

Abstract
Background/Aim
This study aimed to report a rare case of erythroderma or exfoliative dermatitis as a paraneoplastic syndrome of prostate adenocarcinoma. Exfoliative dermatitis is a rare inflammatory skin condition that is characterized by desquamation and erythema involving more than 90% of the body surface area. It is a clinical manifestation and usually associated with various underlying cutaneous disorders, drug induced reactions and malignancies.
Case Report
Herein we report a case of 55-year-old male patient who presented with progressively diffuse scaling and erythematous rash of 3 months duration. He was diagnosed with untreated prostate adenocarcinoma about 2 months prior his admission. Skin biopsy confirmed exfoliative erythroderma diagnosis. He was investigated extensively for other pathologies, however all work up remained negative except a CT finding of large heterogeneous prostate gland with elevated PSA which was consistent with prostate cancer. Daily oral prednisone for one week and hydrocortisone cream provided partial clinical improvement. The patient was discharged on tapering steroid to follow-up with urology and oncology for further underlying prostate carcinoma management.
Conclusion
We concluded that the ongoing erythroderma was a paraneoplastic syndrome of prostate adenocarcinoma. Hence, early detailed history and routine screening of malignancy-related biomarkers is warranted on any individuals presenting with such symptoms.
Keywords: Exfoliative dermatitis, erythroderma, prostate cancer, paraneoplastic syndrome
Generalized exfoliative dermatitis or erythroderma is a rare skin condition characterized by erythema/scaling of greater than 90% of the skin surface area, lymphadenopathy, hypothermia, tachycardia and significant pruritus. It was first described by Ferdinand Von Hebra in 1868 as a generalized skin redness and scaling (1). Erythroderma is a syndrome or clinical manifestation which is usually associated with a variety of diseases including preexisting dermatosis, drug exposure, infections, herbal medicines, and rarely underlying malignancies (2). As a paraneoplastic syndrome of visceral malignancies, erythroderma has only been reported in 0.8-1% of total cases (3,4). Based on expert analysis, erythroderma is usually benign and doesn’t pose a significant risk of death, however if it is fulminant, it can be life-threatening and is associated with a high mortality risk specially in hospitalized patients (5,6). Herein we present a case of exfoliative dermatitis associated with underlying prostate adenocarcinoma which by itself is a very rare presentation and has only been reported in few cases in the literature.
Case Report
A 55-years-old male patient admitted at our Institution on November 2019 for progressively worsening diffuse scaling and erythematous rash associated with occasional itching, significant weight loss (about 40 lb), and night sweats. Three months prior to his admission, the skin rash had started on his arm and chest that progressively spread all over the body for which he visited the ER twice, prescribed topical steroid with antihistaminic but no significant improvement was achieved. His past medical history was remarkable for hypertension, and recently diagnosed prostate adenocarcinoma for one month without treatment. Amlodipine was the only medication the patient has been taking at home. Family history was unremarkable for any dermatological disease or cancer history. He had no history of alcohol or tobacco use in the past. Clinically, the patient was hemodynamically stable. Skin examination demonstrated generalized scaling, flaking and erythema involving >90% of the body surface area including scalp, face, trunk and extremities with evident signs of scratching due to significant pruritus (Figure 1). Palms and soles along oral mucosa were spared. Bilateral non-tender axillary and inguinal lymphadenopathy were present. Envisioned differential diagnosis included paraneoplastic manifestation from prostate adenocarcinoma, cutaneous T cell lymphoma (CTCL) or new onset of inflammatory dermatosis. Laboratory examination including differential blood count, clinical chemistry, rheumatoid factors, antinuclear antibody, cyclic citrullinated peptide, bullous pemphigoid autoantibodies, hepatitis panel and HIV were unremarkable except elevated serum prostate specific antigen (PSA) of 21 ng/ml (1-1.5 ng/ml). A computerized tomography (CT) of abdomen with contrast showed a large heterogeneous prostate gland (Figure 2). CT thorax with contrast revealed bilateral axillary lymphadenopathy, measuring up to 2 cm. An excisional biopsy from right axillary lymph node demonstrated histological features of dermatopathic lymphadenopathy with florid proliferation of Langerhans cells in paracortical areas with HMB-45 negative immunostaining (Figure 3). Histopathological result of skin punch biopsy showed spongiosis, lichenoid infiltrates, parakeratosis, and psoriasiform hyperplasia with dermis contains histiocytes, lymphocytes, and rare eosinophils (Figure 4). Special stains (GMS, PAS, AFB) for fungal and acid-fast organisms were negative. No malignant infiltrating cells were detected. The patient’s generalized pruritis was partially relieved with oral antihistaminics and topical corticosteroids. However, daily oral prednisone 1 mg/kg per day for a week along with corticosteroid cream did provide partial clinical improvement of exfoliative erythroderma. The patient was referred to the urology and oncology clinic for prompt initiation of underlying prostate carcinoma treatment. Per chart review of outpatient oncology notes, the patient has been reported to have significant improvement of erythroderma following surgical procedure and androgen deprivation therapy in six months of follow-up.
Figure 1. Clinical presentation of diffuse erythroderma on trunk and extremities. A: Diffuse erythematous rash of bilateral dorsal aspect of hands. B: Diffuse erythema and scaling rash over trunk, chest and arms. C: Scaling erythematous rash of lower extremity.

Figure 2. CT scan of abdomen and pelvis showing enlarged prostate gland.

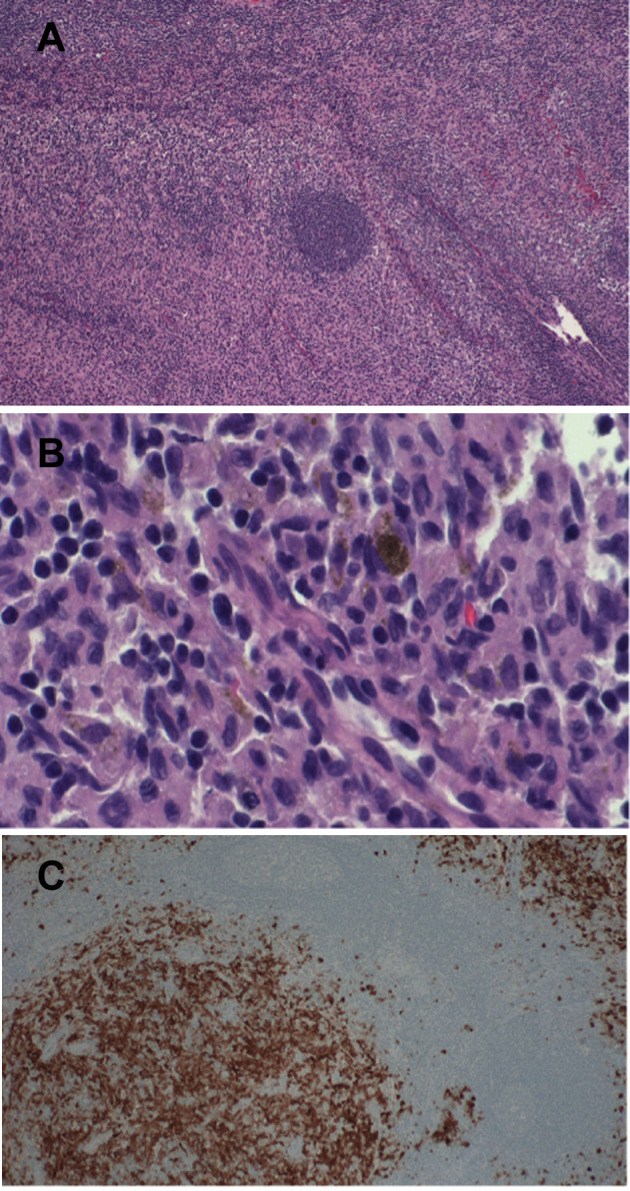
Figure 3. Histopathological examination of excisional lymph node biopsy. A: Intermediate power view of the axillary lymph nose. The paracortical expansion by proliferating interdigitating dendritic cells, Langerhans, histiocytes and lymphocytes are predominant with a remnant of follicle in the center (H&E original magnification ×200). B: High power view shows proliferating interdigitating dendritic cells and Langerhans cells mixed with lymphocytes and melanin-containing macrophages (H&E original magnification ×400). C: Langerhans cells and interdigitating dendritic cells are accentuated by S100 immunohistochemical stain (original magnification ×100).

Figure 4. Histopathological examination of skin punched biopsy. A: Low power view of the skin punch biopsy shows acanthosis and parakeratosis in addition to derma inflammation and spongiosis (H&E original magnification ×100). B: High power view shows the lichenoid nature of inflammation in some areas.
Review of the literature. To identify the published reports of erythroderma as a paraneoplastic phenomenon of prostate adenocarcinoma, a comprehensive review of literature using the search terms ’erythroderma, exfoliative dermatitis and prostate cancer’ was performed. Only five cases of prostate cancer-associated erythroderma were found to have been previously reported in the literature. We included the relevant information such as age of diagnosis, associated malignancy, clinical presentation, treatment and outcome in the Table I. By creating such a table, we aimed to give the readers a short overview of the published data in the literature in order to emphasize on the rarity of this phenomenon.
Table I. Reported cases of exfoliative dermatitis in the literature.

Discussion and Conclusion
Erythroderma, or generalized exfoliative dermatitis, is a rare severe inflammatory skin condition (11). Epidemiologically, the overall incidence of erythroderma both in the USA and the world is unknown and has not yet been addressed, however, a recent retrospective study from Portugal reported an incidence of 9.4 cases/year and 11.9% in hospitalized patients. A different study from India recorded the incidence of erythroderma in outpatient dermatology offices as 35 per 100,000 patients (0.035%) (4,5,12). Studies have shown a male predominance with male-to-female ratio ranging from 2 and 4 to 1 and a mean age of onset between 40 to 60 years (13). The physiopathogenic mechanisms of erythroderma varies according to the underlying causes. Even though, the exact mechanism is not fully understood, however the proposed common pathogenesis is believed to be due to increased expression of adhesion molecules in epithelial cells (VCAM-1, ICAM-1, E-selectin, and P-selectin) which ultimately increases dermal inflammation and epidermal proliferation through an increase in mitosis that causes an increase in overall epidermal cells numbers, and increased cell turnover, with decreases in transit time through the epidermis (14,15). There is a repeated turnover of epithelial cells in normal epidermis. Initially, cell division occurs near the basal layer and they move toward the periphery where they become well-keratinized in approximately 10-12 days. Subsequently, the cells are sloughed off after being remained in the stratum corneum for another 12-14 days. In contrast, the number of cells in the germinative layer and their mitotic rate is increased in exfoliative dermatitis. The transit time of cells through the epidermis is shortened. As a result, the exfoliated scales are incompletely keratinized and contain material normally retained by the skin which may result in a negative nitrogen balance and result in significant scale loss (7.2 g-22.6 g per day) (16). The other common pathophysiological mechanism of exfoliative erythroderma is increased blood flow to the skin, with impaired barrier function, which also results in increased insensible fluid loss through transpiration. Patients might experience dehydration and reflex tachycardia. In severe cases, high-output cardiac failure may occur (17,18). The most common underlying etiology for erythroderma is preexisting dermatoses, drugs induced, and malignancies, whilst the rest of cases remain idiopathic (12). Based on several reports, about 1% of erythroderma cases have a neoplasic or paraneoplastic etiology (4). Malignancies that have a strong association with erythroderma, including but not limited to CTCL (cutaneous T-cell lymphoma), laryngeal, thyroid, breast, lung, esophageal, gastric, hepatocellular, tongue, gallbladder, colon, fallopian tube and prostate cancers are reported (12,19). Most of the time, it is difficult to determine the association of erythroderma and malignancies, however if erythroderma develops insidiously and progressively in the absence of previous skin disease and shows resistance to standard therapy, by that time, an underlying malignancy should be strongly considered (14,20). After renal cell carcinoma, prostate cancer is the second most common urological malignancy to be associated with paraneoplastic syndromes. It typically occurs in the setting of advanced prostate cancer with poor prognosis (3,21). In the literature, more than one hundred cases of different paraneoplesatic syndromes including those caused by endocrine or hormonal effects, immune mechanisms, and other neurological or hematological effects associated with prostate cancer have been reported. Among those, only a few cases have been related to dermatological conditions such as dermatomyositis sweat syndrome and erythroderma. Although rare, erythroderma as a dermatological condition arising from prostate cancer is well documented in the literature (21,22).
Clinically, erythroderma has a gradual and insidious onset in the setting of malignancies (9). The classical clinical feature of erythroderma is bright red patches followed by the appearance of a white or yellow scale involving especially the head, trunk and genital region and tends to spread to most of the skin surface in a matter of days or weeks (23). It usually, but not always spares the palms, soles and the mucous membranes (24). Skin tightness, and pruritis occurs in nearly all patients, and more than half of the patients may present with fever as well. More than half of patients also develop lymphadenopathy, splenomegaly, and hepatomegaly that may suggest a drug hypersensitivity or malignancy (12). Other rare symptoms including hair loss and nail findings such as subungual hyperkeratosis, onycholysis, ridging, dry or brittle nails, or nail shedding may also be present (5,14).
To diagnose erythroderma as an underlying cause of internal malignancy, there needs to be a history of insidious development, refractoriness to standard therapies, absence of preexisting dermatosis and progressive decompensation. Prostate cancer should be highly suspected in male patients with erythroderma older than 45 years as the incidence of this malignancy increases with age old and have elevated PSA level (5,9).
The majority of erythroderma cases can be diagnosed easily with the clinical finding of generalized erythema and desquamation involving ≥90% of the skin surface area, however due to variety of triggering causes, defining the exact underlying pathology is a challenge for physicians and a profound clinicopathological correlation should be established (17,25). Therefore, a skin biopsy is a mandatory first step workup of erythrodermic cases, which requires a highly trained pathologist to provide a precise diagnosis (25). Several studies report that skin biopsies are helpful in diagnoses of 53-66% of erythroderma cases, however, a considerable number of cases (39.1%) still remain inconclusive as idiopathic not matching the final diagnosis (12,26). Based on previous studies, the most frequent histopathological findings in erythroderma were hyperkeratosis, acanthosis, spongiosis, and perivascular inflammatory infiltrate (27).
In most cases, erythroderma can be severe or life-threatening which requires inpatient care for further investigation and treatment (28). Regardless of underlying etiology, supportive care is the initial management of all types of erythroderma that mainly involves nutrition assessment, monitoring, regulating environmental temperature, and ensuring metabolic and hemodynamic stability. Colloid baths and wet compresses can improve skin barrier functions along with emollient creams with low-potency topical corticosteroids (11). Additionally, sedation with antihistamines can alleviate scratching and relieve pruritus and anxiety, whilst preventing secondary skin infections (20). Erythroderma as a paraneoplastic syndrome of prostate cancer mostly resolves upon treatment of the underlying tumor, however some cases fail to respond and require further treatment with systemic corticosteroids or other immunosuppressant such as methotrexate and cyclosporine (20,29). Chemotherapeutic agents can be considered for advanced prostate cancer where the paraneoplastic syndrome represents first manifestation of progression of the tumor (21).
In conclusion, although rare it is important to keep prostate cancer among our differential diagnosis in patients that present with unexplained dermatological findings like exfoliative dermatitis.
Conflicts of Interest
None of the Authors have any financial or personal bias to declare. The Authors report no conflicts of interest.
Authors’ Contributions
SR Ghafouri completed the background research, drafted and edited the manuscript and the was the grantor of the publication. I. Wahdayar, N Whited, MN Hakim, S. Gaur and F. Dihowm edited and completed the manuscript.
References
- 1.Balasubramaniam P, Berth-Jones J. Erythroderma: 90% skin failure. Hosp Med. 2004;65(2):100–102. doi: 10.12968/hosp.2004.65.2.12068. [DOI] [PubMed] [Google Scholar]
- 2.Miyashiro D, Sanches JA. Erythroderma: a prospective study of 309 patients followed for 12 years in a tertiary center. Sci Rep. 2020;10(1):9774. doi: 10.1038/s41598-020-66040-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Momm F, Pflieger D, Lutterbach J. Paraneoplastic erythroderma in a prostate cancer patient. Strahlenther Onkol. 2002;178(7):393–395. doi: 10.1007/s00066-002-0967-y. [DOI] [PubMed] [Google Scholar]
- 4.Yuan XY, Guo JY, Dang YP, Qiao L, Liu W. Erythroderma: A clinical-etiological study of 82 cases. Eur J Dermatol. 2010;20(3):373–377. doi: 10.1684/ejd.2010.0943. [DOI] [PubMed] [Google Scholar]
- 5.Okoduwa C, Lambert WC, Schwartz RA, Kubeyinje E, Eitokpah A, Sinha S, Chen W. Erythroderma: review of a potentially life-threatening dermatosis. Indian J Dermatol. 2009;54(1):1–6. doi: 10.4103/0019-5154.48976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Akhyani M, Ghodsi ZS, Toosi S, Dabbaghian H. Erythroderma: a clinical study of 97 cases. BMC Dermatol. 2005;5:5. doi: 10.1186/1471-5945-5-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Schwartz RA, Trotter MG. Generalized vitiligo after erythroderma. Dermatologica. 1983;167(1):42–46. doi: 10.1159/000249744. [DOI] [PubMed] [Google Scholar]
- 8.Li S, Yu X, Wang T. Papuloerythroderma of Ofuji. JAMA Dermatol. 2020;156(12):1365. doi: 10.1001/jamadermatol.2020.2973. [DOI] [PubMed] [Google Scholar]
- 9.Rosen T, Chappell R, Drucker C. Exfoliative dermatitis: presenting sign of internal malignancy. South Med J. 1979;72(6):652–653. [PubMed] [Google Scholar]
- 10.Danny GC, Swaminathan A, Rajesh G, Veeraraghavan M. Paraneoplastic erythroderma as a protean manifestation of adenocarcinoma prostate. Indian J Dermatol. 2020;65(1):72–74. doi: 10.4103/ijd.IJD_189_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mistry N, Gupta A, Alavi A, Sibbald RG. A review of the diagnosis and management of erythroderma (generalized red skin) Adv Skin Wound Care. 2015;28(5):228–36. doi: 10.1097/01.ASW.0000463573.40637.73. quiz 237-8. [DOI] [PubMed] [Google Scholar]
- 12.César A, Cruz M, Mota A, Azevedo F. Erythroderma. A clinical and etiological study of 103 patients. J Dermatol Case Rep. 2016;10(1):1–9. doi: 10.3315/jdcr.2016.1222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sehgal VN, Srivastava G. Exfoliative dermatitis. A prospective study of 80 patients. Dermatologica. 1986;173(6):278–284. [PubMed] [Google Scholar]
- 14.Austad SS, Athalye L. Exfoliative Dermatitis. 2021 [PubMed] [Google Scholar]
- 15.Sigurdsson V, de Vries IJ, Toonstra J, Bihari IC, Thepen T, Bruijnzeel-Koomen CA, van Vloten WA. Expression of VCAM-1, ICAM-1, E-selectin, and P-selectin on endothelium in situ in patients with erythroderma, mycosis fungoides and atopic dermatitis. J Cutan Pathol. 2000;27(9):436–440. doi: 10.1034/j.1600-0560.2000.027009436.x. [DOI] [PubMed] [Google Scholar]
- 16.Kanthraj GR, Srinivas CR, Devi PU, Ganasoundari A, Shenoi SD, Deshmukh RP, Suresh BJ, Pai SB. Quantitative estimation and recommendations for supplementation of protein lost through scaling in exfoliative dermatitis. Int J Dermatol. 1999;38(2):91–95. doi: 10.1046/j.1365-4362.1999.00408.x. [DOI] [PubMed] [Google Scholar]
- 17.Salami TA, Enahoro Oziegbe O, Omeife H. Exfoliative dermatitis: patterns of clinical presentation in a tropical rural and suburban dermatology practice in Nigeria. Int J Dermatol. 2012;51(9):1086–1089. doi: 10.1111/j.1365-4632.2011.05400.x. [DOI] [PubMed] [Google Scholar]
- 18.Banerjee S, Ghosh S, Mandal RK. A study of correlation between clinical and histopathological findings of erythroderma in North Bengal population. Indian J Dermatol. 2015;60(6):549–555. doi: 10.4103/0019-5154.169124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tan GF, Kong YL, Tan AS, Tey HL. Causes and features of erythroderma. Ann Acad Med Singap. 2014;43(8):391–394. [PubMed] [Google Scholar]
- 20.Karakayli G, Beckham G, Orengo I, Rosen T. Exfoliative dermatitis. Am Fam Physician. 1999;59(3):625–630. [PubMed] [Google Scholar]
- 21.Hong MK, Kong J, Namdarian B, Longano A, Grummet J, Hovens CM, Costello AJ, Corcoran NM. Paraneoplastic syndromes in prostate cancer. Nat Rev Urol. 2010;7(12):681–692. doi: 10.1038/nrurol.2010.186. [DOI] [PubMed] [Google Scholar]
- 22.Matzkin H, Braf Z. Paraneoplastic syndromes associated with prostatic carcinoma. J Urol. 1987;138(5):1129–1133. doi: 10.1016/s0022-5347(17)43524-5. [DOI] [PubMed] [Google Scholar]
- 23.Sehgal VN, Srivastava G, Sardana K. Erythroderma/exfoliative dermatitis: a synopsis. Int J Dermatol. 2004;43(1):39–47. doi: 10.1111/j.1365-4632.2004.01975.x. [DOI] [PubMed] [Google Scholar]
- 24.Agarwal S, Khullar R, Kalla G, Malhotra YK. Nose sign of exfoliative dermatitis: a possible mechanism. Arch Dermatol. 1992;128(5):704. [PubMed] [Google Scholar]
- 25.Cuellar-barboza A, Ocampo-candiani J, Herz-ruelas M. A Practical approach to the diagnosis and treatment of adult erythroderma. Actas Dermo-Sifiliográficas (English Edition) 2020;109(9):777–790. doi: 10.1016/j.adengl.2018.05.033. [DOI] [PubMed] [Google Scholar]
- 26.Megna M, Sidikov AA, Zaslavsky DV, Chuprov IN, Timoshchuk EA, Egorova U, Wenzel J, Nasyrov RA. The role of histological presentation in erythroderma. Int J Dermatol. 2017;56(4):400–404. doi: 10.1111/ijd.13488. [DOI] [PubMed] [Google Scholar]
- 27.Tomasini C, Aloi F, Solaroli C, Pippione M. Psoriatic erythroderma: a histopathologic study of forty-five patients. Dermatology. 1997;194(2):102–106. doi: 10.1159/000246075. [DOI] [PubMed] [Google Scholar]
- 28.Rothe MJ, Bernstein ML, Grant-Kels JM. Life-threatening erythroderma: diagnosing and treating the “red man”. Clin Dermatol. 2005;23(2):206–217. doi: 10.1016/j.clindermatol.2004.06.018. [DOI] [PubMed] [Google Scholar]
- 29.Masuda H, Urushibara M, Kihara K. Successful treatment of dermatomyositis associated with adenocarcinoma of the prostate after radical prostatectomy. J Urol. 2003;169(3):1084. doi: 10.1097/01.ju.0000047281.73280.7e. [DOI] [PubMed] [Google Scholar]