

Abstract
Engaging youth in evidence‐based health education has the capacity to positively impact their experiences of health and illness across the lifespan. In particular, pain science education is now an established part of the treatment arsenal for persistent pain conditions in adults, and there are calls to build educational resources for youth with pain. In this paper, we argue that high‐quality online animated videos are a potentially excellent medium to engage youth at a mass level in pain science education. We present and compare two collaborations between clinician‐scientists and industry to create and disseminate online animated videos for pain science education (“Mysterious Science of Pain” and “Tame the Beast”). We discuss the advantages, disadvantages, and methods of evaluation for each approach, as well as summarizing overall lessons learned. We provide this information as a guiding framework for clinician‐scientists to collaborate with industry in building engaging and impactful health education resources for young people.
Keywords: call to action, online animated videos, pain science education, pediatric pain, YouTube
1. INTRODUCTION
Education is a keystone of many therapies for youth. Clinicians are expected to provide effective education that translates across multiple learning styles and developmental stages. High‐quality animations provide an ideal opportunity to engage youth in health education online. Animations are particularly well‐suited for illustrating abstract or hard‐to‐visualize phenomena relevant to health science, such as neuroanatomy and brain functions. Video animations also have the additional benefit of being able to be easily shared via the Internet. Certainly, the Internet has facilitated widespread health education by removing the physical and temporal limitations of face‐to‐face methods of learning. Today's youth are growing up in an advanced technological age with free, rapid, and easy access to information, including health‐related content, available on the Internet. 1 The Internet is indeed a primary source of health care information for youth and adults alike, 2 , 3 facilitating rapid and widespread knowledge mobilization. Health‐related online content can be developed, shaped, and shared by anyone, including clinicians and health researchers, providing an opportunity for dissemination of evidence‐based health information. 4 Given the accessibility of health‐related content online, and the technological savvy of today's youth, online resources are likely an excellent medium to engage youth across the globe in evidence‐based health education.
Unfortunately, those with content knowledge (eg, clinicians) are unlikely to also possess skills to produce high‐quality resources, 5 nor the time and funding. One option is to utilize currently available video resources. There are a number of online platforms that allow for hosting and sharing of videos. Platforms frequently recommend uploading high‐quality videos (eg, YouTube.com recommends video resolution of 1080p HD (1920 × 1080 pixels)); however, low‐resolution videos are also common. In addition, the content of uploaded health information does not need to be peer‐reviewed, so the quality of the information is uncertain. In some areas of health, there are gaps in the educational content covered in freely available videos. 6 These limitations are barriers to delivering high‐quality, scientifically accurate, and evidence‐based education.
In this paper, we advocate for the collaboration between clinician‐scientists and the animation industry to harness the power of online animated videos to engage multitudes of youth in health education across the globe. We use examples from pain science education to offer a blueprint for building such collaborations, including strengths and weaknesses of two different approaches, and overall lessons learned. Pain science education also referred to as “pain neuroscience education,” “therapeutic neuroscience education,” and “Explaining Pain” (among others) 7 focuses on explaining the biopsychosocial mechanisms underlying pain. 8 Pain science education provides a foundation for pain management education via an understanding of the principles that guide biopsychosocial interventions for persistent pain, 9 fitting within collaborative frameworks such as the Knowledge to Action process. 10 As an educational intervention, it is one possible component of a broader knowledge translation strategy, that could also comprise many other strategies. 11 While there is currently no available evidence on efficacy from randomised controlled trials in children, trials are currently underway. 12 , 13 Nonetheless, pain science education is commonly, but not universally, implemented in multi‐ and inter‐disciplinary care in pediatric pain clinics internationally. 14 The implementation of this approach in children with persistent pain is based on clinical experience as well as a growing evidence base in adults. Systematic reviews indicate that pain science education improves pain and functional outcomes in adults with persistent pain, especially when combined with biopsychosocially framed interventions, but as a stand‐alone intervention, the effects on pain and disability are small. 15 , 16 , 17 A recent trial of pain science education for adults with acute back pain failed to replicate improvements in pain intensity, but secondary outcomes raise the possibility of clinically important benefits in investigation and care seeking, likelihood of recurrence, pain‐related attitudes, and disability. 18 Taken together, the evidence base suggests that, in adults, pain science education improves patients’ knowledge about pain as well as their attitudes toward a biopsychosocial approach to care, including multidisciplinary treatment and self‐management strategies. 8 , 15 , 16 , 17 One critical step in the pathway toward a substantial evidence base in adults has been the development of resources and one might expect that a similar step will facilitate moving beyond the preliminary suggestions that pain science education will be of benefit for youth with pain, 7 , 9 , 19 toward more empirical data.
In this paper, we present two approaches to creating online animated videos, using examples from pain science education. Using these approaches as a framework, we aim to: (a) explain the process of creating the two videos, (b) discuss the advantages, disadvantages, and methods for evaluating these approaches, and (c) summarize lessons learned and a call to action to create educational resources for youth with pain. The examples we present are a collaboration with TED‐Ed (“Mysterious Science of Pain”) 20 and with a private creative company (“Tame the Beast”). 21
2. TWO APPROACHES FOR CREATING ONLINE ANIMATED VIDEOS OF PAIN SCIENCE EDUCATION
In Table 1, we summarize and compare two different approaches (Figure 1) to creating online animated videos for pain science education.
TABLE 1.
Comparison of two approaches for creating online animated videos of pain science education
| Variable | TED‐Ed mysterious science of pain | Tame the beast |
|---|---|---|
| Initial clinical purpose | To supplement face‐to‐face pain science education | To inspire research‐based action in the treatment of pain |
| Author of first draft (content expert) | JWP | GLM & D. Moen |
| Ownership | TED‐Ed | GLM & D. Moen |
| Cost | Nil to content expert | $60 000 AUD (50/50 private and unrestricted grant contribution) |
| Team | Educator, voice narrator, animators, factchecker, audio—all contribute for free and the director and producers are employed by TED‐Ed | Private media company (Sam Chisolm Creative): market research, concept and strategy development, production. Narrator (GLM) |
| Number of hours provided by the content expert |
Draft script—2 h Ongoing input throughout development—approximately 5 h |
Education of concept to creative team—14 h Narration—1 h |
| Time from idea to publishing | 6 mo | 12 mo |
| Online reach a (total view count) | 1 305 000 | 960 000 |
| Offline reach (estimated view count) | Unknown | 4 200 000 b |
| “Next step for the viewer” when viewed on the host website | Attached online “lessons” for each video with quizzes, links and more info—targeted at school children | Tame the Beast website very clearly advertised within video as a “next step,” discuss with health professional |
| Dissemination | Social media, particularly via key organisations, leading experts, consumer groups and advocacy groups, public health services |
Total online reach is a result of the addition of view counts on the video's host website, YouTube and Facebook (publicly available).
G.LM estimated offline view count via known hospital waiting room and private practice loops, and third‐party websites, based on 10% of people in waiting rooms known to have it looping watching it, that is, 10% of 8% (for most, TTB takes up 5 min of an hour‐long loop; some the loops are 30, 40, 46, and 52 min, but I have based figure on longest and most common loop length) of waiting room visitors.
FIGURE 1.

YouTube thumbnail images for (A) “Mysterious Science of Pain” and (B) “Tame the Beast”
The first video we present is the “Mysterious Science of Pain,” developed in collaboration with TED‐Ed. 20 TED‐Ed is a global education platform that creates and hosts animations to spark learners’ curiosity. 22 A physiotherapist with no previous experience in animation (JWP) completed the educator nomination form on the TED‐Ed website, pitching the idea for the video. The initial impetus for this proposal was to create a tool that would supplement face‐to‐face pain science education in a clinical setting. Once accepted, a 30‐minute phone call followed, where TED‐Ed producers guided the topic further. As the content expert, JWP then wrote an 800‐word draft script with scholarly referencing to support the scientific claims made in the video and suggested animation ideas. Refining the script (3 months) and the animation and production (another 3 months) were iterative and collaborative processes. Throughout these six months, JWP provided input to refine the language and the scientific backing of the content. The animation team also helped shape the content for the video, for example creating the “castle” metaphor to illustrate the protective nature of pain. The video was published on May 20, 2019, (Figure 2A) and has been disseminated online on platforms including YouTube (https://youtube.com/watch?v=eakyDiXX6Uc) and Facebook.
FIGURE 2.
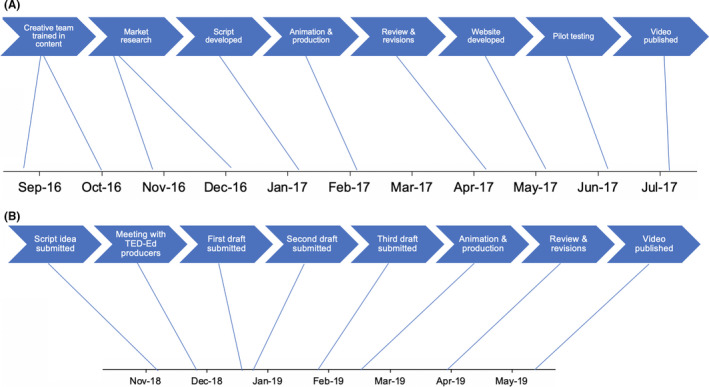
The timeline for the development and production of the (A) Tame the Beast and (B) TED‐Ed Mysterious Science of Pain videos. The multiple drafts in this process were guided by both the TED‐Ed team refining the language to be more concise, and JWP refining the science by providing citations for every phrase of the script
The second video we present is “Tame the Beast: It's Time to Rethink Persistent Pain.” This video was designed to be embedded and viewed on the dedicated website that was developed to inspire research‐based action in the treatment of pain. 21 This Tame the Beast initiative was a collaboration between a pain scientist/clinician/educator (GLM), a clinical physiotherapist (David Moen, Form Physiotherapy, Adelaide, Australia), and a governmental statutory authority (Return to Work South Australia). The content experts (GLM and DM) approached several creative firms with the idea. The selected creative firm implemented a comprehensive “concept to resource” process. Key components of that process were as follows: 12 hours direct pain science education from the content experts; international market research; competitor and precedent analysis; concept development; review and selection of optimal hosting strategy and dissemination channels; script and animation development; beta testing including acceptability and engagement; final production and hosting. This process took 12 months and the video was published on July 26, 2017 (Figure 2B). It has been disseminated online on a dedicated website (www.tamethebeast.org), and via Facebook and YouTube (https://www.youtube.com/watch?v=ikUzvSph7Z4).
3. ADVANTAGES, DISADVANTAGES, AND METHODS FOR EVALUATING THESE APPROACHES
3.1. Advantages for the content expert
The main advantages common to both approaches are that the content expert can co‐create freely accessible content that is produced by highly skilled creative experts; the resource can be shared online and offline (eg, waiting room monitors) and embedded into websites with clinical content (eg, quizzes); the script is readily available and subtitles are easily integrated in many languages; the transcript can be easily translated into almost any language as soon as the transcript is made available; and the animation's audio can be translated (at TED‐Ed's discretion for TED‐Ed or at a cost for Tame the Beast). For the Mysterious Science of Pain approach, the content expert (in this case, JWP) provided no financial outlay and the video rapidly reached a wide pre‐established audience via a credible fact‐checked platform. The video was embedded into TED‐Ed curricula with quizzes and resources linked through their website. For the Tame the Beast approach, the content expert had control over final scripting and messages, and the video can be modified and translated for research projects without ownership issues. In addition, in the case of the Tame the Beast video, branding and dissemination of the video was based on customized market research and consumer testing with an opportunity to build a specific subscriber database with usage statistics.
3.2. Disadvantages for the content expert
One disadvantage common to both approaches is that the videos cannot easily be edited or updated (ie, editing is cost‐ and time‐resource intensive and relies on the skill of animators). In addition, the assessment of reach relies on potentially imprecise algorithms and third‐party data, which are difficult to collect. Other websites hosting the video also have recommendation services that cannot be controlled by the content expert and so may unintentionally promote content with contrasting educational messages (eg, YouTube's recommended video panel). Disadvantages specific to the Mysterious Science of Pain approach are that the content expert does not have ownership of the video, the video cannot easily be modified and translated for research projects due to a lack of ownership. For the Tame the Beast approach, the main disadvantages to the content experts are the upfront cost, the need to source a creative company, the need to self‐promote and market the video with no immediate audience base, additional costs for translating into different languages (approximately $5000 AUD was quoted for Tame the Beast). The additional flexibility and control offered by the Tame The Beast approach comes at a cost and therefore requires consideration of funding. Including evaluative methodologies will likely be key to securing funding through traditional grant agencies.
3.3. Methods for evaluation
Using observations of video sharing on social media and individual feedback provided to JWP and GLM, both videos are known to have been utilized in clinical settings (eg, waiting rooms, one‐to‐one appointments, group pain management programs, and patient information sessions), online via web searches and in closed group platforms (eg, Facebook groups), and in academic settings (eg, modules within health professional university degrees). The videos are also being implemented in a range of third‐party educational programs. Study designs that would be useful to evaluate the resources include focus groups with viewers of the video, controlled intervention studies examining conceptual change, and experimental studies examining the impact of watching the video on experimentally induced pain indices.
When putting time and resources into developing health education videos, it is important and optimal to measure their impact. One way to begin to assess potential impact is to track dissemination including engagement metrics. 23 Traditional methods for evaluating reach of scientific content, that is, number of citations, are now being extended to capture the interconnected digital world that we live in using “Altmetrics”, 24 and we are applying these metrics to scientific video content. There is inevitably some imprecision in tracking these metrics given the open‐source nature of the Internet, but data from popular video‐sharing sites (eg, YouTube, Facebook) provide a representation of dissemination. Figure 3A shows the total online view counts of both videos (as of 21 October 2019) across three platforms (the hosting website, YouTube, and Facebook). While both videos share similar view counts on the Facebook platform, they differ such that comparatively Tame the Beast has been viewed more via its dedicated website, likely reflecting its targeted dissemination strategy, and the Mysterious Science of Pain video that has been viewed more via YouTube, likely reflecting the large number of TED‐Ed YouTube subscribers. Figure 3B illustrates a typical “viral” trendline of YouTube videos, depicting the total number of views of Mysterious Science of Pain across time having an initial spike in views that flattens out over time. While we present only the data from the hosting website and two platforms with publicly available view counts, there are additional unaccounted data attributable to the fact that some users will not share the original video but will instead download the video and upload it to their own social media page or website. In addition to view counts, which can be taken to reflect “reach,” additional interactive components such as “comments” and “likes,” which can be taken to reflect “engagement” because they show the user has interacted in some way. 23 At the time of writing this manuscript, the Mysterious Science of Pain video had received 804 YouTube comments, 17 000 likes, and 169 dislikes. The Tame the Beast video had received 39 YouTube comments, 914 likes, and 19 dislikes. The range of positive and negative comments on both videos illustrate the challenges of misinterpretation and the potential for cyber bullying on this platform.
FIGURE 3.
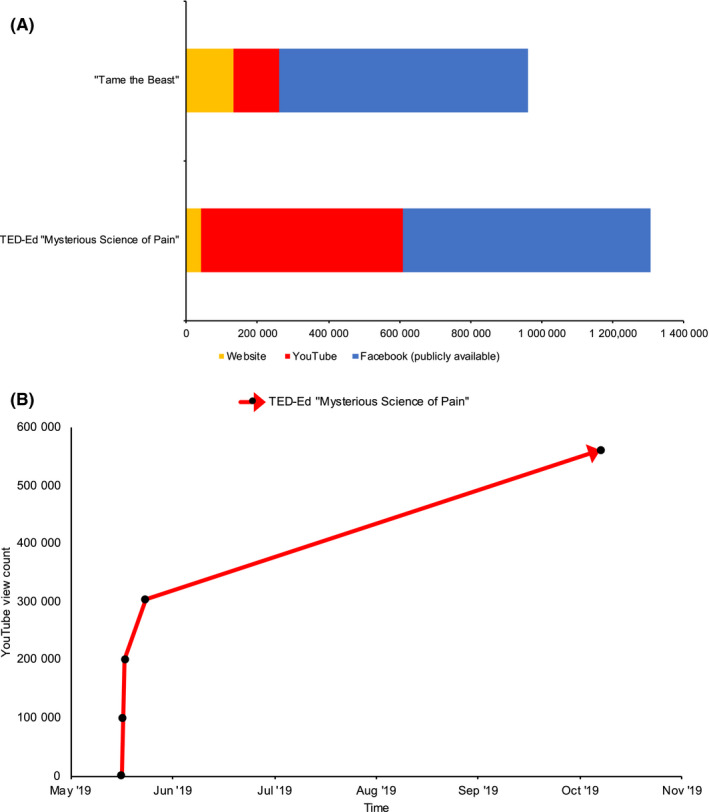
A, Online view counts of “Tame the Beast” and “Mysterious Science of Pain” (as of October 21, 2019) across three platforms. B, Online view counts on YouTube of “Mysterious Science of Pain” across time, as an example of the typical shape of view count trendlines
More fine‐grained data regarding the viewers of the videos are difficult to acquire. The content expert of the Mysterious Science of Pain video (JWP) was able to obtain limited demographic data from Ted‐Ed, revealing that the video had been viewed in 50 countries and that the majority of viewers were aged between 13 and 24 years. In contrast, content experts of the Tame the Beast video have full access to analytic data including country of use, self‐reported age of viewers, view counts, and daily average views. In addition, because Tame the Beast is privately owned and uploaded, other analytics are available including retention of viewers watching the whole video (60%, in contrast to the market research average for similar length videos in health domain being 30%) and retention of viewers after an industry standard 20 seconds “recognition” period (93%). This is usually interpreted as suggesting that, once the viewer decides whether or not the topic is relevant to them, 93% watch the entire video. Preliminary data from pilot studies (Moseley, GL, unpublished) suggest Tame the Beast results in both measurable shifts in pain‐related knowledge and a shift in treatment choices when healthy controls are presented with a “virtual patient” scenario such as that used in a very brief intervention related to radiological reports. 25
4. LESSONS LEARNED AND A CALL TO ACTION TO CREATE EDUCATIONAL RESOURCES
4.1. Lessons learned
Many lessons were learned through both approaches to creating online animated videos. Table 2 presents a series of practical and conceptual tips to guide individuals in creating their own educational videos, including in collaboration with industry.
TABLE 2.
Lessons learned, and related practical and conceptual tips
| Lesson learned | Practical/conceptual tips |
|---|---|
| Know your purpose: a creative team relies on you articulating clearly what it is you want to achieve |
|
| Know your message: a creative team relies on you articulating clearly what you know and want to share. Remember you are the content expert |
|
| Know your audience |
|
| Be clear on ownership and final approval |
|
| Know your limits. You may be the content expert but if you partner with a creative team, respecting that they are the delivery and communications experts is important |
|
| Fact‐check: this is an important quality control step. An army of viewers will be ready to spot the fiction amidst the fact |
|
4.2. Call to action
We would like to call the research, and clinical community to prioritise education as a valid part of our treatment arsenal. Clinical guidelines for acute and persisting pain, for children and adults, and for every country for which they exist, identify education as the first line of care (eg, for back pain 26 ). Adult data clearly show that pain science education is important and beneficial, and that when patients do learn a new way of understanding pain, truly excellent outcomes become possible. 27 Of several barriers to achieving a shift in understanding, the limited availability of scientifically sound and research‐based resources would seem a surmountable one. There are at least two important reasons that developing more resources that are freely available will have a widespread beneficial effect. First, that pain is influenced by one's social and cultural context means that one resource is unlikely to be optimal for all. Second, the information available to people in pain is diverse and of variable quality. In a noisy space, a greater presence of scientifically sound and research‐based resources is likely to have a super‐additive effect; the impact of viewing one resource is likely to be enhanced if the next resource is consistent in message and recommendations. Inherent in our recommendation to develop resources is that those resources are both peer reviewed, potentially by content experts or not‐for‐profit providers of pain education (current options include Pain Revolution, Pain Australia and Pain BC (Canada)), and consumer reviewed. Third, the resources are evaluated, with respect to their reach, engagement, and cognitive impact. We see great value in embedding evaluation strategies within such resources, perhaps where viewers can opt in to answering questions on completing the video. We also suggest that particular attention be given to facilitating resources to cultural, linguistic, and developmental groups for whom current resources are inappropriate; this likely includes children. Finally, we strongly recommend collaborating with creative industry professionals to take advantage of the capabilities of online animated videos to engage youth around the world in health education.
CONFLICT OF INTEREST
JWP is the educator for the TED‐Ed Mysterious Science of Pain animation. GLM is the main character and narrator in the Tame the Beast animation. He receives royalties for several books on pain that are advertised as resources on the Tame the Beast website and he also receives speaker fees for talks on pain and rehabilitation. Funding for the Tame the Beast website was provided by Return to Work South Australia and an anonymous private donor. He has other disclosures not immediately related to this work: GLM has received support from AIA Australia, Swisse, Gallagher Bassett, Kaiser Permanente, Workers' Compensation Boards in Australia, Europe and North America, the International Olympic Committee, Port Adelaide Football Club, Arsenal Football Club, Seqirus and various professional organisations and learned societies. He receives royalties for several books on pain and speakers’ fees for talks on pain and rehabilitation. Both videos discussed in the manuscript were based on a large literature base concerning contemporary pain science concepts. The authors have collaborated on previous projects, but the two online animations were developed completely independently.
Pate JW, Heathcote LC, Simons LE, Leake H, Moseley GL. Creating online animated videos to reach and engage youth: Lessons learned from pain science education and a call to action. Paediatr Neonatal Pain. 2020;2:131–138. 10.1002/pne2.12015
Oral presentation specifically regarding the process of developing a resource collaboratively with TED‐Ed, at the Australian Physiotherapy Association 2019 “Transform” conference in Adelaide, Australia, titled, “How to engage hundreds of thousands of people in learning about pain: the ‘what’, ‘why’, and ‘how’”.
REFERENCES
- 1. Mitsutake S, Shibata A, Ishii K, Oka K. Associations of eHealth literacy with health behavior among adult internet users. J Med Internet Res. 2016;18(7):e192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. McMullan M. Patients using the internet to obtain health information: how this affects the patient–health professional relationship. Patient Educ Couns. 2006;63(1–2):24‐28. [DOI] [PubMed] [Google Scholar]
- 3. Gordon NP, Hornbrook MC. Differences in access to and preferences for using patient portals and other eHealth technologies based on race, ethnicity, and age: a database and survey study of seniors in a large health plan. J Med Internet Res. 2016;18(3):e50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Paige SR, Krieger JL, Stellefson ML. The influence of eHealth literacy on perceived trust in online health communication channels and sources. J Health Commun. 2017;22(1):53‐65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Reay SD, Collier G, Douglas R, et al. Prototyping collaborative relationships between design and healthcare experts: mapping the patient journey. Design Health. 2017;1(1):65‐79. [Google Scholar]
- 6. Heathcote LC, Pate JW, Park AL, et al. Pain neuroscience education on YouTube: a systematic review. bioRxiv. 2018:492967. [Google Scholar]
- 7. Robins H, Perron V, Heathcote LC, Simons LE. Pain neuroscience education: state of the art and application in pediatrics. Children. 2016;3(4):43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Moseley GL, Butler DS. Fifteen years of explaining pain: the past, present, and future. J Pain. 2015;16(9):807‐813. [DOI] [PubMed] [Google Scholar]
- 9. Leake H, Heathcote LC, Simons LE, et al. Talking to teens about pain: a modified Delphi study of adolescent pain science. Can J Pain. 2019;3(1):200‐208, 10.1080/24740527.2019.1682934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Graham ID, Logan J, Harrison MB, et al. Lost in knowledge translation: time for a map? J Contin Educ Health Prof. 2006;26(1):13‐24. [DOI] [PubMed] [Google Scholar]
- 11. Davis D, Davis N. Selecting educational interventions for knowledge translation. CMAJ. 2010;182(2):E89‐E93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Pas R, Meeus M, Malfliet A, et al. Development and feasibility testing of a Pain Neuroscience Education program for children with chronic pain: treatment protocol. Braz J Phys Ther. 2018;22(3):248‐253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Pas R. Pain neuroscience education in healthy children 2017. https://clinicaltrials.gov/ct2/show/NCT03164343. Accessed Oct 22, 2019.
- 14. Harrison LE, Pate JW, Richardson PA, Ickmans K, Wicksell RK, Simons LE. Best‐evidence for the rehabilitation of chronic pain Part 1: pediatric pain. J Clin Med. 2019;8(9):1267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Watson JA, Ryan CG, Cooper L, et al. Pain neuroscience education for adults with chronic musculoskeletal pain: a mixed‐methods systematic review and meta‐analysis. J Pain. 2019;20:1140.e1‐1140.e22. [DOI] [PubMed] [Google Scholar]
- 16. Wood L, Hendrick PA. A systematic review and meta‐analysis of pain neuroscience education for chronic low back pain: short‐and long‐term outcomes of pain and disability. Eur J Pain. 2019;23(2):234‐249. [DOI] [PubMed] [Google Scholar]
- 17. Louw A, Zimney K, Puentedura EJ, Diener I. The efficacy of pain neuroscience education on musculoskeletal pain: a systematic review of the literature. Physiother Theory Pract. 2016;32(5):332‐355. [DOI] [PubMed] [Google Scholar]
- 18. Traeger AC, Lee H, Hübscher M, et al. Effect of intensive patient education vs placebo patient education on outcomes in patients with acute low back pain: a randomized clinical trial. JAMA Neurol. 2019;76(2):161‐169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Pate J, Hush J, Hancock M, et al. A child’s concept of pain: an international survey of pediatric pain experts. Children. 2018;5(1):12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. TED‐Ed . The mysterious science of pain ‐ Joshua W. Pate. 2019. https://ed.ted.com/lessons/the‐mysterious‐science‐of‐pain‐joshua‐w‐pate. Accessed October 22, 2019.
- 21. Moen D, Moseley GL.Tame the beast: it's time to rethink persistent pain. 2017. www.tamethebeast.org. Accessed October 22, 2019.
- 22. TED . TED‐Ed 2019. https://ed.ted.com/about. Accessed Oct 22, 2019.
- 23. Allen HG, Stanton TR, Di Pietro F, Moseley GL. Social media release increases dissemination of original articles in the clinical pain sciences. PLoS ONE. 2013;8(7):e68914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Rosenkrantz AB, Ayoola A, Singh K, Duszak R. Alternative metrics (“altmetrics”) for assessing article impact in popular general radiology journals. Acad Radiol. 2017;24(7):891‐897. [DOI] [PubMed] [Google Scholar]
- 25. Karran EL, Medalian Y, Hillier SL, Moseley GL. The impact of choosing words carefully: an online investigation into imaging reporting strategies and best practice care for low back pain. PeerJ. 2017;5:e4151‐e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Koes BW, van Tulder M, Lin C‐WC, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non‐specific low back pain in primary care. Eur Spine J. 2010;19(12):2075‐2094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Lee H, McAuley JH, Hübscher M, Kamper SJ, Traeger AC, Moseley GL. Does changing pain‐related knowledge reduce pain and improve function through changes in catastrophizing? Pain. 2016;157(4):922‐930. [DOI] [PubMed] [Google Scholar]