

Abstract
Objectives:
To test the null hypotheses that supplementation of verbal information with written information when obtaining consent to orthodontic treatment has no effect on (1) anxiety, motivation and apprehension related to treatment and (2) compliance in the early stages of fixed appliance therapy.
Materials and Methods:
Seventy-six adolescents who were due to start fixed appliance therapy were randomly allocated to receive verbal information only or verbal and written information before orthodontic treatment. Participants' anxiety, motivation, and apprehension were assessed using a questionnaire that was completed prior to meeting the orthodontic clinician (T1), following consent to treatment (T2), and after 12 weeks of treatment (T3). Appointment attendance, appliance breakages, and periodontal scores were used as measures of patient compliance.
Results:
Sixty participants completed the study. At T2 there was no change in anxiety scores for either group (P = .412); however, increased motivation was detected in the group that had been given both written and verbal information (P = .049). At T3 both groups demonstrated similar reductions in anxiety (P = .311) and apprehension (P = .790) and similar levels of motivation (P = .756). A reduction in periodontal scores (P = .065), better appointment attendance (P = .732), and fewer breakages (P = .525) were reported in the group that was given additional information, although these changes were not statistically significant.
Conclusions:
Supplementation of verbal information with written information resulted in improved motivation for orthodontic treatment but had no statistically significant effect on anxiety, apprehension, or patient compliance.
Keywords: Health education, Adolescent orthodontic anxiety, Adolescent orthodontic compliance
INTRODUCTION
Concerns relating to discomfort and the psychosocial implications of wearing fixed appliances can lead to high levels of anxiety, especially at the beginning of treatment.1 Patients who are anxious and poorly informed regarding the risks of orthodontic treatment may fail to attend appointments and demonstrate poor compliance.2 In a recent study of 51 orthodontists, adequate verbal and nonverbal communication promoted compliance during treatment.3
Information may be provided orally, verbally, with visual aids including videotapes, or in combination.4,5 Improved recall has been described when oral information was supplemented by written and visual material.6 However, simple provision of more information does not necessarily result in greater patient understanding.7
There has been extensive research into improving provision and retention of information.3,4,7,8 However, few studies have explored the relationship between adolescent anxiety, apprehension, motivation, and compliance in orthodontics.
The present study sought to investigate the effects of providing additional written information during the consent process on adolescents' anxiety, apprehension, motivation, and compliance in the preliminary stages of orthodontic treatment.
MATERIALS AND METHODS
Ethical approval was obtained from the East London and City Ethics Committee before the trial commenced (07/Q0603/43, April 2007). A randomized, controlled, questionnaire-based study was carried out at the Royal London Dental Institute between April 2007 and May 2008.
All patients were between 12 and 16 years of age, had not undergone orthodontic treatment previously, and required dual-arch fixed appliance therapy. A computer-generated unstratified allocation sequence was used to randomize participants into two groups. Participants in the intervention group received both verbal and written information when consenting to orthodontic treatment, whereas participants in the control group received verbal information only. The written information was in a leaflet format about fixed appliances. It was designed, illustrated, and written to be both appealing and comprehensible to children. A Gunning Fog test was applied to assess readability prior to use.
Subsequent to initial pilot testing of the questionnaire and information leaflet, the content of the verbal information given was standardized according to the British Orthodontic Society guidelines9 on fixed appliances. It was decided that the chief investigator (NSW) should also read through the leaflet given to participants in the intervention group. Throughout the study, both the participants and treating clinicians were blinded to group allocation, although the investigator responsible for obtaining consent (NSW) was not blinded.
Participants completed questionnaires prior to meeting the orthodontic clinician (T1), following consent to treatment approximately 4 weeks later (T2), and after 12 weeks of treatment (T3). The first six questions of the questionnaire were based on a short form of Spielberger's State-Trait Anxiety Inventory10,11 that was used to measure the patients' current state of anxiety. It comprised six statements:
I feel calm.
I am tense.
I feel upset.
I am relaxed.
I feel content.
I am worried.
Participants answered by selecting from four available responses that ranged from “not at all” to “very much.” Scores were summed, yielding a total that could range from 6 (not at all anxious) to 24 (very anxious).
The second part of the questionnaire consisted of questions designed from focus group interviews to assess motivation and apprehension using a visual analogue scale (VAS).12 This was a horizontal 10-cm line anchored by 0 (“not at all”) and 10 (“very much”); responses were made by placing a vertical line on the scale. Six questions assessed motivation:
Do your teeth bother you?
If it was possible, how much would you like to change the appearance of your teeth?
Do you think your teeth need straightening?
Do you think orthodontic treatment is good for your health?
How motivated are you to have orthodontic treatment with braces?
Was it your own decision to undergo orthodontic treatment?
The final four questions measured apprehension:
Do you think it is going to be difficult to wear braces?
Are you worried about having orthodontic treatment?
Are you worried about how you are going to look with braces on?
Have you ever been teased about the appearance of your teeth?
To determine the overall motivation and apprehension scores, the authors multiplied the results by 10 and calculated the mean for each domain; higher scores reflected higher levels of motivation or apprehension. Finally, a basic periodontal examination was undertaken by one investigator to detect active inflammation; scores for each sextant were combined to give an overall score. In addition, missed appointments and casualty attendance due to fixed appliance breakage were recorded as a measure of compliance.
Participants were asked to complete the questionnaire at three appointments (Figure 1). To determine the reproducibility of the questionnaire, 20% of the participants completed two further questionnaires with at least 60 minutes allowed to pass between completion of the first and second questionnaire. To avoid bias resulting from the learning effect, participants were not provided with additional information between the two assessments.
Figure 1.
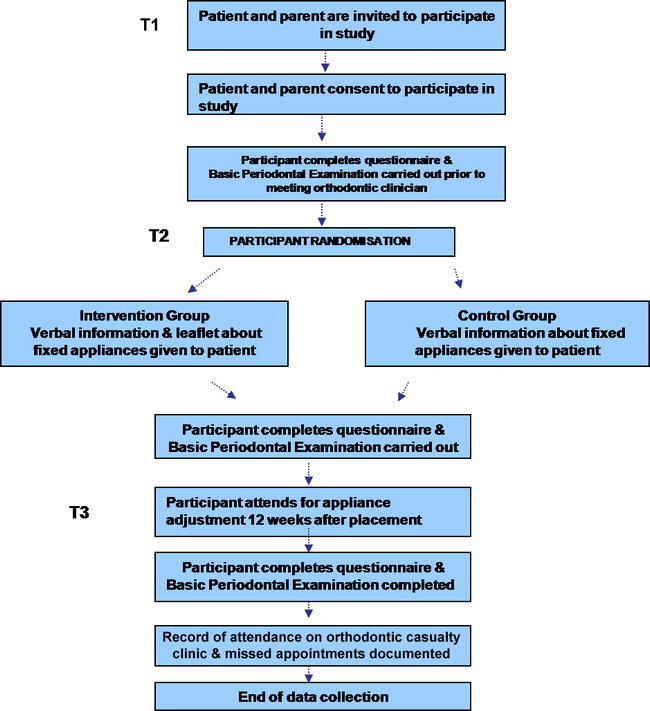
Flow chart of the study at stages T1, T2, and T3.
Statistics
Data were entered into SPSS software (version 13.0, Chicago, Ill) for analysis. Because the data did not follow a normal distribution, the Mann-Whitney U-test was used to compare changes between the groups throughout the study. A P value of .05 was considered significant. The reproducibility of the shortened version of the State-Trait Anxiety Inventory was confirmed using Bland and Altman's technique.13
RESULTS
Over a 13-month period, 76 patients (control group n = 38; intervention group n = 38) were recruited and completed the initial stages of the study (T1 and T2). Sixteen participants were lost to follow-up (Figure 2).
Figure 2.
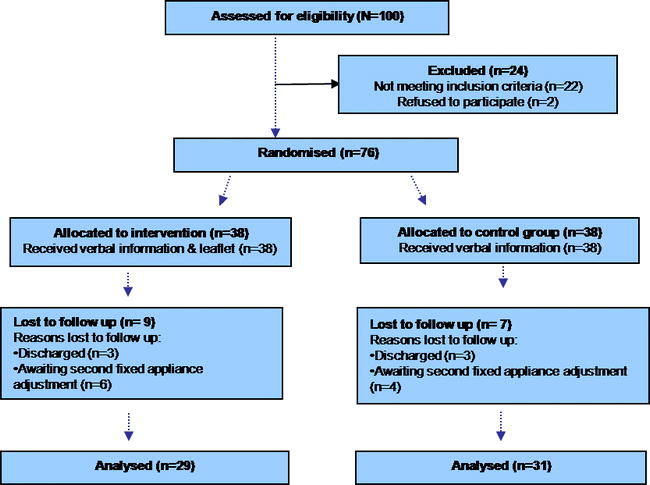
Flow chart of participants through the study.
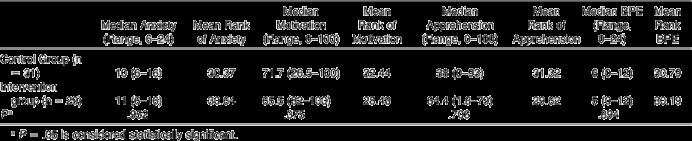
The study population was predominantly female (64%) and had a mean age of 13 years (42%). At T1 the two groups were similar with respect to gender (P = .734) and age (P = .649). There were also no statistically significant differences between the groups at the outset with respect to anxiety, treatment motivation, apprehension, and basic periodontal examination scores (Table 1).
Table 1.
Medians, Ranges, Mean Ranks, and P Values for Anxiety, Motivation, Apprehension, and Basic Periodontal Examination (BPE) Scores Recorded at T1 for the Control and Intervention Groups
There was no median change in anxiety scores for either group between T1 and T2 (P = .412; Table 2). There was a statistically significant difference in motivation scores between the groups after consent to orthodontic treatment, with the intervention group becoming more motivated (P = .049).
Table 2.
Median Changes,a Mean Ranks, and P Values for Anxiety, Motivation, Apprehension, and Basic Periodontal Examination (BPE) Scores Between T1 and T2 for the Control and Intervention Groups
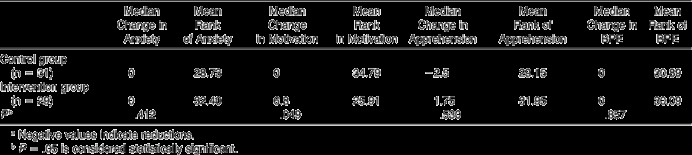
Although a generalized reduction in anxiety, motivation, and apprehension as treatment progressed was demonstrated by the negative differences between T1 and T3 for both groups, these differences were not significant (Table 3). The intervention group's periodontal condition improved between T1 and T3, in contrast to the control group's periodontal condition, which deteriorated, although the change was not statistically significant (P = .065). A greater number of failed appointments and appliance breakages were recorded in patients who had not been given supplemental information, but this difference also failed to reach statistical significance (Figures 3 and 4).
Table 3.
Median Changes,a Mean Ranks, and P Values for Anxiety, Motivation, Apprehension, and Basic Periodontal Examination (BPE) Scores Between T1 and T3 for the Control and Intervention Groups
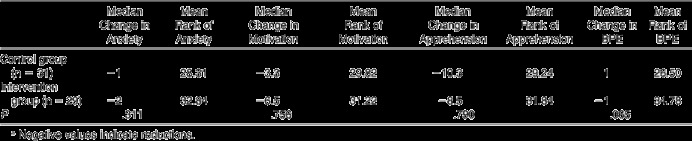
Figure 3.
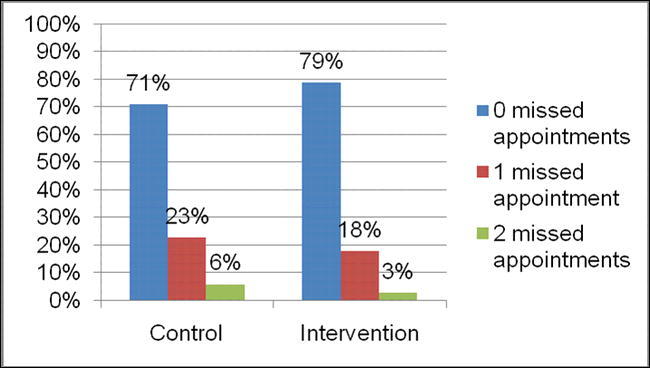
Missed appointments during the study.
Figure 4.
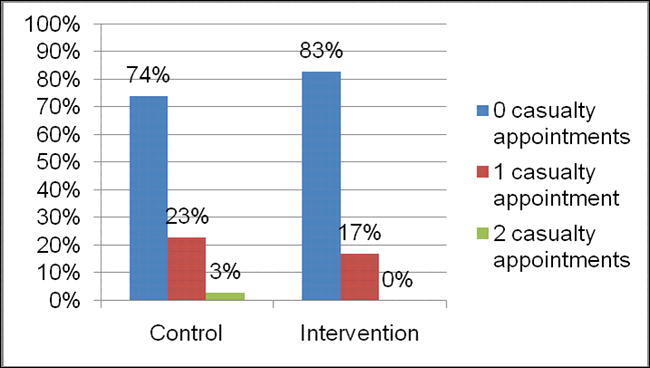
Attendance at the orthodontic casualty clinic.
DISCUSSION
Factors influencing the overall adolescent treatment experience include a preoccupation with dental appearance as a result of teasing,14 desire to undergo treatment, and preconceived ideas of what treatment involves15 and what it can achieve. Supplemental information has been shown to improve information recall,7 which could translate into enhanced compliance and motivation. In addition, information about the nature and extent of malocclusion and the necessary treatment may allow patients to feel greater emotional control and to perceive less discomfort during orthodontic treatment.16
It was, therefore, expected that participants would be less anxious following the provision of supplementary information during the consent process; however, both groups exhibited the same median anxiety score following consent to treatment, regardless of what information had been provided (P = .530). This finding may be related to the use of photographs in the information leaflet depicting demineralization and gingivitis that were the result of poor oral hygiene and dental neglect. This finding is in agreement with Kerrigan et al,17 who proposed that extensive information can compound apprehension.
This outcome contrasts with the findings of Jackson and Lindsay,18 who reported that anxiety before treatment in new dental patients was reduced following provision of an informative leaflet. However, in the present study, anxiety scores had fallen at 12 weeks following commencement of fixed appliance therapy. This is not surprising, since by this point in therapy participants are typically conditioned to treatment and have learned to manage associated discomfort. These findings are in agreement with those of Sari et al,1 who reported that patients undergoing orthodontic treatment for 12 months had lower anxiety levels than those about to embark on treatment.
The disparity in motivation scores between the groups following consent to orthodontic treatment suggests that the leaflet had a beneficial effect; the intervention group was significantly more motivated (P = .049). This enhanced motivation was reflected in fewer missed appointments and appliance breakages and enhanced periodontal scores in this group. However, the differences failed to reach statistical significance; this may be a reflection of inadequate statistical power because of the small patient sample.
The importance of good oral hygiene when fixed appliances are in place was emphasized during the consent process. Deterioration in the oral hygiene and periodontal condition of participants in the control group suggests that verbal information alone may be insufficient. Similar results were found in a study by Redmond et al,19 who observed a positive effect on oral health behavior with a reported increased frequency in brushing following provision of oral health promotion leaflets for young adolescents.
Missed appointments and appliance breakages are known to prolong orthodontic treatment by at least 6 weeks.20 Increased treatment duration is also known to be linked to deleterious effects, including root resorption21 and decalcification. Consequently, the likelihood of prolonged treatment along with poor oral hygiene in patients given insufficient information confirms the value of detailed and effective information provision as part of the informed consent process.
Lew22 found that improvement in dentofacial appearance is the most important single factor motivating both patients and parents to seek orthodontic treatment. This would help to explain the positive impact of the leaflet, which illustrated the improvements that could be achieved and reinforced the participants' desire and motivation for treatment.
The initial positive effect of written information on treatment motivation was not always sustained. This may be a result of the participants' poor retention of information. Limited retention of information has been noted in other studies,3,23 highlighting the need to remind patients of key information at follow-up appointments.
CONCLUSIONS
Supplementation of verbal information with detailed written information during the consent process had a positive effect on motivation without influencing levels of treatment-related anxiety and apprehension.
This provision of written information could result in enhanced patient compliance with fewer missed appointments and appliance breakages, but this finding was not statistically significant.
REFERENCES
- 1.Sari Z, Uysal T, Karaman A. L, Sargin N, Ure O. Does orthodontic treatment affect patients' and parents anxiety levels? Eur J Orthod. 2005;27:155–159. doi: 10.1093/ejo/cjh072. [DOI] [PubMed] [Google Scholar]
- 2.Thickett E, Newton J. T. Using written material to support recall of orthodontic information: a comparison of three methods. Angle Orthod. 2006;76:243–250. doi: 10.1043/0003-3219(2006)076[0243:UWMTSR]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.Bos A, Hoogstraten J, Prahl-Andersen B. Towards a comprehensive model for the study of compliance in orthodontics. Eur J Orthod. 2005;27(3):296–301. doi: 10.1093/ejo/cji003. [DOI] [PubMed] [Google Scholar]
- 4.Patel J. H, Moles D. R, Cunningham S. J. Factors affecting information retention in orthodontic patients. Am J Orthod Dentofacial Orthop. 2008;133:61–67. doi: 10.1016/j.ajodo.2007.07.019. [DOI] [PubMed] [Google Scholar]
- 5.Lees A, Rock W. P. A comparison between written, verbal, and videotape oral hygiene instruction for patients with fixed appliances. J Orthod. 2000;27:323–327. doi: 10.1093/ortho/27.4.323. [DOI] [PubMed] [Google Scholar]
- 6.Thomson A. M, Cunningham S. J, Hunt N. P. A comparison of information retention at an initial orthodontic consultation. Eur J Orthod. 2001;23(2):169–178. doi: 10.1093/ejo/23.2.169. [DOI] [PubMed] [Google Scholar]
- 7.Mortensen M. G, Kiyak H. A, Omnell L. Patient and parent understanding of informed consent in orthodontics. Am J Orthod Dentofacial Orthop. 2003;124:541–550. doi: 10.1016/s0889-5406(03)00639-5. [DOI] [PubMed] [Google Scholar]
- 8.Sheard C, Garrud P. Evaluation of generic patient information: effect on health outcomes, knowledge and satisfaction. Patient Educ and Couns. 2006;61:43–47. doi: 10.1016/j.pec.2005.02.004. [DOI] [PubMed] [Google Scholar]
- 9.Fixed appliances information leaflet. London: British Orthodontic Society; 2007. Available at: http://www.bos.org.uk/publicationslinks/patientinformationleaflets/fixedappliances.htm Accessed August 14, 2009. [Google Scholar]
- 10.Marteau T. M, Bekker H. The development of a six-item short form of the state scale of the Spielberger State-Trait Anxiety Inventory (STAI) Br J Clin Psychol. 1992;31:301–306. doi: 10.1111/j.2044-8260.1992.tb00997.x. [DOI] [PubMed] [Google Scholar]
- 11.Spielberger C. D, Gorsuch R. L. Manual for the StateTrait Anxiety Inventory (Form Y) Palo Alto, CA: Consulting Psychologists Press; 1983. pp. 1–5. [Google Scholar]
- 12.Feldmann I, List T, John M. T, Bondermark L. Reliability of a questionnaire assessing experiences of adolescents in orthodontic treatment. Angle Orthod. 2007;77:311–317. doi: 10.2319/0003-3219(2007)077[0311:ROAQAE]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Bland J. M, Altman D. G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986:307–310. [PubMed] [Google Scholar]
- 14.Shaw W. C, Meek S. C, Jones D. S. Nicknames, teasing, harassment, and the salience of dental features among school children. Br J Orthod. 1980;7:75–80. doi: 10.1179/bjo.7.2.75. [DOI] [PubMed] [Google Scholar]
- 15.Habibian M, Gelbier S, Munday B. A. Perceived information needs in respect of orthodontics amongst 11–12-year-old girls: a study through health visitor sessions in schools. Int J Paediatr Dent. 2003;13:348–355. doi: 10.1046/j.1365-263x.2003.00486.x. [DOI] [PubMed] [Google Scholar]
- 16.Sergl H. G, Klages U, Zentner A. Pain and discomfort during orthodontic treatment: causative factors and effects on compliance. Am J Orthod Dentofacial Orthop. 1998;114:684–669. doi: 10.1016/s0889-5406(98)70201-x. [DOI] [PubMed] [Google Scholar]
- 17.Kerrigan D. D, Thevasagayam R. S, Woods T. O, McWelch I, Thomas W. E, Shorthouse A. J, Dennison A. R. Who's afraid of informed consent? BMJ. 1993;306:298–300. doi: 10.1136/bmj.306.6873.298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jackson C, Lindsay S. Reducing anxiety in new dental patients by means of leaflets. Br Dent J. 1995;179:163–167. doi: 10.1038/sj.bdj.4808865. [DOI] [PubMed] [Google Scholar]
- 19.Redmond C. A, Hamilton F. A, Kay E. J, Worthington A. V, Blinkhorn A. S. An investigation into the value and relevance of oral health promotion leaflets for young adolescents. Int Dent J. 2001;51:164–168. doi: 10.1002/j.1875-595x.2001.tb00834.x. [DOI] [PubMed] [Google Scholar]
- 20.Skidmore K. J, Brook K. J, Thomson W. M, Harding W. J. Factors influencing treatment time in orthodontic patients. Am J Orthod Dentofacial Orthop. 2006;129:230–238. doi: 10.1016/j.ajodo.2005.10.003. [DOI] [PubMed] [Google Scholar]
- 21.Apajalahti S, Peltola J. S. Apical root resorption after orthodontic treatment—a retrospective study. Eur J Orthod. 2007;29:408–411. doi: 10.1093/ejo/cjm016. [DOI] [PubMed] [Google Scholar]
- 22.Lew K. K. Attitudes and perceptions of adults towards orthodontic treatment in an Asian Community. Community Dent Oral Epidemiol. 1993;21:21–35. doi: 10.1111/j.1600-0528.1993.tb00715.x. [DOI] [PubMed] [Google Scholar]
- 23.Ley P. Communicating with Patients. London: Croom Helm; 1988. [Google Scholar]