

Abstract
Multiple myeloma is characterized by the presence of M-protein (monoclonal) in blood or urine. These proteins are immunoglobulins which are produced by a clone of abnormally proliferating B-lymphocytes and/or plasma cells. To evaluate M-protein, serum protein electrophoresis (SPEP) is used where a single band, known as M-band is seen. This band is usually seen in the gamma globulin region. However, in rare entities like biclonal gammopathy, two M-bands appear simultaneously at different positions on SPEP which may be attributed to the clonal expansion of two different neoplastic cell lines. Here, we describe an atypical case of IgA-kappa multiple myeloma, where two M-bands (one in the beta region and one in the gamma globulin region) were found during SPEP. This simulated a picture of biclonal gammopathy. However the monoclonal nature of this M-protein was proved by performing immunofixation electrophoresis (IFE). Further, we put across images to explain how IFE helps in differentiating between apparent and true biclonality.
Keywords: Electrophoresis, Monoclonal, Biclonal, Gammopathy
Introduction
Monoclonal proteins are immunoglobulins seen in hematological disorders such as monoclonal gammopathies. Rapidly proliferating clone of B-lymphocytes and/or plasma cells produce these—proteins and these can be detected in blood and/or urine. They are found most commonly in multiple myeloma, monoclonal gammopathy of undetermined significance (MGUS) and Waldenstorm’s Macroglobulinemia [1–3].
Five isotypes of M-protein are detected namely, IgG, IgA, IgM, IgD and IgE. However, IgG (52%) and IgA (21%) are the most commonly detected isotypes [1]. Detection is done by serum protein electrophoresis (SPEP) wherein an M-protein is seen as a single discrete monoclonal band (M-band), mostly in gamma globulin region. M-Band may also be seen in the beta region in case of IgA or IgM isotype. Presence of single bands are most common. However, in case of clonal expansion of two different neoplastic cell lines (in 3–4% of multiple myeloma), two distinct M-bands may be seen together. This condition, known as biclonal gammopathy, is seen to have a strong association with multiple myeloma and lymphoproliferative disorders. If seen in association with MGUS, the condition is known as double gammopathy of undetermined significance (DGUS/BGUS) [2]. Clinical importance of biclonal gammopathies lies in the fact that assessment of both the clonal proteins may help in evaluating the synchronicity of response of the two clones during treatment and follow-up and help in patient management and decision making. Besides, double M-bands are frequently associated with leukemias and lymphomas) [3, 4]. However, in one study it was seen that no biclonal gammopathies of undetermined significance (BGUS) evolved to a malignant disease. In a high percentage of patients, at least one of the two clonal components disappeared, sometimes spontaneously [5].
Here, we present a case of multiple myeloma which showed double M-bands in SPEP in the absence of true biclonality. The absence of biclonality in our case was proved by performing immunofixation electrophoresis (IFE).
A 62 year old male from Haryana presented with back pain since 2 months in a corporate hospital in North India. On general examination there was no pallor. On routine investigation, Hb = 12.8 g/dL, WBC = 8400/μL, PCV slightly reduced (38.5%) with slightly raised ESR (14 mm/h) was recorded. Biochemical investigations revealed total protein = 8.2 g/dL, albumin = 4.4 g/dL with normal albumin/globulin ratio. Renal function test (urea = 44 mg/dL, creatinine = 1 mg/dL) were normal. Lactate dehydrogenase was also within normal limit (LDH = 151 U/L) On radiological examination, intervertebral disc space was slightly reduced at C5–C6 and L4–L5 levels.
However, keeping in view the age of the patient and persisting nature of pain, he was adviced admission for follow up of suspected multiple myeloma even though the routine investigations appeared normal.
Bone marrow biopsy showed hypercellular marrow with 28% plasma cells. β 2-microglobulin was increased (4.19 mg/L). The findings were further substantiated by capillary electrophoresis performed on serum sample on Minicap, Sebia. IFE was performed using a Hydrasys system (Sebia). Both systems were used according to the manufacturers’ instructions.
The gel picture (Fig. 1) showed two distinct M-bands (M1 and M2 in the beta and gamma globulin region respectively). The densitometric tracing (Fig. 2) showed two distinct M-bands (M1 and M2) as well. This led us to suspect a possibility of biclonality. Also, since one of the M-bands was present in the Beta region, a monoclonal M-protein of IgM or IgA (known for its tendency to aggregate) isotype producing a second M-band due to polymeric form was also suspected [3]. Monoclonal IgA molecules have a tendency to dimerize, and the resulting dimer often has a different mobility than the monomer parent molecule, thereby, yielding two bands on SPEP in some cases of IgA monoclonal gammopathies.
Fig. 1.
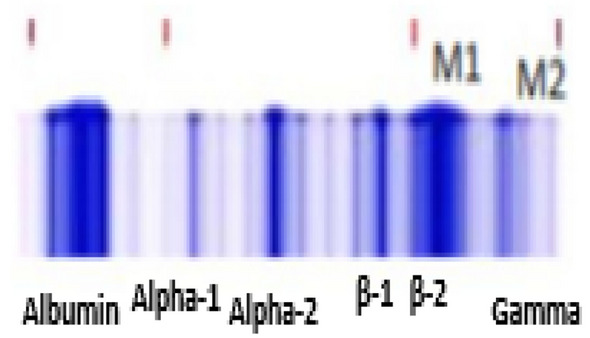
Gel picture showing two bands, M1 in the beta-2 region and M2 in the gamma globulin region
Fig. 2.

Densitometric tracing showing two bands, M1 in the beta-2 region and M2 in the gamma globulin region
To differentiate whether the case is of monoclonal or biclonal gammopathy, two methods are used. In the first method, a repeat SPEP on the sample can be done in reducing conditions by pretreatment of 10 μL sample with 100 μL of β-mercaptoethanol which depolymerizes the multimers and helps in better distinction of double gammopathies. This simple and inexpensive method can be used in facilities where IFE is not available.
In case of true biclonal gammopathy, both the M-bands as seen on SPEP would reappear on the repeat run. In case of monoclonal gammopathy, the sample will present with only one monoclonal component. Thus this simple process would also be sufficient to rule out biclonality.
However we preferred doing IFE as this facility was available in our institute. IFE revealed two bands in IgA lane at different positions along with corresponding two bands in one of the Light Chains lanes i.e. IgA kappa IgA kappa (Fig. 3) [2]. Thus it can be safely concluded that the two M-bands on SPEP originated from the same monoclonal protein, thus ruling out biclonality.
Fig. 3.

Immunofixation electrophoresis showing expansion of IgA-kappa, IgA-kappa chains
Thus both the methods ruled out biclonality.
We further took up additional myeloma work-up which involved serum free light chain levels (Kappa light chain = 359 mg/L (↑), lambda light chain = 4.96 mg/L, free kappa/lambda ratio = 72.379 (↑) The patient was thus diagnosed to have multiple myeloma and started on chemotherapy regimen after due consent.
Apart from helping in differentiating between monoclonal and biclonal gammopathy, IFE is also helpful in understanding if the band in the beta region is due to a monoclonal protein or fibrinogen. The band can be caused by the presence of fibrinogen which can occur due to insufficient clotting of sample. However, this ‘fibrinogen’ band disappears on IFE as it does not bind to any specific antisera used. Thus, in such situations, IFE is helpful in reaching a diagnostic conclusion [2, 3].
Discussion
Multiple myeloma is a cancer of the plasma cells and accounts for 2% of all cancer deaths [3]. Workup of M-protein evaluation begins with SPEP in laboratory settings. M-proteins produced by the IgA variety of Immunoglobulin are seen to produce atypical patterns in SPEP and may make the diagnosis difficult. There might me more anodal migration (close to the β-region) due to lower isoelectric ph. Also, since IgA has quaternary structure, it might lead to sequestration of its light chain epitopes leading to apparent absence of its light chains on IFE. Confounding due to fibrinogen band has also been implicated [2, 3].
In our patient, SPEP revealed two M-band, one in the beta region (M1) and one in the gamma globulin region (M2) thus simulating biclonal gammopathy. However, on IFE we found the heavy chain to be of IgA isotype. This has certain clinical relevance. First of all, IgA paraproteins tend to aggregate and form polymers [3] and hence the two M-bands could be attributed to polymeric forms of a single M-protein.
Secondly, patients with more highly polymerized IgA are more likely to develop the hyperviscosity syndrome and may need additional medications and changes in management protocol [6].
Also, thirdly, it has been seen that polymeric IgA may lead to overestimation of serum calcium levels or underestimation of Hb levels. This apparent increase in calcium is mediated by calcium binding to paraprotein secreted by multiple myeloma cells. This might lead the clinician to make incorrect diagnosis and hence formulating wrong or unnecessary treatment [6, 7]. However it needs to be evaluated if these instances of hypercalcemia are generic to all myelomas or specific to biclonal gammopathies.
The multiple bands on SPEP when the monoclonal protein is IgA may also be attributed to its difference in mobility of the polymers of IgA than the parent monomeric M-protein and hence two M-bands are seen.
Also, SPEP after pretreatment with reducing agents (such as β-mercaptoethanol and dithiothreitol) can prove to be a cost-effective method to distinguish true biclonality from polymeric forms [3]. β-Mercaptoethanol is a reductant that depolymerizes IgA polymers by disrupting disulfide bonds. Multiple bands from IgA polymers are reduced to a single M-spike thus explaining monoclonality. However, in true biclonal gammopathies, the pretreatment will not lead to breakage of the disulphide bonds and hence both the bands will remain intact.
Acknowledgements
We acknowledge the contribution of our technical team led by Miss Kamini V. and Mr. Bikram Singh for their invaluable support in keeping the instrument in good running condition.
Author’s Contribution
Dr. P. Jain was responsible for collection of the case and formulating the write-up. Dr. R. Choudhary and Dr. A.K. Harith contributed with critical review of the article. Dr. C. Yadav was responsible for proof reading and formatting the images.
Funding
Not applicable.
Compliance with Ethical Standards
Conflict of interest
There are no conflict of interest.
Patient Consent
Patient consent has been taken for sharing the image with the journal while concealing the identity.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Nair B, Waheed S, Szymonifka J, Shaughnessy JD, Crowley J, Barlogie B. Immunoglobulin isotypes in multiple myeloma: laboratory correlates and prognostic implications in total therapy protocols. Br J Haematol. 2009;145(1):134. doi: 10.1111/j.1365-2141.2008.07547.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Srinivasan VK, Bhagat P, Bansal F, Chhabra S. Occurrence of double monoclonal bands on protein electrophoresis: an unusual finding. Indian J Hematol Blood Transfus. 2016;32(1):84–88. doi: 10.1007/s12288-015-0622-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bora K, Das U, Barman B, Ruram AA. Monoclonal gammopathy with double M-bands: an atypical presentation on serum protein electrophoresis simulating biclonal gammopathy. Indian J Pathol Microbiol. 2017;60(4):590. doi: 10.4103/IJPM.IJPM_311_17. [DOI] [PubMed] [Google Scholar]
- 4.Guastafierro S, Ferrara MG, Sica A, Parascandola RR, Santangelo S, Falcone U. Serum double monoclonal components and hematological malignancies: only a casual association? Review of 34 cases. Leuk Res. 2012;36(10):74–77. doi: 10.1016/j.leukres.2012.05.008. [DOI] [PubMed] [Google Scholar]
- 5.García P, Enciso-Alvarez K, Diaz F, Vargas JA, Moraru M, Yebra M. Biclonal gammopathies: retrospective study of 47 patients. Rev Clín Esp (Engl Ed) 2015;215(1):18–24. doi: 10.1016/j.rce.2014.07.003. [DOI] [PubMed] [Google Scholar]
- 6.Roberts WL, Fontenot JD, Lehman CM. Overestimation of hemoglobin in a patient with an IgA-κ monoclonal gammopathy. Arch Pathol Lab Med. 2000;124(4):16–18. doi: 10.5858/2000-124-0616-OOHIAP. [DOI] [PubMed] [Google Scholar]
- 7.Pearce CJ, Hine TJ, Peek K. Hypercalcaemia due to calcium binding by a polymeric IgA x-paraprotein. Ann Clin Biochem. 1991;28(3):29–34. doi: 10.1177/000456329102800305. [DOI] [PubMed] [Google Scholar]