

Abstract
Objective:
To estimate and compare the duration of the pubertal growth peak in Class I and Class III subjects.
Materials and Methods:
The data examined consisted of pretreatment lateral cephalometric records of 218 skeletal Class I or Class III subjects (93 female and 125 male subjects) of white ancestry. The duration of the pubertal peak was calculated from the average chronological age intervals between stages CS3 and CS4 of the cervical vertebral maturation in Class I vs Class III groups (t-test).
Results:
In skeletal Class I subjects, the pubertal peak had a mean duration of 11 months, whereas in Class III subjects it lasted 16 months. The average difference (5 months) was statistically significant (P < .001).
Conclusions:
The growth interval corresponding to the pubertal growth spurt (CS3–CS4) was longer in Class III subjects than in subjects with normal skeletal relationships; the larger increases in mandibular length during the pubertal peak reported in the literature for Class III subjects may be related to the longer duration of the pubertal peak.
Keywords: Cervical vertebral maturation, Chronological age, Skeletal Class I and Class III, Pubertal peak, Skeletal age
INTRODUCTION
One of the most important factors in orthodontic treatment planning is the growth potential of the patient.1–4 Human growth and development are not uniform, with accelerations and decelerations in the growth velocity of different skeletal components at various developing maturational stages.5–7 The onset of puberty varies with sex, population, and the environment.8
For many years researchers5–16 have tested biological indicators to determine growth potential in adolescents. The classical parameters considered were body weight,12 body height,9–11 menarche,8,13 sexual maturation characteristics,7,13,14 chronological age,14 dental development,5,8,15 and skeletal development.5,7,16 Hand-wrist radiographs have been used widely as a reliable analysis to establish skeletal age.5–7 Unfortunately, the hand-wrist method requires additional radiation exposure when used in orthodontic treatment planning. In 1972 Lamparski17 created the first standards of cervical vertebral maturation as related to chronological age and to skeletal maturation as observed on hand-wrist radiographs. Subsequently many authors3–6,18–24 have proven that cervical vertebral maturation (CVM) has a high level of correlation with individual skeletal maturation. O'Reilly and Yanniello3 in 1988, Franchi et al in 2000,4 and Baccetti et al in 200522 demonstrated that the greatest increase in mandibular length occurred during the pubertal growth spurt and that this could be assessed during the interval between CS3 and CS4.
The onset, the duration, and the completion of the pubertal spurt in mandibular growth are relevant aspects in dentofacial orthopedics, as treatment outcomes and stability may be influenced by the maturational status of the patient.20 The literature provides indications about the duration of the pubertal peak in those with Class I occlusions, whereas information about the duration of the growth peak in persons with Class III malocclusion is lacking. This information is important, especially when considering the relationship among pubertal changes, mandibular growth, and Class III malocclusion. Reyes et al25 have reported that the pubertal growth spurt starts later and presents with an increased amount of mandibular lengthening in Class III patients vs persons with normal occlusion. The current investigation sought to evaluate the duration of the pubertal growth spurt in subjects with Class III malocclusion vs subjects with normal occlusion by using a reliable indicator of skeletal maturity (CVM method).
MATERIALS AND METHODS
The lateral cephalograms of 900 orthodontically untreated subjects, ages 8 through 18 years, were analyzed. The CVM stage on each radiograph was assessed according to the method of Baccetti et al,22 and skeletal class was assessed according to Björk's cephalometric analysis.26,27 The CVM staging was performed by one investigator and checked for accuracy by a second expert examiner.
The lateral cephalograms were analyzed on a conventional viewing screen and traced on acetate by the two observers. The measurements were made with mutual agreement between the two operators.
The criteria for inclusion in the survey were:
Cephalograms of good quality.
Caucasian ancestry.
No previous orthodontic treatment.
No congenitally missing or extracted teeth.
No systematic diseases that could have affected general development.
Skeletal Class I or III, with the diagnosis based on the A-N-Pog angle by Björk analysis (Class I = −0.5° ≤ A-N-Pog ≤ 4°; Class III = A-N-Pog < −0.5°).26,27
Vertical skeletal relationship (NL/ML angle by Björk analysis) ranging from 19° to 33°.26,27
Skeletal stages CS3 or CS4 based on the CVM method.22 CS3 corresponds to the initial stage of the accelerative portion of the pubertal growth peak, and CS4 corresponds to the final stage of the accelerative portion of the pubertal growth peak in adolescents.22
The final sample consisted of 218 subjects (93 female and 125 male subjects) with skeletal maturity of CS3 (113 cephalograms: 67 Class I subjects [28 female and 39 male subjects] and 46 Class III subjects [27 female and 19 male subjects]) or CS4 (105 cephalograms: 56 Class I subjects [34 female and 22 male subjects] and 40 Class III subjects [36 female and 13 male subjects]).
Statistical Analysis
Descriptive statistics for chronologic age (rounded to the month) were evaluated for each class group and for each CVM stage group. The variable “age” was tested with the Shapiro-Wilks test to confirm normal distribution and Levene's analysis of variance exploratory test for confirmation of homogeneity. No statistical significance was assessed. Student t-tests for independent samples (P < .05) were used to compare the age intervals between CS3 and CS4 in the Class I vs Class III subjects as well as between genders in the two skeletal groups. Statistical computations were performed by means of software (Statistica 8.0, Stat Soft Inc, for Windows XP, Tulsa, Okla).
RESULTS
Descriptive statistics for all the Class I and Class III groups investigated are shown in Table 1. No statistically significant differences in the duration of the CS3–CS4 interval were observed between genders. Differences in average chronological age between Class I and Class III subjects from stage CS3 to stage CS4 are shown in Table 2. The CS3–CS4 age interval was significantly longer (P < .001) in Class III subjects than in Class I subjects (average difference of 5 months; Table 2 and Figure 1). This difference was characterized by a significant effect size.28 The effect size was larger than two, which means that the average effect was much greater than the interindividual variability expressed by the average standard deviation.
Table 1.
Descriptive Statistics

Table 2.
Average Duration of the Pubertal Peak Interval in the Two Different Types of Skeletal Disharmony

Figure 1.
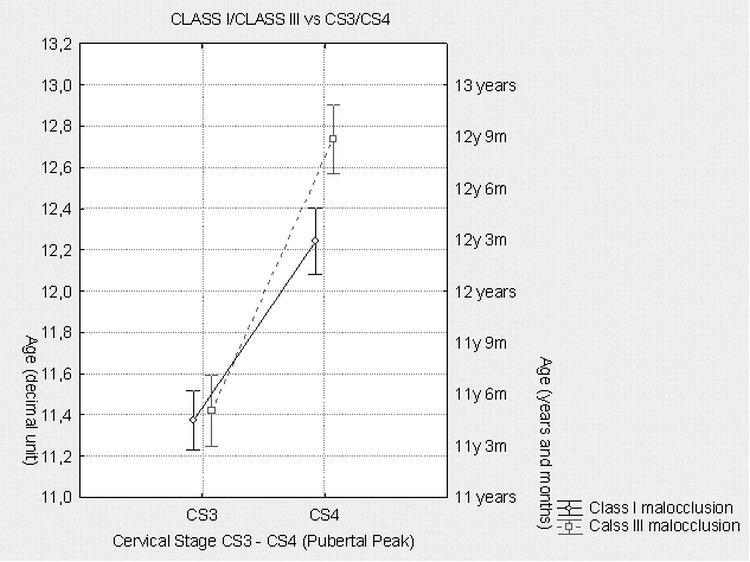
Box-and-whiskers diagram for skeletal Class I and Class III malocclusions. The significant difference in duration of the pubertal peak between Class I and Class III groups is approximately 5 months (P < .001).
DISCUSSION
The literature provides abundant evidence that the anteroposterior maxillomandibular relationship of untreated subjects with Class III malocclusion can worsen during the adolescent growth period, with special regard to the growth spurt period, and that this may affect treatment timing and stability of treatment outcomes.22,29,30 The present investigation sought to obtain information about the duration of the pubertal peak in untreated persons with Class III skeletal relationships when compared to those with normal skeletal relationships. The cephalometric records of 123 untreated white subjects with Class I skeletal relationships were compared with those of 95 untreated white subjects with skeletal Class III relationships, and the differences in the duration of the pubertal growth spurt (assessed as CS3–CS4 interval in the CVM analysis22) were evaluated.
Reyes et al25 reported that, in those with a Class III malocclusion, the largest “increase” in mandibular length (coincident with the pubertal peak) occurred, on average, 1 year later in both sexes with Class III skeletal relationships than it did in those with Class I relationships. The amount of mandibular growth was significantly greater in those with Class III relationships than in those with Class I relationships.25 In the current investigation the average chronological age at onset of the pubertal peak was very similar for both skeletal Class I and Class III subjects (average chronological age was 11 years 5 months). However, the pubertal growth spurt interval ended earlier for skeletal Class I subjects (average age of 12 years 3 months) than in skeletal Class III subjects (average age of 12 years 9 months). On average, therefore, the pubertal peak for Class I subjects lasted 11 months (in agreement with previous indications of the literature4,20–22), whereas in subjects with Class III malocclusion it lasted for a longer period (16 months). The difference in duration was statistically significant. Of course, the results reported in the present study are derived from cross-sectional data, and they do not express true longitudinal changes. However, the number of persons comprising the samples at both stages, along with the highly significant effect size of the difference in the “duration” of the growth spurt in the two groups, enforce the statistical significance of the outcomes.
The results of the current study may also entail a clinically significant aspect in relation to the enhanced amount of mandibular growth in subjects with Class III malocclusion compared to persons with normal occlusion.25 In other words, the increased mandibular length in Class III persons at the pubertal growth spurt25 could be linked to the longer duration of the pubertal peak in these subjects.
CONCLUSIONS
The average time of onset of pubertal peak in both Class I and Class III subjects is similar: 11 years and 5 months.
In Class I subjects, the interval between CS3 and CS4 (duration of pubertal peak) lasts 11 months, whereas it lasts 16 months in skeletal Class III malocclusion.
The greater increase in mandibular length in Class III subjects compared to that in Class I subjects during puberty might be associated with the longer duration of the pubertal peak in Class III subjects as reported in the literature.
Acknowledgments
The authors wish to thank Professor Geoffrey Shaw for his help with editing the manuscript and Mr Marek Michalski for assisting with the statistical evaluation of the data.
REFERENCES
- 1.Ricketts R. Facial and denture changes during orthodontic treatment as analyzed from the temporomandibular joint. Am J Orthod. 1955;41:163–179. [PubMed] [Google Scholar]
- 2.Singer J. Physiologic timing of orthodontic treatment. Angle Orthod. 1980;50:322–333. doi: 10.1043/0003-3219(1980)050<0322:PTOOT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.O'Reilly M, Yanniello G. J. Mandibular growth changes and maturation of cervical vertebrae—a longitudinal cephalometric study. Angle Orthod. 1988;58:179–184. doi: 10.1043/0003-3219(1988)058<0179:MGCAMO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 4.Franchi L, Baccetti T, McNamara J., Jr Mandibular growth as related to cervical vertebral maturation and body height. Am J Orthod Dentofacial Orthop. 2000;118:335–340. doi: 10.1067/mod.2000.107009. [DOI] [PubMed] [Google Scholar]
- 5.San Roman P, Palma J. C, Oteo D, Nevado E. Skeletal maturation determined by cervical vertebrae development. Eur J Orthod. 2002;24:303–311. doi: 10.1093/ejo/24.3.303. [DOI] [PubMed] [Google Scholar]
- 6.Hassel B, Farman A. Skeletal maturation evaluation using cervical vertebrae. Am J Orthod Dentofacial Orthop. 1995;107:58–66. doi: 10.1016/s0889-5406(95)70157-5. [DOI] [PubMed] [Google Scholar]
- 7.Fishman L. Chronological versus skeletal age, an evaluation of craniofacial growth. Angle Orthod. 1979;49:181–189. doi: 10.1043/0003-3219(1979)049<0181:CVSAAE>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Björk A, Helm S. Prediction of the age of maximum pubertal growth in body height. Angle Orthod. 1967;37:134–143. doi: 10.1043/0003-3219(1967)037<0134:POTAOM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Nanda R. S. The rates of growth of several facial components measured from serial cephalometric roentgenograms. Am J Orthod. 1955;41:658–673. [Google Scholar]
- 10.Bambha J. K. Longitudinal cephalometric roentgenographic study of face and cranium in relation to body height. J Am Dent Assoc. 1961;63:776–799. doi: 10.14219/jada.archive.1961.0289. [DOI] [PubMed] [Google Scholar]
- 11.Hunter W. S. The correlation of facial growth with body height and skeletal maturation at adolescence. Angle Orthod. 1966;36:44–54. doi: 10.1043/0003-3219(1966)036<0044:TCOFGW>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Green L. J. The interrelationships among height, weight, and chronological, dental, and skeletal ages. Angle Orthod. 1961;31:189–193. [Google Scholar]
- 13.Hägg U, Taranger J. Menarche and voice changes as indicators of the pubertal growth spurt. Acta Odontol Scand. 1980;38:179–186. doi: 10.3109/00016358009004718. [DOI] [PubMed] [Google Scholar]
- 14.Hägg U, Taranger J. Maturation indicators and the pubertal growth spurt. Am J Orthod. 1982;82:299–309. doi: 10.1016/0002-9416(82)90464-x. [DOI] [PubMed] [Google Scholar]
- 15.Hägg U, Matsson L. Dental maturity as an indicator of chronological age: the accuracy and precision of three methods. Eur J Orthod. 1985;7:25–35. doi: 10.1093/ejo/7.1.25. [DOI] [PubMed] [Google Scholar]
- 16.Grave K. C, Brown T. Skeletal ossification and the adolescent growth spurt. Am J Orthod. 1976;69:611–619. doi: 10.1016/0002-9416(76)90143-3. [DOI] [PubMed] [Google Scholar]
- 17.Lamparski D. G. Skeletal Age Assessment Utilizing Cervical Vertebrae [master's thesis] Pittsburgh, Penn: Department of Orthodontics, The University of Pittsburgh; 1972. [Google Scholar]
- 18.Mito T, Sato K, Mitani H. Cervical vertebral bone age in girls. Am J Orthod Dentofacial Orthop. 2002;122:380–385. doi: 10.1067/mod.2002.126896. [DOI] [PubMed] [Google Scholar]
- 19.Garcia-Fernandez P, Torre H, Flores L, Rea J. The cervical vertebrae as maturational indicators. J Clin Orthod. 1998;23:221–226. [PubMed] [Google Scholar]
- 20.Baccetti T, Franchi L, McNamara J., Jr An improved version of the cervical vertebral maturation (CVM) method for assessment of mandibular growth. Angle Orthod. 2002;72:316–323. doi: 10.1043/0003-3219(2002)072<0316:AIVOTC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 21.Franchi L, Baccetti T, McNamara J. A., Jr The cervical vertebral maturation method: some need for clarification. Am J Orthod Dentofacial Orthop. 2003;123:19A–20A. doi: 10.1067/mod.2003.69. [DOI] [PubMed] [Google Scholar]
- 22.Baccetti T, Franchi L, McNamara J., Jr The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin Orthod. 2005;11:119–129. [Google Scholar]
- 23.Flores-Mir C, Burgess C. A, Champney M, Jensen R. J, Pitcher M. R, Major P. W. Correlation of skeletal maturation stages determined by cervical vertebrae and hand-wrist evaluations. Angle Orthod. 2006;76:1–5. doi: 10.1043/0003-3219(2006)076[0001:COSMSD]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 24.Gandini P, Mancini M, Andreani F. A Comparison of hand-wrist bone and cervical vertebral analyses in measuring skeletal maturation. Angle Orthod. 2006;76(6):984–989. doi: 10.2319/070605-217. [DOI] [PubMed] [Google Scholar]
- 25.Reyes B. C, Baccetti T, McNamara J., Jr An estimate of craniofacial growth in class III malocclusion. Angle Orthod. 2005;76:577–584. doi: 10.1043/0003-3219(2006)076[0577:AEOCGI]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 26.Björk A. Prediction of mandibular growth rotation. Am J Orthod. 1969;55:585–599. doi: 10.1016/0002-9416(69)90036-0. [DOI] [PubMed] [Google Scholar]
- 27.Björk A, Skieller V. Normal and abnormal growth of mandible: a synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur J Orthod. 1983;5:1–46. doi: 10.1093/ejo/5.1.1. [DOI] [PubMed] [Google Scholar]
- 28.Cohen J. Statistical Power Analysis for the Behavioral Sciences 2nd ed. Mahwah, NJ: Lawrence Erlbaum; 1988. [Google Scholar]
- 29.Baccetti T, Franchi L, McNamara J., Jr Cephalometric variables predicting the long-term success or failure of combined rapid maxillary expansion and facial mask therapy. Am J Orthod Dentofacial Orthop. 2004;126:16–22. doi: 10.1016/j.ajodo.2003.06.010. [DOI] [PubMed] [Google Scholar]
- 30.Baccetti T, Franchi L, Cameron C, McNamara J., Jr Treatment timing for rapid maxillary expansion. Angle Orthod. 2001;71:343–350. doi: 10.1043/0003-3219(2001)071<0343:TTFRME>2.0.CO;2. [DOI] [PubMed] [Google Scholar]