

Abstract
A significant proportion of patients with Crohn’s disease (CD) present with, or progress to, moderate to severe disease activity. These patients are at high-risk for surgery, hospitalization, disease-related complications, corticosteroid-dependence, and serious infections. Optimal management of outpatients with moderate-severe luminal and/or fistulizing (including perianal) CD often requires the use of immunomodulator (thiopurines, methotrexate) and/or biologic therapies including tumor necrosis factor (TNF)-α antagonists, vedolizumab, or ustekinumab, either as monotherapy, or in combination (with immunomodulators), to mitigate these risks. Decisions about optimal drug therapy in moderate-severe CD are complex, with limited guidance on comparative efficacy and safety of different treatments, leading to considerable practice variability. Since the last iteration of these guidelines published in 2013, significant advances have been made in the field, including the regulatory approval of two new biologic agents, vedolizumab and ustekinumab. Therefore, the American Gastroenterological Association prioritized updating clinical guidelines on this topic. To inform the clinical guidelines, this technical review was completed in accordance with the GRADE framework. The review addressed the following focused questions (in adult outpatients with moderate-severe luminal CD): (1) overall and comparative efficacy of different medications for induction and maintenance of remission in patients with or without prior exposure to TNF-α antagonists, (2) comparative efficacy and safety of biologic monotherapy vs. combination therapy with immunomodulators, (3) comparative efficacy of a top-down (upfront use of biologics and/or immunomodulator therapy) vs. step-up treatment strategy (acceleration to biologic and/or immunomodulator therapy only after failure of 5-aminosalicylates), and (4) role of corticosteroids and 5-aminosalicylates for induction and/or maintenance of remission. Finally, in adult outpatients with moderate-severe fistulizing CD, this review addressed: (5) efficacy of pharmacological interventions for achieving fistula, and (6) role of adjunctive antibiotics without clear evidence of active infection.
INTRODUCTION
Crohn’s disease (CD) is a chronic inflammatory bowel disease that generally begins in young adulthood and lasts throughout life. Although the incidence and prevalence of CD has stabilized in Western Europe and North America (affecting >0.2% of the population), its incidence continues to rise in newly industrialized countries.1 Based on population-based cohort studies, the majority of patients with CD have a relapsing-remitting course, with >50% patients requiring corticosteroids during the course of their disease.2 Historically, prior to the introduction of biologic agents, approximately 20% patients with CD would be hospitalized every year, and 1-, 5- and 10-year risk of surgery in patients with CD was 24%, 36% and 47%, respectively.3 Over the last two decades, several therapeutic measures have improved disease outcomes including: (1) earlier diagnosis, (2) introduction and increasing uptake of biologic agents like tumor necrosis factor (TNF)-α antagonists, (3) changes in approach to management of IBD with targeted use of disease-modifying immunosuppressive therapy with treatment intensification based upon systematic evaluation of symptoms and disease activity, and (4) earlier detection and endoscopic management of colorectal neoplasia4. Consequently, in the biologic era, 1- and 5-year risk of hospitalization is 26% and 40%, respectively, and 1-, 5- and 10-year risk of surgery in patients with CD is 12%, 18% and 26%, respectively.5, 6
Conventionally, clinical trials have focused on (cross-sectional) disease activity assessment, leading to regulatory approval and real-world use of immunosuppressive and/or biologic therapies for patients with moderate to severely active disease after failure of conventional therapy. However, over the last decade, there is increasing recognition that (longitudinal) disease severity assessment, which accounts for cumulative disease-related damage and impact of disease on lifestyle is vital, to risk-stratify patients and ensure timely initiation of risk-congruent disease-modifying therapy.7 The number of pharmacologic agents available to treat moderate-severe CD has grown over the last 7 years since the last iteration of this guideline, and now includes an anti-integrin agent (vedolizumab) and an interleukin 12/23 antagonists (ustekinumab), with several others in the pipeline. With the availability of multiple treatment options with differences in efficacy and safety profiles, there is considerable practice variability in the use of these drugs in the treatment of outpatients and inpatients with moderate-severe CD.8, 9 Variations in practice may have unintended negative consequences in patient outcomes. Therefore, the American Gastroenterological Association (AGA) prioritized updating prior clinical guidelines on the topic.10
Objectives of the Review
This technical review focuses on drugs and treatment strategies for the management of adult (≥18 years) outpatients with moderate-severe luminal and/or fistulizing (including perianal) CD. Patients with moderate-severe luminal CD are those with moderate to severe disease activity based on the Crohn’s disease activity index, patients who are corticosteroid-dependent or corticosteroid-refractory CD, and/or patients with severe endoscopic disease activity (large and/or deep ulcers). While we intended to address management of fistulizing CD, most of the evidence for fistulizing disease is reported for perianal CD.
This technical review addresses the following clinical questions:
Overall and comparative efficacy and safety of pharmacological therapies including thiopurines, methotrexate, TNF-α antagonists (infliximab, adalimumab, certolizumab pegol), vedolizumab, natalizumab and ustekinumab for the induction and maintenance of remission in adult outpatients with moderate-severe CD, in patients with or without prior exposure to TNF-α antagonists;
Comparative efficacy and safety of biologic monotherapy vs. in combination with immunomodulator agents (thiopurines or methotrexate) for the induction and maintenance of remission in adult outpatients with moderate-severe CD;
Comparison of a top-down (upfront use of biologics and/or immunomodulator therapy) vs. step-up treatment strategy (acceleration to biologic and/or immunomodulator therapy only after failure of 5-aminosalicylates [5-ASA]) in adult outpatients with moderate-severe CD;
Role of corticosteroids or 5-ASA for the induction and maintenance of remission in adult outpatients with moderate-severe CD
In adult outpatients with fistulizing CD, what is the efficacy and safety of the following drugs: TNF-α antagonists (infliximab, adalimumab, certolizumab pegol), vedolizumab, and ustekinumab, immunomodulator monotherapy (thiopurines, methotrexate), antibiotics?
In adult patients with fistulizing CD (without abscess), is adding antibiotics to standard medical management superior to medical management alone?
This technical review does not address the role of therapeutic drug monitoring in management of biologic-treated patients with IBD (see separate AGA guideline and technical review),11, 12 optimal treatment targets and monitoring strategies in patients with moderate-severe CD, impact of pharmacological interventions on the risk of colorectal neoplasia in patients with CD, role of biosimilars in the management of CD or the surgical management of patients with moderate-severe luminal and/or perianal CD. The results of this technical review were used to inform the development of the accompanying clinical guidelines on the pharmacological management of patients with moderate-severe luminal and fistulizing CD.
METHODS
Overview
This technical review and the accompanying guideline were developed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework. The members of the technical review panel were selected based on their clinical expertise and methodological training in guideline development. They went through a thorough vetting process for potential conflicts of interest in accordance with the AGA Conflict of Interest Disclosure Process. Through an iterative process, the participants developed focused clinical questions on the pharmacological management of moderate-severe CD, updating prior questions and adding new questions of interest. After the focused questions were approved by the AGA Governing Board (on September 3, 2019), the technical review team identified relevant outcomes, systematically reviewed and summarized the evidence for each outcome across studies, and then rated the certainty of the evidence across all outcomes for each clinical question.
Formulation of Clinical Questions and Outcome Measurement
Using the PICO format, which frames a clinical question by defining a specific Population (P), Intervention (I), Comparator (C), and Outcomes (O), the team finalized 11 questions to be addressed (Table 1). In outpatients with moderate-severe luminal CD, induction and maintenance of clinical remission were considered critical outcomes for decision-making, whereas achieving endoscopic remission, corticosteroid-free remission and serious adverse events (serious infections and malignancy) were considered important outcomes. While the technical review panel recognized discordance between clinical symptoms and endoscopic activity in patients with CD, clinical remission was deemed to be a more patient-centered outcome that led to regulatory approval of all biologic agents. Patient surveys have suggested that patients perceive improving quality of life and complete resolution of symptoms as treatment objectives; only 12.8% prioritize normalization of colonoscopy as treatment objective.13 Clinical remission was most commonly measured using the Crohn’s disease activity index (CDAI), based on abdominal pain, bowel movements, general wellbeing, complications of disease, abdominal mass, anemia and weight change. In this scale, scores <150 suggest clinical remission, and scores 150–220, 221–450 and >450 denoting mild, moderate and severe disease, respectively.14 For the specific question on efficacy of a strategy of top-down therapy vs. gradual step-up therapy, preventing disease-related complications and surgery was deemed to be the critical outcome. In outpatients with moderate-severe fistulizing CD, induction and maintenance of fistula remission (generally defined as complete cessation of fistula drainage) was considered critical outcome.
Table 1.
Focused clinical questions on the pharmacological management of moderate to severe Crohn’s disease, and corresponding questions in PICO format addressed in this technical review
| S# | Focused Question | PICO Question | |||
|---|---|---|---|---|---|
| Patients | Intervention | Comparator | Critical Outcomes | ||
| OUTPATIENTS with MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | |||||
| 1A. | In adult outpatients with moderate to severe CD, what is the overall efficacy of TNF-α antagonists (infliximab, adalimumab, certolizumab pegol), vedolizumab and ustekinumab for induction and maintenance of remission? | Adult outpatients with moderate to severe CD |
|
Placebo |
|
| 1B. | In adult outpatients with moderate to severe CD, what is the efficacy and safety of natalizumab? | Adult outpatients with moderate to severe CD |
|
Placebo |
|
| 2. | In adult outpatients with moderate to severe CD, what is the comparative efficacy of different biologic agents (infliximab, adalimumab, certolizumab pegol, vedolizumab, ustekinumab), in biologic-naïve and in patients with prior TNF-α antagonist exposure, for induction and maintenance of remission? | Adult outpatients with moderate to severe CD, (A) biologic-naïve and (B) prior exposure to TNF-α antagonist |
|
Placebo or another active comparator |
|
| 3. | In adult outpatients with moderate to severe CD, what is the efficacy of immunomodulator monotherapy (thiopurines, methotrexate) for induction and maintenance of remission? | Adult outpatients with moderate to severe CD |
|
Placebo (or 5-aminosalicylates) |
|
| 4. | In adult outpatients with moderate to severe CD, is biologic monotherapy (infliximab, adalimumab, certolizumab pegol, vedolizumab, ustekinumab superior to immunomodulator monotherapy (thiopurines, methotrexate) for induction and maintenance of remission? | Adult outpatients with moderate to severe CD | Monotherapy with
|
Immunomodulators (thiopurines or methotrexate) |
|
| 5. | In adult outpatients with moderate to severe CD, is combination therapy of a biologic agent (infliximab, adalimumab, certolizumab pegol, vedolizumab, ustekinumab) with an immunomodulator (thiopurines or methotrexate) superior to biologic monotherapy for induction and maintenance of remission? | Adult outpatients with moderate to severe CD | Combination therapy with of a biologic agent (infliximab, adalimumab, certolizumab pegol, vedolizumab, ustekinumab) + immunomodulator (thiopurines or methotrexate) |
|
|
| 6. | In patients with quiescent CD on combination therapy with biologic and immunomodulators, is ongoing combination therapy superior to withdrawal of immunomodulators in maintaining remission? | Adult outpatients who achieve remission on combination therapy with biologic and immunomodulators | Discontinuation of immunomodulators |
|
|
| 7. | In adult outpatients with moderate to severe CD, is top-down therapy superior to step therapy for achieving remission, and preventing disease complications? | Adult outpatients with moderate to severe CD | Top-down therapy
|
Step therapy
|
|
| 8. | In adult outpatients with moderate to severe CD, what is the overall efficacy of corticosteroids (systemic prednisone or budesonide) for induction and maintenance of remission? | Adult outpatients with moderate to severe CD |
|
|
|
| 9. | In adult outpatients with moderate to severe CD, what is the overall efficacy of sulfasalazine or 5-aminosalicylates for induction and maintenance of remission? | Adult outpatients with moderate to severe CD |
|
|
|
| OUTPATIENTS with MODERATE TO SEVERE FISTULIZING CROHN’S DISEASE | |||||
| 10. | In adult outpatients with fistulizing CD, what is the efficacy and safety of the following drugs: TNF-α antagonists (infliximab, adalimumab, certolizumab pegol), vedolizumab, and ustekinumab, immunomodulator monotherapy (thiopurines, methotrexate), antibiotics? | Adults with fistulizing CD |
|
Placebo/No treatment |
|
| 11. | In adult patients with fistulizing CD (without abscess), is adding antibiotics to TNF-α antagonists superior to TNF-α antagonists alone? | Adults with fistulizing CD (without abscess) receiving TNF-α antagonists |
|
Placebo |
|
Table 2 summarizes key messages for all PICOs.
Table 2.
Summary of key messages from this evidence synthesis
Question 1A. In adult outpatients with moderate-severe CD, what is the efficacy of TNF-α antagonists (infliximab, adalimumab, certolizumab pegol), vedolizumab, and ustekinumab for induction and maintenance of remission?
|
Question 2. In adult outpatients with moderate-severe CD, what is the comparative efficacy of the different biologic agents (infliximab, adalimumab, golimumab, vedolizumab, ustekinumab) for induction and maintenance of remission, in biologic-naïve patients, and in patients with prior TNF-α antagonist exposure?
|
Question 3. In adult outpatients with moderate-severe CD, what is the efficacy of immunomodulator monotherapy (thiopurines, methotrexate) for induction and maintenance of remission?
|
Question 4. In adult outpatients with moderate-severe CD, is biologic monotherapy (infliximab, adalimumab, certolizumab pegol, vedolizumab, ustekinumab), superior to immunomodulator monotherapy (thiopurines, methotrexate) for induction and maintenance of remission?
|
Question 5. In adult outpatients with moderate-severe CD, is combination therapy of a biologic agent (infliximab, adalimumab, certolizumab pegol, vedolizumab, ustekinumab) with an immunomodulator (thiopurines or methotrexate) superior to biologic monotherapy for induction and maintenance of remission?
|
Question 6. In adult outpatients with quiescent CD on combination therapy with biologic agents and immunomodulators for >6 months, is ongoing combination therapy superior to withdrawal of immunomodulators or biologic agent in decreasing the risk of relapse?
|
Question 7. In adult outpatients with moderate to severe CD, is top-down treatment strategy (early use of combination therapy with biologic agents with immunomodulators) superior to step therapy (escalation to biologic-based therapy only after failure of 5-aminosalicylates and/or immunomodulators) for achieving remission, and preventing disease complications?
|
Question 8. In adult outpatients with moderate to severe CD, what is the efficacy of corticosteroids (prednisone or budesonide) for induction and maintenance of remission?
|
Question 9. In adult outpatients with moderate to severe CD, what is the efficacy of sulfasalazine and 5-aminosalicylates for induction and maintenance of remission?
|
Question 10. In adults with fistulizing CD, what is the efficacy and safety of the following drugs: TNF-α antagonists (infliximab, adalimumab, certolizumab pegol), vedolizumab, ustekinumab, immunomodulator monotherapy (thiopurines, methotrexate) and antibiotics?
|
Question 11. In adult patients with fistulizing CD (without abscess), is adding antibiotics to TNF-α antagonists superior to TNF-α antagonists alone?
|
Estimating Absolute Magnitude of Benefit
For trials of induction and maintenance therapy evaluating efficacy of interventions vs. placebo, a minimal clinically important difference (MCID) was set at 10%. Hence, if the relative risk of medication for failure to achieve and maintain remission was >0.90, then the medication did not meet the MCID and was not deemed to have a clinically meaningful effect over placebo.
In order to provide a synthesis of the risks and benefits of different interventions, to calculate absolute effect estimates, the technical review team relied on pooled placebo clinical remission rates. In trials of induction therapy with biologic agents, induction of clinical remission with placebo was set at 20%, and maintenance of clinical remission was set at 24%.15 In trials of thiopurines and methotrexate which reported steroid-free remission as outcome, pooled rates across placebo arms were used.
Search Strategy and Study Selection Criteria
An experienced medical librarian performed a systematic literature search of multiple electronic databases (Ovid Medline In-Process & Other Non-Indexed Citations, Ovid MEDLINE, EMBASE, and Wiley Cochrane Library) using a combination of controlled vocabulary terms supplemented with keywords. The search was initially conducted on August 4, 2019. A focused update using PubMed for new randomized controlled trials (RCTs) on PICOs of interest was performed on July 31, 2020. For evidence synthesis, RCTs conducted in adults with moderate-severe CD, either luminal or fistulizing disease, evaluating interventions of interest (corresponding to relevant PICOs) were included. If RCT-level evidence was not available for specific PICOs, then observational studies were included to inform evidence. Minimum trial duration for induction and maintenance therapy was 2 weeks and 16 weeks, respectively. Trials in patients with ulcerative colitis were excluded; if a trial included both patients with CD and ulcerative colitis, it was included only if results were stratified by disease or if >70% participants had CD. Since safety outcomes are not well informed by RCTs, representative large cohort studies and high-quality systematic reviews/meta-analyses were used to inform risk of serious infections and malignancy with different therapies. Separate systematic literature reviews were performed to identify studies informing cost-effectiveness and patients’ values and preferences for different management strategies in moderate-severe CD. In addition, studies on issues of racial, ethnic, and social disparities and issues of general health equity pertinent to the topic were identified. Details of the search strategy are reported in the Online Supplement. A total of 6,238 articles were identified.
Data Extraction and Statistical Analysis
Data abstraction was conducted in duplicate, independently, by two investigators (JF and SS), with disagreements or questions of accuracy resolved by discussion and consensus with the technical review team.
For trials of induction and maintenance therapy, outcomes were abstracted and reported as failure to induce clinical remission (in patients with active disease), and failure to maintain remission (in patients with quiescent disease at trial entry), respectively. All analyses were conducted using true intention-to-treat analysis; patients lost to follow-up or excluded from analysis for other reasons were deemed to be treatment failures. Pooled relative risk (RR) or odds ratios (OR) and 95% confidence intervals (CI), were calculated using the Mantel-Haenszel fixed-effects model (in the absence of conceptual heterogeneity and if <5 studies) or the DerSimonian-Liard random-effects model.16 Statistical heterogeneity was assessed using the I2 statistic.17 Small study effects were examined using funnel plot symmetry and Egger’s regression test, though it is important to recognize that these tests are unreliable when the number of studies is <10.18 Direct comparisons were performed using RevMan v5.3 (Cochrane Collaboration, Copenhagen, Denmark). Due to a paucity of head-to-head trials of active agents, to inform comparative efficacy of different pharmacologic interventions, we relied on a recent network meta-analysis performed by Singh et al using a multivariate, consistency model, random-effects meta-regression as described by Ian White.19 This meta-analysis was rated as moderate quality based on AMSTAR-2 criteria.20
Certainty or Quality of Evidence
The certainty of evidence (also known as the quality of evidence) was judged using the GRADE framework.21 For questions of comparative efficacy of different pharmacological interventions for which effect estimates were derived from direct and network meta-analyses, we used the following approach: when direct evidence was available from head-to-head comparisons, this was considered the best available evidence; if there were no direct comparisons between two interventions (and hence, no direct meta-analysis was feasible), effect estimates from the network meta-analysis were used. In applying GRADE to network meta-analysis, first we judged the certainty of evidence for direct comparisons then we rated the indirect estimates, starting at the lowest rating of the two pairwise estimates that contributed as first-order loops.22 We rated down further for imprecision or intransitivity (i.e. dissimilarity between studies in terms of clinical or methodological characteristics). It is important to note that GRADE in the context of clinical guidelines may be different than GRADE in the context of systematic reviews, since the former relies on more comprehensive assessment of risks and benefits, with varying thresholds of confidence for decision-making.
Evidence-to-Decision Framework
Since this technical review was used to inform the development of clinical guidelines, besides a comprehensive risk-benefit analysis, information about additional factors such as patients’ values and preferences, cost-effectiveness, equity, and resource utilization were also reviewed.23 These data are summarized in the Results section.
RESULTS
Risk stratification of Crohn’s disease
The International Organization for the Study of Inflammatory Bowel Diseases (IOIBD) proposed an overall index of disease severity using a modified Delphi panel. These patients with high disease severity are at high risk of adverse disease-related complications including surgery, hospitalization and disability.24 In this index, in patients with CD most important factors suggestive of high disease severity (in order of relative weights) based on a combination of structural damage, inflammatory burden and impact of quality of life are: large or deep mucosal lesions on endoscopy or imaging, presence of fistula and/or perianal abscess, intestinal resections, particularly of segments >40cm, presence of stoma, extensive disease (ileal involvement >40cm, or pancolitis), at least 10 loose stools/week, presence of strictures, elevated C-reactive protein, lack of symptomatic improvement with prior exposure to biologics and/or immunosuppressive agents, significant impact of disease on activities of daily living, low albumin, presence of anorectal symptoms (anorectal pain, bowel urgency, incontinence, discharge, tenesmus), anemia, daily abdominal pain and corticosteroid use within the last 1 year.
Such an empirical approach to risk stratification can inform treatment decisions, wherein patients at higher risk of disease complications may benefit from more effective therapy despite treatment-related risks. While we did not use this, or other risk stratification schemes in informing absolute effect size with different interventions, we anticipate that healthcare providers would incorporate risk stratification in informing decisions.
Safety of Pharmacological Therapies for Moderate-Severe CD
Before discussing the focused questions related to the efficacy and comparative efficacy of pharmacologic therapies for moderate-severe CD, we have briefly summarized the overall and comparative safety of different pharmacological interventions in large cohort studies and clinical trials, focusing on serious infections and malignancy. It is important to note that clinical trials are selective in enrollment with short duration of follow-up, and data from these trials are often not able to adequately assess the safety of different therapies.
Risk of Serious and Opportunistic Infections:
Findings from key nationwide or nationally representative cohort studies on risk of serious and opportunistic infections with IBD pharmacotherapies have been summarized in Supplemental Table 1. Across studies, most consistent risk factors for serious infections are high disease activity and inadequate disease control, need for corticosteroids and opiate medication and concomitant use of immunomodulators.25, 26
TNF-α antagonists:
Safety registries have suggested that TNFα antagonists may be associated with 1.5–2 times higher risk of serious infections as compared to other immunosuppressive agents. In the TREAT registry of 6,273 patients with moderate to severely active CD (3,440 infliximab-treated and 2,833 other-treatments-only) with up to 13 years of follow-up, serious infections occurred at 2.2 events per 100 person-years (PY) in infliximab-treated patients compared to 0.9/100-PY in other-treatments-only patients.27 In the PYRAMID registry of 5,025 adalimumab-treated patients followed for up to 6 years, treatment emergent serious infections were reported at a rate of 4.7 events per 100-PY from 556 patients (11.1%).28 In a retrospective French population-based cohort study using the national health insurance database of 85,850 TNFα antagonist- and/or immunomodulator-treated patients, Kirchgesner and colleagues observed that the combination of TNFα antagonist and immunomodulators is associated with a higher risk of serious infections (requiring hospitalization) (2.2 per 100-PY) as compared to patients treated with TNFα antagonist monotherapy (1.9 per 100-PY) which itself is associated with higher risk of infection as compared to immunomodulator monotherapy (1.1 per 100-PY).29 In a Danish propensity score matched population-based cohort study, Andersen and colleagues estimated that TNFα antagonist-based therapy is associated with 2.1 times higher risk of serious infections within 1 year, as compared to immunomodulator-based therapy.30 In a meta-analysis of comparative studies including registries and observational comparative effectiveness studies, risk of serious infections was modestly higher with combination therapy of TNFα antagonist and immunomodulators vs. TNFα antagonist monotherapy (6 cohorts, relative risk [RR], 1.19; 95% CI, 1.03–1.37]).31 Based on 5 cohorts, median rate of serious infections with TNFα antagonist monotherapy and immunomodulator monotherapy was 3.9 and 2.2 per 100-PY, respectively, with corresponding risk of serious infections being 64% higher with TNFα antagonist monotherapy (RR, 1.64; 95% CI, 1.19–2.27]). In a retrospective cohort study using Medicare-Medicaid databases, Lewis and colleagues observed that the risk of serious infections with TNF-α antagonists was not significantly different than risks with prolonged corticosteroids, and the former was associated with lower mortality.32
Vedolizumab:
By virtue of gut-specificity of its receptor, vedolizumab is presumed to be a safer biologic, though long-term safety data from registry studies are lacking. Integrated safety analysis from registration trials of vedolizumab (1,349 patients with CD) showed that the risk of serious infections was low, and not significantly different than rates in placebo-treated patients.33 Among patients with CD, the incidence rate of serious infections was 3.4 per 100 p-y, with perianal abscesses being the most common infection. Opportunistic infections were reported in 30 patients with CD, the most common of which were clostridial infections.
Ustekinumab:
Registry studies and large real-world observational studies of ustekinumab in CD are awaited. In an integrated safety analysis of data from 6 phase 2/3 trials of ustekinumab including 2,574 patients (1,733-PY), incidence of serious infections was 5.02 per 100-PY (vs. 5.53 in placebo-treated patients).34 Extrapolating from other autoimmune diseases like psoriasis, the risk of serious infections with ustekinumab monotherapy may be lower as compared to TNFα antagonist monotherapy. However, these findings on the relative safety of ustekinumab in patients with psoriasis should be interpreted with caution, as the dose of ustekinumab approved for use in CD is at least 50% higher than the dose used in psoriasis.
Risk of Malignancy:
Findings from key nationwide or nationally representative cohort studies on the risk of malignancy with IBD pharmacotherapies have been summarized in Supplemental Table 2.
Thiopurines:
Thiopurines have been consistently associated with increased risk of lymphoproliferative diseases. In a meta-analysis of 18 studies, the standardized incidence rate of lymphoma in thiopurine-treated patients was 4.9 (95% CI, 3.1–7.8), with higher rates being reported in referral-center studies (standardized incidence rate [SIR], 9.2) vs. population-based studies (SIR, 2.8).35 The level of risk was statistically significant after 1 year of exposure, and risk was elevated in current (SIR, 5.7), but not former users (SIR, 1.4). On modeling, Kotlyar and colleagues estimate the number of patients needed to be treated with thiopurines to cause 1 additional lymphoma ranges from 4,598 in those 20–29 years to 325 in those 70–79 years. In another meta-analysis of 8 studies, Ariyaratnam and Subramanian estimated a 2.3-times higher risk of non-melanoma skin cancer in thiopurine-treated patients (95% CI, 1.5–3.5).36 Methotrexate has been variably associated with either no significant or a 1.5–5.0-times increased risk of lymphoproliferative disease, based on studies in patients with rheumatoid arthritis.37
TNF-α antagonists:
Several large population-based studies have identified no association between TNF-α antagonist exposure and solid-organ malignancy.38, 39 TNF-α antagonists have been variably associated with a 2–5-fold increased risk of lymphoid malignancy in population-based studies. In a French population-based study, Lemaitre and colleagues estimated the annual incidence of lymphoma in patients treated with TNF-α antagonist monotherapy vs. unexposed patients to be 0.41 per 1,000 person-years vs. 0.26 per 1,000 person-years; after adjusting for covariates, risk of lymphoma was 2.4-times higher in patients treated with TNF-α antagonist monotherapy.40 This risk was comparable to risk observed in patients treated with thiopurine monotherapy (OR, 0.93; 95% CI, 0.60–1.44). On meta-analysis of 4 high-quality observational studies, risk of lymphoma did not differ between TNF-α antagonist monotherapy and thiopurine monotherapy with pooled incidence rate ratio of 0.72 (95% CI, 0.48–1.07).41 Patients exposed to combination therapy had 6.1-times higher of risk lymphoma, as compared to unexposed patients, and 2.3–2.5 times higher risk as compared to patients exposed to monotherapy with either agent. In contrast, long-term follow-up of clinical trials or registry-based studies have not observed an increased risk of malignancy in patients treated with TNF-α antagonist monotherapy. On analysis of 1,594 patients with CD treated with adalimumab in clinical trials, over 3,050 person-years of exposure, Osterman and colleagues observed an increased risk of malignancy in patients treated with combination therapy (SIR, 3.0; 95% CI, 1.7–5.1), but not adalimumab monotherapy (SIR, 0.6; 95% CI, 0.2–1.6).42 Compared with patients receiving adalimumab monotherapy, those patients receiving combination therapy had an increased risk of malignancy other than non-melanoma skin cancer (RR, 2.8; 95% CI, 1.1–7.4) and of non-melanoma skin cancer (RR, 3.5; 95% CI, 1.1–11.1). In a large prospective registry (PYRAMID) of 5025 adalimumab-treated patients with Crohn’s disease over 16,680.4 person-years of follow-up, observed lymphoma rate with adalimumab was lower than the estimated background rate.28 Regardless, the FDA has issued a black box warning on the increased risk of malignancy with TNF-α antagonists (https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/103772s5359lbl.pdf, accessed August 21, 2018).
Vedolizumab:
Although long-term follow-up and real-world evidence is lacking, safety analyses of clinical trials and open-label extension studies have not observed any significant increase in risk of solid-organ or hematological malignancies with vedolizumab. Loftus and colleagues reported malignancy in 50/2,243 patients with IBD (including 32/1,349 patients with CD, with incidence rate of 0.8 per 100 PY) with vedolizumab exposure in the GEMINI long-term extension study.33 Indirect treatment comparison network meta-analysis of 23 RCTs suggested no difference in risk of malignancy between patients treated with TNF-α antagonist vs. vedolizumab (OR, 0.87; 95% CI, 0.26–2.88).43
Ustekinumab:
In an integrated safety analyses of phase 2/3 trials of ustekinumab for psoriasis, psoriatic arthritis and CD, the incidence of malignancy (excluding non-melanoma skin cancer) was low and comparable among ustekinumab-treated patients (0.4 per 100py) and placebo-treated patients (0.2 per 100py).34 Combined across indications, the standardized incidence rate for malignancies (excluding cervical cancer in situ and NMSC per SEER) in the ustekinumab and placebo groups were 0.6 (0.3–1.0) and 0.3 (0.0–1.9), respectively, with overlapping 95% CIs.
Other side effects associated with these medications are summarized in the online supplement.
PHARMACOLOGICAL MANAGEMENT OF PATIENTS WITH MODERATE TO SEVERE LUMINAL CROHN’S DISEASE
Question 1A. In adult outpatients with moderate-severe CD, what is the efficacy of TNF-α antagonists (infliximab, adalimumab, certolizumab pegol), vedolizumab, and ustekinumab for induction and maintenance of remission?
Key Messages:
In patients with moderate to severely active Crohn’s disease, infliximab and adalimumab are probably more effective than placebo for inducing remission (moderate certainty of evidence); certolizumab pegol may be more effective than placebo for inducing remission (low certainty of evidence)
In patients with quiescent moderate to severe Crohn’s disease, infliximab, adalimumab and certolizumab pegol are probably more effective than placebo for maintaining remission (moderate certainty of evidence)
In patients with moderate to severely active Crohn’s disease, vedolizumab may be more effective than placebo for inducing remission (low certainty of evidence). In patients with quiescent moderate to severe Crohn’s disease, vedolizumab is probably more effective than placebo for maintaining remission (moderate certainty of evidence).
In patients with moderate to severely active Crohn’s disease, ustekinumab is probably more effective than placebo for inducing remission (moderate certainty of evidence). In patients with quiescent moderate to severe Crohn’s disease, ustekinumab is probably more effective than placebo for maintaining remission (moderate certainty of evidence).
Effect estimate:
Overall, 13 RCTs informed the efficacy of different biologic agents for induction of remission in patients with moderate-severe luminal CD, and 9 trials informed their efficacy for maintenance of remission. Patients across all trials and treatment arms were generally comparable in terms of baseline prognostic variables, inclusion/exclusion criteria, and co-interventions, though trials of non-TNF-targeting biologics had a higher proportion of patients who had been previously exposed to TNF-α antagonists. Definitions of outcomes were generally similar across trials based on CDAI, and assessed between weeks 4 to 12 for induction therapy, and week 22 to 54 for maintenance therapy. Relative and absolute effect estimates are shown in Table 3.
Table 3.
GRADE Evidence Profile comparing infliximab, adalimumab, certolizumab pegol, vedolizumab and ustekinumab with placebo for induction and maintenance of remission in patients with moderate to severe luminal Crohn’s disease. Note, to calculate absolute effect estimate, we used pooled placebo rate of 20% for induction of remission, and 24% for maintenance of remission
| INFLIXIMAB COMPARED TO PLACEBO FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with infliximab | |||||
| Induction of clinical remission (CRITICAL) | 43/54 (79.6%) | 23/52 (44.2%) | RR 0.54 (0.39 to 0.75) | 92 fewer per 1,000 (from 122 fewer to 50 fewer) | 106 (2 RCTs) | ⨁⨁⨁◯1 MODERATE |
| Maintenance of clinical remission (CRITICAL) | 87/110 (79.1%) | 69/113 (61.1%) | RR 0.77 (0.65 to 0.92) | 55 fewer per 1,000 (from 84 fewer to 19 fewer) | 223 (1 RCT) | ⨁⨁⨁◯1 MODERATE |
| ADALIMUMAB COMPARED TO PLACEBO FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with adalimumab | |||||
| Induction of clinical remission (CRITICAL) | 239/263 (90.9%) | 196/268 (73.1%) | RR 0.82 (0.75 to 0.89) | 36 fewer per 1,000 (from 50 fewer to 22 fewer) | 531 (3 RCTs) | ⨁⨁⨁◯1 MODERATE |
| Maintenance of clinical remission (CRITICAL) | 180/210 (85.7%) | 127/212 (59.9%) | RR 0.70 (0.62 to 0.79) | 72 fewer per 1,000 (from 91 fewer to 50 fewer) | 422 (3 RCTs) | ⨁⨁⨁◯1 MODERATE |
| CERTOLIZUMAB PEGOL COMPARED TO PLACEBO FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with certolizumab pegol | |||||
| Induction of clinical remission (CRITICAL) | 489/608 (80.4%) | 455/616 (73.9%) | RR 0.92 (0.86 to 0.98) | 16 fewer per 1,000 (from 28 fewer to 4 fewer) | 1224 (3 RCTs) | ⨁⨁◯◯2 LOW |
| Maintenance of clinical remission (CRITICAL) | 443/536 (82.6%) | 393/542 (72.5%) | RR 0.88 (0.83 to 0.93) | 29 fewer per 1,000 (from 41 fewer to 17 fewer) | 1078 (2 RCTs) | ⨁⨁⨁◯3 MODERATE |
| VEDOLIZUMAB COMPARED TO PLACEBO FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with Vedolizumab | |||||
| Induction of clinical remission (CRITICAL) | 320/355 (90.1%) | 357/429 (83.2%) | RR 0.92 (0.87 to 0.97) | 16 fewer per 1,000 (from 26 fewer to 6 fewer) | 784 (2 RCTs) | ⨁⨁◯◯2 LOW |
| Maintenance of clinical remission (CRITICAL) | 120/153 (78.4%) | 94/154 (61.0%) | RR 0.78 (0.67 to 0.91) | 53 fewer per 1,000 (from 79 fewer to 22 fewer) | 307 (1 RCT) | ⨁⨁⨁◯1 MODERATE |
| USTEKINUMAB COMPARED TO PLACEBO FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with ustekinumab | |||||
| Induction of clinical remission (CRITICAL) | 515/588 (87.6%) | 460/589 (78.1%) | RR 0.90 (0.85 to 0.94) | 96 fewer per 1,000 (from 131 fewer to 53 fewer) | 1177 (3 RCTs) | ⨁⨁⨁◯3 MODERATE |
| Maintenance of clinical remission (CRITICAL) | 137/204 (67.2%) | 101/200 (50.5%) | RR 0.75 (0.64 to 0.89) | 168 fewer per 1,000 (from 242 fewer to 74 fewer) | 404 (2 RCT) | ⨁⨁⨁◯1 MODERATE |
|
GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
Rated down for imprecision since optimal information size not met (<200 events)
Rated down for very serious imprecision since effect estimate was smaller than the minimal clinically important difference of at least 10% over placebo
Rated down for serious imprecision since 95% CI of effect estimate was smaller than the minimal clinically important difference of at least 10% over placebo
Infliximab vs. placebo:
All trials evaluating the efficacy of infliximab were conducted in biologic-naïve patients. Based on two RCTs (106 patients), infliximab induction therapy was superior to placebo for induction of remission (Supplemental Figure 1).44, 45 In one trial, only a single induction dose of infliximab was administered and outcomes were assessed at week 4. In 1 RCT of 223 patients, infliximab maintenance therapy was more effective than placebo in maintaining remission (Supplemental Figure 2).46
Adalimumab vs. placebo:
Based on three trials (531 patients), standard induction therapy with adalimumab was superior to placebo for induction of remission (Supplemental Figure 1).47–49 47, 50–53,47, 50–53,47, 50–53Of note, one trial was conducted exclusively in biologic-naïve patients, whereas another trial (GAIN) was conducted exclusively in patients with prior intolerance or secondary loss of response to infliximab; none of these patients had prior primary non-response to a TNF-α antagonist. Based on three trials (422 patients) in which responders to induction therapy were re-randomized to adalimumab or placebo, adalimumab was superior to placebo for maintenance of remission (Supplemental Figure 2).49, 54, 55
Certolizumab pegol vs. placebo:
Based on three trials of induction therapy (1,224 patients), certolizumab pegol was significantly more effective than placebo for induction of clinical remission in patients with moderate-severe CD (Supplemental Figure 1).56–58 However, the relative magnitude of benefit was 0.92 (RR, 0.92; 95% CI, 0.86–0.92), which was smaller than the pre-defined MCID threshold of 10% over placebo. In two trials of maintenance therapy (1,078 patients), in which responders to induction therapy were re-randomized to certolizumab pegol or placebo, certolizumab pegol was superior to placebo for maintenance of clinical remission (Supplemental Figure 2).56, 59
Vedolizumab vs. placebo:
In two trials (784 patients), vedolizumab was significantly more effective than placebo for induction of clinical remission in patients with moderate-severe CD (Supplemental Figure 3A).60, 61 However, the relative magnitude of benefit was 0.92 (RR, 0.92; 95% CI, 0.87–0.97) which was smaller than the pre-defined MCID threshold of 10% over placebo. Importantly, in these trials, 50–75% patients were previously exposed to TNF-α antagonist(s). In a subset of biologic-naïve patients, vedolizumab was significantly and clinically more effective than placebo (RR, 0.86; 95% CI, 0.77–0.95). Among patients with clinical response to vedolizumab at week 6 or 10, one trial of maintenance therapy demonstrated that vedolizumab was superior to placebo for maintenance of remission (Supplemental Figure 3B).60
Ustekinumab vs. placebo:
Based on three trials (1,177 patients), ustekinumab was superior to placebo for induction of clinical remission in patients with moderate-severe CD (Supplemental Figure 4A).62, 63 Two trials included only patients with prior exposure to TNF-α antagonist(s). Among patients with clinical response to ustekinumab at week 6 or 8, two trials of maintenance therapy demonstrated that ustekinumab was superior to placebo for maintenance of remission (Supplemental Figure 4B).62, 63
GRADE Certainty of Evidence:
Table 3 summarizes the GRADE certainty of evidence for the studies referenced above. Most of these studies were conducted as registration trials, sponsored by industry. There was no important inconsistency or indirectness identified. For most analyses, the total number of events was <200 (except induction and maintenance of remission with certolizumab pegol, and induction of remission with ustekinumab), and hence, evidence was rated down for imprecision due to failure to reach optimal information size. Additionally, for comparisons of certolizumab pegol vs. placebo, and vedolizumab vs. placebo for induction of remission, evidence was rated down twice for very serious imprecision since the summary risk estimate was below the pre-defined MCID threshold of 10% over placebo.
Potential Harms of Intervention:
Adverse effects associated with different medications have been summarized above. In addition, safety data from the pivotal clinical trials of maintenance therapies with these agents are summarized in Supplemental Table 3.
Discussion:
Unlike the prior technical review on this topic, we decided to analyze each TNF-α antagonist separately to better inform comparative efficacy of different agents. While moderate certainty of evidence supported the use of infliximab or adalimumab of inducing remission, only low certainty of evidence supported the use of certolizumab pegol since it did not reach the pre-defined MCID over placebo. Of note, while infliximab and adalimumab (and vedolizumab and ustekinumab) have been approved by the FDA for inducing and maintaining remission, certolizumab pegol has only been approved for maintaining clinical response in patients with moderate to severely active CD who have an inadequate response to conventional therapy. Certolizumab pegol has not been approved for management of CD by the European Medical Agency and in Canada.
Question 1B. In adult outpatients with moderate-severe CD, what is the efficacy and safety of natalizumab?
Key Message:
In patients with moderate to severely active Crohn’s disease, natalizumab is probably more effective than placebo for inducing and maintaining remission (moderate certainty of evidence). However, natalizumab is associated with a serious, potentially fatal infection, progressive multifocal leukoencephalopathy caused by reactivation of the John Cunningham virus (low certainty of evidence).
Effect estimate:
In two trials of biologic-naïve patients (1,424 patients), natalizumab was more effective than placebo for inducing remission, although the 95% CI of the effect estimate crossed the 10% MCID threshold (RR, 0.88; 95% CI, 0.82–0.96) (Supplemental Figure 5A).64, 65 In one trial of 338 patients with initial response to induction therapy, natalizumab was more effective than placebo in maintaining remission (Supplemental Figure 5B).64
Potential harms of intervention:
Most common adverse events observed in clinical trials of natalizumab in CD were headache and upper respiratory infections. Importantly, during post-marketing surveillance, cases of progressive multifocal leukoencephalopathy (PML) were identified. This is a demyelinating disease of the brain caused by reactivation of the John Cunningham (JC) virus, without specific treatment beyond reconstitution of the immune system; 3-month mortality with PML is 20–50%, and survivors frequently experience long-term neurological deficits.66 In a comprehensive review of post-marketing sources, clinical studies, and an independent Swedish registry, Bloomgren and colleagues identified 212 confirmed cases of PML among 99,571 patients with multiple sclerosis treated with natalizumab (2.1 cases per 1,000 patients).67 All 54 patients with PML for whom samples were available before the diagnosis were positive for anti-JC virus antibodies. When the risk of PML was stratified according to three risk factors (anti-JC virus antibodies, prior use of immunosuppressants, and increased duration of natalizumab treatment), the risk of PML was lowest among the patients who were negative for anti-JC virus antibodies, with the incidence estimated to be 0.09 cases or less per 1,000 patients (95% CI, 0 to 0.48). Patients who were positive for anti-JC virus antibodies, had taken immunosuppressants before the initiation of natalizumab therapy, and had received 25 to 48 months of natalizumab treatment had the highest estimated risk (incidence, 11.1 cases per 1,000 patients [95% CI, 8.3 to 14.5]). Following these observations, natalizumab is available only through a special restricted distribution program called the TOUCH® Prescribing Program, and should be used as monotherapy. Natalizumab should not be administered to patients who are positive for JC-virus antibodies at baseline (approximately 57% of patients with multiple sclerosis); patients who are started on this agent require frequent monitoring for JC virus seroconversion.68
GRADE Certainty of Evidence:
The overall body of evidence supporting the efficacy of natalizumab over placebo was rated as moderate certainty, being rated down for imprecision (Table 4). Low certainty evidence from observational studies suggested natalizumab is probably associated with risk of PML, particularly in patients who are positive for anti-JC virus antibody.
Table 4.
GRADE Evidence Profile comparing natalizumab with placebo for induction and maintenance of remission, and risk of progressive multifocal leukoencephalopathy in patients with moderate to severe luminal Crohn’s disease.
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
|---|---|---|---|---|---|---|
| Risk with placebo | Risk with natalizumab | |||||
| Induction of clinical remission (CRITICAL) | 323/431 (74.9%) | 633/983 (64.4%) | RR 0.88 (0.82 to 0.96) | 24 fewer per 1,000 (from 36 fewer to 8 fewer) | 1414 (2 RCTs) | ⨁⨁⨁◯1 MODERATE |
| Maintenance of clinical remission (CRITICAL) | 133/170 (78.2%) | 76/168 (45.2%) | RR 0.58 (0.48 to 0.70) | 101 fewer per 1,000 (from 125 fewer to 72 fewer) | 338 (1 RCT) | ⨁⨁⨁◯2 MODERATE |
| Risk of progressive multifocal leukoencephalopathy (CRITICAL) | Positive for JC virus antibody: 0% | ~1% | RR >20 | 99,571 (Registry) | ||
| Negative for JC virus antibody: 0% | ~0.01% | 11.1 per 1,000 patients (95% CI, 8.3 to 14.5) | ⨁⨁◯◯3 LOW | |||
Rated down for imprecision since 95% CI of effect estimate was smaller than the minimal clinically important difference of at least 10% over placebo
Rated down for imprecision since optimal information size not met (<200 events)
Rated down for risk of bias (derived from observational studies)
Discussion:
The efficacy and safety of natalizumab was not examined in the prior technical review. Natalizumab was the first non-TNF-α-targeting biologic for the management of CD in 2008. While it was effective for inducing and maintaining remission, extensive post-marketing surveillance evaluation confirmed a causative association with PML. CD is not a fatal condition, and only affords a modestly higher excess lifetime mortality as compared to the general population; in contrast, PML carries a very poor prognosis.69 Considering PML is very unlikely to occur in the general population with CD, any excess risk of this condition observed with CD is highly unacceptable.
Question 2. In adult outpatients with moderate-severe CD, what is the comparative efficacy of the different biologic agents (infliximab, adalimumab, golimumab, vedolizumab, ustekinumab) for induction and maintenance of clinical remission, in biologic-naïve patients, and in patients with prior TNF-α antagonist exposure?
Key Messages:
In biologic-naïve patients with moderate to severely active Crohn’s disease, infliximab, adalimumab, and ustekinumab are probably more effective than certolizumab pegol (moderate certainty of evidence), and vedolizumab may be more effective than certolizumab pegol (low certainty of evidence) in inducing remission.
In biologic-naïve patients with moderate to severely active Crohn’s disease, infliximab may be more effective than ustekinumab or vedolizumab for inducing remission (low certainty of evidence). The benefit of adalimumab over ustekinumab or vedolizumab for inducing remission is uncertain (very low certainty of evidence).
In patients with moderate to severely active Crohn’s disease with prior TNFα antagonist exposure, ustekinumab is probably more effective than no treatment (moderate certainty of evidence), and vedolizumab may be more effective than no treatment (low certainty of evidence), in inducing remission. In a subset of patients with intolerance to or prior response to infliximab (with subsequent loss of response), adalimumab is probably more than no treatment in inducing remission (moderate certainty of evidence).
In patients with moderate to severely active Crohn’s disease with prior TNFα antagonist exposure, the benefit of adalimumab, ustekinumab or vedolizumab over each other was uncertain (very low certainty of evidence).
In patients with quiescent moderate-severe CD with initial clinical response to induction therapy, adalimumab is probably more effective than certolizumab pegol (moderate certainty of evidence) in maintaining remission. Adalimumab may be more effective than vedolizumab and ustekinumab in maintaining clinical remission (low certainty of evidence).
In patients with quiescent moderate-severe CD with initial clinical response to induction therapy, the benefit of infliximab over certolizumab pegol, vedolizumab or ustekinumab in maintaining remission is uncertain (low to very low certainty of evidence).
Effect estimates and certainty of evidence:
Induction of remission, biologic-naïve patients:
No head-to-head trials were identified and all evidence on comparative efficacy was derived from a previously published network meta-analysis.19 Overall, 8 RCTs including 1,458 biologic-naïve patients with moderate-severe Crohn’s disease, treated with infliximab (2 trials), adalimumab (2 trials), certolizumab pegol (1 trial), vedolizumab (2 trials) and ustekinumab (1 trial) were included. Results of network meta-analysis are summarized in Table 5. There was moderate confidence in estimates supporting the use of infliximab over certolizumab pegol (OR, 4.33; 95% CI, 1.83–10.27) (evidence rated down for imprecision), and low confidence in estimates supporting its use over vedolizumab (OR, 2.20; 95% CI, 0.79–6.07) and ustekinumab (OR, 2.14; 95% CI, 0.89–5.15) (evidence rated down for very serious imprecision); there was moderate confidence in estimates supporting the use of ustekinumab (OR, 2.02; 95% CI, 1.09–3.75) and adalimumab (OR, 2.97; 95% CI, 1.16–6.70) over certolizumab pegol (evidence rated down for imprecision). There was no significant difference in the efficacy of ustekinumab and vedolizumab as a first-line agent (very low certainty evidence).
Table 5.
GRADE Summary of Findings reporting the comparative efficacy of different pharmacological agents for inducing clinical remission in biologic-naïve patients with moderate to severe luminal Crohn’s disease based on network meta-analysis
| Medications | Relative effect (Odds ratio, 95% CI) | Overall Quality of Evidence |
|---|---|---|
| Selected agents vs. Infliximab | ||
| Adalimumab | 0.64 (0.22–1.88) | Low (very serious imprecision) |
| Certolizumab pegol | 0.23 (0.10–0.55) | Moderate (imprecision) |
| Vedolizumab | 0.46 (0.16–1.26) | Low (very serious imprecision) |
| Ustekinumab | 0.47 (0.19–1.12) | Low (very serious imprecision) |
| Selected agents vs. Adalimumab | ||
| Certolizumab pegol | 0.36 (0.15–0.86) | Moderate (imprecision) |
| Vedolizumab | 0.71 (0.25–1.98) | Low (very serious imprecision) |
| Ustekinumab | 0.73 (0.30–1.76) | Low (very serious imprecision) |
| Selected agents vs. Certolizumab pegol | ||
| Vedolizumab | 1.97 (0.88–4.41) | Low (very serious imprecision) |
| Ustekinumab | 2.02 (1.09–3.75) | Moderate (imprecision) |
| Selected agents vs. Vedolizumab | ||
| Ustekinumab | 1.02 (0.45–2.32) | Low (very serious imprecision) |
Even though trials of infliximab used non-conventional infliximab doses or dosing regimens (one trial only used single dose, another trial treated all patients concomitantly with thiopurines), we opted not to rate down for intransitivity since effect estimates using conventional dosing regimens were likely to be more favorable
Induction of remission in patients with prior TNFα antagonist exposure:
No head-to-head trials were identified and all evidence on comparative efficacy was derived from a previously published network meta-analysis.19 Overall, 6 RCTs including 1,606 patients with moderate-severe CD with prior exposure to TNFα antagonists were identified. These included thee trials conducted exclusively in patients with prior exposure to TNFα antagonists (1 trial of adalimumab, 2 of ustekinumab), and two subgroup analyses of phase III trials (1 each of adalimumab and vedolizumab); one trial of vedolizumab (GEMINI-III) included 75% patients with prior exposure to TNFα antagonists. One trial of adalimumab (GAIN) selectively included only patients with prior response or intolerance to infliximab, and excluded patients with non-response to infliximab. There were no trials of infliximab or certolizumab pegol in patients with prior exposure to TNFα antagonists, that met inclusion criteria. On network meta-analysis, compared to placebo, moderate certainty evidence supported the use of ustekinumab (OR, 2.58; 95% CI, 1.50–4.44) for induction of clinical remission (evidence rated down due to imprecision) (Table 6). In a subset of patients with intolerance to or prior response to infliximab (with subsequent loss of response), moderate certainty evidence supported the use of adalimumab (OR, 3.57; 95% CI, 1.66–7.65) (evidence rated down due to imprecision). Low certainty evidence supported the use of vedolizumab (OR, 1.53; 95% CI, 0.77–3.06) for induction of clinical remission over placebo, due to very serious imprecision (very wide confidence intervals, crossing unity). On indirect comparison of active interventions, though the effect estimated favored adalimumab and ustekinumab over vedolizumab, the certainty of evidence was rated as very low due to very serious imprecision and intransitivity due to differences in patients included in trials of adalimumab and ustekinumab or vedolizumab. Prior treatment exposure and response is an important effect modifier. Study level estimates did not report what proportion of patients had exposure to more than one TNFα antagonist, exposure to multiple different classes of biologics, and reasons for failure of prior biologics (primary non-response vs. secondary loss of response vs. intolerance).
Table 6.
GRADE Summary of Findings reporting the comparative efficacy of different pharmacological agents for inducing clinical remission in patients with prior exposure to TNFα antagonists with moderate to severe luminal Crohn’s disease based on network meta-analysis
| Medications | Relative effect (Odds ratio, 95% CI) | Overall Quality of Evidence |
|---|---|---|
| Selected agents vs. Placebo | ||
| Adalimumab | 3.57 (1.66–7.65) | Moderate (imprecision, indirectness * ) |
| Vedolizumab | 1.53 (0.77–3.06) | Low (very serious imprecision) |
| Ustekinumab | 2.58 (1.50–4.44) | Moderate (imprecision) |
| Selected agents vs. Adalimumab | ||
| Vedolizumab | 0.43 (0.15–1.20) | Very low (very serious imprecision, intransitivity¶) |
| Ustekinumab | 0.72 (0.28–1.85) | Very low (very serious imprecision, intransitivity¶) |
| Selected agents vs. Vedolizumab | ||
| Ustekinumab | 1.68 (0.68–4.15) | Very low (very serious imprecision, intransitivity¶) |
Adalimumab comparison vs. placebo was rated down for indirectness (since adalimumab trials excluded patients with primary non-response to infliximab (i.e., only included patients who had secondary loss of response or intolerance). When focusing on a subset of patients with patients with intolerance to or prior response to infliximab (with subsequent loss of response), evidence was rated as moderate quality
All comparisons of vedolizumab vs. ustekinumab vs. TNFα antagonists were rated down for intransitivity due to differences in patient characteristics. Study level estimates did not report what proportion of patients had exposure to more than one TNF-α antagonist, exposure to multiple different classes of biologics, and reasons for failure of prior biologics (primary non-response vs. secondary loss of response vs. intolerance).
Maintenance of remission in patients with clinical response to induction therapy:
No head-to-head trials of maintenance therapy were identified and all evidence on comparative efficacy was derived from a previously published network meta-analysis.19 Overall, 9 RCTs including 1,854 patients with moderate-severe Crohn’s disease, treated with infliximab (2 trials), adalimumab (3 trials), certolizumab pegol (1 trial), vedolizumab (1 trial) and ustekinumab (2 trials) were included. All trials re-randomized patients who responded to induction therapy, regardless of prior TNF-α antagonist exposure status. On comparison of active interventions, moderate certainty evidence supported the use of adalimumab over certolizumab pegol (OR, 1.97; 95% CI, 1.04–3.73) (evidence rated down for imprecision) (Table 7). Low certainty evidence supported the use of adalimumab over ustekinumab (OR, 2.19; 95% CI, 1.15–4.16) and vedolizumab (OR, 1.96; 95% CI, 0.93–3.85) for maintenance of remission (evidence rated down for imprecision and intransitivity due to difference in characteristics of patients included in trials, particularly with regard to prior exposure to TNF-α antagonists). The benefit of other interventions over one another was uncertain.
Table 7.
GRADE Summary of Findings reporting the comparative efficacy of different pharmacological agents for MAINTAINING CLINICAL REMISSION in all patients with moderate to severe Crohn’s disease, who have responded to induction therapy, regardless of prior biologic exposure, based on network meta-analysis
| Medications | Relative effect (Odds ratio, 95% CI) | Overall Quality of Evidence |
|---|---|---|
| Selected agents vs. Infliximab | ||
| Adalimumab | 1.54 (0.75–3.17) | Low (very serious imprecision) |
| Certolizumab pegol | 0.78 (0.41–1.51) | Low (very serious imprecision) |
| Vedolizumab | 0.81 (0.39–1.67) | Very low (very serious imprecision, intransitivity*) |
| Ustekinumab | 0.71 (0.37–1.36) | Very low (very serious imprecision, intransitivity*) |
| Selected agents vs. Adalimumab | ||
| Certolizumab pegol | 0.51 (0.27–0.96) | Moderate (imprecision) |
| Vedolizumab | 0.51 (0.26–1.07) | Low (imprecision, intransitivity*) |
| Ustekinumab | 0.46 (0.24–0.87) | Low (imprecision, intransitivity*) |
| Selected agents vs. Certolizumab pegol | ||
| Vedolizumab | 1.03 (0.54–1.97) | Very low (very serious imprecision, intransitivity*)0 |
| Ustekinumab | 0.90 (0.51–1.59) | Very low (very serious imprecision, intransitivity*) |
| Selected agents vs. Vedolizumab | ||
| Ustekinumab | 0.87 (0.46–1.66) | Low (very serious imprecision) |
All comparisons of vedolizumab and ustekinumab vs. TNFα antagonists were rated down for intransitivity, since a significant proportion of patients in trials of vedolizumab and ustekinumab had previously been exposed to TNFα antagonists
Potential Harms of Intervention:
There has been very limited direct assessment of comparative safety of different biologic interventions. In the network meta-analysis of clinical trials of maintenance therapy, the rate of serious infections was low, and was not deemed amenable to network meta-analysis. Large real-world comparative safety data on TNF-α antagonists vs. vedolizumab vs. ustekinumab were not identified.
Discussion:
The previous technical review did not examine the comparative efficacy of different biologic agents. In the absence of head-to-head trials, evidence derived from indirect comparisons has been used to inform clinical practice and guidelines. All of the trials included in the analysis reported on biologic-naïve patients and patients with prior TNF-α antagonist exposure separately, had comparable inclusion criteria, trial design, prevalence of risk factors that likely influence treatment response, and used similar outcome measures. Therefore, in the opinion of the technical review team, a comparison across trials could be undertaken without the introduction of significant intransitivity at least for biologic-naïve patients. Though all TNF-α antagonists have similar mechanism of action, the differences in efficacy between infliximab, adalimumab and certolizumab pegol may be related to difference in the pharmacokinetics and bioavailability of the drugs given their different dosing schema and route of administration. Limited real-world observational studies have suggested comparable risk of hospitalization and surgery with infliximab vs. adalimumab,70 and a lower risk of unplanned healthcare utilization with infliximab vs. certolizumab pegol.71 Ongoing head-to-head trials would further enhance clinical decision-making and our confidence in comparative efficacy of different medications.
In contrast to biologic-naïve patients, the technical review team was concerned about significant intransitivity in trials comparing patients with prior TNF-α antagonist exposure. Patients treated with adalimumab in clinical trials generally had exposure to only a single TNF-α antagonist. In contrast, in trials of vedolizumab, or ustekinumab, a significant proportion of patients may have been exposed to 2 or more biologic agents prior to clinical trial intervention and may be inherently be difficult to treat. Similarly, there may be potential differences in efficacy of 2nd line interventions depending on underlying reason for discontinuation of prior TNF-α antagonist (primary non-response vs. secondary loss of response vs. intolerance).72 In trials of adalimumab, only patients with loss of response or intolerance to a prior TNF-α antagonist were included; patients with primary non-response to TNF-α antagonist were excluded. In contrast, in trials of vedolizumab and ustekinumab, a substantial proportion of patients had inadequate response to a TNF-α antagonist (primary non-response). Because of these important uncertainties and differences between study populations, we opted to rate down evidence for intransitivity the evidence regarding prior TNF-α antagonist exposed patients. Recent registry studies have compared real-world effectiveness and safety of ustekinumab vs. vedolizumab in patients with CD with prior failure of TNF-α antagonists. In a French observational study of 239 patients with TNF-α antagonist-refractory CD, Alric and colleagues observed that treatment with ustekinumab was associated with higher rate of clinical remission (vs. vedolizumab: 54.4% vs 38.3%; OR, 1.92; 95% CI, 1.09–3.39) but not steroid-free clinical remission (44.7% vs 34.0%; OR, 1.57; 95% CI, 0.88–2.79), as compared to vedolizumab at week 48.73 Townsend and colleagues observed a higher rate of steroid-free clinical remission in ustekinumab-treated patients as compared to vedolizumab-treated patients in their cohort of 130 patients with TNF-α antagonist-refractory CD (at 2 months: OR, 2.79; 95% CI, 1.06–7.39; at 12 months: OR, 2.01; 95% CI, 0.89–4.56).74 In a Dutch registry-based study, Beimans and colleagues observed higher rates of corticosteroid-free clinical remission (ustekinumab vs. vedolizumab: OR, 2.58; 95% CI, 1.36–4.90) and biochemical remission (OR, 2.34; 95% CI, 1.10–4.96) with ustekinumab; safety outcomes were comparable between the two groups (infections: OR, 1.26; 95% CI, 0.63–2.54; hospitalizations: OR, 0.67; 95% CI, 0.32–1.39).75
Safety is a key factor in clinical decision-making. However, there was limited evidence to inform comparative safety of different interventions. There are two key factors that determine the safety of biologic therapy in patients with CD. First, the intrinsic immunosuppressive effect of the agent, and second, its effectiveness in controlling disease, achieving corticosteroid-free remission and avoiding disease-related complications.76 Biologically, vedolizumab may cause less systemic immune suppression as compared to TNF-α antagonists and ustekinumab. However, the most consistent risk factors for serious infections have been underlying disease severity and concomitant use of corticosteroids and immunosuppressive therapies. By adequately controlling disease activity and minimizing corticosteroid use, a strategy using effective medications to induce and maintain corticosteroid-free remission may be associated with a lower risk of serious infections as compared to using an ineffective but potentially ‘safer’ medication.
Question 3. In adult outpatients with moderate-severe CD, what is the efficacy of immunomodulator monotherapy (thiopurines, methotrexate) for induction and maintenance of clinical remission?
Key Messages:
In adult outpatients with moderate to severely active Crohn’s disease, the benefit of thiopurine monotherapy for inducing remission is uncertain (very low certainty of evidence). In patients with moderate-severe Crohn’s disease in steroid-induced remission, thiopurines may be effective for maintaining remission (low certainty of evidence).
In adult outpatients with moderate to severely active Crohn’s disease, subcutaneous methotrexate is probably more effective than placebo for inducing remission (moderate certainty of evidence). In adult outpatients with quiescent moderate-severe Crohn’s disease, subcutaneous methotrexate is probably more effective than placebo for maintaining remission (moderate certainty of evidence). The benefit of oral methotrexate for inducing and maintaining remission in patients with moderate-severe Crohn’s disease is uncertain (very low certainty of evidence).
In adult outpatients with moderate to severe Crohn’s disease, the benefit of methotrexate over thiopurines for inducing or maintaining remission was uncertain (very low certainty of evidence).
Effect estimates and certainty of evidence:
Thiopurines for moderate-severe CD, induction and maintenance of remission:
Compared to the previous technical review in 2013, no new trials evaluating the efficacy of thiopurines for inducing remission were identified.10, 77 In 5 trials (380 patients), thiopurines were not significantly more effective than placebo in achieving corticosteroid-free clinical remission in corticosteroid-dependent patients with CD (Supplemental Figure 6A). The overall body of evidence supporting the use of thiopurines for induction of remission was rated as very low certainty, due to serious risk of bias (due to inadequate blinding and allocation concealment), indirectness (since these trials did not truly assess induction of remission, but rather the ability to achieve corticosteroid-free clinical remission, over a wide range of time, using a variety of disease activity indices with definitions inconsistent with modern definitions of remission) and serious imprecision (due to wide 95% CI) (Table 8). Since the last technical review, two more RCTs (beyond 3 RCTs in the original review) evaluating the efficacy of thiopurines for maintaining corticosteroid-free clinical remission were identified.78, 79 On meta-analysis, thiopurines were significantly more effective than placebo or no treatment (RR, 0.62; 95% CI, 0.47–0.81) for maintaining corticosteroid-free clinical remission (Supplemental Figure 6B). The overall body of evidence was rated down for serious risk of bias (inadequate blinding) and imprecision (due to low event rate not meeting optimal information size) (Table 8).
Table 8.
GRADE Evidence Profile comparing thiopurines, subcutaneous and oral methotrexate with placebo for induction and maintenance of remission in patients with moderate to severe luminal Crohn’s disease.
| THIOPURINES COMPARED TO PLACEBO FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with thiopurines | |||||
| Achieving clinical remission (CRITICAL) | 115/183 (62.8%) | 102/197 (51.8%) | RR 0.87 (0.71 to 1.06) | 82 fewer per 1,000 (from 182 fewer to 38 more) | 380 (5 RCTs) | ⨁◯◯◯1,2,3 VERY LOW |
| Relapse after achieving clinical remission (CRITICAL) | 75/172 (43.6%) | 49/175 (28.0%) | RR 0.62 (0.47 to 0.81) | 166 fewer per 1,000 (from 231 fewer to 83 fewer) | 347 (5 RCT) | ⨁⨁◯◯1,4 LOW |
| SUBCUTANEOUS METHOTREXATE COMPARED TO PLACEBO FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with subcutaneous methotrexate | |||||
| Achieving clinical remission (CRITICAL) | 38/47 (80.9%) | 57/94 (60.6%) | RR 0.75 (0.61 to 0.93) | 202 fewer per 1,000 (from 315 fewer to 57 fewer) | 141 (1 RCT) | ⨁⨁⨁◯4 MODERATE |
| Relapse after achieving clinical remission (CRITICAL) | 22/36 (61.1%) | 14/40 (35.0%) | RR 0.57 (0.35 to 0.94) | 263 fewer per 1,000 (from 397 fewer to 37 fewer) | 76 (1 RCT) | ⨁⨁⨁◯4 MODERATE |
| ORAL METHOTREXATE COMPARED TO PLACEBO FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with oral methotrexate | |||||
| Achieving clinical remission (CRITICAL) | 14/26 (53.8%) | 16/26 (61.5%) | RR 1.14 (0.72 to 1.82) | 75 more per 1,000 (from 151 fewer to 442 more) | 52 (1 RCT) | ⨁◯◯◯5,6 VERY LOW |
| Relapse after achieving clinical remission (CRITICAL) | 4/12 (33.3%) | 1/10 (10.0%) | RR 0.30 (0.04 to 2.27) | 233 fewer per 1,000 (from 320 fewer to 423 more) | 22 (1 RCT) | ⨁◯◯◯5,6 VERY LOW |
|
GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
Rated down for risk of bias (due to inadequate blinding and allocation concealment)
Rated down for indirectness (since these trials did not truly assess induction of remission, but rather the ability to achieve corticosteroid-free clinical remission, over a wide range of time, using a variety of disease activity indices with definitions inconsistent with modern definitions of remission)
Rated down for imprecision since 95% CI crosses unity
Rated down for imprecision since optimal information size not met (<200 events)
Rated down for indirectness (used low dose oral methotrexate <15mg/week)
Rated down for very serious imprecision due to very wide 95% CI (unable to rule out significant risk of harm with intervention)
Methotrexate (subcutaneous and oral) for moderate-severe CD, induction and maintenance of remission:
In contrast to the previous technical review, we opted to examine different routes and dosing of methotrexate separately, due to differences in efficacy. In one trial (141 patients) evaluating subcutaneous methotrexate (25mg per week) for induction of remission, methotrexate was significantly more effective than placebo for inducing remission (RR, 0.75; 95% CI, 0.61–0.93) (Supplemental Figure 7A).80 Similarly, in one trial (76 patients) evaluating subcutaneous methotrexate (15mg per week) vs. placebo for maintenance of remission in patients who achieved remission with 16–24 weeks of open-label subcutaneous methotrexate (25mg per week), Feagan and colleagues observed subcutaneous methotrexate was more effective than placebo for maintaining corticosteroid-free remission (RR, 0.57; 95% CI, 0.34–0.94) (Supplemental Figure 7B).81 The overall body of evidence supporting subcutaneous methotrexate for inducing and maintaining remission in patients with moderate-severe CD was moderate certainty, with evidence being rated down for imprecision due to small sample size (Table 8). In contrast, a single RCT examining oral methotrexate 12.5mg every week demonstrate this dose and route of administration was not effective for inducing remission in patients with corticosteroid-dependent active CD (RR, 1.14; 95% CI, 0.72–1.82) (Supplemental Figure 8A).82 In the same trial, risk of relapse in 22 patients achieving remission was not different between those continuing on oral methotrexate 12.5mg per week vs. those receiving placebo (RR, 0.30; 95% CI, 0.04–2.27) (Supplemental Figure 8B). The overall body of evidence was rated as very low certainty due to indirectness (use of low-dose methotrexate) and very serious imprecision (very wide 95% CI) (Table 8).
Thiopurine versus methotrexate for moderate-severe CD, induction and maintenance of remission:
The evidence profile for this comparison was similar to the previous technical review. No additional studies were identified. In three RCTs, with variables doses and routes of administration, methotrexate failed to show or exclude a beneficial or detrimental effect over thiopurines on failure of remission at 24 to 36 weeks (RR, 1.17; 95% CI, 0.82–1.67). The overall body of evidence was rated as very low certainty due to indirectness and very serious imprecision due to very wide confidence intervals. In two small RCTs (50 patients) in which patients who achieved remission with initial therapy were followed up to 38 to 76 weeks for risk of disease relapse, the results failed to show or exclude a beneficial effect of methotrexate over thiopurines (RR, 0.53; 95% CI 0.22–1.27). Evidence was rated as very low certainty due to indirectness (lack of randomization at start of maintenance therapy) and very serious imprecision due to very wide confidence intervals.
Potential Harms of Intervention:
Risks of side effects with thiopurines and methotrexate have been summarized above. Besides the direct risks associated with these therapies, risks associated with use of ineffective therapies and delay in initiation of more effective therapies also need to be considered when evaluating potential harms of these interventions.
Discussion:
Based on evidence presented above, thiopurine monotherapy may be effective for maintaining corticosteroid-free remission in patients with CD; however, the benefit of thiopurines for induction of remission is unclear. Thiopurines have a slow onset of action, and so they have conventionally been used as maintenance agents, rather than induction agents. In a double-blind clinical trial (AZTEC), Panes and colleagues randomly assigned patients with newly diagnosed CD (<8 weeks) to azathioprine vs. placebo.78 At 76 weeks, no significant differences were observed in rates of corticosteroid-free clinical remission, CD-related hospitalization or surgery between the two groups. On post-hoc analyses, in a subset of patients requiring corticosteroids at trial entry, no significant difference was observed between azathioprine vs. placebo for maintaining sustained corticosteroid-free clinical remission (17/37 [36.2%] vs. 13/45 [28.9%], p=0.51). In another post-hoc analysis, azathioprine-treated patients experienced lower risk of moderate to severe clinical relapse as compared to placebo-treated patients (8/68 [11.8%] vs. 19/63 [30.2%], p=0.01). Real-world cohort studies and meta-analyses have confirmed effectiveness of thiopurines in reducing the risk of surgery in patients with CD.83 Differences in the efficacy of methotrexate in CD were observed based on route of administration and dose; only subcutaneous methotrexate at doses of 15mg/week or higher was effective in achieving remission, whereas oral methotrexate at doses <15mg/week was not effective. It is unclear whether this is a function of the route of methotrexate administration, dose administered, or both.
Question 4. In adult outpatients with moderate-severe CD, is biologic monotherapy (infliximab, adalimumab, certolizumab pegol, vedolizumab, ustekinumab), superior to immunomodulator monotherapy (thiopurines, methotrexate) for induction and maintenance of clinical remission?
Key Messages:
In adult outpatients with moderate to severely active CD, biologic monotherapy may be superior to thiopurine monotherapy for achieving remission (low to moderate certainty of evidence). In patients with quiescent moderate to severe Crohn’s disease, biologic monotherapy may be superior to thiopurine monotherapy for maintaining remission (low certainty of evidence).
In adult outpatients with moderate to severe CD, the benefit of biologic monotherapy over subcutaneous methotrexate monotherapy for achieving and maintaining remission is uncertain (very low certainty of evidence).
Effect estimates and certainty of evidence:
Biologic monotherapy vs. thiopurine monotherapy for moderate-severe CD, induction and maintenance of remission:
Only a single, three-arm RCT, SONIC, in biologic- and immunomodulator-naïve patients with moderate-severe CD, comparing infliximab vs. azathioprine vs. infliximab+azathioprine was identified that directly informed this evidence.84 While this trial was not powered to examine differences in efficacy of infliximab vs. azathioprine, a significantly higher proportion of infliximab-treated patients achieved corticosteroid-free clinical remission at all time points, including week 6 (failure to achieve corticosteroid-free clinical remission, infliximab vs. azathioprine: 119/169 vs. 146/170, p<0.01) and 10 (106/169 vs. 129/170, p<0.01). At the 26-week primary efficacy endpoint of the trial, infliximab was more effective than azathioprine in achieving corticosteroid-free clinical remission (RR, 0.79; 95% CI, 0.67–0.94), and endoscopic remission (defined as resolution of ulcers) (65/93 vs. 91/109, p<0.01). Overall quality of evidence supporting the use of infliximab monotherapy over thiopurine monotherapy for induction of remission was rated as moderate certainty, being rated down for imprecision due to low event rate (Table 9).
Table 9.
GRADE Evidence Profile comparing biologic monotherapy vs. thiopurine monotherapy for achieving remission in patients with moderate to severe luminal Crohn’s disease. Note, no trials of non-TNF biologic therapy vs. thiopurines was identified.
| BIOLOGIC MONOTHERAPY COMPARED TO IMMUNOMODULATOR MONOTHERAPY FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with immunomodulator monotherapy | Risk with biologic monotherapy | |||||
| Induction of clinical remission (CRITICAL) | 129/170 (75.9%) | 90/169 (53.3%) | RR 0.70 (0.60 to 0.83) | 228 fewer per 1,000 (from 304 fewer to 129 fewer) | 339 (1 RCT) | ⨁⨁⨁◯1 MODERATE |
| Maintenance of clinical remission (CRITICAL) | 34/75 (45.3%) | 33/97 (34.0%) | RR 0.75 (0.52 to 1.09) | 113 fewer per 1,000 (from 281 fewer to 41 more) | 172 (blinded extension of 1 RCT) | ⨁⨁◯◯2,3 LOW |
|
GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
Rated down for imprecision since optimal information size not met (<200 events)
Rated down for indirectness (since characteristics of patients entering blinded extension was unclear, and did not necessarily included patients with quiescent disease; responding patients were not re-randomized)
Rated down for imprecision since 95% CI crosses unity
No trials of maintenance therapy in patients with quiescent moderate-severe CD comparing biologic monotherapy vs. thiopurine monotherapy were identified. The SONIC trial provided indirect evidence on efficacy of these agents for maintaining remission, with a subset of patients entering a blinded extension to 50 weeks. Baseline characteristics of patients who opted to enter the blinded extension is not available, so their remission status at the time of entering the blinded extension is unclear; it is conceivable that patients in remission or responding to index therapy may preferably choose to enroll in blinded extension. Of 97 infliximab monotherapy-treated and 75 azathioprine-treated patients who opted to participate in blinded extension to week 50, 33 and 34 patients failed to achieve corticosteroid-free clinical remission, respectively (RR, 0.75; 95% CI, 0.52–1.09). Overall quality of evidence supporting the use of infliximab monotherapy over thiopurine monotherapy for maintenance of remission was rated as low certainty, being rated down for indirectness (since characteristics of patients entering blinded extension was unclear and did not necessarily include patients with quiescent disease; responding patients were not re-randomized) and serious imprecision due to wide confidence intervals.
No trials comparing other biologic agents vs. thiopurines for induction or maintenance of remission were identified; evidence for this question was informed indirectly from evidence presented in focused questions 1 and 3. Low to moderate certainty evidence supported the use of biologic agents over placebo in inducing remission in patients moderate to severely active CD with failure of conventional therapy (frequently including patients who had failed thiopurine therapy), whereas very low certainty suggested uncertain benefit of thiopurines for induction of remission, in biologic-naïve patients. Hence, based on indirectness of evidence, the overall body of evidence supporting the use of non-infliximab biologic monotherapy over thiopurine monotherapy for induction of remission was rated as low certainty; no single summary estimate could be drawn. For maintenance of remission, in the absence of head-to-head comparison for non-infliximab biologic monotherapy vs. thiopurine monotherapy, and evidence in focused questions 1 and 3 providing low to moderate certainty evidence supporting the use of biologics and thiopurines for maintaining remission, the benefit of biologic monotherapy vs. thiopurine monotherapy for maintaining remission in patients with quiescent CD was uncertain (very low certainty of evidence, rated down for very serious indirectness and imprecision).
Biologic monotherapy vs. methotrexate monotherapy for moderate-severe CD, induction and maintenance of remission:
No RCTs comparing biologic monotherapy vs. methotrexate monotherapy for induction and maintenance of remission were identified. Evidence for this question was informed indirectly from evidence presented in focused questions 1 and 3. With low to moderate certainty evidence supporting the use of biologics and methotrexate for inducing and maintaining remission, the benefit of biologic monotherapy vs. methotrexate monotherapy for inducing and maintaining remission in patients with moderate-severe CD was uncertain (very low certainty of evidence, rated down for very serious indirectness and imprecision).
Potential Harms of Intervention:
As noted above, there may be a slightly higher risk of serious and opportunistic infections with biologic agents vs. immunomodulators. Both TNFα antagonists and thiopurine monotherapy have been associated with a comparable increase in risk of lymphoma.
Discussion:
The pivotal SONIC trial confirmed the efficacy of infliximab monotherapy vs. thiopurine monotherapy for inducing remission. In a subset of likely responding patients who opted to enroll in a blinded extension of SONIC to 50 weeks, infliximab monotherapy was not significantly more effective than azathioprine monotherapy for achieving clinical remission to 50 weeks. In contrast, in a network meta-analysis published in 2014, adalimumab and infliximab had a greater than 98% probability of being superior to thiopurines for maintenance of remission, although it is important to note that there is considerable heterogeneity in the design and conduct of trial comparing biologics and immunomodulators.85 Similarly, in viewing surgically-induced remission as a more robust form of disease quiescence, network meta-analyses have confirmed a higher efficacy of TNFα antagonists over thiopurine monotherapy for preventing endoscopic relapse and clinical relapse.86 Hence, indirect evidence may suggest that biologic agents, particularly, infliximab and adalimumab may be more effective than thiopurine monotherapy for maintaining remission.
Whether there is any difference between biologic monotherapy vs. methotrexate in inducing and maintaining of remission is unclear, given the lack of head-to-head trials. No significant differences were identified in the previously mentioned network meta-analysis for individual biologic agents vs. methotrexate, though adalimumab monotherapy had >90% probability of being superior to methotrexate for both induction or maintenance of remission.85
Question 5. In adult outpatients with moderate-severe CD, is combination therapy of a biologic agent (infliximab, adalimumab, certolizumab pegol, vedolizumab, ustekinumab) with an immunomodulator (thiopurines or methotrexate) superior to biologic monotherapy for induction and maintenance of remission?
Key Messages:
In adult outpatients with moderate to severely active CD, combination therapy with infliximab + thiopurines is probably superior to infliximab monotherapy for inducing remission (moderate certainty of evidence); combination therapy with infliximab + methotrexate may be superior to infliximab monotherapy for inducing remission (low certainty of evidence). In patients with quiescent moderate to severe Crohn’s disease, combination therapy with infliximab + thiopurines or methotrexate may be superior to infliximab monotherapy for maintaining remission (low certainty of evidence).
In adult outpatients with moderate-severe CD, combination therapy with adalimumab + thiopurines or methotrexate may be superior to adalimumab monotherapy for inducing and maintaining remission (very low certainty of evidence)
In adult outpatients with moderate-severe CD, the benefit of combination therapy with vedolizumab or ustekinumab + thiopurines or methotrexate over corresponding biologic monotherapy for inducing and maintaining remission is uncertain (very low certainty of evidence)
Effect estimates and certainty of evidence:
Combination therapy with infliximab + thiopurines vs. infliximab monotherapy for moderate-severe CD, induction and maintenance of remission:
Two trials provided data on the efficacy of infliximab + thiopurines vs. infliximab monotherapy in patients with moderate-severe CD.45, 84 Based on meta-analysis, combination therapy was more effective than infliximab monotherapy for induction of remission in patients with moderate to severely active CD (RR, 0.77; 95% CI, 0.64–0.92) (Supplemental Figure 9A). Overall quality of evidence supporting the use of combination therapy with infliximab + thiopurines over infliximab monotherapy for induction of remission was rated as moderate certainty, being rated down for imprecision due to low event rate (Table 10). Even though statistical heterogeneity was observed, both studies suggested a superior efficacy with variability being observed in the magnitude of effect. Hence, evidence was not rated down for heterogeneity.
Table 10.
GRADE Evidence Profile comparing the combination of biologics + immunomodulators (thiopurines, methotrexate) with biologic monotherapy for induction and maintenance of remission in patients with moderate to severe luminal Crohn’s disease.
| INFLIXIMAB + THIOPURINES COMPARED TO INFLIXIMAB MONOTHERAPY FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with infliximab monotherapy | Risk with infliximab + thiopurines | |||||
| Achieving clinical remission (CRITICAL) | 122/196 (62.2%) | 92/200 (47.5%) | RR 0.77 (0.64 to 0.92) | 143 fewer per 1,000 (from 224 fewer to 50 fewer) | 396 (2 RCTs) | ⨁⨁⨁◯1 MODERATE |
| Maintenance of clinical remission (CRITICAL) | 112/196 (57.1%) | 84/200 (42.0%) | RR 0.74 (0.60 to 0.90) | 149 fewer per 1,000 (from 229 fewer to 57 fewer) | 396 (2 RCTs) | ⨁⨁◯◯1,2 LOW |
| INFLIXIMAB + METHOTREXATE COMPARED TO INFLIXIMAB MONOTHERAPY FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with infliximab monotherapy | Risk with infliximab + methotrexate | |||||
| Achieving clinical remission (CRITICAL) | 14/63 (22.2%) | 15/63 (23.8%) | RR 1.07 (0.57 to 2.03) | 16 more per 1,000 (from 96 fewer to 229 more) | 126 (1 RCT) | ⨁⨁◯◯3 LOW |
| Maintenance of clinical remission (CRITICAL) | 17/63 (27.0%) | 20/63 (31.7%) | RR 1.18 (0.68 to 2.03) | 49 more per 1,000 (from 86 fewer to 278 more) | 126 (1 RCT) | ⨁⨁◯◯3 LOW |
| ADALIMUMAB + THIOPURINES COMPARED TO ADALIMUMAB MONOTHERAPY FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with adalimumab monotherapy | Risk with adalimumab + thiopurines | |||||
| Achieving clinical remission (CRITICAL) | 20/85 (30.8%) | 28/91 (30.8%) | RR 1.31 (0.80 to 2.14) | 73 more per 1,000 (from 47 fewer to 268 more) | 176 (1 RCT) | ⨁◯◯◯3,4,5 VERY LOW |
| Maintenance of clinical remission (CRITICAL) | 24/85 (28.2%) | 29/91 (31.9%) | RR 1.13 (0.72 to 1.78) | 37 more per 1,000 (from 79 fewer to 220 more) | 176 (1 RCT) | ⨁◯◯◯3,4,5 VERY LOW |
|
GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
Rated down for imprecision since optimal information size not met (<200 events)
Rated down for indirectness (since patients had active disease at baseline, rather than quiescent disease)
Rated down for very serious imprecision due to very wide 95% CI (unable to rule out significant risk of harm with intervention)
Rated down for risk of bias (unblinded study, very high rates of discontinuation due to treatment intolerance as compared to other studies)
Rated down for indirectness (used endoscopic remission as surrogate since primary outcome of clinical remission could be biased due to open-label design)
No true trials of maintenance therapy in patients with quiescent moderate-severe CD comparing infliximab + thiopurines vs. infliximab monotherapy were identified. Both the SONIC trial and RCT by Lemann et al included patients with active disease at baseline who were treated through week 50/52.45, 84 On meta-analysis, combination therapy was more effective than infliximab monotherapy for maintenance of remission (RR, 0.74; 95% CI, 0.60–0.90) (Supplemental Figure 9B). As above, the SONIC trial additionally provided indirect evidence on efficacy of these agents for maintaining remission, with a subset of patients entering blinded extension to 50 weeks. Baseline characteristics of patients who opted to enter blinded extension is not available, so their remission status at time of blinded extension is unclear; it is conceivable that patients in remission or responding to index therapy may preferably choose to enroll in blinded extension. Of 108 patients treated with infliximab + azathioprine and 97 infliximab monotherapy-treated patients who opted to participate in blinded extension to week 50, 28 and 33 patients failed to achieve corticosteroid-free clinical remission, respectively (RR, 0.76; 95% CI, 0.50–1.16). Overall quality of evidence supporting the use of combination therapy with infliximab + thiopurines over infliximab monotherapy for maintenance of remission was rated as low certainty, being rated down for indirectness (since patients had active disease at baseline, rather than quiescent disease) and imprecision due to low event rate (Table 10).
Combination therapy with infliximab + methotrexate vs. infliximab monotherapy for moderate-severe CD, induction and maintenance of remission:
In a single, double-blind, 50-week RCT, Feagan and colleagues compared infliximab + methotrexate vs. infliximab monotherapy in 126 patients with CD who had initiated prednisone induction therapy within the preceding 6 weeks.87 No significant differences were observed in failure to achieve corticosteroid-free clinical remission at week 14 between combination therapy and infliximab monotherapy (15/63 vs. 14/63; RR, 1.07; 95% CI, 0.57–2.03). Extending to 50 weeks, no significant differences were observed in failure to maintain corticosteroid-free clinical remission between combination therapy and infliximab monotherapy (20/63 vs. 17/63; RR, 1.18; 95% CI, 0.68–2.03). Indirect evidence suggested higher infliximab trough concentrations and lower risk of immunogenicity in patients receiving combination therapy as compared with patients receiving infliximab monotherapy, which has been associated with higher effectiveness and treatment persistence in infliximab-treated patients. Additionally, several large well-designed observational studies have confirmed higher effectiveness of combination therapy over biologic monotherapy, particularly for TNFα antagonists.88, 89 Hence, the overall body of evidence supporting the use of combination therapy with infliximab + methotrexate over infliximab monotherapy for induction and maintenance of remission was rated as low certainty, rated down for very serious imprecision (Table 10).
Combination therapy with adalimumab + thiopurines vs. adalimumab monotherapy for moderate-severe CD, induction and maintenance of remission:
In a single, open-label, RCT, from the DIAMOND study group in Japan, biologic-and immunomodulator-naïve patients with moderate to severely active CD were randomized to adalimumab + azathioprine vs. adalimumab monotherapy for 52 weeks.90 At 26 weeks (primary study end point), no significant differences were observed in failure to achieve clinical remission (28/91 vs. 20/85; RR, 1.31; 95% CI, 0.80–2.14). Importantly, in this trial, 15 patients (16.5%) treated with combination group and 1 patient (1.2%) in the adalimumab monotherapy group withdrew due to side effects of the medications, and primary analyses were performed using non-responder imputation. Such high rates of treatment-related drug withdrawals have not been observed with prior trials of thiopurine or combination therapy with infliximab. On objective evaluation of endoscopy at week 26, combination therapy was associated with significantly higher rates of endoscopic remission vs. adalimumab monotherapy (48/57 [84.2%] vs. 37/58 [63.2%], p=0.02). On extension to 52 weeks, no significant differences were observed for maintenance of clinical remission between combination therapy vs. adalimumab monotherapy (failure to maintain remission: 29/91 vs. 24/85; RR, 1.13; 95% CI, 0.72–1.78); data specifically for subset of patients in remission at week 26 were not available. On analysis of patients with endoscopy both at randomization and week 52 follow-up, no significant differences were observed in proportion of patients with endoscopic remission with combination therapy vs. adalimumab monotherapy (39/49 [79.6%] vs. 37/53 [69.8%], p=0.36). Overall, the quality of evidence supporting the use of combination therapy with adalimumab + thiopurines over adalimumab monotherapy for induction and maintenance of remission was rated as very low certainty, being rated down for risk of bias (unblinded study, very high rates of discontinuation due to treatment intolerance as compared to other studies), indirectness (use of endoscopic remission as surrogate, besides clinical remission) and imprecision (due to low event rate) (Table 10).
Combination therapy with vedolizumab or ustekinumab + thiopurines (or methotrexate) vs. vedolizumab or ustekinumab monotherapy for moderate-severe CD, induction and maintenance of remission:
No randomized trials were identified comparing combination therapy of newer non-TNF-targeting biologics with immunomodulators vs. monotherapy with the corresponding biologic. In a systematic review and meta-analysis of 9 studies of vedolizumab in CD (post-hoc analyses of RCTs and observational studies), combination therapy was not superior to vedolizumab monotherapy for achieving clinical outcomes during induction or maintenance (odds of favorable clinical outcomes: OR, 0.84; 95% CI, 0.53–1.33).91 Similarly, in 15 studies of ustekinumab, no benefit was observed with combination therapy vs. ustekinumab monotherapy (15 studies; OR, 1.1; 95% CI, 0.87–1.38). In this meta-analysis, clinical benefit was variably defined as clinical remission, clinical response, or physician global assessment, and studies evaluated both induction and maintenance of remission/response. Importantly, in both RCTs and observational studies, the majority of patients had previously failed immunomodulators. The overall body of evidence supporting the use of combination therapy of newer non-TNF-targeting biologics with immunomodulators vs. monotherapy with the corresponding biologic derived primarily from observational studies was rated as very low certainty due to risk of bias and very serious imprecision.
Potential Harms of Intervention:
As noted above, combination therapy with biologic agents + immunomodulators may be associated with a modestly higher risk of serious infections over biologic monotherapy. The combination of thiopurines with TNF-α antagonists is associated with a 2–3 fold higher risk of lymphoma, as compared to TNF-α antagonist monotherapy.
Discussion:
Combining biologic agents with immunomodulators may increase efficacy through several potential mechanisms. First, immunomodulators have their independent efficacy in patients with CD, which may add to the benefits observed with biologics. Second, immunomodulators have been consistently shown to decrease the risk of immunogenicity of biologic agents, and may increase trough concentrations of these agents. The former may explain clear benefits in achieving clinical and endoscopic remission with infliximab + azathioprine in the SONIC trial, as well as higher rates of endoscopic remission with adalimumab + azathioprine in the DIAMOND trial. In contrast, in the COMMIT trial comparing infliximab + methotrexate vs. infliximab monotherapy, approximately 25% patients had previously failed thiopurines.
TNFα antagonists, particularly infliximab, are more immunogenic as compared to more recently developed non-TNF-directed biologic agents. In a systematic review, 2.9–60.8%, 0.3–35.0%, 3.3–25.3%, 1–4.1% and <1% of infliximab-, adalimumab-, certolizumab pegol-, vedolizumab- and ustekinumab-treated patients developed anti-drug antibodies, with a significant proportion of these being neutralizing antibodies.92 Hence, adding immunomodulators to prevent immunogenicity in TNFα antagonist-treated patients may be particularly beneficial in patients with unfavorable pharmacokinetics, or those with prior immunogenicity to TNFα antagonists, even in patients who previously failed to respond to immunomodulators. In a recent RCT in patients with IBD with pharmacokinetic failure of 1st TNFα antagonist, Roblin and colleagues observed that adding thiopurines at time of starting the 2nd TNFα antagonist significantly decreased risk of clinical relapse and unfavorable pharmacokinetics, as compared to TNFα antagonist monotherapy.93 In contrast, with very low rates of immunogenicity with vedolizumab or ustekinumab, the potential benefit of combination therapy with these agents in terms of mitigating antibody formation may be less than with TNFα antagonists.
Question 6. In adult outpatients with quiescent CD on combination therapy with biologic agents and immunomodulators for >6 months, is ongoing combination therapy superior to withdrawal of immunomodulators or biologic agent in decreasing the risk of relapse?
Key Messages:
In adult patients with quiescent CD on combination therapy with biologic and immunomodulators for >6 months, the benefit of ongoing combination therapy over withdrawal of immunomodulators is uncertain (very low certainty of evidence).
In adult patients with quiescent CD on combination therapy with biologic and immunomodulators for >6 months, the benefit of ongoing combination therapy over withdrawal of biologics is uncertain (very low certainty of evidence).
Effect estimates and certainty of evidence:
We identified three RCTs (161 patients) in patients who achieved and maintained remission on combination therapy with TNFα antagonists and immunomodulators (majority on thiopurines) on for at least 6m (2 trials of infliximab-, 1 trial of adalimumab-based combination therapy).94–96 On meta-analysis, no significant differences were observed in the risk of relapse over 12–24m in patients who continued combination therapy vs. withdrew immunomodulators (28/78 vs. 29/83; RR, 1.02; 95% CI, 0.71–1.46) (Supplemental Figure 10). The overall body of evidence supporting the continuation of combination therapy was rated as very low certainty, with evidence being rated down for serious risk of bias (unblinded trials) and very serious imprecision (due to very wide 95% CI, unable to exclude significant benefit or harm with continuing combination therapy) (Table 11).
Table 11.
GRADE Evidence Profile comparing continuation of combination of biologic agent + immunomodulator therapy (thiopurines, methotrexate) vs. withdrawal of immunomodulators for preventing relapse in adult patients with quiescent CD on combination therapy with biologic and immunomodulators for >6 months.
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
|---|---|---|---|---|---|---|
| Risk with continuing combination of biologic agent + immunomodulator therapy | Risk with withdrawal of immunomodulators | |||||
| Risk of relapse at 12m (CRITICAL) | 28/78 (35.9%) | 29/83 (34.9%) | RR 1.02 (0.71 to 1.46) | 7 more per 1,000 (from 101 fewer to 161 more) | 161 (3 RCT) | ⨁◯◯◯1,2 VERY LOW |
Rated down for risk of bias (unblinded studies)
Rated down for very serious risk of imprecision (due to very wide 95% CI, unable to exclude significant benefit or harm with continuing combination therapy
No RCTs evaluating systematic withdrawal of biologic therapy in patients with quiescent CD on combination therapy were identified. In a prospective cohort study of 115 CD patients on combination therapy for >1y, with clinical remission for at least >6m, withdrawal of infliximab was associated with 44% and 52% risk of relapse at 1- and 2-years.97 The vast majority of patients were able to re-capture response with re-introduction of infliximab, and the de-escalation strategy was deemed to be successful in 70% patients over 7 years.98
Potential Harms of Intervention:
Primary potential harm of intervention is risk of disease relapse with withdrawal of immunomodulators. Additionally, since immunomodulators favorably modify the pharmacokinetics of biologics, and decrease risk of immunogenicity, it is possible that patients may lose response to biologic therapy. However, the risk may be small, especially if biologic trough concentrations are monitored closely. Besides risk of relapse, one concern with withdrawal of a biologic (and continuation of immunomodulators) is development of immunogenicity with prolonged drug holiday, which may render the drug ineffective in a small proportion of patients at time of re-introduction and cause infusion reactions. As noted earlier, long-term combination therapy with biologic agents + immunomodulators may be associated with a modestly higher risk of serious infections, and 2–3 fold higher risk of lymphoma, over biologic monotherapy. Lymphoma risks returns to baseline within 12 months of stopping thiopurines.99
Discussion:
In patients with long-standing quiescent CD, de-escalation of immunosuppressive therapy is one of the most frequently asked questions by patients. Given risk of relapse with treatment de-escalation, shared decision-making and eliciting patients’ values and preferences regarding acceptable risks of relapse with de-escalation are important. Systematic withdrawal of immunomodulators with continuation of biologic monotherapy is one favored de-escalation strategy in patients on combination therapy. Based on three open-label RCTs, withdrawal of immunomodulators in selected patients with quiescent CD for at least 6m was not associated with increased risk of relapse over 12–24m as compared with continuation of combination therapy. Moreover, withdrawal of immunomodulators was not associated with emergence of unfavorable pharmacokinetics in patients who continued on biologic monotherapy.
No trials evaluated discontinuation of biologics in patients who were in remission on combination therapy. Most studies suggest a 35–45% risk of relapse within 1–2 years of discontinuing TNFα antagonists, which may be unacceptable to patients.100 However, with recognition that endoscopic and/or histologic remission may represent deeper remission in patients with CD, the predicted risk of relapse with de-escalation may be lower in patients who achieve these endpoints on combination therapy, as compared to those only in clinical and biochemical remission. Additionally, with the emergence of newer therapies with different mechanisms of action and lower immunogenicity, risks of withdrawal of biologic therapy may be lower since alternative therapies may be available to manage relapse in case re-introduction of index biologic therapy is not effective.
Question 7. In adult outpatients with moderate to severe CD, is a top-down treatment strategy (early use of combination therapy with biologic agents with immunomodulators) superior to step therapy (escalation to biologic-based therapy only after failure of 5-aminosalicylates and/or immunomodulators) for achieving remission, and preventing disease complications?
Key Message:
In adult outpatients with moderate to severely active Crohn’s disease, a top-down treatment strategy (early use of combination therapy with biologic agents with immunomodulators) may be more effective than step therapy (escalation to biologic-based therapy only after failure of 5-aminosalicylates and/or immunomodulators) for achieving remission and preventing disease-related complications (low certainty of evidence)
Effect estimates and certainty of evidence:
Evidence informing this question was derived from several different types of RCTs. In an open-label RCT in 133 patients with recently diagnosed CD who were naïve to corticosteroids, immunomodulators and biologics, D’Haens and colleagues randomized patients with active disease to early combined immunosuppression (3 doses of infliximab induction therapy followed by episodic dosing as needed) vs. conventional step therapy in which patients received corticosteroids, followed, in sequence, by azathioprine and infliximab.101 At 52 weeks, 40/65 (61.5%) patients in the early combined immunosuppression group were in corticosteroid- and surgery-free remission without corticosteroids, as compared with compared with 23/64 (42.2%) patients in the step therapy arm (RR for failure to achieve remission, 0.67; 95% CI, 0.46–0.97). Long-term extension of this trial to 8 years suggested lower rates of clinical relapse, corticosteroid use and TNFα antagonist use in patients randomized to early combined immunosuppression.102 The evidence from this trial was rated as low certainty due to risk of bias (due to open-label trial evaluating a subjective outcome), and imprecision (since optimal information size not reached) (Table 12). In another open-label cluster randomized trial (REACT), 39 community practices to either an algorithmic approach of early combined immunosuppression, or conventional management of CD, and followed 1,982 patients for 2 years.103 In the early combined immunosuppression group, practitioners were educated on initiation of adalimumab and immunomodulator in case of failure to achieve clinical remission with a 4–12 week tapering course of corticosteroids, whereas practitioners in the usual care group were allowed to manage per preference. At 12m, there was no significant difference in the rate of corticosteroid-free clinical remission in the two groups (early combined immunosuppression vs. usual care: 66% vs. 62%), which was the primary outcome of the study. However, at 24-months, patients in practices randomized to early combined immunosuppression had significantly lower rates of major adverse disease-related complications (composite of hospitalization, surgery or disease complications including abscess, fistula, stricture, serious worsening of disease activity or extra-intestinal manifestations) as compared to conventional management (hazard ratio, 0.73; 95% CI, 0.62–0.86). Evidence from REACT was rated as moderate certainty due to risk of bias (open-label trial, with site-level and not patient-level randomization) (Table 12). Both of these trials supposed early use of combination therapy with biologics, specifically infliximab and adalimumab and immunomodulators in patients with active CD. In REACT, the risk of CD-related complications was lower with early combined immunosuppression in a subset of patients with corticosteroid-dependent, or corticosteroid-refractory CD.
Table 12.
GRADE Evidence Profile comparing top-down treatment strategy (early use of combination therapy with biologic agents with immunomodulators) versus step therapy (escalation to biologic-based therapy only after failure of 5-aminosalicylates and/or immunomodulators), and early thiopurine therapy versus conventional therapy, for achieving remission and preventing disease complications for moderate to severe luminal Crohn’s disease
| TOP-DOWN TREATMENT STRATEGY (EARLY USE OF COMBINATION THERAPY WITH BIOLOGIC AGENTS WITH IMMUNOMODULATORS) VERSUS STEP THERAPY (ESCALATION TO BIOLOGIC-BASED THERAPY ONLY AFTER FAILURE OF 5-AMINOSALICYLATES AND/OR IMMUNOMODULATORS) FOR ACHIEVING REMISSION AND PREVENTING DISEASE COMPLICATIONS FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with step therapy | Risk with early combined immunosuppression | |||||
| Achieving clinical remission (CRITICAL) | 26/65 (40.0%) | 41/64 (64.1%) | RR 0.62 (0.44 to 0.89) | 243 fewer per 1,000 (from 359 fewer to 70 fewer) | 129 (1 RCT) | ⨁⨁◯◯1,2 LOW |
| Preventing disease complications (CRITICAL) | 342/898 (38.1%) | 369/1084 (34.0%) | HR 0.73 (0.62 to 0.86) | 103 fewer per 1,000 (from 145 fewer to 53 fewer) | 1982 (1 RCT) | ⨁⨁⨁◯1 MODERATE |
| EARLY THIOPURINE THERAPY (AT OR WITHIN 6 MONTHS OF DIAGNOSIS) VS. CONVENTIONAL THERAPY FOR PREVENTING DISEASE FLARE FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with conventional therapy | Risk with early thiopurine use | |||||
| Failure to achieve corticosteroid-free remission (CRITICAL) | 61/67 (91.0%) | 58/65 (89.2%) | RR 1.02 (0.91 to 1.14) | 18 more per 1,000 (from 82 fewer to 127 more) | 132 (1 RCT) | ⨁⨁◯◯1,3 LOW |
|
GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
Rated down for risk of bias (open-label trial)
Rated down for imprecision since optimal information size not met (<200 events)
Rated down for imprecision since 95% CI crosses unity
In contrast, 5-aminosalicylates are not effective for the management of moderate-severe CD (see question 9 below). While thiopurines are effective for maintaining remission in patients with quiescent CD, its role in step therapy was informed in an open-label trial of adults with recently diagnosed CD at risk for disabling disease.79 In this trial, Cosnes and colleagues randomized 122 patients to either early initiation of azathioprine (within 6m of CD diagnosis) vs. conventional management in which azathioprine was introduced only in cases of corticosteroid dependency, chronic active disease with frequent flares, poor response to corticosteroids, or development of severe perianal disease. Over a 3-year follow-up, time spent in corticosteroid-free clinical remission was comparable between the two treatment groups. No significant differences were observed in the risk of corticosteroid-requiring flare (58/65 [89%] vs. 61/67 [91%], p=0.73), hospitalization (22/65 [34%] vs. 26/67 [39%], p=0.74) or CD-related surgery (5/65 [8%] vs. 4/67 [6%], p=0.68). Evidence from this trial was rated as low certainty due to risk of bias (open-label trial) and imprecision (very wide confidence intervals) (Table 12).
Based on these trials, combining direct evidence favoring early combined immunosuppression over conventional management, and indirect evidence suggesting lack of benefit of 5-aminosalicylates in moderate-severe CD and lack of benefit of early azathioprine use over azathioprine-based step therapy, we inferred that a top-down treatment strategy based on combination therapy may be more effective then step therapy in which biologics are introduced only after failure of 5-aminosalicylates and/or immunomodulators. Evidence was rated as low certainty due to risk of bias noted in contributing evidence and indirectness (differences in comparators, variability in outcomes).
Potential Harms of Intervention:
Routine implementation of early combined immunosuppression may overtreat some patients, particularly those at low risk of CD-related complications Risks associated with combination therapy have been discussed earlier. However, these risks should be interpreted in the context of risks of CD-related complications that may be associated with step therapy.
Discussion:
Registrations trials and subsequent regulatory approval for biologics focused on patients who had failed conventional management with 5-aminosalicylates and/or immunomodulators. They provide limited guidance on optimal timing of use of these agents in the management of CD. As noted earlier, treatment strategy in which patients gradually step up from 5-aminosalicylates and/or immunomodulators to biologic-based therapy may not suitable, especially for patients at high-risk of disease complications, in whom early introduction of biologics agents combined with immunomodulators may be preferred. At the same time, routine use of early combined immunosuppression for all patients may overtreat some patients, exposing them to treatment-related risks and costs without substantial benefit. Optimal risk stratification and subsequent implementation of risk-congruent treatment strategies are warranted to minimize the risk of short- and long-term complications and bowel damage. Unfortunately, prediction models to identify patients at high risk of complications or ‘disease severity’ indices have not been well validated. Ideally, evidence regarding top-down vs. step-up therapy would be best informed by a pragmatic RCT comparing outcomes in patients assigned to risk-congruent therapy vs. conventional management.
Question 8. In adult outpatients with moderate to severe CD, what is the efficacy of corticosteroids (prednisone or budesonide) for induction and maintenance of remission?
Key Messages:
In adult outpatients with moderate to severely active Crohn’s disease involving the distal ileum, controlled ileal release budesonide may be effective for inducing remission (low certainty of evidence). In patients with quiescent moderate-severe CD involving the distal ileum, controlled ileal release budesonide may be effective for maintaining remission (low certainty of evidence). However, it important to note that budesonide has only been approved by the FDA for mild-moderate CD for short term use.
In adult outpatients with moderate to severely active Crohn’s disease, prednisone may be effective for inducing remission (low certainty of evidence). In patients with quiescent moderate-severe CD, prednisone may not be effective for maintaining remission (low certainty of evidence).
In adult outpatients with moderate to severely active Crohn’s disease involving the distal ileum, prednisone is probably more effective than controlled ileal release budesonide for inducing remission (moderate certainty of evidence).
Effect estimates and certainty of evidence:
Budesonide vs. placebo, induction and maintenance of remission:
We identified three RCTs (367 patients) comparing controlled ileal release (CIR) budesonide vs. placebo in patients with CD involving distal ileum and/or ascending colon for induction of remission; two trials were conducted exclusively in patients with mild-moderate CD.104–106 On meta-analysis, CIR budesonide 9mg/d was more effective than placebo in inducing remission (RR, 0.74; 95% CI, 0.60–0.91) (Supplemental Figure 11A). Quality of evidence was rated as low, rated down for indirectness (trials focused on patients with mild to moderately active disease, with CDAI between 180–400) and imprecision (optimal information size not met) (Table 13).
Table 13.
GRADE Evidence Profile comparing budesonide versus systemic corticosteroids versus placebo, for inducing and maintaining remission for moderate to severe luminal Crohn’s disease
| BUDESONIDE COMPARED TO PLACEBO FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE INVOLVING DISTAL ILEUM AND/OR CECUM AND ASCENDING COLON | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with budesonide | |||||
| Induction of clinical remission (CRITICAL) | 104/133 (78.2%) | 131/246 (53.3%) | RR 0.74 (0.60 to 0.91) | 203 fewer per 1,000 (from 313 fewer to 70 fewer) | 379 (3 RCT) | ⨁⨁◯◯1,2 LOW |
| Maintenance of clinical remission (CRITICAL) | 78/145 (53.8%) | 62/145 (42.8%) | RR 0.79 (0.62 to 1.00) | 113 fewer per 1,000 (from 204 fewer to 0 fewer) | 290 (4 RCT) | ⨁⨁◯◯1,2 LOW |
| 2 Rated down for imprecision since optimal information size not met (<200 events) | ||||||
| SYSTEMIC CORTICOSTEROIDS COMPARED TO PLACEBO FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with prednisone | |||||
| Induction of clinical remission (CRITICAL) | 91/135 (67.4%) | 53/132 (40.2%) | RR 0.57 (0.45 to 0.72) | 290 fewer per 1,000 (from 371 fewer to 182 fewer) | 267 (2 RCTs) | ⨁⨁◯◯1,2 LOW |
| Maintenance of clinical remission (CRITICAL) | 94/131 (71.8%) | 95/138 (68.8%) | RR 1.01 (0.81 to 1.29) | 7 more per 1,000 (from 136 fewer to 208 more) | 269 (3 RCTs) | ⨁⨁◯◯3,4 LOW |
| 4 Rated down for imprecision (wide 95% CI that could not exclude significant benefit or harm) | ||||||
| BUDESONIDE COMPARED WITH SYSTEMIC CORTICOSTEROIDS FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with systemic corticosteroids | Risk with budesonide | |||||
| Induction of clinical remission (CRITICAL) | 179/295 (60.7%) | 186/356 (52.2%) | RR 1.20 (1.01 to 1.44) | 79 more per 1,000 (from 4 more to 173 more) | 651 (5 RCT) | ⨁⨁⨁◯1 MODERATE |
|
GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
| 1 Rated down for risk of bias (sequence generation and allocation concealment not adequately reported) | ||||||
We identified four RCTs (290 patients) comparing controlled ileal release (CIR) budesonide vs. placebo in patients with CD involving distal ileum and/or ascending colon for maintenance of budesonide-induced clinical remission.107–110 On meta-analysis, CIR budesonide 6mg/d was more effective than placebo in maintaining remission at 1 year (RR, 0.79; 95% CI, 0.62–1.00) (Supplemental Figure 11B). Quality of evidence was rated as low, rated down for indirectness (patients with mild to moderately active disease who may intrinsically be at lower risk of relapse as compared to patients with moderate to severely active CD) and imprecision (95% CI reaching unity) (Table 13).
Systemic corticosteroids vs. placebo, induction and maintenance of remission:
In two RCTs (267 patients) conducted in 1979 and 1984 in patients with active CD, systemic corticosteroids at prednisone dose equivalents up to 60mg/d were more effective than placebo in inducing clinical remission (RR, 0.57; 95% CI, 0.45–0.73) (Supplemental Figure 12A).111, 112 The overall quality of evidence was rated as low certainty, being rated down for serious risk of bias (sequence generation and allocation concealment not adequately reported) and imprecision (optimal information size not met); though considerable heterogeneity was observed in effect estimates, both trials demonstrated higher efficacy with the intervention and evidence was not rated down for inconsistency (Table 13).
In three RCTs (269 patients), systemic corticosteroids were no more effective than placebo for maintaining corticosteroid-induced remission (RR, 1.02; 95% CI, 0.81–1.29) (Supplemental Figure 12B).111–113 The overall body of evidence was rated down due to risk of bias (unclear randomization scheme) and serious imprecision (wide 95% CI that could not exclude significant benefit or harm) (Table 13).
Budesonide vs. systemic corticosteroids, induction and maintenance of remission:
In five RCTs (651 patients) comparing CIR budesonide vs. systemic corticosteroids in patients with CD involving distal ileum and/or ascending colon for induction of remission (majority with mild-moderately active disease) over 8–12 weeks, CIR budesonide was inferior to systemic corticosteroids for inducing remission (RR for failure to induce remission, 1.20; 95% CI, 1.01–1.44) (Supplemental Figure 13).114–118 Overall quality of evidence was rated as moderate, being rated down for risk of bias (sequence generation and allocation concealment not reported adequately) (Table 13).
Potential harms of intervention:
Side effects of short- and long-term systemic corticosteroid therapy are well known, and include (but are not limited to) weight gain, irritability and mood disturbances, insomnia, increased risk of serious infections, hyperglycemia, hypertension, osteoporosis, cataract, adrenal insufficiency, etc. CIR budesonide is better tolerated, and due to extensive first-pass metabolism in the liver, systemic corticosteroid exposure is very low. In maintenance trials up to 1 year, budesonide 6mg/d did not significant lower serum cortisol levels and did not adversely impact bone density.
Discussion:
Corticosteroids play a critical role in the symptomatic management of patients with active luminal CD across the spectrum of disease activity. They are rapidly acting and induce clinical improvement within 1 week in the majority of patients. CIR budesonide, by virtue of its localized release in the distal ileum and high first-pass metabolism, is effective for mild to moderately active distal ileal and/or ascending colon CD and may be better tolerated than systemic corticosteroids. However, neither of these agents are recommended for long-term use. While systemic corticosteroids were not shown to be effective for maintenance of remission, CIR budesonide was effective in a subset of patients with mild-moderate CD in budesonide-induced clinical remission. There’s limited data on budesonide’s ability to achieve endoscopic remission, and it’s effect on modifying the risk of disease-related complications. Use of CIR budesonide for maintenance therapy may distract from use of an optimal and effective maintenance therapy such as immunomodulators and/or biologic agents. The FDA has approved CIR budesonide only for short-term use, and not as long-term maintenance therapy.
Question 9. In adult outpatients with moderate to severe CD, what is the efficacy of sulfasalazine and 5-aminosalicylates for induction and maintenance of remission?
Key Messages:
In adult outpatients with moderate to severely active CD, sulfasalazine may be effective for induction of remission (very low certainty of evidence). In adult outpatients with quiescent moderate-severe CD, the benefit of sulfasalazine for maintenance of remission is uncertain (very low certainty of evidence).
In adult outpatients with moderate to severely active CD, the benefit of mesalamine for induction of remission is uncertain (very low certainty of evidence). In adult outpatients with quiescent moderate-severe CD, mesalamine is probably not effective for maintenance of remission (moderate certainty of evidence).
Effect estimates and certainty of evidence:
Sulfasalazine vs. placebo/no treatment, induction and maintenance of remission:
We relied on previously published meta-analysis to inform this body of evidence; these meta-analyses were rated as moderate quality.119–121 In three RCTs (289 patients) conducted between 1979 to 1984 in patients with active CD (unclear disease severity or activity), sulfasalazine was more effective than placebo for induction of remission over 6 to 17 weeks (RR, 0.78; 95% CI, 0.65–0.93) (Supplemental Figure 14). Overall quality of evidence was rated as very low certainty, rated down for serious risk of bias (sequence generation and allocation concealment not reported adequately), indirectness (baseline disease activity not well-defined as contemporary trials with inclusion of patients with mild to moderately active disease) and imprecision (optimal information size not met) (Table 14).
Table 14.
GRADE Evidence Profile comparing sulfasalazine and mesalamine versus placebo, for inducing and maintaining remission for moderate to severe luminal Crohn’s disease
| SULFASALAZINE COMPARED TO PLACEBO FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |||||||
| Risk with placebo | Risk with sulfasalazine | |||||||||||
| Induction of clinical remission (CRITICAL) | 105/148 (70.9%) | 78/141 (55.3%) | RR 0.78 (0.65 to 0.93) | 156 fewer per 1,000 (from 248 fewer to 50 fewer) | 289 (3 RCTs) | ⨁◯◯◯1,2,3 VERY LOW | ||||||
| Maintenance of clinical remission (CRITICAL) | 132/225 (58.7%) | 112/190 (58.9%) | RR 0.98 (0.82 to 1.17) | 12 fewer per 1,000 (from 106 fewer to 100 more) | 415 (4 RCTs) | ⨁◯◯◯1,4,5 VERY LOW | ||||||
| 5 Rated down for very serious imprecision (wide 95% CI that could not exclude significant benefit or harm) | ||||||||||||
| MESALAMINE COMPARED WITH SYSTEMIC CORTICOSTEROIDS FOR MODERATE TO SEVERE LUMINAL CROHN’S DISEASE | ||||||||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |||||||
| Risk with placebo | Risk with mesalamine | |||||||||||
| Induction of clinical remission (CRITICAL) | 109/127 (85.8%) | 142/185 (76.8%) | RR 0.90 (0.80 to 1.00) | 68 more per 1,000 (from 72 fewer to 268 more) | 312 (2 RCTs) | ⨁◯◯◯1,2,3 VERY LOW | ||||||
| Maintenance of clinical remission (CRITICAL) | 472/1016 (46.5%) | 472/998 (47.3%) | RR 1.03 (0.92 to 1.16) | 14 more per 1,000 (from 37 fewer to 74 more) | 2014 (11 RCTs) | ⨁⨁⨁◯4 MODERATE | ||||||
|
GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||||||||
| 4 Rated down for serious imprecision (wide 95% CI that could not exclude significant benefit or harm) | ||||||||||||
In four RCTs (415 patients) conducted between 1977 to 1984 in patients with quiescent CD, no significant difference was observed between sulfasalazine and placebo for maintenance of corticosteroid-free clinical remission (RR, 0.98; 95% CI, 0.82–1.17). The overall body of evidence was rated as very low certainty, with evidence being rated down for serious risk of bias (sequence generation and allocation concealment not reported adequately), indirectness (wide variability in patient characteristics and outcome measures) and very serious imprecision (very wide 95% CI) (Table 14).
Mesalamine vs. placebo/no treatment, induction and maintenance of remission:
In two RCTs in patients with active CD (unclear disease severity or activity) comparing mesalamine vs. placebo (excluding two trials in which concomitant prednisone was allowed), mesalamine did not reach the pre-specified MCID threshold of 10% over placebo (RR, 0.90; 95% CI, 0.81–1.00) (Supplemental Figure 15A). Overall quality of evidence was rated as very low, being rated down for risk of bias, indirectness (wide variability in patient characteristics and outcome measures) and imprecision (MCID of 10% over placebo not met) (Table 14).
In 11 RCTs (2,014 patients) in patients with quiescent CD, mesalamine was not more effective than placebo for maintaining remission (RR, 1.02; 95% CI, 0.92–1.16) (Supplemental Figure 15B). The overall body of evidence favoring lack of difference between mesalamine and placebo for maintenance of remission was rated as moderate, with evidence being rated down for imprecision (modest benefit and harm could not be excluded). Though there was indirectness due to wide variability in patient characteristics and outcome measures, it was deemed that applying these findings to patients with moderate to severe CD would further bias findings towards null (Table 14).
Potential harms of intervention:
Mesalamine is well-tolerated and is not an immunosuppressive medication and carries low risk of major side effects. In contrast, sulfasalazine is not as well tolerated as mesalamine, with higher rate of treatment discontinuation due to adverse events. The main risks associated with the use of these therapies with uncertain efficacy for inducing remission in patients with CD are due to delay in initiation of more effective therapies which leads to higher risk of disease-related complications. Moreover, these medications have not been shown to be effective for maintenance of remission, which would warrant switching to an alternative therapy which would likely be an immunosuppressive agent. Hence, any potential long-term safety advantage may be lost.
Discussion:
Mesalamine is the most commonly used medication for patients with CD, despite evidence suggesting a lack of efficacy for both induction and maintenance of remission.122 While the premise of using a non-immunosuppressive, oral agent is appealing to both patients and providers, reliance on these ineffective medications in patients with moderate-severe CD, at high risk of disease complications, is likely to cause harm due to inadequate disease control. These medications are not approved by the FDA for use in patients with CD, let alone patients with moderate-severe CD.
PHARMACOLOGICAL MANAGEMENT OF ADULT PATIENTS WITH FISTULIZING CROHN’S DISEASE
Question 10. In adults with fistulizing CD, what is the efficacy and safety of the following drugs: TNF-α antagonists (infliximab, adalimumab, certolizumab pegol), vedolizumab, ustekinumab, immunomodulator monotherapy (thiopurines, methotrexate) and antibiotics?
Key Messages:
In adults with symptomatic fistulizing CD, infliximab is probably effective for achieving fistula closure (moderate certainty of evidence). In patients with fistulizing CD in remission, infliximab is probably effective for maintaining fistula closure (moderate certainty of evidence).
In adults with symptomatic fistulizing CD, the benefit of adalimumab and certolizumab pegol in achieving fistula closure is uncertain (very low certainty of evidence). In patients with fistulizing CD in remission, adalimumab and certolizumab pegol may be effective for maintaining fistula closure (low certainty of evidence).
In adults with symptomatic fistulizing CD, the benefit of vedolizumab in achieving fistula closure is uncertain (low quality evidence). In patients with fistulizing CD in remission, vedolizumab may be effective for maintaining fistula closure (low certainty of evidence).
In adults with symptomatic fistulizing CD, ustekinumab may be effective for achieving fistula closure (low quality evidence). In patients with fistulizing CD in remission, ustekinumab may be effective for maintaining fistula closure (low certainty of evidence).
In adults with symptomatic fistulizing CD, the benefit of immunomodulator monotherapy in achieving fistula closure is uncertain (very low certainty of evidence). In patients with fistulizing CD in remission, immunomodulator monotherapy may be effective for maintaining fistula closure (low certainty of evidence).
In adults with symptomatic fistulizing CD, antibiotic monotherapy with ciprofloxacin may have a small benefit in achieving fistula closure (low certainty of evidence).
Effect estimates and certainty of evidence:
Infliximab vs. placebo, achieving and maintaining fistula remission:
In one clinical trial of 94 patients with CD with symptomatic draining fistula (90% perianal), infliximab was more effective than placebo for achieving complete fistula closure on 2 consecutive visits (RR, 0.52; 95% CI, 0.34–0.78) within 18 weeks.123 Quality of evidence was rated as moderate, being rated down for imprecision (optimal information size not met). In one RCT of 194 patients with CD who achieved fistula response with induction therapy (90% perianal), maintenance therapy with infliximab was effective in maintaining fistula remission at 54 weeks.124 Quality of evidence was rated as moderate, being rated down for imprecision (optimal information size not met) (Table 15).
Table 15.
GRADE Evidence Profile evaluating biologic agents versus placebo for achieving and maintaining fistula remission in patients with moderate to severe fistulizing Crohn’s disease.
| INFLIXIMAB COMPARED TO PLACEBO FOR MODERATE TO SEVERE FISTULIZING CROHN’S DISEASE | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with infliximab | |||||
| Achieving fistula remission (CRITICAL) | 27/31 (87.1%) | 14/31 (45.2%) | RR 0.52 (0.34 to 0.78) | 418 fewer per 1,000 (from 575 fewer to 192 fewer) | 62 (1 RCT) | ⨁⨁⨁◯1 MODERATE |
| Maintenance of fistula remission (CRITICAL) | 79/99 (79.8%) | 58/96 (60.4%) | RR 0.76 (0.63 to 0.92) | 192 fewer per 1,000 (from 295 fewer to 64 fewer) | 195 (1 RCT) | ⨁⨁⨁◯1 MODERATE |
| ADALIMUMAB COMPARED TO PLACEBO FOR MODERATE TO SEVERE FISTULIZING CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with adalimumab | |||||
| Achieving fistula remission (CRITICAL) | 28/31 (90.3%) | 31/32 (90.3%) | RR 1.08 (0.93 to 1.27) | 72 more per 1,000 (from 63 fewer to 244 more) | 63 (2 RCTs) | ⨁◯◯◯2,3 VERY LOW |
| Maintenance of clinical remission (CRITICAL) | 40/47 (85.1%) | 19/30 (63.3%) | RR 0.73 (0.54 to 0.97) | 236 fewer per 1,000 (from 401 fewer to 26 fewer) | 77 (1 RCT) | ⨁⨁◯◯1,2 LOW |
| CERTOLIZUMAB PEGOL COMPARED TO PLACEBO FOR MODERATE TO SEVERE FISTULIZING CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with certolizumab pegol | |||||
| Achieving fistula remission (CRITICAL) | 58/91 (63.7%) | 47/74 (63.5%) | RR 1.01 (0.80 to 1.27) | 6 more per 1,000 (from 127 fewer to 171 more) | 165 (2 RCTs) | ⨁◯◯◯2,3 VERY LOW |
| Maintenance of clinical remission (CRITICAL) | 25/30 (83.3%) | 18/28 (64.3%) | RR 0.77 (0.56 to 1.06) | 155 fewer per 1,000 (from 297 fewer to 41 more) | 58 (1 RCT) | ⨁⨁◯◯1,2 LOW |
| VEDOLIZUMAB COMPARED TO PLACEBO FOR MODERATE TO SEVERE FISTULIZING CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk of placebo | Risk with vedolizumab | |||||
| Achieving fistula remission (CRITICAL) | 16/18 (88.9%) | 28/39 (71.8%) | RR 0.81 (0.63 to 1.04) | 169 fewer per 1,000 (from 329 fewer to 36 more) | 57 (1 RCT) | ⨁◯◯◯2,4,5 VERY LOW |
| Maintenance of clinical remission (CRITICAL) | 16/18 (88.9%) | 27/39 (69.2%) | RR 0.78 (0.60 to 1.02) | 196 fewer per 1,000 (from 356 fewer to 18 more) | 57 (1 RCT) | ⨁⨁◯◯2,4 LOW |
| USTEKINUMAB COMPARED TO PLACEBO FOR MODERATE TO SEVERE FISTULIZING CROHN’S DISEASE | ||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with placebo | Risk with ustekinumab | |||||
| Achieving fistula remission (CRITICAL) | 67/77 (87.0%) | 52/70 (74.3%) | RR 0.85 (0.73 to 1.00) | 131 fewer per 1,000 (from 235 fewer to 0 fewer) | 147 (4 RCTs)a | ⨁⨁◯◯1,2 LOW |
| Maintenance of clinical remission (CRITICAL) | 6/11 (54.5%) | 3/15 (20%) | RR 0.37 (0.12 to 1.15) | 344 fewer per 1,000 (from 480 fewer to 82 more) | 26a (1 RCT) | ⨁⨁◯◯1,2 LOW |
|
GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
Rated down for imprecision since optimal information size not met (<200 events)
Rated down for risk of bias (since randomization was not stratified by presence or absence of fistula)
Rated down for very serious imprecision (wide 95% CI which could not rule out significant risk of benefit or harm with intervention)
Rated down for imprecision (95% CI crosses unity)
Rated down for indirectness (all patients received induction therapy with the biologic)
Pooled analysis of patients in 3 ustekinumab RCTs
Pooled analysis of patients in 2 ustekinumab RCTs
Adalimumab or certolizumab pegol vs. placebo, achieving and maintaining fistula remission:
In subgroup analyses of two RCTs including 77 patients with symptomatic draining fistula, adalimumab was not effective in inducing complete fistula closure (RR, 1.08; 95% CI, 0.93–1.27) within 4 weeks.48, 125 Similarly, in subgroup analysis of two RCTs including 165 patients with symptomatic draining fistula, certolizumab pegol was not effective in inducing complete fistula remission (RR, 1.01; 95% CI, 0.80–1.27).56, 126 Overall quality of evidence for both these agents was rated as very low certainty being rated down for very serious imprecision (wide 95% CI which could not rule out significant risk of benefit or harm with intervention) and risk of bias (since randomization was not stratified by presence or absence of fistula) (Table 15).
In subgroup analysis of one RCT which included 117 patients with luminal CD with response to induction dose with adalimumab, with active draining fistula at trial initiation (unclear fistula status at time of re-randomization after initial adalimumab dose), adalimumab was more effective than placebo for achieving complete fistula closure by 26 weeks (RR, 0.73; 95% CI, 0.54–0.97).47 In subgroup analysis of one RCT with 58 patients with luminal CD with response to induction dose with certolizumab pegol, with active draining fistula at trial initiation (unclear fistula status at time of re-randomization after initial certolizumab pegol dose), certolizumab pegol was numerically more effective than placebo for achieving complete fistula closure by 26 weeks (RR, 0.77; 95% CI, 0.56–1.06).126 Overall quality of evidence for both these agents was rated as low certainty being rated down for serious imprecision (low event rate) and risk of bias (since randomization was not stratified by presence or absence of fistula) (Table 15).
Vedolizumab vs. placebo, achieving and maintaining fistula remission:
In subgroup analysis of the GEMINI 2 trial including 165 patients with active CD who received induction therapy with vedolizumab with clinical response of luminal disease and had symptomatic draining fistula at baseline (unclear fistula status at time of re-randomization after initial vedolizumab dose), vedolizumab may be more effective than placebo for achieving complete fistula closure (RR, 0.81; 95% CI, 0.63–1.04) within 14 weeks.127 Of note, all patients in this trial had received initial induction therapy with vedolizumab, and those with clinical response based on CDAI were re-randomized to vedolizumab vs. placebo. Overall quality of evidence was rated as very low certainty, being rated down for risk of bias (since randomization was not stratified by presence or absence of fistula), indirectness (since all patients received induction therapy with vedolizumab) and imprecision (95% CI crossing unity). In the same trial, on extension to 52 weeks, maintenance therapy with vedolizumab may be more effective than placebo achieving fistula remission (RR, 0.78; 95% CI, 0.60–1.02). Overall quality of evidence was rated as low certainty, being rated down for risk of bias (since randomization was not stratified by presence or absence of fistula), and imprecision (95% CI crossing unity) (Table 15). In a phase 4 RCT comparing two doses of vedolizumab (standard dose vs. standard dose + additional dose at week 10) for fistulizing CD, no differences were observed in rates of fistula closure at week 30 between the two doses (7/14 vs. 5/14).128
Ustekinumab vs. placebo, achieving and maintaining fistula remission:
In a pooled analysis of 4 trials of induction therapy with ustekinumab, Sands and colleagues identified 238 patients with active draining fistula (100% perianal).129 Ustekinumab was more effective than placebo in achieving complete closure of fistula (RR, 0.85; 95% CI, 0.73–1.99). Quality of evidence was rated as low certainty, being rated down for risk of bias (since randomization was not stratified by presence or absence of fistula), and imprecision (optimal information size not met). In extension of the IM-UNITI maintenance trial in which all patients received induction therapy with ustekinumab, and responding patients were randomized to ustekinumab vs. placebo, ustekinumab was associated with a higher rate of achieving fistula remission at week 44 (RR, 0.37; 95% CI, 0.12–1.15).129 Quality of evidence was rated as low certainty, being rated down for risk of bias (since randomization was not stratified by presence or absence of fistula), and imprecision (wide 95% CI crossing unity) (Table 15).
Thiopurines vs. placebo, achieving and maintaining fistula remission:
In subgroup analysis of a single RCT including 10 patients with active draining fistula (80% perianal), azathioprine was not effective in achieving fistula healing defined as partial or complete closure by 16 weeks (RR, 1.00; 95% CI, 0.08–11.93).130 Overall quality of evidence was rated as very low certainty due to risk of bias (subgroup analysis where randomization was not stratified by presence or absence of fistula) and very serious imprecision (very wide 95% CI where significant benefit or harm with thiopurines could not be excluded). In subgroup analysis of one trial of maintenance therapy with thiopurines in which 2 patients achieved clinical remission luminally with active draining fistula. In this analysis, the 1 fistula patient who responded to active therapy failed to maintain response, while the 1 fistula patient who responded to placebo successfully maintained response. Overall quality of evidence was rated as very low certainty due to risk of bias and very serious imprecision (Table 16).
Table 16.
GRADE Evidence Profile evaluating thiopurines or antibiotics versus placebo for achieving fistula remission in patients with moderate to severe fistulizing Crohn’s disease.
| THIOPURINES COMPARED TO PLACEBO FOR MODERATE TO SEVERE FISTULIZING CROHN’S DISEASE | |||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | ||
|---|---|---|---|---|---|---|---|
| Risk with placebo | Risk with thiopurines | ||||||
| Achieving fistula remission (CRITICAL) | 1/5 (20%) | 1/5 (20%) | RR 1.00 (0.08 to 11.93) | 0 fewer per 1,000 (from 184 fewer to 1,000 more) | 10 (1 RCT) | ⨁◯◯◯1,2 VERY LOW | |
| 2 Rated down for very serious imprecision (very wide 95% CI where significant benefit or harm with thiopurines could not be excluded) | |||||||
| ANTIBIOTICS COMPARED TO PLACEBO FOR MODERATE TO SEVERE FISTULIZING CROHN’S DISEASE | |||||||
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | ||
| Risk with placebo | Risk with antibiotics | ||||||
| Induction of clinical remission (CRITICAL) | 7/8 (87.5%) | 14/17 (82.4%) | RR 0.94 (0.67 to 1.33) | 18 fewer per 1,000 (from 210 fewer to 315 more) | 35 (1 RCT) | ⨁⨁◯◯2 LOW | |
| 1 Rated down for very serious imprecision (very wide 95% CI where significant benefit or harm with thiopurines could not be excluded) | |||||||
|
GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | |||||||
No specific studies compared methotrexate vs. placebo for fistula remission. In subgroup analysis of one RCT comparing methotrexate vs. azathioprine in patients with fistulizing CD, methotrexate was slightly better than azathioprine in achieving fistula remission over 26 weeks (failure to achieve fistula remission, methotrexate vs. azathioprine: 2/6 vs. 4/6, p=0.28).
Antibiotics vs. placebo, achieving and maintaining fistula remission:
In a single 3-arm RCT, 25 patients with active draining perianal fistula were randomized to ciprofloxacin, metronidazole or placebo for 10 weeks.131 Neither ciprofloxacin, nor metronidazole was more effective than placebo in achieving complete fistula closure (RR, 0.94; 95% CI, 0.67–1.33). None of the patients randomized to metronidazole alone achieved partial or complete fistula closure. Overall quality of evidence was rated as low certainty due to very serious imprecision (very wide 95% CI where significant benefit or harm with antibiotic monotherapy could not be excluded). No trials of maintenance therapy with antibiotics were identified (Table 16).
Potential harms with interventions:
Specific side effects with all medications have been previously discussed.
Discussion:
Fistulizing or penetrating CD is a particularly severe form of CD, reported in 17–50% of patients, cause substantial morbidity, and are difficult to treat, often requiring combined medical and surgical management. Pharmacotherapies specifically for fistulizing CD have not been well-studied, and most data on efficacy is drawn from sub-group analyses from pivotal registration trials. In these trials, perianal CD are most common, with limited data on internal penetrating disease such as enteroenteric, enterovesicular and enterocutaneous fistulae. There was variability in the definition and timing of outcome assessment. For this technical review, we opted to combine all forms of fistulizing CD, and largely relied on RCTs. Surgical management of fistulizing CD was outside the scope of the guideline and technical review. Infliximab is the only biologic agent that has specifically been evaluated against placebo in patients with fistulizing disease and has the strongest body of evidence supporting its use for achieving fistula closure. For most other medications, low to very low certainty of evidence was available, primarily due to risk of bias in post-hoc subgroup analyses and sparse data.
Question 11. In adult patients with fistulizing CD (without abscess), is adding antibiotics to TNF-α antagonists superior to TNF-α antagonists alone?
Key Message:
In adults with symptomatic fistulizing CD without perianal abscess, combination of TNF-α antagonists with antibiotics is probably more effective than TNF-α antagonists alone for achieving fistula closure (moderate certainty of evidence).
Effect estimates and certainty of evidence:
In two RCTs in patients with actively draining perianal fistula, TNF-α antagonists (infliximab and adalimumab) in combination with ciprofloxacin (for 12 weeks) was significantly more effective than corresponding TNF-α antagonist alone in achieving fistula closure over 12–18 (RR, 0.42; 95% CI, 0.26–0.68).132, 133 The certainty of evidence was rated as moderate being rated down for imprecision (optimal information size not met). Even though differences were observed in the effect size in the two trials, we did not rate down for heterogeneity (Table 17).
Table 17.
GRADE Evidence Profile evaluating antibiotics combined with TNFα antagonists versus TNFα antagonists alone for achieving fistula remission in patients with moderate to severe fistulizing Crohn’s disease.
| TNFα ANTAGONISTS AND ANTIBIOTICS COMPARED TO TNFα ANTAGONISTS FOR MODERATE TO SEVERE FISTULIZING CROHN’S DISEASE | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Study event rates (95% CI) | Relative effect (95% CI) | Absolute effect* | No of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with TNFα antagonists alone | Risk with TNFα antagonists and antibiotics | |||||
| Achieving fistula remission (CRITICAL) | 31/44 (70.5%) | 13/45 (28.9%) | RR 0.42 (0.26 to 0.68) | 409 more per 1,000 (from 521 fewer to 225 fewer) | 89 (2 RCTs) | ⨁⨁⨁◯1 MODERATE |
|
GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
Rated down for imprecision (low event rate)
Potential harm of intervention:
Fluoroquinolones carry a black box warning from the FDA for disabling and potentially irreversible serious adverse reactions including risk of tendinitis and tendon rupture, peripheral neuropathy and central nervous system effects.
Discussion:
Bacteria play a part in fistula development in patients with CD. Hence, adding antibiotics may improve fistula healing by controlling microflora present in the fistula tract. While current trials suggest a short-term benefit with adding ciprofloxacin for 12 weeks to TNFα antagonists, on extension to 24 weeks (after stopping ciprofloxacin at week 12), Dewint and colleagues observed that three patients randomized to the combination treatment group lost response with fistula recurrence, whereas the number of patients in the adalimumab monotherapy group who had reached the primary endpoint at week 12 remained stable at week 24. This might the need for long-term ciprofloxacin beyond 12 weeks to maintain fistula remission.
EVIDENCE-TO-DECISION FRAMEWORK
Patients’ Values and Preferences of CD Therapy
Most patients with CD are benefit-driven, preferring the use of therapies with the highest likelihood of maintaining remission; a smaller group of patients are more risk averse, wishing to minimize potential toxicities, including infection and cancer, even at the expense of reduced likelihood of maintaining remission of CD. In an online patient-preference survey of 812 patients with CD, latent class analysis demonstrated 3 distinct groups of survey responders whose choices were strongly influenced by avoidance of active symptoms (61%), avoidance of corticosteroid use (25%), or avoidance of risks of cancer, infection or surgery (14%) when choosing a therapy.134 Class membership was correlated with age, sex, mean short CD activity index score and corticosteroid avoidance. Hazlewood and colleagues similarly observed that in a cohort of 155 patients with CD, 55% patients were prioritized treatment benefits, 21% prioritized corticosteroid avoidance and 20% placed higher importance on avoiding treatments with a risk of cancer or infection.135 In a discrete choice experiment study of 202 patients with IBD (77 patients with CD), Bewtra and colleagues observed that to delay relapse by 5 years, patients were willing to accept up to a 28% chance of having a serious infection and 1.8% chance of having a lymphoma.136 These maximal acceptable risk rates were lower in patients with CD than ulcerative colitis. These rates vary depending on disease state – patients with active disease are willing to accept comparatively less risk than patients with no active symptoms to achieve a given improvement in time to relapse. For example, to delay a relapse for 1.5 years, patients currently in remission would be willing to accept a 15.6% risk of infection and 1.1% risk of lymphoma, whereas patients currently experiencing symptoms were willing to accept only 8.5% risk of infection and 0.5% risk of lymphoma. Recognizing the heterogeneity of patient preferences among those suffering from CD, physicians ought to engage patients in shared decision-making with adequate contextualization of risks and benefits, and tailor treatment options based on patient preference.
Cost-effectiveness
Though several cost-effectiveness analyses have been performed, they have shown conflicting findings due in part to differences in cost of therapies in diverse healthcare systems globally. In most analyses, infliximab or adalimumab dominated other biologic agents; however, none of the agents met conventional cost-effectiveness thresholds.137
Equity
A recent review on the effects of race and ethnicity on the management of IBD patients highlights issues around access to care, insurance coverage, and use of medical therapies, specifically biologic agents.138 While some studies demonstrated that African Americans, Asians, or Hispanic patients with CD were less likely to receive biologics compared with Whites, other studies have shown no differences in the use of immunomodulators of TNFα antagonists among patients of different races of ethnicities.139–141 The is evidence of differences in insurance coverage, however, with African Americans and Hispanic populations less likely to have commercial insurance and more likely to have Medicaid or be uninsured.142, 143
KNOWLEDGE GAPS AND FUTURE DIRECTIONS
While several significant advancements have been made in the treatment of patients with moderate to severe luminal and fistulizing CD, this technical review identified some key knowledge gaps which merit further evaluation to inform clinical guidelines and practice.
Risk stratification and shared decision-making: Several prognostic factors have been identified that predict higher risk of surgery and disease complications in patients with CD.24 There is considerable heterogeneity within CD, based on disease location, behavior and early course and presentation. However, there is a paucity of risk prediction models, based on clinical, biochemical, serological, genetic and other factors that can accurately stratify patients in terms of their short- and long-term disease-related risks and disability. This results in frequent over- and under-treatment of patients at low- and high-risk of disease complications, respectively, and delay in appropriate care. Developing such models may allow implementation of risk-congruent treatment strategies and appropriate utilization of expensive therapies. Similarly, risk-stratification strategies to identify patients at high risk of developing treatment-related complications are limited. Validated risk prediction models to accurately identify patients at high risk of disease- vs. treatment-related complications, and how different treatments modify these risks, is vital to know and communicate effectively to patients. Pairing this information with patients’ values and preferences would facilitate shared decision-making, as the treatment landscape rapidly evolves in this field.
Personalization and positioning of therapies: With increasing availability of different biologic agents, and promising targeted immunosuppressive agents in development, for treating outpatients with moderate-severe CD, there is clearly a need for identifying biomarkers predictive of response to individual therapies, to facilitate optimal choice of therapies. While awaiting biomarkers, validated clinical prediction models may be helpful, if sufficiently discriminatory to help identify patients who have a low vs. high probability of response to specific therapies. Ongoing research efforts using multi-omic platforms using serum, stool and tissue specimens have potential to inform biomarkers predictive of response to specific therapies. Once these are available, clinical trials or prospective comparative effectiveness studies using integrated clinical-, pharmacokinetic- and biomarker-based treatment positioning strategies vs. usual care could provide guidance on appropriate management strategies.
Management of CD in special populations: With rising incidence and prevalence of CD in older patients, evidence-based treatment strategies for this population are much needed.144 Management of these patients warrants careful consideration of the risks of disease-related vs. treatment-related complications and extra-intestinal complications (e.g., cardiovascular disease, malignancy, etc.), in the context of patients’ values and preferences, functional status and comorbidities. Similarly, racioethnic minorities including African Americans and Hispanics, immigrants, etc. have traditionally been under-represented in clinical trials.138 Prior studies have demonstrated lower utilization of advanced medical and surgical therapies, inferior healthcare access, lower adherence to therapy and inferior IBD-related outcomes in these patients. Hence, a more comprehensive understanding of disease burden, course and treatment effectiveness and access is warranted in these patients.
Treatment targets in CD: While it is well known that there may be significant discrepancy in symptoms and endoscopic findings in patients with CD, particularly small bowel CD, until recently, clinical trials have often not routinely incorporated endoscopic evaluation in assessing efficacy of therapy. While treating to a target of symptomatic remission has been shown to decrease risk of disease complications, it remains to be seen whether routinely treating to a target of endoscopic remission, even in asymptomatic patients, offers substantial additional benefit.145 Such an approach, while suggested in expert consensus statements, can challenging for several reasons, including the need for frequent biochemical and/or endoscopic monitoring and switching empirically between therapies in the absence of predictive biomarkers of response to specific agents. Such empiric switching may inadvertently result in transitioning to a less effective therapy, potentially increasing the risk of disease flare and causing harm. Such an approach would require a careful assessment of the anticipated magnitude of benefit in downstream consequences (decreasing surgery, healthcare utilization) vs. risks and costs, with treating to different treatment targets. Different therapies have different rates of achieving different targets, often incrementally more difficult from clinical and biochemical, to endoscopic, to histologic remission, and may result different intensity of therapies with associated risks and costs.
Novel therapies: Even the most effective pharmacological therapies for patients with moderate-severe CD are effective in achieving clinical remission in 40–50% of patients, with frequent loss of response. Novel agents with targeting different aspects of the inflammatory pathways, novel combinations to optimize response to existing therapies, as well as novel dietary and microbiota-directed therapies are warranted to improve outcomes of patients with CD.
Management of fistulizing CD: As noted above, fistulizing CD is a particularly severe form of CD with substantial morbidity, yet there is little evidence to inform optimal treatment approach. While medical and surgical co-management is often required, optimal management strategies need to be defined. Local injection of mesenchymal stem cells in fistula tracts appears promising.146
Supplementary Material
{kind=link}
{kind=link}
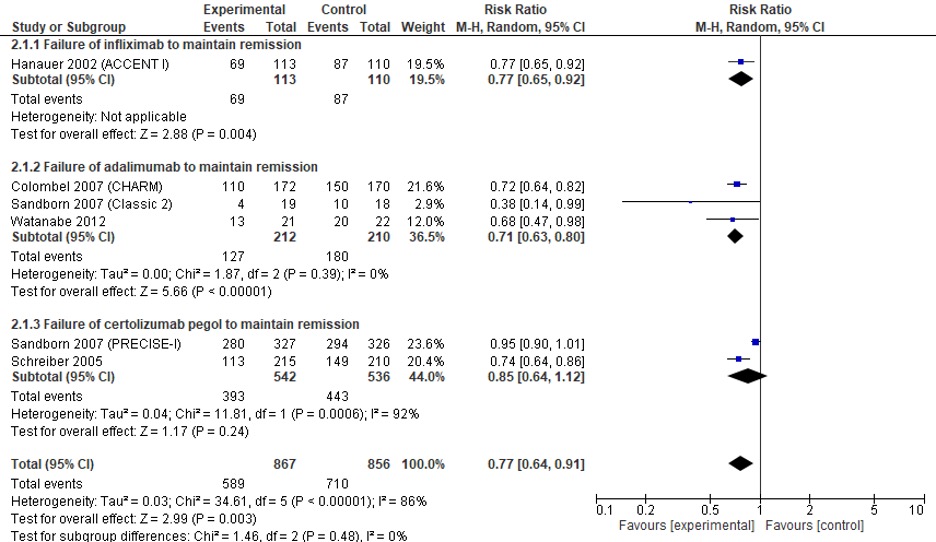{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
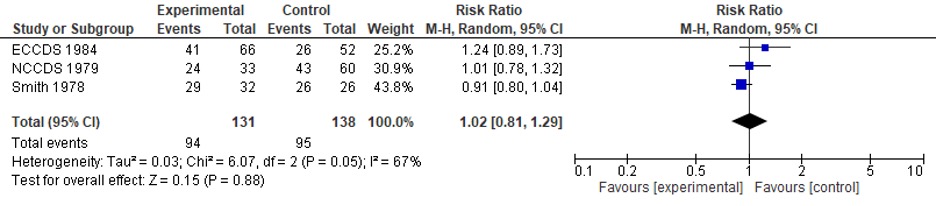{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgements:
The authors sincerely thank Ms. Kellee Kaulback, Medical Information Officer, Health Quality Ontario, for helping in the literature search for this technical review.
Disclosures:
Siddharth Singh: Supported by NIH/NIDDK K23DK117058; research grants from AbbVie and Janssen.
Deborah Proctor - PI for multi-center studies with AbbVie, Celgene, Bristol-Myers Squibb and Parexel
Frank I. Scott: Research grants from Takeda Pharmaceuticals USA, Janssen Pharmaceuticals, the NIH, and the Crohn’s and Colitis Foundation. He has received personal fees from PRIME Incorporated, Janssen Pharmaceuticals, Takeda Pharmaceuticals, and Merck Pharmaceuticals.
Yngve Falck-Ytter: None
Joseph Feuerstein: None
REFERENCES
- 1.Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet 2018;390:2769–2778. [DOI] [PubMed] [Google Scholar]
- 2.Peyrin-Biroulet L, Loftus EV, Colombel JF, et al. The natural history of adult crohn’s disease in population-based cohorts. American Journal of Gastroenterology 2010;105:289–297. [DOI] [PubMed] [Google Scholar]
- 3.Frolkis AD, Dykeman J, Negron ME, et al. Risk of surgery for inflammatory bowel diseases has decreased over time: a systematic review and meta-analysis of population-based studies. Gastroenterology 2013;145:996–1006. [DOI] [PubMed] [Google Scholar]
- 4.Burr NE, Lord R, Hull MA, et al. Decreasing Risk of First and Subsequent Surgeries in Patients With Crohn’s Disease in England From 1994 through 2013. Clin Gastroenterol Hepatol 2019;17:2042–2049 e4. [DOI] [PubMed] [Google Scholar]
- 5.Burisch J, Kiudelis G, Kupcinskas L, et al. Natural disease course of Crohn’s disease during the first 5 years after diagnosis in a European population-based inception cohort: an Epi-IBD study. Gut 2019;68:423–433. [DOI] [PubMed] [Google Scholar]
- 6.Jeuring SF, van den Heuvel TR, Liu LY, et al. Improvements in the Long-Term Outcome of Crohn’s Disease Over the Past Two Decades and the Relation to Changes in Medical Management: Results from the Population-Based IBDSL Cohort. Am J Gastroenterol 2017;112:325–336. [DOI] [PubMed] [Google Scholar]
- 7.Siegel CA, Bernstein CN. Identifying Patients With Inflammatory Bowel Diseases at High vs Low Risk of Complications. Clin Gastroenterol Hepatol 2020;18:1261–1267. [DOI] [PubMed] [Google Scholar]
- 8.Ananthakrishnan AN, Kwon J, Raffals L, et al. Variation in treatment of patients with inflammatory bowel diseases at major referral centers in the United States. Clin Gastroenterol Hepatol 2015;13:1197–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Weaver KN, Kappelman MD, Sandler RS, et al. Variation in Care of Inflammatory Bowel Diseases Patients in Crohn’s and Colitis Foundation of America Partners: Role of Gastroenterologist Practice Setting in Disease Outcomes and Quality Process Measures. Inflamm Bowel Dis 2016;22:2672–2677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Terdiman JP, Gruss CB, Heidelbaugh JJ, et al. American Gastroenterological Association Institute guideline on the use of thiopurines, methotrexate, and anti-TNF-alpha biologic drugs for the induction and maintenance of remission in inflammatory Crohn’s disease. Gastroenterology 2013;145:1459–63. [DOI] [PubMed] [Google Scholar]
- 11.Vande Casteele N, Herfarth H, Katz J, et al. American Gastroenterological Association Institute Technical Review on the Role of Therapeutic Drug Monitoring in the Management of Inflammatory Bowel Diseases. Gastroenterology 2017;153:835–857.e6. [DOI] [PubMed] [Google Scholar]
- 12.Feuerstein JD, Nguyen GC, Kupfer SS, et al. American Gastroenterological Association Institute Guideline on Therapeutic Drug Monitoring in Inflammatory Bowel Disease. Gastroenterology 2017;153:827–834. [DOI] [PubMed] [Google Scholar]
- 13.Casellas F, Herrera-de Guise C, Robles V, et al. Patient preferences for inflammatory bowel disease treatment objectives. Dig Liver Dis 2017;49:152–156. [DOI] [PubMed] [Google Scholar]
- 14.Best WR, Becktel JM, Singleton JW, et al. Development of a Crohn’s disease activity index. National Cooperative Crohn’s Disease Study. Gastroenterology 1976;70:439–44. [PubMed] [Google Scholar]
- 15.Jairath V, Zou G, Parker CE, et al. Systematic review with meta-analysis: placebo rates in induction and maintenance trials of Crohn’s disease. Alimentary Pharmacology and Therapeutics 2017;45:1021–1042. [DOI] [PubMed] [Google Scholar]
- 16.DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177–88. [DOI] [PubMed] [Google Scholar]
- 17.Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ 2003;327:557–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lin L, Chu H. Quantifying publication bias in meta-analysis. Biometrics 2018;74:785–794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Singh S, Fumery M, Sandborn WJ, et al. Systematic review and network meta-analysis: first- and second-line biologic therapies for moderate-severe Crohn’s disease. Aliment Pharmacol Ther 2018;48:394–409. [DOI] [PubMed] [Google Scholar]
- 20.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017;358:j4008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol 2011;64:401–6. [DOI] [PubMed] [Google Scholar]
- 22.Brignardello-Petersen R, Bonner A, Alexander PE, et al. Advances in the GRADE approach to rate the certainty in estimates from a network meta-analysis. J Clin Epidemiol 2018;93:36–44. [DOI] [PubMed] [Google Scholar]
- 23.Alonso-Coello P, Oxman AD, Moberg J, et al. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ 2016;353:i2089. [DOI] [PubMed] [Google Scholar]
- 24.Siegel CA, Whitman CB, Spiegel BMR, et al. Development of an index to define overall disease severity in IBD. Gut 2018;67:244–254. [DOI] [PubMed] [Google Scholar]
- 25.Beaugerie L, Kirchgesner J. Balancing Benefit vs Risk of Immunosuppressive Therapy for Individual Patients With Inflammatory Bowel Diseases. Clin Gastroenterol Hepatol 2019;17:370–379. [DOI] [PubMed] [Google Scholar]
- 26.Beaugerie L, Rahier JF, Kirchgesner J. Predicting, Preventing, and Managing Treatment-Related Complications in Patients With Inflammatory Bowel Diseases. Clin Gastroenterol Hepatol 2020;18:1324–1335 e2. [DOI] [PubMed] [Google Scholar]
- 27.Lichtenstein GR, Feagan BG, Cohen RD, et al. Serious infection and mortality in patients with Crohn’s disease: more than 5 years of follow-up in the TREAT registry. Am J Gastroenterol 2012;107:1409–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.D’Haens G, Reinisch W, Panaccione R, et al. Lymphoma Risk and Overall Safety Profile of Adalimumab in Patients With Crohn’s Disease With up to 6 Years of Follow-Up in the Pyramid Registry. Am J Gastroenterol 2018;113:872–882. [DOI] [PubMed] [Google Scholar]
- 29.Kirchgesner J, Lemaitre M, Carrat F, et al. Risk of Serious and Opportunistic Infections Associated With Treatment of Inflammatory Bowel Diseases. Gastroenterology 2018;155:337–346 e10. [DOI] [PubMed] [Google Scholar]
- 30.Nyboe Andersen N, Pasternak B, Friis-Moller N, et al. Association between tumour necrosis factor-alpha inhibitors and risk of serious infections in people with inflammatory bowel disease: nationwide Danish cohort study. BMJ 2015;350:h2809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Singh S, Facciorusso A, Dulai PS, et al. Comparative Risk of Serious Infections With Biologic and/or Immunosuppressive Therapy in Patients With Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. Clin Gastroenterol Hepatol 2020;18:69–81 e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lewis JD, Scott FI, Brensinger CM, et al. Increased Mortality Rates With Prolonged Corticosteroid Therapy When Compared With Antitumor Necrosis Factor-alpha-Directed Therapy for Inflammatory Bowel Disease. Am J Gastroenterol 2018;113:405–417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Loftus EV Jr., Feagan BG, Panaccione R, et al. Long-term safety of vedolizumab for inflammatory bowel disease. Aliment Pharmacol Ther 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Sandborn WJ, Feagan BG, Danese S, et al. Safety of Ustekinumab in Inflammatory Bowel Disease: Pooled Safety Analysis of Results from Phase 2/3 Studies. Inflamm Bowel Dis 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kotlyar DS, Lewis JD, Beaugerie L, et al. Risk of lymphoma in patients with inflammatory bowel disease treated with azathioprine and 6-mercaptopurine: a meta-analysis. Clinical Gastroenterology & Hepatology 2015;13:847–58.e4; quiz e48–50. [DOI] [PubMed] [Google Scholar]
- 36.Ariyaratnam J, Subramanian V. Association between thiopurine use and nonmelanoma skin cancers in patients with inflammatory bowel disease: a meta-analysis. Am J Gastroenterol 2014;109:163–9. [DOI] [PubMed] [Google Scholar]
- 37.Sepriano A, Kerschbaumer A, Smolen JS, et al. Safety of synthetic and biological DMARDs: a systematic literature review informing the 2019 update of the EULAR recommendations for the management of rheumatoid arthritis. Ann Rheum Dis 2020;79:760–770. [DOI] [PubMed] [Google Scholar]
- 38.Nyboe Andersen N, Pasternak B, Basit S, et al. Association between tumor necrosis factor-alpha antagonists and risk of cancer in patients with inflammatory bowel disease. JAMA 2014;311:2406–13. [DOI] [PubMed] [Google Scholar]
- 39.Muller M, D’Amico F, Bonovas S, et al. TNF inhibitors and risk of malignancy in patients with inflammatory bowel diseases: a systematic review. J Crohns Colitis 2020. [DOI] [PubMed] [Google Scholar]
- 40.Lemaitre M, Kirchgesner J, Rudnichi A, et al. Association Between Use of Thiopurines or Tumor Necrosis Factor Antagonists Alone or in Combination and Risk of Lymphoma in Patients With Inflammatory Bowel Disease. JAMA 2017;318:1679–1686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Chupin A, Perduca V, Meyer A, et al. Systematic review with meta-analysis: comparative risk of lymphoma with anti-tumour necrosis factor agents and/or thiopurines in patients with inflammatory bowel disease. Aliment Pharmacol Ther 2020. [DOI] [PubMed] [Google Scholar]
- 42.Osterman MT, Sandborn WJ, Colombel JF, et al. Increased risk of malignancy with adalimumab combination therapy, compared with monotherapy, for Crohn’s disease. Gastroenterology 2014;146:941–9. [DOI] [PubMed] [Google Scholar]
- 43.Bonovas S, Fiorino G, Allocca M, et al. Biologic Therapies and Risk of Infection and Malignancy in Patients With Inflammatory Bowel Disease: A Systematic Review and Network Meta-analysis. Clin Gastroenterol Hepatol 2016;14:1385–1397 e10. [DOI] [PubMed] [Google Scholar]
- 44.Targan SR, Hanauer SB, van Deventer SJ, et al. A short-term study of chimeric monoclonal antibody cA2 to tumor necrosis factor alpha for Crohn’s disease. Crohn’s Disease cA2 Study Group. New England Journal of Medicine 1997;337:1029–35. [DOI] [PubMed] [Google Scholar]
- 45.Lemann M, Mary JY, Duclos B, et al. Infliximab plus azathioprine for steroid-dependent Crohn’s disease patients: a randomized placebo-controlled trial. Gastroenterology 2006;130:1054–61. [DOI] [PubMed] [Google Scholar]
- 46.Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenance infliximab for Crohn’s disease: The ACCENT I randomised trial. Lancet 2002;359:1541–1549. [DOI] [PubMed] [Google Scholar]
- 47.Hanauer SB, Sandborn WJ, Rutgeerts P, et al. Human anti-tumor necrosis factor monoclonal antibody (adalimumab) in Crohn’s disease: the CLASSIC-I trial. Gastroenterology 2006;130:323–33; quiz 591. [DOI] [PubMed] [Google Scholar]
- 48.Sandborn W, Rutgeerts P, Enns R, et al. Adalimumab induction therapy for Crohn disease previously treated with infliximab: a randomized trial. Annals of internal medicine. Volume 146, 2007:829–839. [DOI] [PubMed] [Google Scholar]
- 49.Watanabe M, Hibi T, Lomax K, et al. Adalimumab for the induction and maintenance of clinical remission in Japanese patients with Crohn’s disease. Journal of crohn’s & colitis. Volume 6, 2012:160–173. [DOI] [PubMed] [Google Scholar]
- 50.Reinisch W, Sandborn WJ, Hommes DW, et al. Adalimumab for induction of clinical remission in moderately to severely active ulcerative colitis: results of a randomised controlled trial. Gut 2011;60:780–7. [DOI] [PubMed] [Google Scholar]
- 51.Sandborn WJ, Van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients with moderate-to-severe ulcerative colitis. Gastroenterology 2012;142:257–265.e3. [DOI] [PubMed] [Google Scholar]
- 52.Suzuki Y, Motoya S, Hanai H, et al. Efficacy and safety of adalimumab in Japanese patients with moderately to severely active ulcerative colitis. Journal of gastroenterology. Volume 49, 2014:283–294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Hanauer S, Sandborn W, Rutgeerts P, et al. Human anti-tumor necrosis factor monoclonal antibody (adalimumab) in Crohn’s disease: the CLASSIC-I trial. Gastroenterology. Volume 130, 2006:323–333. [DOI] [PubMed] [Google Scholar]
- 54.Sandborn W, Hanauer S, Rutgeerts P, et al. Adalimumab for maintenance treatment of Crohn’s disease: results of the CLASSIC II trial. Gut. Volume 56, 2007:1232–1239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Colombel JF, Sandborn WJ, Rutgeerts P, et al. Adalimumab for maintenance of clinical response and remission in patients with Crohn’s disease: the CHARM trial. Gastroenterology 2007;132:52–65. [DOI] [PubMed] [Google Scholar]
- 56.Sandborn W, Feagan B, Stoinov S, et al. Certolizumab pegol for the treatment of Crohn’s disease. New England journal of medicine. Volume 357, 2007:228–238. [DOI] [PubMed] [Google Scholar]
- 57.Sandborn W, Schreiber S, Feagan B, et al. Certolizumab pegol for active Crohn’s disease: a placebo-controlled, randomized trial. Clinical gastroenterology and hepatology. Volume 9, 2011:670–678.e3. [DOI] [PubMed] [Google Scholar]
- 58.Schreiber S, Rutgeerts P, Fedorak RN, et al. A randomized, placebo-controlled trial of certolizumab pegol (CDP870) for treatment of crohn’s disease. Gastroenterology 2005;129:807–818. [DOI] [PubMed] [Google Scholar]
- 59.Schreiber S, Khaliq-Kareemi M, Lawrance IC, et al. Maintenance therapy with certolizumab pegol for Crohn’s disease. New England Journal of Medicine 2007;357:239–250. [DOI] [PubMed] [Google Scholar]
- 60.Sandborn W, Feagan B, Rutgeerts P, et al. Vedolizumab as induction and maintenance therapy for Crohn’s disease. New England journal of medicine. Volume 369, 2013:711–721. [DOI] [PubMed] [Google Scholar]
- 61.Sands BE, Feagan BG, Rutgeerts P, et al. Effects of vedolizumab induction therapy for patients with Crohn’s disease in whom tumor necrosis factor antagonist treatment failed. Gastroenterology 2014;147:618–627.e3. [DOI] [PubMed] [Google Scholar]
- 62.Feagan B, Sandborn W, Gasink C, et al. Ustekinumab as Induction and Maintenance Therapy for Crohn’s Disease. New England journal of medicine. Volume 375, 2016:1946–1960. [DOI] [PubMed] [Google Scholar]
- 63.Sandborn WJ, Gasink C, Gao LL, et al. Ustekinumab induction and maintenance therapy in refractory Crohn’s disease. N Engl J Med 2012;367:1519–28. [DOI] [PubMed] [Google Scholar]
- 64.Sandborn WJ, Colombel JF, Enns R, et al. Natalizumab induction and maintenance therapy for Crohn’s disease. New England Journal of Medicine 2005;353:1912–1925. [DOI] [PubMed] [Google Scholar]
- 65.Targan S, Feagan B, Fedorak R, et al. Natalizumab for the treatment of active Crohn’s disease: results of the ENCORE Trial. Gastroenterology. Volume 132, 2007:1672–1683. [DOI] [PubMed] [Google Scholar]
- 66.Brew BJ, Davies NW, Cinque P, et al. Progressive multifocal leukoencephalopathy and other forms of JC virus disease. Nat Rev Neurol 2010;6:667–79. [DOI] [PubMed] [Google Scholar]
- 67.Bloomgren G, Richman S, Hotermans C, et al. Risk of natalizumab-associated progressive multifocal leukoencephalopathy. N Engl J Med 2012;366:1870–80. [DOI] [PubMed] [Google Scholar]
- 68.Paz SPC, Branco L, Pereira MAC, et al. Systematic review of the published data on the worldwide prevalence of John Cunningham virus in patients with multiple sclerosis and neuromyelitis optica. Epidemiol Health 2018;40:e2018001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Duricova D, Pedersen N, Elkjaer M, et al. Overall and cause-specific mortality in Crohn’s disease: a meta-analysis of population-based studies. Inflamm Bowel Dis 2010;16:347–53. [DOI] [PubMed] [Google Scholar]
- 70.Singh S, Andersen NN, Andersson M, et al. Comparison of infliximab with adalimumab in 827 biologic-naive patients with Crohn’s disease: a population-based Danish cohort study. Aliment Pharmacol Ther 2018;47:596–604. [DOI] [PubMed] [Google Scholar]
- 71.Singh S, Heien HC, Sangaralingham LR, et al. Comparative Effectiveness and Safety of Anti-Tumor Necrosis Factor Agents in Biologic-Naive Patients With Crohn’s Disease. Clin Gastroenterol Hepatol 2016;14:1120–1129 e6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Singh S, George J, Boland BS, et al. Primary Non-Response to Tumor Necrosis Factor Antagonists is Associated with Inferior Response to Second-line Biologics in Patients with Inflammatory Bowel Diseases: A Systematic Review and Meta-analysis. Journal of Crohn’s & colitis 2018;12:635–643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Alric H, Amiot A, Kirchgesner J, et al. The effectiveness of either ustekinumab or vedolizumab in 239 patients with Crohn’s disease refractory to anti-tumour necrosis factor. Aliment Pharmacol Ther 2020;51:948–957. [DOI] [PubMed] [Google Scholar]
- 74.Townsend T, Razanskaite V, Dodd S, et al. Comparative effectiveness of ustekinumab or vedolizumab after one year in 130 patients with anti-TNF-refractory Crohn’s disease. Aliment Pharmacol Ther 2020;52:1341–1352. [DOI] [PubMed] [Google Scholar]
- 75.Biemans VBC, van der Woude CJ, Dijkstra G, et al. Ustekinumab is associated with superior effectiveness outcomes compared to vedolizumab in Crohn’s disease patients with prior failure to anti-TNF treatment. Aliment Pharmacol Ther 2020;52:123–134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Holmer A, Singh S. Overall and comparative safety of biologic and immunosuppressive therapy in inflammatory bowel diseases. Expert Rev Clin Immunol 2019;15:969–979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Dassopoulos T, Sultan S, Falck-Ytter YT, et al. American Gastroenterological Association Institute technical review on the use of thiopurines, methotrexate, and anti-TNF-alpha biologic drugs for the induction and maintenance of remission in inflammatory Crohn’s disease. Gastroenterology 2013;145:1464-78.e1-5. [DOI] [PubMed] [Google Scholar]
- 78.Panés J, López-Sanromán A, Bermejo F, et al. Early azathioprine therapy is no more effective than placebo for newly diagnosed Crohn’s disease. Gastroenterology. Volume 145, 2013:766–774. [DOI] [PubMed] [Google Scholar]
- 79.Cosnes J, Bourrier A, Laharie D, et al. Early administration of azathioprine vs conventional management of Crohn’s Disease: a randomized controlled trial. Gastroenterology. Volume 145, 2013:758–65.e2; quiz e14-5. [DOI] [PubMed] [Google Scholar]
- 80.Feagan BG, Rochon J, Fedorak RN, et al. Methotrexate for the treatment of Crohn’s disease. The North American Crohn’s Study Group Investigators. New England Journal of Medicine 1995;332:292–7. [DOI] [PubMed] [Google Scholar]
- 81.Feagan BG, Fedorak RN, Irvine EJ, et al. A comparison of methotrexate with placebo for the maintenance of remission in Crohn’s disease. New England Journal of Medicine 2000;342:1627–1632. [DOI] [PubMed] [Google Scholar]
- 82.Oren R, Moshkowitz M, Odes S, et al. Methotrexate in chronic active Crohn’s disease: A double-blind, randomized, Israeli multicenter trial. American Journal of Gastroenterology 1997;92:2203–2209. [PubMed] [Google Scholar]
- 83.Chatu S, Subramanian V, Saxena S, et al. The role of thiopurines in reducing the need for surgical resection in Crohn’s disease: a systematic review and meta-analysis. Am J Gastroenterol 2014;109:23–34; quiz 35. [DOI] [PubMed] [Google Scholar]
- 84.Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, azathioprine, or combination therapy for Crohn’s disease. New England Journal of Medicine 2010;362:1383–1395. [DOI] [PubMed] [Google Scholar]
- 85.Hazlewood GS, Rezaie A, Borman M, et al. Comparative effectiveness of immunosuppressants and biologics for inducing and maintaining remission in Crohn’s disease: a network meta-analysis. Gastroenterology 2015;148:344–54.e5; quiz e14-5. [DOI] [PubMed] [Google Scholar]
- 86.Singh S, Garg SK, Pardi DS, et al. Comparative efficacy of pharmacologic interventions in preventing relapse of Crohn’s disease after surgery: a systematic review and network meta-analysis. Gastroenterology 2015;148:64–76.e2; quiz e14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Feagan BG, McDonald JW, Panaccione R, et al. Methotrexate in combination with infliximab is no more effective than infliximab alone in patients with Crohn’s disease. Gastroenterology 2014;146:681–688.e1. [DOI] [PubMed] [Google Scholar]
- 88.Targownik LE, Benchimol EI, Bernstein CN, et al. Combined Biologic and Immunomodulatory Therapy is Superior to Monotherapy for Decreasing the Risk of Inflammatory Bowel Disease-Related Complications. J Crohns Colitis 2020;14:1354–1363. [DOI] [PubMed] [Google Scholar]
- 89.Targownik LE, Benchimol EI, Bernstein CN, et al. Upfront Combination Therapy, Compared With Monotherapy, for Patients Not Previously Treated With a Biologic Agent Associates With Reduced Risk of Inflammatory Bowel Disease-related Complications in a Population-based Cohort Study. Clin Gastroenterol Hepatol 2019;17:1788–1798 e2. [DOI] [PubMed] [Google Scholar]
- 90.Matsumoto T, Motoya S, Watanabe K, et al. Adalimumab Monotherapy and a Combination with Azathioprine for Crohn’s Disease: a Prospective, Randomized Trial. Journal of crohn’s & colitis. Volume 10, 2016:1259–1266. [DOI] [PubMed] [Google Scholar]
- 91.Yzet C, Diouf M, Singh S, et al. No Benefit of Concomitant Immunomodulator Therapy on Efficacy of Biologics That Are Not Tumor Necrosis Factor Antagonists in Patients With Inflammatory Bowel Diseases: A Meta-Analysis. Clin Gastroenterol Hepatol 2020. [DOI] [PubMed] [Google Scholar]
- 92.Vermeire S, Gils A, Accossato P, et al. Immunogenicity of biologics in inflammatory bowel disease. Therap Adv Gastroenterol 2018;11:1756283X17750355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Roblin X, Williet N, Boschetti G, et al. Addition of azathioprine to the switch of anti-TNF in patients with IBD in clinical relapse with undetectable anti-TNF trough levels and antidrug antibodies: a prospective randomised trial. Gut 2020;69:1206–1212. [DOI] [PubMed] [Google Scholar]
- 94.Roblin X, Boschetti G, Williet N, et al. Azathioprine dose reduction in inflammatory bowel disease patients on combination therapy: an open-label, prospective and randomised clinical trial. Aliment Pharmacol Ther 2017;46:142–149. [DOI] [PubMed] [Google Scholar]
- 95.Van Assche G, Magdelaine-Beuzelin C, D’Haens G, et al. Withdrawal of immunosuppression in Crohn’s disease treated with scheduled infliximab maintenance: a randomized trial. Gastroenterology 2008;134:1861–8. [DOI] [PubMed] [Google Scholar]
- 96.Hisamatsu T, Kato S, Kunisaki R, et al. Withdrawal of thiopurines in Crohn’s disease treated with scheduled adalimumab maintenance: a prospective randomised clinical trial (DIAMOND2). J Gastroenterol 2019;54:860–870. [DOI] [PubMed] [Google Scholar]
- 97.Louis E, Mary JY, Vernier-Massouille G, et al. Maintenance of remission among patients with Crohn’s disease on antimetabolite therapy after infliximab therapy is stopped. Gastroenterology 2012;142:63–70 e5; quiz e31. [DOI] [PubMed] [Google Scholar]
- 98.Reenaers C, Mary JY, Nachury M, et al. Outcomes 7 Years After Infliximab Withdrawal for Patients With Crohn’s Disease in Sustained Remission. Clin Gastroenterol Hepatol 2018;16:234–243 e2. [DOI] [PubMed] [Google Scholar]
- 99.Khan N, Abbas AM, Lichtenstein GR, et al. Risk of lymphoma in patients with ulcerative colitis treated with thiopurines: a nationwide retrospective cohort study. Gastroenterology 2013;145:1007–1015 e3. [DOI] [PubMed] [Google Scholar]
- 100.Torres J, Boyapati RK, Kennedy NA, et al. Systematic Review of Effects of Withdrawal of Immunomodulators or Biologic Agents From Patients With Inflammatory Bowel Disease. Gastroenterology 2015;149:1716–30. [DOI] [PubMed] [Google Scholar]
- 101.D’Haens G, Baert F, van AG, et al. Early combined immunosuppression or conventional management in patients with newly diagnosed Crohn’s disease: an open randomised trial. Lancet (london, england). Volume 371, 2008:660–667. [DOI] [PubMed] [Google Scholar]
- 102.Hoekman DR, Stibbe JA, Baert FJ, et al. Long-term Outcome of Early Combined Immunosuppression Versus Conventional Management in Newly Diagnosed Crohn’s Disease. J Crohns Colitis 2018;12:517–524. [DOI] [PubMed] [Google Scholar]
- 103.Khanna R, Bressler B, Levesque B, et al. Early combined immunosuppression for the management of Crohn’s disease (REACT): a cluster randomised controlled trial. Lancet (london, england). Volume 386, 2015:1825–1834. [DOI] [PubMed] [Google Scholar]
- 104.Greenberg GR, Feagan BG, Martin F, et al. Oral budesonide for active Crohn’s disease. Canadian Inflammatory Bowel Disease Study Group. New England Journal of Medicine 1994;331:836–41. [DOI] [PubMed] [Google Scholar]
- 105.Tremaine WJ, Hanauer SB, Katz S, et al. Budesonide CIR capsules (once or twice daily divided-dose) in active Crohn’s disease: A randomized placebo-controlled study in the United States. American Journal of Gastroenterology 2002;97:1748–1754. [DOI] [PubMed] [Google Scholar]
- 106.Suzuki Y, Motoya S, Takazoe M, et al. Efficacy and tolerability of oral budesonide in Japanese patients with active Crohn’s disease: a multicentre, double-blind, randomized, parallel-group Phase II study. Journal of Crohn’s & colitis 2013;7:239–47. [DOI] [PubMed] [Google Scholar]
- 107.Greenberg GR, Feagan BG, Martin F, et al. Oral budesonide as maintenance treatment for Crohn’s disease: a placebo-controlled, dose-ranging study. Canadian Inflammatory Bowel Disease Study Group. Gastroenterology 1996;110:45–51. [DOI] [PubMed] [Google Scholar]
- 108.Ferguson A, Campieri M, Doe W, et al. Oral budesonide as maintenance therapy in Crohn’s disease--results of a 12-month study. Global Budesonide Study Group. Alimentary Pharmacology & Therapeutics 1998;12:175–83. [DOI] [PubMed] [Google Scholar]
- 109.Lofberg R, Rutgeerts P, Malchow H, et al. Budesonide prolongs time to relapse in ileal and ileocaecal Crohn’s disease. A placebo controlled one year study. Gut 1996;39:82–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Hanauer S, Sandborn WJ, Persson A, et al. Budesonide as maintenance treatment in Crohn’s disease: a placebo-controlled trial. Alimentary Pharmacology & Therapeutics 2005;21:363–71. [DOI] [PubMed] [Google Scholar]
- 111.Malchow H, Ewe K, Brandes J, et al. European Cooperative Crohn’s Disease Study (ECCDS): results of drug treatment. Gastroenterology. Volume 86, 1984:249–266. [PubMed] [Google Scholar]
- 112.Summers RW, Switz DM, Sessions JT Jr, et al. National cooperative Crohn’s disease study: Results of drug treatment. Gastroenterology 1979;77:847–869. [PubMed] [Google Scholar]
- 113.Smith RC, Rhodes J, Heatley RV, et al. Low dose steroids and clinical relapse in Crohn’s disease: a controlled trial. Gut 1978;19:606–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Bar-Meir S, Chowers Y, Lavy A, et al. Budesonide versus prednisone in the treatment of active Crohn’s disease. The Israeli Budesonide Study Group. Gastroenterology 1998;115:835–40. [DOI] [PubMed] [Google Scholar]
- 115.Campieri M, Ferguson A, Doe W, et al. Oral budesonide is as effective as oral prednisolone in active Crohn’s disease. The Global Budesonide Study Group. Gut. Volume 41, 1997:209–214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Gross V, Andus T, Caesar I, et al. Oral pH-modified release budesonide versus 6-methylprednisolone in active Crohn’s disease. German/Austrian Budesonide Study Group. European journal of gastroenterology & hepatology. Volume 8, 1996:905–909. [PubMed] [Google Scholar]
- 117.Rutgeerts P, Lofberg R, Malchow H, et al. A comparison of budesonide with prednisolone for active Crohn’s disease. New England Journal of Medicine 1994;331:842–5. [DOI] [PubMed] [Google Scholar]
- 118.Tursi A, Giorgetti GM, Brandimarte G, et al. Beclomethasone dipropionate for the treatment of mild-to-moderate Crohn’s disease: an open-label, budesonide-controlled, randomized study. Medical Science Monitor 2006;12:PI29–32. [PubMed] [Google Scholar]
- 119.Akobeng AK, Zhang D, Gordon M, et al. Oral 5-aminosalicylic acid for maintenance of medically-induced remission in Crohn’s disease. Cochrane Database Syst Rev 2016;9:CD003715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Ford AC, Kane SV, Khan KJ, et al. Efficacy of 5-aminosalicylates in Crohn’s disease: systematic review and meta-analysis. Am J Gastroenterol 2011;106:617–29. [DOI] [PubMed] [Google Scholar]
- 121.Lim WC, Wang Y, MacDonald JK, et al. Aminosalicylates for induction of remission or response in Crohn’s disease. Cochrane Database Syst Rev 2016;7:CD008870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Noureldin M, Cohen-Mekelburg S, Mahmood A, et al. Trends of 5-Aminosalicylate Medication Use in Patients With Crohn Disease. Inflamm Bowel Dis 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Present DH, Rutgeerts P, Targan S, et al. Infliximab for the treatment of fistulas in patients with Crohn’s disease. New England Journal of Medicine 1999;340:1398–405. [DOI] [PubMed] [Google Scholar]
- 124.Sands BE, Anderson FH, Bernstein CN, et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. N Engl J Med 2004;350:876–85. [DOI] [PubMed] [Google Scholar]
- 125.Colombel JF, Schwartz DA, Sandborn WJ, et al. Adalimumab for the treatment of fistulas in patients with Crohn’s disease. Gut 2009;58:940–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Schreiber S, Lawrance IC, Thomsen OO, et al. Randomised clinical trial: certolizumab pegol for fistulas in Crohn’s disease - subgroup results from a placebo-controlled study. Alimentary Pharmacology & Therapeutics 2011;33:185–93. [DOI] [PubMed] [Google Scholar]
- 127.Feagan BG, Schwartz D, Danese S, et al. Efficacy of vedolizumab in fistulising Crohn’s disease: Exploratory analyses of data from GEMINI 2. Journal of Crohn’s & colitis 2018;17:17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Schwartz DP-BL, Lasch K, Adsul S, Danese S. Efficacy and safety of 2 vedolizumab IV regimens in patients with perianal fistulising Crohn’s disease: results of the ENTERPRISE study. J Crohns Colitis 2020;14:S418. [Google Scholar]
- 129.Sands BE, Gasink C, Jacobstein D, et al. Fistula healing in pivotal studies of ustekinumab in Crohn’s disease. Gastroenterology 2017;152 (5 Supplement 1):S185. [Google Scholar]
- 130.Present DH, Korelitz BI, Wisch N, et al. Treatment of Crohn’s disease with 6-mercaptopurine. A long-term, randomized, double-blind study. New England Journal of Medicine 1980;302:981–7. [DOI] [PubMed] [Google Scholar]
- 131.Thia KT, Mahadevan U, Feagan BG, et al. Ciprofloxacin or metronidazole for the treatment of perianal fistulas in patients with Crohn’s disease: a randomized, double-blind, placebo-controlled pilot study. Inflammatory Bowel Diseases 2009;15:17–24. [DOI] [PubMed] [Google Scholar]
- 132.West RL, van der Woude CJ, Hansen BE, et al. Clinical and endosonographic effect of ciprofloxacin on the treatment of perianal fistulae in Crohn’s disease with infliximab: a double-blind placebo-controlled study. Alimentary Pharmacology & Therapeutics 2004;20:1329–36. [DOI] [PubMed] [Google Scholar]
- 133.Dewint P, Hansen BE, Verhey E, et al. Adalimumab combined with ciprofloxacin is superior to adalimumab monotherapy in perianal fistula closure in Crohn’s disease: a randomised, double-blind, placebo controlled trial (ADAFI). Gut 2014;63:292–9. [DOI] [PubMed] [Google Scholar]
- 134.Bewtra M, Reed SD, Johnson FR, et al. Variation Among Patients With Crohn’s Disease in Benefit vs Risk Preferences and Remission Time Equivalents. Clin Gastroenterol Hepatol 2020;18:406–414 e7. [DOI] [PubMed] [Google Scholar]
- 135.Hazlewood GS, Pokharel G, Deardon R, et al. Patient preferences for maintenance therapy in Crohn’s disease: A discrete-choice experiment. PLoS One 2020;15:e0227635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Bewtra M, Fairchild AO, Gilroy E, et al. Inflammatory Bowel Disease Patients’ Willingness to Accept Medication Risk to Avoid Future Disease Relapse. Am J Gastroenterol 2015;110:1675–81. [DOI] [PubMed] [Google Scholar]
- 137.Pillai N, Dusheiko M, Burnand B, et al. A systematic review of cost-effectiveness studies comparing conventional, biological and surgical interventions for inflammatory bowel disease. PLoS One 2017;12:e0185500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Barnes EL, Loftus EV Jr., Kappelman MD. Effects of Race and Ethnicity on Diagnosis and Management of Inflammatory Bowel Diseases. Gastroenterology 2020. [DOI] [PubMed] [Google Scholar]
- 139.Nguyen GC, LaVeist TA, Harris ML, et al. Racial disparities in utilization of specialist care and medications in inflammatory bowel disease. Am J Gastroenterol 2010;105:2202–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Lin KK, Sewell JL. The effects of race and socioeconomic status on immunomodulator and anti-tumor necrosis factor use among ambulatory patients with inflammatory bowel disease in the United States. Am J Gastroenterol 2013;108:1824–30. [DOI] [PubMed] [Google Scholar]
- 141.Sewell JL, Inadomi JM, Yee HF, Jr. Race and inflammatory bowel disease in an urban healthcare system. Dig Dis Sci 2010;55:3479–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Nguyen GC, Sam J, Murthy SK, et al. Hospitalizations for inflammatory bowel disease: profile of the uninsured in the United States. Inflamm Bowel Dis 2009;15:726–33. [DOI] [PubMed] [Google Scholar]
- 143.Ma C, Smith MK, Guizzetti L, et al. Assessing National Trends and Disparities in Ambulatory, Emergency Department, and Inpatient Visits for Inflammatory Bowel Disease in the United States (2005–2016). Clin Gastroenterol Hepatol 2020;18:2500–2509 e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Ananthakrishnan AN, Nguyen GC, Bernstein CN. AGA Clinical Practice Update on Management of Inflammatory Bowel Disease in Elderly Patients: Expert Review. Gastroenterology 2021;160:445–451. [DOI] [PubMed] [Google Scholar]
- 145.Colombel JF, Panaccione R, Bossuyt P, et al. Effect of tight control management on Crohn’s disease (CALM): a multicentre, randomised, controlled phase 3 trial.[Erratum appears in Lancet. 2018 Dec 23;390(10114):2768; PMID: 29169669]. Lancet 2018;390:2779–2789. [DOI] [PubMed] [Google Scholar]
- 146.Panes J, Garcia-Olmo D, Van Assche G, et al. Expanded allogeneic adipose-derived mesenchymal stem cells (Cx601) for complex perianal fistulas in Crohn’s disease: a phase 3 randomised, double-blind controlled trial. Lancet 2016;388:1281–90. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.