

Abstract
The incidence of thyroid cancer continues to increase, representing the 5th most common cancer type in the USA today (Sherman, Lancet 361(9356):501–11, 2003). The current study sought to analyze the global burden of thyroid cancer utilizing the publicly accessible GLOBOCAN database. An estimated 586,202 cases of thyroid cancer were reported in 2020, making thyroid cancer the 10th most common cancer worldwide. The majority of thyroid cancer cases occurred in countries with a high or very high Human Development Index (HDI), accounting for 91% of new cases. With respect to the World Health Organization (WHO) regions, the Western Pacific had the highest incidence of thyroid cancer accounting for 47.6% of cases despite representing only 25.4% of the world’s population. Thyroid cancer incidence and mortality are expected to increase by 29.9% and 67%, respectively, by the year 2040. The African region is projected to experience the highest increase in both incidence (84.3%) and mortality (100.3%) over this time period. The results of our study demonstrate that the incidence and mortality of thyroid cancer vary by the geographic location and socio-economic status. Although the incidence was noted to be the highest in very high HDI countries and the Western Pacific region, mortality was noted to be disproportionately higher in the low HDI countries and African region. This may be due to discrepancies in access to care and/or environmental exposures such as ionizing radiation and iodine deficiency. Further measures are required to improve the outcomes from thyroid cancer regardless of the geographic location or socio-economic status.
Keywords: Thyroid cancer, Global health, Incidence, Mortality, Geography, Sociodemographics
Introduction
The incidence of thyroid cancer around the world continues to increase [1]. In the USA, thyroid cancer remains the 5th most common cancer type [1]. Differentiated thyroid cancer, including papillary and follicular thyroid cancer, is the most common subtype constituting greater than 90% of cases. The prognosis remains excellent and life expectancy of patients treated for differentiated thyroid cancer does not differ significantly from the general population [2].
Based on the classification outlined by the World Health Organization (WHO) [2], papillary cancer consists of more than ten subtypes with variable risk stratifications. Some histopathologic variants such as tall cell, columnar cell, and hobnail are associated with more unfavorable outcomes [3].
Some of the risk factors for the development of thyroid cancer include exposure to ionizing radiation via radiotherapy or nuclear fallout. Familial thyroid carcinoma and other familial syndromes increase the likelihood of thyroid cancer development. PTEN, Cowden’s disease, and multiple endocrine neoplasia type 2 (MEN2) are all syndromes associated with thyroid cancer.
Pre-operative evaluation of thyroid cancer includes a thorough neck ultrasound with imaging of the thyroid gland as well as the central and lateral neck compartments. Any concerning lymph nodes warrant a biopsy to confirm the diagnosis of locoregional metastatic disease. Surgery is the mainstay of therapy, but recommendations differ based on the size and extent of thyroid cancer. According to the latest American Thyroid Association (ATA) guidelines, patients with primary tumor size greater than 4 cm, lymph node involvement, distant metastases or extrathyroidal extension (ETE) are recommended to undergo a total thyroidectomy [3]. A compartmental lymph node dissection is indicated for positive lymph node involvement. For cancers between the size of 1 and 4 cm lacking evidence of ETE or lymph node involvement, the appropriate initial operation may be thyroid lobectomy or total thyroidectomy [3]. Thyroid cancer under 1 cm in size may be adequately treated with a thyroid lobectomy, unless clear indication for removal of contralateral lobe exists [3]. Additional treatment with radioactive iodine (RAI) depends on the risk of recurrence, but is specifically indicated for residual remnant ablation and metastatic thyroid cancer treatment.
Although the incidence of thyroid cancer is increasing, the level of increase may vary depending on the geographic location and prevalence of imaging modality utilization. Previous research has revealed that 50% of thyroid cancer global burden resides in Southern and Eastern Asia [4]. Countries with a high sociodemographic index harbor one-third of patients with thyroid cancer [4]. Further geographic evaluation may provide insight into region-based differences in thyroid cancer incidence and mortality that may improve health care resource allocation with regard to treatments and policies.
This study sought to analyze the global burden of thyroid cancer with a focus on variations in the burden of disease based on geographic location and socio-economic development.
Methods
GLOBOCAN provides access to comprehensive data on global and regional cancer burden, which is further stratified by various metrics such as geographic location and socio-economic development [5]. The accuracy of data is based on the availability of data in each country or region, which sometimes may be limited in certain low- and middle-income countries (LMICs) [5]. The sources utilized to gather data vary by individual country, and may include observational rates or country- or region-specific cancer registries. In some countries where none of the above is available, estimates are arrived based on comparable projections from other countries within geographic proximity of the index country [5]. Some of the population-based cancer registries accessed by GLOBOCAN include the International Association of Cancer Registries (IACR) and the Global Initiative for Cancer Registry Development (GICR) [5].
The publicly available GLOBOCAN database 2.0 was accessed to obtain data regarding the global burden of thyroid cancer. Intrinsic variables within the GLOBOCAN database were extracted to provide datapoints that were used to generate the results. The GLOBOCAN project combines data from 185 countries or territories around the world. It includes data on specific cancer types such as estimates of incidence, mortality, and prevalence by age and sex [5]. Details on the data source and methods have been previously described [5, 6]. The methodology of stratification based on socio-economic standing or the Human Development Index (HDI) and World Health Organization (WHO) regions has been described previously [7].
Age-standardized rate (ASR) is utilized by GLOBOCAN and this corrects for variations in burden of cancer based on age for different geographic populations. The purpose of ASR is to correct for differences in ages among countries, since age significantly impacts the risk of development of cancer and its outcomes. ASR is calculated as an average of age-specific rates per 100,000 persons over a given period of time [5].
Human Development Index (HDI) accounts for socio-economic status of various countries by summarizing three areas of human development including life expectancy at birth and literacy rates among adults as well as tertiary education enrollment rates and gross domestic product per head adjusted for purchasing-power parity [8]. Based on the HDI, individual countries are divided into four categories, namely low HDI-LHDI (HDI < 0.550), medium HDI-MHDI (HDI ≥ 0.550), high HDI-HHDI (HDI ≥ 0.700), and very high HDI-VHHDI (HDI ≥ 0.800) [8]. The countries included within each category are again available on the GLOBOCAN website [5, 8].
A list of cancer registries that contributed to the GLOBOCAN data can be found on their website [5]. The methods used to estimate the age- and sex-specific incidence and mortality rates by cancer are based on the specific country and are summarized on the GLOBOCAN website [5]. The prevalence estimates were calculated using a formula provided on the GLOBOCAN website for review [5, 9].
Results
An estimated 586,000 cases of thyroid cancer were reported worldwide in 2020 (Table 1), which makes thyroid cancer the 10th most common cancer (Fig. 1). Female incidence was estimated at 449,000 compared to male incidence of 137,000, making thyroid cancer three times more common among females (Table 1). However, mortality rates remain low, but differ by gender. Mortality among males totaled 15,900 compared to 27,700 deaths in females (Table 1). Compared another way, cumulative risk for females is estimated at 0.05 compared to males at 0.04, making male mortality from thyroid cancer disproportionate to the incidence (Table 1).
Table 1.
| Thyroid | 2020 | 2040 | % increase |
|---|---|---|---|
| Estimated number of cases from 2020 to 2040 | |||
| World incidence | 586,000 | 761,000 | 29.9 |
| Males | 137,000 | 185,000 | 34.8 |
| Females | 449,000 | 576,000 | 28.4 |
| World mortality | 43,600 | 72,900 | 67 |
| Males | 15,900 | 26,700 | 67.9 |
| Females | 27,700 | 46,200 | 66.5 |
| All cancers excluding non-melanoma skin cancer | |||
| World incidence | 18,100,000 | 28,000,000 | 56.7 |
| Males | 9,340,000 | 15,000,000 | 62.5 |
| Females | 8,750,000 | 13,000,000 | 50.3 |
| World mortality | 9,890,000 | 16,200,000 | 63.7 |
| Males | 5,490,000 | 9,150,000 | 66.8 |
| Females | 4,400,000 | 7,030,000 | 59.8 |
Fig. 1.
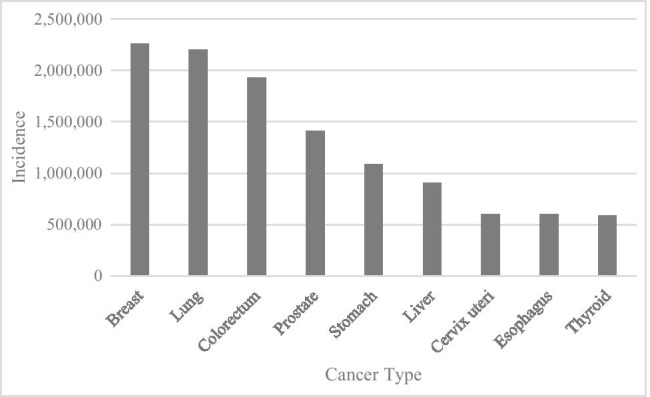
Incidence of the ten most prevalent cancers worldwide in 2020 [13, 14]
Thyroid cancer was responsible for approximately 43,600 (previously recorded as 41,071 in 2018) deaths in 2020 (Table 1). The majority of thyroid cancer cases occurred in countries with high or very high HDI with incidence rates of 321,625 (compared to 276,499 in 2018) and 212,643 (220,219 in 2018), respectively (Tables 2 and 3). The vast majority of worldwide case numbers are represented by these countries with high HDI status at 91% (previously 88% in 2018). However, the mortality from thyroid cancer in countries with high and very high HDI accounts for only 73% (previously 66% in 2018) of the deaths (Tables 2 and 3).
Table 2.
Incidence and mortality of thyroid cancer in 2020 by the WHO region, continent, and HDI status [13, 14]
| Thyroid cancer incidence | Thyroid cancer mortality | 5-year prevalence number | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Number | Rank | % | Cum Risk | Number | Rank | % | Cum Risk | Number | |
| WHO region | |||||||||
| African region (AFRO) | 11,756 | 16 | 1.4 | 0.18 | 3233 | 25 | 0.59 | 0.07 | 28,747 |
| Americas region (PAHO) | 125,624 | 5 | 3.1 | 1.03 | 6826 | 24 | 0.48 | 0.05 | 453,429 |
| East Mediterranean region (EMRO) | 21,882 | 12 | 3 | 0.34 | 3403 | 21 | 0.74 | 0.07 | 58,014 |
| Europe region (EURO) | 104,193 | 14 | 2.2 | 0.83 | 7637 | 26 | 0.35 | 0.04 | 359,139 |
| South-East Asia region (SEARO) | 43,651 | 16 | 1.9 | 0.21 | 8619 | 25 | 0.6 | 0.05 | 122,887 |
| Western Pacific region (WPRO) | 279,035 | 9 | 4.2 | 1.04 | 13,923 | 23 | 0.35 | 0.04 | 929,077 |
| Continents | |||||||||
| World | 586,202 | 10 | 3 | 0.68 | 43,646 | 25 | 0.44 | 0.05 | 1,984,927 |
| Africa | 18,457 | 15 | 1.7 | 0.22 | 4443 | 22 | 0.62 | 0.07 | 47,595 |
| Latin America/Caribbean | 63,368 | 6 | 4.3 | 0.86 | 4406 | 24 | 0.62 | 0.06 | 209,541 |
| Northern America | 62,256 | 12 | 2.4 | 1.26 | 2420 | 25 | 0.35 | 0.03 | 243,888 |
| Asia | 349,897 | 10 | 3.7 | 0.65 | 25,668 | 24 | 0.44 | 0.05 | 1,139,172 |
| Europe | 87,162 | 15 | 2 | 0.83 | 6399 | 27 | 0.33 | 0.04 | 325,708 |
| Oceania | 5062 | 10 | 2 | 1 | 310 | 24 | 0.45 | 0.05 | 19,023 |
| HDI status | |||||||||
| Low HDI | 10,508 | 16 | 1.6 | 0.19 | 3220 | 22 | 0.73 | 0.08 | 21,835 |
| Medium HDI | 41,225 | 17 | 1.8 | 0.18 | 8368 | 25 | 0.55 | 0.05 | 111,316 |
| High HDI | 321,625 | 9 | 4.4 | 0.88 | 18,934 | 23 | 0.42 | 0.05 | 1,056,960 |
| Very high HDI | 212,643 | 14 | 2.4 | 1 | 13,117 | 25 | 0.38 | 0.04 | 794,816 |
Table 3.
| 2020 | 2040 | |||
|---|---|---|---|---|
| Continent | Incidence | Mortality | Incidence (% increase) | Mortality (% increase) |
| Asia | 349,897 | 25,668 | 442,929 (26.6) | 45,639 (77.8) |
| Europe | 87,162 | 6399 | 85,490 (− 1.9) | 8264 (29.1) |
| Latin America and Caribbean | 63,368 | 4406 | 83,361 (31.6) | 7987 (81.3) |
| Northern America | 62,256 | 2420 | 71,055 (14.1) | 3625 (49.8) |
| Africa | 18,457 | 4443 | 34,006 (84.2) | 8901 (100.3) |
| Oceania | 5062 | 310 | 6635 (31.1) | 486 (56.8) |
ASR incidence in 2020 was the highest in the Republic of Korea at 26.6. For comparison, the USA ranks 14th in terms of estimated ASR incidence rate in 2020, which equates to a value of 11.8 (Table 4). When comparing mortality, however, the US rates are equivalent to the Republic of Korea at 0.3 (Table 4). Both countries are considered very high HDI countries. The highest ranking mortality with an ASR of 2.7 is the country of Samoa, a Polynesia island group, which has a corresponding ASR incidence of 8.9 (Table 4). Samoa is considered a high HDI country. Disparities may exist between countries in terms of stage of disease at diagnosis and access to intervention for cure.
Table 4.
| Thyroid cancer incidence | Thyroid cancer mortality | |||
|---|---|---|---|---|
| Continent | Number | ASR | Number | ASR |
| Asia | 349,897 | 6.4 | 25,668 | 0.44 |
| Republic of Korea | 17,788 | 26.6 | 386 | 0.30 |
| Europe | 87,162 | 8.3 | 6399 | 0.33 |
| Latin America and the Caribbean | 63,368 | 8.6 | 4406 | 0.53 |
| North America | 62,256 | 12.4 | 2420 | 0.30 |
| USA | 52,912 | 11.8 | 2161 | 0.30 |
| Africa | 18,457 | 2.0 | 4443 | 0.62 |
| Ethiopia | 3203 | 4.3 | 927 | 1.5 |
| Egypt | 2661 | 2.9 | 472 | 0.61 |
| Oceania | 5062 | 9.7 | 310 | 0.45 |
| Samoa | 15 | 8.9 | 4 | 2.7 |
Breakdown of thyroid cancer by the WHO region revealed the Western Pacific region to have the highest rates of thyroid cancer diagnoses in 2020 at 279,035 making it the 9th most common cancer type in that area (Table 2). Compared to population percentage, the Western Pacific region accounts for 25.4% of the world’s population as of 2018, but accounts for 47.6% of thyroid cancer cases and 31.9% of deaths attributed to the disease in 2020 (Table 2). The African region had the highest percentage of cases resulting in mortality (number of deaths due to thyroid cancer divided by prevalence of thyroid cancer cases multiplied by 100) at 11.25%. This was followed by the South-East Asia region at 7.01% with single digit percentages for the remaining regions (5.87%, 2.13%, 1.51%, and 1.49% for the East Mediterranean region, Europe region, Americas region, and Western Pacific region, respectively).
Although not entirely explicable by income status, the Africa region has the lowest gross domestic product (GDP) value per capita of the WHO regions. Economic status also appears to play a role in the outcomes of patients with thyroid cancer based on HDI status. Although the greatest number of cases by incidence rates is noted in the high to very high HDI groups, when comparing prevalence to mortality, the low HDI group has the highest ratio (mortality divided by prevalence × 100). The highest proportion of thyroid cancer–related mortality compared to prevalence was in the low HDI group at 14.75 followed by the medium HDI group at 7.52 (Table 2).
Overall, the estimated number of incident cases of all types of cancer from 2020 to 2040 is expected to increase by 56.7% (Table 1). Thyroid cancer, in particular, is projected to increase 29.9% over the same time period (Table 1; Fig. 2a). Mortality from thyroid cancer, however, is estimated to increase by 67% for both sexes (Fig. 2b). Again, thyroid cancer incidence is projected to increase by the greatest percentage in the WHO Africa region at 84.2 (Table 3). This also corresponds to projected increase in mortality due to thyroid cancer in the same region at 100.3%, which is the most significant predicted increase among all WHO regions (Table 3). Thyroid cancer’s increase in incidence, which is partially attributed to increased utilization of imaging modalities, may begin to eventually plateau. However, the steady increase in mortality may be due to extraneous factors which are thought to contribute to the development of thyroid cancer such as environmental exposures and obesity. Additional studies may reveal causal relationships that would potentially influence development of the disease and outcomes.
Fig. 2.
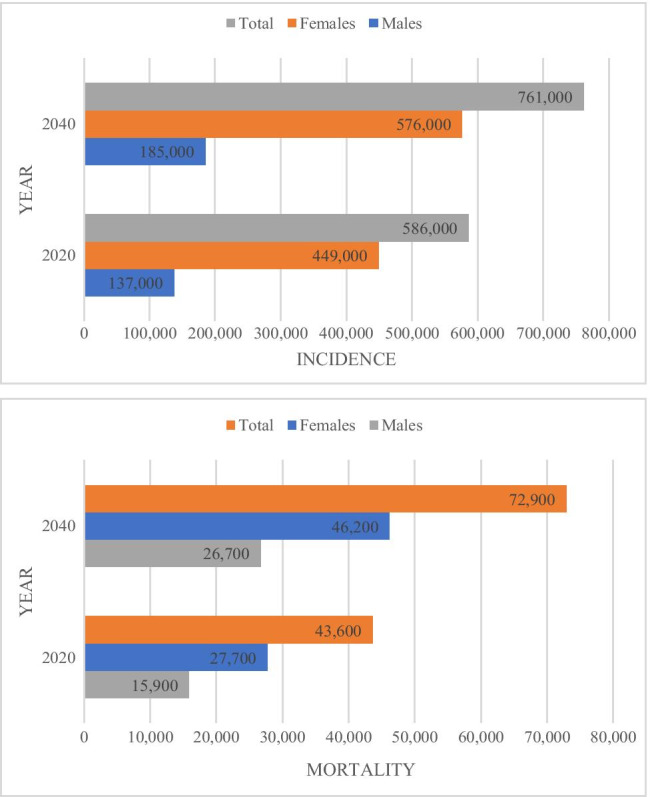
a Projected incidence of thyroid cancer by sex from 2020 to 2040 [1, 2]. b Projected mortality of thyroid cancer by sex from 2020 to 2040 [1, 2]
Discussion
The aim of this study was to evaluate the trends and analyze the burden of thyroid cancer around the globe. The burden of disease is projected to increase, as is the associated malignancy-related death rate. The incidence of disease does not uniformly impact all areas of the world and varies by socio-economic development. This may point to decreased access to imaging modalities, such as ultrasound, and access to care in general. As a counter point, thyroid cancer may be over-diagnosed in high-income countries, which may not contribute to a large burden on mortality.
It has been suggested that geographic areas across the globe with previously high mortality rates secondary to thyroid carcinoma included regions with iodine deficiency [10]. Iodine deficiency is associated with benign thyroid disease, which is a known risk factor for the development of thyroid carcinoma, such as iodine-deficient goiter [11].
Another known risk factor for the development of thyroid cancer is ionizing radiation. Improved control of nuclear waste may be contributing to decline in thyroid cancer mortality [12].
Limitations
Limitations from this study include those from data source collection and also from thyroid cancer knowledge gaps, in general. Thyroid cancer development likely has multiple contributing factors ranging from environmental exposures to diet and lifestyle. Many of these remain undefined and future studies are required to elicit true contributions.
GLOBOCAN data does not distinguish thyroid cancer subtypes, but rather groups thyroid cancer as a whole. Thyroid cancer subtypes are not clarified and therefore, understanding mortality risk is limited. In particular, distribution of high-risk subtypes of thyroid cancer is unknown, which may alter mortality rates.
Additional limitations are inherently based on the GLOBOCAN database, which have previously been described [7]. Data collected based on cancer registries or estimates from neighboring country’s cancer registries may limit application of these results. Compared with developed countries, less developed countries may have incomplete population and mortality estimates, affecting the accuracy of rates. Additionally, cancer registries in less developed countries are likely representative of metropolis regions, thereby not a true representation of the country as a whole.
This study is not intended to be utilized to determine causality or factors influencing mortality of thyroid cancer. Results may reveal geographic disparities that allude to potential environmental exposures that encourage development of thyroid cancer and may be helpful for future studies. In summary, thyroid cancer disease burden has and is increasing around the globe, but certain geographic locations and socio-economic factors may influence the disparities demonstrated in this study.
Conclusions
The majority of thyroid cancers have an overall excellent prognosis. Revealing underlying discrepancies between geographic areas in terms of mortality may be beneficial in order to level the mortality rates by improving cancer care. Given the highlighted anticipated continued increase in thyroid cancer incidence regardless of geography, an importance must be placed on outcomes. In particular, low HDI groups and the WHO Africa region have unexpectedly high mortality to prevalence ratios, indicating an area in need of improvement. This may be due to inherently prevalent environmental exposures and development of specific thyroid cancer subtypes; however, it may also be due to problems with access to care and early cancer detection. Additional studies evaluating timing and stage of disease at diagnosis may elicit the cause of the prevalence to mortality discrepancy based on geographic region. Environmental exposure studies would aid in proper risk stratifying in particular areas at risk. This important work has lent toward exposing underlying differences based on population groups that hopefully initiates the development of future studies, which will narrow the profound treatment gap in thyroid cancer treatment and thereby improve outcomes globally.
Author Contribution
Not applicable.
Data Availability
Publicly accessible GLOBOCAN database.
Code Availability
Not applicable.
Declarations
Conflict of Interest
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Sherman SI. Thyroid carcinoma. Lancet. 2003;361(9356):501–511. doi: 10.1016/s0140-6736(03)12488-9. [DOI] [PubMed] [Google Scholar]
- 2.Schmidbauer B, Menhart K, Hellwig D, et al. Differentiated thyroid cancer-treatment: state of the art. Int J Mol Sci. 2017;18(6):1292. doi: 10.3390/ijms18061292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Haugen BR, Alexander EK, Bible KC, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133. doi: 10.1089/thy.2015.0020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Deng Y, Li H, Wang M, et al. Global burden of thyroid cancer from 1990 to 2017. JAMA Netw Open. 2020;3(6):e208759. doi: 10.1001/jamanetworkopen.2020.8759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ferlay J, Ervik M, Lam F et al. (2020) Global Cancer Observatory: cancer today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today.
- 6.Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):e359–e386. doi: 10.1002/ijc.29210. [DOI] [PubMed] [Google Scholar]
- 7.Are C, Chowdhury S, Ahmad H, et al. Predictive global trends in the incidence and mortality of pancreatic cancer based on geographic location, socio-economic status, and demographic shift. J Surg Oncol. 2016;114(6):736–742. doi: 10.1002/jso.24410. [DOI] [PubMed] [Google Scholar]
- 8.Bray F, Jemal A, Grey N, et al. Global cancer transitions according to the human development index (2008–2030): a population-based study. Lancet Oncol. 2012;13(8):790–801. doi: 10.1016/S1470-2045(12)70211-5. [DOI] [PubMed] [Google Scholar]
- 9.Engholm G, Ferlay J, Christensen N, et al. NORDCAN–a Nordic tool for cancer information, planning, quality control and research. Acta Oncol. 2010;49(5):725–736. doi: 10.3109/02841861003782017. [DOI] [PubMed] [Google Scholar]
- 10.Kolonel LN, Hankin JH, Wilkens LR, et al. An epidemiologic study of thyroid cancer in Hawaii. Cancer Causes Control. 1990;1(3):223–234. doi: 10.1007/BF00117474. [DOI] [PubMed] [Google Scholar]
- 11.Franceschi S, Preston-Martin S, Dal Maso L et al. (1999) A pooled analysis of case-control studies of thyroid cancer. IV. Benign thyroid diseases. Cancer Causes Control 10(6):583–95. 10.1023/a:1008907227706. [DOI] [PubMed]
- 12.Cardis E, Kesminiene A, Ivanov V, et al. Risk of thyroid cancer after exposure to 131I in childhood. J Natl Cancer Inst. 2005;97(10):724–732. doi: 10.1093/jnci/dji129. [DOI] [PubMed] [Google Scholar]
- 13.Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi: 10.3322/caac.21492. [DOI] [PubMed] [Google Scholar]
- 14.Ferlay J, Colombet M, Soerjomataram I, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144(8):1941–1953. doi: 10.1002/ijc.31937. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Publicly accessible GLOBOCAN database.
Not applicable.