

Abstract
Objective:
To describe tongue pressure changes before, during, and after crib appliance therapy in mixed dentition open bite cases.
Materials and Methods:
A crib appliance was applied to each of the 13 patients in the study group. The control group consisted of six patients. Tongue pressures were measured using a diaphragm-type pressure transducer during rest position and swallowing in changing intervals for 12 months in both groups. Tongue pressures were performed on the upper first molar, upper and lower central incisors, and on the middle spur of the crib appliance.
Results:
In the study group, the initial resting tongue pressure on the upper molar increased after appliance insertion and was followed by a decreasing trend for 12 months. The resting tongue pressures on the upper and lower incisors remained lower than initial values at the end of 12 months. Swallowing pressures returned to initial values at the end of 12 months, and the changes were insignificant. The resting and swallowing tongue pressures on the middle spur of the crib appliance decreased gradually during the 10 months (P < .05). Pressure changes in the control group were insignificant for all measurements. Open bite values in the study group increased significantly by the end of 12 months.
Conclusions:
Measurements performed on the crib confirm the tongue adaptation to environmental changes. Resting tongue pressures at the 12th month remained lower than the initial values. These findings indicate adaptive behavior of the tongue to open bite closure and the new position of the incisors.
Keywords: Tongue pressure, Open bite, Pressure transducer, Crib appliance
INTRODUCTION
The etiology of open bite malocclusion lies within factors such as unfavorable growth pattern, heredity, digit habits (thumb or finger sucking), retained infantile swallowing habit, enlarged lymphatic tissue, tongue function, and posture. Because of the complex nature, etiology, and dentofacial pattern, treatment strategies may include behavior modification or orthodontic and orthopedic therapy.1,2
The question of whether muscle function affects bone morphology or adapts to local changes is still being discussed. Thus, it has been of interest to find out whether tongue thrust is a cause of anterior open bite or the reverse is true. The tongue is a powerful muscular organ that exerts strong pressure at frequent intervals during the daytime and nighttime. In tongue thrusting habits, the tongue is thrust between the upper and lower teeth each time the patient swallows.3–9
Several researchers have emphasized the importance of intraoral pressure, and tongue function has been studied by different imaging techniques. However, tongue pressure has been studied less than the pressures exerted by the lip and cheek.10–19 As a result, we aimed to investigate and discuss the changes in tongue pressure during rest position and swallowing before and after crib appliance therapy in growing subjects with anterior open bite and tongue thrust.
MATERIALS AND METHODS
Nineteen patients with anterior open bite in the mixed dentition stage with tongue thrusting were selected among the patients seeking orthodontic treatment at Marmara University Department of Orthodontics. The study group, who underwent 10 months of crib appliance therapy, consisted of 13 patients (age range: 7 years 11 months–12 years 1 month). The control group consisted of 6 patients (age range: 7 years 7 months–9 years 11 months). Tongue pressure measurements in rest position and during swallowing 10 mL of water were recorded in both groups.
All parents and guardians gave informed consent after having received a full explanation of the study. The Ethical Review Board of the Marmara University Institute of Health Sciences approved this study.
An EPL-BO diaphragm-type pressure transducer was used for the measurements (Entran-Sensors and Electronics, Fairfeld, NJ). In order to monitor the values, a Measurements Group product P-3500 Strain Indicator was used (Instruments Division, Measurement Groups Inc, Raleigh, NC). The pressure transducer was calibrated and used as described in a previous study.12
The crib appliance was bent from 0.8-mm stainless steel wire on the stone models of each patient in the study group and was adjusted to the upper molar bands. The appliance was modified for the attachment of the pressure transducer to the palatal side of the upper first molar and middle spur of the crib as seen in Figures 1 and 2a–c. Once applied, the appliance was not removed for 10 months. Acrylic caps for the upper and lower central incisors and a carrier for the upper first molar, bent from 0.7-mm stainless steel, were prepared to serve as carriers for the pressure transducer for both the study and control groups (Figure 3).
Figure 1.

Crib appliance bent on stone model from 0.8-mm stainless steel wire.
Figure 2.
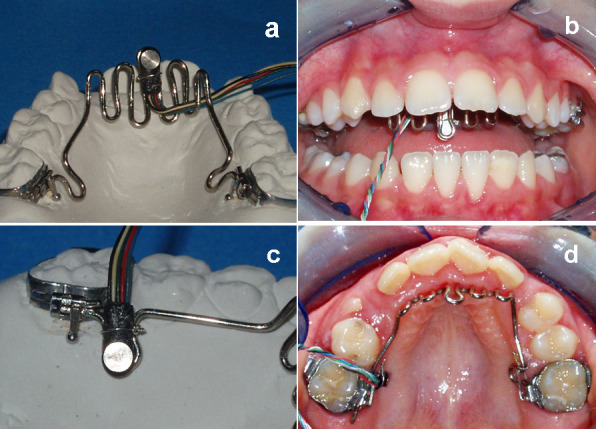
(a) Pressure transducer applied to the middle spur of the crib appliance on the stone model. (b) Pressure transducer applied to the middle spur of the crib appliance in the mouth. (c) Pressure transducer applied to the upper molar on the stone model. (d) Pressure transducer applied to the palatal side of upper molar when the crib appliance was in the mouth.
Figure 3.
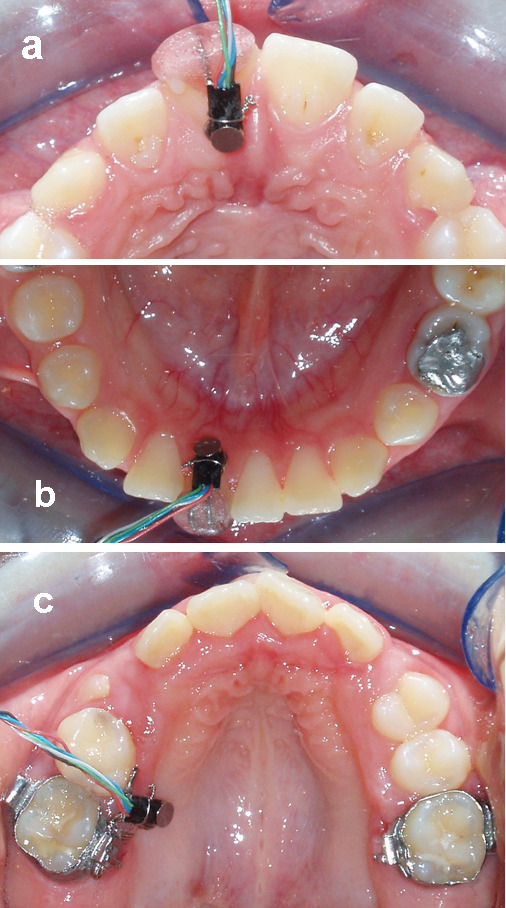
(a) Pressure transducer applied to the upper central incisor in the mouth. (b) Pressure transducer applied to the lower central incisor in the mouth. (c) Pressure transducer applied to the upper first molar in the mouth.
During measurements, the patient was seated in a dental chair with the head in the natural head position. Each swallowing measurement was repeated five times, and each time, patients were asked to swallow 10 mL of water. The average of five values was calculated. For resting tongue pressure measurements, the average of five values appearing on the screen was calculated.
Initially, resting and swallowing tongue pressures were measured from the upper right first molar and the upper and lower right central incisors in both study and control groups. These measurements were repeated at 10 and 12 months in both groups. After initial measurements, the crib was applied to the patients in the study group. Resting and swallowing tongue pressures were performed from the upper first molar and the middle spur of the crib appliance at the time of insertion, 1 week after insertion, then at 1 month, 3 months, 6 months, and 10 months. At the 10th month, when the crib was removed, and 2 months after removal of the appliance (12th month), the upper first molar and upper and lower central incisor measurements were repeated as above (Figures 2, 3).
Statistical calculations were carried out with the NCSS 2007 program (NCSS, Kaysville, Utah). The Friedman test was used in the comparison of the groups' repeated intervals. If the test revealed significance, Dunn's multiple comparison test was utilized post hoc to compare the subgroups. The Mann-Whitney U-test was used to compare groups, and the chi-square test was performed during evaluation of the qualitative data. Wilcoxon (z) was employed in the assessment of pre- and posttreatment values. Results were evaluated within a 95% confidence interval. The statistical significance level was established at P < .05. To evaluate measurement error, five patients were selected at random, and the total procedure was repeated 10 minutes later, at the same appointment. All procedures were performed by the same observer.
RESULTS
Open Bite Value
The beginning open bite value in the study group increased from −2.12 ± 1.12 mm to 0.62 ± 2.08 mm at the end of 12 months (P < .05). The difference between the groups became significant at the 12th month (Table 1).
Table 1.
Average Open Bite Values (mm) for Both Groups and Comparison Between and Within Groups

Crib Appliance
The resting tongue pressure on the crib appliance decreased from 21.09 ± 14.55 g/cm2 to 12.8 ± 2.41 g/cm2 at the end of the 10th month. Similarly, swallowing tongue pressure decreased from 216.43 ± 65.79 g/cm2 to 142.95 ± 29.2 g/cm2 at the 10th month (P < .05).
The difference between the pretreatment–10th month swallowing pressure and 1st month–10th month resting tongue pressure was statistically significant (P < .05; Table 2).
Table 2.
Median, Mean, and Standard Deviation Pressure Values (g/cm2) on Crib Appliance During Rest and Swallow

Upper First Molar
Resting tongue pressure on the upper first molar in the study group vastly increased after appliance insertion, from 16.66 ± 6.37 g/cm2 to 27 ± 11.56 g/cm2. It started decreasing by the first week, and was measured as 12.57 ± 3.65 g/cm2 at the 12th month. Swallowing tongue pressures similarly increased at the time of appliance insertion but returned to initial values at the 12th month (Tables 3, 4).
Table 3.
Median, Mean, and Standard Deviation Pressure Values (g/cm2) for Upper First Molar During Rest and Swallow

Table 4.
Statistical Significance Table for Upper First Molar Pressure Measurements During Rest and Swallow

For resting tongue pressure values, the difference between the study and control groups at the 10th and 12th months was significant. For swallowing pressures, the difference between the study and control groups at the beginning, the 10th month, and the 12th month was not statistically significant (Table 5).
Table 5.
Average Resting and Swallowing Pressure Values (g/cm2) for Upper First Molar in Study and Control Groups

Upper Central Incisor
In the study group, the initial resting tongue pressure measured 16.42 ± 8.95 g/cm2.
At the 10th month, it showed a slight decrease, and it measured 11.63 ± 4.7 g/cm2 at the 12th month. However, it remained the same in the control group, which measured 19.5 ± 14.95 g/cm2 and 19.1 ± 3.79 g/cm2 at the beginning and at the 12th month, respectively. The difference between the study and control groups for the resting pressure value at the 12th month was significant (P < .05).
Swallowing tongue pressure in the study group showed a decrease at the end of the 10th month. and it remained lower than the initial values the following 2 months. However, the differences between the study and control groups for swallowing pressures at all times were insignificant (Table 6).
Table 6.
Average Resting and Swallowing Tongue Pressure Values (g/cm2) for Upper Central İncisor in Study and Control Groups

Lower Central Incisor
During the 10 months of crib appliance wear, the resting tongue pressure in the study group decreased from 15.26 ± 5.27 g/cm2 to 11.83 ± 2.98 g/cm2 and remained lower than the initial values at the 12th month. The values remained the same in the control group. Swallowing pressures in the study group decreased at the end of the 10th month and returned to the initial values the following 2 months. However, swallowing pressure remained essentially the same in the control group at all times. Differences between the groups for resting and swallowing tongue pressures were insignificant (Table 7).
Table 7.
Average Resting and Swallowing Tongue Pressure Values (g/cm2) for Lower Central Incisor in Study and Control Groups

DISCUSSION
Anterior open bite is one of the most challenging malocclusions for orthodontists. While some authors believe the crib appliance to be a successful treatment tool and that correcting the tooth positions in open bite cases should cause changes in swallowing patterns, others claim the opposite. The main reason for this controversy might be individual variations in the adaptive capacity of the tongue.1,2 In this manner, Cleall6 carried out a study on tongue movement using cinefluorography in patients wearing a palatal crib. He reported that the crib forced the tongue to function in a posterior and higher position. Recently, Sayın et al20 studied the initial effects of the tongue crib by means of MRI. They stated that the tongue tip was positioned more posteriorly when the crib was in place and, to compensate for this posterior position, adaptive changes occurred. A lack of success with crib therapy reported by Subtelny and Sakuda2 was associated with crib wear of less than 6 months. It has been reported that using a compliance-free, fixed appliance for the correction of open bite and inhibition of habits produces more favorable results.21,22 We chose to use a fixed crib appliance that would remain in the mouth for 10 months. Our objective was to find out the effects of the crib on tongue pressures in growing subjects. We included a control group to find out whether changes were due to appliance wear or to growth itself. The control group patients, who were still in the mixed dentition stage at the end of the study, were treated immediately afterward.
Several techniques have been described for the measurement of intraoral muscle forces and pressures. Electrodynamic measurement using strain gauges have been accepted as a reliable method of evaluating forces and pressures exerted by muscles and soft tissues in various parts of the skeletal system. Besides, an EPL-BO diaphragm-pressure transducer has been reported to be the superior measuring device by many researchers.12,13,17,18,23
In evaluating intraoral pressures, the importance of repeated measurements is emphasized.11,23–25 To obtain the most accurate pressure values, we recorded the five respective values appearing on the screen during rest position. For the swallowing function, it is difficult to assess the onset and the end of the function, as there may be a preparatory activity and a complex form of multiple peaks appearing on the screen of the strain indicator. In our study, the maximum value appearing on the screen for each of five swallows was recorded.
After initial pressure measurements in both groups, we applied the crib appliance to the patients in the study group and did not remove it for 10 months in order not to disturb the expected adaptive behavior of the tongue. As the crib appliance was not removed for 10 months, upper and lower central incisor measurements in the study group could only be performed at the beginning, at 10 months (when the crib was removed), and at 12 months (2 months after removal). This is the reason the control group's measurements were performed at only three intervals.
Investigators who have carried out studies on patients wearing a palatal crib reported that the tongue adapts to the environmental changes.6–8,20 Fink26 has suggested that the effectiveness of crib or spur therapy lies not in a restraining action on the tongue dynamically, but instead lies in its ability to redirect the resting position of the tongue into a less critical posture. Related to the idea of soft tissue adaptation, Soo and Moore18 investigated intraoral lip pressures in 10 children undergoing lip bumper therapy for 8 months. They reported that resting and speaking lip pressures showed significant increases 1 month after placement and then decreased to near or below pretreatment levels by the end of the seventh month, possibly an adaptive response. Correspondingly, Moawad et al15 examined lip pressure changes after 1 week of simulated dental arch expansion. Midline lip pressure decreased significantly after the 1-week period, also suggesting an adaptive response. In our study we found decreases in resting tongue pressures and, even after removal of the crib appliance, the pressures did not return to their initial values. Our findings support the idea of soft tissue adaptation as do the studies mentioned above.
Pressures created during swallowing function are reported to be much higher than those created during rest position and phonation. The values we obtained are in line with the studies suggesting the idea.12,13,27–29
According to measurements performed on the middle spur of the crib appliance, both swallowing and resting tongue pressures showed a regular decrease during 10 months of crib wear (P < .05). These findings are in agreement with the studies supporting the soft tissue–adaptation hypothesis.6–8,20
In the study group, after installation of the appliance, both swallowing and resting pressures on the upper molar vastly increased and continued increasing during the first week. We believe that these increases are due to the restricted area and restricted forward movement of the tongue. After the first week, the values showed a gradual decrease and, even at the 10th month when the appliance was removed, the pressures remained lower than initial values. Besides, the difference between the study group and the control group was significant for the 10th- and 12th-month resting pressure values. These results call for studies to determine whether the tongue has an adaptive capability in response to environmental changes.6–8,20
For the upper and lower central incisors in the study group, swallowing tongue pressures decreased after 10 months, then returned to their initial values 2 months after removal of the appliance. The resting tongue pressure on the upper central incisor remained significantly lower when compared with the control group at the 12th month, which may indicate tongue adaptation to the new position of the incisors with open bite closure. Similarly, Fröhlich et al11 claimed that the negative correlations they found between the amount of overjet, size of the upper dental arch, and resting tongue pressure on the upper incisors confirm the hypothesis of the tongue's adaptive role. The tongue adapts to an existing morphology rather than actively molding dental arches. Similarly, Proffit30 observed lower tongue pressures in Australian Aborigines than in Americans. although Aborigines have wider dental arches.
CONCLUSIONS
Crib appliance wear resulted in a disturbance in intraoral pressure equilibrium.
Open bite closure was significant in the study group.
Resting and swallowing tongue pressures remained essentially the same in the control group.
Resting tongue pressures at the 12th month remained lower than initial values in the study group.
Swallowing tongue pressures returned to baseline values in the study group at the 12th month.
Significant decreases in resting and swallowing pressures on the crib appliance in the study group suggest tongue adaptation to the new position created by the appliance.
Acknowledgments
We would like to acknowledge the technical support of Dr Toros Alcan in this study.
REFERENCES
- 1.Epker B. N, Fish L. C. Surgical-orthodontic correction of open bite deformity. Am J Orthod. 1977;71:278–299. doi: 10.1016/0002-9416(77)90188-9. [DOI] [PubMed] [Google Scholar]
- 2.Subtelny J. D, Sakuda M. Open bite: diagnosis and treatment. Am J Orthod. 1964;50:37–58. [Google Scholar]
- 3.Bauder R, Muhl Z. Estimation of tongue volume from magnetic resonance imaging. Angle Orthod. 1991;61:175–183. doi: 10.1043/0003-3219(1991)061<0175:EOTVFM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 4.Proffit W. R. Equilibrium theory revisited: factors influencing position of the teeth. Angle Orthod. 1978;48:175–186. doi: 10.1043/0003-3219(1978)048<0175:ETRFIP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 5.Schwetska-Polly R, Engelke W, Hoch G. Electromagnetic articulography as a method for detecting the influences of spikes on tongue movement. Eur J Orthod. 1995;17:411–417. doi: 10.1093/ejo/17.5.411. [DOI] [PubMed] [Google Scholar]
- 6.Cleall J. F. Deglutition: a study of form and function. Am J Orthod. 1965;51:566–594. doi: 10.1016/0002-9416(65)90028-x. [DOI] [PubMed] [Google Scholar]
- 7.Miline I. M, Cleall J. F. Cineflourographic study of functional adaptation of the oropharyngeal structures. Angle Orthod. 1970;40:267–283. doi: 10.1043/0003-3219(1970)040<0267:CSOFAO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Subtelny J. D. Malocclusions, orthodontic corrections, and orofacial muscle adaptation. Angle Orthod. 1970;40:170–201. doi: 10.1043/0003-3219(1970)040<0170:MOCAOM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Tulley W. J. A critical appraisal of tongue thrusting. Am J Orthod. 1969;55:640–650. doi: 10.1016/0002-9416(69)90040-2. [DOI] [PubMed] [Google Scholar]
- 10.Brader A. C. Dental arch form related with intraoral forces: PR = C. Am J Orthod. 1972;61:541–561. doi: 10.1016/0002-9416(72)90106-6. [DOI] [PubMed] [Google Scholar]
- 11.Fröhlich K, Ingervall B, Thuer U. Further studies of the pressure from the tongue on the teeth in young adults. Eur J Orthod. 1992;14:229–239. doi: 10.1093/ejo/14.3.229. [DOI] [PubMed] [Google Scholar]
- 12.Küçükkeleş N, Ceylanoğlu C. Changes in lip, cheek, and tongue pressures after rapid maxillary expansion using diaphragm pressure transducer. Angle Orthod. 2003;73:662–668. doi: 10.1043/0003-3219(2003)073<0662:CILCAT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Lindemann D. E, Moore R. N. Measurement of intraoral muscle forces during functional exercises. Am J Orthod. 1990;97:289–300. doi: 10.1016/0889-5406(90)70101-H. [DOI] [PubMed] [Google Scholar]
- 14.Mitchell J. I, Williamson E. H. A comparison of maximum perioral muscle forces in North American Blacks and Whites. Angle Orthod. 1978;48:126–131. doi: 10.1043/0003-3219(1978)048<0126:ACOMPM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Moawad M. I, Shellhart W. C, Matheny J, Paterson R. L, Hicks E. P. Lip adaptation to stimulated dental arch expansion. Part 2: One week of stimulated expansion. Angle Orthod. 1996;4:255–260. doi: 10.1043/0003-3219(1996)066<0255:LATSDA>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 16.Shellhart W. C, Moawad M. I, Matheny J, Paterson R. L, Hicks E. P. A prospective study of lip adaptation during six months of simulated mandibular dental arch expansion. Angle Orthod. 1997;1:47–54. doi: 10.1043/0003-3219(1997)067<0047:APSOLA>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 17.Shellhart W. C, Moawad M. I, Paterson R. L, Matheny J. Lip adaptation to stimulated dental arch expansion. Part 1: Reliability and precision of two lip pressure measurement mechanisms. Angle Orthod. 1996;4:249–254. doi: 10.1043/0003-3219(1996)066<0249:LATSDA>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 18.Soo N. D, Moore R. N. A technique for measurement of intraoral lip pressure with lip bumper therapy. Am J Orthod. 1991;99:409–417. doi: 10.1016/S0889-5406(05)81574-4. [DOI] [PubMed] [Google Scholar]
- 19.Takahashi S, Ono T, Ishiwata Y, Kuroda T. Effect of changes in the breathing mode and body position on tongue pressure with respiratory-related oscillations. Am J Orthod. 1999;115:239–246. doi: 10.1016/S0889-5406(99)70324-0. [DOI] [PubMed] [Google Scholar]
- 20.Sayn MÖ, Akn E, Karaçay Ş, Bulakbaşı N. Initial effects of the tongue crib on tongue movements during deglutition: a cine-magnetic resonance imaging study. Angle Orthod. 2006;76:400–405. doi: 10.1043/0003-3219(2006)076[0400:IEOTTC]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 21.Cozza P, Baccetti T, Franchi L, Mucedero M. Comparison of two early treatment protocols for open bite malocclusions. Am J Orthod Dentofacial Orthop. 2007;132:743–747. doi: 10.1016/j.ajodo.2005.11.045. [DOI] [PubMed] [Google Scholar]
- 22.Giuntini V, Franchi L, Baccetti T, Mucedero M, Cozza P. Dentoskeletal changes associated with fixed and removable appliances with a crib in open-bite patients in mixed dentition. Am J Orthod Dentofacial Orthop. 2008;133:77–80. doi: 10.1016/j.ajodo.2007.07.012. [DOI] [PubMed] [Google Scholar]
- 23.Thüer U, Sieber R, Ingervall B. Cheek and tongue pressures in the molar areas and the atmospheric pressure in the palatal vault in young adults. Eur J Orthod. 1999;21:299–309. doi: 10.1093/ejo/21.3.299. [DOI] [PubMed] [Google Scholar]
- 24.Ingervall B, Thuer U. Cheek pressure and head posture. Angle Orthod. 1988;1:47–57. doi: 10.1043/0003-3219(1988)058<0047:CPAHP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 25.Peng C, Jost-Brinkmann P, Yoshida N, Chou H, Lin C. Comparison of tongue functions between mature and tongue-thrust swallowing—an ultrasound investigation. Am J Orthod Dentofacial Orthop. 2004;125:562–570. doi: 10.1016/j.ajodo.2003.06.003. [DOI] [PubMed] [Google Scholar]
- 26.Fink F. S. Resting position of tongue important [letter] Angle Orthod. 1990;60:244–245. [PubMed] [Google Scholar]
- 27.Fröhlich K, Thüer U, Ingervall B. Pressure from the tongue on the teeth in young adults. Angle Orthod. 1991;1:17–24. doi: 10.1043/0003-3219(1991)061<0017:PFTTOT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 28.Halazonetis D. J, Katsavaris E, Spyropoulos M. N. Changes in cheek pressure following rapid maxillary expansion. Eur J Orthod. 1994;16:295–300. doi: 10.1093/ejo/16.4.295. [DOI] [PubMed] [Google Scholar]
- 29.Thüer U, Ingervall B. Pressure from the lips on the teeth and malocclusion. Am J Orthod. 1986;90:234–242. doi: 10.1016/0889-5406(86)90070-3. [DOI] [PubMed] [Google Scholar]
- 30.Proffit W. R. Muscle pressures and tooth position: North American whites and Australian Aborigines. Angle Orthod. 1975;45:1–11. doi: 10.1043/0003-3219(1975)045<0001:MPATPN>2.0.CO;2. [DOI] [PubMed] [Google Scholar]