

Abstract
Background
Patient safety during anesthesia is crucially dependent on the monitoring of vital signs. However, the values obtained must also be perceived and correctly classified by the attending care providers. To facilitate these processes, we developed Visual-Patient-avatar, an animated virtual model of the monitored patient, which innovatively presents numerical and waveform data following user-centered design principles. After a high-fidelity simulation study, we analyzed the participants’ perceptions of 3 different monitor modalities, including this newly introduced technique.
Objective
The aim of this study was to collect and evaluate participants’ opinions and experiences regarding 3 different monitor modalities, which are Visual-Patient-avatar, Split Screen (avatar and Conventional monitor alongside each other), and Conventional monitor after using them during simulated critical anesthetic events.
Methods
This study was a researcher-initiated, single-center, semiquantitative study. We asked 92 care providers right after finishing 3 simulated emergency scenarios about their positive and negative opinions concerning the different monitor modalities. We processed the field notes obtained and derived the main categories and corresponding subthemes following qualitative research methods.
Results
We gained a total of 307 statements. Through a context-based analysis, we identified the 3 main categories of “Visual-Patient-avatar,” “Split Screen,” and “Conventional monitor” and divided them into 11 positive and negative subthemes. We achieved substantial interrater reliability in assigning the statements to 1 of the topics. Most of the statements concerned the design and usability features of the avatar or the Split Screen mode.
Conclusions
This study semiquantitatively reviewed the clinical applicability of the Visual-Patient-avatar technique in a high-fidelity simulation study and revealed the strengths and limitations of the avatar only and Split Screen modality. In addition to valuable suggestions for improving the design, the requirement for training prior to clinical implementation was emphasized. The responses to the Split Screen suggest that this symbiotic modality generates better situation awareness in combination with numerical data and accurate curves. As a subsequent development step, a real-life introduction study is planned, where we will test the avatar in Split Screen mode under actual clinical conditions.
Keywords: avatar, patient monitoring, semiquantitative research, simulation study, situation awareness, user-centered design, visual-patient-avatar
Introduction
Although perioperative mortality directly attributable to anesthesia is low in high-income countries and has significantly declined over the last 50 years, the World Health Organization describes anesthesiologic and surgical complications as the leading cause of preventable perioperative morbidity and mortality [1-4].
Among all anesthesia complications leading to permanent brain damage or death, two-thirds are caused by inaccurate situation awareness. This concept developed by Mica Endsley comprises a chain of information processing including the three core levels of perception (level 1), comprehension (level 2), and projection (level 3), whereby level 1 is most frequently affected [5-7]. For appropriate decision-making and thus avoiding errors, a situation must be recognized, its severity assessed, and the correct next steps taken while anticipating future progress. This cognitive process is influenced by individual factors such as experience and environmental resources. Well-established methods such as perioperative checklists were developed with the intention of improving environmental resources [8]. In addition, new tools are needed to impact situation awareness positively and thus reduce perioperative anesthesiologic complications.
Hence, we developed Visual-Patient-avatar as a beneficial environmental factor on situation awareness in patient monitoring. This avatar-based visualization on a patient monitor displays an animated model of the measured numerical parameters combining principles of logic and user-centered design [9]. Previous computer-based studies have shown that more vital signs were observed when using this new technique, subjective diagnostic confidence increased, and perceived workload declined compared to conventional patient monitoring [10-12]. However, the use of Visual-Patient-avatar in a high-fidelity simulation study has not yet been analyzed, including its qualitative aspects.
This study aims to collect and assess the opinions and experiences of participants concerning the three different patient monitoring modalities, which are (1) Visual-Patient-avatar, (2) Split Screen (avatar and conventional patient monitoring side by side), and (3) conventional, after using them in simulated critical anesthesia events [13]. We sought to capture the advantages and disadvantages of the different monitor settings to foster the avatar’s development and, in the future, facilitate its implementation in everyday clinical practice.
Methods
Approval and Consent
The Cantonal Ethics Committee of Zurich in Switzerland issued a declaration of no objection after reviewing the study protocol (Business Management System for Ethics Committees Req-2020-00059). All participants signed written informed consent for the use of their data for research purposes and participated voluntarily without any financial compensation.
Study Design
This is a researcher-initiated, single-center, semiquantitative study investigating physicians’ and nurses’ perceptions of using Visual-Patient-avatar in simulated critical anesthesia events. We conducted this study at the University Hospital of Zurich in Switzerland, in May 2020. We included the same 104 care providers grouped in 52 teams of a recently published study that evaluated avatar-based patient monitoring in a high-fidelity simulation study [13].
Previous Avatar-Based Patient Monitoring Simulation Study and Participant Interviews
This recently published study showed noninferiority of Split Screen compared with Conventional monitoring for performance during anesthesia crisis events. The probability of communicating the correct reason for the emergency was increased using the Visual-Patient-avatar as the monitor modality [13]. Figure 1 shows the 13 available vital signs and an example with possible deviations and additionally. Part (A) depicts an awake patient with vital signs within normal range. The avatar’s body pulsates during patient monitoring, whereby the frequency and extension indicate the pulse rate and blood pressure, respectively. In part (B), we demonstrate a desaturated (purple color), deeply sedated (eyes closed) patient with muscle relaxation (floppy extremities). Hypotension is represented by the gap between the purple body and the white boundary line. If the body temperature leaves the normal range, ice crystals or heat waves become visible around the avatar. Additionally, Multimedia Appendix 1 provides an animated version of the 2 examples.
Figure 1.
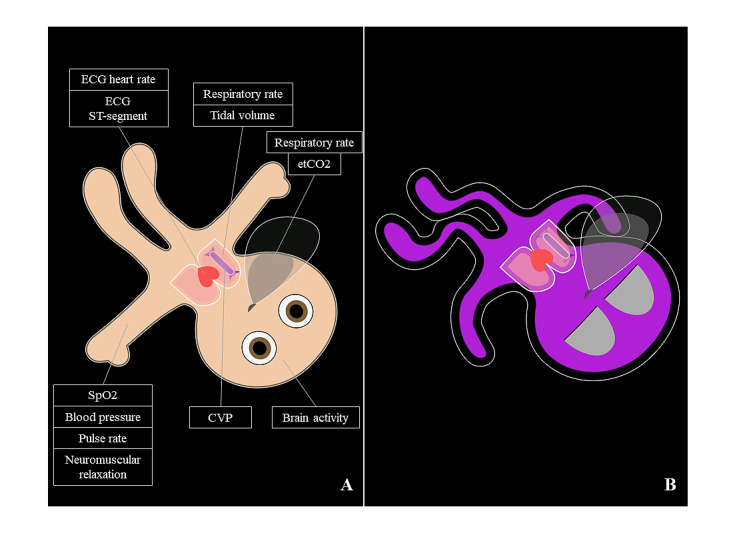
Two examples of Visual-Patient-avatar used during the high-fidelity simulation. CVP: central venous pressure; ECG: electrocardiogram; etCO2: end-tidal carbon dioxide; SpO2: peripheral oxygen saturation; ST: ST-segment.
After a short briefing and a training scenario, the participants completed 3 different emergency scenarios, each with 1 of the following 3 different monitor modalities: only Visual-Patient-avatar, Split Screen, and only conventional, number-based and waveform-based monitor. Figure 2 illustrates an example of a Split Screen display during simulation, and the video in Multimedia Appendix 2 shows a recording of a simulation scenario. After completing all scenarios, we asked the following 2 questions: “What do you like about the monitor settings? Eg, particular strengths?” and “What do you dislike about the monitor settings? Eg, potential problems, limitations?” The study authors TRR and SS recorded the participants’ responses as field notes on an iPad (Apple Inc). The participants reviewed the final field note transcripts, modifying or adding to them if warranted.
Figure 2.
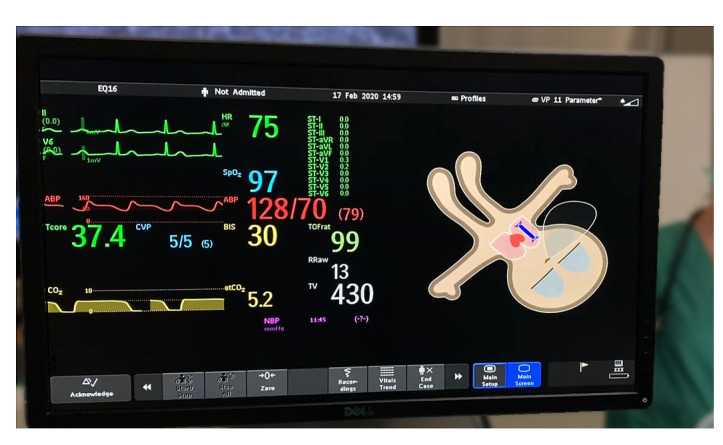
Example of a Split Screen display during simulation with the Conventional monitor on the left and the Visual-Patient-avatar on the right side. The beige skin tone corresponds to a normal peripheral oxygen saturation, and closed eyes imply a sedated patient.
Semiquantitative Analysis
After collecting all answers, we translated them from German to English using an online translating service, Deepl (DeepL GmbH). In Multimedia Appendix 3, we provide the complete translated field notes. There were no comments made from 12 participants. To gain a first impression by identifying frequently mentioned terms, we excluded filler words such as “and” or “the” and performed a word count using Microsoft Word (Microsoft Corporation). Although the word count does not provide information about the content of individual statements, this approach helped us to identify similar expressions. Subsequently, we grouped the statements using the template approach, identified main topics, and generated a coding tree, which we modified until all essential and frequent statements could be classified [14,15]. According to the recommendations of reporting qualitative research, study authors SA and LB, who were not involved in the interview process, evaluated the statements independently of each other, using the final coding tree displayed in Figure 3, which was created using draw.io (Seibert Media GmbH) [16-18]. Before determining a joint code in case of disagreement, we calculated the interrater reliability to validate the rating.
Figure 3.
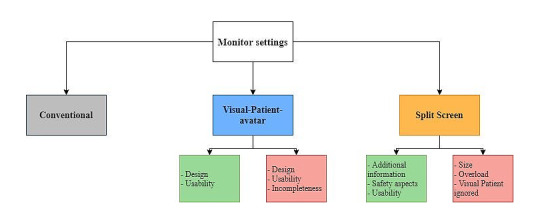
Hierarchical coding tree concerning user perceptions of the 3 different monitor modalities. The green boxes include positive subthemes of the respective major topic. The red boxes contain negative subthemes of the corresponding major topic.
Statistical Analysis
We report the number of statements and their percentages relating to the superior topics. To manage our data and to generate the figures, we used Microsoft Word and Microsoft Excel. To quantify the interrater reliability, when assigning the individual statements to a particular topic of the final coding tree, we calculated the Cohen kappa using R, version 4.0.5 (R Foundation for Statistical Computing) [19]. To estimate percent agreement, we used Microsoft Excel.
Results
Participant and Field Notes Characteristics
We acquired field notes between May 4, 2020, and May 28, 2020. All participants were employees of the University Hospital of Zurich. Of the total 104 participants, 92 (88%) senior physicians, resident physicians, nurse anesthetists, and trainee nurse anesthetists took part in the interview process right after completing the simulation scenarios. Table 1 provides a detailed description of the study and participant characteristics.
Table 1.
Study and participant characteristics in detail (n=92).
| Study and participant characteristics | Values |
| Participants who submitted field notes, n (%) | 92 (88) |
| Female participants, n (%) | 46 (50) |
| Senior physicians, n (%) | 14 (15) |
| Resident physicians, n (%) | 33 (36) |
| Nurse anesthetists, n (%) | 30 (33) |
| Trainee nurse anesthetists, n (%) | 17 (16) |
| Total anesthesia experience (years), mean (IQR) | 6.6 (1.5-8) |
Analyzing the field notes obtained, we identified 329 individual statements consisting of 2807 words. Of 329 statements, 22 (7%) were not comprehensible to us in terms of content even after several discussions, so we classified them as “not codable.” Statements in this category included subjective opinions such as “I like it” (participant #13.1). The remaining 307 statements were analyzed semiquantitatively, which allows the calculation of the proportions of individual statements among the main topics and subthemes without applying statistical tests [20,21]. Overall, the ratio of statements to the question, “What do you like about the monitor settings” (144/307, 47%) compared to the negative perceptions (163/307, 53%) was balanced.
Semiquantitative Analysis
Beginning our semiquantitative analysis, we performed word counts to expose potential main themes. The analysis revealed that “Visual Patient” was the most frequently occurring term in the field notes obtained to answer both the positive (35 times in 144 statements) and negative questions (38 times in 163 statements).
Based on using qualitative research methods and testing 3 monitor modalities, the final coding tree contains the 3 main categories of Visual-Patient-avatar, Split Screen, and Conventional monitor, as well as 4 main topics with 11 subthemes. When independently assigning all 327 statements received to 1 of these topics, the study authors SA and LB achieved 80% interrater agreement with a substantial Cohen kappa of 0.78 [22]. In the case of differently coded statements, a review and joint assignment followed to achieve 100% interrater agreement after the second round of coding. Figure 4 visualizes the percentage distribution of all statements among the different categories. The 3 main categories are located in the innermost circle. The associated major topics and subthemes are displayed hierarchically toward the outside. Table 2 outlines the major topics with examples. In the subsequent sections, we describe the individual categories in detail with percentages and examples. The calculations refer to the codable statements.
Figure 4.
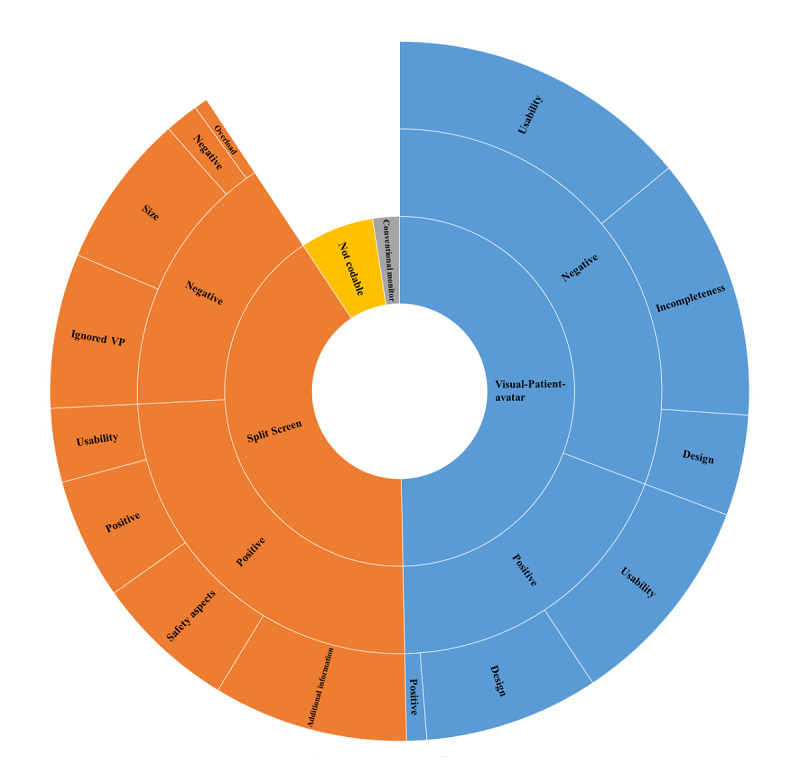
Sunburst diagram to reflect the user perceptions of the 3 different monitor settings. The width of a section represents the respective percentage of the topic on all given statements (N=307). Ignored VP: ignored Visual-Patient-avatar.
Table 2.
The major topics with participant count, percentages, and examples.
| Major topics and subthemes | Examples | ||
| Visual-Patient-avatar positive (61/307, 20%) |
|
||
|
|
Design |
|
|
|
|
Usability |
|
|
| Visual-Patient-avatar negative (99/307, 32%) |
|
||
|
|
Design |
|
|
|
|
Usability |
|
|
|
|
Incompleteness |
|
|
| Split Screen positive (79/307, 26%) |
|
||
|
|
Additional information |
|
|
|
|
Safety aspects |
|
|
|
|
Usability |
|
|
| Split Screen negative (60/307, 20%) |
|
||
|
|
Size |
|
|
|
|
Overload |
|
|
|
|
Visual-Patient-avatar ignored |
|
|
| Conventional monitor (8/307, 3%) |
|
||
aParticipant number.
Statements About Visual-Patient-Avatar
We assigned 160 of 307 (52%) statements to the main category Visual-Patient-avatar. Through inductive free coding, the 2 major topics, Visual-Patient-avatar positive (61/307, 20%) and Visual-Patient-avatar negative (99/307, 32%), were revealed.
We divided the positive major topic into the 2 subthemes, design (26/307, 8%) and usability (32/307, 10%). Concerning design features, the participants distinguished the simplified (participant #13.2) and realistic (participant #17.1) appearance of the avatar. Participant #11.2 outlined that “Especially oxygenation and body temperature is illustrated well.” The participants also recognized advantages in terms of usability. They found that Visual-Patient-avatar is “Intuitively understandable” (participant #31.1), “Gives a good overview” (participant #34.1), and helps to grasp the situation quickly (participant #37.1). We allocated more common statements such as “Integration of all values on one avatar” (participant #47.2) to the major topic Visual-Patient-avatar positive (3/307, 1%).
Regarding negative properties of the avatar, the participants’ responses depicted design (15/307, 5%), usability (45/307, 15%), and incompleteness (39/307, 13%) as subthemes. For participant #43.2, the thorax displayed too small, and the vena cava representation was unclear. Others raised concerns about possible misinterpretations (participant #46.1) because of the unfamiliar (participant #48.2) and confusing (participant #48.1) vital sign presentation within Visual-Patient-avatar technique. Without concrete values (participant #35.2) and curves such as the electrocardiogram (participant #42.2), the avatar did not help in solving the emergency scenarios.
Statements About the Split Screen
In 139 of 307 (46%) statements, the participants noticed this main category, which we classified into the major topics Split Screen positive (79/307, 26%) and Split Screen negative (60/307, 20%).
In interrater consent, the positive major topic included the 3 subthemes additional information (29/307, 9%), safety aspects (21/307, 7%), and usability (11/307, 4%). Through “Increasing attention” (participant #10.1), “Faster recognition of changes” (participant #29.2), and the “Quick overview” (participant #45.2), the participants perceived a higher level of safety. Several participants found the Split Screen mode overall “Helpful” (participant #47.1) and “Effective” (participant #17.1) in its use. We allocated responses that generally considered the combination advantageous to the major topic, positive Split Screen (18/307, 6%).
The negative major topic concerning Split Screen enclosed the 3 subthemes, “size,” “overload,” and “Visual-Patient-avatar ignored.” These were named, respectively, in 23/307 (7%), 23/307 (7%), and 9/307 (3%) statements. The participants criticized the small display and thus the difficulty of detecting details of the curves (participant #20.1) and the Visual-Patient-avatar (participant #21.2). Furthermore, they claimed the Split Screen to be crowded (participant #30.2), and that there is “Too much information at once in the emergency” (participant #12.2). In addition, the analysis of the field notes discovered that several participants ignored the avatar. General annotations such as “Not sure about the added benefit” (participant #48.1) were assigned to the major topic, negative Split Screen (5/307, 2%).
Statements About the Conventional Monitor
A small number of the field notes referred to the main category Conventional monitor (8/307, 3%). Some participants just stated that they “Prefer the usual monitor view” (participant #26.1). Furthermore, we grouped responses that mentioned the familiar audio support in this main category.
Discussion
Principal Findings
This semiquantitative single-center study explored the impressions of anesthesia personnel when using the existing Conventional monitor compared with the new modality Visual-Patient-avatar—either the avatar only or the Split Screen variant. User perceptions can uncover improvement opportunities, and their consideration is essential for the success of new medical techniques. We assigned most of the statements to the main category Visual-Patient-avatar, highlighting positive characteristics and negative features such as the absence of quantitative data. Many annotations also evaluated the Split Screen modality, while only a few participants commented on the well-known Conventional monitor. The latter seems coherent as Visual-Patient-avatar is a novelty and thus attention catching.
The avatar’s development was guided by the idea of providing a monitor tool that improves situation awareness through its user-centered design principles. Following the definition of a user-centered design through Mica Endsley [9], many participants stated the avatar technique to include beneficial design and usability features such as being simplified and intuitive (positive Visual-Patient-avatar: 61/307, 20%). When used with the Conventional monitor in Split Screen mode, Visual-Patient-avatar increases attention and provides a quick overview. Possible changes in vital signs can then be quantified using the conventional display (safety aspects: 21/307, 7%). The aspect of time saving through faster detection is essential in patient care, as for example, postoperative renal dysfunction is related to the overall duration of hypotension during general anesthesia [23].
Many participants claimed the missing numbers and curves when using only the avatar makes a more precise diagnosis impossible (incompleteness: 39/307, 13%). In Visual-Patient-avatar, the data for each vital sign is preprocessed to show different states (no data, too low, normal, or too high), aiming to reduce complexity. We understand the technology as a supplement, which cannot replace the Conventional monitor; however, it can improve care providers’ situation awareness by presenting information that is easy to perceive and comprehend.
On the question, “What did you dislike about the monitor settings?”, this analysis found that size (23/307, 7%) and overload (23/307, 7%) were the main critical points concerning the Split Screen mode. During the simulation study, the scenarios run on 12-inch patient monitors (Philips IntelliVue MX500; Koninklijke Philips NV, Amsterdam, The Netherlands). However, the technique for the real-life clinical implementation is compatible with the Philips IntelliVue MX 550 monitor, which offers a larger display of 15 inches. This fact can mitigate the criticism, but it is known that a high information load can have a detrimental effect on the ability to set priorities and can confuse the individual [24]. This would contradict the basic idea of Visual-Patient-avatar and must be kept in mind.
The impression of an overload could also occur because the technique of the Visual-Patient-avatar and its implementation as Split Screen variant is new and therefore cognitively demanding. Accordingly, several participants mentioned being unfamiliar with the avatar, whether used individually or in Split Screen mode. Upon introduction of the new technique into clinical routine, all users will receive education and training lessons. Nevertheless, it will take time to get used to the new monitor modalities and fully implement them mentally, as especially very experienced care providers have been working with the Conventional monitor modality for decades. The successful implementation of new techniques can be demonstrated by the sonographically guided insertion of central venous catheters [25]. After initial skepticism, this method is nowadays preferred both in the literature and clinically, as the complication rate is lower than with landmark-guided puncture [26].
To achieve a high level of user acceptance, an intuitive interface and cognitive ease are crucial points [27]. Visual-Patient-avatar presents the information close to clinical reality. For example, the avatar’s skin turns purple in case of hypoxemia, or its eyes are open when the brain-activity sensor detects a high signal. The participants’ appreciation of the realistic and clear vital sign display (design: 26/307, 8%) is in line with the results of the study by Wachter and colleagues [28], which shows that an anatomically related interface is particularly intuitive. However, together with design and technical specialists from Philips (Koninklijke Philips NV), an intensive redesign process was carried out to improve weaknesses in the design, such as the vena cava display. Even though some steps are still needed until clinical introduction, we expect visualization techniques to have a great future in medicine after this study. It is encouraging that Hamilton Medical AG provides the “dynamic lung” in ventilators to visualize specific lung parameters [29].
Strengths and Limitations
This study has several limitations. In qualitative and semiquantitative analysis, the structure and results are developed inductively and cannot be applied to a broader population as it does not investigate statistical significance. Nevertheless, this approach allowed us to gain firsthand perceptions and experiences from our participants right after using the different monitor modalities. Generally, a nonquantitative assessment stays close to the participants’ point of view, implying a certain subjectivity [30,31]. However, this is put into perspective by the high number of participants and their diversity. As a single-center study, possible selection bias cannot be excluded. It is conceivable that the results vary under different circumstances.
To date, only computer-based studies have been conducted with the Visual-Patient-avatar [10,11]. One of the strengths is the high-fidelity simulation, which made it possible to test the new technique realistically during anesthesiologic emergency scenarios and to derive conclusions for its use under clinical conditions [32]. Thus, we obtained the first opinions on Visual-Patient-avatar directly after experiencing the urgency of emergent patient treatment. These findings greatly impact the further development of the technique up to the point of clinical implementation.
Conclusion
We designed this study to determine care providers’ perceptions concerning monitor modalities incorporating the Visual-Patient-avatar technique. One of the key findings was that the participants experienced the avatar technique’s underlying design principles and characteristics positively under active use in the context of a high-fidelity simulation. This insight complements those of earlier studies using the Visual-Patient-avatar technique in computer-based studies [33]. The participants confirmed the value of the Split Screen mode through its combination of visual impressions and simultaneous quantification with numerical parameters. This monitor variant, planned for future clinical implementation, gives a quick overview and draws attention to changes specified by the conventional part. The next step in the development is a planned real-life introduction study of the avatar in Split Screen mode under actual clinical conditions. This modality’s weakness, based on the large amount of information displayed, will be reflected in the further planning process and will be reviewed through future studies. By testing the avatar in a simulated clinical environment for the first time, we are taking a significant step toward our vision: to help care providers in situations of high cognitive load to better prioritize information and thus positively influence decision-making for the patient’s benefit.
Acknowledgments
The authors are thankful to the study participants for their time and effort. Furthermore, the authors thank biostatistician Julia Braun-Gruebel for her statistical advice regarding this manuscript. This study was funded by the Institute of Anesthesiology, University Hospital of Zurich, Switzerland.
Video with two examples of an animated Visual-Patient-avatar.
Video of simulations scenario presenting Visual-Patient-avatar and Conventional monitor.
The translated field notes of 92 participants. The brackets [] indicate which parts were each assessed as one statement.
Footnotes
Availability of Data and Materials
The data sets used and analyzed during this study are available from the corresponding author upon reasonable request.
Authors' Contributions: Conception and design: SA, SS, TRR, CBN, DRS, DWT, and LB. Acquisition of data: SA, SS, TRR, CBN, DWT, and LB. Analysis and interpretation of data: SA, DRS, DWT, and LB. Drafting of the article or critical revision of the manuscript: SA, SS, TRR, CBN, DRS, DWT, and LB. Final approval of the version to be published: SA, SS, TRR, CBN, DRS, DWT, and LB.
Conflicts of Interest: DWT and CBN are designated inventors of Visual-Patient-avatar technology, for which the University of Zurich holds various patents and trademarks. There are cooperation and licensing agreements with Philips Medizin Systeme Böblingen GmbH, Böblingen, Germany; Koninklijke Philips NV, Amsterdam, The Netherlands; Philips Research/Philips Electronics Nederland BV, Eindhoven, The Netherlands, Philips North America, Cambridge, MA, USA. Under these agreements, DWT receives grant support, and DWT and CBN receive travel support and may receive royalties. DWT, CBN, and DRS are designated inventors of Visual Clot technology, for which the University of Zurich holds various patents and trademarks. The University of Zurich signed a letter of intent for a cooperation and licensing agreement with Instrumentation Laboratory Company/Werfen Corporation, Bedford, MA, USA and Barcelona, Spain. Under resulting agreements, they may receive royalties. DWT, CBN, and DRS received travel support for consulting Instrumentation Laboratory, Bedford, MA, USA. DWT received honoraria and travel support from the Swiss Foundation for Anesthesia Research, Zurich, Switzerland. DRS’s academic department is receiving grant support from the Swiss National Science Foundation, Berne, Switzerland, the Swiss Society of Anesthesiology and Perioperative Medicine, Berne, Switzerland, the Swiss Foundation for Anesthesia Research, Zurich, Switzerland, Vifor SA, Villars-sur-Glâne, Switzerland, and Vifor (International) AG, St. Gallen, Switzerland. DRS is cochair of the ABC-Trauma Faculty, sponsored by unrestricted educational grants from Novo Nordisk Health Care AG, Zurich, Switzerland, CSL Behring GmbH, Marburg, Germany, LFB Biomédicaments, Courtaboeuf Cedex, France, and Octapharma AG, Lachen, Switzerland. DRS received honoraria or travel support for consulting or lecturing from the following: Danube University of Krems, Austria; US Department of Defense, Washington; European Society of Anesthesiology and Intensive Care, Brussels, BE; Korean Society for Patient Blood Management, Seoul, Korea; Korean Society of Anesthesiologists, Seoul, Korea; Network for the Advancement of Patient Blood Management, Haemostasis and Thrombosis, Paris, France; Alexion Pharmaceuticals Inc, Boston, MA, USA; Bayer AG, Zürich, Switzerland; B. Braun Melsungen AG, Melsungen, Germany; CSL Behring GmbH, Hattersheim am Main, Germany and Berne, Switzerland; Celgene International II Sàrl, Couvet, Switzerland; Daiichi Sankyo AG, Thalwil, Switzerland; Haemonetics, Braintree, MA, USA; Instrumentation Laboratory (Werfen), Bedford, MA, USA; LFB Biomédicaments, Courtaboeuf Cedex, France; Merck Sharp & Dohme, Kenilworth, New Jersey, USA; Novo Nordisk Health Care AG, Zurich, Switzerland; PAION Deutschland GmbH, Aachen, Germany; Pharmacosmos A/S, Holbaek, Denmark, Pfizer AG, Zürich, Switzerland; Pierre Fabre Pharma, Alschwil, Switzerland; Portola Schweiz GmbH, Aarau, Switzerland, Roche Diagnostics International Ltd, Reinach, Switzerland; Sarstedt AG & Co., Sevelen, Switzerland and Nümbrecht, Germany; Shire Switzerland GmbH, Zug, Switzerland; Tem International GmbH, Munich, Germany; Vifor Pharma, Munich, Germany; Neuilly sur Seine, France and Villars-sur-Glâne, Switzerland, Vifor (International) AG, St. Gallen, Switzerland; and Zuellig Pharma Holdings, Singapore, Singapore.
References
- 1.WHO Guidelines for Safe Surgery 2009. World Health Organization. 2009. [2022-03-07]. http://apps.who.int/iris/bitstream/handle/10665/44185/9789241598552_eng.pdf;jsessionid=BC88C8E245C68B57989D3EBAFC3FC3EE?sequence=1 . [PubMed]
- 2.Irwin MG, Kong VKF. Quantifying and communicating peri-operative risk. Anaesthesia. 2014 Dec;69(12):1299–303. doi: 10.1111/anae.12881. doi: 10.1111/anae.12881. [DOI] [PubMed] [Google Scholar]
- 3.Li G, Warner M, Lang BH, Huang L, Sun LS. Epidemiology of anesthesia-related mortality in the United States, 1999-2005. Anesthesiology. 2009 Apr;110(4):759–65. doi: 10.1097/aln.0b013e31819b5bdc. https://pubs.asahq.org/anesthesiology/article-lookup/doi/10.1097/aln.0b013e31819b5bdc . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bainbridge D, Martin J, Arango M, Cheng D, Evidence-based Peri-operative Clinical Outcomes Research (EPiCOR) Group Perioperative and anaesthetic-related mortality in developed and developing countries: a systematic review and meta-analysis. Lancet. 2012 Sep 22;380(9847):1075–81. doi: 10.1016/S0140-6736(12)60990-8.S0140-6736(12)60990-8 [DOI] [PubMed] [Google Scholar]
- 5.Schulz CM, Krautheim V, Hackemann A, Kreuzer M, Kochs EF, Wagner KJ. Situation awareness errors in anesthesia and critical care in 200 cases of a critical incident reporting system. BMC Anesthesiol. 2016 Jan 16;16:4. doi: 10.1186/s12871-016-0172-7. https://bmcanesthesiol.biomedcentral.com/articles/10.1186/s12871-016-0172-7 .10.1186/s12871-016-0172-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Schulz CM, Burden A, Posner KL, Mincer SL, Steadman R, Wagner KJ, Domino KB. Frequency and Type of Situational Awareness Errors Contributing to Death and Brain Damage: A Closed Claims Analysis. Anesthesiology. 2017 Aug;127(2):326–337. doi: 10.1097/ALN.0000000000001661. https://pubs.asahq.org/anesthesiology/article-lookup/doi/10.1097/ALN.0000000000001661 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Schulz CM, Endsley MR, Kochs EF, Gelb AW, Wagner KJ. Situation awareness in anesthesia: concept and research. Anesthesiology. 2013 Mar;118(3):729–42. doi: 10.1097/ALN.0b013e318280a40f. https://pubs.asahq.org/anesthesiology/article-lookup/doi/10.1097/ALN.0b013e318280a40f . [DOI] [PubMed] [Google Scholar]
- 8.WHO's patient-safety checklist for surgery. The Lancet. 2008 Jul 05;372(9632):1. doi: 10.1016/S0140-6736(08)60964-2.S0140-6736(08)60964-2 [DOI] [PubMed] [Google Scholar]
- 9.Endsley M. Designing for situation awareness: an approach to user-centered design. Boca Raton, Florida, US: CRC Press; 2012. Jan 18, pp. 1–396. [Google Scholar]
- 10.Garot O, Rössler J, Pfarr J, Ganter MT, Spahn DR, Nöthiger CB, Tscholl DW. Avatar-based versus conventional vital sign display in a central monitor for monitoring multiple patients: a multicenter computer-based laboratory study. BMC Med Inform Decis Mak. 2020 Feb 10;20(1):26. doi: 10.1186/s12911-020-1032-4. https://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/s12911-020-1032-4 .10.1186/s12911-020-1032-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tscholl DW, Handschin L, Neubauer P, Weiss M, Seifert B, Spahn DR, Noethiger CB. Using an animated patient avatar to improve perception of vital sign information by anaesthesia professionals. Br J Anaesth. 2018 Sep;121(3):662–671. doi: 10.1016/j.bja.2018.04.024. https://linkinghub.elsevier.com/retrieve/pii/S0007-0912(18)30332-5 .S0007-0912(18)30332-5 [DOI] [PubMed] [Google Scholar]
- 12.Tscholl DW, Rössler J, Handschin L, Seifert B, Spahn DR, Nöthiger CB. The Mechanisms Responsible for Improved Information Transfer in Avatar-Based Patient Monitoring: Multicenter Comparative Eye-Tracking Study. J Med Internet Res. 2020 Mar 16;22(3):e15070. doi: 10.2196/15070. https://www.jmir.org/2020/3/e15070/ v22i3e15070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Roche TR, Said S, Braun J, Maas EJC, Machado C, Grande B, Kolbe M, Spahn DR, Nöthiger CB, Tscholl DW. Avatar-based patient monitoring in critical anaesthesia events: a randomised high-fidelity simulation study. Br J Anaesth. 2021 May;126(5):1046–1054. doi: 10.1016/j.bja.2021.01.015.S0007-0912(21)00034-9 [DOI] [PubMed] [Google Scholar]
- 14.Brooks J, King N. Doing Template Analysis: Evaluating an End of Life Care Service. Sage Research Methods Cases. 2014:1–20. doi: 10.4135/978144627305013512755. http://eprints.hud.ac.uk/id/eprint/19707/1/Brooks_and_King_doingTA_EoLCservice.pdf . [DOI] [Google Scholar]
- 15.Brooks J, McCluskey S, Turley E, King N. The Utility of Template Analysis in Qualitative Psychology Research. Qual Res Psychol. 2015 Apr 03;12(2):202–222. doi: 10.1080/14780887.2014.955224. http://europepmc.org/abstract/MED/27499705 .955224 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007 Dec;19(6):349–57. doi: 10.1093/intqhc/mzm042.mzm042 [DOI] [PubMed] [Google Scholar]
- 17.O'Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014 Sep;89(9):1245–51. doi: 10.1097/ACM.0000000000000388. https://journals.lww.com/24979285.pmid . [DOI] [PubMed] [Google Scholar]
- 18.Dossett LA, Kaji AH, Cochran A. SRQR and COREQ Reporting Guidelines for Qualitative Studies. JAMA Surg. 2021 Sep 01;156(9):875–876. doi: 10.1001/jamasurg.2021.0525.2778475 [DOI] [PubMed] [Google Scholar]
- 19.McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb) 2012;22(3):276–82. http://www.biochemia-medica.com/2012/22/276 . [PMC free article] [PubMed] [Google Scholar]
- 20.Kostoff RN. Semiquantitative methods for research impact assessment. Technological Forecasting and Social Change. 1993 Nov;44(3):231–244. doi: 10.1016/0040-1625(93)90070-n. [DOI] [Google Scholar]
- 21.Webster CS, McKillop A, Bennett W, Bagg W. A Qualitative and Semiquantitative Exploration of the Experience of a Rural and Regional Clinical Placement Programme. Med Sci Educ. 2020 Jun;30(2):783–789. doi: 10.1007/s40670-020-00949-6. http://europepmc.org/abstract/MED/34457735 .949 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977 Mar;33(1):159–74. [PubMed] [Google Scholar]
- 23.Zarbock A, Koyner JL, Hoste EAJ, Kellum JA. Update on Perioperative Acute Kidney Injury. Anesth Analg. 2018 Nov;127(5):1236–1245. doi: 10.1213/ANE.0000000000003741. [DOI] [PubMed] [Google Scholar]
- 24.Schick AG, Gordon LA, Haka S. Information overload: A temporal approach. Accounting, Organizations and Society. 1990 Jan;15(3):199–220. doi: 10.1016/0361-3682(90)90005-f. [DOI] [Google Scholar]
- 25.Cameron KA, Cohen ER, Hertz JR, Wayne DB, Mitra D, Barsuk JH. Barriers and Facilitators to Central Venous Catheter Insertion: A Qualitative Study. J Patient Saf. 2021 Dec 01;17(8):e1296–e1306. doi: 10.1097/PTS.0000000000000477.01209203-202112000-00087 [DOI] [PubMed] [Google Scholar]
- 26.Teichgräber UK, Benter T, Gebel M, Manns MP. A sonographically guided technique for central venous access. AJR Am J Roentgenol. 1997 Sep;169(3):731–3. doi: 10.2214/ajr.169.3.9275887. [DOI] [PubMed] [Google Scholar]
- 27.Agarwal R, Karahanna E. Time Flies When You're Having Fun: Cognitive Absorption and Beliefs about Information Technology Usage. MIS Quarterly. 2000 Dec;24(4):665. doi: 10.2307/3250951. [DOI] [Google Scholar]
- 28.Wachter SB, Agutter J, Syroid N, Drews F, Weinger MB, Westenskow D. The employment of an iterative design process to develop a pulmonary graphical display. J Am Med Inform Assoc. 2003;10(4):363–72. doi: 10.1197/jamia.M1207. http://europepmc.org/abstract/MED/12668693 .M1207 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ventilation Cockpit: A common user interface. Hamilton Medical. 2021. [2021-11-30]. https://www.hamilton-medical.com/ja/Solutions/Ventilation-Cockpit-user-interface.html .
- 30.Neergaard MA, Olesen F, Andersen RS, Sondergaard J. Qualitative description - the poor cousin of health research? BMC Med Res Methodol. 2009 Jul 16;9:52. doi: 10.1186/1471-2288-9-52. https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/1471-2288-9-52 .1471-2288-9-52 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Carr LT. The strengths and weaknesses of quantitative and qualitative research: what method for nursing? J Adv Nurs. 1994 Oct;20(4):716–21. doi: 10.1046/j.1365-2648.1994.20040716.x. [DOI] [PubMed] [Google Scholar]
- 32.Merry AF, Hannam JA, Webster CS, Edwards K, Torrie J, Frampton C, Wheeler DW, Gupta AK, Mahajan RP, Evley R, Weller JM. Retesting the Hypothesis of a Clinical Randomized Controlled Trial in a Simulation Environment to Validate Anesthesia Simulation in Error Research (the VASER Study) Anesthesiology. 2017 Mar;126(3):472–481. doi: 10.1097/ALN.0000000000001514. https://pubs.asahq.org/anesthesiology/article-lookup/doi/10.1097/ALN.0000000000001514 . [DOI] [PubMed] [Google Scholar]
- 33.Tscholl DW, Rössler J, Said S, Kaserer A, Spahn DR, Nöthiger CB. Situation Awareness-Oriented Patient Monitoring with Visual Patient Technology: A Qualitative Review of the Primary Research. Sensors (Basel) 2020 Apr 09;20(7):2112. doi: 10.3390/s20072112. https://www.mdpi.com/resolver?pii=s20072112 .s20072112 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video with two examples of an animated Visual-Patient-avatar.
Video of simulations scenario presenting Visual-Patient-avatar and Conventional monitor.
The translated field notes of 92 participants. The brackets [] indicate which parts were each assessed as one statement.