

Abstract
Objective:
To evaluate volumetric variations in the palate following rapid expansion, both immediately after treatment and over time.
Materials and Methods:
The sample was composed of 30 patients in early mixed dentition treated with a Haas-type device cemented onto the primary second molars. The mean age of the patients upon commencement of expansion was 7 years and 6 months (standard deviation [SD], 12 months). Measurement of palatal volume was conducted via 3D acquisition of plaster models using laser scanning before treatment (T1), upon device removal (T2), and 2.6 years afterward (T3).
Results:
The volume of the palate increased in a statistically significant fashion from T1 to T2 and from T1 to T3, and it decreased in a nonsignificant fashion from T2 to T3.
Conclusions:
Palatal volume significantly increases with rapid maxillary expansion (RME) treatment with insignificant relapse. The use of virtual 3D models with the aid of Apposite software permits evaluation of the morphologic and volumetric changes induced by orthodontic treatment.
Keywords: Volume, Palate, RME, Laser
INTRODUCTION
Rapid maxillary expansion (RME) is a universally employed technique for correction of transversal deficits of the upper arch in adolescent patients. Various studies have evaluated the dental and skeletal effects of RME using different techniques from manual measurements and plaster models1–3 to laterolateral,4–7 posteroanterior,2,3,5,7,8 and occlusal1,9 radiography; nonetheless, the measurements carried out in these studies all relied on 2-dimensional (2D) analytical methods.
Nowadays the availability of 3-dimensional (3D) imaging systems permits clinicians and researchers to evaluate changes in orthodontic treatment in three spatial dimensions. Garib et al10 compared the dentoskeletal effects of Hyrax- and Haas-type expanders, using spiral computed tomography (CT), and Garret11 employed cone-bean computed tomography (CBCT) to study the effects of RME on the upper jaw.
Phatouros12 investigated morphologic changes in the palate after RME, using 3D images obtained via CT scanning of plaster models, and Oliveira13 compared the results obtained with Haas- and Hyrax-type expanders using a 3D method involving laser scanning and computer analysis of plaster models; in addition, anteroposterior cephalograms were obtained.
Marini and Bonetti14 used photogrammetry to study 3D palatal changes following RME. This technique permits the dimensions and morphology of 3D changes to be measured using photographs of the object as a starting point.
De Felippe et al15 evaluated the effects of RME by calculating the variations it induced on interdental diameters, molar tipping, and palatal area and volume, using 3D digital images obtained via laser scanning of plaster models.
The aim of our study was to evaluate volumetric variations in the palate, both immediately subsequent to RME and over time, in patients in early mixed dentition, using the 3D acquisition technique of laser scanning plaster models. We investigated volumetric alterations in the palate following the active phase of expansion and stability over time of the results achieved.
MATERIALS AND METHODS
The sample analyzed consisted of 30 patients (18 females and 12 males) in early mixed dentition treated with a Haas-type device cemented onto the E teeth. The mean age of the patients, treated by the same operator, at the start of expansion was 7 years and 5 months (standard deviation [SD], 12 months). All patients had good-quality upper E teeth without caries and well-formed roots as shown by panoramic radiograph. This project was approved by the Department Committee at the University of Ferrara, and informed consent was obtained from parents.
In all cases, activation of the device was carried out by a single turn of its screws per day until the palatal cusp of the upper first molar came into contact with the buccal cusp of the lower first molar. Upon completion of the expansion phase, the device was used to maintain the expanded jaw for a period of 12 months (SD, 3 months) before it was removed.
Impressions of the maxillary arch were taken at three different intervals during the course of expansion: at the start of treatment, T1; upon removal of the device (mean, 12 months; SD, ±3), T2; and after an observation period, before the second phase of orthodontic treatment with a fixed appliance, T3 (mean, 2.6 years; SD, ±1.1). All impressions were taken in vinyl polysiloxane (2 Penta H, 2 Light Body; 3M ESPE Express, Leicestershire, UK) using the double-impression technique, and then were cast in class 4 extra-hard white plaster (ZETA, Orthodontic Stone; WhipMix Corp, Louisville, Ky) within 24 hours.
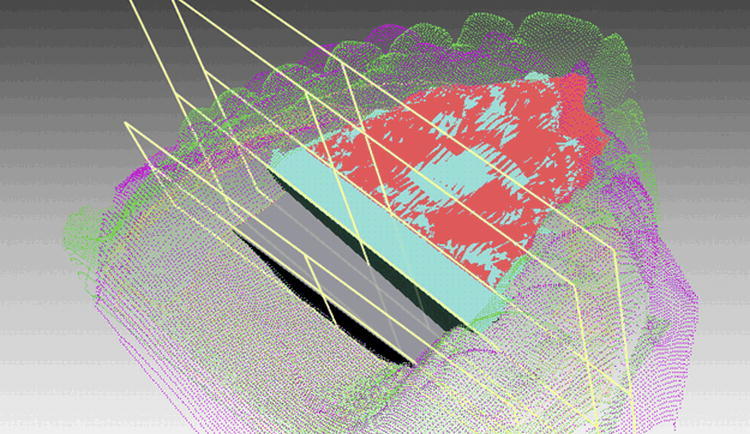
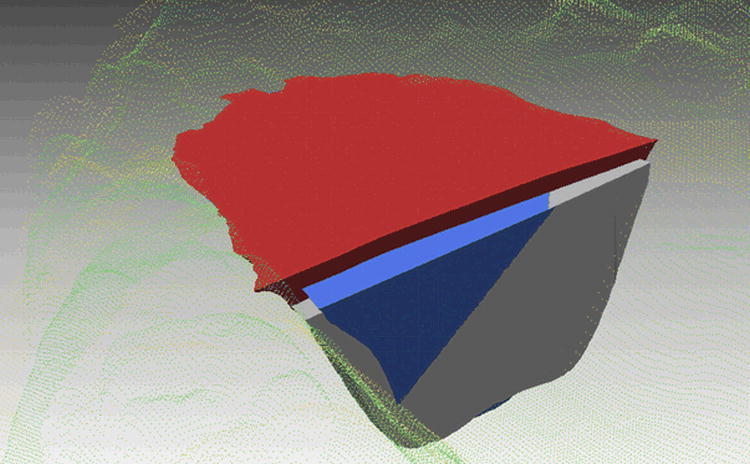
The plaster models obtained then were subjected to piezoelectric scanning (Roland Active Piezo Sensor Modela MDX-15; Roland DG Mid Europe SRL, Acquaviva Picena, Italy) (Figure 1). This scan processing system, together with Apposite software (RapidForm 2006; INUS Technology, Seoul, Korea) permits the following: (1) accurate 3D reconstruction of the model to be obtained16; (2) precise measurements; and (3) the volume of the scanned object to be evaluated. Once the 3D models had been obtained, the planes to “pack” the model were defined so the volume of the palate could be calculated. The horizontal plane was obtained by uniting the following three points: one at the lowest point of the gingival margin of one central incisor and two at the lowest points of the gingival margin of the first permanent molars (Figure 2). The posterior limiting plane was tangent to the distal surface of the first molars and necessarily formed an angle of 90 degrees with the horizontal plane (Figure 3). Once the planes had been defined, it was necessary to remove the unnecessary points (ie, those corresponding to the teeth above the horizontal plane and the “heel” of the model) from the mesh so the volume could be obtained (Figure 4).
Figure 1.
“Roland Picza mdx-15/20” Model
Figure 2.
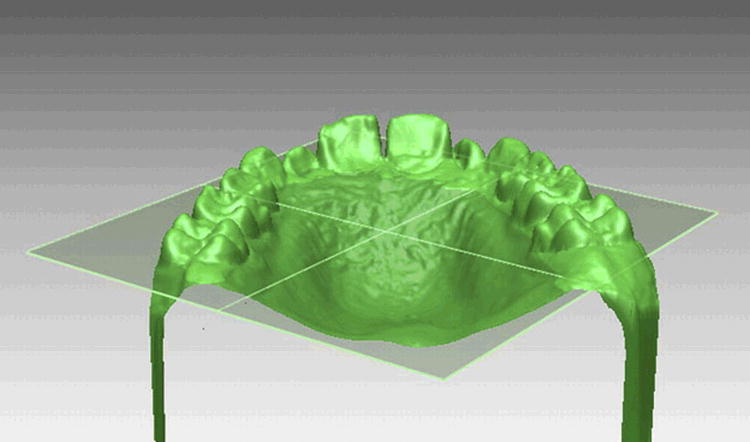
View of horizontal plane
Figure 3.
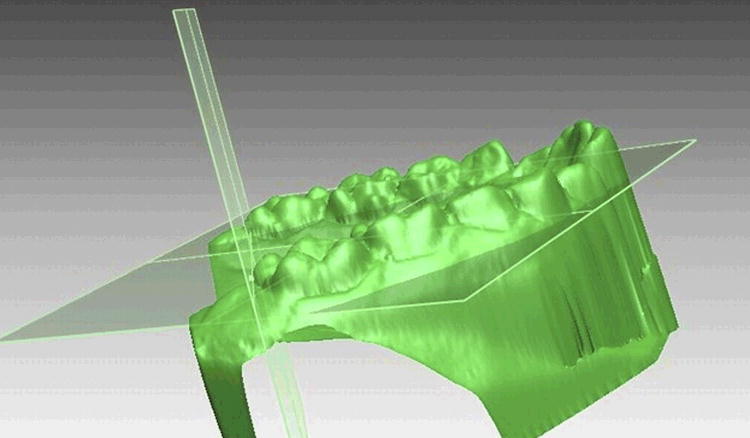
Intersection between horizontal and vertical planes
Figure 4.
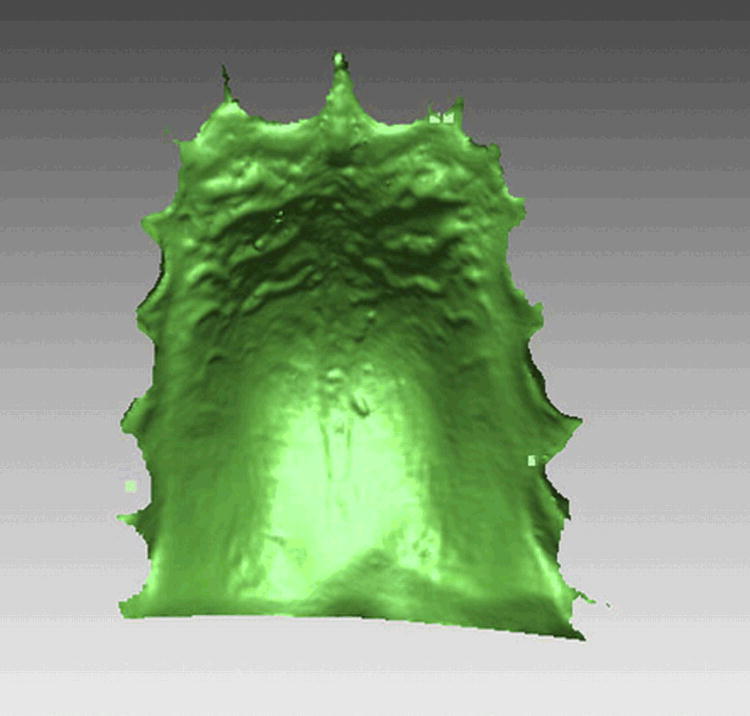
Mesh after cleaning
Volumes desired were obtained by closing the various planes. Palatal volume was defined as the volume between the reference surfaces and the palatal surface. This volume was visualized as a solid (Figure 5), and a data table that included this value was drafted (Figure 6).
Figure 5.
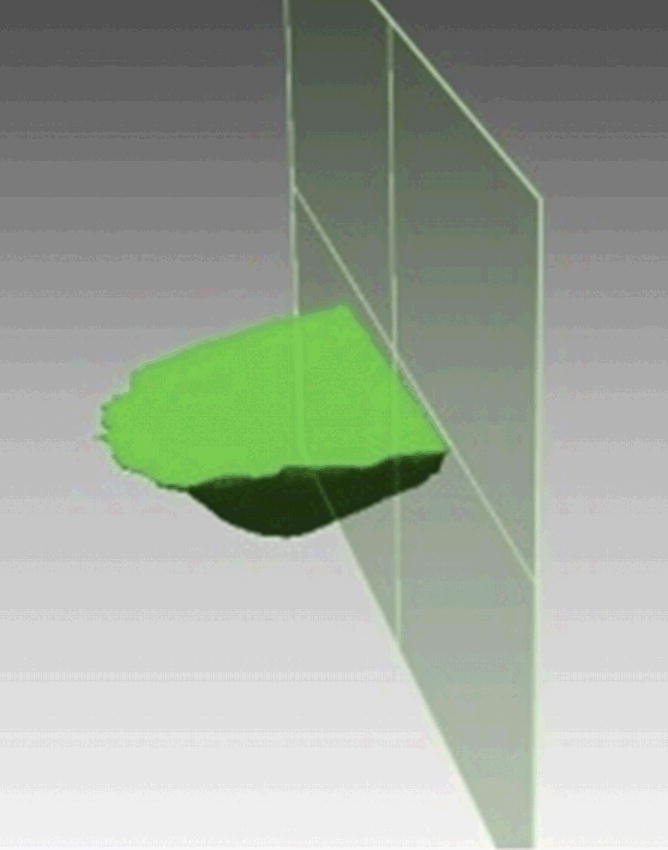
Volume of palate visualized as a solid
Figure 6.
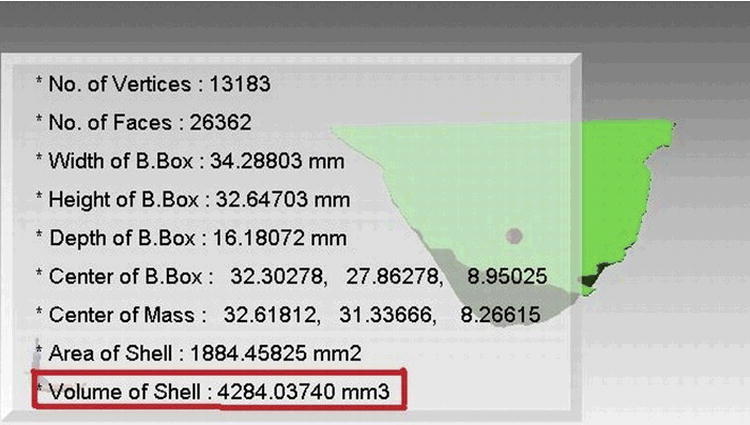
Measurements table
We decided to identify stable reference points on the sagittal and transverse planes to consent to superimposition of the digital models and thus to visual evaluation of the volumetric variations provoked by expansion therapy. We decided to use the palatine rugae as an anatomic reference zone for this purpose (Figures 7a,b,c, and Figure 8), as these rugae are stable in both anteroposterior and transversal directions and are easy to recognize.
Figure 7.
(A) Volume at T1. (B) Volume at T2. (C) Volume at T3
Figure 8.
Superimpositions T1, T2, and T3
In 1955, Lysell17 affirmed that the palatine rugae have unique characteristics and may be used for identification purposes. Peavy and Kendricks18 also concluded their study by stating that the palatine rugae do not undergo appreciable alteration during orthodontic treatment. Almeida19 highlighted that the palatine rugae are suitable anatomic sites for reference points in longitudinal analysis of the transversal and anteroposterior planes of models. Bailey20 evaluated the stability of the palatine rugae in extractive and nonextractive orthodontic treatment. Data obtained indicate that the palatine rugae did not undergo modification in patients without treatment, but statistically significant variations in the positions of the first and second rugae were found in the extraction cases. However, the author concludes that the median and lateral points of the third palatine ruga are stable enough to use as reference points when evaluating dental movements. Hoggan and Sadowsky21 evidenced the stability of the palatine rugae in a sample treated with extraction of the first upper premolars.
The studies cited above evaluated and confirmed palatine rugae stability in the sagittal and transverse planes. Recently, however, an article has been published22 regarding their stability in the vertical plane. The results of this study demonstrate that the vertical position of the palatine rugae changes, with the degree of alteration being greater in the first rugae than in the second and least in the third. The authors conclude that the third palatine ruga is thus the most reliable for use as a reference point in the short term.
Statistical Analysis
Palatal volumes are expressed as means ± SD. To compare the mean measurement of the same parameter at three different time intervals, an F analysis of variance (ANOVA) test for repeated measurements was employed. To apply this test, the validity premises (ie, normal distribution of data in each step) were verified, correlations were noted between means and SDs for each step, as were homoschedasticity and sphericity of the measurements. The Bonferroni test was used for post hoc verification.
RESULTS
Volumetric measurement of the palate was carried out for each patient at T1, T2, and T3, and the measurements obtained are reported in Table 1, where the volume is expressed in mm3.
Table 1. .
Palatal Volume of Each Patient Expressed in mm3 at T1, T2, and T3
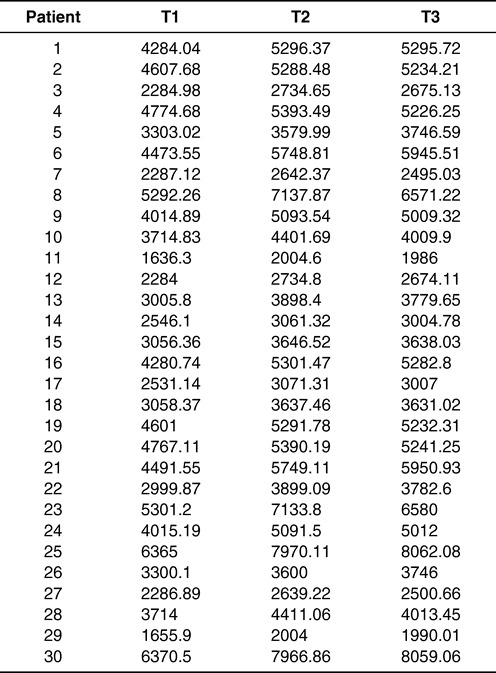
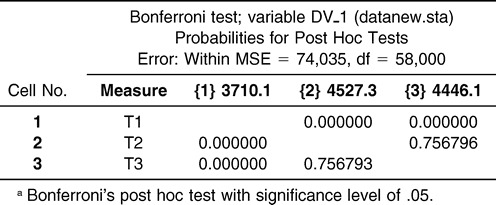
Before treatment (T1), the mean palatal volume was 3710.1 mm3, upon removal of the expander (T2) it was 4527.3 mm3, and upon long-term re-examination (T3) it was 4446.1 mm3 (Tables 2 and 3). Between T1 and T2, a statistically significant increase in volume (P < .00000001) of 21% was revealed, whereas the reduction in volume between T2 and T3 (P = .76) of 2% was not found to be significant; thus the increase in volume between T1 and T3 (0.00000001) of 19% was statistically significant (Table 4).
Table 2. .
Descriptive Statistics

Table 3. .
Graph Representing Changes in Sample Means at T1, T2, and T3a
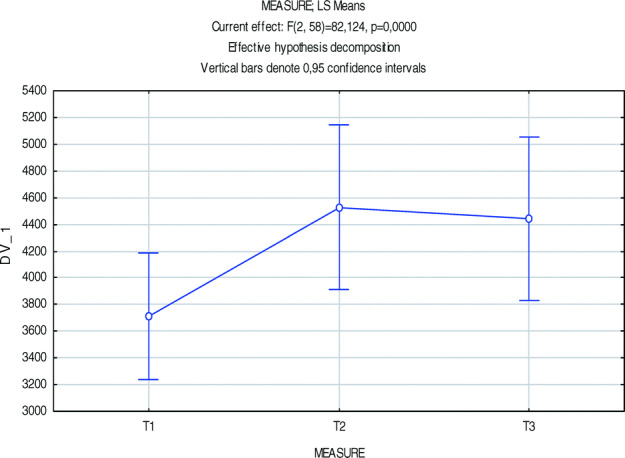
Table 4. .
Statistical Differencesa
DISCUSSION
Various studies have evaluated the skeletal and dental effects induced by rapid palatal expansion using two-dimensional analysis.1–9 New 3D-imaging techniques, however, permit clinicians and researchers to evaluate changes in three-dimensional space.
Garib et al10 compared the dentoskeletal effects of Hyrax- and Hass-type devices using CT. The limitation of this study was the small size of the sample (8 subjects). Garrett et al11 evaluated the skeletal effects of rapid expansion via CBCT, which permits 3D imaging with minimal distortion and exposure to low levels of radiation.23 Oliveira et al13 evaluated morphologic changes in the upper jaw after palatal expansion using a 3D method; the technique employed, laser scanning and subsequent computerized analysis of models, was found to be accurate, fast, and relatively inexpensive. In this study, only linear measurements were considered.
Volumetric evaluation was carried out by De Felippe et al,15 who obtained digital models via scanning of plaster casts. In this study, measurement of the palatal area was executed before expansion (T1), upon removal of the expander (T3), and between 9 and 12 months after the expander was taken out (T4). Their results demonstrate a statistically significant increase in volume between T1 and T3, and between T1 and T4, and an insignificant relapse between T3 and T4.
Phatouros and Goonewardene12 scanned plaster models using CT. Linear measurement of their digital models produced results comparable with those carried out by using a gauge to measure plaster models. This study did not seek to evaluate volumetric alterations of the palate, although the authors did emphasize the importance of such an investigation, stating that 3D imaging techniques such as laser or CT scanning could be used to obtain further information about changes to the volume of the palate during rapid expansion.
Marini and Bonetti14 used photogrammetry to calculate the degree of volumetric change in the palate after rapid expansion. These authors determined that all patients showed an increase in palatal volume and transverse diameter after rapid expansion, despite a slight relapse during the 6 months following treatment. The technique employed in this study, despite the fact that it is very precise in terms of linear measurement of transverse diameters, was slightly less meticulous as far as volumetric measurements were concerned.
To build upon and clarify the results obtained by the abovementioned authors, we set up a system of acquisition, elaboration, and reproduction of models, with the aim of evaluating palatal expansion from a volumetric perspective.
Via statistical analysis, the present study revealed a significant increase in palatal volume following rapid expansion, whereas the reduction in volume that occurred between device removal and subsequent reevaluation was not statistically significant.
Results of this research indicate that an increase in palatal volume of mean 817.2 mm3 (ie, 21%) occurred between T1 and T2. This volumetric variation was both statistically and clinically significant. These results confirm those reported in other articles, which document an increase in skeletal and dental transversal diameters,11–13 an increase in the perimeter of the dental arch,12,24,25 and/or an increase in palatal area13 after expansive treatment. We found a mean volumetric reduction between T2 and T3 of 81.2 mm3, or 2%. This volumetric variation was statistically, but not clinically, significant.
With the rugae used as points of reference, these volumetric variations are evident from the graphic superimpositions of palatine volumes. These graphic representations clearly demonstrate the increase in volume that occurs during the active phase of expansion and a slight relapse after a fairly long observation period following removal of the expander.
Several articles have documented the percentage of relapse in the postretention period, which oscillates between the 0% found by Haas,26 the 10% reported by Herberger,27 and the 25% to 30% noted by Stockfish.28 The study carried out by Haas26 demonstrated absolute dental and skeletal stability in all cases studied. However, several limitations were present, including the small size of the sample (10 cases), the use not only of a separator but of other orthodontic appliances as well, and the extremely variable duration of the postretention period (from 2 to 6 years). Herberger27 evaluated a much larger sample (55 subjects) and preserved a certain homogeneity with regard to age (from 9 to 14 years), but this investigation also was carried out after orthodontic treatment involving rapid expansion was followed by the use of fixed appliances.
The high degree of relapse noted by Stockfish28 could be due to the extreme variation in age among members of his sample (6 to 32 years). The data obtained in the present study are in line with those reported by Marini and Bonetti,14 and by De Filippe,15 all of whom found that relapse was not significant.
The minimal degree of relapse between T2 and T3 found in this study could be due to any of three factors: (1) the young age of the patients (mean, 7.5 years), which led to a good orthopedic result, (2) the prolonged retention period (about 12 months), which permitted complete remineralization of the palatine suture, and (3) the repositioning of the tongue within the arches following an increase in upper diameter.
With regard to the second point, Hicks29 reported that the degree of relapse is linked to the maintenance procedures carried out post expansion. According to this author, removal of the expander immediately after the active expansion phase can result in a percentage relapse of up to 45%, whereas fixed maintenance for 2 to 3 months leads to 10% to 23% relapse, and a removable maintenance device provokes 22% to 25% relapse. Zimring and Isaacson30 demonstrated that the force that determines relapse continues to act for at least 6 weeks following expansion.
Regarding the third point, a reduction in volume was seen in 24 patients, and an increase in volume (a mean of 3%) was noted in 6. This increase could be due to repositioning of the tongue, or to the natural increase in size that occurs during growth.30–32
The mean increase in volume between T1 and T3 was 736 mm3, that is, 19%. An increase in palatal volume was seen in all patients treated. These results are consistent with those obtained by Marini and Bonetti,14 who found that the palatal volume of all patients was increased at 6 months following removal of the expander, and with those of De Filippe,15 who carried out postexpansion evaluation 9 to 12 months after the device was removed.
The results of the present study indicate that rapid expansion of the jaw is efficacious in increasing the volume of the palate, and that this criterion is stable over time, even though a slight relapse occurs after device removal. This study considered only variations in the skeletal and alveolar volume of the palate induced by the orthopedic effect of rapid expansion. The dental effects were not evaluated, as all patients were in mixed dentition during the active phase (T1-T2) and had permanent dentition at T3; thus no effective comparison of the orthodontic effects could be made.
CONCLUSIONS
Rapid maxillary expansion is an efficacious means of increasing the volume of the palate and remains stable over time.
Application of reverse engineering technology via laser scanning of plaster models to obtain 3D virtual models overcomes the limitations of 2D analysis.
REFERENCES
- 1.Lamparski D, Rinchuse D, Close J, Sciote J. Comparison of skeletal and dental changes between 2-point and 4-point rapid palatal expanders. Am J Orthod Dentofacial Orthop. 2003;123:321–328. doi: 10.1067/mod.2003.10. [DOI] [PubMed] [Google Scholar]
- 2.Silva Filho O, Padro Montes L, Torelly L. Rapid maxillary expansion in the deciduous and mixed dentition evaluated through posteroanterior cephalometric analysis. Am J Orthod Dentofacial Orthop. 1995;107:268–275. doi: 10.1016/s0889-5406(95)70142-7. [DOI] [PubMed] [Google Scholar]
- 3.Cross D, McDonald J. Effect of rapid maxillary expansion on skeletal, dental, and nasal structures: a postero-anterior cephalometric study. Eur J Orthod. 2000;22:519–528. doi: 10.1093/ejo/22.5.519. [DOI] [PubMed] [Google Scholar]
- 4.Wertz R. Skeletal and dental changes accompanying rapid midpalatal suture opening. Am J Orthod Dentofacial Orthop. 1970;58:41–66. doi: 10.1016/0002-9416(70)90127-2. [DOI] [PubMed] [Google Scholar]
- 5.Chung C, Font B. Skeletal and dental changes in the sagittal, vertical, and transverse dimensions after rapid palatal expansion. Am J Orthod Dentofacial Orthop. 2004;126:569–575. doi: 10.1016/j.ajodo.2003.10.035. [DOI] [PubMed] [Google Scholar]
- 6.Biederman W. Rapid correction of Class III malocclusion by midpalatal expansion. Am J Orthod Dentofacial Orthop. 1973;63:47–55. doi: 10.1016/0002-9416(73)90109-7. [DOI] [PubMed] [Google Scholar]
- 7.Sari Z, Uysal T, Serdan U, Basciftci F. Rapid maxillary expansion. Is it better in the mixed or in the permanent dentition? Angle Orthod. 2003;73:654–661. doi: 10.1043/0003-3219(2003)073<0654:RMEIIB>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Memikoglu T, Iseri H. Effects of bonded rapid maxillary expansion appliance during orthodontic treatment. Angle Orthod. 1999;69:251–256. doi: 10.1043/0003-3219(1999)069<0251:EOABRM>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Mundstock K, Barreto G, Meloti A. Rapid maxillary expansion with the Hyrax appliance: an occlusal radiographic evaluation study. World J Orthod. 2007;8:277–284. [PubMed] [Google Scholar]
- 10.Garib D, Henriques J, Janson G, Freitas M, Coelho R. Rapid maxillary expansion—tooth-tissue–borne versus tooth-borne expanders: a computed tomography evaluation of dentoskeletal effects. Angle Orthod. 2005;75:548–557. doi: 10.1043/0003-3219(2005)75[548:RMETVT]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Garrett B, Caruso J, Rungcharassaeng K, Ferrage J, Kim J, Taylor G. Skeletal effects to the maxilla after rapid maxillary expansion assessed with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2008;134:8.e1–8.e11. doi: 10.1016/j.ajodo.2008.06.004. [DOI] [PubMed] [Google Scholar]
- 12.Phatouros A, Goonewardene M. Morphologic changes of the palate after rapid maxillary expansion: a 3-dimensional computed tomography evaluation. Am J Orthod Dentofacial Orthop. 2008;134:117–124. doi: 10.1016/j.ajodo.2007.05.015. [DOI] [PubMed] [Google Scholar]
- 13.Oliveira N, Da Silveira A, Kusnoto B, Viana G. Three-dimensional assessment of morphologic changes of the maxilla: a comparison of 2 kinds of palatal expanders. Am J Orthod Dentofacial Orthop. 2004;126:354–362. doi: 10.1016/j.ajodo.2003.07.008. [DOI] [PubMed] [Google Scholar]
- 14.Marini I, Bonetti G. A, Achilli V, Salemi G. A photogrammetric technique for the analysis of palatal three-dimensional changes during rapid maxillary expansion. Eur J Orthod. 2007;29:26–30. doi: 10.1093/ejo/cji069. [DOI] [PubMed] [Google Scholar]
- 15.De Felippe N. L. O, Da Silveira A. C, Viana G, Kusnoto B, Smith B, Evans C. A. Relationship between rapid maxillary expansion and nasal cavity size and airway resistance: short- and long-term effects. Am J Orthod Dentofacial Orthop. 2008;134:370–382. doi: 10.1016/j.ajodo.2006.10.034. [DOI] [PubMed] [Google Scholar]
- 16.Mazzoli A, Germani M, Moriconi G. Application of optical digitizing techniques to evaluate the shape accuracy of anatomical models derived from CT data. J Oral Maxillofac Surg. 2007;65:1410–1418. doi: 10.1016/j.joms.2005.11.083. [DOI] [PubMed] [Google Scholar]
- 17.Lysell I. Plicae palatinae transverse and palla incisiva in man: a morphological genetic study. Acta Odontol Scand. 1955;13:5–137. [PubMed] [Google Scholar]
- 18.Peavy D, Kendricks G. The effect of tooth movement on the palatine rugae. J Prosth Dent. 1967;18:536–542. doi: 10.1016/0022-3913(67)90219-3. [DOI] [PubMed] [Google Scholar]
- 19.Almeida M, Phillips C, Kula K, Tulloch C. Stability of the palatal rugae as landmarks for analysis of dental cast. Angle Orthod. 1995;65:43–48. doi: 10.1043/0003-3219(1995)065<0043:SOTPRA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 20.Bailey J, Esmailnejad A, Almeida M. Stability of the palatal rugae as landmarks for analysis of dental cast in extraction and non extraction cases. Angle Orthod. 1996;66:73–78. doi: 10.1043/0003-3219(1996)066<0073:SOTPRA>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 21.Hoggan B, Sadowsky C. The use of palatal rugae for the assessment of anteroposterior tooth movements. Am J Orthod Dentofacial Orthop. 2001;119:482–488. doi: 10.1067/mod.2001.113001. [DOI] [PubMed] [Google Scholar]
- 22.Cristou P, Kiliaridis S. Vertical growth–related changes in the position of palatal rugae and maxillary incisors. Am J Orthod Dentofacial Orthop. 2008;133:81–86. doi: 10.1016/j.ajodo.2007.07.009. [DOI] [PubMed] [Google Scholar]
- 23.Scarfe W, Barman A, Sukovic P. Clinical applications of cone-bean computed tomography in dental practice. J Can Dent Assoc. 2006;72:75–80. [PubMed] [Google Scholar]
- 24.Brust E, McNamara J. A., Jr . Center for Human Growth and Development. Ann Arbor, MI: University of Michigan; 1995. Arch dimensional changes concurrent with expansion in mixed dentition patients. Michigan Growth Series. [Google Scholar]
- 25.Adkins M, Nanda R, Curier G. Arch perimeter changes on rapid palatal expansion. Am J Orthod Dentofacial Orthop. 1990;97:194–199. doi: 10.1016/S0889-5406(05)80051-4. [DOI] [PubMed] [Google Scholar]
- 26.Haas A. Long term post treatment evaluation of rapid palatal expansion. Angle Orthod. 1980;50:189–217. doi: 10.1043/0003-3219(1980)050<0189:LPEORP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 27.Herberger T. Rapid palatal expansion: long term stability and periodontal implication. Orthodontics and Orthopaedic Treatment in the Mixed Dentition. In: McNamara J, Brudon W, editors. Ann Arbor, MI: Needham Press; 1993. [Google Scholar]
- 28.Stockfish J. Rapid expansion of the maxilla—success and relapse. Trans Eur Orthod Soc. 1969:469–481. [PubMed] [Google Scholar]
- 29.Hicks E. Slow maxillary expansion: a clinical study of the skeletal versus dental response to low-magnitude force. Am J Orthod Dentofacial Orthop. 1978;73:121–141. doi: 10.1016/0002-9416(78)90183-5. [DOI] [PubMed] [Google Scholar]
- 30.Zimring J, Isaacson R. Forces produced by rapid maxillary expansion. Angle Orthod. 1965;35:178–186. doi: 10.1043/0003-3219(1965)035<0178:FPBRME>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 31.Melsen B. Palatal growth studied on human autopsy material. Am J Orthod Dentofacial Orthop. 1975;68:42–54. doi: 10.1016/0002-9416(75)90158-x. [DOI] [PubMed] [Google Scholar]
- 32.Melsen B, Melsen F. The postnatal development of the palatomaxillary region studied on human autopsy material. Am J Orthod Dentofacial Orthop. 1982;82:329–342. doi: 10.1016/0002-9416(82)90467-5. [DOI] [PubMed] [Google Scholar]