

Abstract
Objective:
To evaluate the long-term changes in maxillary arch widths, overjet, and overbite in patients who were treated with rapid maxillary expansion (RME) followed by edgewise appliances.
Materials and Methods:
The material for the study consisted of study casts taken from 41 patients (19 males, 22 females) on four different occasions (before treatment, T1; after RME, T2; after treatment, T3; and during follow-up period, T4). The upper intercanine, interpremolar, and intermolar widths and overjet and overbite were measured on each set of study casts. Mean age of the subjects was 13.2 ± 1.3 years (range, 11.2–16.9 years) at T1, 13.3 ± 1.3 years (range, 11.3–17 years) at T2, 15.5 ± 1.4 years (range, 13.1–18.8 years) at T3, and 20.4 ± 1.6 years (range, 17.9–24.8 years) at T4.
Results:
The net increase in intercanine width, interpremolar width, intermolar width, overjet, and overbite was 1.4 ± 2.4 mm, 4.6 ± 2.6 mm, 4.3 ± 2.5 mm, 0.1 ± 0.6 mm, and 0.2 ± 0.6 mm, respectively, and the relapse rates were 37% for intercanine width, 19% for interpremolar width, and 17% for intermolar width at the end of the follow-up period.
Conclusions:
A significant amount of relapse occurred in maxillary arch widths at the postretention assessment, the greatest being in intercanine width. RME significantly decreased overbite and increased overjet, and a statistically significant decrease was observed in both overbite and overjet at the postretention assessment.
Keywords: RME, Long-term stability of RME
INTRODUCTION
The concept of midpalatal suture opening was first described by Angell in 1860.1 Rapid maxillary expansion (RME) has been a popular method for eliminating transverse discrepancy between the dental arches due to maxillary constriction for more than 40 years.2,3 Widening of the maxilla by RME provides correction of posterior crossbites and gain in arch perimeter in patients with tooth-size/arch-size discrepancies.4–7 Midpalatal suture opening can be accomplished in both children and adults, but with advancing maturity the rigidity of the skeletal components limits the extent and the stability of the expansion, which may involve fracturing the bony interdigitations.8–11 Differences in immediate treatment outcome and stability have also been attributed to appliance design and rate of expansion. Haas12 suggests that rapid palatal expansion with a soft tissue–borne appliance is superior to a totally tooth-borne palatal expander (ie, Hyrax). He believes the former delivers a more parallel expansive force on the two maxillary segments that is distributed evenly to both the teeth and alveolar processes.
The few long-term RME studies have shown that increments in maxillary transverse dimension are relatively stable.12,13 It has been argued that the arch width added by opening the midpalatal suture can be considered permanent because the midpalatal repair involved new bone formation. The permanence of change added by tooth movement and alveolar bending, on the other hand, is questionable.2 Two studies strongly demonstrate that RME accomplished by a tissue-borne appliance with reinforced dental anchorage can produce an orthopedic (skeletal) change with excellent stability of both the orthopedic and orthodontic corrections.12,14
The aim of this study, therefore, was to evaluate the long-term changes in maxillary dental arch widths and overjet and overbite in patients who were treated with tooth-/tissue-borne full coverage bonded RME appliance followed by edgewise appliances.
MATERIALS AND METHODS
The material of the study consisted of 164 sets of study casts taken from 41 subjects (19 males and 22 females) on four different occasions; pretreatment (T1), post-RME (T2), posttreatment (T3), and follow-up (T4). Mean age of the subjects was 13.2 ± 1.3 years (range, 11.2–16.9 years) at T1, 13.3 ± 1.3 years (range, 11.3–17 years) at T2, 15.5 ± 1.4 years (range, 13.1–18.8 years) at T3, and 20.4 ± 1.6 years (range, 17.9–24.8 years) at T4.
The patients' records were selected on the basis of the following criteria:
Had Class I or Class III incisor relationship with transverse maxillary constriction at the onset of the treatment.
Had been treated with no extraction.
Had been treated with edgewise appliances after rapid maxillary expansion.
Had post-RME retention with a transpalatal arch placed between upper first molars during fixed appliance therapy.
Clinical Management
All patients underwent RME with a splint-type tooth- and tissue-borne appliance.15 The acrylic part of the appliance extended over the occlusal and middle third of the vestibular surfaces of all teeth. The thickness of the occlusal acrylic surface was limited to the freeway space and was in contact with all lower teeth. A Hyrax screw was placed in the acrylic plate at the first molars and as near to the palate as possible. The Hyrax screw (Dentaurum, Pforzheim, Germany) was used to increase the rigidity of the appliance. The appliances were activated with a one-fourth turn twice per day in the first week and once per day after the sutures were mobilized. Expansion was stopped once the palatal cusps of the upper posterior teeth came into contact with the lingual cusps of lower posterior teeth. The expansion time was 3.4 to 4 weeks (mean, 3.5 weeks). The appliance used for rapid maxillary expansion was cleaned and reused as a retention appliance for three months. For subsequent retention, a transpalatal arch with extended palatal arms resting on the palatal surfaces of upper premolars was placed between first molars and the treatment was then continued with edgewise appliances.
Retention Protocol
At the end of the orthodontic treatment, all patients were instructed to wear a maxillary Hawley retainer 24 hours a day for two years and a fixed canine-to-canine lingual retainer was used for retention in the lower arch.
Model Measurements
The cusp tip was marked on the top point of the measured cusp using a 0.5-mm 2H pencil. All measurements were then made directly on the study casts using an electronic digital caliper and rounded to the nearest 0.01 mm. The following measurements were made on the study casts:
Intercanine width (IC): Distance between the tips of the cusps of the maxillary canines.
Interpremolar width (IP): Distance between the tips of the buccal cusps of the maxillary 1st premolars.
Intermolar width (IM): Distance between the tips of the mesiobuccal cusps of the maxillary 1st molars.
Overjet: The horizontal overlap of the incisors, being positive if the upper incisor is ahead of the lower incisor and negative if the lower incisor is in front of the upper incisor.
Overbite: The vertical overlap of the incisors when the posterior teeth are in contact; classified as positive if the incisors overlap vertically and negative if they are vertically separated.
To assess the reproducibility of the measurements, all measurements were repeated on 40 randomly selected sets of study casts at two time intervals. The difference between the measurements did not exceed 0.06 mm, which was considered insignificant.
Statistical Analysis
Student's t-test was performed to evaluate the possible sex differences in the variables examined in different phases. A paired samples t-test was performed to evaluate the alterations in variables examined in different phases.
RESULTS
The results of the Student's t-test revealed that there was no statistically significant sex difference between variables examined in different phases. Therefore, further analyses were performed on the group as a whole. Descriptive statistics of the intercanine width, inter-premolar width, intermolar width, overjet, and overbite in different evaluation phases are shown in Table 1.
Table 1. .
Descriptive Statistics of the Maxillary Arch Widths, Overjet and Overbitea
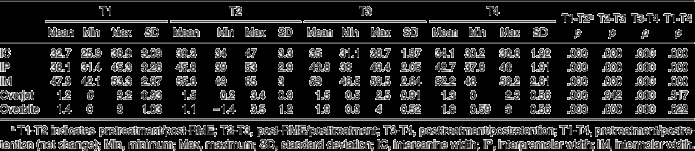
RME and fixed-appliance treatment produced absolute increases in maxillary arch widths. However, some width increases due to RME were reversed during fixed appliance treatment (65% decrease in intercanine width, 26% decrease in interpremolar width, 34% decrease in intermolar width). The relapse rates were 37% for intercanine width, 19% for interpremolar width, and 17% for intermolar width at post retention period (P < .001).
The overjet increased by 0.3 ± 0.4 mm after rapid maxillary expansion, remained unchanged after treatment, and decreased by 0.2 ± 0.3 mm after retention. The net increase was 0.1 ± 0.6 mm. However, the comparison of pretreatment and follow-up records revealed no statistically significant change in overjet (P > .05). The overbite decreased by 0.3 ± 0.4 mm after RME, increased by 0.8 ± 0.9 mm after treatment, and decreased by 0.3 ± 0.3 mm after retention. The net increase was 0.2 ± 0.6 mm (P < .05).
Changes observed in maxillary arch widths and overjet and overbite in different phases are shown in Figures 1 and 2.
Figure 1.
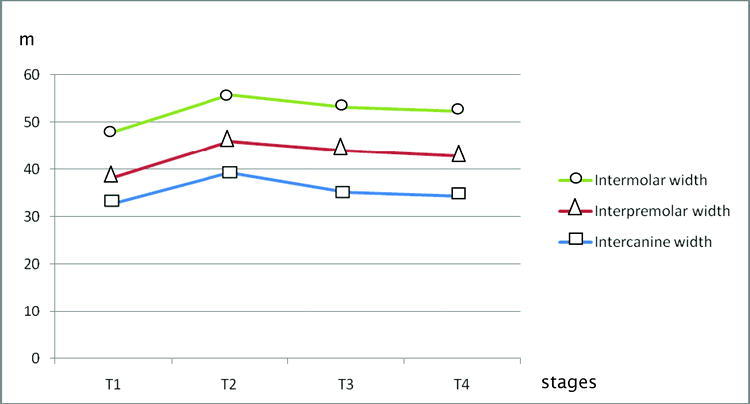
Changes observed in maxillary arch widths
Figure 2.
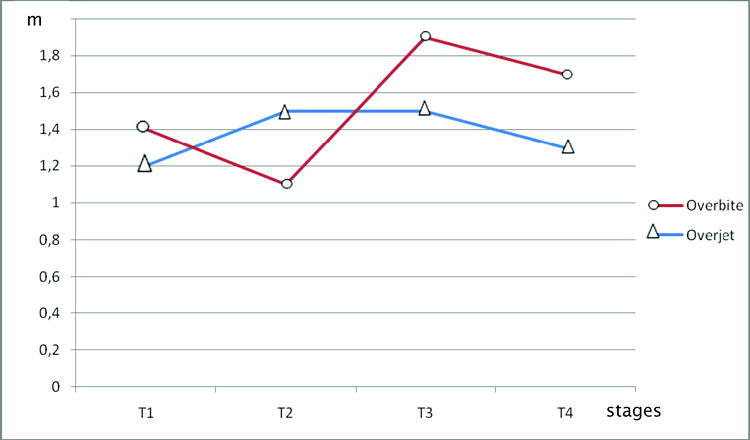
Changes observed in overjet and overbite
DISCUSSION
The present longitudinal study evaluated the changes in upper arch dimensions and overjet and overbite in patients who were treated with RME followed by fixed appliances. At the onset of the treatment, all patients exhibited maxillary constriction and crowding in varying degrees. A full-coverage acrylic cap splint type RME appliance was used for RME in all patients.
Expansion through maxillary suture widening by rapid maxillary expanders has been claimed to promote stability after retention. Stability has been attributed to the skeletal component of arch enlargement obtained by the expansion appliance as opposed to dental expansion as a result of edgewise appliance mechanotherapy. Studies on immediate treatment effects of rapid palatal expansion have reported increases in arch width as a result of combined skeletal and dental expansion. Short-term follow-up has indicated a rebound effect of the dental component, yet relative stability of the skeletal aspect of the expansion.2,8,12 The implant studies by Krebs during a 7-year observation period found a substantial reduction in dental arch width after discontinuing retention, which continued for as long as 4 to 5 years.13
Herold16 reported a net increase of 3.2 mm in intercanine width in his long-term study in which the Hyrax appliance was used. Linder-Aronson and Lindgren17 reported a net increase of 2.1 mm and a relapse rate of 62% in their subjects, who were treated with the Hyrax appliance. Stockfish18 reported a smaller relapse rate (50%). Moussa et al19 found a net increase of 3.6 mm in intercanine width in their long-term study. In the present study, the net increase in intercanine width was 1.4 mm, and the relapse rate was 37%. At the postretention assessment, intercanine width had decreased by 0.8 mm. This finding concurs with that of Moussa et al.19 In the present study, however, 65% of the expansion achieved in intercanine width with RME was lost during fixed appliance treatment leading to a smaller net increase. This can be attributed to the blocked-out canines, which moved into their correct positions with fixed appliance treatment.
In a study of long-term effects, McNamara et al20 reported that inter-first-premolar width increased by 4.9 mm with RME followed by fixed appliance treatment and relapsed 0.6 mm in the long term, leaving a net increase of 4.3 mm.20 In the present study, inter-first-premolar width increased by 7.6 mm after RME, decreased by 2 mm after treatment, and relapsed 1 mm in the long term. As a result, the net increase approximated that of McNamara et al.20
In the present study, the net increase in intermolar width was 4.2 mm and the relapse rate was 16.8% over a 5-year follow-up period. Final intermolar width was 4.6 mm larger than its pretreatment dimension and closely approximated its posttreatment dimension. Linder-Aronson and Lindgren17 reported a net increase of 5.9 mm in their 5-year posttreatment study. Herold16 reported a net increase of 3.9 mm over a period of observation similar to that of Linder-Aronson and Lindgren.17 Moussa et al,19 using the Haas appliance, found a net increase of 5.5 mm in the study subjects, who had been out of retention for 8 to 10 years. McNamara et al20 reported a net increase of 4.5 mm in their long-term study in which a Haas appliance was used. Spillane and McNamara,21 using acrylic-bonded expanders, reported an average of 5 mm residual expansion 2.4 years after expansion. Lima et al,22 using the Haas appliance, evaluated the long-term effects of RME and reported a net increase of 5.6 mm over an observation period of 5 years. On the basis of these findings, it can be suggested that the splint-type tooth- and tissue-borne RME appliance used in the present study did not provide an advantage over the RME appliances used in the aforementioned studies with regard to long-term stability.
Garib et al23 evaluated the long-term effects of RME on dental arches through lateral cephalometric radiographs taken from patients who were treated with RME followed by fixed edgewise treatment. When compared with the control group, they found a net overjet decrease of 0.6 mm. However, no statistically significant changes were found concerning overbite. In this study, overjet increased after RME, whereas overbite decreased. The net increase in overjet was 0.1 mm and was statistically insignificant. The net increase in overbite, however, was 0.2 mm which was statistically significant. Follow-up records revealed a 0.3-mm relapse in overbite.
CONCLUSIONS
RME and fixed appliance treatment produced absolute increases in maxillary arch widths. However, some width increases due to RME were reversed during fixed appliance treatment, and a significant amount of relapse occurred in the long term, the greatest being in intercanine width.
RME significantly decreased overbite and increased overjet, and a statistically significant decrease was observed in both overbite and overjet at the postretention assessment.
REFERENCES
- 1.Angell E. H. Treatment of irregularities of the permanent adult teeth. Dental Cosmos. 1860;1:540–544. [Google Scholar]
- 2.Haas A. J. Rapid expansion of the maxillary dental arch and nasal cavity by opening the midpalatal suture. Angle Orthod. 1961;31:73–90. [Google Scholar]
- 3.McNamara J. A., Jr Maxillary transverse deficiency. Am J Orthod Dentofacial Orthop. 2000;117:567–570. doi: 10.1016/s0889-5406(00)70202-2. [DOI] [PubMed] [Google Scholar]
- 4.Haberson V. A, Myers D. R. Midpalatal suture opening during functional posterior crossbite correction. Am J Orthod. 1978;74:310–313. doi: 10.1016/0002-9416(78)90207-5. [DOI] [PubMed] [Google Scholar]
- 5.Hesse K. L, Årtun J, Joondeph D. R, Kennedy D. B. Changes in condylar position and occlusion associated with maxillary expansion for correction of functional unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 1997;111:410–418. doi: 10.1016/s0889-5406(97)80023-6. [DOI] [PubMed] [Google Scholar]
- 6.McNamara J. A, Jr, Brudon W. L. Ann Arbor, Mich: Needham Press; 1993. Orthodontic and Orthopedic Treatment in the Mixed Dentition; pp. 67–93. [Google Scholar]
- 7.Adkins M. D, Nanda R. S, Currier G. F. Arch perimeter changes on rapid palatal expansion. Am J Orthod Dentofacial Orthop. 1990;97:194–199. doi: 10.1016/S0889-5406(05)80051-4. [DOI] [PubMed] [Google Scholar]
- 8.Wertz R. A. Skeletal and dental changes accompanying rapid maxillary suture opening. Am J Orthod. 1980;58:41–66. doi: 10.1016/0002-9416(70)90127-2. [DOI] [PubMed] [Google Scholar]
- 9.Krebs A. A. Expansion of the midpalatal suture, studied by means of metallic implants. Acta Odontol Scand. 1959;17:491–501. [Google Scholar]
- 10.Zimring J. F, Isaacson R. J. Forces produced by rapid maxillary expansion. III. Forces present during retention. Angle Orthod. 1965;35:178–186. doi: 10.1043/0003-3219(1965)035<0178:FPBRME>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Berlocher W. C, Mueller B. H, Tinaoff N. The effect of maxillary palatal expansion on the primary dental circumference. Pediatr Dent. 1980;2:27–30. [PubMed] [Google Scholar]
- 12.Haas A. J. Long-term post-treatment evaluation of rapid palatal expansion. Angle Orthod. 1980;50:189–218. doi: 10.1043/0003-3219(1980)050<0189:LPEORP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Krebs A. Midpalatal suture expansion studies by the implant method over a seven year period. Trans Europ Orthod Soc. 1964;40:131–142. [PubMed] [Google Scholar]
- 14.Haas A. J. The treatment of maxillary deficiency by opening the midpalatal suture. Angle Orthod. 1965;35:200–217. doi: 10.1043/0003-3219(1965)035<0200:TTOMDB>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Basciftci F. A, Karaman A. I. Effects of a modified acrylic bonded rapid maxillary expansion appliance and vertical chin cap on dentofacial structures. Angle Orthod. 2002;72:61–71. doi: 10.1043/0003-3219(2002)072<0061:EOAMAB>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 16.Herold J. S. Maxillary expansion: a retrospective study of three methods of expansion and their long-term sequelae. Br J Orthod. 1989;16:195–200. doi: 10.1179/bjo.16.3.195. [DOI] [PubMed] [Google Scholar]
- 17.Linder-Aronson A, Lindgren J. The skeletal and dental effects of rapid maxillary expansion. Br J Orthod. 1979;6:25–29. doi: 10.1179/bjo.6.1.25. [DOI] [PubMed] [Google Scholar]
- 18.Stockfish H. Rapid expansion of the maxilla-success and relapse. Trans Eur Orthod Soc. 1969;45:469–481. [PubMed] [Google Scholar]
- 19.Moussa R, O'Reilly M. T, Close J. M. Long-term stability of rapid palatal expander treatment and edgewise mechanotherapy. Am J Orthod Dentofacial Orthop. 1995;108:478–488. doi: 10.1016/s0889-5406(95)70048-x. [DOI] [PubMed] [Google Scholar]
- 20.McNamara J. A, Jr, Baccetti T, Franchi L, Herberger T. A. Rapid maxillary expansion followed by fixed appliances: a long-term evaluation of changes in arch dimensions. Angle Orthod. 2003;73:344–353. doi: 10.1043/0003-3219(2003)073<0344:RMEFBF>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 21.Spillane L. M, McNamara J. A., Jr Maxillary adaptation to expansion in the mixed dentition. Semin Orthod. 1995;1:176–187. doi: 10.1016/s1073-8746(95)80021-2. [DOI] [PubMed] [Google Scholar]
- 22.Lima A. L, Lima Filho R. M, Bolognese A. M. Long-term clinical outcome of rapid maxillary expansion as the only treatment performed in Class I malocclusion. Angle Orthod. 2005;75:416–420. doi: 10.1043/0003-3219(2005)75[416:LCOORM]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 23.Garib D. G, Henriques J. F, Carvalho P. E, Gomes S. C. Longitudinal effects of rapid maxillary expansion. Angle Orthod. 2007;77:442–448. doi: 10.2319/0003-3219(2007)077[0442:LEORME]2.0.CO;2. [DOI] [PubMed] [Google Scholar]