

Abstract
Background
Non-communicable diseases (NCDs) are the leading cause of death worldwide. However, current evidence regarding the efficacy and cost-effectiveness of community intervention and health promotion programs for NCDs, specifically hypertension, obesity, diabetes, and dyslipidemia, in East and Southeast Asia has not yet been systematically reviewed. We systematically reviewed the literature from East and Southeast Asian countries to answer 2 clinical questions: (1) do health promotion programs for hypertension, obesity, diabetes, and dyslipidemia reduce cardiovascular events and mortality; and (2) are these programs cost-effective?
Methods and Results
Electronic literature searches were performed across Medline, Cochrane Library, and Ichushi using key words and relevant subject headings related to randomized controlled trials, comparative studies, quasi-experimental studies, or propensity score matching that met eligibility criteria that were defined for each question. In all, 3,389 records were identified, of which 12 full-text articles were reviewed. Three papers were from Japan, 7 were from China/Hong Kong Special Administrative Region, and 2 were from South Korea. None were from Southeast Asia. Four papers examined the effect of community intervention or health promotion on the incidence of cardiovascular events or mortality. Eight studies examined the cost-effectiveness of interventions.
Conclusions
The literature review revealed that community intervention and health promotion programs for the control of NCDs are a cost-effective means of reducing cardiovascular events and mortality in East Asian countries.
Key Words: Asia, Community intervention, Health policy, Health promotion program, Non-communicable disease
Non-communicable diseases (NCDs), such as hypertension, diabetes, obesity, and dyslipidemia, are a huge social burden in many countries; collectively, these diseases now account for over 50% of deaths globally.1 These NCDs are characterized by slow development, a long morbidity period, and multiple causes. They depress earnings, wages, workforce participation, and labor productivity and increase job turnover, early retirement, and disability.2,3 However, these diseases are preventable, and several global action plans targeting risk factors for cardiovascular diseases and diabetes have been implemented worldwide.4 In 2013, the World Health Organization (WHO) put forth its global action plan for the prevention of NCDs.5,6
In Europe, which, of the 6 WHO regions, is the most affected by NCDs,7 health policy should aim not only to improve individual health behaviors, but also to reduce socioeconomic inequality.8 The WHO-NCD global surveillance strategy is based on a multidimensional view of disease determinants including physiological influences, lifestyle influences, environmental influences, and social structure.
In the US, to meet the chronic disease burden, the US Centers for Disease Control and Prevention (CDC) uses 4 cross-cutting strategies: (1) epidemiology and surveillance to monitor trends and inform programs; (2) environmental approaches that promote health and support healthy behaviors; (3) health system interventions to improve the effective use of clinical and other preventive services; and (4) community resources linked to clinical services that sustain improved management of chronic conditions.9
In developing countries, despite rather positive results of randomized controlled trials (RCTs), a firm conclusion about the effectiveness of public health interventions against NCDs is not yet possible because of the limited number of studies in low- and middle-income countries.10
Compared with Europe and the US, there is little information about health promotion for NCD in East or Southeast Asia. However, in Japan, the health status of the population has improved rapidly over the past half-century and, for the past decade, Japan has been ranked number 1 globally for population health metrics, including life expectancy and healthy life expectancy at birth.11 Japan has experienced an epidemiological transition from infectious to non-infectious diseases, followed by a gradual decrease in cerebrovascular diseases; however, as life expectancy has increased and Japan’s economy has developed, the burden of NCDs has also increased, accounting for approximately 60% of total deaths in 2012.12 Treatments for NCDs now consume approximately 30% of total medical and long-term care expenditure in Japan.13 Addressing these burdens will require focused policies and renewed political attention.2,14 However, the current evidence of the effectiveness of community intervention and health promotion programs for the prevention of NCDs in East or Southeast Asia has not been systematically reviewed. In addition, the WHO recognizes the need for greater prevention of NCDs in the Western Pacific region.15
In this study, by conducting a systematic review of the literature, we examined the efficacy of community interventions and health promotion programs for reducing cardiovascular events and mortality in in East and Southeast Asian countries. We first constructed 4 clinical questions (see below) associated with the treatment of NCDs, specifically hypertension, obesity, diabetes, and dyslipidemia, in Japan compared with other East and Southeast Asian countries and then used the PICO (Participants, Interventions, Comparators, and Outcomes) process to answer those questions. The interventions examined were educational programs designed to reduce the incidence of NCDs and improve associated clinical outcomes.
The main outcomes were a reduction in the incidence of NCDs and whether the interventions were cost-effective. Other outcome measures included quality of life, economic burden, and caregiver burden. Two rounds of screening of the literature search results were conducted, followed by the construction of tables summarizing the studies and research findings.
Clinical Questions
The 4 clinical questions addressed in this study were as follows:
1. Do community intervention and health promotion programs for the prevention of hypertension, diabetes, obesity, or dyslipidemia reduce cardiovascular events and mortality in Japan?
2. Do community intervention and health promotion programs for the prevention of hypertension, diabetes, obesity, or dyslipidemia reduce cardiovascular events and mortality in East and Southeast Asian countries?
3. Are community intervention and health promotion programs for the prevention of hypertension, diabetes, obesity, or dyslipidemia cost-effective in Japan?
4. Are community intervention and health promotion programs for the prevention of hypertension, diabetes, obesity, or dyslipidemia cost-effective in East and Southeast Asian countries?
Methods
Search Strategy
The bibliographic databases Medline, Cochrane Library, and Ichushi (Japanese) were searched (Figure). The search strategy was configured for each database by using index terms and free text words, including the terms “NCDs”, “Cardiovascular Diseases”, “Hypertension”, “Prevention & Control”, “Healthy People Programs”, “Health Promotion”, “Japan”, “East Asia”, “Southeast Asia”, “Economics”, “Costs”, “Expenditure”, “Budget”, and “Economy”, as well as other terms suitable for a PICO analysis. The search terms used for each database are provided in Supplementary Tables 1–3. The search included only studies published in English and Japanese before April 2019. The Cochrane Collaboration Risk of Bias Tool was used to evaluate the risk of bias.16 A study was given an overall rating of low-to-intermediate risk of bias if the RCT was not thought to be at high risk of bias for any domain of study quality.
Figure.
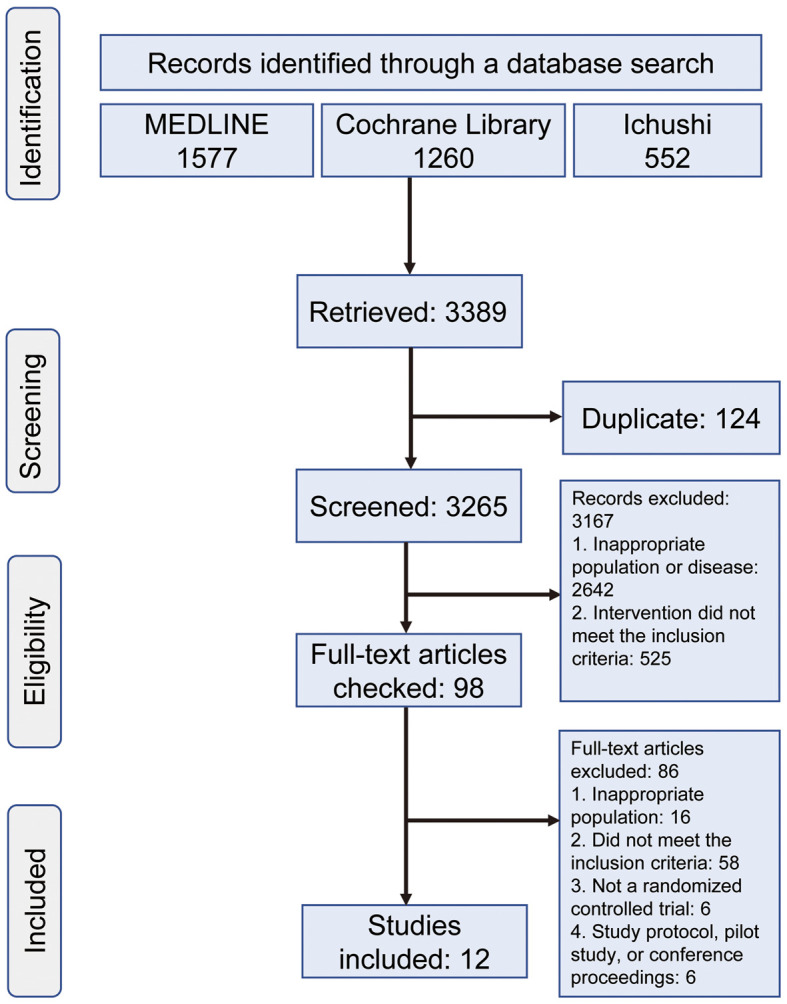
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram of the articles included in the analysis.
Article Selection
Articles were selected by following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.17 We included only articles describing original research that used a randomized-controlled, comparative, or quasi-experimental design or used propensity score matching with measurable outcomes and evaluated health interventions for the management of NCDs in Japan or East and Southeast Asian countries. We excluded papers that: only had an abstract; were a review, development, usability, or feasibility study; examined a non-Asian population; or described interventions for which the end-users were not patients with NCDs. We also excluded papers when the intervention was performed at a hospital or when the study did not incorporate any self-management process.
Data Extraction and Analysis
Two authors (A.H., A.S.) screened the publications, first based on the title and abstract and then through full-text reviews. Any discrepancies were resolved by consensus between the 2 authors. Descriptive characteristics of the studies, including study design, sample size, target disease, and age and sex proportions, were extracted. Then, the interventions described in the studies were summarized, along with any control treatments used. Any self-management processes incorporated in the interventions were excepted. Finally, the statistical results for the outcomes reported in the studies were summarized based on study design and effectiveness.
This systematic review did not include empirical research; therefore there were no human participants.
Results
Of the 3,389 studies identified through the literature search, only 12 full-text articles met all the inclusion and exclusion criteria; these articles are summarized in Tables 1–4.18–29 Three papers were from Japan, 7 from China/Hong Kong Special Administrative Region, and 2 from South Korea. None of the articles were from institutes in Southeast Asia. Four papers examined the effect of community intervention or health promotion on the incidence of cardiovascular events or mortality; the duration of interventions ranged from 21.5 months to 15 years, and the studies targeted populations with hypertension, diabetes, impaired glucose intolerance, or obesity. Eight studies examined the cost-effectiveness of interventions for hypertension, diabetes, and obesity.
Table 1.
Studies Used to Answer Clinical Question 1
| Underlying disease |
Study design |
Study | n | Country | Intervention | Duration (years) |
Comparison | Population | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Hypertension | Comparative | Iso et al18 | 4,687 | Japan | Systematic blood pressure screening and health education |
5 | Full and minimal intervention | Hypertension patients |
In men, stroke incidence declined more (P<0.001) in the community that received the full-intensity program (42%, 53%, and 75% in the period 1970–1975, 1976–1981, and 1982–1987, respectively) than in the community that received the minimal-intensity program (5% increase, 20% decrease, and 29% decrease, respectively) |
| In women, the stroke incidence declined 45–65% in both communities for the 3 time periods | |||||||||
| Changes in stroke prevalence paralleled those in stroke incidence | |||||||||
| Obesity | Quasi-experimental | Hoshuyama et al19 |
21,626 | Japan | Health education program |
15 | Obese participants, non-participant comparative obese controls, and non-participant reference subjects |
Obesity patients |
Male participants showed significantly lower mortality risk for all-cause death (HR 0.54; 95% CI 0.31–0.94) and had a significantly different survival curve (P=0.014, log-rank test) compared with non-participant obese controls |
CI, confidence interval; HR, hazard ratio.
Table 4.
Studies Used to Answer Clinical Question 4
| Underlying disease |
Study design |
Study | n | Country | Intervention | Duration | Comparison | Population | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Hypertension | Comparative | Xie et al24 | – | China | To inform health policymakers and health care delivery |
– | Intensive and standard hypertension control |
Hypertension patients |
The incremental cost-effectiveness ratio for intensive hypertension control was estimated at US$1,240 per QALY compared with standard hypertension control |
| Intensive hypertension control is more cost-effective than standard hypertension control in China. The cost of adverse events was US$678–1,131 per QALY | |||||||||
| Hypertension | Comparative | Bai et al23 | 4,902 | China | Hypertension control program by face-to-face interview |
1 year | Before and after the program |
Hypertension patients |
The total cost of implementing the intervention was US$35,252, or US$7.17 per participant in 2009 |
| On average, SBP decreased from 143 to 131 mmHg (P<0.001) and DBP decreased from 84 to 78 mmHg (P<0.001). The SBP decreases ranged from 7.6 to 17.8 mmHg and DBP decreases ranged from 3.9 to 8.3 mmHg | |||||||||
| Cost-effectiveness ratios ranged from US$0.53 to US$0.73 per person per 1-mmHg SBP decrease, and from US$0.92 to US$1.42 per person per 1-mmHg DBP decrease | |||||||||
| Hypertension | Comparative | Lim et al25 | 85 | South Korea |
Customized community-based visiting health service |
8 weeks | Benefit estimations among 3 different benefit estimation models |
Blood pressure >140/90 mmHg |
Three models were examined: a standard deterministic estimation model, a repeated-measures deterministic estimation model, and a transitional probability estimation model. The estimated net benefit of the 3 different methods was US$1,273.01, −US$3,749.42, and −US$5,122.55, respectively |
| Diabetes | Propensity score matching |
Lian et al26 | 23,162 | China (Hong Kong) |
PEP | 5 years | PEP vs. non-PEP groups | Type 2 diabetes patients |
The PEP cost per subject was US$247 |
| There was a significantly lower cumulative incidence of all-cause mortality (2.9% vs. 4.6%; P<0.001), any diabetes complication (9.5% vs. 10.8%; P=0.001), and any cardiovascular event (6.8% vs. 7.6%; P=0.018) in the PEP group | |||||||||
| The cost per any-cause death, diabetes complication avoided, or cardiovascular event avoided was US$14,465, US$19,617, and US$30,796, respectively | |||||||||
| Diabetes | Comparative study |
Zhang et al29 | 1.94 million |
China | Multimedia health promotion campaign for diabetes |
4 years | Before and after the campaign |
Diabetes patients |
To cover 1,000 individuals, the program spent US$6.6 on the use of the Diabetes Risk Score flyer, 31.3¢ on an education booklet, US$9.4 on a newspaper campaign, and 37.5¢ on radio programs |
| Obesity | Comparative study |
Chung et al27 | 50 | China (Hong Kong) |
Face-to-face and teledietetics services |
24 weeks | Comparison of the groups |
50 adults aged 20–50 years with a BMI ≥23 kg/m2 |
At Week 6, the face-to-face group showed greater reductions in all variables than the teledietetics group. At Week 12, the effects reversed. At Week 24, the cumulative reductions in weight and body fat were significantly higher in the teledietetics than those face-to-face group (both P<0.0001) |
| The observed direct cost for 1% weight loss and 1% body fat loss was US$28.24 and US$17.09, respectively | |||||||||
| Obesity | Comparative study |
Joo et al28 | 925 | South Korea |
Visiting (V)-type program and a remote (R)-type program |
12 weeks | V- vs. R-type | Obese patients | The total cost for the intention-to-treat subjects was US$116,993 and US$24,555 in the V- and R-type programs, respectively |
| The average amount that the participants were willing to pay was US$71 and US$21 in the V- and R-type programs, respectively | |||||||||
| The cost-effectiveness of the V-type community-based short-duration obesity control program was higher than that of the R-type program |
BMI, body mass index; PEP, Patient Empowerment Program; QALY, quality-adjusted life-year.
Clinical Question 1
The first clinical question asked whether community intervention and health promotion programs for the prevention of hypertension, diabetes, obesity, or dyslipidemia reduce cardiovascular events and mortality in Japan. The literature search identified 2 community intervention studies conducted in Japan,18,19 1 examining hypertension and 1 examining obesity (Table 1).
Hypertension In 1998, Iso et al examined the effectiveness of a full- vs. minimal-intensity community program for the prevention of hypertension.18 In men, the incidence of stroke was decreased more (P<0.001) in the community that received the full-intensity program (42%, 53%, and 75% decreases in the period 1970–1975, 1976–1981, and 1982–1987, respectively) than in the community that received the minimal-intensity program (5% increase, 20% decrease, and 29% decrease in the period 1970–1975, 1976–1981, and 1982–1987, respectively). In women, the incidence of stroke was decreased by 45–65% in both intervention communities for the 3 time periods. Changes in stroke prevalence paralleled those in stroke incidence.18
Obesity In 2015, Hoshuyama et al examined the effect of a health education program (Brain-Oriented Obesity Control System [BOOCS]) to prevent mortality in obese individuals.19 The BOOCS program had 2 core principles:
• do not prohibit or order yourself as possible
• do something pleasant for yourself
and 3 basic rules:
• do not practice what you dislike, even if it is good for your health
• do not prohibit what you like, even if it is bad for your health
• do only what you like among good things and matters for your health.
A quasi-experimental 15-year follow-up study (1993–2007) was conducted with a total of 13,835 male and 7,791 female Japanese workers divided into 3 groups: obese participants in the BOOCS program (1,565 males, 742 females), non-participant comparative obese controls (1,230 males, 605 females), and non-participant reference subjects without obesity (11,012 males, 6,426 females). The male participants showed significantly lower risk of all-cause death (hazard ratio [HR] 0.54; 95% confidence interval [CI] 0.31–0.94) and had a significantly improved survival curve (P=0.014, log-rank test) compared with the non-participant obese controls.19
Clinical Question 2
The second clinical question asked whether community intervention and health promotion programs for the prevention of hypertension, diabetes, obesity, or dyslipidemia reduce cardiovascular events and mortality in East and Southeast Asian countries. The literature search identified 2 community intervention studies,20,21 1 conducted in Hong Kong and 1 conducted in China, both examining diabetes (Table 2).
Table 2.
Studies Used to Answer Clinical Question 2
| Underlying disease |
Study design |
Study | n | Country | Intervention | Duration | Comparison | Population | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Diabetes | Propensity score matching |
Wong et al20 | 795 | China (Hong Kong) |
PEP | 21.5 months | 352 PEP participants, 443 non-participants |
Chinese patients with type 2 diabetes and without previous CVD events |
After adjusting for confounding variables, PEP participants had a lower rate of all-cause mortality (HR 0.564; 95% CI 0.445–0.715; P<0.001), first cardiovascular event (HR 0.807; 95% CI 0.696–0.935; P=0.004), and stroke (HR 0.702; 95% CI 0.569–0.867; P=0.001) than non-participants |
| Diabetes | Cluster randomized trial |
Li et al21 | 577 | China | Lifestyle intervention groups (diet, exercise, or both) |
6 years (intervention), 20 years (follow-up) |
Randomized (1:1:1:1) to the control group or a lifestyle intervention group (diet, exercise, or both). |
Adults with impaired glucose tolerance |
Cumulative incidence of CVD-related mortality was 11.9% (95% CI 8.8–15.0) and 19.6% (95% CI 12.9–26.3) in the intervention and control groups, respectively (HR 0.59; 95% CI 0.36–0.96; P=0.033) |
| All-cause mortality was 28.1% (95% CI 23.9–32.4) and 38.4% (95% CI 30.3–46.5) in the intervention and control groups, respectively (HR 0.71; 95% CI 0.51–0.99; P=0.049) | |||||||||
| The incidence of diabetes was 72.6% (95% CI 68.4–76.8) vs. 89.9% (95% CI 84.9–94.9) in the intervention and control groups, respectively (HR 0.55; 95% CI 0.40–0.76; P=0.001) |
CVD, cardiovascular disease; PEP, Patient Empowerment Program. Other abbreviations as in Table 1.
Diabetes In Hong Kong, Wong et al reported that a patient empowerment program in a population-based cohort of patients with type 2 diabetes in the primary care setting was associated with a lower risk of first cardiovascular event and all-cause mortality.20 A cohort of 27,278 Chinese patients with type 2 diabetes and without a previous cardiovascular event on or before the baseline study recruitment date was assessed the Hong Kong administrative healthcare database from 2008 to 2013. The patient empowerment program was provided to the patients at primary care outpatient clinics through community-trained professional educators. During a median of 21.5 months of follow-up, 795 patients (352 program participants, 443 non-participants) experienced a first cardiovascular event. After adjustment for confounding variables, program participants had a lower rate of all-cause mortality (HR 0.564; 95% CI 0.445–0.715; P<0.001), first cardiovascular event (HR 0.807; 95% CI 0.696–0.935; P=0.004), and stroke (HR 0.702; 95% CI 0.569–0.867; P=0.001) compared with program non-participants.20
In China, Li et al examined the effect of lifestyle intervention on long-term outcomes in adults with impaired glucose tolerance who participated in the Da Qing Diabetes Prevention Study, which was a cluster randomized trial involving 33 clinics in Da Qing, China.21 In all, 577 adults with impaired glucose tolerance were randomized (1 : 1 : 1 : 1) to the control group or a lifestyle intervention group (diet, exercise, or both). The cumulative incidence of cardiovascular disease-related mortality was 11.9% (95% CI 8.8–15.0) in the intervention group compared with 19.6% (95% CI 12.9–26.3) in the control group (HR 0.59; 95% CI 0.36–0.96; P=0.033). All-cause mortality was 28.1% (95% CI 23.9–32.4) in the intervention group compared with 38.4% (95% CI 30.3–46.5) in the control group (HR 0.71; 95% CI 0.51–0.99; P=0.049).
Clinical Question 3
The third clinical question asked whether community intervention and health promotion programs for hypertension, diabetes, obesity, or dyslipidemia are cost-effective in Japan. The literature search identified a single report that investigated the cost-effectiveness of a community intervention and health promotion program for hypertension in Japan (Table 3).
Table 3.
Study Used to Answer Clinical Question 3
| Underlying disease |
Study design |
Study | n | Country | Intervention | Duration (months) |
Comparison | Population | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Hypertension | Comparative | Yamagishi et al22 |
193 | Japan | Counseling guidance program |
9 | Full-intervention vs. minimal- intervention communities |
Hypertension patients in Akita Prefecture, Japan |
The prevalence and incidence of stroke were consistently lower in the full- than minimal- intervention community throughout the same time period |
| The incremental cost was −JPY28,358 per capita over 24 years | |||||||||
| Budget impact: cost of public health services per capita, 4,741 JPY/year; cost of hypertension treatment per capita, −7,126 JPY/year; cost of stroke treatment per capita, −2,500 JPY/year; total cost per capita, −4,884 JPY/year |
Hypertension In Japan, Yamagishi et al reported a hypertension detection and control program, initiated in 1963 in Akita Prefecture, that examined communities provided with a full or minimal intervention.22 The full-intervention program was found to be cost-saving at 13 years after the start of the program and to be more effective at decreasing the prevalence and incidence of stroke than the minimal-intervention program over the same time period. The incremental cost was −JPY28,358 per capita over 24 years.22 The national government support of this program may have contributed, in part, to the substantial decline in stroke incidence and mortality that was largely responsible for the increase in Japanese life expectancy.
Clinical Question 4
The fourth clinical question asked whether community intervention and health promotion programs for hypertension, diabetes, obesity, or dyslipidemia are cost-effective in East and Southeast Asian countries. The literature search identified 7 studies (3 from China, 2 from Hong Kong, and 2 from South Korea) that examined the cost-effectiveness of community intervention and health promotion programs for the prevention of hypertension, diabetes mellitus, and obesity (Table 4).23–29
Hypertension Bai et al reported on the cost-effectiveness of a hypertension control program implemented in China.23 In that study, information was collected on program costs and health outcomes in 3 community health centers over a 1-year period. The participants were 4,902 people aged ≥18 years with hypertension (systolic blood pressure [SBP] ≥140 mmHg and/or diastolic blood pressure [DBP] ≥90 mmHg, or on antihypertensive medication). SBP and DBP changes in the populations were estimated through face-to-face interviews and physical examinations of a random sample of 818 participants. The total cost of implementing the intervention in 2009 was US$35,252, or US$7.2 per participant. On average, SBP decreased from 143 to 131 mmHg (P<0.001) and DBP decreased from 84 to 78 mmHg (P<0.001); the SBP decreases ranged from 7.6 to 17.8 mmHg and the DBP decreases ranged from 3.9 to 8.3 mmHg. Cost-effectiveness ratios ranged from US$0.53 to US$0.73 per person per 1-mmHg SBP decrease, and from US$0.92 to US$1.42 per person per 1-mmHg DBP decrease. Per capita costs varied widely across the communities, as did changes in SBP and DBP, but cost-effectiveness was comparable.23
Xie et al reported that intensive hypertension control to inform health policymakers and healthcare delivery systems would prevent 2.2 million coronary heart disease events and 4.4 million stroke events in Chinese hypertensive patients in 10 years compared with standard hypertension control.24 The incremental cost-effectiveness ratio for intensive hypertension control was estimated at US$1,219 per quality-adjusted life-year compared with standard hypertension control. This study showed that intensive hypertension control is more cost-effective than standard hypertension control in China.24
Lim et al reported data from community-based hypertension management programs implemented by the nursing service in South Korea.25 Three benefit estimation models were compared: a standard deterministic estimation model; a repeated-measures deterministic estimation model; and a transitional probability estimation model. The estimated net benefit using these 3 different models was −US$1,273.01, −US$3,749.42, and −US$5,122.55, respectively. The transitional probability estimation model showed the most realistic benefit estimation, because it traced possible paths of changing status between time points and it accounted for both positive and negative benefits.25
Diabetes and Obesity Lian et al reported that the cost per subject of a patient empowerment program for type 2 diabetes was US$247 during a 5-year period in a risk assessment and management program conducted in Hong Kong.26 There was a significantly lower cumulative incidence of all-cause mortality (2.9% vs. 4.6%; P<0.001), any diabetes complication (9.5% vs. 10.8%; P=0.001), and any cardiovascular event (6.8% vs. 7.6%; P=0.018) in the program participants versus controls. The cost per any-cause death, diabetes complication, or cardiovascular event avoided was US$14,465, US$19,617, and US$30,796, respectively.26
Chung et al evaluated the effectiveness of teledietetics on weight loss for 24 weeks and the cost-effectiveness of weight loss achieved through face-to-face and teledietetics services.27 That study was conducted at a community health center and a community dietetics clinic in Hong Kong and had a quasi-experimental design. The face-to-face group received 12 dietary counseling sessions and recorded their diet in a log book. The teledietetics group attended 3 group nutrition seminars and recorded their diet on a web-based platform. Direct and indirect costs were used to compute cost-effectiveness ratios. At Week 6, the face-to-face group showed greater reductions in all variables compared with the teledietetics group. At Week 12, the effects reversed. At Week 24, the cumulative reductions in weight and body fat in the teledietetics group were significantly higher than in the face-to-face group (both P<0.0001). The observed direct cost for 1% weight loss and 1% body fat loss was US$28.24 and US$17.09, respectively.27 These findings suggest that the teledietetics model was more cost-effective for weight reduction than the face-to-face dietetics model.
Joo et al evaluated two 12-week community-based obesity control programs in South Korea;28 one was a visiting-type program (V-type; n=515) administered by a public health center and the other was a remote-type program (R-type; n=410) using a website and a mobile phone-based short message service. The total cost for the intention-to-treat subjects was US$116,993 and US$24,555 in the V- and R-type programs, respectively. In the per-protocol subjects, 66% of V-type program participants (n=117) and 13% of R-type program participants (n=15) achieved the target bodyweight reduction (5%), and the cost per person was US$227 (V-type) and US$60 (R-type). The cost per person achieving the target weight reduction was US$975 (V-type) and US$1,637 (R-type). The average amount that the participants were willing to pay was US$71 (V-type) and US$21 (R-type). The cost-effectiveness of the V-type community-based short-duration obesity control program was higher than that of the R-type program.28
Discussion
In this systematic review we found that community intervention and health promotion programs for the control of NCDs are a cost-effective means of reducing the incidence of cardiovascular events and mortality in Japan and other East Asian countries. However, direct evidence of the effects and cost-effectiveness of these programs for reducing the incidence of cardiovascular events and mortality in Japan or East and Southeast Asian countries remains limited. Furthermore, in the present study we were unable to identify any appropriate studies from Southeast Asia, and no studies from any of the study countries examined the efficacy and cost-effectiveness of community intervention and health promotion programs for the prevention or control of dyslipidemia.
Prevention of Stroke and Cardiovascular Disease
Hypertension is a major global public health issue in the 21st century. In Health Japan 21, a 10-year plan for the promotion of national health established by the government of Japan, extension of the national healthy life span is the most important indicator for health and longevity.30
However, many of the studies included in the present review compared only target data with data collected within a 1-year follow-up period. In the Japanese data, a community-based hypertension control program augmented the decline in stroke incidence and prevalence only among men.18 The effect of the program may differ between the sexes. That study attributed the success of that community program to active participation of existing health resources in the detection and control of hypertension and to consistently high participation in blood pressure screenings, follow-up examinations, and community-wide health education activities.18
In patients with obesity, the data of BOOCS program19 coincide with previous reports31–33 in that both all-cause and cancer mortality were associated with obesity. There may have been a so-called “legacy effect” in that study because only the participant group showed mortality benefit after better body mass index control disappeared. These effects brought about by the BOOCS program may have resulted in a protective effect against mortality in that study. Further investigations are needed to examine the reduction in cardiovascular events or mortality by long-term community service intervention.
Cost-Effectiveness of Measures for NCDs
Long-term follow-up is necessary to confirm whether reported improvements in clinical outcomes can be translated into actual reductions in cardiovascular complications and mortality and whether certain approaches are cost-effective. Although the details of the interventions varied significantly, most studies examined here concluded that educational interventions were cost-effective or cost saving. However, careful interpretation is needed regarding the relationship between per capita costs and program effectiveness, differences in intervention levels, and differences in health status. In the US, 2 randomized controlled studies have suggested that lifestyle education for hypertension is cost-effective, depending on the willingness-to-pay threshold.34,35 Accumulation of such cost-effectiveness data in the Asian context will be helpful for policy makers when making resource allocation decisions. Even in Japan, we could not find a relatively recent or current study that showed the cost-effectiveness of health promotion for NCDs. To prevent chronic diseases, health policy should aim not only to improve individual health behaviors in the population, but also to reduce socioeconomic inequality. Our study suggests promoting a healthy lifestyle even in disadvantaged socioeconomic classes as a strategy to improve the health conditions of the whole population.
Future Health Interventions
Various novel health interventions for NCDs are currently being considered in East Asia. For example, eHealth interventions have been shown to improve blood pressure control and are therefore a promising approach for the management of hypertension.36 However, the effectiveness of eHealth approaches to induce self-care behavioral change and psychosocial well-being is insufficient.37 Therefore, rigorously designed studies examining the effects of eHealth interventions on self-care in hypertension patients are needed to provide robust evidence and to address the increasing healthcare needs of patients with hypertension.
This epidemiological burden, coupled with population aging, presents an exceptionally serious sustainability challenge, even among the richest countries that are members of the Organization for Economic Co-operation and Development (OECD). Strategic and political leadership of the WHO and multilateral agencies would likely play essential roles in the struggle that has just begun.
Study Limitations
Several limitations of this review should be addressed. Our literature search provided only small RCTs with which we could answer our clinical questions. In addition, the lack of a unified definition of the thresholds of blood pressure, blood glucose level, and body weight to define target populations and control targets may have resulted in heterogeneity among the studies examined. These limitations should be taken into account when interpreting the studies we present. In addition, in this review we did not search for grey literature, nor did we examine healthcare resource utilization. Finally, because there is little information available regarding how community intervention and health promotion programs are actually applied in the real world, it remains unknown as to what kind of intervention is best. Taken together, the findings of this review reveal the urgent need for Asian countries to develop further evidence-based policies and programs and to encourage greater interdisciplinary research for the prevention and management of NCDs.
Conclusions
Here, through a systematic literature review, we provide an overview of the community intervention and health promotion programs implemented in Japan and other East Asian countries in the past 3 decades for the prevention of stroke and cardiovascular disease or for the control of other NCDs. Through this review, we hope to share the East Asian experience with other countries currently tackling or expecting to tackle sharp increases in the incidence of NCDs. The challenge to prevent NCDs includes the implementation of multisectoral approaches, the setting of clear goals and targets, the establishment of effective monitoring and evaluation mechanisms, adequately addressing social problems, adjusting previous findings to the local context, and foreseeing future demographic transitions. Japan is committed to contributing to the world as a forerunner experiencing the health care-related challenges posed by unprecedented demographic change, and to sharing its lessons as part of the global quest to create a world where everyone can live a longer and healthier life.2
Community intervention and health promotion programs seem to be cost-effective approaches for reducing the incidence of stroke, cardiovascular events, and mortality in Japan and other East Asian countries. However, none of the studies included in the present study examined the efficacy and cost-effectiveness of such programs for the control of dyslipidemia. One of the likely reasons for this is that within healthcare systems, the treatment of dyslipidemia is generally not a priority with respect to the prevention of cardiovascular disease, as compared with hypertension, diabetes, and obesity. However, treatment of dyslipidemia may help reduce the number of preventable deaths. Thus, efforts to prevent cardiovascular disease should focus on the development of evidence-based public policies and improving asset allocations. In addition, none of the articles included in this study were from institutes located in Southeast Asia. Further investigations are needed to address this lack of knowledge.
Sources of Funding
This work was funded by the World Health Organization (WHO) Center for Health Development (Kobe, Japan; part of WHO’s Global Health Systems and Innovation Cluster in Geneva).
Disclosures
The Department of Geriatric Medicine, National Center for Geriatrics and Gerontology receives research promotion grants. The authors declare that they have no conflicts of interest.
Supplementary Files
Supplementary Table 1. Supplementary Table 2. Supplementary Table 3
Acknowledgment
The authors express their sincere appreciation to Toshiyuki Swa for his important contributions to the literature searches conducted in this study.
Data Availability
All data relevant to the study are included in the article or uploaded as supplementary information.
References
- 1. Hunter DJ, Reddy KS.. Noncommunicable diseases. N Engl J Med 2013; 369: 1336–1343. [DOI] [PubMed] [Google Scholar]
- 2. Ezoe S, Noda H, Akahane N, Sato O, Hama T, Miyata T, et al.. Trends in policy on the prevention and control of non-communicable diseases in Japan. Health Syst 2017; 3: 268–277. [DOI] [PubMed] [Google Scholar]
- 3. Chen S, Kuhn M, Prettner K, Bloom DE.. The macroeconomic burden of noncommunicable diseases in the United States: Estimates and projections. PLoS One 2018; 13: e0206702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Ali MK, Jaacks LM, Kowalski AJ, Siegel KR, Ezzati M.. Noncommunicable diseases: Three decades of global data show a mixture of increases and decreases in mortality rates. Health Aff (Millwood) 2015; 34: 1444–1455. [DOI] [PubMed] [Google Scholar]
- 5. World Health Organization.. Global action plan for the prevention and control of NCDs 2013–2020. 2013. https://www.who.int/publications/i/item/9789241506236 (accessed April 21, 2021).
- 6. World Health Assembly.. Follow-up to the political declaration of the high-level meeting of the general assembly on the prevention and control of non-communicable diseases WHA6610. Sixty-sixth World Health Assembly. 2013. https://apps.who.int/gb/ebwha/pdf_files/WHA66/A66_R10-en.pdf?ua=1 (accessed April 21, 2021).
- 7. World Health Organization.. Noncommunicable diseases country profiles. 2014. http://www.who.int/nmh/publicatons/ncd-profiles-2014/en/ (accessed April 21, 2021).
- 8. Bono F, Matranga D.. Socioeconomic inequality in non-communicable diseases in Europe between 2004 and 2015: Evidence from the SHARE survey. Eur J Public Health 2019; 29: 105–110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Bauer UE, Briss PA, Goodman RA, Bowman BA.. Prevention of chronic disease in the 21st century: Elimination of the leading preventable causes of premature death and disability in the USA. Lancet 2014; 384: 45–52. [DOI] [PubMed] [Google Scholar]
- 10. Stephani V, Opoku D, Quentin W.. A systematic review of randomized controlled trials of mHealth interventions against non-communicable diseases in developing countries. BMC Public Health 2016; 16: 572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. GBD 2013 DALYs and HALE Collaborators; Murray CJL, Barber RM, Foreman KJ, Abbasoglu Ozgoren A, Abd-Allah F, Abera SF, et al.. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: Quantifying the epidemiological transition. Lancet 2015; 386: 2145–2191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Ikeda N, Inoue M, Iso H, Ikeda S, Satoh T, Noda M, et al.. Adult mortality attributable to preventable risk factors for non-communicable diseases and injuries in Japan: A comparative risk assessment. PLoS Med 2012; 9: e1001160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Ministry of Health, Labour and Welfare, Statistics and Information Department.. Estimates of national medical care expenditure 2014 [in Japanese]. 2016. http://www.mhlw.go.jp/toukei/saikin/hw/k-iryohi/14/dl/kekka.pdf (accessed March 21, 2017).
- 14. Kaneko H, Morita H, Komuro I.. Beautiful harmony of the Japanese precious healthcare legacies for the new imperial era. Circ J 2020; 84: 371–373. [DOI] [PubMed] [Google Scholar]
- 15. The Government of Japan.. Regional workshop on leadership and advocacy for the prevention and control of noncommunicable diseases. Manila: World Health Organization Western Pacific Region, 2020; 1–8.
- 16. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al.. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011; 343: d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Moher D, Liberati A, Tetzlaff J, Altman DG.. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J Clin Epidemiol 2009; 62: 1006–1012. [DOI] [PubMed] [Google Scholar]
- 18. Iso H, Shimamoto T, Naito Y, Sato S, Kitamura A, Iida M, et al.. Effects of a long-term hypertension control program on stroke incidence and prevalence in a rural community in northeastern Japan. Stroke 1998; 29: 1510–1518. [DOI] [PubMed] [Google Scholar]
- 19. Hoshuyama T, Odashiro K, Fukata M, Maruyama T, Saito K, Wakana C, et al.. Mortality benefit of participation in BOOCS program: A follow-up study for 15 years in a Japanese working population. J Occup Environ Med 2015; 57: 246–250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Wong CKH, Wong WCW, Wan YF, Chan AKC, Chung KL, Chan FWK, et al.. Patient Empowerment Programme in primary care reduced all-cause mortality and cardiovascular diseases in patients with type 2 diabetes mellitus: A population-based propensity-matched cohort study. Diabetes Obes Metab 2015; 17: 128–135. [DOI] [PubMed] [Google Scholar]
- 21. Li G, Zhang P, Wang J, An Y, Gong Q, Gregg EW, et al.. Cardiovascular mortality, all-cause mortality, and diabetes incidence after lifestyle intervention for people with impaired glucose tolerance in the Da Qing Diabetes Prevention Study: A 23-year follow-up study. Lancet Diabetes Endocrinol 2014; 2: 474–480. [DOI] [PubMed] [Google Scholar]
- 22. Yamagishi K, Sato S, Kitamura A, Kiyama M, Okada T, Tanigawa T, et al.. Cost-effectiveness and budget impact analyses of a long-term hypertension detection and control program for stroke prevention. J Hypertens 2012; 30: 1874–1879. [DOI] [PubMed] [Google Scholar]
- 23. Bai Y, Zhao Y, Wang G, Wang H, Liu K, Zhao W.. Cost-effectiveness of a hypertension control intervention in three community health centers in China. J Prim Care Community Health 2013; 4: 195–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Xie X, He T, Kang J, Siscovick DS, Li Y, Pagan JA.. Cost-effectiveness analysis of intensive hypertension control in China. Prev Med 2018; 111: 110–114. [DOI] [PubMed] [Google Scholar]
- 25. Lim JY, Kim MJ, Park CG, Kim JY.. Comparison of benefit estimation models in cost-benefit analysis: A case of chronic hypertension management programs. J Korean Acad Nurs 2011; 41: 750–757. [DOI] [PubMed] [Google Scholar]
- 26. Lian J, McGhee SM, So C, Chau J, Wong CKH, Wong WCW, et al.. Five-year cost-effectiveness of the Patient Empowerment Programme (PEP) for type 2 diabetes mellitus in primary care. Diabetes Obes Metab 2017; 19: 1312–1316. [DOI] [PubMed] [Google Scholar]
- 27. Chung LMY, Law QPS, Fong SSM, Chung JWY, Yuen PP.. A cost-effectiveness analysis of teledietetics in short-, intermediate-, and long-term weight reduction. J Telemed Telecare 2015; 21: 268–275. [DOI] [PubMed] [Google Scholar]
- 28. Joo NS, Park YW, Park KH, Kim CW, Kim BT.. Cost-effectiveness of a community-based obesity control programme. J Telemed Telecare 2010; 16: 63–67. [DOI] [PubMed] [Google Scholar]
- 29. Zhang YL, Gao WG, Pang ZC, Sun JP, Wang SJ, Ning F, et al.. Diabetes self-risk assessment questionnaires coupled with a multimedia health promotion campaign are cheap and effective tools to increase public awareness of diabetes in a large Chinese population. Diabet Med 2012; 29: e425–e429. [DOI] [PubMed] [Google Scholar]
- 30. National Institutes of Biomedical Innovation, Health and Nutrition.. Health Japan 21 (the second term). https://www.nibiohn.go.jp/eiken/kenkounippon21/en/kenkounippon21/mokuhyou.html#Table02 (accessed March 19, 2022).
- 31. Ford ES.. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: A summary of the evidence. Diabetes Care 2005; 28: 1769–1778. [DOI] [PubMed] [Google Scholar]
- 32. Hung CS, Lin JW, Hwang JJ, Tsai RY, Li AT.. Using paper chart based clinical reminders to improve guideline adherence to lipid management. J Eval Clin Pract 2008; 14: 861–866. [DOI] [PubMed] [Google Scholar]
- 33. Itoh H, Kaneko H, Kiriyama H, Kamon T, Fujiu K, Morita K, et al.. Metabolically healthy obesity and the risk of cardiovascular disease in the general population: Analysis of a nationwide epidemiological database. Circ J 2021; 85: 914–920. [DOI] [PubMed] [Google Scholar]
- 34. Datta SK, Oddone EZ, Olsen MK, Orr M, McCant F, Gentry P, et al.. Economic analysis of a tailored behavioral intervention to improve blood pressure control for primary care patients. Am Heart J 2010; 160: 257–263. [DOI] [PubMed] [Google Scholar]
- 35. Troyer JL, McAuley WJ, McCutcheon ME.. Cost-effectiveness of medical nutrition therapy and therapeutically designed meals for older adults with cardiovascular disease. J Am Diet Assoc 2010; 110: 1840–1851. [DOI] [PubMed] [Google Scholar]
- 36. Jung H, Lee JE.. The impact of community-based eHealth self-management intervention among elderly living alone with hypertension. J Telemed Telecare 2017; 23: 167–173. [DOI] [PubMed] [Google Scholar]
- 37. Ma Y, Cheng HY, Cheng L, Sit JWH.. The effectiveness of electronic health interventions on blood pressure control, self-care behavioural outcomes and psychosocial well-being in patients with hypertension: A systematic review and meta-analysis. Int J Nurs Stud 2019; 92: 27–46. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Table 1. Supplementary Table 2. Supplementary Table 3
Data Availability Statement
All data relevant to the study are included in the article or uploaded as supplementary information.