Google Scholar]
- 31.Nestel E, Walsh J. S. Substitution of a transposed premolar for a congenitally absent lateral incisor. Am J Orthod Dentofacial Orthop. 1988;93:395–399. doi: 10.1016/0889-5406(88)90098-4. [DOI] [PubMed] [Google Scholar]
- 32.Shapira Y, Kuftinec M. M, Stom D. Maxillary canine-lateral incisor transposition—orthodontic management. Am J Orthod Dentofacial Orthop. 1989;95:439–444. doi: 10.1016/0889-5406(89)90306-5. [DOI] [PubMed] [Google Scholar]
- 33.Laptook T, Silling G. Canine transposition—approaches to treatment. J Am Dent Assoc. 1983;107:746–748. doi: 10.14219/jada.archive.1983.0330. [DOI] [PubMed] [Google Scholar]
- 34.Platzer K. M. Mandibular incisor-canine transposition. J Am Dent Assoc. 1968;76:778–784. doi: 10.14219/jada.archive.1968.0121. [DOI] [PubMed] [Google Scholar]