

Abstract
Exercise prevents and aids treatment of coronary heart disease, hypertension, heart failure, diabetes mellitus, obesity and depression, reduces cardiac events and improves survival. However, evidence suggests that the relationship between exercise and mortality may be curvilinear, with modest additional benefit at higher levels. Intensive exercise has also been associated with increased atrial fibrillation risk, although its clinical implications are not well understood. Other proposed adverse effects of exercise on the heart, including reduced right ventricular function, elevated cardiac biomarkers, myocardial fibrosis and coronary artery calcification, are less substantiated. Current evidence cannot affirm that extreme exercise is dangerous and future studies should combine large cohorts to obtain a statistically reliable limit. Associations between features of the athlete’s heart and cardiovascular morbidity and mortality should also be explored.
Key words: arrhythmias, atrial fibrillation, BJCA, exercise, heart diseases, sports, ventricular remodelling
Introduction
With semi-professional sporting events becoming more accessible,1 the effect of endurance training on the body is increasingly relevant, not just in elite athletes, but also fitness enthusiasts. Exercise prevents and aids treatment of coronary heart disease (CHD), hypertension, heart failure, diabetes mellitus, obesity and depression,2,3 reduces cardiac events,1 and improves survival.4,5 However, there is concern excessive exercise could have adverse cardiac effects.2 This article aims to address whether an upper limit to mortality benefits of exercise exists, consider physiological and potentially pathological changes in the athlete’s heart, and discuss implications on exercise recommendation and future research. The dangers of sports in individuals with underlying rhythm and structural abnormalities, while important, are beyond the focus of this article.
Exercise and mortality: is there an upper limit?
Physical activity (PA) improves all-cause and cardiovascular disease (CVD) mortality,4,5 but evidence suggests dwindling gains at high levels (table 1).5,6 A U-shaped dose-response curve between exercise and mortality was previously described, with progressive loss of benefit past an upper limit.5 More recently, it appears this relationship may be curvilinear. Gain in mortality benefit was steepest at moderate PA (3–5 times recommendations) with modest additional benefit at higher levels, but no indication of harm even at 10 times the recommended level.6 A small study presented at the American Heart Association (AHA) 2019 meeting found no CVD deaths in 66 athletes performing extreme exercise (≥10,000 metabolic equivalents of task [MET]-minutes/week).7 In aggregate, there is presently no defined upper limit of mortality benefit from exercise.
Table 1. Overview of the impact of exercise on mortality and potential adverse effects on the heart as evidenced in current literature.
|
Key findings |
Relevant studies |
|---|---|
|
All-cause mortality and CVD mortality | |
|
|
|
Ventricular function | |
|
La Gerche et al. (2014)8 |
|
Myocardial fibrosis | |
|
van de Schoor et al. (2016)9 |
|
Atrial fibrillation | |
|
Andersen et al. (2013)10 Thelle et al. (2013)11 Svedberg et al. (2019)14 |
|
Coronary artery calcification | |
|
Aengevaeren et al. (2017)12 Merghani et al. (2017)13 |
Key: AF = atrial fibrillation; CAC = coronary artery calcium; CVD = cardiovascular disease; LGE = late gadolinium enhancement; RV = right ventricle
The athlete’s heart
Acute aerobic exercise can increase cardiac output (CO) by fourfold in healthy untrained individuals and eightfold in elite athletes, largely mediated by increased stroke volume (SV).3 With chronic exercise (figure 1), exercise-induced cardiac remodelling (EICR) such as left ventricular (LV) hypertrophy and dilation of all cardiac chambers develops. These enhance diastolic filling and augment SV, further increasing CO and maximal oxygen uptake.1,3 The athlete’s electrocardiogram (ECG) differs from the general healthy population (e.g. benign arrhythmias, axis deviation, voltage criterion, ST changes) due to increased vagal tone and enlarged cardiac dimensions.1 While physiological adaptations to exercise within certain parameters improves performance,3 intensive exercise has been associated with reduced right ventricular (RV) function,8 elevated cardiac biomarkers,2 myocardial fibrosis,9 atrial fibrillation (AF),10,11 and coronary artery calcification (CAC).12,13 These are discussed below and key study findings summarised in table 1.
Figure 1. Visual representation of the morphological and physiological adaptations in the heart with chronic exercise.
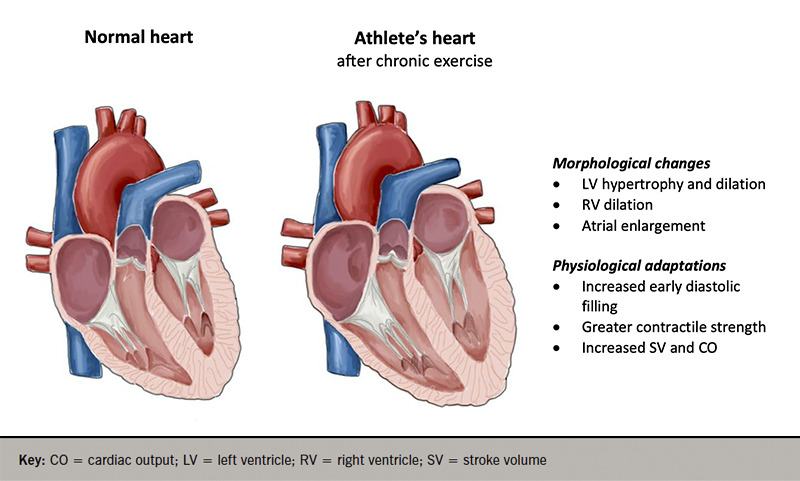
Key: CO = cardiac output; LV = left ventricle; RV = right ventricle; SV = stroke volume
Remodelling and ventricular function
EICR may be difficult to distinguish from pathology, and some athletes have cardiac dimensions exceeding pathological thresholds.1 Further, some propose that not all EICR may be benign.2 Intensive endurance exercise has been associated with RV enlargement and reduced systolic function, most pronounced after longer events and faster timings.8 Although changes normalised within 6–11 days, it is unknown if repeated transient reduction in RV function, with inadequate myocardial recovery in between, may damage the heart in the long term.
Myocardial fibrosis
Myocardial fibrosis, measured as late gadolinium enhancement (LGE) on cardiac magnetic resonance (CMR) imaging, is present in some athletes (5.9% in a systematic review).9 Location varies widely, but fibrosis was most frequently found near the interventricular septum and RV insertion points. Some speculate transient injury during exercise results in scarring.9 Serological markers associated with damage (e.g. cardiac troponins, creatine kinase-MB, B-type natriuretic peptide) transiently rise during and after exercise,2 and were found to correspond to reduced RV function.8 However, it is unusual that myocardial fibrosis was detected in only a small proportion of athletes, considering most engaged in high PA. Certain individuals may be genetically susceptible and LGE pattern variation (non-specific, ischaemic, myocarditic and hypertrophic)9 also raises the possibility that myocardial fibrosis occurs in those with underlying cardiac disease.4
Atrial fibrillation
Lower AF risk is seen with low-to-moderate exercise, but intensive PA may increase risk.4 Elite skiers who participated in more races had increased AF incidence,10 and highly active men were three times more likely to be prescribed flecainide, a surrogate marker for lone AF, than sedentary men.11 Clinical implications of AF in athletes are not completely understood, but a recent study found lower stroke and mortality incidence in skiers with AF compared with non-skiers with AF. Stroke risk was still higher, however, compared with non-skiers without AF.14 Atrial enlargement and increased parasympathetic tone may contribute to AF in athletes.2,14 There is currently no indication that chronic exercise promotes dangerous ventricular arrhythmias in those without underlying disease.10
Coronary artery calcification
CHD is the leading cause of exercise-related sudden cardiac death in older athletes (>35 years old).1,4 CAC predicts atherosclerotic plaque burden and risk of adverse cardiovascular events.12 Male athletes are more likely to have CAC than sedentary men and among athletes, increased lifelong exercise is associated with higher CAC prevalence.12 However, athletes often have predominantly calcified plaques, whereas less active individuals usually have mixed plaques, which are associated with significantly higher cardiovascular risk.12,13 Athletes have a lower CHD risk than non-athletes,12 and the clinical significance of CAC in athletes remains unclear. It is possible exercise may facilitate plaque remodelling and confer stability.4
Moving forward
The AHA recommends at least 150–300 minutes of moderate or 75–150 minutes of vigorous aerobic PA weekly.15 Arguably, a curvilinear relationship between exercise and mortality does not greatly change recommendations for the general population. Many engage in too little exercise and encouraging any level of PA is the priority. Indeed, exercise significantly improves survival, irrespective of amount, when compared with inactivity.5,6 With the highest gains at the start of the dose-response curve, clinicians can be heartened that encouraging patients to begin exercising may confer the most benefit. For elite and highly active amateur athletes, there appears no immediate need to caution against excessive exercise from a mortality standpoint. Current evidence has yet to define an upper limit of benefit, with continued marginal gains even at PA 10 times the recommended level.6 The proportion of individuals engaging in PA at the highest ends of the dose-response curve is small, therefore, future studies should combine large cohorts to obtain a statistically reliable limit. Well-controlled intervention studies are important to address confounders in observational data.
The association between high PA levels and AF potentially describes an adverse effect on the athlete’s heart. While exercise may offset some stroke risk in athletes with AF, the risk is still higher compared with non-athletes without AF.14 Risk stratification for anticoagulation is similar to non-athletes but management nuances should be explored.4 The other propositions are less substantiated: long-term effects of transiently reduced RV function are uncertain, non-exercise related underlying causes may contribute to myocardial fibrosis and the clinical implications of CAC in athletes are unknown. A series of insults from vigorous exercise in a susceptible individual may be harmful, but this should not form the basis on which to restrict exercise training.4 Future studies should include longer follow-up for long-term effects, and explore associations between specific features of the athlete’s heart and cardiovascular morbidity and mortality.
Conclusion
Current evidence cannot affirm that high levels of exercise are dangerous, although there is an indication of diminishing mortality benefit and increased AF risk. There is still much to learn about the athlete’s heart, and clinicians should remain open to potential harms in order to fairly advise athletes aiming for sporting excellence. For the rest of us, as with nearly everything in medicine, exercise in moderation may be the wise approach.
Key messages
Exercise has significant health benefits, reduces cardiac events and improves survival. There may be diminishing mortality benefit at higher levels of exercise but an upper limit has yet to be defined
High levels of exercise are associated with increased atrial fibrillation (AF) risk, although its clinical implications are not well understood. Risk stratification for anticoagulation is extrapolated from data from non-athletes, and nuances in the management of this specific group should be explored
Intensive exercise may be associated with adverse structural and functional changes in the heart. However, their significance is unclear and further study is needed to explore their impact on cardiovascular morbidity and mortality
Editors’ note
This article was the prize-winning entry in the National Essay Prize 2020 of the British Junior Cardiologists’ Association (BJCA).
Funding Statement
Funding None.
Footnotes
Conflicts of interest
None declared.
References
- 1.Sharma S, Merghani A, Mont L. Exercise and the heart: the good, the bad, and the ugly. Eur Heart J. 2015;36:1445–1453. doi: 10.1093/eurheartj/ehv090. [DOI] [PubMed] [Google Scholar]
- 2.O’Keefe JH, Patil HR, Lavie CJ, et al. Potential adverse cardiovascular effects from excessive endurance exercise. Mayo Clin Proc. 2012;87:587–595. doi: 10.1016/j.mayocp.2012.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lavie CJ, Arena R, Swift DL, et al. Exercise and the cardiovascular system: clinical science and cardiovascular outcomes. Circ Res. 2015;117:207–219. doi: 10.1161/CIRCRESAHA.117.305205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rao P, Hutter AM, Baggish AL. The limits of cardiac performance: can too much exercise damage the heart? Am J Med. 2018;131:1279–1284. doi: 10.1016/j.amjmed.2018.05.037. [DOI] [PubMed] [Google Scholar]
- 5.Schnohr P, Marott JL, Lange P, Jensen GG. Longevity in male and female joggers: the Copenhagen City Heart study. Am J Epidemiol. 2013;177:683–689. doi: 10.1093/aje/kws301. [DOI] [PubMed] [Google Scholar]
- 6.Arem H, Moore SC, Patel A, et al. Leisure time physical activity and mortality: a detailed pooled analysis of the dose-response relationship. JAMA Intern Med. 2015;175:959–967. doi: 10.1001/jamainternmed.2015.0533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.DeFina LF, Wright BB, Willis BL, et al. Abstract 14863: athletes performing extraordinary physical activity (>10,000 MET·Min/Week) at no greater risk of all-cause or cardiovascular disease mortality. Circulation. 2019;140:A14863. Available at: https://www.ahajournals.org/doi/10.1161/circ.140.suppl_1.14863. [Google Scholar]
- 8.La Gerche A, Burns AT, Mooney DJ, et al. Exercise-induced right ventricular dysfunction and structural remodelling in endurance athletes. Eur Heart J. 2012;33:998–1006. doi: 10.1093/eurheartj/ehr397. [DOI] [PubMed] [Google Scholar]
- 9.van de Schoor FR, Aengevaeren VL, Hopman MTE, et al. Myocardial fibrosis in athletes. Mayo Clin Proc. 2016;91:1617–1631. doi: 10.1016/j.mayocp.2016.07.012. [DOI] [PubMed] [Google Scholar]
- 10.Andersen K, Farahmand B, Ahlbom A, et al. Risk of arrhythmias in 52 755 long-distance cross-country skiers: a cohort study. Eur Heart J. 2013;34:3624–3631. doi: 10.1093/eurheartj/eht188. [DOI] [PubMed] [Google Scholar]
- 11.Thelle DS, Selmer R, Gjesdal K, et al. Resting heart rate and physical activity as risk factors for lone atrial fibrillation: a prospective study of 309 540 men and women. Heart. 2013;99:1755–1760. doi: 10.1136/heartjnl-2013-303825. [DOI] [PubMed] [Google Scholar]
- 12.Aengevaeren VL, Mosterd A, Braber TL, et al. Relationship between lifelong exercise volume and coronary atherosclerosis in athletes. Circulation. 2017;136:138–148. doi: 10.1161/CIRCULATIONAHA.117.027834. [DOI] [PubMed] [Google Scholar]
- 13.Merghani A, Maestrini V, Rosmini S, et al. Prevalence of subclinical coronary artery disease in masters endurance athletes with a low atherosclerotic risk profile. Circulation. 2017;136:126–137. doi: 10.1161/CIRCULATIONAHA.116.026964. [DOI] [PubMed] [Google Scholar]
- 14.Svedberg N, Sundström J, James S, Hållmarker U, Hambraeus K, Andersen K. Long-term incidence of atrial fibrillation and stroke among cross-country skiers. Circulation. 2019;140:910–920. doi: 10.1161/CIRCULATIONAHA.118.039461. [DOI] [PubMed] [Google Scholar]
- 15.Piercy KL, Troiano RP. Physical activity guidelines for Americans from the US Department of Health and Human Services. Circ Cardiovasc Qual Outcomes. 2018;11:e005263. doi: 10.1161/CIRCOUTCOMES.118.005263. [DOI] [PubMed] [Google Scholar]