Zusammenfassung
Einleitung Die COVID-19-Pandemie bedeutet einschneidende Maßnahmen für das nationale Gesundheitssystem. Dies bot den Anlass, die klinischen und ökonomischen Leistungsindikatoren der gynäkologischen und geburtshilflichen Versorgung des Universitätsklinikums Marburg als regionaler universitärer Maximalversorger zu analysieren. Hierzu wurden die Auswirkungen auf die monatlichen stationären und ambulanten Fallzahlvolumina sowie die entsprechenden ICD- und DRG-Kodierungen ausgewertet, um etwaige Versorgungsdefizite aufzudecken.
Material und Methoden Die Studie basiert auf einer retrospektiven Datenanalyse therapierter stationären und ambulanten Fälle der Jahre 2016 bis 2020. Hierzu wurden über das klinikinterne Leistungscontrolling-Programm QlikView die Daten von 9487 Fällen der Klinik für Gynäkologie und 19597 Fällen der Klinik für Geburtshilfe ausgewertet.
Ergebnisse Es bildet sich eine der nationalen Pandemiedynamik folgende Abnahme der gynäkologischen stationären Fallzahlen um –6% ab, während das geburtshilfliche Fallzahlvolumen um +11% im Jahr 2020 steigt. Insgesamt fallen die Effekte für die ambulante Versorgung geringer aus. Zudem lässt sich eine standortbezogene Abnahme der C50 „Bösartige Neubildungen der Brustdrüse“ und C56 „Bösartige Ovarialtumoren“ Diagnosen um –7,4% bzw. –14% feststellen. Eine Rückkehr zu dem Leistungsniveau des Vorjahres konnte im ambulanten in 3 und im stationären Sektor in 5 Monaten erreicht werden.
Schlussfolgerung Die negativen Auswirkungen der COVID-19-Pandemie treffen vorwiegend die Klinik für Gynäkologie. Durch das Vertrauen in die Sicherheit der universitären Versorgung und das Serviceangebot, werdende Väter nach Schnelltestung am Geburtsprozess teilhaben zu lassen, konnte eine Fallzunahme in der Geburtshilfe erreicht werden. Die Rückkehr zu präpandemischen Leistungsniveaus gestaltet sich weiterhin schleppend, während sich der ohnehin weniger betroffene ambulante Sektor zügiger erholt. Der standortbezogene Rückgang der Diagnosen C50 und C56 ist besorgniserregend und bedarf epidemiologischer Aufarbeitung. Die fallzahlbezogenen Auswirkungen der Pandemie bilden sich gleichsam in den ökonomischen Leistungskennzahlen ab.
Keywords: COVID-19, pandemic, healthcare research, maximum care provider, university hospital
Introduction
Since the start of the rapid pandemic spread of COVID-19 in the spring of 2020, societies worldwide have been subjected to significant restrictions. Many measures have been politically imposed which place restrictions on work and social life, in a repeating pattern of lockdowns and gradual attempts to ease restrictions. In order to provide planning certainty and avoid reaching critical capacity within the health system, strong political measures have been imposed on the structure and organization of medical care; these measures have at times made it all but impossible for German hospitals to carry out their regular operations. As a result, restrictions on elective surgery, adjustments to processes with a requirement for pre-hospital triage, and a shortage of medical staff due to quarantine requirements brought even well-established structures in the gynecology and obstetrics departments of the University Hospital of Marburg into a precarious position.
In 2020 the Federal Republic of Germany experienced two waves of infections from the COVID-19 pandemic; each wave was associated with different restrictions and measures applied to medical services. One month after the first case of illness from the coronavirus was recorded in the Bavarian district of Starnberg on January 27, the federal government created a crisis team to work on a collaborative, nationwide response to the pandemic. On March 10, when the coronavirus had finally spread to all of the German federal states, schools started to close and the German borders were closed to incoming travelers. Following this, on March 22, the first restrictions were imposed on movement and social contact; these restrictions were kept in place until April 20. Creators of health policy responded with a knee-jerk restriction on elective surgery programs, so as to free up the intensive care capacity that might be required. For this reason, regular clinical operations almost came to a complete standstill, and medical care was focused henceforth on emergency care and urgent surgery. As the dynamics of the pandemic accelerated into a second wave of infections, with a corresponding rise in new COVID-19 cases in September 2020, the federal and state governments decided to take measures to mitigate risk in social, gastronomy and retail settings, but did not explicitly impose new restrictions on hospital operating capacity. This development gave rise to a new “lockdown light” on November 2 2020, which was made more stringent on December 16, shortly before the Christmas holiday period, due to the continuing spread of the pandemic.
In this article, we specifically aim to present how the measures associated with the two lockdowns in 2020 impacted on case numbers in the gynecology and obstetrics departments of the University Hospital of Marburg as the sole regional maximum care hospital. For this purpose, in addition to the chronological progression in case numbers, we present the corresponding changes in ICD diagnosis codes and records of DRG services compared with the previous year. Finally, we will consider inpatient and outpatient care separately and look at the specific effects on these services, so as to form a picture of how long it took to return to a normal level of service delivery. Moreover, we will also take a look at the impact of the pandemic on central economic performance indicators.
Materials and Methods
Statistical methods
The analysis is based on a retrospective evaluation of data from all inpatient and outpatient cases treated in the gynecology and obstetrics clinic at the University Hospital of Marburg from 2016 up to and including 2020, as well as a corresponding overall assessment of the University Hospital of Marburg for the years 2019 and 2020. The evaluation is based exclusively on descriptive statistical methods. To present the chronological evolution of central performance indicators during the above-mentioned observation period, we calculated the four-year, three-year and two-year averages for the years 2016 to 2019, preceding the pandemic, and compared them with the equivalent values from 2020 so as to form relative and absolute statistical comparisons. For this purpose, we focused our observations on developments in monthly case numbers, the primary ICD diagnoses, the corresponding record of services in the form of case-based DRG, and basic financial parameters for costs and revenue, duration of inpatient admissions, and the case mix index.
Selection of patients
We captured and evaluated case-based treatment data and health economics performance data for 9487 cases in the gynecology clinic and 19597 cases in the obstetrics clinic during the observation period from 2016 to 2020. To compare the economic performance indicators, we calculated the corresponding average values for all of the 86479 inpatient cases treated in the University Hospital of Marburg in the years 2019 and 2020. Similarly, with reference to the ICD secondary diagnosis “U07.1 COVID-19, virus identified”, we captured all 283 COVID-19 cases treated at the University Hospital of Marburg during 2020, and checked them for equivalent performance indicators. In order to meet the compliance and ethics guidelines in place at the University Hospital of Marburg, the data were anonymized, and no patient-specific case numbers were used.
Data analysis
The data used for this analysis, and for the comparison of the basic clinical and financial performance parameters for gynecological and obstetrics services and for the hospital as a whole, were generated retrospectively for the period from 2016 to 2020 using QlikView, the internal performance monitoring program at the University Hospital of Marburg, which records all of the medical, nursing and equipment services that are coded in the hospital IT system. The QlikView program, from QlikTech (Radnor, USA), is a classic data analysis software which makes it possible to map the clinical treatment services in connection with the corresponding financial performance indicators, in the form of both raw data and interactive analyses. We generated the relevant raw data and interactive analyses using QlikView, then processed them in Excel using descriptive statistical methods.
Results
The results from this retrospective data analysis are presented below. First, we take a look at the relative developments in monthly inpatient and outpatient case numbers, separated into gynecology and obstetrics cases. Following this, we present a detailed evaluation of the top 25 recorded primary ICD diagnoses. In this context, we look in particular at the relative and absolute differences in performance indicators for 2020 seen between the comparison with the previous year, 2019, and with the calculated four-year averages for 2016 to 2019. A central aspect of this analysis comprises the differences between the primarily acute focus of medical care in the obstetrics clinic, compared with the predominantly elective focus of cancer treatment and gynecological tumor surgery in the gynecology clinic. Following this, we present our insights from the retrospective observation of the services delivered in the period from 2016 to 2019, compared relatively to current services and services delivered during the 2020 pandemic year. This enables us to map out the impact of the developing dynamics of the pandemic and the associated restrictions and measures on the chronological evolution of clinical and financial performance indicators. Finally, we present the COVID-19 cases that were treated at the obstetrics and gynecology clinic at the University Hospital of Marburg during 2020, and we provide an outlook on developments for central financial performance indicators relating to total costs and revenues, duration of inpatient admissions, and the case mix index.
Inpatient Case Numbers Compared with the Previous Year
Obstetrics
The services provided at the clinic for obstetrics and perinatal medicine range from prenatal diagnostics and ultrasound to special fetal surgery procedures, through to obstetrics monitoring, acute medical care in the delivery room, and follow-up care in the post-natal ward. Besides caesarean sections and surgical treatment of injuries sustained during childbirth, the range of surgical services also includes special procedures for fetal surgery.
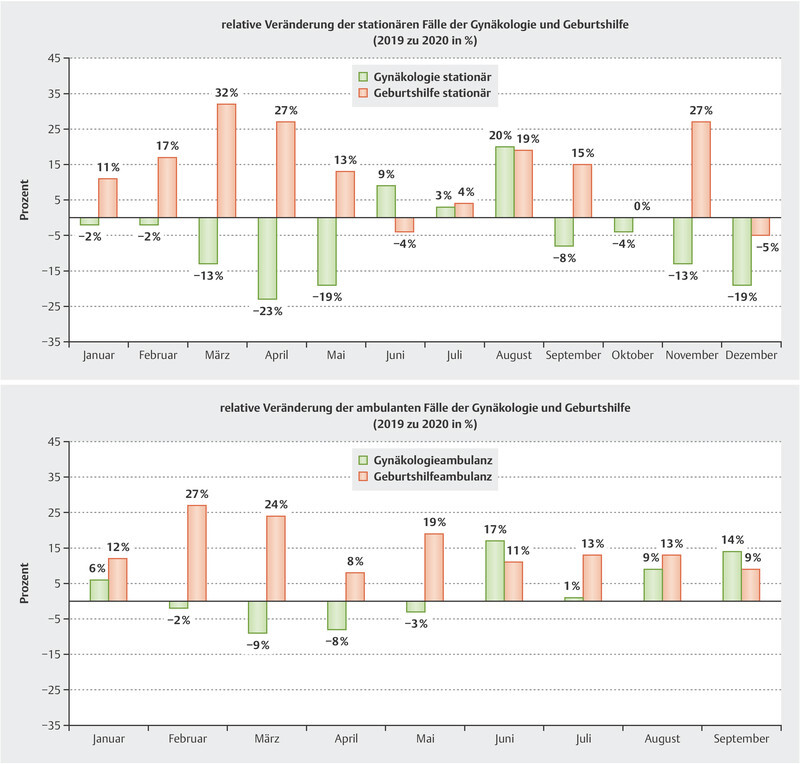
In direct comparison with 2019, the year immediately preceding the pandemic year 2020, we saw an increase in the number of obstetrics cases. The months of June and December proved to be exceptions, showing a relative drop in the number of obstetrics cases, of 4% and 5% respectively, compared with the corresponding performance data from 2019, whereas data for the entire year showed a monthly increase in the volume of services, with an 11% relative increase in case numbers. The highest relative monthly percentage increase of 32% was recorded in March 2020.
Gynecology
While the gynecology, gynecological endocrinology and oncology clinic also provides basic gynecological care as well as advice on all aspects of reproductive medicine, the main focus is on gynecological tumor surgery. The available surgical expertise covers all areas of gynecological cancer and treatment for carcinomas of the breast, ovaries, endometrium, cervix and vulva.
The gynecology clinic saw a relative drop in case numbers compared with the year immediately preceding. The relative monthly comparative data show a relative decrease in service volumes, averaging 11%, for the first five months of 2020. The month of April 2020 showed the highest drop compared with the previous year, based on a relative drop in service volume by 23% for the entire year of 2020. In the three following months, June, July and August, there was a transitory relative increase in case numbers, by an average of 11% compared with the previous year; the case numbers then fell again during the autumn and winter months. In this context, the decline shown in the relative comparative data, with an 11% average monthly drop in case numbers, appears to be comparatively high. The drop in relative case numbers continues throughout the observation period, ending at −6% for the whole year. Considering the equivalent performance indicators for the study period from 2017 to 2019, we can see that the gynecology clinic previously recorded a relative increase in surgery case numbers of 6.7% and 8% respectively for the comparison years 2017 to 2018 and 2018 to 2019.
Outpatient Case Numbers Compared with the Previous Year
Due to the different methods used to record services, we currently only have data for outpatient care at the university outpatient service up to September 2020. Fig. 1 shows that the drop in outpatient case numbers was smaller than the drop in inpatient case numbers. For gynecology outpatient services, the relative drop in case numbers in the months during the first lockdown (February to April 2020) was 7%, compared with a 14% drop in inpatient case numbers. The biggest relative drop in outpatient cases of 9% occurred in March, while the biggest drop in monthly inpatient cases of 23% occurred in April. For university outpatient obstetrics services, there was not a single drop in monthly case numbers. In fact, outpatient obstetrics services experienced a 15% increase in case numbers in 2020 compared with the previous year.
Fig. 1.
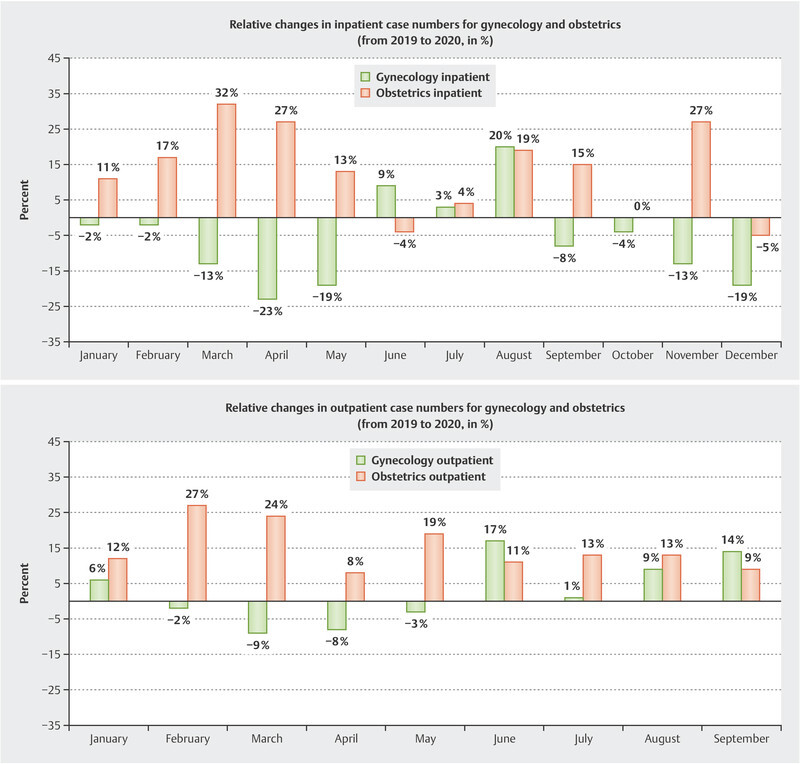
Relative monthly change in inpatient and outpatient case numbers for gynecology and obstetrics (2020 compared with 2019).
Changes to ICD Primary Diagnoses
As well as observing trends relating to developments in case numbers for inpatient and outpatient care at the gynecology clinic, we also recorded and compared the most frequent ICD primary diagnoses, and mapped this data so as to investigate not just changes in case volumes, but also the actual impact on demand for clinical treatment of particular illnesses.
Obstetrics
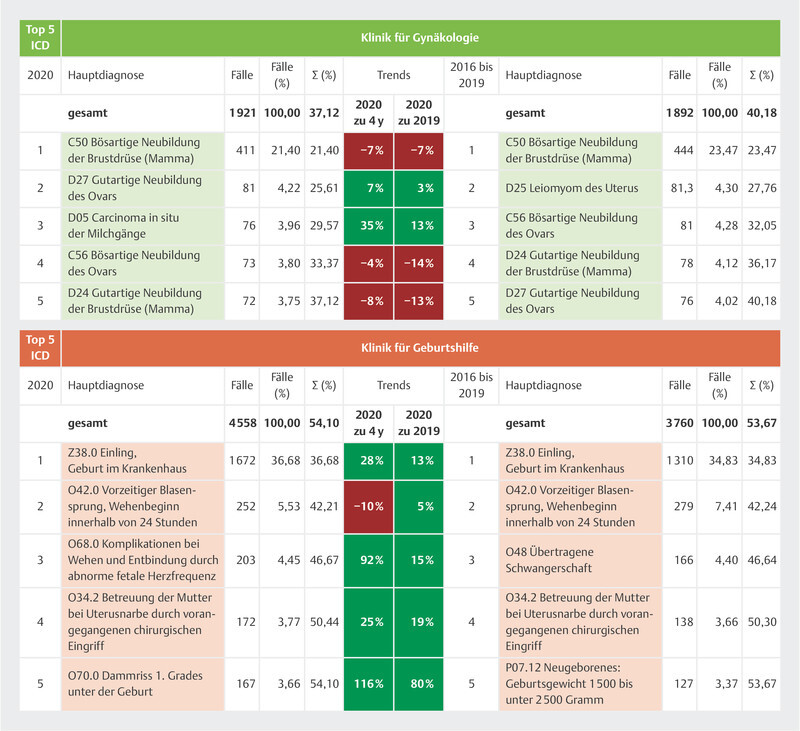
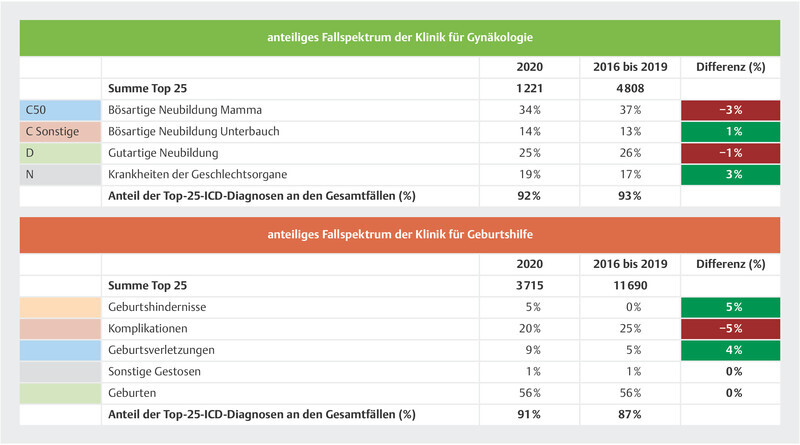
For this purpose, we compared data from 19597 cases treated in the obstetrics clinic over the past five years. The 25 most common ICD primary diagnoses, amounting to 4558 cases, represent 81.51% of all cases coded in 2020. Out of the top 25, births represented the largest service category at 56% of all primary diagnoses, followed by obstetric complications at 20%, childbirth injuries at 9%, obstructed labor at 5%, and other events at 1%. The ICD diagnosis Z38.0 “Single liveborn infant, born in hospital” was the most frequent of all primary diagnoses with an ICD code, at 36.68%; this diagnosis saw a growth of 28% at the University Hospital of Marburg in 2020 compared with the four previous years. The direct comparison between 2020 and 2019 also showed a 13% increase in ICD Z38.0 diagnoses. Fig. 2 presents in detail the developments for the five most common ICD primary diagnoses occurring in obstetric care at the University Hospital of Marburg, and explores the corresponding comparisons between 2020 and 2019 and the quarterly trends for the period from 2016 to 2019.
Fig. 2.
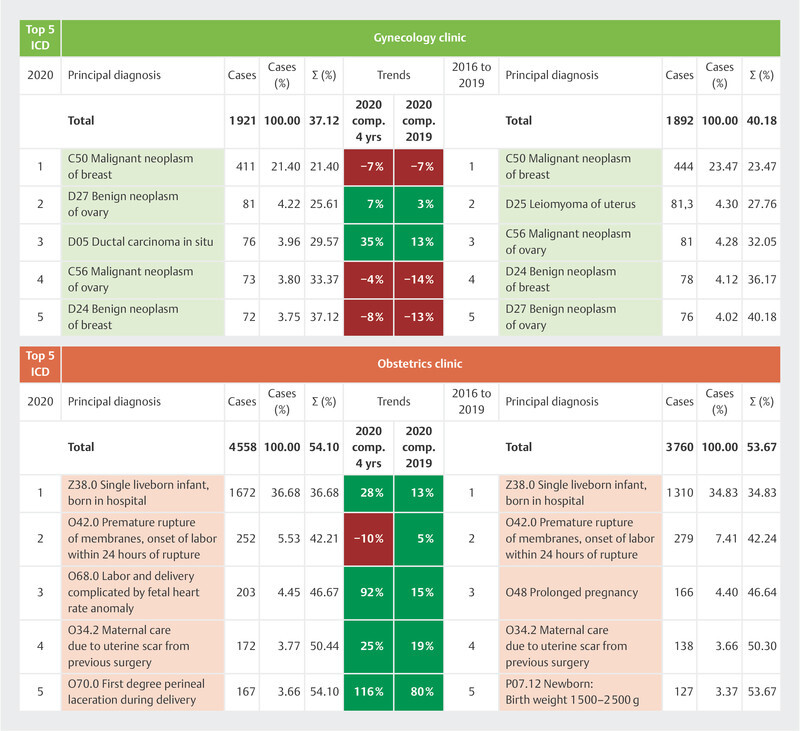
Detailed analysis of top 5 ICD primary diagnoses in the gynecology and obstetrics clinic (2016–2020).
Gynecology
Just as for the data analysis for the obstetrics clinic, we also evaluated the ICD primary diagnoses for the past five years for the gynecological services. Overall, we captured and compared 9487 cases that occurred during the observation period. The 25 most common ICD primary diagnoses in 2020, accounting for 1921 of the patients treated, represented 64% of all coded primary diagnoses. Among these, malignant neoplasm of the breast came in the top position at 34%, followed by benign neoplasms at 25%, other diseases of the genital tract at 19%, and malignant neoplasms of the abdomen at 14%. The most common ICD primary diagnosis, C50 “Malignant neoplasm of breast”, was made in 411 cases in 2020; a direct comparison between 2020 and 2019 shows a considerable drop in cases of 7.38% for this diagnosis. In terms of numbers, the biggest discrepancy between the four-year trend (+77%) and the direct comparison with the previous year (+8%) was seen with ICD diagnosis T85.82 “Capsular fibrosis of breast due to breast prosthesis and implant”. Fig. 2 illustrates in detail the relative increases and decreases for the five most common diagnosis codes based on the ICD primary diagnosis in question for the relevant comparison periods.
Finally, in Fig. 3 we arranged the 25 most common ICD codes for gynecology and obstetrics into etiological subgroups based on the first digit of the ICD code, so as to illustrate proportional shifts in the range of case types.
Fig. 3.
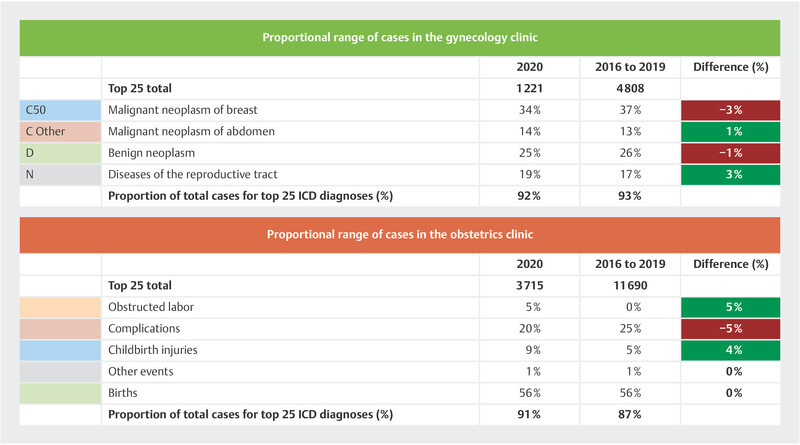
Proportional comparison of the range of ICD cases occurring in the gynecology and obstetrics clinic (from 2016 to 2020).
Changes to DRG
For the identified cases, we also analyzed the corresponding DRG codes. In addition to the diagnosis definition according to ICD code, this also gives an overview of the most prominent surgical, interventional, and drug treatments delivered for the cases included in this study, as well as the final health cost of these cases based on a fixed sum per case.
Obstetrics
The 25 most common DRG codes represent 96.88% of all the cases included in this analysis. In 2020, 46% of the 25 most common DRG codes related to newborns, 28% to vaginal deliveries, and 19% to caesarean sections. Compared with the average value for the comparison period of 2016 to 2019, the relative proportion of newborns and vaginal deliveries among the top 25 DRG codes increased by 3% and 10% respectively, while the relative frequency of caesarean sections decreased by 10%. At 37.06%, DRG P67E “Single liveborn infant, birth weight > 2,499 g” represented the most commonly coded diagnosis-related group. This code was subject to a growth trend, with an increase of 67% during the period from 2016 to 2019, and 12% from 2019 to 2020.
Gynecology
The 25 most common DRG case groups for gynecology represent 79.44% of all coded diagnosis-related groups for the cases included in this analysis. Among the 25 most common DRGs, breast operations accounted for 47%, and abdominal operations accounted for 44%. Compared with the 2016 to 2019 comparison period, there was an increase in the relative proportion of abdominal operations among the top 25 DRGs, while the relative proportion of breast operations saw a decrease. This is reflected in the most frequently coded DRGs. While in the 2016 to 2019 period the code J23Z “Major breast surgery procedures with malignant neoplasm” was still the most frequently coded DRG at 6.5%, in 2020, the DRG N21A “Hysterectomy for reasons other than malignant neoplasm” took the top place with 7.13%.
Treated Cases of COVID-19
Based on the ICD code “U07.1 COVID-19, virus identified”, a total of 283 COVID-19 patients were hospitalized at the University Hospital of Marburg during the 2020 pandemic year. With a total population of 245754, the district of Marburg-Biedenkopf recorded 5181 cases of COVID-19 in 2020. Moreover, 78.8% of the hospitalized COVID-19 cases were treated in an internal medicine ward. Over the whole year of 2020, five patients with a COVID-19 infection were hospitalized at the obstetrics and gynecology clinic at the University Hospital of Marburg. All five were obstetrics patients. This was because the patients in question were infected with COVID-19 perinatally, while patients with an active COVID-19 infection were excluded from admission to the gynecology clinic through preoperative triage based on nasopharyngeal swab PCR testing or rapid antigen testing. If a patient with a primary gynecological diagnosis became infected and was subsequently hospitalized, for example postoperatively in the context of adjuvant radiotherapy or chemotherapy, the patient was supposed to be transferred to an internal medicine ward and treated there. However, we do not know of any cases where this occurred.
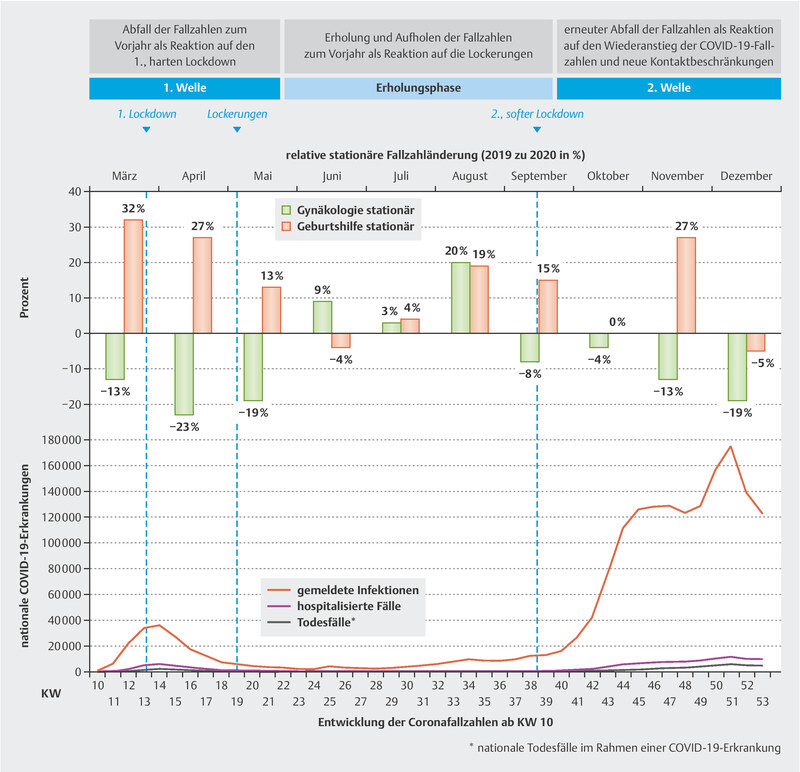
Fig. 4 illustrates the developments in relative monthly case numbers in the gynecology and obstetrics clinic for 2020 compared with 2019, and places this in the context of the chronological progression of national COVID-19 infections.
Fig. 4.
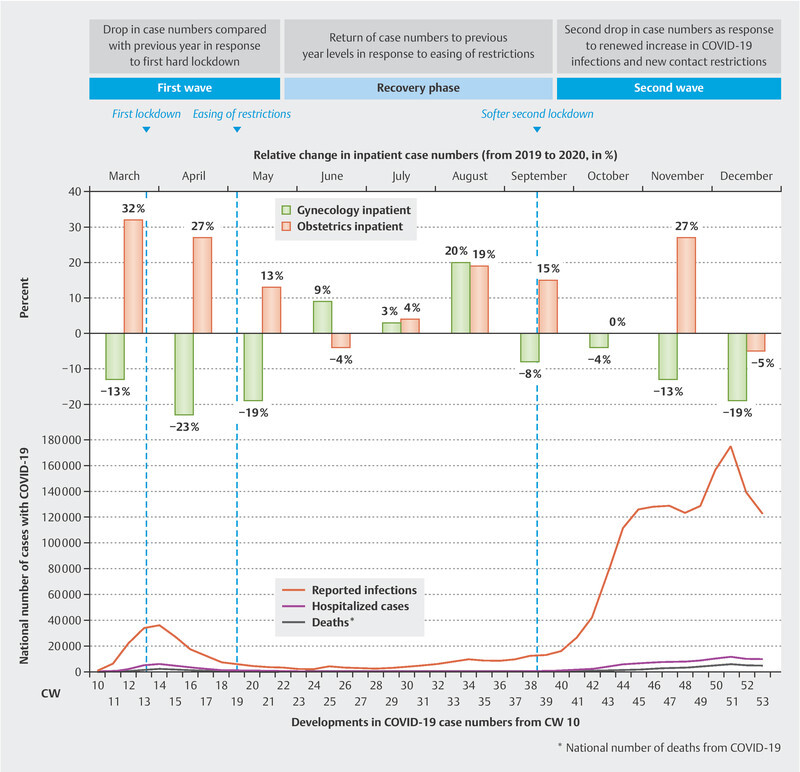
Presentation of the chronological development in national COVID-19 infections and relative monthly changes to inpatient case numbers.
Effects on Key Financial Performance Indicators
Fig. 5 illustrates the relative changes in total costs and total revenues, by month, for the 2020 pandemic year compared to 2019. For this purpose, in order to represent the purely operational results of the gynecology department as an independent discipline, we have disregarded the proportional costs and revenues of the gynecology clinic in relation to the overall business result for the University Hospital of Marburg, i.e., the proportional financial result, operating result and investment result, as well as taxes.
Fig. 5.
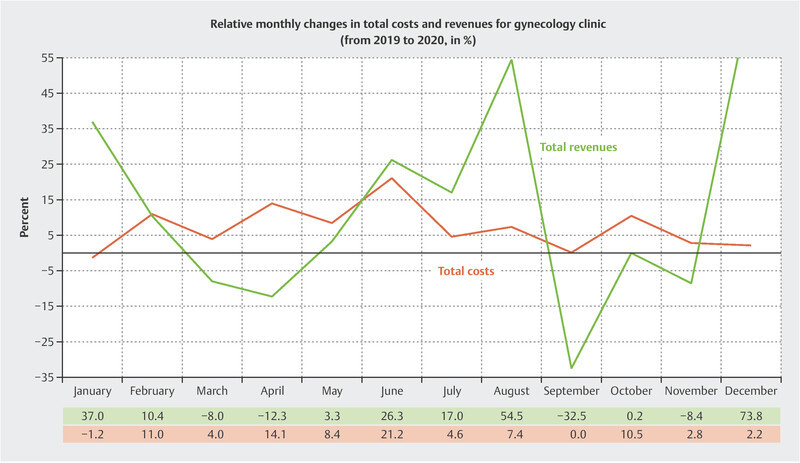
Presentation of the chronological development of relative monthly changes to total costs and total revenues of the gynecology clinic (2020 compared with 2019).
Overall, during the 2020 pandemic year there was a relative increase in total revenues and total costs of 10.6% and 7% respectively compared with 2019. Finally, we were able to determine a relative increase of 98% in the net result for the gynecology clinic compared with the previous year. The gynecological case mix index dropped by 2.3%, while it rose by 3.4% for the hospital as a whole. Similarly, there was a 25% relative drop in the number of short-term admissions, while the number of long-term admissions increased by 111%.
Discussion
In order to determine the significance of these results and the conclusions drawn from them for the regional and nationwide service obligations of the University Hospital of Marburg, it is necessary to have a basic understanding of the regional situation regarding the provision of gynecology and obstetrics services. As the sole provider of inpatient gynecology and obstetrics services in the district of Marburg-Biedenkopf, an area with approx. 250000 inhabitants, not only does the University Hospital of Marburg, in collaboration with over 80 registered physicians and approx. 7 providers of basic inpatient care, form a close-knit service network; it also forms a critical part of the gynecology and obstetrics care infrastructure at state level, occupying a facility covering 8660 km 2 and serving approx. 850000 inhabitants of the Schwalm-Eder-Kreis, Vogelsberg, Waldeck-Frankenberg, Marburg-Biedenkopf and Lahn-Dill-Kreis districts in North and Middle Hesse, as well as a large proportion of the approx. 500000 inhabitants of the Siegen-Wittgenstein and Hochsauerlandkreis districts of North-Rhine Westphalia. The next closest maximum care hospitals are the Kassel Hospital, located 75 km to the north, and the Gießen University Hospital, located 35 km to the south, while approx. 50 km to the east and west the Schwalmstadt and Dillenburg hospitals provide basic inpatient care for patients in peripheral locations, but cannot offer a comprehensive range of services. This is why the University Hospital of Marburg acts as a central regional and interregional center of competence, not only for gynecological cancer diagnosis and treatment, but also for obstetrics services. In this context, a closely structured collaboration between the peripheral providers of basic care, physicians providing outpatient treatment, and the neighboring maximum care hospitals in Kassel and Gießen has evolved in order to guarantee a full range of gynecology services in the context of regional cancer centers and special diagnosis and treatment in the field of obstetrics and prenatal care. At the national level, the University Hospital of Marburg delivers a public supply mandate which, especially in regard to gynecological cancer with a focus on abdominal tumors, clearly extends beyond the described regional and interregional borders.
The changes in case numbers identified in this study give a striking illustration of the difference between gynecological tumor surgery, which is primarily elective, and obstetric services which are primarily set up to deliver acute care. While the provision of obstetric services remains almost completely unaffected with regard to changes in monthly case numbers at the University Hospital of Marburg, even showing a clear growth of 11% in inpatient services for the year as a whole compared to the previous year, gynecology services followed the national chronological dynamics of the COVID-19 pandemic, recording a 6% drop in inpatient case numbers. This divergent development in the two departments is rooted in the primary measures taken by the clinic management, which was refined over time through a targeted action plan developed in close consultation with the different departments.
The COVID-19 Action Plan and Influence Wielded by the Clinic Management
The initial management response to the spread of the COVID-19 pandemic consisted of imposing an almost complete halt on the elective surgery program, in order to free up staff and ventilators in case they were needed, and to impose a complete contact ban on external visitors in order to prevent nosocomial infection of patients with COVID-19. In addition to this, there was an abrupt decline in uptake of outpatient services, which we attributed to outpatients initially fearing an increased risk of infection in clinical settings, although the clinic management did not place any explicit restrictions on the outpatient services offered. With the development of the pandemic over time, there has been increasing refinement of the pandemic action plan and hygiene plan in consultation with the different medical departments; with regard in particular to the mandate of the gynecology department to provide oncology and obstetrics services, these refinements served to guarantee an independent leadership style on the part of the clinic management, which was able to adapt to the evolving situation.
Establishing and refining the triage system
The entire university hospital adopted an extensive triage system which had already been proven internationally to be a key measure in enabling health providers to stay on top of the volatile dynamics of the pandemic. At first, patients underwent PCR testing prior to hospitalization; this was later exchanged for the more cost-effective rapid antigen testing. Emergency admissions underwent an identical process in a separate emergency area, and were only released from isolation and transferred to a ward after returning a negative test. At present, patients and visitors may only enter the university hospital if they have returned a current negative rapid antigen test or if they have proof of double vaccination.
Implementation of structured hygiene measures
Due to ongoing refinements in the context of how the pandemic is evolving over time, we are only able to provide a basic outline of the clinic’s internal hygiene plan. As explained above, pre-admission PCR testing, which has subsequently been extended to include nasopharyngeal rapid testing, is the key. Testing makes it possible to avoid unnecessary visits to the clinic by people infected with COVID-19, for example in the context of routine follow-up outpatient appointments, while patients who do need to attend the clinic are steered directly into a COVID-19 workflow. In this context, this also means that pregnant women with COVID-19, after their baby has been delivered in the delivery room, are transferred to one of the COVID-19 wards, and are cared for externally by the gynecology and obstetrics team while occupying a bed outside of the gynecology ward. Moreover, for inpatients or in cases of suspicion, repeat testing provides an additional level of security. The entire hospital has imposed an explicit visitor ban. In consultation with the clinic management, there is some flexibility, with exceptions made for cancer patients, palliative care patients, ICU patients, and obstetrics patients; demand differs in intensity according to the incidence rate at the given time, and these exceptions are handled decentrally by the department in question. For gynecology, this means that cancer patients may receive visits from their partner or close relatives according to the judgement of the chief medical officer of the ward. In the obstetrics clinic, partners are allowed to participate in the entire birthing process provided they have returned a negative test. Similarly, partners have regular opportunities to visit the prenatal monitoring ward. Upon leaving the hospital premises, the individuals must expect repeat testing. Overall, these arrangements reflect increased trust on the part of the clinic management in the efforts made by the gynecology and obstetrics clinic to maintain good hygiene; they have also been the object of critical discussion. In our opinion, emotional support from loved ones is essential in the context of cancer and obstetrics patients. The gynecology and obstetrics clinic at the University Hospital of Marburg would never envisage a complete ban on visitors in this context. The low number of COVID-19 cases in both clinics has proved that this does not constitute an increased risk for the spread of infection. In the case of clinic staff who became infected with COVID-19, all of the primary infectious contacts were among their private acquaintances.
COVID-19 workflow separated from regular service provision
Based on a successful triage process, intensive efforts were made right at the outset to separate the COVID-19 workflow completely from regular service provision by setting up an isolated process, located in the emergency department, from which patients were transferred to an interdisciplinary COVID-19 unit. It has been demonstrated that regular service provision can and must continue, even during a pandemic, so as not to jeopardize the treatment of other conditions or risk poorer medical outcomes. It is certainly possible to keep COVID-19 out of regular inpatient and outpatient services, as can be seen from the example of the gynecology clinic at the University Hospital of Marburg, operating as a regional maximum care hospital. Accordingly, at the Marburg location, cancelling outpatient appointments or shifting to video consultations proved either unnecessary or had already been initiated or established, for example, the teledermatology video consultations held in the dermatology and allergies clinic at the University Hospital of Marburg. Through adequate triage and separation of the COVID-19 processes from regular gynecology services, it was possible to prevent nosocomial infection with COVID-19. Similarly, there were only a few individual cases of staff off work due to illness or quarantine requirements. Through consistent testing of the clinic staff by the department for clinic hygiene after every confirmed contact with a COVID-19 patient, it was possible to avoid closing entire departments and wards.
Establishing reliable modelling for regional utilization of capacities
Beyond this, the triage and separation of COVID-19-free processes from the pandemic response opened the way for informed modelling that could be used to predict regional capacity utilization based on epidemiological and care-related parameters. Consequently, the management developed an important tool for predicting and proactively allocating treatment capacities according to the regional dynamics of the pandemic. Considering the constantly recurring spikes in infections, the virus mutations, and the slow progress of vaccinations in Germany, the hospital’s ability to proactively manage its own capacities is a key factor in remaining economically viable while still meeting its service mission as a leading regional health care provider. This means that in the event of a rapid increase in incidence, the University Hospital of Marburg has the ability at any time to re-establish COVID-19 departments and intensive care units and isolate them from other clinic operations, as was already done during the first wave of infections in 2020.
Boosting regional communication and collaboration between service providers
In the end, the ability for facilities to closely control their own capacities opens up the possibility for regional services to be managed independently, without having to rely on unwieldy political measures. Because the pandemic initially destroyed patients’ trust that it would be safe to be treated in a hospital setting, and trust in the national crisis management plan in the health care sector has been waning perceptibly during the course of the pandemic, it is especially important to boost communication at the regional level. As a leading regional healthcare provider, we need to actively communicate the measures that have been implemented and the associated performance indicators; not only to assure safe treatment for COVID-19 patients, but also to guarantee a full range of services for all medical conditions going forward. For outpatient services in particular, intensive communication is key to retaining trust, and maintaining a high level of demand for the services provided by the outpatient clinics.
The description of the action plan formulated by the clinic management at the University Hospital of Marburg shows that a structured hygiene plan combined with close consultation between the management and the medical departments, with continuous improvement and refinement of the measures adopted, is key to avoiding internal infections. To achieve this, close consultation is required between the various medical departments, the hospital management and the hygiene department. As long as the COVID-19 workflow can be kept separate from the usual operations, the rate of infections within the region permitting, normal clinical operations can continue without restrictions.
Discussion on Obstetrics Services
The positive development in the number of obstetrics cases needs to be discussed critically in the context of the regional care situation during 2020. Basically, the case numbers in the obstetrics clinic at the University Hospital of Marburg had increased during the previous years due to successive closure of obstetrics facilities in the outlying areas, for example the obstetrics departments in the Biedenkopf and Wehrda district hospitals. This explains the fact that the number of births managed at the university hospital increased by 4.6% from 2017 to 2018, and by a further 15.2% between 2018 and 2019. However, since 2019, a stable, centralized service for obstetrics care has been in place. The next closest labor wards are located to the north, east and west in the smaller outlying facilities of the Frankenberg District Hospital (approx. 35 km away), the Asklepios Schwalm-Eder clinics in the Schwalmstadt hospital (approx. 50 km away) and the Lahn-Dill clinics in Dillenburg (approx. 50 km away). However, none of the clinics mentioned above is able to provide comprehensive medical expertise or specialized prenatal diagnosis and treatment; accordingly, in cases that exceed the limits of their competence, these facilities fall back on the services offered at the University Hospital of Marburg. The next closest hospital providing maximum care for obstetrics patients, with comprehensive medical expertise, is the University Hospital of Gießen (located approx. 35 km to the south). In the Marburg-Biedenkopf district, the Geburtshaus Marburg midwife service provides an alternative option for natural deliveries. To our knowledge, none of the facilities mentioned above had to close or restrict their services during the 2020 pandemic year due to COVID-19; accordingly, we have not observed any direct external effects on the uptake of obstetrics services. However, there were clear differences in the practices adopted with regard to hygiene and limiting contact. Through consistent, fine-grained PCR testing and rapid antigen testing at the University Hospital of Marburg it remained possible at all times for partners to attend the birthing process, while most regional service providers imposed major restrictions on partners being present during the birth. At the University Hospital of Marburg, this offer was limited to partners of the woman in question; other friends or family members were not allowed to attend the birth. Moreover, this arrangement represented an absolute exception in the inpatient setting; in all other departments, such as ICU units, exceptions to allow visitors were only made in the case of end-of-life care. One year after the pandemic outbreak of the novel coronavirus with its single-stranded RNA genome, the consequences of a COVID-19 infection for pregnancies during the prenatal, perinatal and postnatal stages remain unclear; possible effects relating to an increase in pregnancy complications in the presence of COVID-19 infection are still being discussed, and to date, there is no standardized, scientifically proven treatment regime for pregnant women infected with COVID-19 1 2 3 4 5 . Accordingly, in our opinion, there are two factors responsible for the positive trend in case numbers in the obstetrics department. Firstly, the high level of trust that patients have in receiving safe, COVID-19-free care in the delivery ward of a maximum care university hospital has led to increased demand for the obstetrics services offered at the University Hospital of Marburg. Secondly, many couples chose to have their babies delivered at the Marburg university hospital delivery suite due to our policy of allowing partners to attend the birth provided that they underwent a nasopharyngeal PCR test or a rapid antigen test for COVID-19, a service which was not always offered by the other regional providers.
Discussion on Gynecology Care
The 6% drop in relative numbers of gynecology cases goes against the growth trend of the previous two years, which saw an increase of 6.7% and 8% respectively. Based on the observations set out above, this can be attributed to the massive restrictions placed on the elective surgery program, a game-changing measure which was established at the national level as a primary health policy measure responding to the accelerated dynamics of the pandemic. The principle on which this measure was based, i.e., freeing up ventilation capacity and minimizing the risk of intraoperative infection between medical staff and patients, has so far not been confirmed at the regional level at the University Hospital of Marburg. In our opinion, the reduction in gynecology case numbers does not mean that it is not possible to provide gynecological tumor surgery with adequate protection for the patients, some of whom are immunosuppressed. Our observations of the COVID-19 cases handled at the university hospital proves that it is possible, with reliable pre-admission triage, to prevent patients contracting nosocomial COVID-19 infections with a high level of confidence. With the approval of COVID-19 rapid antigen tests, enabling preoperative triage in the context of pre-admission testing of cancer patients to be organized more efficiently, the prevailing opinion that is now expressed in the literature is that treatment of gynecological tumors should continue in accordance with the generally accepted treatment guidelines, provided that this does not jeopardize any critical regional infrastructure or lead to a shortage of staff or ventilators. Many international studies from Italy, the USA, Korea, Croatia and China indicate that it is possible to deliver safe treatment of gynecological tumors even during a global pandemic, without increasing the risk to patients of nosocomial infection or a higher rate of mortality associated with COVID-19 6 7 8 9 10 11 12 13 14 15 .
Considering the comparison we undertook of changes in relative monthly case numbers in inpatient and outpatient services, it is clear that the obstetrics services remained largely unaffected by the COVID-19 pandemic. For gynecology services at the University Hospital of Marburg, the fact that the negative impact on outpatient services was less severe than the impact on inpatient care can be seen as a positive aspect. Moreover, the outpatient gynecology services were much quicker to recover from the negative developments than the inpatient services. In May 2020, after just three months, outpatient services had returned to normal service delivery, while inpatient case numbers only returned to levels seen in the previous year in July 2020, after five months. In our opinion, this is due to the fact that patients were initially hesitant to make use of outpatient services during the pandemic for fear of contracting a COVID-19 infection in a hospital setting. Through targeted communication, we were able to quickly rebuild patients’ trust in receiving safe treatment at the university hospital outpatient clinics. The prolonged negative trend in the inpatient setting can be attributed primarily to restrictions made to the elective surgery program, which were only gradually eased as we moved into summer.
Considering the developments in case numbers, the big losers were the patients diagnosed with “Capsular fibrosis of breast due to breast prosthesis and implant” (T85.82) and “Hypertrophy of breast” (N62). However, this development is not so surprising given that these ICD codes are for reduction mammoplasty or reconstruction with implants; it illustrates the fact that, during the pandemic, the elective surgery program and available capacities were focused in a targeted way on cancer patients who required prompt treatment. Overall, however, if we consider the ICD diagnosis codes, we can establish that in 2020, the first year of the pandemic, at the regional level there had already been a concerning decline in the number of C50 “Malignant neoplasm of breast” and C56 “Malignant neoplasm of ovary” diagnoses, each dropping by 7.4% and 14% respectively. In our opinion, it seems logical that the rate of cancer cases would not decrease due to a global epidemic of an infectious disease; for this reason, the decrease in the number of gynecological cancer operations performed, combined with a decrease in initial cancer diagnoses, presents a critical risk to quality of care and to the rate of mortality associated with cancer.
In pandemic hotspots such as New York City, critical restrictions were imposed on the treatment of gynecological cancers. According to records kept by the New York Presbyterian Hospital Association, 39% of all gynecological tumor patients received treatment that was modified due to COVID-19. Of these modifications, surgical procedures were most often affected, making up 67%, while chemotherapy and radiation therapy were modified respectively in 22% and 19% of cases 16 . Matsuo et al. carried out a retrospective study investigating the risks of changing treatment procedures for early-stage cervical carcinoma in response to recommendations that gynecological tumor surgery should be deferred, or at times completely replaced with chemoradiotherapy. For the patient cohort with IB to IIA stages of squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinomas of the cervix, for which the gold standard treatment consists of laparoscopic surgery or open abdominal hysterectomy, the authors of this study were able to establish a significantly increased risk of parametrial tumor invasion, as well as a moderate increase in mortality 17 . The future impact of delaying gynecological surgery, as well as initial diagnoses potentially being made at a later TNM stage, will only become clear in the coming years through epidemiological monitoring and analysis; this needs to be the subject of meticulous scientific observation.
The final comparison of the range of diagnoses shows that the number of gynecological malignancies dropped in absolute terms by 23.5 cases, while the proportion of underlying malignant diseases among the top 25 ICD codes fell from 50% to 47%. Moreover, the proportion of benign neoplasms also fell by 1%, or 4.25 cases, compared with the previous year, while the number of ICD-coded diagnoses for other diseases of the reproductive tract rose by 36.75 cases, increasing their proportion of overall cases from 17% to 19%. Based on a total of 1221 cases, which represents the total number of cases for the 25 most common ICD codes, accounting for 63.56% of all ICD-coded diagnoses for 2020, we are only able to make very limited observations regarding any shift in the range of diagnoses. However, the results indicate that there was a decrease in the number of tumor cases treated as part of the case load at the University Hospital of Marburg, which did not reflect the actual incidence of malignant diseases, and that, contrary to this trend, the proportion of other diseases of the reproductive tract treated at the hospital actually increased during the pandemic year.
Economic Perspective
Due to the positive trend in case numbers, we did not find it necessary to present the progress of key financial performance indicators for the obstetrics clinic at the University Hospital of Marburg. The case-related performance data also show that the key financial performance indicators remained largely unaffected by the pandemic. Accordingly, a detailed presentation and discussion of the overall financial result with regard to the COVID-19 pandemic does not promise any insights worthy of discussion.
In contrast, the chronological progression of relative revenues for the gynecology department, following the changing dynamics of the pandemic during the 2020 business year, shows greater fluctuations than does a pure consideration of case numbers. During the first wave of infections there was a clear drop in revenues for the months of March and April, averaging a 10% decrease compared with the previous business year 2019. However, in contrast to the relative changes in case numbers, there was a rebound in revenues in May; these recovered much more quickly than the surgery case numbers which were heavily reduced due to restrictions. On the other hand, the negative trend that occurred in September with the second wave of infections, with a 33% drop in total revenues, was significantly larger than could be expected in the first instance based on developments in case numbers. The negative impact of the second wave of pandemic infections on revenues was distinctly greater than the equivalent impact from the first wave. This contrasts with the clear impact that the first wave had on surgery case numbers, described above in our case number analysis. The rapid increase in total revenues in December can be attributed to the accounting practice of deferring additional fees until the last month of the year.
An observation of cost trends in relative comparison to the previous year shows a clear increase in costs, with the greatest cost burden clearly occurring during the summer months. This is consistent with the clear increase in surgical case numbers during the summer of 2020, serving to offset the impact of the first wave of the pandemic, which logically resulted in increased costs. The fact that costs continued to increase despite the relative decrease in case numbers described above, i.e., in March through to May or September, October, and November, can be explained by separating out the monthly trends for staffing costs and materials costs. This showed that the predominantly variable cost of materials followed the monthly dynamics of the case numbers, dropping in synchrony with the waves of infection, while staffing costs for 2020 rose on average by 16%. We can, therefore, conclude that the fixed costs of the gynecology clinic, which include staffing costs, remained unaffected by the monthly trends caused by the pandemic; accordingly, we can determine a 7% increase in total costs for gynecology services for the whole year of 2020.
Essentially, the number of short-term admissions (above the threshold length for admission but below the average length of admission) fell by 25% compared with 2019; in contrast, long-term admissions (above the average length of admission but below the upper threshold for length of admission) increased by 111% in response to a decrease in absolute case numbers in the 2020 pandemic year. This indicates a relative increase in the duration of hospital admissions as a response to the drop in patient turnover; because of impending reductions based on DRGs where the minimum threshold period for admission was exceeded, this cannot be explained from a purely economic perspective. Interestingly, however, the gynecology and obstetrics clinic showed only a minimal decrease in the case-related case mix index (CMI) as a key indicator for the overall complexity of the cases treated, with a 2.3% drop for gynecology and no change for obstetrics, while for the University Hospital of Marburg as a whole, the case complexity according to the CMI solidified, with an increase of 3.4%. In our opinion, one factor that contributed to this was the reactive, cross-departmental focus on complex diseases and tendency to avoid elective hospital admissions in the context of the pandemic. Another factor was the high average CMI value, at 2.3, for the 283 treated COVID-19 cases; of these cases, those that required hospital admission were patients with multiple morbidities who had an average of 16.5 coded secondary diagnoses compared with 2.9 for the gynecology patients treated in 2020. The clear increase in the average length of admission, combined with a slight decrease in overall complexity of the treated cases, shows that during the 2020 pandemic year the gynecology clinic responded to the lower rate of patient throughput by adopting a more conservative discharge policy, but without actively changing its range of services. Active revenue management and the receipt of additional off-budget payments led to an improved operational result, with an increase in net revenue despite increased cost and reduced case numbers.
From this we can see that the two waves of COVID-19 infections and associated measures had an impact on the net financial result. Initially, the 98% relative increase in the gynecology clinic’s net financial result appears to be substantial; however, it can be explained due to changes in accounting practices and changes to the revenue structure, such as the six-fold increase in additional charges. It does not, therefore, reflect the clinic’s real operational result. Accordingly, the 7% increase in total costs compared with the previous year and a 3% decrease in DRG revenues provide an unambiguous indicator for the impact of the pandemic on the clinic’s overall financial result. Thus we are able to establish that our observations relating to case numbers are reflected in the financial results, and that the obstetrics clinic was able to maintain a stable economic performance, while the gynecology clinic was subject to the changing dynamics of the pandemic and achieved an increase in its net financial result due to additional charges assigned in the bookkeeping procedure.
Conclusion
The goal of this article was to evaluate the impact of the coronavirus pandemic on inpatient and outpatient case numbers at a supraregional maximum care university hospital, to identify any effects on trends relating to the range of clinical services provided and structured measures of economic performance in the form of ICD primary diagnoses and DRG codes, and to determine how long it took to return to a pre-pandemic level of service provision. In this process, we hoped to uncover any shortfalls in the care provided.
Our analysis of the case data showed that obstetrics services, including both inpatient and outpatient services, remained largely unaffected, and continued to follow the growth trend from the previous year. In our assessment, this is based on two factors: the trust that patients have in receiving safe, high-quality care at our university facility, and the fact that the University Hospital of Marburg allowed prospective fathers to attend the entire birthing process, in spite of the pandemic, provided that they underwent nasopharyngeal PCR testing or a rapid antigen test.
In contrast, for gynecology services, we were able to demonstrate that the pandemic had a considerable negative impact on case numbers and on inpatient services. Based on inpatient case numbers, the impact on elective cancer surgery was clearly greater than the impact on outpatient services.
In the gynecology clinic it took just three months for outpatient services to return to a pre-pandemic level of medical care and financial performance, while inpatient services took five months to return to the performance levels of the previous year.
Based on ICD and DRG codes, the range of services in both subareas remained largely unaffected in 2020 compared with 2019. However, the location-based relative decrease in C50 “Malignant neoplasm of breast” and C56 “Malignant neoplasm of ovary” diagnoses, by 7.4% and 14% respectively, is a clear cause for concern, and needs to be the subject of detailed epidemiological analysis and scientific follow-up.
The effects of the pandemic can be identified in the progression of the financial KPIs; however, the extent of the economic impact differs from that observed in the case data.
Note
The authors are solely responsible for the opinions expressed in this article; these do not necessarily reflect the views, decisions or guidelines of the institutions with which the authors are associated.
Acknowledgement
We would like to thank Sascha Domröse, from the Controlling Department at the University Hospital of Marburg for his support and help in training us to analyze data using the QlikView performance management software.
Danksagung
Wir danken Herrn Dipl.-Ök. Sascha Domröse aus der Controlling-Abteilung des Universitätsklinikums Marburg für die Unterstützung und Schulung zur Datenanalyse mithilfe des Leistungscontrollingprogramms QlikView.
Footnotes
Conflict of Interest The authors declare that they have no conflict of interest.
References/Literatur
- 1.Stumpfe FM, Titzmann A, Schneider MO et al. SARS-CoV-2 Infection in pregnancy – a review of the current literature and possible impact on maternal and neonatal outcome. Geburtshilfe Frauenheilkd. 2020;80:380–390. doi: 10.1055/a-1134-5951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Klaritsch P, Ciresa-König A, Pristauz-Telsnigg G. COVID-19 during pregnancy and puerperium – a review by the Austrian Society of Gynaecology and Obstetrics (OEGGG) Geburtshilfe Frauenheilkd. 2020;80:813–819. doi: 10.1055/a-1207-0702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cavalcante MB, Cavalcante CTMB, Braga ACS et al. COVID-19 treatment: drug safety prior to conception and during pregnancy and breastfeeding. Geburtshilfe Frauenheilkd. 2021;81:46–60. doi: 10.1055/a-1247-5271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Recker F, Weber E, Strizek B et al. Lung sonography in obstetrics during COVID-19. Geburtshilfe Frauenheilkd. 2020;80:1026–1032. doi: 10.1055/a-1228-4242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bein B, Bachmann M, Huggett S et al. SARS-CoV-2/COVID-19: evidence-based recommendations on diagnosis and therapy. Geburtshilfe Frauenheilkd. 2020;80:491–498. doi: 10.1055/a-1156-3991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yekedüz E, Utkan G, Ürün Y. A systematic review and meta-analysis: the effect of active cancer treatment on severity of COVID-19. Eur J Cancer. 2020;141:92–104. doi: 10.1016/j.ejca.2020.09.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lee S, Lim AR, Kim MJ et al. Innovative countermeasures can maintain cancer care continuity during the coronavirus disease-2019 pandemic in Korea. Eur J Cancer. 2020;136:69–75. doi: 10.1016/j.ejca.2020.06.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Vrdoljak E, Sullivan R, Lawler M. Cancer and coronavirus disease 2019; how do we manage cancer optimally through a public health crisis? Eur J Cancer. 2020;132:98–99. doi: 10.1016/j.ejca.2020.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Moran HK, Brooks JV, Spoozak L. Undergoing active treatment for gynecologic cancer during COVID-19: A qualitative study of the impact on healthcare and social support. Gynecol Oncol Reports. 2020;34:100659. doi: 10.1016/j.gore.2020.100659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Perrone AM, Dondi G, Giunchi S et al. COVID-19 free oncologic surgical hub: The experience of reallocation of a gynecologic oncology unit during pandemic outbreak. Gynecol Oncol. 2021;161:89–96. doi: 10.1016/j.ygyno.2020.09.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.van Dam PA, Huizing M, Papadimitriou K et al. High mortality of cancer patients in times of SARS-CoV-2: Do not generalize! Eur J Cancer. 2020;138:225–227. doi: 10.1016/j.ejca.2020.07.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wright JD, Advincula AP. Gynecologic surgical considerations in the era of COVID-19. Semin Perinatol. 2020;44:151296. doi: 10.1016/j.semperi.2020.151296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Omarini C, Maur M, Luppi G et al. Cancer treatment during the coronavirus disease 2019 pandemic: Do not postpone, do it! Eur J Cancer. 2020;133:29–32. doi: 10.1016/j.ejca.2020.04.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Leung E, Pervaiz Z, Lowe-Zinola J et al. Maintaining surgical care delivery during the COVID-19 pandemic: A comparative cohort study at a tertiary gynecological cancer centre. Gynecol Oncol. 2021;160:649–654. doi: 10.1016/j.ygyno.2020.12.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Indini A, Aschele C, Cavanna L et al. Reorganisation of medical oncology departments during the novel coronavirus disease-19 pandemic: a nationwide Italian survey. Eur J Cancer. 2020;132:17–23. doi: 10.1016/j.ejca.2020.03.024. [DOI] [PubMed] [Google Scholar]
- 16.Frey MK, Fowlkes RK, Badiner NM et al. Gynecologic oncology care during the COVID-19 pandemic at three affiliated New York City hospitals. Gynecol Oncol. 2020;159:470–475. doi: 10.1016/j.ygyno.2020.09.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Matsuo K, Huang Y, Matsuzaki S et al. Effect of delay in surgical therapy for early-stage cervical cancer: An implication in the coronavirus pandemic. Eur J Cancer. 2020;139:173–176. doi: 10.1016/j.ejca.2020.08.025. [DOI] [PMC free article] [PubMed] [Google Scholar]