

Abstract
Emotional awareness has been previously investigated among clinicians. In this work, we bring to the fore of research the interest to uncover emotional awareness of clinicians during the tele-mental health session. The study reported here aimed at determining whether clinicians process their own emotions, as well as those of the client, in a computer-mediated context. Also, clinicians’ decision-making process was assessed because such action appears to be related to the way they feel and recognise how those emotions may change their thinking and impact their interaction with clients. We estimated that such ability in clinicians’ would be contrasted when the psychotherapy-session level is conducted via various technologies. Participant of the study were presented by stimuli in different modes of delivery (e.g. text, audio, and video). The experiment indicates that the ability to manage, perceive, and utilise emotions was as being satisfactory during all modes of delivery. In essence, the findings contribute to the field of remote therapy suggesting emotional awareness as a key cognitive factor in diagnosis.
Keywords: Emotional awareness, Emotional intelligence, Diagnosis, Decision-making, Computer-mediated psychotherapy, Human-computer interaction, E-mental health
Introduction
Emotional awareness is an ability to recognise the emotions or feelings expressed by others, or experienced by oneself [51, 52]. Individuals with a high level of emotional awareness detect and discriminate emotional states accurately [51, 53, 88]. It has been argued that the ability to recognise emotions in others can contribute to personal relationships, such as fostering happy and stable relationships between couples [10]. In the case of building friendships between peers, research shows that emotional awareness increases knowledge of one another, and thus enables people to arrange their professional, economic, or political relationships in beneficial and respectful ways [41].
Emotional awareness is also useful in the healthcare sector [3, 39]. It is supported by studies in which various method of treatment including cognitive-behavioural therapy, client-centred therapy and emotion-focused therapy (EFT) were employed to make clients be aware of their emotions and to use these emotions in a more adaptive manner [28, 92]. For example, clinical studies have demonstrated that the enhancement of emotional awareness in patients with eating disorders can increase their involvement in therapy and is linked to improvements in their conditions [57]. In consistent with this finding, Kim and his colleagues [45] show that an increased level of emotional awareness in patients with clinical depression condition can improve and accelerate their treatment effects.
Given the usefulness of emotional awareness in therapeutic settings, and therapeutic training [39, 86], one could assume that clinicians would be better able to identify emotions in others than members of the general public [83]. In other words, it is argued that clinicians who have higher emotional awareness will be more resilient to the anxieties when they practice and become less likely to experience fatigue, which in turn can cause better doctor-patient relationships, and improve the satisfaction level in patients [46, 63]. This is not a new notion though. Machado et al. [56] had investigated emotional awareness among different groups and showed that psychotherapists were indeed better able to identify basic emotions in others than were other groups of people. Further, it has been found that if a psychotherapist was aware of the emotions expressed by their clients throughout the therapeutic process, the process was deemed easier and more often ended with positive outcomes for the client [42]. Similarly, it has been demonstrated that clinical reasoning, including examination, analysis, and consultation, are improved when psychotherapists deliberate over a client’s emotional states [59].
It also has to be noted that therapists should be aware of their own emotions while they seek to recognise and analyse a client’s psychological state. The literature shows that mood (as a longer-term affective state) can influence social relationships between people [8]. Specifically, Gurman [31, 32] argued that therapists need to be aware of their own emotions because clients with severe mental health problems can affect a therapist’s mood and thus their health. Gurman also stated that assessing the daily emotional experiences of therapists will elucidate the way that they regulate the therapeutic process. To this end, researchers have found that therapists’ negative moods can have a destructive influence on how they process information in health-related tasks, such as mental health screening or diagnosis [29, 30, 64, 65, 74]. The corollary of this is that therapists’ positive moods enhance the therapeutic alliance [6]. For example, Elkind [24] and Gurman [31, 32] found that therapists who were mentally ‘in tune’ with their clients engaged more effectively with them.
To date, a number of studies have demonstrated that communication can be enhanced if people are capable of identifying expressed emotions [20, 89]. It has been demonstrated that a strong awareness of bodily symptoms as well as the ability to segregate emotions (i.e. attending to one’s own emotions and the others) can decrease the occurrence of somatic complaints in adults [72]. Of particular note in clinical settings is the psychotherapist’s emotional awareness, which plays an important role in therapeutic interactions [39]. However, little research has focussed on the emotional awareness of clinicians who engage in computer-mediated psychotherapy (CMP) and, given the increased importance of telecommunication technologies in psychotherapy, this is clearly an important field of exploration.
Two inquiries are therefore sought in the current study. Experiment 1 encapsulates the first inquiry by assessing whether CMP-like sessions inhibit the emotional awareness of clinicians. Emotional awareness is a multidimensional construct with clearly defined and well-operationalised factors (e.g. perceiving, integrating, and understanding emotions in oneself or others), but technology may challenge the ability to apply the skills needed to be aware of the emotions expressed by others. An important consideration is that different people can feel and express different emotions in different ways, even though there is general agreement about the basic emotions [21–23, 61]. This could influence the way people define their emotional states and think about themselves, but ‘expression’ will be controlled in the following experiment. Also, computer-mediated communication (CMC) has the potential to (1) impair affective perception, (2) inhibit emotional engagement, and (3) interfere with the ability to respond appropriately to the emotions of communicators.
A secondary goal of experiment 1 is to explore the relationship between exposure to emotions and the therapist’s awareness of their own emotions, specifically as it relates to communication via technology. This is important because spending long hours at a computer can place physical and mental health at risk. Feeling tired, stressed, or depressed are common computer-induced health conditions that may interfere with a clinician’s perceptual and diagnostic efficacy [7, 90]. Furthermore, it has been argued that understanding the therapist’s emotional states can provide valuable information about the therapeutic process [62]. Psychotherapists usually deal with emotionally distressing situations which may affect their own emotional well-being and ability to engage with their clients. Therefore, based on the work of Hancock and his colleagues [33], it is hypothesised that the use of technology and exposure to the negative emotions expressed by a client will negatively impact the mood of the clinician. This, in turn, will interfere with a therapist’s emotional awareness, including the ability to identify and recognise emotions during a CMP-like session.
Experiment 2 seeks the second inquiry of the study and is the first of its kind to explore the potential mediating role CMC might have between emotional awareness and decision-making. It was deemed important to understand how emotional awareness influenced analytical decision-making when cybertherapists are provided with psychotherapeutic content during video-based CMP.
Figure 1 provides an illustration of the conceptual model that underlies this experiment. In this model, emotional perception is an ability that psychotherapists possess that influences their decision-making. Alvandi et al. [4] has shown that the accurate perception of emotions increases engagement with the client’s problems. Understanding whether clinicians are sensitive to this emotional information can also help them with the diagnostic process [82]. However, the awareness of emotions/emotionality of communication per se might not impact how decisions are made. An understanding of one’s own emotions, and an ability to employ emotional responses, is also likely to assist clinicians in understanding if their clients’ emotions have a positive or negative impact on the clinician’s decision-making. This is where a measure of emotional intelligence is valuable. Emotional intelligence which can be used as an alternative to emotional awareness has been referred to as a person’s ability to monitor their own, and others’, emotions in order to use this information appropriately and guide their thinking and behaviour [17].
Fig. 1.
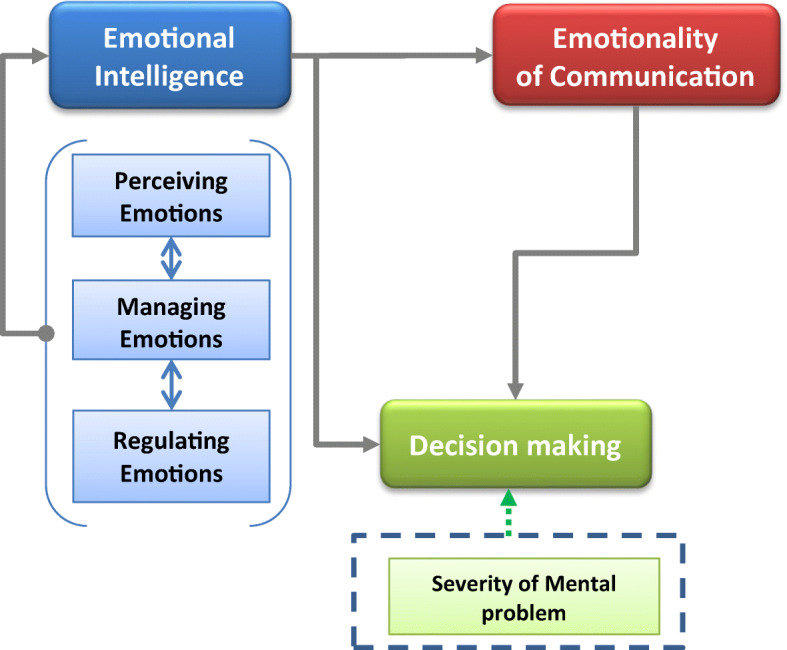
The conceptual model of emotional awareness involved in the diagnostic process of therapeutic communication
Previous studies have confirmed that people’s judgments and behaviours in their workplace are affected by their level of emotional intelligence [70, 81]. Emotional intelligence is also important in the context of therapeutic communication [80]. It can be thought of as a cognitive ability that influences the way clinicians engage with the emotional states of their clients, and how they use emotional information in the decisions they make regarding treatment. Kaplowitz et al. [42] showed that in face-to-face sessions, therapists with higher emotional intelligence produce more accurate assessments. In face-to-face clinical settings, mindful examination of clients’ mental disorders is vital for psychotherapeutic diagnosis, good clinical treatment, and productive care [44, 48]. Other literature links emotional intelligence and conscious decision-making. In a study assessing interns, Rieck and Callahan [71] show that emotional intelligence is valuable because it enabled these people to use emotional information to benefit their subsequent therapeutic actions.
The impetus for this experiment stems from recent research demonstrating that emotions and awareness of emotions have a central role in decision-making [13]. Furthermore, the relationship between emotional awareness and decision-making is an essential component of psychotherapy [5]. As discussed, emotional awareness allows clinicians (and patients) to manage therapy better. For accurate diagnosis of disorders, psychotherapists need to correctly identify relevant information communicated by clients, in addition to recognising relevant symptoms. This information may take the form of personal and emotional information. Emotional information is very important here because it reveals a client’s feelings, mood, thought processes, conflict resolution strategies, and behaviours in day-to-day situations [29, 43]. However, it has been suggested that CMP does not convey the same richness of emotional information (verbal and nonverbal) as direct, face-to-face interactions. Therefore, the second experiment will attempt to determine whether the nature of mental problems presented via technology impacts (1) the emotional awareness of cybertherapists and (2) their ability to engage with cyberclients.
Based on this information, the hypotheses are as follows:
H1. It is, therefore, predicted that the emotional awareness of cybertherapists will be decreased after using technology.
H2. There is a positive correlation between emotional intelligence and the ability of cybertherapists to perceive emotions.
H3. The quality and quantity of emotional information available via technology will negatively impact the diagnostic ability of cybertherapists.
H4. Higher levels of emotional intelligence will improve cybertherapists’ decision-making abilities.
Method
Participants
In experiment 1, 10 men and 12 women participated. They had an average of 34.3 years (SD = 10.07 years, range 23–54 years). Thirteen (59.1%) participants were native English speakers, while 9 (40.9%) had learned English as a second language. The education level of 14 (63.6%) of the participants was postgraduate, while six (27.3%) had an undergraduate degree as their highest qualification; two (9.1%) participants had another qualification. Participants were grouped into two categories: Those who had received training in psychology, and those who had not. Five (22.7%) participants with a background in psychology were professionals or students in the field of psychology or counselling, while another four (18.2%) were from medicine or nursing. Lastly, five (22.7%) participants without training in psychology were professionals or students from the social/human sciences, five (22.7%) were from the engineering/natural sciences, and three (13.6%) described themselves as possessing expertise in another field.
In experiment 2, 60 people participated. They were 20 (33.30%) men, 39 (65.00%) women, and one (1.70%) participant described themselves as female-to-male transgender. The majority of participants (N = 48 [80%]) were native English speakers from Australia, the USA, the UK, and Ireland. Participants had a mean age of 49.40 years (SD = 13.85 years, range 21–79 years). In terms of education, 20.00% (N = 12) had a PhD, 60.00% (N = 36) had postgraduate training, 11.67% (N = 7) undergraduate, 5.00% (N = 3) had a diploma and 3.33% (N = 2) had completed secondary school.
All of the participants in experiment 2 described their occupation as being within the psychological and health services field. Specifically, 56 (93.3%) participants were trained psychologists or accredited counsellors, one (1.7%) described her occupation as being in ‘medicine’ and three (5%) had occupations other than psychotherapy and counselling. Of those participants not working directly in psychotherapy, two persons (3.34%) described their profession as ‘social and human sciences’, while one (1.67%) worked in market research as an occupational psychologist. As part of a demographics questionnaire, participants were asked about their online or telecounselling experience. Thirty-seven people were currently offering online or telecounselling services. Another eight participants had previously offered online or telecounselling services. Fifteen participants, however, had no previous experience with online or telecounselling services.
Two female clinical psychologists served as panellists in experiment 2. They were native English speakers. They both had postgraduate qualifications and an average of 15 years experience practicing or working in psychology. One evaluator had offered online/telecounselling services and the other had provided only face-to-face psychotherapy. These expert evaluators assessed the severity of the psychological problems presented in the stimuli by rating the emotionality of the communicated content. Their ratings were used as a benchmark from which the assessments provided by the participants were compared.
Measures
The participants’ emotional states were assessed using the Positive and Negative Affect Schedule (PANAS). The Emotional Awareness Questionnaire (EAQ) assessed whether participants were aware of, and appreciated, their current emotional state. Three other measures were used to assess the decision-making abilities and emotional awareness of participants: The Assessing Emotions Scale (AES), the Emotionality in Cyberspace (EiC) instrument, and the Decision-Making Questionnaire (DMQ). Details of these measures are provided below.
The Positive and Negative Affect Schedule
The PANAS is a psychometric scale used to measure the moods of participants at different times, e.g. at present or last week [93]. This instrument was developed to assess positive and negative moods (e.g. guilty, active, ashamed). Ten statements from the PANAS ask about positive emotions, while the other 10 ask about negative emotions. Participants respond to the items on a 5-point Likert scale (ranging from 1 ‘very slightly or not at all’ to 5 ‘extremely’). A positive affect score is calculated by adding the positive emotional items together, and a negative affect score is calculated by adding negative emotional items together. A higher ‘positive’ score indicates a better mood.
The PANAS instrument has good reliability and validity. The Cronbach’s alpha has been reported to range from 0.86 to 0.90 for the positive affect (PA) scale and 0.84 to 0.87 for negative affect (NA) scale [15, 18]. In the current experiment, the PANAS Cronbach’s alphas were 0.84 for the PA scale and 0.68 for the NA scale.
Emotional Awareness Questionnaire
Rieffe et al.’s [72] EAQ is a psychometric scale used to measure how well people understand and regulate their emotions. It is comprised of 30 items, grouped into six subscales of emotional awareness or emotional functioning: ‘Differentiating emotions’, ‘Verbal sharing of emotions’, ‘Not hiding emotions’, ‘Bodily awareness of emotions’, ‘Attending to others’ emotions’ and ‘Analysing of own emotions’. Twenty items are negatively formulated and thus are reversed-scored. Participants choose one of three ratings (1 = not true, 2 = sometimes true, 3 = often true) to respond to EAQ items. A syntax developed by EAQ’s developers is used to compute a score for each category.
The EAQ has acceptable validity and reliability and is promising for differentiating between aspects of emotional awareness [14, 72]. The Cronbach’s alpha coefficient has been reported as ranging from 0.61 to 0.77 [14, 49, 50]. In this experiment, reliability for the EAQ reached 0.61 (pre-experiment) and 0.55 (post-experiment).
The Assessing Emotions Scale
The Assessing Emotions Scale (AES) is a 33-item self-report inventory that measures an individual’s emotional intelligence [78]. The AES employs a five-point Likert scale, rated from 1 (strongly disagree) to 5 (strongly agree). Total scores are calculated by reverse coding some items (i.e. items 5, 28, and 33) and then summing all items. Scores can range from 33 to 165, with higher scores indicating a greater level of emotional intelligence. The scale can also assess the original components of Salovey and Mayer’s [75] theory of emotional intelligence via the subscales: perception of emotions (10 items), managing one’s own emotions (9 items), managing others’ emotions (8 items), and utilising emotions.
The AES has been used to assess emotional intelligence in several areas, including mental health, employment, and academia [16, 36, 76, 77, 79]. Such studies have reported the AES’s reliability to be acceptable, with Cronbach’s alpha for total scale scores ranging between 0.87 and 0.90. The reliability achieved in the current study was similar (i.e. alpha coefficient of 0.84). Table 1 shows that the subscales also have good internal consistency scores that were comparable with reports by Schutte et al. [78]. Schutte et al. [78] listed 48 studies and found that (1) perception of emotions had an alpha between 0.76 and 0.80, (2) managing one’s own emotions was between 0.63 and 0.78, (3) the alpha for managing others’ emotions was 0.66, and (4) utilising emotions was 0.55.
Table 1.
The reliability of the emotional intelligence subscales used in the experiment 2
| Categories | Cronbach’s alpha if item deleted |
|---|---|
| Perception of emotion | 0.741 |
| Managing own emotions | 0.752 |
| Managing others’ emotion | 0.754 |
| Utilising emotion | 0.789 |
The Emotionality in Cyberspace
The EiC is an instrument developed by the author to evaluate a person’s ability to perceive the emotional content of technology-based communication [4]. Based on previous research [6, 9, 25, 58, 69], four subscales were included in this questionnaire. One of these, intensity, measures the perceived magnitude of emotions expressed by the speaker (e.g. the client). Emotional valence relates to the perceived quality (e.g. positive or negative) of the speaker’s expressions [6]. Potency measures the perceived strength of the expressed emotions [58]. When nonverbal cues are available, actions (e.g. rotating the body away from the screen), gaze behaviours (e.g. staring), and facial expressions (e.g. lowered eye-brows) can signal how potent emotions are in speakers. Activation indicates how connected speakers are (consciously) to their own emotions [35]. This factor helps determine if the emotional expression is influenced by the goals of the communication.
The EiC is a self-report measure of emotionality in which the participants rate communication on Visual Analog Scales (VASs) ranging from ‘0’ (not at all) to ‘100’ (a great deal). The overall experience of emotionality is calculated by summing the scores of all factors. Cronbach’s coefficient for EiC was recorded 0.75 [2, 4].
Decision-Making Questionnaire
The DMQ was developed by the authors to assess the decision-making abilities of participants. The questions in this survey ask participants to determine whether they believed the person in a vignette was suffering from a mental health issue. The possible responses are ‘no problem’, ‘personal issues but not significant’, ‘significant issue(s) that need(s) professional help’, and two other options that include ‘minor problem requiring no action’, ‘mild problem but definitely present’, and ‘moderately severe problem’. These options should indicate more complex decision-making.
In addition to these response options, participants also scored the ‘intensity of the psychological problem’ on a VAS between ‘0’ to ‘100’, with zero being ‘weak’ and 100 being ‘very severe’. Participants only marked this scale if they diagnosed the client as having a significant psychological problem. This measure aimed to connect the intensity of mental health problems to the intensity of the emotions displayed in the vignette.
Materials
Two video clips, each of approximately 4 min duration, were used as the stimuli in this experiment. The two clips were edited extracts from a single video simulating an intake interview that had depressive-anxiety theme. The second clip contained more emotional information than the first, as confirmed by the panellists—who found that the first clip contained fewer emotional expressions (e.g. behavioural and verbal cues) and less emotional information than the second clip (Mfirst clip = 262 and Msecond clip = 348).
Although the quality of the video’s resolution and audio was kept as consistent as possible across both vignettes, the two clips contained different presentations of a single psychological problem. The first clip displayed was from a medium distance in which participants observed facial (emotional) expressions and few body language cues from the speaker, and a partial view of the environment. The second clip, however, was displayed with a medium-wide shot. In that clip, participants still had enough information to assess the speaker’s facial expressions, and relatively more of his body language and background information were observable.
The vignettes were used with the intention to simulate conditions in which (1) clinicians may view the clients through various screen sizes and videoconferencing programs (e.g. Skype) or the client’s webcam placement on the screen or table (including its angle) may not generate the best quality visual information from the clients or (2) users do not have access to a high-speed internet connection, or videoconferencing was conducted via lower resolution digital webcams.
Procedure
Participants of experiment 1 were invited to take part in the experiment via flyers placed on the Monash University Gippsland campus Student Union (MUGSU) and the Psychology Department’s bulletin boards. Written consent was obtained prior to the experimental session, after reading the explanatory statement and being provided with a brief description of the study. Participants then completed a demographics survey.
Pre-experiment questionnaires assessed each participant’s level of emotional awareness (EAQ) and their emotional state (PANAS) prior to the intervention. Participants then acted as cybertherapists in a 90-min psychotherapeutic-like session. After the intervention, participants completed the PANAS and EAQ to assess their post-experiment emotional awareness and mood.
Experiment 2 was advertised in the form of a web announcement after receiving ethics approval from the Monash University Human Research Ethics Committee (MUHREC). The call for participation was posted on the university website and Facebook pages and in a Psychotherapy and Counselling Federation of Australia’s (PACFA) online newsletter. The advertisement was also emailed to some research groups and individuals whose contact details were available on the Australian Counselling Association (ACA) and Anxiety and Depression Association of America (ADAA) websites.
Potential participants were directed to the online survey where they read the Explanatory Statement and Consent Form prior to participating. To participate, they needed to click an ‘I agree’ button. Participants were then asked to fill out the Assessing Emotions Scale. They then watched one of the two clips (the order of which were counterbalanced) and filled out the EiC scale and the DMQ. Participants then watched the other clip and filled out these two surveys again. After completing the surveys for the second time, the participants were thanked for their time and the experiment was ended. The experiment took approximately 30 min per participant to complete.
Results
Experiment 1
The results are collapsed across modes of delivery (i.e. simulated telephone and Skype) because it was aimed to assess the influence of CMP on emotional awareness, and thus, type of CMP was not of particular interest. Therefore, the technologies employed were not compared with each other.
Table 2 provides descriptive statistics for the subscales of emotional awareness. As can be seen in Table 2, attending to another’s emotions was rated the highest by participants, while bodily awareness of emotions was rated the lowest.
Table 2.
The subscales of the Emotional Awareness Questionnaire (EAQ)
| Subclasses | Scale | Mean | Std. error | 95% confidence interval | |
|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||
| Differentiating emotions | Pre | 1.48 | .08 | 1.33 | 1.63 |
| Post | 1.56 | .08 | 1.40 | 1.71 | |
| Verbal sharing of emotions | Pre | 1.41 | .11 | 1.20 | 1.63 |
| Post | 1.44 | .11 | 1.23 | 1.66 | |
| Not hiding emotions | Pre | 1.06 | .11 | .83 | 1.29 |
| Post | 1.05 | .13 | .79 | 1.31 | |
| Bodily awareness of emotions | Pre | .67 | .09 | .49 | .85 |
| Post | .63 | .12 | .40 | .87 | |
| Attending to others emotions | Pre | 1.63 | .09 | 1.45 | 1.81 |
| Post | 1.66 | .09 | 1.45 | 1.83 | |
| Analysis of own emotions | Pre | 1.60 | .09 | 1.42 | 1.77 |
| Post | 1.65 | .12 | 1.41 | 1.89 | |
First Hypothesis (H1)
Factor Analysis of Emotional Awareness Questionnaire
The test sought to determine whether or not technology-based interventions, in general, impede emotional awareness in clinicians. It was hypothesised that a cybertherapists’ level of emotional awareness would be diminished during CMP sessions due to the limits associated with virtual communication (e.g. reduced access to visual cues). To examine this hypothesis, a mixed-model ANOVA was conducted to assess any difference in the pre- and post-intervention EAQ scores of the same subscale (e.g. differentiate emotions pre- and post-intervention). The results were corrected for multiple comparisons by using Bonferroni adjustments. The effect of the same subscales were not statistically significant (F(5, 100) = .39, p = .85, η2 = 0.02. This finding suggests that the CMP session did not reduce the participants’ emotional awareness.
It was also assumed that a background in psychology was associated with having higher levels of emotional awareness. A mixed-model ANOVA was used to test this assumption. EAQ subscales were used as the dependent variables and ‘expertise in psychology’ was used as the between-subjects factor. Results revealed no significant differences between scores on the EAQ scales of participants with and without training in psychology, F(5, 100) = 1.12, p = .36, partial η2 = 0.06. This finding suggests that training in psychology does not modify one’s emotional awareness. Interestingly, while people without a background in psychology rated analysing their own emotions the highest, those with psychology backgrounds rated differentiating emotions the highest (see Fig. 2).
Fig. 2.

The impact of psychological training on emotional awareness
Despite achieving a result contrary to the hypothesis, the relationships between certain subscale scores were also of interest in the current study. The subscales describe how people engage with feelings and emotional communication during CMP. As such, a regression analysis was run and indicated that the pre-intervention scores of ‘attending to own emotions’ explained a significant proportion of the variance in post-intervention ‘attending to others emotions’ scores, F(1, 21) = 24.33, p < .001, R2 = .54, R2Adjusted = .53. The ability to attend to others’ emotions was predicted by a participant’s ability to attend to their own emotions, β = .75, t(58) = 4.94, p < .001. Further, pre-intervention ‘verbal sharing of emotions’ and post-intervention ‘attending to others emotion’ were correlated, F(1, 21) = 6.87, p < .01, R2 = .26, R2Adjusted = .21. Participant’s willingness to verbally share their emotions predicted an increase in their ability to attend to other’s emotions, β = .51, t(58) = 2.62, p < .01.
Mood in Relation to Emotional Awareness
The second part of the experiment sought to assess the emotional states of participants. Table 3 presents descriptive statistics relating to the Positive and Negative Affect Scale (PANAS) [93].
Table 3.
Scores on the Positive and Negative Affect Schedule (PANAS)
| Number | Mean | Median | Range | Min | Max | SD | |
|---|---|---|---|---|---|---|---|
| Pre-test | |||||||
| Positive | 22 | 31.28 | 31.50 | 23 | 20 | 43 | 5.91 |
| Negative | 22 | 13.55 | 11.5 | 18 | 10 | 28 | 4.87 |
| Post-test | |||||||
| Positive | 22 | 29.87 | 31 | 25 | 16 | 41 | 7.20 |
| Negative | 22 | 12.73 | 11 | 12 | 10 | 22 | 3.72 |
Due to problems associated with virtual communication (e.g. lack of information on which to base decisions), it was hypothesised that technology would impact participants’ moods during the trial. To test any changes in participants’ moods, data were assessed via a mixed-model ANOVA. No significant main effects were found between the pre-test and post-test PANAS scores for positive, F(1, 20) = 2.78, p = .12, η2 = 0.13, or for pre- and post-negative scores, F(1, 20) = 0.80, p = .39, η2 = 0.04 (see Fig. 3). Therefore, the hypothesis that a technology-based session may reduce the mood of the participants was rejected.
Fig. 3.

Self-rated mood during technology-based communication
It was also assumed that if clinicians began the session in a bad mood it would impact their emotional awareness and the ability to emotionally engage with their clients. Linear regression analysis was used to test if participants’ pre-test feelings affected their post-test emotional awareness. Regression analysis showed that participants’ who scored their positive mood higher before the trial had higher ‘attend to others emotions’ after the trial, β = .56, t(3.02), p < .007. More importantly, participants’ post-intervention ‘differentiating emotions’ scores were significantly related to their pre-intervention ‘negative mood’ scores, R2 = .37, F(1, 21) = 11.63, p < .003. The analysis showed that participants’ ability to differentiate emotions in others was impeded by a negative pre-intervention mood, β = − .61, t(− 3.41), p < .003.
In conclusion, the mood of participants did not change from pre- to post-CMP-like sessions. However, the participating users’ negative mood seemed to lower their emotional awareness. The results support the view that a more positive mood pre-session may increase a therapist’s ability to express, analyse, and engage with other’s feelings.
Experiment 2
The AES
To assess whether or not emotional awareness influenced the diagnostic ability of participants, their level of emotional intelligence was surveyed using the Assessing Emotions Scale (AES). Table 4 displays the descriptive statistics for the AES.
Table 4.
Descriptive statistics relating to emotional intelligence as measured by the AES
| Category | Min | Max | Mean | SD |
|---|---|---|---|---|
| Participants (N = 60) | ||||
| Perception of emotion | 31 | 50 | 44.05 | 4.85 |
| Managing own emotion | 25 | 45 | 37.90 | 4.74 |
| Managing others emotion | 24 | 40 | 34.37 | 3.50 |
| Utilising emotion | 17 | 30 | 25.45 | 3.03 |
| Total score of emotional intelligence | 108 | 163 | 141.78 | 11.49 |
| Evaluators (N = 2) | ||||
| Perception of emotion | 41 | 45 | 43 | 2.83 |
| Managing own emotion | 34 | 44 | 39 | 7.07 |
| Managing others emotion | 28 | 32 | 30 | 2.83 |
| Utilising emotion | 25 | 27 | 26 | 1.41 |
| Total score of emotional intelligence | 132 | 144 | 138 | 8.49 |
A MANOVA was used to test whether emotional intelligence differed across the participants and evaluator groups. The results were not significantly different (see Table 5).
Table 5.
Pairwise comparisons of emotional intelligence
| Dependent variable | (I) group | (J) group | Mean difference (I − J) | SE | Sig.a | 95% confidence interval for differencea | |
|---|---|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||||
| Perception of emotions | Participants | Evaluators | 1.050 | 3.47 | .77 | − 5.887 | 7.987 |
| Managing own emotions | Participants | Evaluators | − 1.100 | 3.03 | .72 | − 7.159 | 4.959 |
| Managing others emotions | Participants | Evaluators | 4.367 | 2.51 | .09 | − 0.648 | 9.382 |
| Utilising emotions | Participants | Evaluators | − 0.550 | 2.16 | .80 | − 4.867 | 3.767 |
| Total emotional intelligence | Participants | Evaluators | 3.767 | 8.23 | .65 | − 12.688 | 20.222 |
Based on estimated marginal means
aAdjustment for multiple comparisons: Bonferroni
The EiC
The ability to perceive emotions in others is assumed to be a key element in conducting effective CMP. As such, the ability to determine the valence, intensity, potency, and activation of emotional communication were assessed. Table 6 shows descriptive statistics associated with the two video-based stimuli.
Table 6.
Descriptive statistics relating to perceived emotionality in a videoconferencing scenario
| Valence | Intensity | Potency | Activation | ||||
|---|---|---|---|---|---|---|---|
| Stimulus A | Participants (N = 60) | Mean | 72.05 | 64.40 | 60.70 | 53.19 | |
| SD | 19.40 | 21.65 | 24.83 | 27.70 | |||
| CI | Lower bound | 67.04 | 58.81 | 54.29 | 46.03 | ||
| Upper bound | 77.07 | 69.10 | 67.12 | 60.34 | |||
| Evaluators (N = 2) | Mean | 77.00 | 75.00 | 60.00 | 50.00 | ||
| SD | 1.41 | 9.90 | 15.56 | 21.22 | |||
| CI | Lower bound | 64.30 | − 13.94 | − 79.77 | − 140.60 | ||
| Upper bound | 89.71 | 163.95 | 199.77 | 240.60 | |||
| Stimulus B | Participants (N = 60) | Mean | 89.80 | 88.80 | 74.77 | 81.94 | |
| SD | 12.06 | 11.52 | 24.47 | 19.47 | |||
| CI | Lower bound | 86.69 | 85.83 | 68.45 | 76.91 | ||
| Upper bound | 92.92 | 91.78 | 81.09 | 86.97 | |||
| Evaluators (N = 2) | Mean | 93.00 | 93.00 | 79.50 | 93.00 | ||
| SD | 2.83 | 2.83 | 7.78 | 11.32 | |||
| CI | Lower bound | 67.59 | 67.59 | 9.62 | − 18.65 | ||
| Upper bound | 118.42 | 118.42 | 149.39 | 184.65 | |||
CI 95% confidence interval
The results also showed that the perceptions of the participants were analogous to those of the evaluators (p > .1; see Fig. 4).
Fig. 4.
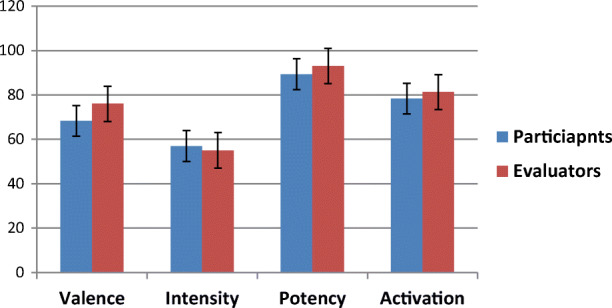
Perception of emotionality between the stimuli and the groups of people
A repeated-measures ANOVA was employed to test the ability of participants to perceive elements of emotionality in others during a therapeutic-like session. The results showed that the perceived level of emotionality was significantly different between the two stimuli, F[1, 59] = 107.10, p < .001, partial η2 = 0.65. This result suggests that a lower level of emotionality was perceived in Stimulus A (M = 62.00, CI [58.13, 67.05]) relative to stimulus B (M = 83.83, CI [80.54, 87.12]). When the individual emotional subscales were considered, the same pattern of results persisted (see Fig. 5). Bonferroni-corrected analyses showed that emotional valence scores, which relate to the perceived quality of the speaker’s emotional arousal, were significantly different (p < .001). Specifically, stimulus B was rated as having more emotional valence. There was also a significant difference between the emotional intensity for stimulus A and stimulus B (p < .001). Again, participants perceived the intensity of the communication in stimulus B as being higher than that of stimulus A. Emotional potency scores were also significantly different for the two stimuli (p < .001). The emotional potency of stimulus A was perceived as less than that of stimulus B. Similarly, emotional activation scores were significantly different across scenarios (p < .001), with participants rating stimulus B as having a higher level of emotional activation than stimulus A.
Fig. 5.
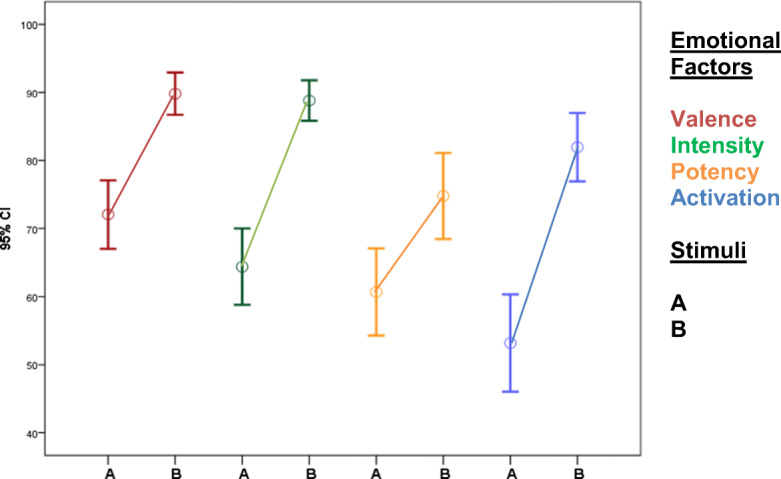
Perception of emotional factors via video-based communication. The graphs draw an error bar of emotional factors scored across the stimuli. The lines in figure provide the expectation that there are overall changes in the trends of emotional factors. According to the lines, the factors are perceived higher in the second stimulus
Second Hypothesis (H2)
The second hypothesis proposed that there would be a relationship between emotional intelligence and the ability of clinicians to perceive emotionality via technology (see Fig. 1). To examine this hypothesis, a regression analysis was conducted. Participants’ total scores for emotional intelligence explained a significant amount of the variance in the ratings of emotionality for stimulus A, F[1, 58] = 11.30, p < .001, R2 = .17, R2Adjusted = .15. This analysis shows that participants’ emotional intelligence is related to their ability to perceive the emotion expressions of others, β = .41, t(59) = 3.37, p < .001. Similarly, the overall emotional intelligence scores explained a significant amount of the variance in the emotionality ratings for stimulus B, F[1, 58] = 2072, p < .001, R2 = .27, R2Adjusted = .25. Participants’ ability to perceive emotions was, again, related to their level of emotional intelligence, β = .52, t(59) = 4.56, p < .001.
The subscales of emotional intelligence were examined to see if they predicted the total emotionality scores in the two stimuli. According to Table 7, all subscales of emotional intelligence had significant roles in the ability to perceive emotionality in stimulus B. However, it seems as though the level of emotionality in stimulus A was related to only the perception of emotion subscale. This suggests that when more emotions are expressed and they are expressed with greater intensity, one’s ability to (1) perceive emotions, (2) manage emotions, and (3) utilise emotions are important in perceiving emotions in others. However, when emotions are displayed less frequently and/or with less intensity, only one’s ability to perceive emotions is relevant.
Table 7.
Estimated emotionality of video-based communication by means of AES components
| Model | Unstandardised coefficients | Standardised coefficients | t | Sig. | |
|---|---|---|---|---|---|
| B | Std. Error | Beta | |||
| Stimulus A | |||||
| Perception of emotion | 5.11 | 1.75 | .36 | 2.93 | .005 |
| Managing own emotions | 4.62 | 2.10 | .28 | 2.21 | .03* |
| Managing others emotions | 5.15 | 2.51 | .26 | 2.06 | .04* |
| Utilising emotions | 6.33 | 2.89 | .28 | 2.20 | .03* |
| Stimulus B | |||||
| Perception of emotion | 3.40 | 1.31 | .33 | 2.60 | .01 |
| Managing own emotions | 4.39 | 1.51 | .36 | 2.91 | .005 |
| Managing others emotions | 7.98 | 1.61 | .55 | 4.98 | .001 |
| Utilising emotions | 5.18 | 2.11 | .31 | 2.45 | .01 |
*These values do not reach significance when adjusted for multiple comparisons
Accordingly, the results suggest that a therapist’s level of emotional intelligence can influence their ability to perceive emotional content in video-based communication.
Third Hypothesis (H3)
The accuracy of the participants’ decision-making was also considered in experiment 2. The third hypothesis predicted that the reduced quality and quantity of emotional information available via video-based communication would impact the diagnostic ability of participants (see Fig. 1). To test this assumption, non-parametric tests were used initially in order to determine the proportion of diagnoses per stimulus. The Mc-Nemar test showed that diagnostic decisions were significantly different in relation to the two stimuli [X2(12, NTotal = 60) = 84.73, p < .001]. That is, participants made different decisions regarding the speaker’s mental health issues in the two stimuli. Chi-square tests were employed to examine which of the choices the participants had selected in each stimulus from the list including ‘no problem’, ‘personal issues but not significant’, ‘significant issue(s) that needs professional help’, ‘minor problem requiring no action’, ‘mild problem but definitely present’, and ‘moderately severe problem’. The chi-square analysis showed that the choice of ‘moderately severe problem’ was selected significantly more often in scenario B (NB = 13, 21.70%) than it was in scenario A (NA = 28, 46.70%) [X2 (1, NTotal = 60) = 4.54, p < .03]. In addition, participants scored ‘a significant mental problem that needs professional psychological help’ differently between stimuli [X2 (1, NTotal = 60) = 10.24, p < .001]. Clinicians were more likely to suggest that the person in stimulus B (NB = 44, 73%) had a significant issue than they were for the person in stimulus A (NA = 28, 46.7%).
It was also deemed important to assess the effect of emotionality on decision-making. Emotionality was computed by integrating the scores of the Emotionality in Cyberspace’s (EiC) subscales (i.e. valence, intensity, potency, and activation). The total score was used to determine if the content of the stimuli had influenced participants’ decision-making. This relationship was tested using a regression analysis the predicted variable (i.e. decision) was dummy coded [34]. Based on the evaluators’ decisions, ‘1’ was set as a reference for ‘significant issue(s) that needs professional help’ and ‘0’ was set for the other options. The results showed that the ‘significant issues’ could be explained by means of the level of emotionality in the first stimulus, F(1, 59) = 7.167, p < .01, R2 = .11, R2Adjusted = .10, as well as in the second stimulus, F(1, 59) = 16.62, p < .001, R2 = .23, R2Adjusted = .21. Also, the results show that this choice (i.e. whether or not a significant issues was present) was better predicted by EiC total score for the second stimulus, β = .48, t(59) = 4.08, p < .001 relative to the first, β = .33, t(59) = 2.67, p < .01 (see Table 8).
Table 8.
Decision-making ability and the perception of emotional factors in video-based communication
| Predicting factors | Unstandardised coefficients | Standardised coefficients | t | Sig. | |
|---|---|---|---|---|---|
| B | Std. error | Beta | |||
| Stimulus A | |||||
| Valence | 0.02 | 0.003 | .43 | 3.60 | .001 |
| Intensity | 0.01 | 0.003 | .39 | 3.20 | .002 |
| Potency | 0.009 | 0.003 | .27 | 2.13 | .03 |
| Activation | 0.001 | 0.002 | − .02 | − 0.122 | .90 |
| Stimulus B | |||||
| Valence | 0.02 | 0.004 | .54 | 4.86 | .001 |
| Intensity | 0.02 | 0.004 | .55 | 5.02 | .001 |
| Potency | 0.005 | 0.002 | .25 | 1.97 | .05 |
| Activation | 0.006 | 0.003 | .26 | 2.06 | .04 |
When participants’ decision was that a ‘significant issue’ was present, there were significant differences in the scores obtained regarding the intensity of the problem. This intensity was different between stimulus A (M = 83, SD = 1.92) and stimulus B (M = 92, SD = 1.52), t(25) = − 5.41, p < .001. This suggests that, even when the problem was thought of as a significant issue, participants rated the issue as being more intense when emotional expressions were also more intense or displayed more frequently. Accordingly, the results suggest that diagnostic procedures can be conducted adequately via video-based communication if a sufficient amount of emotional information is available.
Forth Hypothesis (H4)
The forth hypothesis predicted that clinicians’ emotional intelligence influences their decision-making in relation to a client’s psychological state (see Fig. 1). The relationships between these factors were investigated by comparing participants’ levels of emotional intelligence (as an independent variable) and their diagnostic decisions for each stimulus (as a dependent variable). A regression analysis showed that there was no association between the scores for emotional intelligence and participants’ decisions in relation to stimulus A (p > .1). However, the scores for emotional intelligence and decision-making were significant for stimulus B, F(1, 58) = 5.71, p < .02, R2 = .30, R2Adjusted = .07. The results suggest that decision-making (i.e. whether or not a significant issues was present) is better when emotional intelligence is high, β = .30, t(58) = 2.39, p < .02). This finding was significantly influenced by the AES component ‘managing others’ emotions’, β = .26, t(58) = 2.05, p < .05. These findings suggest that participants recognised and used video-based emotional information when making decisions.
Assessing the Model: Emotional Intelligence in Video-Based Psychotherapy
There is a further, unanswered question regarding the relationship between emotional intelligence and decisions made via video-based communication. It has been claimed that the link between clinicians’ emotional intelligence and their decision-making is influenced by the number, type, and intensity of emotional expressions. A path analysis was therefore the last method employed here to investigate relationships among emotional intelligence, emotionality, and decision-making (see Fig. 1). A structural equation model was used to investigate relationships among emotional intelligence, emotionality, and decision-making. The results showed that the fit indices from the default measurement model fit the data for stimulus A [X2 = 33.13, df = 25, p > .13], and stimulus B [X2 = 35.64, df = 25, p > .05]; in a good model, the value of chi-square should not be significant, i.e. p > .05 [37]. Meanwhile, absolute fit and incremental fit indices were also conducted. The non-normed Comparative Fit Index (CFI; [11]), as well as Normed-Fit Index (NFI; [12]), were calculated and showed an acceptable fit for both stimuli (stimulus A: CFI = .94 and NFI = .85; stimulus B: CFI = .95 and NFI = .87).1 Root Mean square error of approximation (RMSEA) was another index used to measure the fit with the current model [12, 47]. RMSEA would provide a good model fit with an amount less than or equal to 0.05, or an adequate fit with RMSEA less than or equal to 0.08. The data showed an adequate fit with the current model for both stimuli (stimulus A: RMSEA = .07; stimulus B: RMSEA = .08).
Furthermore, and as indicated in Fig. 6, the findings of the model were in accordance with results presented in previous sections. In particular, for the between-neighbourhood component of the model, standardised coefficients (β) between emotional intelligence of participants and their decision-making were .66 for stimulus A and .14 for stimulus B. This shows that emotional intelligence had the most potent relationship with decision-making in stimulus A. However, the neighbourhood involvement was also calculated for decision-making and emotionality with β = .50 for stimulus A and β = .90 for stimulus B. Further relationships were observed between emotional intelligence and emotionality with β = .48 for stimulus A and β = .65 for stimulus B. With respect to these parameter estimates, the current results indicate that the relationship between emotional intelligence and diagnosis was weakened when emotionality of video communication decreased.
Fig. 6.

Stimulus A: the path analysis for decision-making via videoconferencing. Standardised coefficients are presented. Stimulus B: the path analysis for decision-making via videoconferencing. Standardised coefficients are presented
Discussion
The aim of the current study was to investigate the emotional changes in, and the emotional awareness of, people who engage in psychotherapeutic communication via technology. The results do not support the first hypothesis that stated that people would experience a reduction in emotional awareness after interacting with others via technology. That is, level of emotional awareness did not decline as a result of engaging with simulated emotional communication via technology. The findings, therefore, indicate that the effect of using technology, and emotional content delivered via technology, does not impact on the overall level of emotional awareness in users.
The experiment also revealed some notable issues relating to emotional awareness. In this experiment, ‘bodily awareness of emotions’ (one’s own or that of others) was the EAQ subscale rated the lowest and thus seems to be thought of as contributing the least to overall emotional awareness. This may trigger a warning to psychotherapists who use technology. Firstly, lower levels of awareness about body reactions, which play a considerable role in emotional cognition, may limit the amount of meaningful information available for psychotherapy [19]. For example, research implies that awareness of a client’s bodily reactions enables the psychotherapist to perceive the client’s emotional states [66]. Secondly, the self-awareness about physical presence of the psychotherapist is argued to provide a receptive device for emotional information in that such awareness assists processing an effective interaction with clients’ reactions [27]. While these ideas have been considered in face-to-face settings, the present data have allowed endorsement of similar hypotheses for CMP sessions, which more plausibly suggests that if bodily awareness is involved in emotional awareness it may limit a precise computer-mediated psychotherapy.
The results indicate further that, under computer-mediated condition, therapists are capable of attending to their own emotions. Specifically, it was found that analysing more of one’s own emotions contributes to an ability to perceive emotions in others. Consistent with other studies [38, 60], these findings suggest that cybertherapists are capable of analysing and managing emotional engagement with clients via technology. This, in turn, suggests that therapists who are better at analysing their own emotions have an increased chance of improving their emotional relationships with clients [40, 73, 87].
In the first experiment, the mood of users was also investigated. It was assumed that the use of technology in dealing with a person’s intense emotional communication would lower the participants’ mood. Results showed that mood levels did not change drastically from pre- to post-intervention. There were only slight decreases in the positive and a slight increase in the negative mood scores after the session. This finding suggests that CMP did not impact the mood of the participants.
The experiment was also designed to assess the relationship between mood and emotional awareness. Some subscales of emotional awareness showed positive relationships with the self-rated mood of the participants. Based on the regression analysis, a positive mood was related to an increase in participants’ ability to share emotions with others and was associated with their ability to differentiate a client’s emotions. This finding is consistent with those from other studies. For example, Villanueva et al. [91] studied emotional awareness in face-to-face settings that they thought would have an impact on, or are influenced by, children’s moods. Their results showed that a positive mood can improve a child’s emotional awareness by increasing their ability to share, differentiate, and analyse emotions. It is suggested that the more cybertherapists are aware of their own moods, the more likely they are to be able to understand, and differentiate between, their clients’ emotions. This claim is consistent with previous results from face-to-face therapy research. According to the study by Gurman [31], psychotherapists with strong and positive states of mind understand their clients’ emotional experiences without misrepresentations and they also become more influential in their therapy.
Experiment 2 of the paper investigated cybertherapists’ emotional intelligence during CMP sessions. The Emotional Intelligence Scale [78] showed that participants rated their abilities to manage, perceive, and utilise emotions as being satisfactory. Furthermore, participants rated themselves as being reasonably capable in discerning emotions in themselves and others; they scored emotional perception the highest among the other components of emotional intelligence.
Participants also demonstrated good understanding of emotionality in a video-based stimulus. Significant differences were found in the participants’ experiences with the emotional elements of communication. Specifically, the valence and intensity of emotional expressions appeared to aid participants’ ability to perceive emotions via videoconferencing. Furthermore, similarity was found between the participants’ and the evaluators’ experiences of the emotional content of the video-based communication. These findings support those of others who suggest that CMC users do not differ in their abilities to detect emotions in computer-mediated environments [33].
Other three hypotheses in the study supposed a possible relationship between emotional intelligence, emotional perception, and decision-making. The second hypothesis proposed that emotional intelligence has a relationship with the ability to perceive emotions. This hypothesis was supported. The results demonstrated that the components of emotional intelligence (i.e. perceiving, managing, and utilising emotions) predicted ability to perceive emotions.
The third hypothesis focused on the relationship between the ability to perceive emotions in a video-based setting and the diagnostic ability of therapists. The accuracy of decisions increased when appropriate and adequate emotional information was transmitted. More specifically, the analysis revealed that when the amount and intensity of emotional information increased, as in stimulus B, participants identified the client’s emotions more accurately and better judged the severity of his mental condition. In other words, their decisions were sensitive to the content of communication. The findings are consistent with Kaplowitz et al. [42] who demonstrated that therapists can judge clients’ interpersonal problems more accurately when they integrate large amounts of psychological-emotional information [26, 84]. However, it has been demonstrated that clinicians who experience different clients and several clinical settings will certainly have higher skills in recognising emotional states, symptom assessment and diagnosing various mental disorders [1]. The study did not demonstrate that the experience in remote mental care enclosed further the therapeutic skills of participants. All participants exhibited as reliable degree of emotional perception and decision-making compared with the qualified panellists via video-based communication.
Consistent with the desire in face-to-face settings to characterise psychotherapists’ need for conscious examination [44, 48]. The forth hypothesis supposed that a relationship exists between emotional intelligence and the decision-making abilities of cybertherapists. The experiment revealed a significant relationship between the emotional intelligence and decision-making of participants. Judgments about the psychological status of the patient did vary, which seemed to be largely due to the different levels of the participants’ emotional intelligence. The experiment confirmed earlier work that showed that emotional intelligence has a positive influence on decision-making [54, 55]. The experiment also demonstrated that decision-making via technology is related to the skill of managing others’ emotions. The relationship between emotions and diagnostic ability has been reported by Kaplowitz et al. [42] in face-to-face clinical trials. They showed that managing client’s emotions (i.e. affect regulation skills and alleviating symptoms) was a component of emotional intelligence that improved therapeutic outcomes. The findings of the current study support this view.
Ultimately, cybertherapists who can perceive emotions well, manage their clients’ emotional states, and make effective therapeutic decisions, should be able to overcome any limitations associated with computer-mediated environments. This appears to be consistent with other literature [68, 71] in that emotional intelligence has been shown to positively influence outcomes in face-to-face psychotherapy. The experiment also supports prior research that suggests that emotional intelligence has a positive effect on online interactions [67].
Limitations and Future Steps
Although experiment 1 has yielded some interesting findings, its design is not without flaws. First, the number and type of participants was limited. It would thus be advantageous to be able to access more psychotherapists and use these people as participants. Second, it would have been more authentic to employ stimuli from real-life cases but, given ethical constraints, this was not possible. Third, the effect of ‘mode of delivery’ was not considered in this experiment. The experiment was quite demanding of participants and it was deemed necessary to ignore mode of delivery. Future research projects could establish if different modes of CMC affect mood and emotional awareness. Fourth, the present study used commonly applied self-reporting scales in the measurement of emotional awareness and mood. Emotional awareness, however, is a cognitive ability that can be assessed using other, more objective, measures; the lack of financial and laboratory resources impeded employing such measures. Psychophysiological measurements (e.g. electroencephalogram (EEG) or Galvanic Skin Conductance) could be used, for example. With these tools the biophysical level of awareness can be measured while cybertherapists engage with a client in a range of therapeutic conditions. An understanding of the bio-physiology of their interactions can help practitioners qualify and control their engagement level, their emotional understanding of the interaction, and their perception of the emotion during CMP sessions [85].
The focus of these experiments was on gaining insight into emotional intelligence and its influence on interactions when video-based tools are adopted. Here, the interaction was one-way, but future studies should investigate emotional awareness and decision-making when parties communicate with each other. Two-way interactions would provide a more realistic assessment of the influence of emotional awareness on diagnostic decisions. However, logistical limitations prohibited an assessment of two-way interactions here. Relatedly, the mode of delivery is a further concern. An assessment of emotional awareness and decision-making abilities in audio- and text-based modes of delivery is needed. For this study, an intake interview was employed. This was required to conform to ethical restrictions regarding hiring patients and as a means of overcoming the lack of funding available for the research. Although this contributes to knowledge in this area, there is a need to use clinical cases and assess the role of emotional intelligence in those situations. Lastly, there is a need to assess diagnostic accuracy for specific disorders when therapy is conducted in video-based settings.
Summary
The first experiment of the paper investigated whether emotional awareness is influenced by CMC. The experiment found that participants are capable of being emotionally aware in a CMP session. The results demonstrate that participants can perform a good proportion of understating, attending, and analysing their emotions and clients via technology-based communication before and after the experience of a session. Further, the experiment confirmed that the participant mood did not change drastically between pre- and post-intervention. However, a negative mood pre-intervention impacted participants’ awareness of, and ability to recognise, emotions. As such, therapists who use technology when engaging with clients should be further cautious about their negative mood prior to therapy sessions.
The findings obtained in the second experiment of the paper help explain the relationship between emotional intelligence and diagnosis when using video-based communication. The constructs used in the experiment provide a useful framework for predicting decision-making and a cybertherapist’s ability to detect and engage with emotional states in CMP. It is, therefore, claimed that emotional intelligence can quantitatively and qualitatively enhance the way cybertherapists perceive emotional communication and use this information to optimise decision-making in relation to appropriate mental health support. In essence, the findings contribute to the field of remote therapy suggesting emotional intelligence as a key cognitive factor in diagnosis.
Compliance with Ethical Standards
Conflict of Interest
The authors declare that they have no conflict of interest.
Footnotes
CFI and NFI values close to 1 indicate a very good fit.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Aboraya A, Rankin E, France C, El-Missiry A, John C. The reliability of psychiatric diagnosis revisited: the clinician’s guide to improve the reliability of psychiatric diagnosis. Psychiatry (Edgmont) 2006;3(1):41–50. [PMC free article] [PubMed] [Google Scholar]
- 2.Alvandi EO (2017) Emotional agency in telecounselling: a cognitive model. Figshare. Retrieved 3 Feb 2019 from https://monash.figshare.com/articles/Emotional_Agency_in_Telecounselling_A_Cognitive_Model/4644799/1
- 3.Alvandi EO (2019) Cybertherapogy: a conceptual architecting of presence for counselling via technology. International Journal of Psychology and Educational Studies 6(1):30–45. Retrieved 3 Feb 2019 from http://www.ijpes.com/frontend//articles/pdf/v6i1/v06-i01-04pdf.pdf
- 4.Alvandi EO, Van Doorn G, Symmons M (2017) Emotionality in computer-mediated environments: analyzing the emotional content of psychotherapeutic communication. The Journal of Interaction Science (JoIS) 5:34–34
- 5.Annoni M. Reasons and emotions. In: Boniolo G, Sanchini V, editors. Counselling and medical decision-making in the era of personalised medicine. Heidelberg: Springer International Publishing; 2016. pp. 39–48. [Google Scholar]
- 6.Arbuthnott KD, Arbuthnott DW, Thompson VA. The mind in therapy: cognitive science for practice. Mahwah: Erlbaum; 2006. [Google Scholar]
- 7.Arnetz BB (1997). Technological stress: psychophysiological aspects of working with modern information technology. Scand J Work Environ Health, 97–103 [PubMed]
- 8.Arntz A, de Groot C, Kindt M. Emotional memory is perceptual. J Behav Ther Exp Psychiatry. 2005;36(1):19–34. doi: 10.1016/j.jbtep.2004.11.003. [DOI] [PubMed] [Google Scholar]
- 9.Barrett LF. Valence is a basic building block of emotional life. J Res Pers. 2006;40(1):35–55. doi: 10.1016/j.jrp.2005.08.006. [DOI] [Google Scholar]
- 10.Beirne M (2014) The role of emotional awareness in couple relationships. Éisteach 14(4):14–17. Retrieved 13 Aug 2018 from http://www.marybeirne.info/upload/The%20Role%20of%20Emotional%20Awaresess%20in%20Couple%20Relationships.pdf.
- 11.Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238–246. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- 12.Bentler PM, Bonett DG. Significance tests and goodness of fit in the analysis of covariance structures. Psychol Bull. 1980;88(3):588–606. doi: 10.1037/0033-2909.88.3.588. [DOI] [Google Scholar]
- 13.Brosch T, Scherer KR, Grandjean D, Sander D. The impact of emotion on perception, attention, memory, and decision-making. Swiss Med Wkly. 2013;143:w13786. doi: 10.4414/smw.2013.13786. [DOI] [PubMed] [Google Scholar]
- 14.Camodeca M, Rieffe C. Validation of the Italian Emotion Awareness Questionnaire for children and adolescents. Eur J Dev Psychol. 2013;10(3):402–409. doi: 10.1080/17405629.2012.694609. [DOI] [Google Scholar]
- 15.Carvalho HWD, Andreoli SB, Lara DR, Patrick CJ, Quintana MI, Bressan RA, et al. Structural validity and reliability of the Positive and Negative Affect Schedule (PANAS): evidence from a large Brazilian community sample. Rev Bras Psiquiatr. 2013;35(2):169–172. doi: 10.1590/1516-4446-2012-0957. [DOI] [PubMed] [Google Scholar]
- 16.Coetzee M, Schreuder D (2011) The relation between career anchors, emotional intelligence and employability satisfaction among workers in the service industry. Southern African Business Review 15(3):76–97
- 17.Colman AM. A dictionary of psychology (Fourth ed.) Oxford: Oxford University Press; 2015. [Google Scholar]
- 18.Crawford JR, Henry JD. The Positive and Negative Affect Schedule (PANAS): construct validity, measurement properties and normative data in a large non-clinical sample. Br J Clin Psychol. 2004;43(3):245–265. doi: 10.1348/0144665031752934. [DOI] [PubMed] [Google Scholar]
- 19.Damasio AR. The feeling of what happens: body, emotion and the making of consciousness. New York: Harcourt Brace; 1999. [Google Scholar]
- 20.Ekberg S, Shaw AR, Kessler DS, Malpass A, Barnes RK. Orienting to emotion in computer-mediated cognitive behavioral therapy. Res Lang Soc Interact. 2016;49(4):310–324. doi: 10.1080/08351813.2016.1199085. [DOI] [Google Scholar]
- 21.Ekman P, Friesen WV (1978) Facial action coding system. Palo Alto (CA): Consulting Psychologists Press
- 22.Ekman P, Friesen WV (2003) Unmasking the face: a guide to recognizing emotions from facial expressions. Cambridge, MA: MALOR BOOKS
- 23.Ekman P, Rosenberg EL. What the face reveals: basic and applied studies of spontaneous expression using the Facial Action Coding System (FACS) Oxford: Oxford University Press; 1997. [Google Scholar]
- 24.Elkind SN. Resolving impasses in therapeutic relationships. New York: Guilford Press; 1992. [DOI] [PubMed] [Google Scholar]
- 25.Frijda NH. The emotions: studies in emotion and social interaction. Paris: Maison de Sciences de l’Homme; 1986. [Google Scholar]
- 26.Frueh BC, Monnier J, Grubaugh AL, Elhai JD, Yim E, Knapp R. Therapist adherence and competence with manualized cognitive-behavioral therapy for PTSD delivered via videoconferencing technology. Behav Modif. 2007;31(6):856–866. doi: 10.1177/0145445507302125. [DOI] [PubMed] [Google Scholar]
- 27.Geller S, Greenberg L, Watson JC. Therapist and client perceptions of therapeutic presence: the development of a measure. Psychother Res. 2010;20(5):599–610. doi: 10.1080/10503307.2010.495957. [DOI] [PubMed] [Google Scholar]
- 28.Greenberg L. Emotion-focused therapy. Clinical Psychology & Psychotherapy. 2004;11(1):3–16. doi: 10.1002/cpp.388. [DOI] [PubMed] [Google Scholar]
- 29.Greenberg LS, Paivio SC. Working with emotions in psychotherapy. USA: Guilford Press; 2003. [Google Scholar]
- 30.Greenberg L, Pascual-Leone A. Emotion in psychotherapy: a practice-friendly research review. J Clin Psychol. 2006;62(5):611–630. doi: 10.1002/jclp.20252. [DOI] [PubMed] [Google Scholar]
- 31.Gurman AS. Therapists’ mood patterns and therapeutic facilitativeness. J Couns Psychol. 1972;19(2):169–170. doi: 10.1037/h0032407. [DOI] [Google Scholar]
- 32.Gurman AS. Effects of therapist and patient mood on the therapeutic functioning of high-and low-facilitative therapists. J Consult Clin Psychol. 1973;40(1):48–58. doi: 10.1037/h0034032. [DOI] [PubMed] [Google Scholar]
- 33.Hancock JT, Gee K, Ciaccio K, Lin JM-H (2008) I’m sad you’re sad: emotional contagion in CMC. In proceedings of the 2008 ACM conference on Computer supported cooperative work, 295-298. 10.1145/1460563.1460611
- 34.Hardy MA. Regression with dummy variables (quantitative applications in the social sciences) London: AGE Publications India Pvt.Ltd.; 1993. [Google Scholar]
- 35.Hauke G, DallOcchio M (2013) Emotional activation therapy (EAT): intense work with different emotions in a cognitive behavioral setting. European Psychotherapy 1(11):5–29
- 36.Holman MA, Porter SG, Pawlina W, Juskewitch JE, Lachman N. Does emotional intelligence change during medical school gross anatomy course? Correlations with students’ performance and team cohesion. Anat Sci Educ. 2015;9:143–149. doi: 10.1002/ase.1541. [DOI] [PubMed] [Google Scholar]
- 37.Hooper D, Coughlan J, Mullen MR (2008) Structural equation modeling: Guidelines for determining model fit. Electronic Journal of Business Research Methods (EJBRM) 6(1):53–60
- 38.Hughes P, Kerr I. Transference and countertransference in communication between doctor and patient. Adv Psychiatr Treat. 2000;6:57–64. doi: 10.1192/apt.6.1.57. [DOI] [Google Scholar]
- 39.Hutter RV, Oldenhof-Veldman T, Oudejans RR. What trainee sport psychologists want to learn in supervision. Psychol Sport Exerc. 2015;16:101–109. doi: 10.1016/j.psychsport.2014.08.003. [DOI] [Google Scholar]
- 40.Janzen JI, Fitzpatrick MR, Drapeau M, Blake E. The relationship between client attachment and therapist interventions in client-nominated relationship-building incidents/La relation entre l'attachement du client et les interventions thárapeutiques dans les incidents critiques au développement du rapport thérapeutique selon le client. Can J Couns Psychother. 2010;44(4):363–382. [Google Scholar]
- 41.Jennings PA, Greenberg MT. The prosocial classroom: teacher social and emotional competence in relation to student and classroom outcomes. Rev Educ Res. 2009;79(1):491–525. doi: 10.3102/0034654308325693. [DOI] [Google Scholar]
- 42.Kaplowitz MJ, Safran JD, Muran CJ. Impact of therapist emotional intelligence on psychotherapy. J Nerv Ment Dis. 2011;199(2):74–84. doi: 10.1097/NMD.0b013e3182083efb. [DOI] [PubMed] [Google Scholar]
- 43.Kaspi SP, McNally RJ, Amir N. Cognitive processing of emotional information in posttraumatic stress disorder. Cogn Ther Res. 1995;19(4):433–444. doi: 10.1007/BF02230410. [DOI] [Google Scholar]
- 44.Kienle GS, Kiene H. Clinical judgement and the medical profession. J Eval Clin Pract. 2011;17(4):621–627. doi: 10.1111/j.1365-2753.2010.01560.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kim YJ, Park EH, Jon DI, Jung MH, Hong N. Does emotional intelligence fluctuate within clinical depressive condition? Psychiatry investigation. 2017;14(5):532–538. doi: 10.4306/pi.2017.14.5.532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Kirby R. Emotional intelligence and medicine. Trends in Urology & Men's Health. 2016;7(3):30–31. doi: 10.1002/tre.524. [DOI] [Google Scholar]
- 47.Kline RB (2005) Principles and practice of structural equation modeling. 2005. New York: Guilford
- 48.Kraemer HC. The reliability of clinical diagnoses: state of the art. Annu Rev Clin Psychol. 2014;10:111–130. doi: 10.1146/annurev-clinpsy-032813-153739. [DOI] [PubMed] [Google Scholar]
- 49.Lahaye M, Luminet O, Van Broeck N, Bodart E, Mikolajczak M. Psychometric properties of the emotion awareness questionnaire for children in a French-speaking population. J Pers Assess. 2010;92(4):317–326. doi: 10.1080/00223891.2010.482003. [DOI] [PubMed] [Google Scholar]
- 50.Lahaye M, Mikolajczak M, Rieffe C, Villanueva L, Van Broeck N, Bodart E, Luminet O. Cross-validation of the Emotion Awareness Questionnaire for children in three populations. J Psychoeduc Assess. 2011;29(5):418–427. doi: 10.1177/0734282910390013. [DOI] [Google Scholar]
- 51.Lane RD, Schwartz GE. Levels of emotional awareness: implications for psychotherapeutic integration. J Psychother Integr. 1992;2(1):1–8. doi: 10.1037/h0101238. [DOI] [Google Scholar]
- 52.Lane RD, Quinlan DM, Schwartz GE, Walker PA, Zeitlin SB. The Levels of Emotional Awareness Scale: a cognitive-developmental measure of emotion. J Pers Assess. 1990;55(1–2):124–134. doi: 10.1080/00223891.1990.9674052. [DOI] [PubMed] [Google Scholar]
- 53.Lane RD, Reiman EM, Axelrod B, Yun L-S, Holmes A, Schwartz GE. Neural correlates of levels of emotional awareness: evidence of an interaction between emotion and attention in the anterior cingulate cortex. J Cogn Neurosci. 1998;10(4):525–535. doi: 10.1162/089892998562924. [DOI] [PubMed] [Google Scholar]
- 54.Lerner JS, Li Y, Valdesolo P, Kassam KS. Emotion and decision making. Annu Rev Psychol. 2015;66:799–823. doi: 10.1146/annurev-psych-010213-115043. [DOI] [PubMed] [Google Scholar]
- 55.Loewenstein G, Lerner JS. The role of affect in decision making. In: Davidson R, Scherer K, Goldsmith H, editors. Handbook of affective science. New York: Oxford University Press; 2003. pp. 619–642. [Google Scholar]
- 56.Machado PPP, Beutler LE, Greenberg L. Emotion recognition in psychotherapy: impact of therapist level of experience and emotional awareness. J Clin Psychol. 1999;55:39–57. doi: 10.1002/(SICI)1097-4679(199901)55:1<39::AID-JCLP4>3.0.CO2-V. [DOI] [PubMed] [Google Scholar]
- 57.Manjrekar E, Berenbaum H, Bhayani N. Investigating the moderating role of emotional awareness in the association between urgency and binge eating. Eat Behav. 2015;17:99–102. doi: 10.1016/j.eatbeh.2015.01.010. [DOI] [PubMed] [Google Scholar]
- 58.Manstead AS, Lea M, Goh J. Facing the future: emotion communication and the presence of others in the age of video-mediated communication. In: Kappas A, Kramer N, editors. Face-to-face communication over the internet: issues, research, challenges. New York: Cambridge University Press; 2011. pp. 144–175. [Google Scholar]
- 59.Marcum JA. The role of emotions in clinical reasoning and decision making. J Med Philos. 2013;38(5):501–519. doi: 10.1093/jmp/jht040. [DOI] [PubMed] [Google Scholar]
- 60.Markin RD, McCarthy KS, Barber JP. Transference, countertransference, emotional expression, and session quality over the course of supportive expressive therapy: the raters’ perspective. Psychother Res. 2013;23(2):152–168. doi: 10.1080/10503307.2012.747013. [DOI] [PubMed] [Google Scholar]
- 61.Matsumoto D, Ekman P. Facial expression analysis. Scholarpedia. 2008;3(5):4237. doi: 10.4249/scholarpedia.4237. [DOI] [Google Scholar]
- 62.Najavits LM. Researching therapist emotions and countertransference. Cogn Behav Pract. 2000;7(3):322–328. doi: 10.1016/S1077-7229(00)80090-5. [DOI] [Google Scholar]
- 63.Nightingale S, Spiby H, Sheen K, Slade P. The impact of emotional intelligence in health care professionals on caring behaviour towards patients in clinical and long-term care settings: findings from an integrative review. Int J Nurs Stud. 2018;80:106–117. doi: 10.1016/j.ijnurstu.2018.01.006. [DOI] [PubMed] [Google Scholar]
- 64.Norcross JC, Lambert MJ (2011) Evidence-based therapy relationships. Psychotherapy relationships that work: evidence-based responsiveness, 2, 3–23
- 65.Norcross JC, Wampold BE. Evidence-based therapy relationships: research conclusions and clinical practices. Psychotherapy. 2011;48(1):98–102. doi: 10.1037/a0022161. [DOI] [PubMed] [Google Scholar]
- 66.Ogden P, Minton K. Sensorimotor psychotherapy: one method for processing traumatic memory. Traumatology. 2000;6(3):149–173. doi: 10.1177/153476560000600302. [DOI] [Google Scholar]
- 67.Oktan V. The predictive relationship between emotion management skills and internet addiction. Soc Behav Personal Int J. 2011;39(10):1425–1430. doi: 10.2224/sbp.2011.39.10.1425. [DOI] [Google Scholar]
- 68.Parveen S, Shafiq M. Emotional intelligence: implications for counseling and psychotherapy. Indian Journal of Positive Psychology. 2014;5(2):209–201. [Google Scholar]
- 69.Picard RW. Affective computing. USA: MIT press Cambridge; 1997. [Google Scholar]
- 70.Poskey M (2006) The importance of emotional intelligence in the workplace. Why it matters more than personality. Retrieved 13 Aug 2018 from http://rosewoodcoaching.com/pdf/ImportanceOfEmotionalIntelligence.pdf
- 71.Rieck T, Callahan JL. Emotional intelligence and psychotherapy outcomes in the training clinic. Training and Education in Professional Psychology. 2013;7(1):42–52. doi: 10.1037/a0031659. [DOI] [Google Scholar]
- 72.Rieffe C, Oosterveld P, Miers AC, Meerum Terwogt M, Ly V. Emotion awareness and internalising symptoms in children and adolescents: the emotion awareness questionnaire revised. Personal Individ Differ. 2008;45(8):756–761. doi: 10.1016/j.paid.2008.08.001. [DOI] [Google Scholar]
- 73.Robbins SB, Jolkovski MP. Managing countertransference feelings: an interactional model using awareness of feeling and theoretical framework. J Couns Psychol. 1987;34(3):276–282. doi: 10.1037/0022-0167.34.3.276. [DOI] [Google Scholar]
- 74.Salovey P, Birnbaum D. Influence of mood on health-relevant cognitions. J Pers Soc Psychol. 1989;57(3):539–551. doi: 10.1037/0022-3514.57.3.539. [DOI] [PubMed] [Google Scholar]
- 75.Salovey P, Mayer JD. Emotional intelligence. Imagin Cogn Pers. 1990;9(3):185–211. doi: 10.2190/DUGG-P24E-52WK-6CDG. [DOI] [Google Scholar]
- 76.Schutte NS, Malouff JM. Emotional intelligence mediates the relationship between mindfulness and subjective well-being. Personal Individ Differ. 2011;50(7):1116–1119. doi: 10.1016/j.paid.2011.01.037. [DOI] [Google Scholar]
- 77.Schutte NS, Malouff JM, Hall LE, Haggerty DJ, Cooper JT, Golden CJ, Dornheim L. Development and validation of a measure of emotional intelligence. Personal Individ Differ. 1998;25(2):167–177. doi: 10.1016/S0191-8869(98)00001-4. [DOI] [Google Scholar]
- 78.Schutte NS, Malouff JM, Bhullar N. The assessing emotions scale. In: Stough C, Saklofske D, Parker J, editors. The assessment of emotional intelligence. New York: Springer; 2009. pp. 119–135. [Google Scholar]
- 79.Schutte NS, Thorsteinsson EB, Hine DW, Foster R, Cauchi A, Binns C. Experiential and rational processing styles, emotional intelligence and wellbeing. Aust J Psychol. 2010;62(1):14–19. doi: 10.1080/00049530903312865. [DOI] [Google Scholar]
- 80.Schütz A, Nizielski S (2012) Emotional intelligence as a factor in mental health. Mental Notes:23–25. Retrieved 13 Aug 2018 from https://www.uni-bamberg.de/fileadmin/uni/fakultaeten/ppp_lehrstuehle/psychologie_4/pressearchiv/Emotional_Intelligence_as_a_Factor_in_Mental_Health.pdf
- 81.Scott-Ladd B, Chan CC. Emotional intelligence and participation in decision-making: strategies for promoting organizational learning and change. Strateg Chang. 2004;13(2):95–105. doi: 10.1002/jsc.668. [DOI] [Google Scholar]
- 82.Seo M-G, Barrett LF. Being emotional during decision making—good or bad? An empirical investigation. Acad Manag J. 2007;50(4):923–940. doi: 10.5465/amj.2007.26279217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Shahid R, Stirling J, Adams W (2016) Assessment of emotional intelligence in pediatric and med-peds residents. J Contemp Med Edu 4(4):153
- 84.Shore JH, Savin D, Orton H, Beals J, Manson SM. Diagnostic reliability of telepsychiatry in American Indian veterans. Am J Psychiatry. 2007;164(1):115–118. doi: 10.1176/ajp.2007.164.1.115. [DOI] [PubMed] [Google Scholar]
- 85.Simons RF, Detenber BH, Roedema TM, Reiss JE. Emotion processing in three systems: the medium and the message. Psychophysiology. 1999;36(5):619–627. doi: 10.1111/1469-8986.3650619. [DOI] [PubMed] [Google Scholar]
- 86.Simson U, Martin K, Schäfer R, Franz M, Janssen P. Changes in alexithymia and emotional awareness during psychotherapeutic inpatient treatment. Psychother Psychosom Med Psychol. 2005;56(9–10):376–382. doi: 10.1055/s-2006-940127. [DOI] [PubMed] [Google Scholar]
- 87.Stalikas A, Fitzpatrick M. Relationships between counsellor interventions, client experiencing, and emotional expressiveness: an exploratory study. Can J Couns Psychother. 1996;30(4):262–271. [Google Scholar]
- 88.Subic-Wrana C, Beutel ME, Garfield DA, Lane RD. Levels of emotional awareness: a model for conceptualizing and measuring emotion-centered structural change. Int J Psychoanal. 2011;92(2):289–310. doi: 10.1111/j.1745-8315.2011.00392.x. [DOI] [PubMed] [Google Scholar]
- 89.Subic-Wrana C, Beutel ME, Brähler E, Stöbel-Richter Y, Knebel A, Lane RD, Wiltink J. How is emotional awareness related to emotion regulation strategies and self-reported negative affect in the general population. PLoS One. 2014;9(3):e91846. doi: 10.1371/journal.pone.0091846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Taylor W, Furlonger B. A review of vicarious traumatisation and supervision among Australian telephone and online counsellors. Aust J Guid Couns. 2011;21(02):225–235. doi: 10.1375/ajgc.21.2.225. [DOI] [Google Scholar]
- 91.Villanueva L, Górriz AB, Prado-Gascó V, González R (2015) The role of emotion awareness and mood: Somatic complaints and social adjustment in late childhood. Psychology, Health & Medicine 20(4):419–430 [DOI] [PubMed]
- 92.Watson JC, Greenberg LS (2017). Emotion-focused therapy for generalized anxiety. American Psychological Association
- 93.Watson D, Clark LA, Carey G. Positive and negative affectivity and their relation to anxiety and depressive disorders. J Abnorm Psychol. 1988;97(3):346–353. doi: 10.1037/0021-843X.97.3.346. [DOI] [PubMed] [Google Scholar]