

Abstract
Objective:
To prospectively measure occlusal changes in mixed dentition patients who underwent a standardized early expansion protocol.
Materials and Methods:
The treatment sample consisted of 500 patients who were assigned to three groups according to molar relationship: Class I (n = 204), end-to-end (n = 166), and Class II (n = 130). All patients were treated with a bonded rapid maxillary expander (RME) followed by a removable maintenance plate and a transpalatal arch. Mean age at the start of treatment was 8.8 years (T1), with a pre–phase 2 treatment cephalogram (T2) taken 3.7 years later. The control sample consisted of the cephalometric records of 188 untreated subjects (Class 1, n = 79; end-to-end, n = 51; Class II, n = 58).
Results:
The largest change in molar relationship was noted when the Class II treatment group (1.8 mm) was compared with the matched control group (0.3 mm). A positive change was seen in 81% of the Class II treatment group, with almost half of the group improving by ≥2.0 mm. The end-to-end treatment group had a positive change of 1.4 mm, compared with a control value of 0.6 mm, and the Class I group of about 1 mm compared with controls, who remained unchanged (0.1 mm). Skeletal changes were not significant when any of the groups were compared with controls.
Conclusion:
The expansion protocol had a significantly favorable effect on the sagittal occlusal relationships of Class II, end-to-end, and Class I patients treated in the early mixed dentition.
Keywords: Rapid maxillary expansion, Acrylic splint expander, Cephalometrics, Class II malocclusion, Transpalatal arch
INTRODUCTION
During the last three decades, rapid maxillary expansion (RME) has grown in popularity among orthodontists as an important orthopedic adjunct to fixed appliance therapy. Expansion protocols have been advocated for a variety of purposes, including correction of crossbite, elimination of dental crowding, leveling of the curve of Wilson, facilitation of eruption of the permanent canines, increasing the size of the nasal airway, and reduction of unesthetic buccal corridors.1–4
One appliance type that has been shown to provide effective orthopedic treatment in early mixed dentition patients is the bonded acrylic splint expander. A number of articles have appeared in the literature in which the acrylic splint RME appliance was used alone4,5 or in combination with other appliances.6,7
Initially, the major focus of RME treatment was related to crossbite correction and reduction in tooth size/arch size discrepancies and control of the vertical dimension.4 A most interesting observation following initial efforts in the early 1980s to expand Class II patients in the early mixed dentition was the occurrence of a spontaneous improvement of the Class II relationship during the retention period.3 The phenomenon of spontaneous improvement in sagittal relationships forced a rethinking of the concept of Class II correction.
Traditionally, clinicians have viewed a Class II malocclusion as primarily a sagittal and vertical problem. Tollaro and coworkers8 have shown that most Class II malocclusions have a strong transverse component as well, with the maxilla often 3 to 5 mm narrower than it ideally should be relative to the mandible. In Class II patients, a significant deficiency in the dentoskeletal transverse width of the maxilla has been demonstrated on posteroanterior films.9 It can be hypothesized that the expansion of the maxilla, which subsequently is stabilized with a removable palatal plate followed by a transpalatal arch (TPA), induces favorable skeletal and dentoalveolar adaptations in the sagittal dimension, as indicated in a previous investigation.10
Based on years of clinical observation, preliminary outcomes of the study by Wendling and coworkers,10 and a case report describing the same phenomenon by Lima and coworkers,11 rigorous testing of the underlying hypothesis is in order. The aim of this prospective study was to evaluate the hypothesis that expansion of the maxilla in the early mixed dentition followed by stabilization of maxillary changes leads to improvement in sagittal molar relationships prior to comprehensive orthodontic treatment in patients showing Class II, or end-to-end, or Class I malocclusions.
MATERIALS AND METHODS
Data on the treatment sample used in this study were gathered prospectively as part of a larger sample of 1135 consecutively treated patients who underwent a standardized expansion protocol in the early mixed dentition. All patients were treated with a bonded RME followed by a removable palatal plate that was worn full-time at least for 1 year, and by the placement of a soldered transpalatal arch during the transition to the permanent dentition; the lower arch typically was not retained. The following criteria were applied for enrollment of subjects in this clinical trial:
Class I or Class II malocclusion
Early mixed dentition (all first permanent molars erupted, as well as all erupting upper and lower permanent incisors)
No other orthodontic treatment provided
Absence of growth problems (craniofacial syndromes, etc)
A total of 547 patients presented with these specific characteristics and were enrolled in the trial. Two lateral headfilms of each patient were taken: T1—initial headfilm, and T2—prior to phase 2 treatment. To eliminate leeway space as a factor, the T2 film was taken when all second premolars were erupted into occlusion, after a period of approximately 4 years following T1. When the lateral cephalograms were analyzed at the completion of the prospective study, 47 subjects had to be removed from the trial, because there had been technical problems with one or both films (19 subjects), problems with mandibular posture (13 subjects), or lack of reliability in assessing the molar relationship (15 subjects). After these technical dropouts, the final sample for the treated group (TG) consisted of 500 patients (224 males and 276 females).
Control subjects were chosen from the records of three large longitudinal databases on orthodontically untreated children: the University of Michigan Growth Study, the Bolton-Brush Growth Study, and the Denver Child Growth Study. Inclusion criteria were essentially the same as for the treatment group. Particular attention was paid to the stage of dental development and to the interval between the two headfilms. The control group (CG) consisted of 188 subjects (101 males and 87 females).
TG and CG were well matched according to the duration of treatment or observation (3.7 years for TG, and 3.9 years for CG). The average age of TG at T1 was 8.8 ± 1.1 years, and for CG 9.3 ± 0.9 years. At T2, the average age of TG was 12.5 ± 1.2 years, and the average age of CG was 13.2 ± 1.1 years.
Cephalometric Analysis
Both lateral cephalograms of each patient were hand-traced at a single sitting on 0.003″ matte acetate using a 2H lead pencil. Cephalograms were traced by one investigator; landmark location and accuracy of the anatomic outlines were verified by a second. Three occlusal measurements and four skeletal measurements were performed: molar relationship, overbite, and overjet; Point A to Nasion perpendicular (an indication of the sagittal maxillary position relative to the cranial base), Pogonion to Nasion perpendicular (sagittal position of the mandible relative to the cranial base), LAFH (lower anterior facial height), and the mandibular plane angle relative to the Frankfort plane. All measurements were standardized to an enlargement of 8%.
The primary focus of the current investigation was to evaluate changes at the level of the anteroposterior relationship of the maxillary and mandibular first permanent molars. In those instances in which dual images of the molars were observed, a template of the upper and lower molars was constructed specifically for that subject based on the more posterior teeth (including the second molars if present). The template then was positioned midway between the mandibular first molars, so that the location of the mesial contact point of the lower first molars could be determined. The process subsequently was repeated for the maxillary first molars.
Because of the critical nature of the molar relationship measurement, the molar relationship of the entire sample was measured independently by two pairs of investigators (four investigators in all). The average difference between the two sets of measurements was ~0.1 mm for the entire sample. The method error for the other occlusal measures as evaluated by means of Dahlberg's formula12 was smaller than 0.5 mm; it was smaller than 1 degree or 1 mm for the cephalometric variables.
Statistical Analysis
On the basis of values for the molar relationships at T1 (Figure 1), the total treated sample was divided into three groups: Class II group (130 subjects; molar relation >0.5 mm), end-to-end group (166 subjects; molar relation ≥−0.5 mm and ≤0.5 mm), and Class I group (204 subjects; molar relation <−0.5 mm). According to the same categorization, control subjects were assigned to three groups: Class II group (58 subjects), end-to-end subjects (51 subjects), and Class I group (79 subjects).
Figure 1.
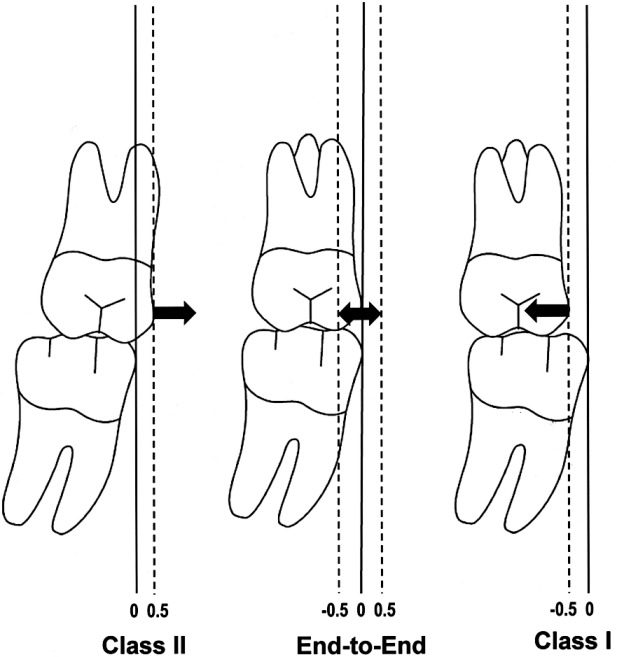
Classification of sagittal molar relationships on cephalometric tracings. Vertical lines are perpendicular to the occlusal plane.
Descriptive statistics, including means and standard deviations, were calculated for the values at T1, as well as for the changes between T1 and T2 of the seven cephalometric measures for the three treated groups and the three control groups. Data were analyzed with a statistical software package (Statistical Package for the Social Sciences [SPSS], version 16.0; SPSS Inc, Chicago, Ill). Statistical significance was tested at P < .05, P < .01, and P < .001.
Following assessment of the normal distribution of the data (Shapiro-Wilks test), independent sample Student's t-tests were used to examine between-group differences in means of the cephalometric measures of the starting forms for all groups. Comparison of T2 – T1 changes over time between treated and untreated groups was accomplished by way of independent sample Student's t-tests.
Z-tests on proportions were used to analyze statistically the proportions of patients vs untreated controls who presented with improvement in the molar relationship during the T1 to T2 interval in each of the three groups, according to initial molar relation. Given the sample sizes of all treatment and control groups and subgroups and a P value of .05, the power of this study was 100%.
RESULTS
Descriptive data and statistical comparisons for starting forms and cephalometric changes for all groups from T1 to T2 are given in Tables 1 through 6.
Table 1.
Comparison of Starting Forms—Class II Sample
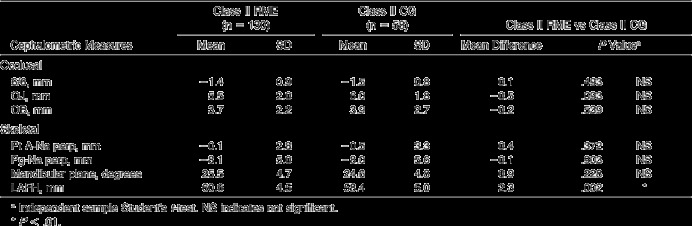
Table 2.
Comparison of Starting Forms—End-to-End Sample
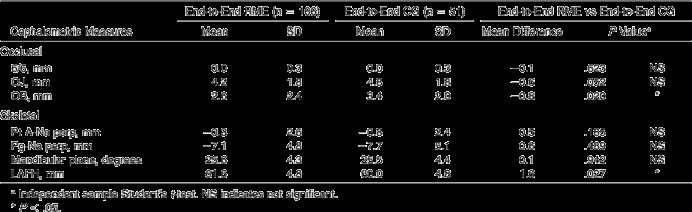
Table 3.
Comparison of Starting Forms—Class I Sample
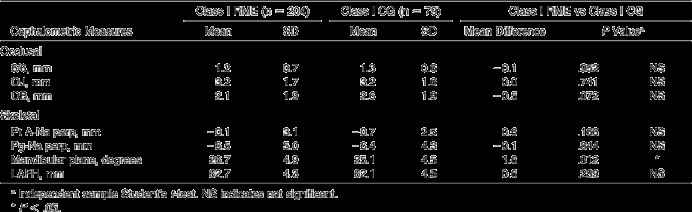
Table 4.
Comparison of Change During Time of Observation—Class II Sample
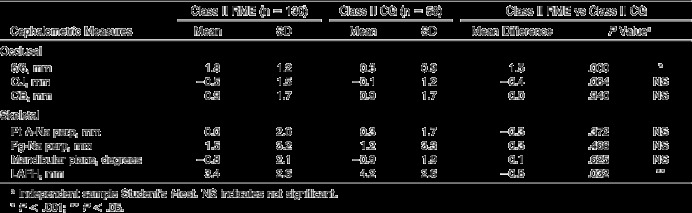
Table 5.
Comparison of Change During Time of Observation—End-to-End Sample
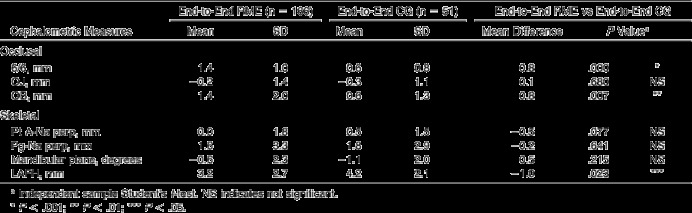
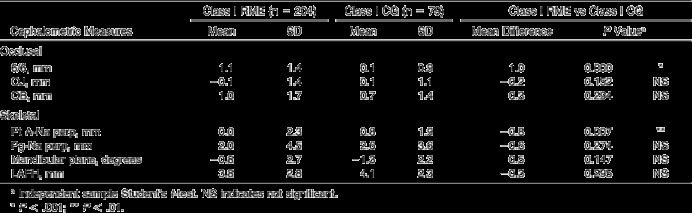
Table 6.
Comparison of Change During Time of Observation—Class I Sample
Analysis of Starting Forms
Occlusal relationships
The average differences in molar relationships between treated and control Class II, end-to-end, and Class I groups were within 0.1 mm in all instances (Tables 1 through 3). No differences in initial overbite or overjet were observed between groups, with the exception of a slightly deeper overbite (3.4 mm) in the end-to-end CG than in the corresponding TG (2.6 mm; P < .05; Table 2).
Skeletal relationships
When skeletal relationships of the three subgroups were evaluated, only minor differences were noted in starting forms. Although no difference in LAFH was seen between Class I groups, the mandibular plane angle was 26.7 degrees in the treatment group and 25.1 degrees in the control group (P < .05; Table 3). LAFH was longer (61.6 mm) in the end-to-end TG than in corresponding controls (60.0 mm; P < .05; Table 2). A similar difference in LAFH was noted between the Class II groups (P < .01; Table 1).
Analysis of Treatment Effects
Occlusal relationships
Changes for the overjet and the overbite showed no significant differences in any of the comparisons between treatment groups and controls. The only exception was a significantly greater increase in overbite in end-to-end TG when compared with the corresponding CG (Table 5), which, however, compensated for the significant difference in overbite in the starting forms (Table 2).
In the analysis of the data regarding molar relations (Figures 2 through 5), the distribution of the changes (ie, negative, neutral, positive) was considered, as was the evaluation of average values:
Figure 2.
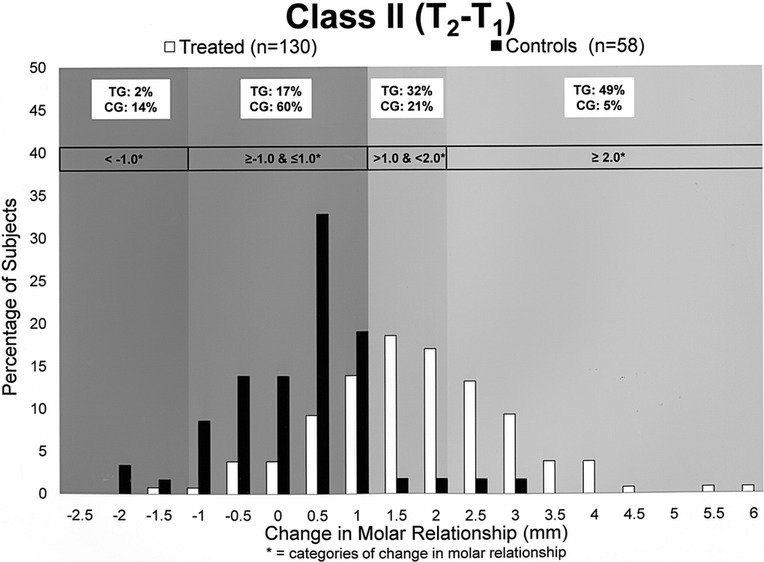
Change in molar relationship: Class II groups.
Figure 3.
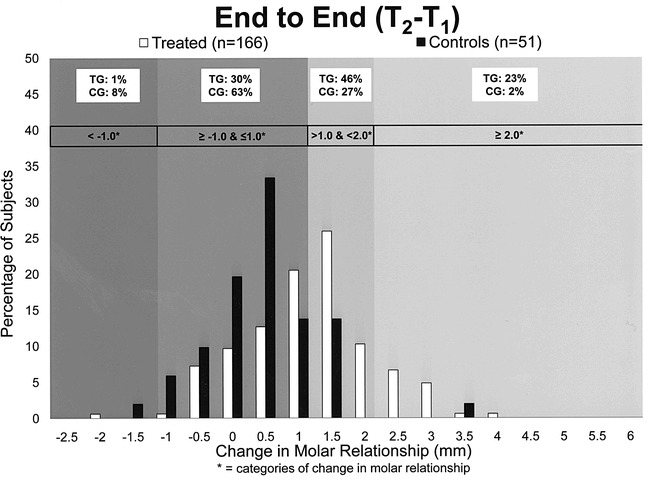
Change in molar relationship: end-to-end groups.
Figure 4.
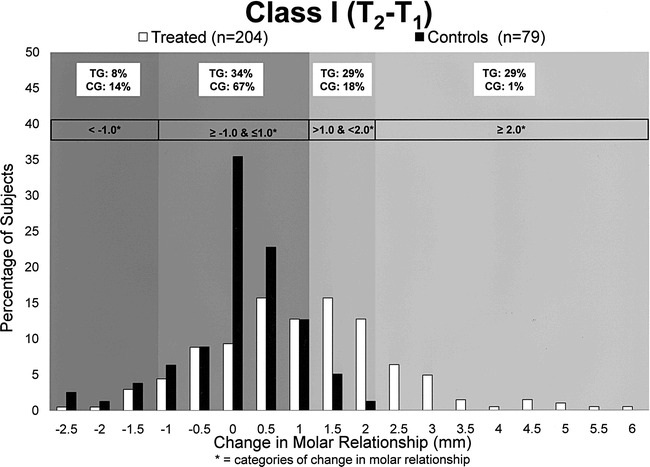
Change in molar relationship: Class I groups.
Figure 5.
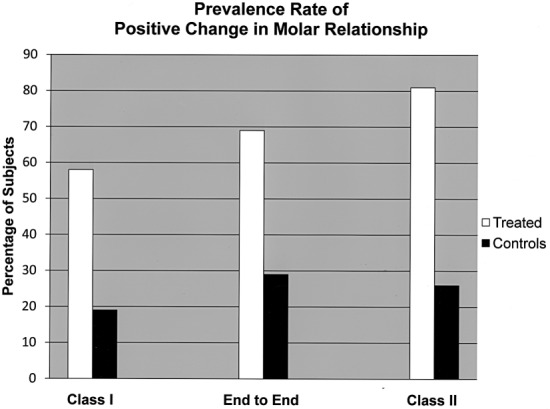
Prevalence rates for positive change in molar relationships in TG vs CG subgroups within each malocclusion group.
A negative change was defined as a change in molar relationship greater than 1 mm toward Class II (<−1.0 mm) between the first and second films.
No change (neutral) is a movement of −1.0 mm to 1.0 mm (≥−1.0 mm and ≤1.0 mm), regardless of the direction of change.
A positive change is a shift greater than 1 mm (>1.0 mm and <2.0 mm) toward Class I. An extremely positive change is a shift of 2 mm or greater (≥2.0 mm) toward Class I.
Class II Groups (Figure 2)
The largest change was noted in the Class II treatment group (an average positive change of 1.8 mm vs 0.3 mm for the untreated Class II group), with an average 1.5 mm difference that was statistically significant (P < .001; Table 4). This difference was characterized by a significant effect size.13 The effect size was larger than 1, which means that the average effect was greater than the interindividual variability expressed by the average standard deviation.
Fourteen percent of the controls presented with a negative change; 60% of the untreated Class II sample had no change in molar relationship from T1 to T2, whereas 26% had a positive change. On the other hand, only 2% and 17% of the Class II treatment group had a negative change or remained unchanged, respectively; 81% had a positive change toward Class I. The statistical comparison between the proportion of patients who presented with an improvement in the molar relation in treated and untreated samples was significant (Z = 7.09; P < .001; Figure 5). Almost half of the treated sample presented with an extremely positive change in molar relationship (≥2 mm); in contrast, only 5% of the untreated Class II sample presented with an extreme improvement.
End-to-End Group (Figure 3)
The end-to-end treatment group had an overall positive change of 1.4 mm in comparison with the control group (0.6 mm), for a net difference of 0.8 mm (P < .001; Table 5). Sixty-nine percent of the treated group had a positive change, with 23% showing extreme improvement; 30% remained unchanged. In the end-to-end control group, 29% demonstrated a positive change, whereas 63% had no change in molar relationship. The difference in the proportion of subjects showing an improvement in molar relationship was significant (Z = 4.93; P < .001; Figure 5). Eight percent of the end-to-end control group had a negative change between T1 and T2, and only 1% of the treatment group had a negative change.
Class I Group (Figure 4)
The smallest change was noted in the Class I group, with virtually no change noted in the control group (0.1 mm); the Class I treatment group demonstrated a positive change of 1.1 mm, with a net average difference between treated and untreated subjects of 1 mm (P < .001; Table 6). Nineteen percent of the untreated Class I sample showed improvement (only 1% improved by 2 mm or more), and 67% remained unchanged. For the Class I treated sample, 58% improved (29% improved by ≥2 mm) and 34% remained unchanged. Differences in the proportions of subjects showing a positive change were significant once again (Z = 5.76; P < .001; Figure 5). It is interesting to note that the molar relationship of 14% of the Class I control group and 8% of the Class I treatment group presented with negative changes during the treatment or observation interval.
Skeletal Relationships
Across groups, no changes were noted in the sagittal relationships of the maxilla (Tables 4 through 6), with the exception of Point A to the Nasion perpendicular, which showed a greater increase in Class I controls. Increases in lower anterior facial height were significantly smaller in the Class II (3.4 mm; Table 4) and end-to-end (3.2 mm; Table 5) treatment groups than in their respective control groups (4.2 mm in both groups; Tables 4 and 5). Although statistically significant, these sagittal and vertical differences can be regarded as clinically insignificant (within 1 mm). No differences were noted in the mandibular plane angle (Tables 4 through 6).
DISCUSSION
This prospective clinical study evaluated a large number of patients who underwent a standardized expansion protocol that included a bonded acrylic splint RME appliance and a transpalatal arch at the end of the transition to the permanent dentition. The results of this investigation, which included comparison of a substantial number of patients (n = 500) vs a large group of untreated control subjects (n = 188), indicated that the treatment protocol used induced positive changes in molar relationship in most patients (Class III malocclusion was not included in this study).
Of particular interest were the occlusal changes noted in Class II and end-to end patients, in whom a positive change toward normal occlusion is desirable. In 81% of Class II patients and 69% of end-to-end patients, a significant positive change was noted, with a change of 2 mm or greater observed in 49% and 23% of Class II and end-to-end patients, respectively. It should be remembered that Class II molar correction or improvement was not the primary intent of the expansion protocol; rather it may be considered a favorable side effect of expansion therapy followed by a space maintenance regimen.
The primary focus of this large-scale investigation has been evaluation of changes in sagittal occlusal relationships, with molar relationship, overjet, and overbite measured. Only four skeletal measures were considered, and they did not show any consistent trend in treated patients vs controls. These outcomes are in agreement with previous long-term longitudinal data on subjects treated with RME in the late mixed dentition followed by fixed appliance therapy.14 Additional studies are warranted to elucidate individual variations in maxillomandibular skeletal response to the expansion protocol, especially with regard to the possibility of forward positioning of the mandible in the postexpansion period, as suggested in a previous study.10
The significant prevalence of improvement in molar relationship following RME treatment appears to be clinically beneficial in subjects showing mild to moderate Class II malocclusion in the mixed dentition. The possible role of the transpalatal arch in avoiding the physiologic mesial drift of maxillary molars during the transitional phase of occlusion deserves to be considered. The TPA has been shown to lack a significant effect in improving anchorage in extraction cases,15 although it may be effective as a space maintenance device to assist the improvement in molar relationships induced by the RME protocol.
CONCLUSIONS
The expansion protocol evaluated in mixed dentition patients, which included the use of a bonded acrylic splint expander and a transpalatal arch just prior to phase 2 treatment, results in an improvement in sagittal relationships in Class II, end-to-end, and Class I patients in comparison with their matched control groups.
Positive changes were observed in 81% of Class II patients, 69% of end-to-end patients, and 58% of Class I patients.
Forty-nine percent of Class II patients, 29% of end-to-end patients, and 23% of Class I patients demonstrated an improvement in sagittal molar relationships of 2 mm or greater. Less than 5% of corresponding control groups had positive changes of 2 mm or greater.
REFERENCES
- 1.Haas A. J. Palatal expansion: just the beginning of dentofacial orthopedics. Am J Orthod. 1970;57:219–255. doi: 10.1016/0002-9416(70)90241-1. [DOI] [PubMed] [Google Scholar]
- 2.Wertz R. A. Changes in nasal airflow incident to rapid maxillary expansion. Angle Orthod. 1968;38:1–11. doi: 10.1043/0003-3219(1968)038<0001:CINAIT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.McNamara J. A., Jr Maxillary transverse deficiency. Am J Orthod Dentofac Orthop. 2000;117:567–570. doi: 10.1016/s0889-5406(00)70202-2. [DOI] [PubMed] [Google Scholar]
- 4.McNamara J. A, Jr, Brudon W. L. Orthodontics and Dentofacial Orthopedics. Ann Arbor, Mich: Needham Press; 2001. [Google Scholar]
- 5.Sarver D. M, Johnston M. W. Skeletal changes in vertical and anterior displacement of the maxilla with bonded rapid palatal expansion appliances. Am J Orthod Dentofac Orthop. 1989;95:462–466. doi: 10.1016/0889-5406(89)90409-5. [DOI] [PubMed] [Google Scholar]
- 6.McNamara J. A., Jr An orthopedic approach to the treatment of Class III malocclusion in young patients. J Clin Orthod. 1987;21:598–608. [PubMed] [Google Scholar]
- 7.McNamara J. A, Jr, Howe R. P. Clinical management of the acrylic splint Herbst appliance. Am J Orthod Dentofac Orthop. 1988;94:142–149. doi: 10.1016/0889-5406(88)90362-9. [DOI] [PubMed] [Google Scholar]
- 8.Tollaro I, Baccetti T, Franchi L, Tanasescu C. D. Role of posterior transverse interarch discrepancy in Class II, Division 1 malocclusion during the mixed dentition phase. Am J Orthod Dentofac Orthop. 1996;110:417–422. doi: 10.1016/s0889-5406(96)70045-8. [DOI] [PubMed] [Google Scholar]
- 9.Franchi L, Baccetti T. Transverse maxillary deficiency in Class II and Class III malocclusions: a cephalometric and morphometric study on postero-anterior films. Orthod Craniofac Res. 2005;8:21–28. doi: 10.1111/j.1601-6343.2004.00312.x. [DOI] [PubMed] [Google Scholar]
- 10.Wendling L. K, McNamara J. A, Jr, Franchi L, Baccetti T. Short-term skeletal and dental effects of the acrylic splint rapid maxillary expansion appliance. Angle Orthod. 2005;75:7–14. doi: 10.1043/0003-3219(2005)075<0007:APSOTS>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Lima R. M, Lima A. C, de Oliveras Ruellas A. C. Spontaneous correction of Class II malocclusion after rapid palatal expansion. Angle Orthod. 2003;73:745–752. doi: 10.1043/0003-3219(2003)073<0745:SCOCIM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Dahlberg G. Statistical Methods for Medical and Biological Students. New York: Interscience Publications; 1940. [Google Scholar]
- 13.Cohen J. Statistical Power Analysis for the Behavioral Sciences 2nd ed. Hillsdale, NJ: Lawrence Erlbaum; 1988. [Google Scholar]
- 14.Chang J. Y, McNamara J. A, Jr, Herberger T. A. A longitudinal study of skeletal side effects induced by rapid maxillary expansion. Am J Orthod Dentofac Orthop. 1997;112:330–337. doi: 10.1016/S0889-5406(97)70264-6. [DOI] [PubMed] [Google Scholar]
- 15.Zablocki H. L, McNamara J. A, Jr, Franchi L, Baccetti T. Effect of the transpalatal arch during extraction treatment. Am J Orthod Dentofac Orthop. 2008;133:852–860. doi: 10.1016/j.ajodo.2006.07.031. [DOI] [PubMed] [Google Scholar]