

Abstract
Background:
Symptoms of social anxiety rise rapidly during adolescence, particularly for girls. Pervasive displays of parental negative affect may increase adolescents’ fear of negative evaluation (FNE), thereby increasing risk for social anxiety symptoms. Adolescent displays of negative affect may also exacerbate parents’ social anxiety symptoms (via FNE of their child or their parenting skills), yet little research has tested transactional pathways of transmission in families. By early adolescence, rates of parent-child conflict rise, and offspring become increasingly independent in their own displays of negative affect, increasing opportunities for hypothesized transactional pathways between parent-adolescent displays of negative affect and social anxiety symptoms.
Methods:
The current study included 129 parents and daughters (11–13; no baseline social anxiety disorder), two-thirds of whom were at high risk for social anxiety due to a shy/fearful temperament. We used actor-partner interdependence models (APIM) to test whether displays of negative facial affect, assessed individually for each parent and daughter during a conflict discussion, would predict their partner’s social anxiety symptoms two years later. Automated facial affect coding assessed the frequency of negative affect during the discussion. Clinician ratings of social anxiety symptoms were completed at baseline and two-year follow-up.
Results:
Both parents and daughters who displayed more frequent negative facial affect at baseline had partners with higher follow-up social anxiety symptoms, an effect that was maintained after accounting for actors’ and partners’ baseline symptoms.
Conclusions:
Findings are consistent with intergenerational models positing that parental negative affective behaviors increase risk for adolescent social anxiety symptoms but also suggest that adolescent negative facial affect may exacerbate parental social anxiety symptoms. These bidirectional effects improve understanding of how social anxiety is maintained within a transactional family structure and highlight that displays of negative affect during parent-adolescent interaction may warrant future examination as a potential treatment target for adolescent social anxiety.
Rates and symptoms of social anxiety disorder (SAD) increase markedly during early adolescence, especially for girls (Asher, Asnaani, & Aderka, 2017). Youth with social anxiety suffer from pervasive fears of negative evaluation (FNE), resulting in high levels of avoidance, distress, and impairment (Leigh & Clark, 2018). Social anxiety runs in families (Hettema, Neale, & Kendler, 2001), and, although there is evidence for both genetic and environmental influences, intergenerational models show that the relative contribution of the environment is larger (Eley et al., 2015).
Parental affective behaviors have been identified as one pathway in the intergenerational transmission of social anxiety (Fox & Kalin, 2014), in part because chronic exposure to parental negative affect may cause or exacerbate FNE in youth (Lebowitz, Leckman, Silverman, & Feldman, 2016). The development of social anxiety is linked to increasing levels of FNE, including FNE from close family members (Rapee & Heimberg, 1997). Early adolescence is a critical developmental window during which rates of FNE precipitously rise, as reflected by increases in social anxiety symptoms and sensitivity to social evaluation during this period (Silk, Davis, McMakin, Dahl, & Forbes, 2012). Negative facial affect displayed during interpersonal interaction is often interpreted as a sign of negative evaluation (Wieser & Brosch, 2012), and individuals with, or at high risk for, social anxiety are more likely to exhibit this interpretation (Tsuji & Shimada, 2018). When parental displays of negative affect are common, as they often are among socially anxious parents (Creswell, Murray, Stacey, & Cooper, 2011), high-risk adolescents may be more likely to develop pervasive FNE, thereby facilitating the unidirectional transmission of social anxiety from parent to adolescent.
Research supports a link between parental negative affect and the subsequent development of adolescent FNE and social anxiety. First, parents may increase children’s risk for social anxiety via modeling. When children observe parents expressing FNE, in part by displays of negative facial affect, they become more likely to exhibit these expressions (Burstein & Ginsburg, 2010; De Rosnay, Cooper, Tsigaras, & Murray, 2006), an effect that is exacerbated when a parent is socially anxious (Murray, Cooper, Creswell, Schofield, & Sack, 2007). Second, the ways in which youth are taught to interpret displays of negative facial affect are important because children of socially anxious parents are more likely to interpret ambiguous social cues and situations as threatening (Podina, Mogoase, & Dobrean, 2013), in part based on how parents have interpreted ambiguous situations for them in the past (Lester, Seal, Nightingale, & Field, 2010). Finally, parental displays of negative facial affect during conflict discussions increase the probability that the adolescent will look away from the parent (Woody et al., 2020), potentially reinforcing avoidance behaviors that maintain FNE (Rapee & Heimberg, 1997). Together, these studies suggest that parents who exhibit more negative facial affect during parent-child interaction may prime their child for FNE and social anxiety.
Although the majority of research has focused on the unidirectional transmission of social anxiety from parent to child, there is preliminary evidence that youth can exacerbate parental anxiety as well (Hughes & Gullone, 2010; Whaley, Pinto, & Sigman, 1999). Early adolescence may be a critical period for such transactional effects because rates of parent-child conflict rise during this period, particularly among girls and their parents (Allison & Schultz, 2004), and early adolescents become increasingly independent in their own displays of negative affect and symptoms of social anxiety (Creswell et al., 2011). Thus, it is possible that more frequent displays of adolescent negative facial affect during parent-adolescent conflict could exacerbate social anxiety in parents. For example, parents may interpret adolescent negative facial affect as reflecting poorly on the adolescent’s social skills or that the adolescent is not listening to the parent, which might increase the parent’s perception that the adolescent will be evaluated negatively by others. Parents may also worry that adolescents’ expression of negative affect reflect negatively upon them or their parenting abilities (de Vente, Majdandžić, Colonnesi, & Bögels, 2011). This could be a critical link in understanding how social anxiety runs in families given research showing that parental fear that their child will be negatively evaluated by others mediates the relation between parent and child social anxiety and the relation between parent social anxiety and hostile/rejective parenting behaviors (de Vente et al., 2011; Schreier & Heinrichs, 2010).
Research testing bidirectional links between parent-adolescent negative facial affect and subsequent social anxiety would further our understanding of how these transactional processes support the transmission of social anxiety in families. Building from prior research, we posited that if either member of the parent-adolescent dyad exhibited more negative facial affect during interaction, then this would represent a risk factor predisposing their partner to future social anxiety symptoms. To empirically test this hypothesis, we utilized actor-partner interdependence models (APIM) (Cook & Kenny, 2005), which have been used successfully to test transactional parent-adolescent outcomes by parsing actor effects (i.e., how much an individual’s current behavior is predicted by their past behavior) from partner effects (i.e., how much an individual’s current behavior is influenced by their partner’s past behavior) (Kenny & Ledermann, 2010).
In addition to the importance of testing transactional effects, the operational definition of negative facial affect was fundamental to our hypotheses. Most past research examining facial affect and social anxiety has been constrained to still images or well-controlled facial expressions made by study confederates, both of which suffer from reduced ecological validity. However, recent technological advances have provided opportunities to assess spontaneous facial affect during live social interaction, a context that is especially relevant for social anxiety. Automated facial affect coding can quantify and classify moment-to-moment changes in facial actions that are associated with stereotypical expressions of negative emotion such as anger, fear, sadness, and disgust (Messinger et al., 2014) and offers a previously validated pathway to assess the frequency of negative facial affect during parent-adolescent interaction (Woody et al., 2020). This approach negates the labor-intensive need for manual classification, which has precluded examinations of spontaneous facial affect during live social interaction in the past. Thus, to address the limitations of prior research, the current study employed automated facial affect coding to assess the frequency of negative facial affect displayed by parents and adolescent during a conflict discussion.
In the current study, we recruited adolescent daughters between the ages of 11–13 and followed them for two years because social anxiety symptoms, particularly for girls, rise during this period (Asher et al., 2017). Although daughters were free from baseline SAD, the sample was enriched for risk due to temperament (~2/3 of girls exhibiting a shy or fearful temperament) (Clauss & Blackford, 2012), which also increased the likelihood that girls would be sensitive to parental displays of negative facial affect (Silk et al., 2012). We chose to assess negative facial affect during a conflict discussion given the greater potential for transactional effects during conflict (Allison & Schultz, 2004). We used APIM to test our hypothesis that more frequent displays of negative facial affect, from both parents and daughters, would predict increased levels of clinician-rated social anxiety symptoms in their partner from baseline to the two-year follow-up.
Methods
Participants
Participants included 129 early adolescent girls ages 11–13 and a parent. Roughly two-thirds of girls (n=85) were classified as having a fearful or shy temperament at baseline [defined as scoring 0.75SD above the mean on either the Fear or Shyness subscale of the Early Adolescent Temperament Scale–Revised (EATQ-R)(Ellis & Rothbart, 2001)]. See Table 1 for demographic and clinical characteristics and Supplement for inclusion/exclusion criteria. At baseline, parents and daughters completed a clinician-rated assessment of social anxiety symptoms and participated in a parent-daughter conflict discussion. Twenty-four months following baseline, participants completed the clinician-rated assessment of social anxiety symptoms again.
Table 1.
Demographic and Clinical Characteristics of the Sample
| Daughters | Parents | |||
|---|---|---|---|---|
| M(SD) | Skewness/Kurtosis(SE) | Parents | Skewness/Kurtosis(SE) | |
| T1 Age | 12.27(.80) | - | 42.62(6.87) | - |
| T1 Family Income | - | - | 7.07(3.19) | - |
| Female | 100% | - | 91% | - |
| Caucasian | 67% | - | 76% | - |
| Black | 19% | - | 19% | - |
| Asian | 2% | - | 1% | - |
| Native American | 1% | - | 1% | - |
| Pacific Islander | 0% | - | 1% | - |
| Multiracial | 11% | - | 2% | - |
| Hispanic | 10% | - | 5% | - |
| T1 Proportion Negative Affect | .02(.06) | 6.81(.23)/54.39(.45) | .04(.11) | 4.34(.22)/21.47(.44) |
| T1 LSAS | 24.65(18.13) | .98(.22)/.49(.43) | 24.46(20.38) | 1.55(.22)/3.66(.43) |
| T24 LSAS | 26.01(23.49) | 1.47(.26)/2.13(.52) | 26.08(18.69) | 1.09(.26)/1.00(.51) |
Note. Values are reported in either M(SD) or percent of sample; T1=Baseline and T24=24-mo follow-up; Family income was coded 1=0–10,000 to 11=100,000+.
Measures
Clinician-Rated Social Anxiety Symptoms.
Clinician ratings of social anxiety symptom severity were obtained using the Liebowitz Social Anxiety Scale (LSAS; (Liebowitz, 1987). The LSAS exhibits satisfactory reliability and validity in assessing social anxiety symptom severity (Heimberg et al., 1999; Masia-Warner et al., 2003). In the current study, inter-rater reliability was excellent for daughters (κ=.96) and parents (κ=.99).
Conflict Discussion.
Before the conflict discussion, parents and daughters separately completed an issues checklist to identify a mutually endorsed common topic of disagreement from the past month. During the five-minute discussion, they were asked to talk about the disagreement and attempt to come up with a solution (see Supplement for additional details).
Automated Facial Affect Coding.
FaceReader 7.1 (Noldus Information Technology, Inc., Leesburg, VA) was used to quantify naturally occurring parent and daughter negative facial affect throughout the conflict discussion. Parents’ and daughters’ faces were videotaped during the discussion using a sampling rate of 30 Hz and the FaceReader Observer XT program was used to classify facial actions stereotypically associated with the six “universal” emotions [happy, sad, angry, surprised, fearful, disgusted; (Ekman, 2016)] and neutral expressions. Each affect classification was assigned an intensity percentage (0–100%) at each sample measurement. Additional details regarding the classification algorithm and validation studies can be found in the Supplement. We used these classification and intensity ratings to identify the predominant affect displayed by each member of the dyad at each sample (i.e., the affect classification with the highest intensity rating that was displayed with at least 50% intensity). We separated predominant affect codes into three bins: neutral, negative (angry, disgusted, sad, fearful), and positive (happy). To calculate the proportion of time each member of the dyad displayed negative affect, we summed the number of samples that were coded as predominantly negative and then calculated the proportion of samples coded as negative relative to the total number of samples.
Analytic Plan
We used APIM as a conceptual and methodological framework to guide our data analytic plan. The key components of the APIM are actor and partner effects. An actor effect measures how much an individual’s current behavior is predicted by their own past behavior. Partner effects measure how much the individual’s current behavior is influenced by their partner’s past behavior, as well as the interdependence among partners in a dyad. A stepwise analytic approach was chosen to assess whether displays of negative affect would predict actor and partner social anxiety symptoms at the 24-mo follow-up, over and above what would be accounted for by parents’ and daughters’ baseline social anxiety symptoms and while controlling for the possibility of suppression effects (see Figure 1 for an overview). Specifically, Model 1 included parents’ and daughters’ symptoms at baseline as predictors of their and their partner’s symptoms at 24-mo follow-up. Model 2 estimated predictive relations between parents’ and daughters’ negative affect as well as their and their partner’s symptoms at 24-mo follow-up. As facilitated by our stepwise approach, together, Model 1 and 2 allowed us to test what each of our predictors (baseline symptoms vs. negative affect) could generally be expected to account for in a multivariate model predicting symptoms at 24-mo follow-up. In Model 3, both symptoms and negative affect were entered as predictors to incrementally parse out the redundant variance that is shared among the two predictors, while also estimating the incremental value of each predictor over and above effects established in Models 1 and 2. Moreover, because it controlled for baseline symptoms, Model 3 (in contrast to Model 2) allowed us to evaluate how much of the change in symptoms was accounted for by negative affect (see Supplement for additional model details).
Figure 1.
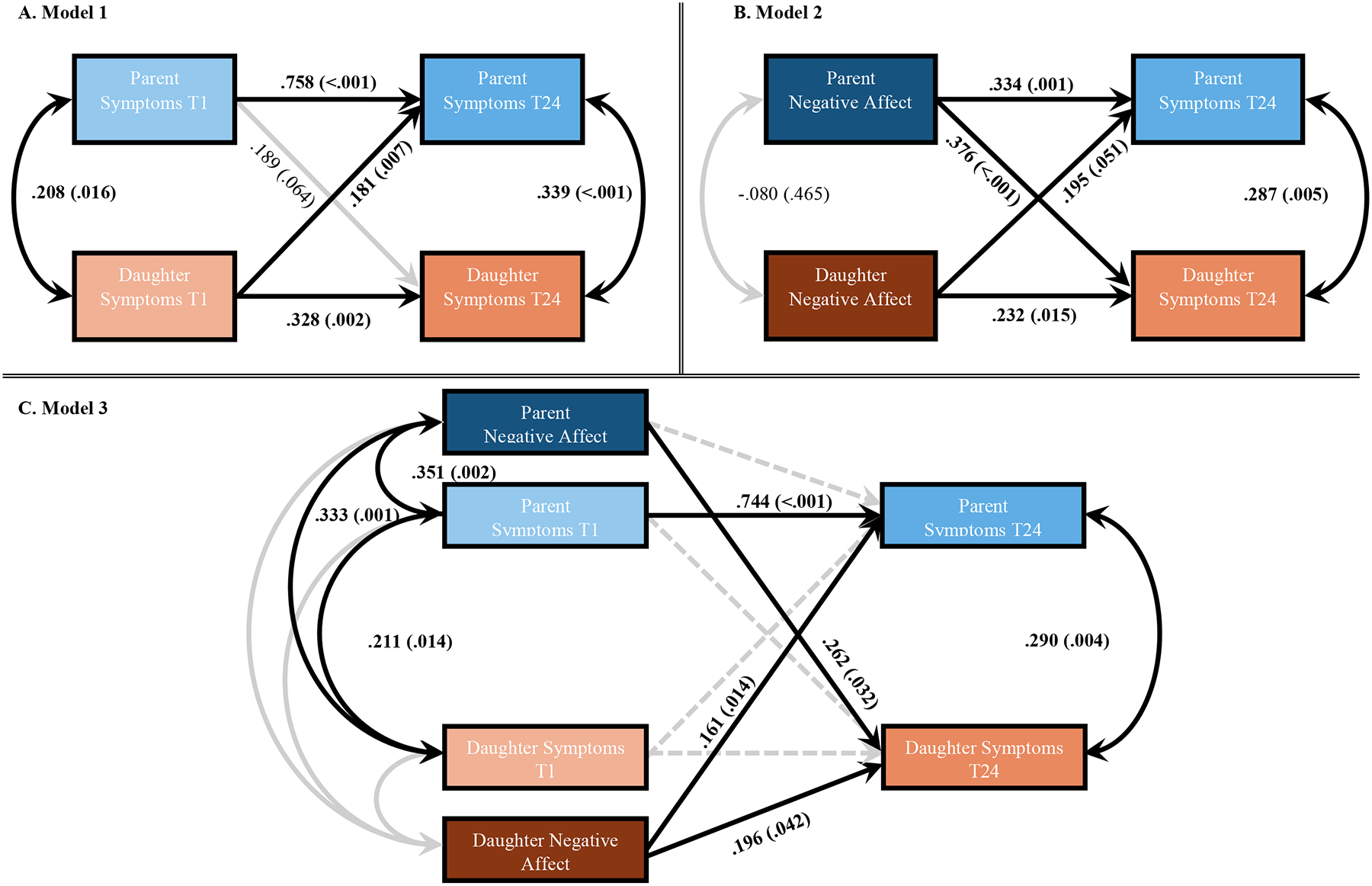
Actor-Partner Interdependence Models (APIM) with standardized coefficients and p-values.
Note. T1=baseline and T24=24-mo follow-up; Solid black lines represent significant paths; Solid grey lines represent non-significant paths; Dashed grey lines represent paths that were significant in Model 1 or 2 but were non-significant in Model 3.
All analyses were adjusted for daughters’ age at baseline and were carried out using Mplus Version 8.4 (Muthén & Muthén, Los Angeles, CA). Age was not significantly linked to any included predictor or outcome variable; therefore, respective coefficients are left out of Figure 1 for parsimony. Missing data were missing completely at random and handled using full information maximum likelihood estimation (see Supplement for missing data details). For each model, absolute fit was assessed using the χ2-test, which yields lower values for better fitting models. Given the limitations of χ2 (Hu & Bentler, 1999), we also assessed other fit indices, including root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), and comparative fit index (CFI). For RMSEA values ≤.05, for SRMR <.08, and CFI and TLI ≥.95 indicate good fit.
Results
Model 1.
Parents’ and daughters’ symptoms at 24-mo follow-up were regressed on baseline assessments of their own symptoms (actor effects), as well as the partner’s symptoms (partner effects). Model 1 allowed for actor’s symptoms to covary with their partner’s symptoms at each timepoint. Standardized coefficients and p-values for each path can be found in Figure 1A. This model fit the data very well: χ2(7)=108.586, p<.001, RMSEA=.000; CFI=1.00; TLI=1.00; SRMR=.000. For both parents and daughters, actor effects of baseline symptoms on follow-up symptoms were positive and significant, though parent actor effects were larger. At both timepoints, symptoms across partners were correlated with each other, with slightly larger coefficients at follow-up. The partner effect for daughters was significant, indicating that daughters who exhibited elevated symptoms at baseline had parents with more elevated symptoms at follow-up. The partner effect for parents was at a trend-level (p=.064).
Model 2.
Parents’ and daughters’ symptoms at 24-mo follow-up were regressed on baseline assessments of their own negative affect during the baseline conflict discussion (actor effects), as well as the partner’s negative affect (partner effects). Symptom and negative affect estimates were set to covary at both timepoints. Coefficients and p-values can be found in Figure 1B. Model fit was excellent: χ2(7)=37.165, p<.000, RMSEA=.000; CFI=1.00; TLI=1.00; SRMR=.000. We found significant, positive actor effects of negative affect on follow-up symptoms, which were slightly higher in parents compared to daughters. Follow-up symptoms across partners were significantly correlated with each other, consistent with Model 1, whereas baseline negative affect across partners was not significantly correlated. Both partner effects were significant, indicating that actors who exhibited more frequent negative affect at baseline had partners with more elevated symptoms at follow-up.
Model 3.
Both symptoms and negative affect at baseline were entered as predictors of follow-up symptoms, while allowing all predictors and outcomes to covary. Coefficients and p-values can be found in Figure 1C. This model fit the data very well: χ2(11)=119.290, p<.000, RMSEA=.000; CFI=1.00; TLI=1.00; SRMR=.000. The significant actor effect of parent baseline symptoms on follow-up symptoms was maintained, consistent with Model 1, whereas daughter actor effects were no longer significant. Partner effects of baseline symptoms on follow-up symptoms were not maintained, although parent and daughter symptoms remained significantly correlated at baseline and follow-up. Consistent with Model 2, bidirectional partner effects of negative affect on follow-up symptoms were maintained. Further, the actor effect of negative affect on follow-up symptoms was maintained for daughters; however, parent actor effects were no longer significant. In addition, Model 3 revealed that parents’ negative affect at baseline was positively associated with both parents’ and daughters’ symptoms at baseline, whereas daughters’ negative affect was neither linked to parents’ nor daughters’ baseline symptoms, nor was it related to parents’ negative affect.
Test of Robustness.
Because most parents in the sample were biological mothers (n=115), we examined whether results would differ when excluding all other parents. Findings were maintained (see Supplement).
Tests of Specificity.
We examined if findings were specific to displays of negative affect or would generalize across other affect displays. Neither positive nor neutral affect (displayed by actors) were related to partners’ follow-up symptoms (see Supplement).
Exploratory Analyses.
To examine whether the effect of actors’ negative affect (an observed display) on partners’ follow-up symptoms would be consistent with the effects of actors’ state anxiety (a subjective experience), we replaced measures of parents’ and daughters’ negative affect with their self-reported anxiety ratings collected during the conflict discussion. Results returned the same pattern, showing that parents and daughters who exhibited higher levels of objective (negative facial affect) and subjective (state anxiety) ratings of anxiety-relevant negative affect during the conflict discussion had partners with elevated symptoms at follow-up (see Supplement). In contrast, actor ratings of happiness and sadness were not related to partner follow-up symptoms (see Supplement).
Conclusions
The current study examined whether negative facial affect displayed by each member of the parent-adolescent dyad during a conflict discussion would predict social anxiety symptoms in their partner from baseline to a two-year follow-up. Our actor-partner interdependence models (APIM) allowed a robust examination of bidirectional pathways of transmission, which has been largely ignored by previous research. By including both negative facial affect and baseline social anxiety symptoms in the omnibus model, we were able to parse out the redundant variance that is shared among these two predictors while also estimating the incremental value of each predictor over and above effects established in earlier models. Notably, this incremental approach revealed that both parents and daughters who displayed more frequent instances of predominantly negative facial affect during the conflict discussion had partners with more social anxiety symptoms at two-year follow-up, an effect that was maintained even after accounting for actors’ and partners’ baseline symptoms. Tests of specificity demonstrated that transactional effects on partners’ follow-up social anxiety symptoms were specific to negative, and not positive or neutral, facial affect. Further, exploratory analyses showed that actors’ subjective experiences of anxiety, but not sadness or happiness, during the conflict discussion returned the same effect on partners’ follow-up symptoms, suggesting that both objective displays and subjective reports of actors’ anxiety-relevant negative affect exerted parallel transactional effects. Together, these findings provide support for our central hypothesis that exposure to negative affect during parent-adolescent interaction plays a bidirectional role in the intergenerational transmission of social anxiety during early adolescence.
Past research demonstrates that chronic exposure to parental negative affect may increase children’s risk for social anxiety, likely by increasing their FNE (Lebowitz et al., 2016). The current study extends our understanding of the intergenerational transmission of social anxiety by suggesting that more frequent displays of negative facial affect, made either by parents or adolescents, may increase vulnerability for future social anxiety symptoms within the family system. However, the mechanisms by which a partner’s negative facial affect exacerbates social anxiety symptoms may differ for parents versus adolescents. For adolescents, parental displays of negative facial affect are posited to exert an effect through modeling [e.g., adolescents mimicking parental affective expression, FNE, and interpretation biases; (Creswell et al., 2011)]. For parents, adolescent displays of negative affect may exacerbate parents’ existing social anxiety symptoms, perhaps inducing anxiety regarding how their child will be evaluated by others or how their child’s behavior will reflect upon them (de Vente et al., 2011; Schreier & Heinrichs, 2010). Therefore, although more frequent partner displays of negative facial affect were associated with longitudinal increases in social anxiety for both parents and adolescents, future research is needed to examine the specific ways in which each member of the parent-adolescent dyad perceives, interprets, and reacts to their partner’s displays of negative affect, as these mechanisms may uniquely maintain or increase social anxiety within the dyad.
Importantly, we examined the incremental value of actor displays of negative affect during parent-daughter interaction over and above each partner’s baseline social anxiety symptoms (thus estimating how much change in symptoms is accounted for by facial affect). Findings from the omnibus model demonstrated that partner effects of baseline social anxiety symptoms on follow-up symptoms seen in earlier models were not maintained once partner effects of displays of negative facial affect were considered, suggesting that this transactional effect was better described by the negative facial affect exhibited during the conflict discussion. These findings suggest that negative affective behavior during parent-child interaction may play a unique role in predicting the transmission of social anxiety in families, in part because it provides an opportunity to assess negative affect in the interpersonal domain, which is a critical context for the manifestation of social anxiety-relevant behaviors. Notably, displays of predominantly negative facial affect were relatively rare both in parents and daughters in the current study (on average, 4% and 2% of samples, respectively), which is consistent with other studies examining the frequency of maternal facial affect during conflict discussions (Woody et al., 2020) and observed emotional states among parent-adolescent dyads (Lougheed & Hollenstein, 2016). Given its rarity, these current findings highlight the salience and relevance of negative facial affect displays during parent-adolescent conflict discussions, especially for individuals who may be sensitive to stereotypical displays of negative affect due to social anxiety. In addition to naturalistic studies examining the intergenerational transmission of social anxiety, the use of automated facial affect coding may be useful in predicting outcomes and identifying targets of social anxiety interventions that include parents as co-clients in order to disrupt cycles of social anxiety in families (Podell & Kendall, 2011).
Although not its primary focus, the current study also provided a novel opportunity to examine actor effects of negative facial affect on the longitudinal development of social anxiety symptoms. Whereas the frequency of negative facial affect in daughters was a significant predictor of their own trajectory of social anxiety symptoms from baseline to follow-up, the same was not true for parents. Several possibilities may explain this effect. First, parent anxiety symptoms were more stable from baseline to follow-up (r=.744), compared to daughters (r=.196). This suggests that, for parents, their own negative facial affect had no incremental value in the prediction of their later social anxiety symptoms over and above baseline symptom assessments. This could reflect that levels of social anxiety symptoms are more entrenched in parents whereas adolescents may not as reliably engage in social anxiety-relevant thoughts and behaviors, leading to an increased likelihood for other intrapersonal variables, such as negative facial affect, to predict later symptoms. Second, more frequent displays of negative facial affect may exist as a trait-like vulnerability for social anxiety that exerts better predictive validity before the initial rise of social anxiety symptoms. Finally, although negative facial affect is historically conceptualized as indexing an individual’s emotional state (Buck, Savin, Miller, & Caul, 1972), it also serves as a non-verbal communication cue to others during interpersonal interaction (Dols, 2017). Parents regulate their own facial affect in part to model emotional responses for their children, whereas the reverse is not often true (Morris, Criss, Silk, & Houltberg, 2017). In contrast, adolescents may be more likely to use facial affect to convey their own intrapersonal affect to a parent. Therefore, the function of negative affect displays during a conflict discussion may be different for parents and adolescents, potentially explaining the discrepancy in actor effects seen within the current study and highlighting potential avenues for future research.
It is important to note the limits of the automated facial affect coding used in the current study. FaceReader was developed to code facial actions that are stereotypically associated with the six “universal” emotions (Ekman, 2016) and neutral states. This includes scowling as an output of anger, frowning as sadness, etc. Yet, more nuanced and culturally-sensitive models of emotion have suggested that there is no prototypic set of facial actions that can be reliably attributed per emotion (Barrett, Adolphs, Marsella, Martinez, & Pollak, 2019). For example, a wide-eyed gasp is stereotypically associated with fear, but it is not uncommon for someone to describe gasping in anger. To partially address this concern, we made an a priori decision not to examine the specific emotion classifications generated by FaceReader and to instead collapse our index of negative affect across facial actions stereotypically associated with anger, fear, disgust, and sadness. This approach likely missed facial actions that are not stereotypically associated with any of these negative emotions but representative of them, nonetheless. However, although it is in need of further refinement, we believe that the benefits of automated facial affect coding (increased ecological validity and objectivity, decreased labor burden) outweigh its limitations, especially because individuals with, or at risk for, higher levels of social anxiety symptoms are vigilant for stereotypical displays of negative emotion (Lebowitz et al., 2016; Wieser & Brosch, 2012).
Although the current study possessed significant strengths, such as examining transactional effects and in vivo negative facial affect, it also had several limitations. First, the sample was comprised of a relatively small, homogeneous group of parent-adolescent dyads (only daughters; 91% mothers; predominantly White). Replicating and extending these hypotheses using larger, more diverse samples will be essential, especially given research showing that production of and inferences about displays of facial affect can differ based on culture (Srinivasan & Martinez, 2018) and gender (Chaplin & Aldao, 2013). Second, due to social desirability demands, the laboratory environment may have limited displays of negative facial affect, as suggested by the non-normal distribution of displays of negative facial affect and zero instances of predominant negative affect displayed by almost half of parents and daughters. Although our findings suggest a protective effect of displaying little to no negative affect in the laboratory setting, future studies examining families “in the wild” would help determine if findings would be maintained under reduced social desirability demands. Finally, we only examined one component of displays of negative affect (facial actions) and future research may benefit from the inclusion of other characteristics such as vocal tone, gestures, and gaze.
In sum, the current study provides evidence for a transactional relation between parent-adolescent displays of negative facial affect and future social anxiety symptoms. More frequent displays of negative facial affect from either parents or adolescents during a conflict discussion predicted increases in social anxiety in their partner two years later, though perhaps via distinct mechanisms. Results are consistent with intergenerational transmission models of social anxiety, which posit that parental affective behaviors are related to parents’ own social anxiety and increase adolescents’ risk for the disorder and its symptoms, and provide preliminary evidence that adolescent affective behaviors influence parental social anxiety as well. In addition to improving our understanding of how social anxiety is maintained within the family structure, these bidirectional effects suggest that the parent-adolescent relationship could serve as a potentially modifiable prevention or intervention target. If replicated and extended, this research has the potential to inform efforts to understand and intervene upon the environmental inputs that shape the course of social anxiety in families.
Supplementary Material
Key Points and Relevance.
Increased parental negative affect is a putative mechanism of the intergenerational transmission of social anxiety, yet little research has examined transactional pathways between parent-adolescent negative affect and social anxiety.
This study used actor-partner interdependence models to determine whether displays of negative facial affect, assessed individually for each parent and their adolescent daughter during a conflict discussion using automated facial affect coding, would predict their partner’s social anxiety symptoms two years later.
Parents and daughters with more frequent negative facial affect had partners with higher follow-up social anxiety symptoms.
Findings suggest that negative facial affect exerts a transactional effect in maintaining social anxiety symptoms in families and that it may be an appropriate target for family-based interventions for social anxiety.
Acknowledgements
This work was supported by the NIMH under grant R01 MH103241 awarded to J.S.S and C.D.L. M.L.W. is supported by NIMH grant K23 MH119225. The authors thank members of the Families, Emotions, Neuroscience & Development laboratory for their help in conducting assessments and data acquisition for this project, Aidan Wright for his statistical consultation, and the participants of the study for their time and willingness to provide data.
Footnotes
Ethical Considerations
Parents in the study provided written consent and adolescents provided verbal assent.
References
- Allison BN, & Schultz JB (2004). Parent-adolescent conflict in early adolescence. Adolescence, 39(153), 101–119. [PubMed] [Google Scholar]
- Asher M, Asnaani A, & Aderka IM (2017). Gender differences in social anxiety disorder: A review. Clinical Psychology Review, 56, 1–12. [DOI] [PubMed] [Google Scholar]
- Barrett LF, Adolphs R, Marsella S, Martinez AM, & Pollak SD (2019). Emotional expressions reconsidered: Challenges to inferring emotion from human facial movements. Psychological Science in the Public Interest, 20(1), 1–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buck RW, Savin VJ, Miller RE, & Caul WF (1972). Communication of affect through facial expressions in humans. Journal of Personality and Social Psychology, 23(3), 362. [DOI] [PubMed] [Google Scholar]
- Burstein M, & Ginsburg GS (2010). The effect of parental modeling of anxious behaviors and cognitions in school-aged children: An experimental pilot study. Behaviour Research and Therapy, 48(6), 506–515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chaplin TM, & Aldao A (2013). Gender differences in emotion expression in children: a meta-analytic review. Psychological Bulletin, 139(4), 735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clauss JA, & Blackford JU (2012). Behavioral inhibition and risk for developing social anxiety disorder: a meta-analytic study. Journal of the American Academy of Child & Adolescent Psychiatry, 51(10), 1066–1075. e1061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cook WL, & Kenny DA (2005). The actor–partner interdependence model: A model of bidirectional effects in developmental studies. International Journal of Behavioral Development, 29(2), 101–109. [Google Scholar]
- Creswell C, Murray L, Stacey J, & Cooper P (2011). Parenting and child anxiety. Anxiety Disorders in Children and Adolescents, 2, 299–322. [Google Scholar]
- De Rosnay M, Cooper PJ, Tsigaras N, & Murray L (2006). Transmission of social anxiety from mother to infant: An experimental study using a social referencing paradigm. Behaviour Research and Therapy, 44(8), 1165–1175. [DOI] [PubMed] [Google Scholar]
- de Vente W, Majdandžić M, Colonnesi C, & Bögels SM (2011). Intergenerational transmission of social anxiety: The role of paternal and maternal fear of negative child evaluation and parenting behaviour. Journal of Experimental Psychopathology, 2(4), 509–530. [Google Scholar]
- Dols JMF (2017). Natural Facial Expression. In Dols JMF & Russell JA (Eds.), The science of facial expression (pp. 457–478). Oxford: Oxford University Press. [Google Scholar]
- Ekman P (2016). What scientists who study emotion agree about. Perspectives on Psychological Science, 11(1), 31–34. [DOI] [PubMed] [Google Scholar]
- Eley TC, McAdams TA, Rijsdijk FV, Lichtenstein P, Narusyte J, Reiss D, … Neiderhiser JM (2015). The intergenerational transmission of anxiety: a children-of-twins study. American Journal of Psychiatry, 172(7), 630–637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellis LK, & Rothbart MK (2001). Revision of the early adolescent temperament questionnaire. Paper presented at the Poster presented at the 2001 biennial meeting of the society for research in child development, Minneapolis, Minnesota. [Google Scholar]
- Fox AS, & Kalin NH (2014). A translational neuroscience approach to understanding the development of social anxiety disorder and its pathophysiology. American Journal of Psychiatry, 171(11), 1162–1173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heimberg RG, Horner K, Juster H, Safren S, Brown E, Schneier F, & Liebowitz M (1999). Psychometric properties of the Liebowitz social anxiety scale. Psychological Medicine, 29(1), 199–212. [DOI] [PubMed] [Google Scholar]
- Hettema JM, Neale MC, & Kendler KS (2001). A review and meta-analysis of the genetic epidemiology of anxiety disorders. American Journal of Psychiatry, 158(10), 1568–1578. [DOI] [PubMed] [Google Scholar]
- Hu L. t., & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. [Google Scholar]
- Hughes EK, & Gullone E (2010). Reciprocal relationships between parent and adolescent internalizing symptoms. Journal of Family Psychology, 24(2), 115. [DOI] [PubMed] [Google Scholar]
- Kenny DA, & Ledermann T (2010). Detecting, measuring, and testing dyadic patterns in the actor–partner interdependence model. Journal of Family Psychology, 24(3), 359. [DOI] [PubMed] [Google Scholar]
- Lebowitz ER, Leckman JF, Silverman WK, & Feldman R (2016). Cross-generational influences on childhood anxiety disorders: pathways and mechanisms. Journal of Neural Transmission, 123(9), 1053–1067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leigh E, & Clark DM (2018). Understanding social anxiety disorder in adolescents and improving treatment outcomes: Applying the cognitive model of Clark and Wells (1995). Clinical Child and Family Psychology Review, 21(3), 388–414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lester KJ, Seal K, Nightingale ZC, & Field AP (2010). Are children’s own interpretations of ambiguous situations based on how they perceive their mothers have interpreted ambiguous situations for them in the past? Journal of Anxiety Disorders, 24(1), 102–108. [DOI] [PubMed] [Google Scholar]
- Liebowitz M (1987). Liebowitz social anxiety scale. Modern Problems of Pharmacopsychiatry, 22, 141–173. [DOI] [PubMed] [Google Scholar]
- Lougheed JP, & Hollenstein T (2016). Socioemotional flexibility in mother-daughter dyads: Riding the emotional rollercoaster across positive and negative contexts. Emotion, 16(5), 620–633. [DOI] [PubMed] [Google Scholar]
- Masia-Warner C, Storch EA, Pincus DB, Klein RG, Heimberg RG, & Liebowitz MR (2003). The Liebowitz social anxiety scale for children and adolescents: an initial psychometric investigation. Journal of the American Academy of Child & Adolescent Psychiatry, 42(9), 1076–1084. [DOI] [PubMed] [Google Scholar]
- Messinger D, Mahoor M, Chow S, Haltigan JD, Cadavid S, & Cohn J (2014). Early emotional communication: Novel approaches to interaction. Social emotions in nature and artifact: Emotions in human and human-computer interaction, Gratch J and Marsella S, Editors, 162–180. [Google Scholar]
- Morris AS, Criss MM, Silk JS, & Houltberg BJ (2017). The impact of parenting on emotion regulation during childhood and adolescence. Child Development Perspectives, 11(4), 233–238. [Google Scholar]
- Murray L, Cooper P, Creswell C, Schofield E, & Sack C (2007). The effects of maternal social phobia on mother–infant interactions and infant social responsiveness. Journal of Child Psychology and Psychiatry, 48(1), 45–52. [DOI] [PubMed] [Google Scholar]
- Podell JL, & Kendall PC (2011). Mothers and fathers in family cognitive-behavioral therapy for anxious youth. Journal of Child and Family Studies, 20(2), 182–195. [Google Scholar]
- Podina IR, Mogoase C, & Dobrean A (2013). Intergenerational transmission of anxiety: evidence for the mediating role of the negative interpretation bias. Journal of Cognitive & Behavioral Psychotherapies, 13(2). [Google Scholar]
- Rapee RM, & Heimberg RG (1997). A cognitive-behavioral model of anxiety in social phobia. Behaviour Research and Therapy, 35(8), 741–756. [DOI] [PubMed] [Google Scholar]
- Schreier S-S, & Heinrichs N (2010). Parental fear of negative child evaluation in child social anxiety. Behaviour Research and Therapy, 48(12), 1186–1193. [DOI] [PubMed] [Google Scholar]
- Silk JS, Davis S, McMakin DL, Dahl RE, & Forbes EE (2012). Why do anxious children become depressed teenagers? The role of social evaluative threat and reward processing. Psychological Medicine, 42(10), 2095–2107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Srinivasan R, & Martinez AM (2018). Cross-cultural and cultural-specific production and perception of facial expressions of emotion in the wild. IEEE Transactions on Affective Computing. [Google Scholar]
- Tsuji Y, & Shimada S (2018). Socially Anxious Tendencies Affect Impressions of Others’ Positive and Negative Emotional Gazes. Frontiers in Psychology, 9, 2111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whaley SE, Pinto A, & Sigman M (1999). Characterizing interactions between anxious mothers and their children. Journal of Consulting and Clinical Psychology, 67(6), 826. [DOI] [PubMed] [Google Scholar]
- Wieser MJ, & Brosch T (2012). Faces in context: a review and systematization of contextual influences on affective face processing. Frontiers in Psychology, 3, 471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woody ML, Price RB, Amole M, Hutchinson E, Benoit Allen K, & Silk JS (2020). Using mobile eye‐tracking technology to examine adolescent daughters’ attention to maternal affect during a conflict discussion. Developmental Psychobiology. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.