

Abstract
Public abortion attitudes are important predictors of abortion stigma and accessibility, even in legal settings like the U.S. and South Africa. With data from the U.S. General Social Survey and South African Social Attitudes Survey, we used ordinal logistic regressions to measure whether abortion acceptability (in cases of poverty and fetal anomaly) is related to attitudes about social welfare programs and gender roles, then assessed differences by race/ethnicity and education. Social welfare program attitudes did not correlate with abortion acceptability in the U.S., but in South Africa, greater support for income equalization (OR: 0.59, 95% CI: 0.41–0.85) and increased government spending on the poor (OR: 0.66, 95% CI: 0.49–0.91) correlated with lower abortion acceptability in circumstances of poverty. This was significant for Black African and higher educated South Africans. In the U.S., egalitarian gender role attitudes correlated with higher acceptability of abortion in circumstances of poverty (OR: 1.18, 95% CI: 1.03–1.36) and fetal anomaly (OR: 1.15, 95% CI: 1.01–1.31). This was significant for White and less educated Americans. In South Africa, egalitarian gender role attitudes correlated with higher abortion acceptability for fetal anomaly (OR: 1.12, 95% CI: 1.01–1.25) overall and among Black and less educated respondents, but among non-Black South Africans they correlated with higher abortion acceptability in circumstances of poverty. These results suggest abortion attitudes are distinctly related to socioeconomic and gender ideology depending one’s national context, race/ethnicity, and socioeconomic status. Reducing abortion stigma will require community-based approaches rooted in intersectional reproductive justice frameworks.
Keywords: Abortion attitudes, gender attitudes, social welfare program attitudes
Introduction
Understanding public abortion attitudes is vital for global health and human rights, because they affect public policies and the social contexts of women’s reproductive decision-making around the world (Jelen, 2015; Jelen & Wilcox, 2003). Negative abortion attitudes can erect barriers to safe abortion care across multiple socio-ecological levels from individuals to institutions and social norms more generally. Women who hold ambivalent or shameful abortion attitudes can delay care-seeking or resort to abortions outside the formal health sector (Foster, Gould, Taylor, & Weitz, 2012; Foster & Kimport, 2013; Harries, Orner, Gabriel, & Mitchell, 2007; Varga, 2002). If women’s intimate partners and family members harbor negative abortion attitudes, this can create interpersonal conflict (Foster et al., 2012; Harries et al., 2007; Varga, 2002), and when health workers are disapproving of abortion, they can dramatically reduce availability and quality of abortion care (Gresh & Maharaj, 2011; Harries, Cooper, Strebel, & Colvin, 2014; Harries, Stinson, & Orner, 2009; Wheeler, Zullig, Reeve, Buga, & Morroni, 2012). Public abortion attitudes can also sway public policy on abortion (for example, funding restrictions, gestational limits, and mandatory waiting periods) and the political composition of governments (Jelen & Wilcox, 2003; Killian & Wilcox, 2008; Medoff & Dennis, 2011). Finally, negative abortion attitudes collectively contribute to perceived and actual social norms of abortion (Shellenberg, Hessini, & Levandowski, 2014; Varga, 2002). When people and systems act upon those attitudes to oppress women who seek abortion care, then abortion attitudes have directly and indirectly contributed to stigma – the social process of ascribing negative attributes to, stereotyping, essentializing, and discriminating against people associated with abortion (Harris, Debbink, Martin, & Hassinger, 2011; Kumar, Hessini, & Mitchell, 2009; Norris et al., 2011).
Discourse surrounding abortion attitudes is highly polarized and intractable, and novel research approaches are needed to build shared understanding for improved abortion acceptability and accessibility. For one, cross-national comparative studies could offer new insights, because they allow for analyses at the country level that unveil similarities and differences that can be obscured when focusing on a single context (Hoffmeyer-Zlotnik & Harkness, 2005). In fact, there has been a concerted effort among social attitude researchers globally to improve the comparability of survey items across countries in order to analyze global trends in public opinion and to identify how social attitudes are sensitive to local contexts – that is, to discern what social phenomenon are true of all societies versus what is true of one society and why (Hoffmeyer-Zlotnik & Harkness, 2005). This has resulted in development of large-scale, multi-national projects such as the International Social Survey Programme, which includes the U.S. General Social Survey (GSS) and the South African Social Attitudes Survey (SASAS) (International Social Survey Programme, 2019).
Further, using a reproductive justice approach (Luna & Luker, 2013; Ross, 2006) rather than the commonly-used reproductive rights framework (United Nations, 1994; 2014), might illuminate often-marginalized perspectives on abortion. Reproductive rights were defined as:
the recognition of the basic right of all couples and individuals to decide freely and responsibly the number, spacing, and timing of their children and to have the information and means to do so…free of discrimination, coercion, and violence
In some settings, the reproductive rights framework has been used to advocate for abortion and contraception, often at the expense of low-income women and women of color, who often face unsupportive social conditions that deny parents the ability to raise children with good health, safety, and dignity (Davis, 2003; Luna & Luker, 2013; Smith, 2005). In contrast, reproductive justice – both a social theory and a community organizing movement – emphasizes intersectionality between gender, race/ethnicity, and class (Crenshaw, 1989); centers the experiences of low-income and women of color; and addresses underlying social inequalities (Luna & Luker, 2013; Ross, 2006). Reproductive justice includes the human rights to have children and to raise those children safely, in addition to the right to control one’s fertility with contraception and abortion (Luna & Luker, 2013; Ross, 2006).
South Africa and the U.S. are particularly interesting for comparative analysis of abortion attitudes given the salience of reproductive injustice in these two countries, which share poignant similarities in their histories of settler colonialism (Frederickson, 1982), slavery (Frederickson, 1982), and population control of non-White and impoverished communities (Bradford, 1991; Davis, 2003; Hodes, 2013; Kuumba, 1993; Schoen, 2005; Stern, 2005). Historically, eugenic campaigns in both countries sought to curb population growth among low-income and non-White communities through forced and coercive means (Hodes, 2013; Schoen, 2005). Today, both South Africa and the U.S. have large social and health inequities by gender, race/ethnicity, and class (Baker, 2010;Coovadia, Jewkes, Barron, Sanders, & McIntyre, 2009; Mullings & Schulz, 2006; Williams, Mohammed, Leavell, & Collins, 2010) including higher risk of unsafe abortion for lower income women and women of color (Fried, 2000; Grossman et al., 2015; Grossman et al., 2010, 2014; Trueman & Magwentshu, 2013). Further investigation would help identify common pathways and processes shaping abortion attitudes and the extent to which they are similar and different across two countries with eugenic histories, contemporary social inequities, and multiple (often conflicting) social ideologies. Given that historical and contemporary reproductive injustices in these two settings have been explicitly racialized and classed, analyses of abortion attitudes that explore differences and similarities across race/ethnicity and socioeconomic status are particularly warranted.
Previous studies in the U.S., South Africa, and around the world have focused on circumstances of pregnancy, attitudes and norms of sexuality, and religion as major predictors of abortion attitudes (Barkan, 2014; Elias, Fullerton, & Simpson, 2015; Jelen & Wilcox, 2003; Patel & Myeni, 2008; 2008; Strickler & Danigelis, 2002; Varga, 2002). Researchers have also demonstrated that gender role attitudes are consistent (albeit weak) predictors of abortion attitudes globally (Carter, Carter, & Dodge, 2009; Jelen, 2015; Strickler & Danigelis, 2002), but small-scale surveys with undergraduate students suggest gender role attitudes might be insignificant in the South African context (Patel & Johns, 2009). Less is known about the potential influences of attitudes toward social welfare programs (i.e., one’s beliefs about income inequality and government assistance for the poor). One study comparing abortion acceptability in the U.S. and Japan found that the locus of responsibility for poverty varies across cultures based on their orientation to the group or individual, and that these cultural differences can influence abortion attitudes (Sahar & Karasawa, 2005). Unlike the U.S., where personal responsibility and individualism dominate national ethos (Sahar & Karasawa, 2005), South Africa is generally oriented toward collectivism and communal practices such as pooling household resources and child-rearing with extended family (Whitworth & Wilkinson, 2013). Notably, this work has inadequately explored non-Black minority groups. It remains unclear whether South African collectivism and/or U.S. individualism influence abortion attitudes or how those relationships might vary across racial/ethnic and socioeconomic groups.
The current study aims to address existing gaps in the literature by: 1) measuring the relationship between abortion attitudes and social welfare program attitudes, 2) examining how attitudes toward gender roles in the family are related to abortion attitudes, and 3) exploring if and how those relationships differ by race/ethnicity and socioeconomic status in the U.S. and South Africa.
Materials and methods
Using the GSS (National Opinion Research Center, 2017) and the SASAS (Human Sciences Research Council, 2015), we assessed the univariate distributions, bivariate relationships, and multivariable ordinal logistic regression models of abortion attitudes, our predictors of interest, and covariates in Stata v. 14 (StataCorp, 2014). A cross-national comparison of these two surveys is not only appropriate but closely aligned with the very purpose of these large-scale research initiatives. Among the numerous aims of the GSS are to ‘monitor and explain trends and constants in attitudes, behaviors, and attributes’ and ‘to compare the United States to other societies in order to place American society in comparative perspective and develop cross-national models of human society’ (National Opinion Research Center, 2018). Similarly, the SASAS is a tool for ‘monitoring change and continuity in a variety of social, economic, and political values over time’ in South Africa, and as a member of cross-national collaborations (e.g., International Social Survey Programme, European Social Survey), it has ‘been able to add an international perspective’ that allows researchers ‘to continually question whether [South African] society is exceptional by identifying commonalities and differences in values with other nations’ (Human Sciences Research Council, 2015).
The GSS is a nationally-representative survey with a multi-stage, full probability sample of the non-institutionalized adult U.S. population including English- and Spanish-speaking individuals (National Opinion Research Center, 2017). The primary sampling units for the GSS are standard metropolitan statistical areas stratified by region, age, and race; the units of selection in the second stage are block groups stratified by race and income (National Opinion Research Center, 2017). Researchers have surveyed approximately 1,300–4,500 individuals almost annually since 1972 (National Opinion Research Center, 2017).
The SASAS also gathers data from a nationally-representative, repeated cross-sectional sample, which is drawn from 1,000 population enumeration areas that are stratified by province, urbanicity, and majority racial group (Human Sciences Research Council, 2015). Researchers have surveyed 3,500–7,000 individuals annually since 2003; respondents must be 16 years or older and residing in South Africa regardless of nationality or citizenship (Human Sciences Research Council, 2015). Notably, while all variables of interest were measured on the 2008 GSS, not all were available from a single year in South Africa. We first used the most recent South African survey from 2016 that included all social welfare program attitudes, then the survey from 2008 that included all gender role attitudes. The original descriptions and response categories for all variables can be found in Table 1.
Table 1.
Variable descriptions from the U.S. general social surveys and the South African social attitudes surveys.
| U.S. General Social Survey | South African Social Attitudes Survey | ||
|---|---|---|---|
| Variable | Original Description | Variable | Original Description |
| Abortion Morality in Case of Fetal Anomaly | Always wrong, almost always wrong, wrong only sometimes, not wrong at all: Do you personally think it is wrong or not wrong for a woman to have an abortion if there is a strong chance of serious defect in the baby? | Abortion Morality in Case of Fetal Anomaly (reverse coded) | Not wrong at all, wrong only sometimes, almost always wrong, always wrong: Do you personally think it is wrong or not wrong for a woman to have an abortion if there is a strong chance of serious defect in the baby? |
| Abortion Morality in Case of Poverty | Always wrong, almost always wrong, wrong only sometimes, not wrong at all: Do you personally think it is wrong or not wrong for a woman to have an abortion if the family has a very low income and cannot afford any more children? | Abortion Morality in Case of Poverty (reverse coded) | Not wrong at all, wrong only sometimes, almost always wrong, always wrong:: Do you personally think it is wrong or not wrong for a woman to have an abortion if the family has a very low income and cannot afford any more children? |
| Support for Gender Equality in Household Roles | Strongly agree, agree, disagree, or strongly disagree: It is much better for everyone involved if the man is the achiever outside the home and the woman takes care of the home and family. | Support for Gender Equality in Household Roles | Strongly agree, agree, neutral, disagree, or strongly disagree: It is much better for everyone involved if the man is the achiever outside the home and the woman takes care of the home and family. |
| Support for Working Motherhood with Preschoolers | Strongly agree, agree, disagree, or strongly disagree: A preschool child is likely to suffer if his or her mother works. | Support for Working Motherhood with Preschoolers | Strongly agree, agree, neutral, disagree, or strongly disagree: A preschool child is likely to suffer if his or her mother works. |
| Support for Working Motherhood (reverse coded) | Strongly agree, agree, disagree, or strongly disagree: A working mother can establish just as warm and secure a relationship with her children as a mother who does not work. | Support for Working Motherhood (reverse coded) | Strongly agree, agree, neutral, disagree, or strongly disagree: A working mother can establish just as warm and secure a relationship with her children as a mother who does not work. |
| Support for Income Equalization (reverse coded) | Some people think that the government in Washington ought to reduce the income differences between the rich and the poor (1).. Others think that the government should not concern itself with reducing this income difference between the rich and the poor (7). | Support for Income Equalization (reverse coded) | Strongly agree, agree, neutral, disagree, or strongly disagree: It is the responsibility of the government to reduce the differences in income between people with high incomes and those with low incomes. |
| Support for Standard of Living (reverse coded) | Some people think that the government in Washington should do everything possible to improve the standard of living of all poor Americans (1)…Other people think it is not the government’s responsibility, and that each person should take care of himself (5). | Support for Standard of Living (reverse coded) | Strongly agree, agree, neutral, disagree, or strongly disagree: The government should provide a decent standard of living for the unemployed. |
| Support for Increased Funding for the Poor (re-coded 1-too much, 2-about right, 3-too little) | I’d like you to tell me whether you think we’re spending too little money (1), about the right amount (2), or too much money (3) on assistance to the poor. | Support for Increased Funding for the Poor | Strongly agree, agree, neutral, disagree, or strongly disagree: The government should spend less on benefits for the poor. |
Abortion attitudes
Respondents for the GSS and SASAS were asked, ‘Do you personally think it is wrong or not wrong for a woman to have an abortion if there is a strong chance of serious defect in the baby?’ and ‘Do you personally think it is wrong or not wrong for a woman to have an abortion if the family has a very low income and cannot afford any more children?’ Their answer choices were ‘always wrong,’ ‘almost always wrong,’ ‘wrong only sometimes,’ or ‘not wrong at all.’
Social welfare program attitudes
The 2008 GSS and 2016 SASAS measured attitudes toward government equalizing income differences, government providing a decent standard of living for the poor/unemployed, and government spending on the poor. The response categories were slightly different in the two countries (see Table 1), so we collapsed the responses in order to create comparable measures. Attitudes toward government equalization of income were measured as 1) government should not equalize incomes between the rich and poor, (2) neither/neutral, or 3) government should equalize incomes between the rich and poor. Attitudes about the government providing a decent standard of living were 1) government should not improve or provide a decent standard of living for the poor, 2) neither/neutral, or 3) government should improve or provide a decent standard of living for the poor. And attitudes about government spending on the poor were measured as 1) government is spending too much on the poor, 2) neutral/government is spending about the right amount, or 3) government should spend more on benefits for the poor.
We used principal component analysis with a loading cut-off at 0.50 to determine whether these three variables could be combined into a single measure that captures the latent component ‘attitudes about social welfare programs.’ In the U.S., all three variables sufficiently loaded (>0.50) onto the first principal component (Eigenvalue = 1.80). Results from South Africa, however, suggested these three variables do not sufficiently load on a single component (Eigenvalue = 1.31; loadings = 0.71income equalization, 0.69standard of living, −0.09spending on the poor). In order to preserve comparability of results across the two countries, we opted to include the three social welfare program attitudes as separate constructs in our models.
Gender role attitudes
To explore the effects of gender role attitudes, we then compared the 2008 GSS to the 2008 SASAS, both of which measured agreement/disagreement with the beliefs that 1) men should be earners and women should be homemakers; 2) preschool-aged children suffer when their mothers work; and 3) that working mothers cannot form equally strong bonds with their children as stay-at-home mothers. We again used principal component analysis with a loading cut-off at 0.50 to combine these three variables into a single, continuous measure in both countries. The principal component analyses suggested a single latent component in both the U.S. (Eigenvalue = 1.86) and South Africa (Eigenvalue = 1.44), and all three variables loaded sufficiently (>0.50) in both countries. We called this latent factor ‘support for egalitarian gender roles,’ where higher scores indicate more egalitarian attitudes. On the 2016 SASAS, family gender roles were not available.
Group differences by race/ethnicity and educational status
To assess group differences in South Africa and the U.S. by race/ethnicity and socioeconomic background, we stratified the models by race/ethnicity and education. In South Africa, we operationalized race/ethnicity as a single variable constructed from population racial group (‘Black African,’ ‘Coloured,’ ‘Indian,’ or ‘White’) and language spoken at home. For stratified analyses, we compared Black African to all other race/ethnicities, because Black Africans are the largest racial/ethnic majority. In the U.S., we operationalized race/ethnicity as ‘non-Hispanic White,’ ‘non-Hispanic Black,’ ‘Hispanic,’ or ‘other non-Hispanic.’ For stratified analyses we compared White to all other race/ethnicities, because White is the majority racial/ethnic group.
We measured education in quartiles for comparability across the U.S. and South Africa, given that education levels are significantly different across the two countries. In the U.S., this was ‘less than high school,’ ‘completed high school,’ ‘completed at least 2 years tertiary education,’ and ‘completed 4 years tertiary education.’ For stratified models, we dichotomized at ‘completed high school’ or less compared to any tertiary education, which approximated an even split into two samples. In South Africa the education categories were ‘primary school or less,’ ‘some secondary school,’ ‘completed secondary school,’ and ‘any tertiary education.’ For stratified models, we again dichotomized at ‘some secondary school’ or less compared to completed secondary school or more, in order to create two even subsamples.
Covariates and missing data
All multivariable models also controlled for gender, marital status, acceptability of premarital sex, age, liberalism/conservatism, religious denomination, religiosity, region, urbanicity, and household income. On the GSS, respondent’s annual household income was measured categorically with 12 categories (e.g., less than $1,000; $1,000–$2,999; $3,000–$3,999; etc.). We dichotomized U.S. income at $25,000 for two reasons. First, the data were highly skewed with a minority of respondents reporting below $25,000; second, this approximates the federal poverty level ($24,800) for a 5-person household in the U.S. in 2008 (Office of the Assistant Secretary for Planning and Evaluation, 2008). On the SASAS, a respondent’s monthly income was measured categorically with 15 categories (e.g., 0–500 Rand; 501–750 Rand; 751–1,000 Rand; 1,001–1,500 Rand, etc.). In 2008, the upper-bound federal poverty line in South Africa was 682 Rand per person per month (~$50 USD), and in 2016 it was 1,077 Rand per person per month (~$75 USD) (Statistics South Africa, 2017). In order to make this measure comparable to the U.S., we dichotomized at 3,000 Rand in 2008 and at 5,000 Rand in 2016 to approximate the federal poverty level for those years. For U.S. analyses, we also employed multiple imputation for data missing completely-at-random due to the GSS split-ballot design. Elsewhere, we used complete case analysis and dropped observations with other forms of missing data (all less than 5%).
Results
Descriptive statistics including weighted (sub)sample sizes are presented in Table 2, and the distributions of abortion attitudes are presented in Figure 1. The effects of social welfare program attitudes and gender role attitudes on abortion acceptability are described below (see Table 3), and group differences by race/ethnicity and education are discussed throughout.
Table 2.
Weighted descriptive statistics and subsample sizes for the current study.
| United States | South Africa | ||||
|---|---|---|---|---|---|
| 2008 Models | 2016 Models | ||||
| GSS Variable | % or mean | n or Variance | SASAS Variable | % or mean | n or Variance |
| Sex | Sex | ||||
| Male | 46% | 778 | Male | 47% | 1132 |
| Female | 54% | 912 | Female | 53% | 1270 |
| Race/Ethnicity | Race/Ethnicity | ||||
| White | 70% | 1188 | Black-Xhosa | 18% | 438 |
| Black | 12% | 206 | Black-Zulu | 24% | 568 |
| Latinx | 13% | 226 | Black-Other | 38% | 913 |
| Other | 4% | 70 | Coloured | 9% | 210 |
| – | – | – | Indian | 3% | 60 |
| – | – | – | White-Afrikaner | 5% | 131 |
| – | – | – | White-English | 3% | 82 |
| Education | Education | ||||
| Some Secondary or Less | 16% | 268 | Primary or Less | 14% | 342 |
| Completed Secondary | 37% | 631 | Some Secondary | 38% | 913 |
| 2 Years Post-secondary | 19% | 315 | Completed Secondary | 37% | 896 |
| 4 Years Post-secondary or More | 28% | 475 | Any Tertiary | 10% | 250 |
| Annual Household Income | Monthly Household Income | ||||
| Less Than $25,000 | 20% | 343 | 1500 Rand or Less | 21% | 508 |
| $25,000 or More | 68% | 1143 | 1501–7500 Rand | 41% | 982 |
| No Response | 12% | 204 | 7501 Rand or More | 13% | 323 |
| – | – | – | Refused/Do Not Know | 25% | 589 |
| Region | Province | ||||
| Eastern North Central | 4% | 65 | Eastern Cape | 13% | 305 |
| Eastern South Central | 12% | 208 | Free State | 14% | 331 |
| Middle Atlantic | 17% | 288 | Gauteng | 2% | 51 |
| Mountain | 6% | 101 | KwaZulu-Natal | 5% | 125 |
| New England | 22% | 375 | Limpopo | 18% | 434 |
| Pacific | 4% | 74 | Mpumalanga | 5% | 130 |
| South Atlantic | 10% | 174 | Northern Cape | 23% | 552 |
| Western North Central | 7% | 122 | Northwest | 8% | 199 |
| Western South Central | 17% | 283 | Western Cape | 11% | 276 |
| Population Size (1,000 people) | 364.32 | 900.45 | Urbanicity | ||
| – | – | – | Urban Formal | 54% | 1296 |
| – | – | – | Urban Informal | 12% | 285 |
| – | – | – | Rural | 34% | 821 |
| Marital Status | Marital Status | ||||
| Married | 56% | 941 | Married | 29% | 706 |
| Widowed/Widower | 5% | 78 | Widowed/Widower | 6% | 143 |
| Divorced or Separated | 14% | 232 | Divorced or Separated | 5% | 112 |
| Never Married | 26% | 439 | Never Married | 60% | 1440 |
| Acceptability of Premarital Sex | 3.05 | 0.002 | Acceptability of Premarital Sex | 2.37 | 0.003 |
| Age | 45.16 | 0.28 | Age | 37.69 | 0.27 |
| Religious Denomination | Religious Denomination | ||||
| Not Religious | 17% | 287 | Not Religious | 15% | 360 |
| Protestant | 54% | 913 | Protestant | 68% | 1639 |
| Catholic | 25% | 421 | Catholic | 3% | 69 |
| Other Religion | 4% | 68 | Other Religion | 14% | 334 |
| Religiosity | 1.31 | 0.001 | Religiosity | 1.73 | 0.002 |
| Political Identity | Political Identity | ||||
| Conservative | 35% | 584 | Conservative | 22% | 517 |
| Moderate | 37% | 624 | Moderate | 31% | 733 |
| Liberal | 26% | 437 | Liberal | 35% | 838 |
| Do Not Know | 3% | 45 | Do Not Know | 13% | 315 |
Figure 1.
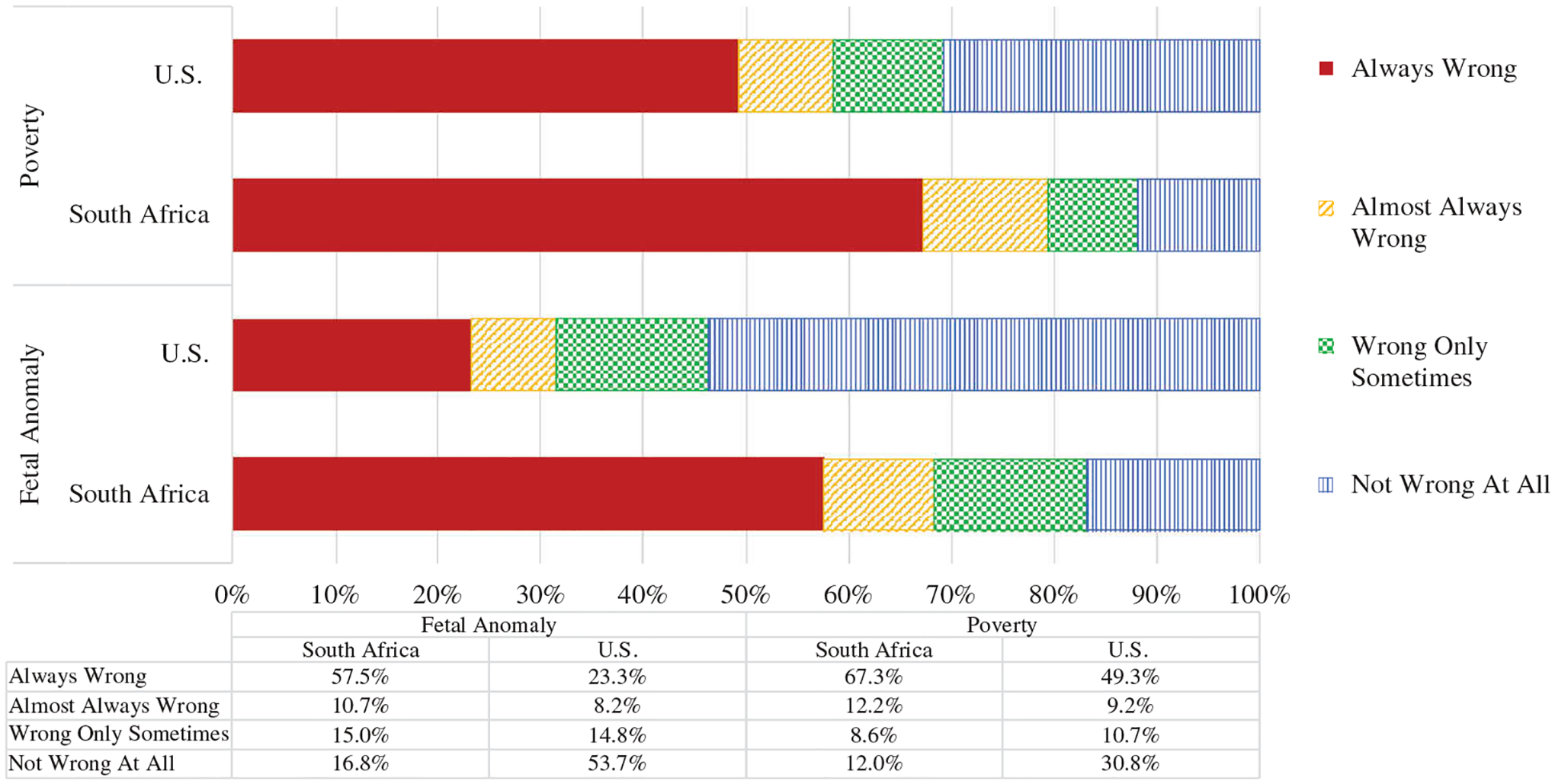
Distribution of abortion morality attitudes in the U.S. (2008) and South Africa (2016) in the case a family is low-income and cannot afford another child and in the case there is a severe fetal anomaly.
Table 3.
Ordinal logistic regression models of abortion acceptability in the U.S. (2008) and South Africa (2016, 2008#).
| United States | South Africa | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Poverty n = 1,690 |
Fetal Anomaly n = 1,690 |
Poverty n = 2,495 |
Fetal Anomaly n = 2,487 |
||||||||||
| Variable | OR | 95% CI | OR | 95% CI | Variable | OR | 95% CI | OR | 95% CI | ||||
| Income Equalization (Ref: Government Should Not Equalize) | Income Equalization (Ref: Government Should Not Equalize) | ||||||||||||
| Neither Agree nor Disagree | 1.05 | 0.66 | 1.66 | 1.12 | 0.70 | 1.78 | Neither Agree nor Disagree | 0.94 | 0.60 | 1.49 | 0.90 | 0.60 | 1.35 |
| Government Should Equalize | 0.93 | 0.63 | 1.37 | 1.03 | 0.69 | 1.51 | Government Should Equalize | 0.59 | 0.41 | 0.85 | 0.92 | 0.69 | 1.25 |
| Standard of Living (Ref: Individuals are Responsible) | Standard of Living (Ref: Individuals are Responsible) | ||||||||||||
| Both Individuals and Government Responsible | 1.50 | 0.98 | 2.28 | 1.01 | 0.69 | 1.47 | Both Individuals and Government Responsible | 1.20 | 0.69 | 2.08 | 0.73 | 0.42 | 1.26 |
| Government is Responsible | 1.53 | 0.97 | 2.41 | 1.06 | 0.65 | 1.73 | Government is Responsible | 1.32 | 0.81 | 2.14 | 0.66 | 0.41 | 1.06 |
| Funding for the Poor (Ref: Spending Too Much) | Funding for the Poor (Ref: Spending Too Much) | ||||||||||||
| Spending About the Right Amount | 0.97 | 0.50 | 1.87 | 1.21 | 0.63 | 2.32 | Spending About the Right Amount | 0.86 | 0.50 | 1.49 | 0.85 | 0.53 | 1.35 |
| Spending Too Little | 0.80 | 0.37 | 1.73 | 1.56 | 0.72 | 3.36 | Spending Too Little | 0.66 | 0.49 | 0.91 | 1.01 | 0.76 | 1.34 |
| Support for Egalitarian Gender Roles in Family | 1.18 | 1.03 | 1.36 | 1.15 | 1.01 | 1.31 | Support for Egalitarian Family Gender Roles # | 0.99 | 0.89 | 1.11 | 1.12 | 1.01 | 1.25 |
| Female | 1.07 | 0.79 | 1.44 | 1.01 | 0.75 | 1.35 | Female | 0.96 | 0.73 | 1.27 | 1.12 | 0.87 | 1.45 |
| Race/Ethnicity (Ref: White) | Race/Ethnicity (Ref: White-English) | ||||||||||||
| non-Hispanic Black | 1.38 | 0.86 | 2.20 | 0.97 | 0.58 | 1.61 | Xhosa | 1.36 | 0.79 | 2.36 | 0.67 | 0.36 | 1.26 |
| Hispanic | 0.88 | 0.54 | 1.41 | 0.86 | 0.50 | 1.46 | Zulu | 0.48 | 0.26 | 0.89 | 0.40 | 0.19 | 0.82 |
| non-Hispanic other race | 1.27 | 0.66 | 2.46 | 1.68 | 0.89 | 3.17 | African-Other | 0.79 | 0.45 | 1.40 | 0.72 | 0.38 | 1.34 |
| – | – | – | – | – | – | – | Coloured | 0.73 | 0.42 | 1.27 | 0.70 | 0.37 | 1.33 |
| – | – | – | – | – | – | – | Indian | 0.68 | 0.31 | 1.49 | 0.61 | 0.26 | 1.45 |
| – | – | – | – | – | – | – | White-Afrikaans | 0.75 | 0.39 | 1.46 | 1.12 | 0.59 | 2.12 |
| Education (Ref: Some Secondary or Less) | Education (Ref: Primary or Less) | ||||||||||||
| Completed Secondary | 1.91 | 1.23 | 2.97 | 1.29 | 0.86 | 1.93 | Some Secondary | 1.20 | 0.82 | 1.76 | 1.57 | 1.12 | 2.20 |
| 2 Years Post-secondary | 2.46 | 1.47 | 4.13 | 1.91 | 1.15 | 3.17 | Completed Secondary | 1.40 | 0.93 | 2.10 | 1.61 | 1.11 | 2.35 |
| 4 Years Post-secondary or More | 3.23 | 2.07 | 5.05 | 2.21 | 1.33 | 3.67 | Any Post-secondary | 2.32 | 1.29 | 4.16 | 2.68 | 1.68 | 4.27 |
| Annual House. Income (Ref: $25,000 or Less) | Monthly Household Income (Ref: 5000 Rand or Less) | ||||||||||||
| More than $25,000 | 1.13 | 0.79 | 1.61 | 1.16 | 0.83 | 1.64 | 5001 Rand or More | 1.01 | 0.71 | 1.43 | 0.79 | 0.56 | 1.11 |
| No Response | 1.16 | 0.68 | 1.96 | 1.81 | 1.05 | 3.10 | Refused/Do Not Know | 0.77 | 0.57 | 1.04 | 0.69 | 0.51 | 0.95 |
Note: All models control for marital status, sex attitudes, age, region, urbanicity, religious denomination, religiosity, and political identity
estimates come from the 2008 South African Social Attitudes Survey analyses
Social welfare program attitudes
The effects of social welfare program attitudes on abortion acceptability varied across the two countries, and in South Africa they varied across race/ethnicity and educational status. In the U.S. multivariable regression models, abortion acceptability in circumstances of poverty was not related to social welfare program attitudes overall or for any racial/ethnic or educational group. For South Africans, however, greater support for income equalization (OR: 0.59, 95% CI: 0.41–0.85) and increased spending on the poor (OR: 0.66, 95% CI: 0.49–0.91) was correlated with lower acceptability of abortion in circumstances of poverty. In the race-specific models, these inverse relationships were statistically significant for Black African respondents (ORincome equalization: 0.56, 95% CI: 0.35–0.88; ORspending on poor:0.59, 95% CI: 0.41–0.84), but not other racial/ethnic groups. In education-specific models, these inverse relationships were statistically significant for South Africans who had completed secondary education (ORincome equalization: 0.51, 95% CI: 0.31–0.83; ORspending on poor: 0.60, 95% CI: 0.40–0.91),
Gender role attitudes
In the U.S., support for egalitarian family gender roles was associated with higher abortion acceptability in circumstances of poverty (OR: 1.18, 95% CI: 1.03–1.36) and fetal anomaly (OR: 1.15, 95% CI: 1.01–1.31). The positive effects on abortion acceptability were statistically significant for White (ORpoverty: 1.23, 95% CI: 1.04–1.45; ORfetal anomaly: 1.18, 95% CI: 1.03–1.36) and less educated Americans (ORpoverty: 1.27, 95% CI: 1.03–1.57; ORfetal anomaly: 1.20, 95% CI: 1.01–1.42). In South Africa, egalitarian family gender roles were associated with higher abortion acceptability for fetal anomaly (OR: 1.12, 95% CI: 1.01–1.25). In race-specific models, egalitarian family gender roles were associated with higher abortion acceptability for fetal anomaly among Black respondents (OR:1.16, 95% CI: 1.02–1.32), but were associated with higher abortion acceptability in circumstances of poverty among non-Black respondents (OR:1.20, 95% CI: 1.01–1.42).
Discussion
In the current study, we observed that abortion acceptability is not associated with social welfare attitudes in the U.S., but in South Africa, greater support for social welfare programs was associated with lower abortion acceptability in circumstances of poverty. We also found that egalitarian gender role attitudes are associated with greater acceptability of abortion in both countries, but under different scenarios. Egalitarian gender attitudes correlated with greater acceptability of abortion in circumstances of poverty in the U.S., but for fetal anomaly in South Africa. Group differences within the countries further complicated these relationships. In South Africa, the negative relationship between social welfare program attitudes and abortion acceptability was only significant for Black respondents and more educated respondents; in both countries, the positive relationship of gender role attitudes was only significant for less educated respondents. Finally, support for gender equality predicted greater abortion acceptability for fetal anomaly for Black Africans in South Africa, but it predicted greater acceptability in the case of poverty for Whites in the U.S. and non-Black South Africans. Together, these results suggest abortion attitudes are distinctly related to socioeconomic and gender ideology depending one’s national context, racial/ethnic identity, and socioeconomic status.
Social welfare program attitudes
Evidence from the current study suggests that Americans decontextualize poverty-related abortion from the social realities of economic inequality and poverty, while South Africans who believe economic inequality should be addressed through government initiatives are more likely to morally disapprove of poverty-related abortion. Even when given the scenario that a ‘family has a very low income and cannot afford any more children,’ U.S. respondents’ attitudes about abortion were disconnected from their attitudes about social welfare initiatives that address poverty. In contrast, South Africans who supported such anti-poverty measures were more likely to feel abortion is wrong if it’s only because a family is low income. In their cross-national comparison of abortion attitudes, Sahar and Karasawa (2005) found traditional and conservative Americans are more likely to hold individual women accountable for their unwanted pregnancy and find their abortions unacceptable, but there was no such relationship in Japan. Perhaps this explains our observation: Americans do not associate social welfare programs with poverty-driven abortion, because they hold the individual woman and not society responsible (for both the pregnancy and the poverty), while South Africans who support public programs for poverty alleviation are more likely to disapprove of poverty-driven abortion. In other words, it is possible that South Africans view poverty-driven abortion as a failure of social welfare programs to meet the needs of low-income women experiencing a pregnancy they cannot afford, rather than a personal failure of the woman individually. In their qualitative research with women accessing abortion in South Africa, Gilbert and Sewpaul (2015, p. 87) consistently found that low-income women situated their abortions in the context of poverty generally and insufficient social welfare programs specifically. One participant explained, ‘I receive Child Support grants…how am I gonna manage? It’s too hard to bring another child when you do not have enough support for her or for him.’
It is true that Americans in our study were generally less supportive of social welfare than South Africans, and previous research does suggest mechanisms by which Americans detach abortion from socioeconomic realities like declining access to social welfare programs. This includes an over-emphasis in the U.S. on personal rather than collective responsibility. For example, Sahar and Kawasaki (2005, p. 291) explain, ‘those [Americans] with more conservative, traditional, religious views perceive the woman as more responsible. This same path does not reach significance in the Japanese model.’ In their qualitative research with low-income women accessing abortion in the U.S., Nickerson, Manski, and Dennis (2014, p. 682) found that women simultaneously resist, internalize, and project stigmatizing stereotypes about low-income women as ‘selfish and irresponsible’ and not deserving of public support through programs like Medicaid. Given this empirical evidence, our observation that attitudes about social welfare programs are not associated with abortion acceptability among less educated and Americans of color is understandable albeit counter-intuitive. Further, restrictive abortion policies, which have proliferated in the U.S. since 2000 (Guttmacher Institute, 2006), are more likely to obstruct safe abortion services for low-income women, who are also more likely to be women of color (Fried, 2000; Upadhyay, Weitz, Jones, Barar, & Foster, 2013). For example, the Hyde Amendment bans the use of federal Medicaid funding for abortion unless in strict cases to save the mother’s life, and this disproportionately bars low-income and women of color from services (Boonstra, 2016; Fried, 2000). In turn, after women are unable to access abortion services they are more likely to live in poverty (Foster et al., 2018). Researchers have found that states where abortion is more restricted are also more likely to have laws restricting social welfare programs like Temporary Assistance to Needy Families (TANF) that would theoretically support lower income families to raise children (Medoff, 2013).
Gender role attitudes
Our gender attitude results also support the hypothesis about different national orientations toward individualism and collectivism, and they point toward how those economic ideologies might intersect with gender inequality and racial/ethnic identity. Generally, researchers have hypothesized that people typically find ‘elective’ abortions (e.g., poverty-related) less acceptable than ‘medical’ abortions (e.g., fetal anomaly), because they are perceived as being within a woman’s control and more constrained by social norms (Sahar & Karasawa, 2005). Similarly, we found that among Whites in the U.S. and non-Blacks in South Africa, greater support for gender equality predicted greater abortion acceptability in the case of poverty. For Black South Africans, however, gender role attitudes predicted greater abortion acceptability in the case of fetal anomaly.
For one, this might reflect South Africa’s history of unsafe, poverty-driven abortion under Apartheid and ongoing social inequalities that have widened in the last 20 years of democracy – both of which disproportionately affected Black South Africans. When abortion was outlawed during Apartheid in 1975, Black women found themselves without the income or structural support to raise children, but they were also unable to access to safe abortion services in-country and were prohibited from traveling to Europe and elsewhere as their White counterparts could (Hodes, 2013). By the 1980s, an estimated 200,000–300,000 illegal abortions occurred annually among deeply impoverished Black women with an average of 425 deaths (95% CI: 78–735 deaths) from complications each year (Hodes, 2013; Rees et al., 1997). After the fall of Apartheid in 1994, the democratically-elected South African government legalized abortion, but the country’s social inequalities have not improved. Since then, although efforts have been made to reduce absolute poverty, the social inequality gaps between and within racial/ethnic groups have actually grown, and Black South Africans – especially Black women – are still more likely to live in poverty (Statistics South Africa, 2013, 2015). Given these historical and contemporary contexts, it is quite possible that poverty-related abortion has a uniquely negative connotation in the South African setting. For the Black majority, this seems to 1) increase the perception that government should address economic inequalities that underlie poverty-related abortion and 2) decrease the likelihood that poverty-related abortion acceptability is linked to gender role attitudes. To us, this suggests Black South African abortion attitudes in the case of fetal anomaly reflect ideologies of motherhood and gender, while poverty-related abortion attitudes more likely reflect women’s lived conditions including their access to social welfare programs and employment.
Strengths and limitations
The current study makes important and novel contributions to the understanding of abortion attitudes and stigma in the U.S. and South Africa, but its limitations must also be noted. For one, we used repeated cross-sectional surveys that inhibit our ability to make claims of causality. Additionally, our secondary analysis is limited by availability of close-ended measures and incongruence of measures over time and across countries. Measuring abortion morality simplistically as ‘always wrong’, ‘almost always wrong’, ‘only wrong sometimes’, and ‘not wrong at all’ and in only two scenarios – poverty and fetal anomaly – misses much of the nuance, ambivalence, and complexity that people feel about abortion. While the abortion attitudes measure used on the GSS and SASAS are common and have been previously validated on national surveys in various settings, other approaches to measuring abortion attitudes could have captured greater variation. For example, some studies have utilized multiple vignettes or scenarios with free response answers that describe broader and deeper perspectives on abortion (Varga, 2002), but such qualitative approaches make it difficult to generalize findings to larger populations. Surveys in both the U.S. (Altshuler, Gerns Storey, & Prager, 2015) and South Africa (Patel & Johns, 2009; Patel & Myeni, 2008) have used quantitative abortion attitudes measures that capture multiple aspects of abortion attitudes such as morality, legal availability, women’s autonomy, and attitudes about personally having an abortion; however, the inconsistency of these measures makes comparison across locations, groups, and time impossible. We were also unable to control for the ordering of survey questions; although researchers have found significant effects on answers to abortion questions depending on the context clues of preceding survey elements (Schuman, Presser, & Ludwig, 1981).
By testing for the effects of several independent variables across multiple models and stratified models, it is also possible some of our statistically significant findings reflect multiple testing effects. Future studies could consider this by focusing on fewer predictors or by adjusting for multiple testing effects.
Finally, the most recent U.S. data came from 2008 when GSS researchers last asked about moral acceptability of abortion, but it is possible these relationships and distributions have changed in the last decade. Similarly, because South African social welfare program attitudes were only collected in 2016 and gender role attitudes in 2008, we are unable to account for potentially confounding factors including broader sociopolitical changes in South Africa over that period. The limitations of our study highlight the need for further research, more current and valid measures that are used consistently over time, and multi-level analyses that connect abortion attitudes to accessibility of services and, ultimately, health outcomes.
Implications
This study challenges the dominant narrative of abortion attitudes by exposing divergent understandings of abortion morality within the same country and across countries, and by identifying relationships – or lack thereof – between abortion morality and attitudes about social welfare policies. In both South Africa (Gilbert & Sewpaul, 2015) and the U.S. (Foster et al., 2012; Nickerson et al., 2014), researchers have emphasized the importance of contextualizing abortion attitudes and abortion decision-making in the structural conditions of women’s lives, as well as the need to focus on women who are marginalized by race/ethnicity and socioeconomic status. Considering our results through that lens, we have identified implications for public health framing, abortion de-stigmatization efforts, abortion provider training, and measurement.
Achieving true reproductive freedom and human dignity will require a nuanced reproductive rights and justice approach that challenges the false dichotomy of pro-choice vs. pro-life rhetoric; encompasses gender, racial/ethnic, and economic inequality; and pays careful heed to differences across settings and population groups. While the current study cannot incorporate the core tenets of reproductive justice including community organizing to address social inequalities, it does consider abortion attitudes as they relate to socioeconomic conditions and ideologies. We believe this moves us toward a reproductive justice framework for understanding abortion attitudes by expanding beyond a traditional feminist approach that centers gender oppression to a more intersectional approach that incorporates economic oppression. Additionally, by looking at group differences by race/ethnicity and socioeconomic status, we also tried to center the experience and perspectives of groups that are often marginalized in traditional research on this topic.
Abortion de-stigmatization and improved access to safe abortion services are certainly needed to ensure health and human rights, but they must be sensitive to historical and contemporary reproductive coercion and implemented alongside welfare initiatives that would alternatively support families to raise their children healthily and with dignity (Luna & Luker, 2013; Ross, 2006). Reducing abortion stigma will, therefore, require community-based approaches rooted in an intersectional reproductive justice framework that considers gender, racial/ethnic, and socioeconomic equality. An excellent example of this approach was when SisterSong, SPARK Reproductive Justice, and other organizations formed a coalition to address new anti-abortion billboards in Atlanta, Georgia that proclaimed ‘Black children are an endangered species’ (Ross, 2011). The coalition relied on community-based organizing to resist messages of ‘black genocide’ in a way to upheld individual’s rights to abortion without erasing the U.S. history of eugenics and continuing economic marginalization of Black women. De-stigmatization campaigns will have to address patriarchal gender attitudes and norms that can underlie abortion stigma, but must be community-based and tailored to the specific histories, challenges, and concerns of a given community. Abortion service providers both experience abortion stigma and can, when not given adequate support and training, internalize and project stigmatizing attitudes about abortion and abortion clients. Providers might benefit from evidence-based de-stigmatization workshops such as the Providers Share Workshop (Harris et al., 2011) and from training in reproductive justice like the programs being developed by Loder and colleagues (Loder, Fuentes, Stalburg, & Harris, 2017).
Finally, our study points to the limitations of abortion attitude measures that are currently used on large-scale surveys. Moving forward, researchers will need to conduct mixed methods research to develop more valid measures that capture the complex nature of abortion attitudes. Notably, if we aim for the public to adopt a human rights framework of abortion, measures will need to expand beyond abortion and capture other facets of ideology relevant to reproductive justice. For example, saying that poverty-related abortion is ‘wrong’ because poverty should be addressed is very different from saying that poverty-related abortion is ‘wrong’ because women should adhere to traditional gender roles. A reproductive rights and justice approach – one that encompasses the needs of all communities especially those marginalized by gender, race/ethnicity, and socioeconomic background – has the potential for broad-based support that can activate diverse communities and spark meaningful social change for women’s health and human rights (Luna & Luker, 2013; Ross, 2006).
Funding
This work was supported by the National Center for Child Health and Development [P2CHD041028].
Footnotes
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Altshuler AL, Gerns Storey HL, & Prager SW (2015). Exploring abortion attitudes of US adolescents and young adults using social media. Contraception, 91(3), 226–233. [DOI] [PubMed] [Google Scholar]
- Baker PA (2010). From apartheid to neoliberalism: Health equity in post-apartheid South Africa. International Journal of Health Services, 40(1), 79–95. doi: 10.2190/HS.40.1.e [DOI] [PubMed] [Google Scholar]
- Barkan SE (2014). Gender and abortion attitudes: Religiosity as a suppressor variable. Public Opinion Quarterly, 78(4), 940–950. doi: 10.1093/poq/nfu047 [DOI] [Google Scholar]
- Boonstra HD (2016). Abortion in the lives of women struggling financially: Why insurance coverage matters. Guttmacher Policy Review, 19, 7. [Google Scholar]
- Bradford H (1991). Herbs, knives and plastic: 150 years of abortion in South Africa. In Science, medicine, and cultural imperialism (pp. 120–147). New York, NY: St. Martin’s Press, Inc. [Google Scholar]
- Carter JS, Carter SK, & Dodge J (2009). Trends in abortion attitudes by race and gender: A reassessment over a four decade period. Journal of Sociological Research, 1(1). Retrieved from http://www.macrothink.org/journal/index.php/jsr/article/view/156 [Google Scholar]
- Coovadia H, Jewkes R, Barron P, Sanders D, & McIntyre D (2009). The health and sealth system of South Africa: Historical roots of current public health challenges. The Lancet, 374, 817–834. doi: 10.1016/S0140-6736(09)60951-X [DOI] [PubMed] [Google Scholar]
- Crenshaw K (1989). Demarginalizing the intersection of race and sex: A black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. University of Chicago Legal Forum, 139–169. [Google Scholar]
- Davis A (2003). Racism, birth control, and reproductive rights. In Feminist postcolonial theory – A reader (pp. 353–367). [Google Scholar]
- Elias VL, Fullerton AS, & Simpson JM (2015). Long-term changes in attitudes toward premarital sex in the United States: Reexamining the role of cohort replacement. The Journal of Sex Research, 52(2), 129–139. doi: 10.1080/00224499.2013.798610 [DOI] [PubMed] [Google Scholar]
- Foster DG, Biggs MA, Ralph L, Gerdts C, Roberts S, & Glymour MM (2018). Socioeconomic outcomes of women who receive and women who are denied wanted abortions in the United States. American Journal of Public Health, 108(3), 407–413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foster DG, Gould H, Taylor J, & Weitz TA (2012). Attitudes and decision making among women seeking abortions at one U.S. clinic. Perspectives on Sexual and Reproductive Health, 44(2), 117–124. [DOI] [PubMed] [Google Scholar]
- Foster DG, & Kimport K (2013). Who seeks abortions at or after 20 weeks? Perspectives on Sexual and Reproductive Health, 45(4), 210–218. doi: 10.1363/4521013 [DOI] [PubMed] [Google Scholar]
- Frederickson GM (1982). White supremacy: A comparative study of American and South African history. Oxford University Press. [Google Scholar]
- Fried MG (2000). Abortion in the United States: Barriers to access. Health and Human Rights, 4, 174–194. [PubMed] [Google Scholar]
- Gilbert I, & Sewpaul V (2015). Challenging dominant discourses on abortion from a radical feminist standpoint. Affilia, 30(1), 83–95. [Google Scholar]
- Gresh A, & Maharaj P (2011). A qualitative assessment of the acceptability and potential demand for medical abortion among university students in Durban, South Africa. The European Journal of Contraception & Reproductive Health Care, 16(2), 67–75. doi: 10.3109/13625187.2010.546534 [DOI] [PubMed] [Google Scholar]
- Grossman D, Holt K, Peña M, Lara D, Veatch M, Córdova D, … Blanchard K (2010). Self-induction of abortion among women in the United States. Reproductive Health Matters, 18 (36), 136–146. [DOI] [PubMed] [Google Scholar]
- Grossman D, White K, Hopkins K, & Potter JE (2014). The Public Health Threat of anti-abortion legislation, Contraception 89(2), 73–74. doi: 10.1016/j.contraception.2013.10.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grossman D, White K, Fuentes L, Hopkins K, Stevenson A, Yeatman S, & Potter JE (2015, November 17). Knowledge, opinion, and experience related to abortion self-induction in Texas. Retrieved from https://liberalarts.utexas.edu/txpep/_files/pdf/TxPEP-Research-Brief-KnowledgeOpinionExperience.pdf
- Guttmacher Institute. (2006). States enacted 52 laws restricting abortion in 2005. News Release. Retrieved from https://www.guttmacher.org/news-release/2006/states-enacted-52-laws-restricting-abortion-2005
- Harries J, Cooper D, Strebel A, & Colvin CJ (2014). Conscientious objection and its impact on abortion service provision in South Africa: A qualitative study. Reproductive Health, 11(16), 1–7. doi: 10.1186/1742-4755-11-16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harries J, Orner P, Gabriel M, & Mitchell E (2007). Delays in seeking an abortion until the second trimester: A qualitative study in South Africa. Reproductive Health, 4(1), 7. doi: 10.1186/1742-4755-4-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harries J, Stinson K, & Orner P (2009). Health care providers’ attitudes towards termination of pregnancy: A qualitative study in South Africa. BMC Public Health, 9(1), 296. doi: 10.1186/1471-2458-9-296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris LH, Debbink M, Martin L, & Hassinger J (2011). Dynamics of stigma in abortion work: Findings from a pilot study of the providers share workshop. Social Science & Medicine, 73(7), 1062–1070. [DOI] [PubMed] [Google Scholar]
- Hodes R (2013). The medical history of abortion in South Africa, c. 1970–2000. Journal of Southern African Studies, 39 (3), 527–542. [Google Scholar]
- Hoffmeyer-Zlotnik J, & Harkness JA (Eds.). (2005). Methodological aspects in cross-national research. Mannheim: ZUMA, Zentrum für Umfragen, Methoden und Analysen. [Google Scholar]
- Human Sciences Research Council. (2015, September 20). South African Social Attitudes Survey (SASAS). Retrieved from http://www.hsrc.ac.za/en/departments/sasas
- International Social Survey Programme. (2019). History of the international social survey programme. Retrieved from January 16, 2019. http://w.issp.org/about-issp/history/
- Jelen TG (2015). Gender role beliefs and attitudes toward abortion: A cross-national exploration. Journal of Research in Gender Studies, 5, 11. [Google Scholar]
- Jelen TG, & Wilcox C (2003). Causes and consequences of public attitudes toward abortion: A review and research agenda. Political Research Quarterly, 56(4), 489–500. doi: 10.1177/106591290305600410 [DOI] [Google Scholar]
- Killian M, & Wilcox C (2008). Do abortion attitudes lead to party switching? Political Research Quarterly, 61(4), 561–573. doi: 10.1177/1065912907312981 [DOI] [Google Scholar]
- Kumar A, Hessini L, & Mitchell EMH (2009). Conceptualising abortion stigma. Culture, Health & Sexuality, 11(6), 625–639. doi: 10.1080/13691050902842741 [DOI] [PubMed] [Google Scholar]
- Kuumba MB (1993). Perpetuating neo-colonialism through population control: South Africa and the United States. Africa Today, 79–85. [PubMed] [Google Scholar]
- Loder C, Fuentes L, Stalburg CM, & Harris LH (2017). A reproductive justice curriculum for physicians: Recommendations from RJ experts. Contraception, 96(4), 305. [Google Scholar]
- Luna Z, & Luker K (2013). Reproductive justice. Annual Review of Law and Social Science, 9(1), 327–352. [Google Scholar]
- Medoff M (2013). Pro-choice versus pro-life: The relationship between state abortion policy and child well-being in the United States. Health Care for Women International. 131118105601001. doi: 10.1080/07399332.2013.841699. [DOI] [PubMed] [Google Scholar]
- Medoff MH, & Dennis C (2011). Trap abortion laws and partisan political party control of state government. American Journal of Economics and Sociology, 70(4), 951–973. [DOI] [PubMed] [Google Scholar]
- Mullings L, & Schulz A Intersectionality and health: An introduction. In Gender, race, class, and health: Intersectional approaches. San Francisco, CA: Jossey-Bass. [Google Scholar]
- National Opinion Research Center. 2017. General social surveys, 1972–2016: Cumulative codebook. Chicago: University of Chicago. Retrieved from http://gss.norc.org/documents/codebook/GSS_Codebook.pdf [Google Scholar]
- National Opinion Research Center. (2018, December 11). General social survey. Retrieved from http://www.norc.org/Research/Projects/Pages/general-social-survey.aspx
- Nickerson A, Manski R, & Dennis A (2014). A qualitative investigation of low-income abortion clients’ attitudes toward public funding for abortion. Women & Health, 54(7), 672–686. [DOI] [PubMed] [Google Scholar]
- Norris A, Bessett D, Steinberg JR, Kavanaugh ML, De Zordo S, & Becker D (2011). Abortion stigma: A reconceptualization of constituents, causes, and consequences. Women’s Health Issues, 21(3), S49–S54. doi: 10.1016/j.whi.2011.02.010 [DOI] [PubMed] [Google Scholar]
- Office of the Assistant Secretary for Planning and Evaluation. (2008, December 1). 2008 health and human services poverty guidelines. Retrieved from https://aspe.hhs.gov/2008-hhs-poverty-guidelines
- Patel CJ, & Johns L (2009). Gender role attitudes and attitudes to abortion: Are there gender differences? The Social Science Journal, 46(3), 493–505. [Google Scholar]
- Patel CJ, & Myeni MC (2008). Attitudes toward abortion in a sample of South African female university students. Journal of Applied Social Psychology, 38(3), 736–750. [Google Scholar]
- Rees H, Katzenellenbogen J, Shabodien R, Jewkes R, Fawcus S, Mclntyre J, … Truter H (1997). The epidemiology of incomplete abortion in South Africa. South African Medical Journal, 87(4), 432–437. [PubMed] [Google Scholar]
- Ross L (2006). Understanding reproductive justice. Atlanta, Georgia: SisterSong. Retrieved from http://www.trustblackwomen.org/our-work/what-is-reproductive-justice/9-what-is-reproductive-justice [Google Scholar]
- Ross L (2011). Fighting Black anti-choice campaigns: Trust Black women. Rewire. Retrieved from https://rewire.news/article/2011/02/28/fighting-black-antiabortion-campaign-trusting-black-women/
- Sahar G, & Karasawa K (2005). Is the personal always political? A cross-cultural analysis of abortion attitudes. Basic and Applied Social Psychology, 27(4), 285–296. [Google Scholar]
- Schoen J (2005). Choice & coercion: Birth control, sterilization, and abortion in public health and welfare. University of North Carolina Press. [Google Scholar]
- Schuman H, Presser S, & Ludwig J (1981). Context effects on survey responses to questions about abortion. Public Opinion Quarterly, 45(2), 216–223. [Google Scholar]
- Shellenberg KM, Hessini L, & Levandowski BA (2014). Developing a scale to measure stigmatizing attitudes and beliefs about women who have abortions: Results from Ghana and Zambia. Women & Health, 54(7), 599–616. doi: 10.1080/03630242.2014.919982 [DOI] [PubMed] [Google Scholar]
- Smith A (2005). Beyond pro-choice versus pro-life: Women of color and reproductive justice. NWSA Journal, 17(1), 119–140. [Google Scholar]
- StataCorp. (2014). Stata statistical software (Version 14). College Station, TX: Author. [Google Scholar]
- Statistics South Africa. 2013. Gender statistics in South Africa 2011. Pretoria, South Africa: Author. Retrieved from http://www.statssa.gov.za/publications/Report-03-10-05/Report-03-10-052011.pdf [Google Scholar]
- Statistics South Africa. (2015). Quarterly labour force survey: Quarter 4, 2014 (Statistical release no. P0211). South Africa. Retrieved from http://www.statssa.gov.za/publications/P0211/P02114thQuarter2014.pdf [Google Scholar]
- Statistics South Africa. (2017). Poverty trends in South Africa: An examination of absolute poverty between 2006 and 2015. Pretoria: Author. [Google Scholar]
- Stern AM (2005). Sterilized in the name of public health: Race, immigration, and reproductive control in modern California. American Journal of Public Health, 95(7), 1128–1138. doi: 10.2105/AJPH.2004.041608 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strickler J, & Danigelis NL (2002). Changing frameworks in attitudes toward abortion. Sociological Forum, 17, 187–201. Retrieved from http://link.springer.com/article/10.1023/A:1016033012225 [Google Scholar]
- Trueman KA, & Magwentshu M (2013). Abortion in a progressive legal environment: The need for vigilance in protecting and promoting access to safe abortion services in South Africa. American Journal of Public Health, 103(3), 397–399. doi: 10.2105/AJPH.2012.301194 [DOI] [PMC free article] [PubMed] [Google Scholar]
- United Nations. (1994). Programme of action. Retrieved from International Conference on Population and Development website: https://www.unfpa.org/sites/default/files/event-pdf/PoA_en.pdf
- United Nations. (2014). Framework of actions for the follow-up to the programme of action of the international conference on population and development beyond 2014. Retrieved from United Nations Population Fund website: http://icpdbeyond2014.org/uploads/browser/files/93632_unfpa_eng.pdf
- Upadhyay UD, Weitz TA, Jones RK, Barar RE, & Foster DG (2013). Denial of abortion because of provider gestational age limits in the United States. American Journal of Public Health, e1–e8. doi: 10.2105/ajph.2013.301378 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varga CA (2002). Pregnancy termination among South African adolescents. Studies in Family Planning, 33(4), 283–298. [DOI] [PubMed] [Google Scholar]
- Wheeler SB, Zullig LL, Reeve BB, Buga GA, & Morroni C (2012). Attitudes and intentions regarding abortion provision among medical school students in South Africa. International Perspectives on Sexual and Reproductive Health, 38(3), 154–163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitworth A, & Wilkinson K (2013). Tackling child poverty in South Africa: Implications of ubuntu for the system of social grants. Development Southern Africa, 30(1), 121–134. doi: 10.1080/0376835X.2013.756219 [DOI] [Google Scholar]
- Williams DR, Mohammed SA, Leavell J, & Collins C (2010). Race, socioeconomic status, and health: Complexities, ongoing challenges, and research opportunities: Race, SES, and health. Annals of the New York Academy of Sciences, 1186(1), 69–101. doi: 10.1111/j.1749-6632.2009.05339.x [DOI] [PMC free article] [PubMed] [Google Scholar]