

Abstract
Background
In patients under general anesthesia, the laryngeal mask airway (LMA) is a valuable alternative to endotracheal intubation to maintain the airway. In this study, we compared the efficacy of LMA with an endotracheal tube (ETT) in plastic and reconstructive surgeries over 2 h on thorax and abdomen under general anesthesia in Hazrat Fatemeh Hospital in Tehran, Iran, in 2020.
Methods
This randomized clinical trial was performed on a sample size of 80, randomly assigned to two groups. The main variables included the ease of placement, recurrent carbon dioxide content, arterial oxygen saturation, and laryngeal and tracheal spasm. In addition, the sub-variables entailed the mean duration of anesthesia, nausea and vomiting, sore throat, and abdominal distension. The obtained data were analyzed by the SPSS software version 25.
Results
In the present study, 76 patients were female. Mean age, recurrent carbon dioxide, arterial oxygen saturation, laryngeal and tracheal spasm, the mean duration of anesthesia, nausea and vomiting, sore throat, and abdominal distension were not significantly different between the two groups.
Conclusions
The results of this study showed that the classic laryngeal mask could be used as a means of airway control in general anesthesia for long-term surgeries of more than 2 h.
Keywords: Anesthesia, Endotracheal Tube, Laryngeal Mask Airway
1. Background
In patients under general anesthesia, laryngeal mask airway (LMA) is a useful substitute for intubation to maintain the airway (1-3). It can be placed without seeing the nasopharyngeal environment and under low pressure around the laryngeal entrance, allowing ventilation with positive pressure (4, 5). This laryngeal mask method was designed by Dr. Brain in 1981 and has been commercially used since 1988 (3-5). The advantages of LMA compared to tracheal intubation are no tracheal injury during tube installation and removal, less airway stimulation, less invasion of the airway tissue, easier installation, and efficient establishment (6-9). Therefore, in adults, it is recommended to use LMA as a substitute for tracheal intubation, especially in patients with a history of intubation, the possibility of difficult intubation diagnosed by an anesthesiologist, and patients whose intubation has failed and ventilation can be performed with a mask (10-12).
Some studies reported hemodynamic alterations and recovery time in the LMA group during general anesthesia were similar to those in the tracheal intubation group (13-15). One of the major problems with plastic and reconstructive surgeries over 2 h is a long-term airway control with a tracheal tube or laryngeal mask, which may cause adverse effects on the airway, including sore throat, ischemia, or damage to the vocal cords, and management decisions can be important and helpful. Therefore, if the patient is nil per os (NPO), the classical LMA can be an appropriate solution (16, 17). Furthermore, in short surgeries, the use of classical LMA with narcotics, midazolam, and propofol without muscle relaxants and with the help of inhaled gasses allows reducing the complications of anesthesia and recovery time at the end of the operation (18, 19).
2. Objectives
We decided to evaluate the effectiveness of classical LMA in comparison with an endotracheal tube (ETT) in plastic and reconstructive surgeries over 2 h on thorax and abdomen under general anesthesia in Hazrat Fatemeh Hospital, Tehran, Iran.
3. Methods
3.1. Study Design
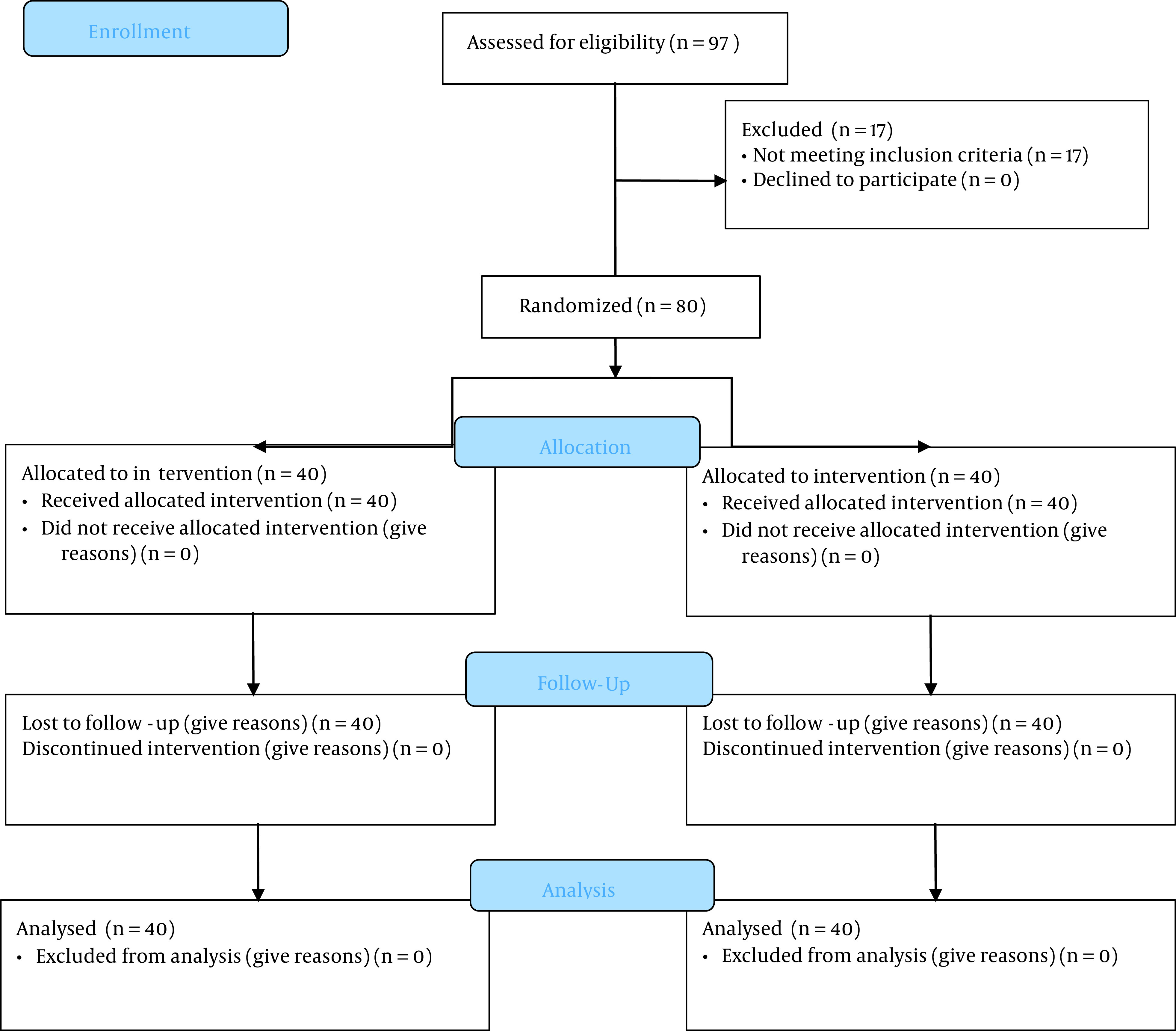
This randomized clinical trial was conducted by a simple randomization method in which a code is given to each patient using a computer-generated random numbers table (MedCalc version 16). Participants were randomly assigned to two groups of LMA and ETT (1:1). This study was performed on 80 patients undergoing thoracic and abdominal surgery under general anesthesia who were referred to Hazrat Fatemeh Hospital affiliated to Iran University of Medical Sciences in Tehran during March 2020-September 2020 (Figure 1). The sample size was calculated to be 40 for each group using a web-based formula considering α = 0.05, 1-β = 0.9, and effect size = 0.71 (12). The inclusion criteria were ASA 1 or 2 based on the physical status classification system and being in the age range of 25 - 60 years. The exclusion criteria entailed being non-NPO, body mass index (BMI) above 35, Latex sensitivity, and history of colds in the last 10 days. By random selection, the participants were assigned to two treatment groups, namely laryngeal mask and endotracheal tube. All patients received the same medication for general anesthesia.
Figure 1. Consort flow diagram.
3.2. General Anesthesia
General anesthesia was the same in both groups. For premedication, 0.2 mg/kg of midazolam plus 3 μg/kg fentanil was used. For induction, 2.5 mg/kg of propofol and 0.5 mg/kg of atracurium were administered intravenously. In addition, 10 μg/kg/min atracurium and 1 μg/kg/min remifentanil were used for the maintenance of GA. After completing the surgery, 0.04 mg/kg neostigmine plus 0.02 mg/kg atropine was applied to reverse the effects of anesthesia. Both groups were studied for variables, such as age, gender, Mallampati score, and BMI. The main variables included the ease of placement, EtCO2, arterial oxygen saturation, and laryngeal and tracheal spasm. The sub-variables encompassed the mean duration of anesthesia, nausea and vomiting, sore throat, and abdominal distension.
3.3. Procedures
In the first group of LMA, the appropriate size is 3, 4, or 5 according to the recommendation of the manufacturer with standard placement (manufactured by IranFormis). In the second group, ETTs were 7 or 7.5 for female patients and 7.5 or 8 for male patients (manufactured by TebTolid). Intracuff pressure of LMA and ETT cuff pressure was 60 cm H2O and 25 cm H2O, respectively. Mechanical ventilation was at a tidal volume of 8 ml/kg and adjusted respiratory rate to maintain an EtCO2 concentration of 35 - 45 mmHg.
3.4. Ethical Considerations
The protocol of this research was approved by the Ethics Committee of Iran University of Medical Sciences (IR.IUMS.FMD.REC.1398.539) and the Iranian Registry of Clinical Trials (IRCT20110513006465N2). Moreover, informed consent was taken from all participants.
3.5. Statistical Analysis
The obtained data were analyzed by the SPSS statistical software version 25. Quantitative findings were reported as mean and standard deviation, and qualitative findings as frequency. Furthermore, independent t-test, Mann-Whitney, chi-square, and Fisher’s exact test were used in the study. P-value < 0.05 was considered statistically significant.
4. Results
Overall, 80 patients were compared into two groups, and 76 participants were female. The age of the LMA group and EET Group was 36.33 ± 12.82 and 34.58 ± 5.92 years, respectively. A comparison of the characteristics of participants in the two groups is shown in Table 1. The results of the chi-square test demonstrated no statistically significant difference between spasms in the cases in the two groups at the 95% confidence level. Our findings revealed that 4 out of 40 LMA patients (10%) and nine subjects in the ETT group (22.5%) had postoperative nausea and vomiting. Moreover, the chi-square test indicated that vomiting and nausea were not significantly different between the two groups in the 95% confidence level. According to the chi-square test, there was no statistically significant difference between the sore throat of patients in the two groups at the 95% confidence level. We observed that five subjects in the LMA group (12.5%) and 12 patients in the ETT group (30%) had a postoperative sore throat. Moreover, the chi-square test showed no statistically significant difference between the abdominal distension of patients in the two groups in the 95% confidence level.
Table 1. Comparison of the Characteristics of Participants Between the Groups LMA and ETT a.
| Variables | Intervention | Total | P-Value | |
|---|---|---|---|---|
| LMA | ETT | |||
| Gender | 0.041 | |||
| Female | 36 (90) | 40 (100) | 76 (95) | |
| Male | 4 (10) | 0 (40) | 4 (5) | |
| Spasm | 1 | |||
| Yes | 2 (5) | 1 (2.5) | 3 (3.8) | |
| No | 38 (95) | 39 (97.5) | 77 (96.3) | |
| Nausea and vomiting | 0.13 | |||
| Yes | 4 (10) | 9 (22.5) | 13 (16.3) | |
| No | 36 (90) | 31 (77.5) | 67 (83.8) | |
| Sore throat | 0.056 | |||
| Yes | 5 (12.5) | 12 (30) | 17 (21.3) | |
| No | 35 (87.5) | 28 (70) | 63 (78.8) | |
| Abdominal distension | 0.288 | |||
| Yes | 6 (15) | 3 (7.5) | 9 (11.3) | |
| No | 34 (85) | 37 (92.5) | 71 (88.8) | |
a Values are expressed as No. (%).
The t-test showed that the mean age difference between the two groups was not statistically significant at a 95% confidence level. The results of the independent samples t-test revealed that the mean arterial oxygen saturation was not significantly different between the two groups at the 95% confidence level. We found that the mean BMI of patients did not have a significant difference between the two groups at a 95% confidence level. Descriptive statistics and the comparison of age, O2 saturation, and BMI between the two groups are presented in Table 2.
Table 2. Descriptive Statistics and the Comparison of Age, O2 Saturation, and BMI Between the Groups LMA and ETT.
| Variables | No. | Mean ± SD | P-Value |
|---|---|---|---|
| Age | 0.436 | ||
| LMA | 40 | 36.33 ± 12.823 | |
| ETT | 40 | 34.58 ± 5.926 | |
| O2 saturation | 0.358 | ||
| LMA | 40 | 99.875 ± 0.4634 | |
| ETT | 40 | 99.95 ± 0.22072 | |
| BMI | 0.102 | ||
| LMA | 40 | 28.48 ± 41.51 | |
| ETT | 40 | 30 ± 4.101 |
Comparison of lung ventilation with the recurrent amount of carbon dioxide index and the duration of anesthesia between the two groups is summarized in Table 3. The results of the Mann-Whitney test showed that the difference between the mean amount of recurrent carbon dioxide of patients in the two groups was not statistically significant at a 95% confidence level. This test revealed that the mean duration of anesthesia was not significantly different between the two groups at a 95% confidence level.
Table 3. Comparison of Lung Ventilation with the Recurrent Amount of Carbon Dioxide Index and Duration of Anesthesia of Patients in the Groups LMA and ETT.
| Variables | No. | Mean | Median | Quartile (1,3) | P-Value |
|---|---|---|---|---|---|
| The amount of recycled carbon dioxide | 0.166 | ||||
| LMA | 40 | 35.43 | 35.5 | 36.7, 34 | |
| ETT | 40 | 34.98 | 34 | 36, 34 | |
| Duration of anesthesia (min) | 0.143 | ||||
| LMA | 40 | 346.88 | 330 | 420, 300 | |
| ETT | 40 | 372.25 | 372 | 420, 334 |
5. Discussion
According to the results of the current study, there is a statistically significant difference between the gender distribution of patients in two groups at a 95% confidence level as the number of females in the ETT group was higher than in the LMA group. Furthermore, the difference between the mean anesthesia duration of the two groups was not significant. However, mean age, BMI, mean Mallampati score, mean carbon dioxide amount, nausea and vomiting, sore throat, abdominal pain, spasm, and arterial oxygen saturation were not significantly different between the two study groups.
Suppiah et al. demonstrated that respiratory complications and hemodynamic changes after extubation were more common in adult patients undergoing endotracheal intubation than in patients who were replaced with LMA at the end of tracheal surgery (5). Akhondi et al. showed that the LMA, as a suitable option in adults, can significantly reduce cough and airway complications following general anesthesia (7).
Our results revealed no significant difference in the Mallampati score of the two research groups. According to an investigation by Bhagwat Lawate et al., ProSealTM laryngeal mask airway (PLMA) can also be an effective airway device in laparoscopic oxygenation and appropriate ventilation surgeries (11). The PLMA is also associated with minimal complications during and after surgery, and pulmonary ventilation is effective despite high airway pressures without gastric distention, aspiration, and relapse (13-15). According to Dumas et al., using LMA to control the airways in patients under general anesthesia for dacryocystorhinostomy surgery was safe and effective, and no aspiration occurred during the application of LMA (13).
Furthermore, in the current study, no significant difference was observed between the two groups of patients in terms of nausea and vomiting. Griffiths et al. indicated that Procyl laryngeal mask, in contrast to the endotracheal tube, does not reduce postoperative pain, nausea, and vomiting. The latter findings were consistent with our results (14). The limitation of our study was that the amount of airway bleeding due to laryngospasm and bronchospasm was not measurable.
5.1. Conclusions
According to the results of this study, LMA is not significantly different from the endotracheal tube in airway management of some specific procedures. It seems that LMA for anesthesia in surgeries over 2 h can be considered an alternative to the endotracheal tube. Further studies are required to determine efficacy of LMA in other types of prolonged surgeries.
Footnotes
Authors' Contribution: Study concept and design: BZ, SASS, and SS; Manuscript drafting: SN, BZ, SASS, and SMHJL; critical revision of the manuscript: SS and SMHJL; Statistical analysis: BZ and SS. All the authors approved the final manuscript version to be published.
Clinical Trial Registration Code: IRCT20110513006465N2. https://en.irct.ir/trial/46380.
Conflict of Interests: The authors certify that they have no affiliations with or involvement in any organization or entity with any financial or non-financial interest in the subject matter or materials discussed in the manuscript.
Data Reproducibility: The dataset presented in the study is available on request from the corresponding author during submission or after its publication.
Ethical Approval: The protocol of this study was approved by the Ethics Committee of Iran University of Medical Sciences (IR.IUMS.FMD.REC.1398.539). Link: ethics.research.ac.ir/EthicsProposalView.php?id=123137
Funding/Support: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent: Informed consent was obtained from all participants.
Contributor Information
Behrooz Zaman, Email: zaman.b@iums.ac.ir.
Samad Noorizad, Email: noorizad.s@iums.ac.ir.
Saeid Safari, Email: drsafari.s@gmail.com.
Seyed Mohamad Hosein Javadi Larijani, Email: abc_291@yahoo.com.
Seyed Alireza Seyed Siamdoust, Email: siamdoust.a@iums.ac.ir.
References
- 1.Gong Y, Xu X, Wang J, Che L, Wang W, Yi J. Laryngeal mask airway reduces incidence of post-operative sore throat after thyroid surgery compared with endotracheal tube: a single-blinded randomized controlled trial. BMC Anesthesiol. 2020;20(1):1–7. doi: 10.1186/s12871-020-0932-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pournajafian A, Alimian M, Rokhtabnak F, Ghodraty M, Mojri M. Success rate of airway devices insertion: laryngeal mask airway versus supraglottic gel device. Anesth Pain Med. 2015;5(2):e22068. doi: 10.5812/aapm.22068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Liu X, Cao H, Tan X, Qiao L, Zhang Q, Shi L. Comparison of the Effect of Laryngeal Mask Airway Versus Endotracheal Tube on Airway Management in Pediatric Patients with Tonsillar Hypertrophy. J Perianesth Nurs. 2021;36(2):142–6. doi: 10.1016/j.jopan.2020.06.020. [DOI] [PubMed] [Google Scholar]
- 4.Park S, Kim GS, Choi DH, Ko JS, Park JB, Son YH, et al. Comparison of Pulmonary Gas Exchange During Kidney Transplantation: Second-Generation Laryngeal Mask Airway vs Endotracheal Tube. Transplant Proc. 2020;52(6):1695–9. doi: 10.1016/j.transproceed.2019.12.057. [DOI] [PubMed] [Google Scholar]
- 5.Suppiah RK, Rajan S, Paul J, Kumar L. Respiratory and hemodynamic outcomes following exchange extubation with laryngeal mask airway as compared to traditional awake extubation. Anesth Essays Res. 2016;10(2):212–7. doi: 10.4103/0259-1162.174469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kotsovolis G, Pliakos I, Panidis S, Gkinas D, Papavramidis T. Comparison Between the Protector Laryngeal Mask Airway and the Endotracheal Tube for Minimally Invasive Thyroid and Parathyroid Surgery. World J Surg. 2019;43(11):2822–8. doi: 10.1007/s00268-019-05122-8. [DOI] [PubMed] [Google Scholar]
- 7.Akhondi M, Sabzevari A, Rahdari A, Imannezhad S. Efficacy of laryngeal airway mask compared with endotracheal tube in reducing coughing following general anesthesia in adults. Rev Clin Med. 2016;3(1):23–7. [Google Scholar]
- 8.Seyed Siamdoust S, Rokhtabnak F, Djalali Motlagh S, Rahimzadeh P, Hassani V, Farnaghizad M. Comparison of the Success Rate of Intubation Between the LMA Fastrach and AirQ-ILA Methods in Patients Undergoing Elective Surgery During General Anaesthesia. Anesth Pain Med. 2018;8(4):e63424. doi: 10.5812/aapm.63424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kim D, Park S, Kim JM, Choi GS, Kim GS. Second generation laryngeal mask airway during laparoscopic living liver donor hepatectomy: a randomized controlled trial. Sci Rep. 2021;11(1):1–7. doi: 10.1038/s41598-021-83173-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hegde HV, Bandi J, Mudakanagoudar MS, Honnannavar KA. Evaluation of performance of Streamlined Liner of the Pharynx Airway, Laryngeal Mask Airway-ProSeal and endotracheal tube in prone position: A prospective, randomised study. Indian J Anaesth. 2018;62(3):173–81. doi: 10.4103/ija.IJA_691_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bhagwat Lawate S, M Keniya V, S Swami S. Evaluation of the efficacy of proseal LMA versus endotracheal intubation for laparoscopic surgeries. Indian J Clin Anaesth. 2020;7(2):285–9. doi: 10.18231/j.ijca.2020.051. [DOI] [Google Scholar]
- 12.Karaaslan E, Akbas S, Ozkan AS, Colak C, Begec Z. A comparison of laryngeal mask airway-supreme and endotracheal tube use with respect to airway protection in patients undergoing septoplasty: a randomized, single-blind, controlled clinical trial. BMC Anesthesiol. 2021;21(1):5. doi: 10.1186/s12871-020-01222-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dumas GA, Bryant AS, Ibey J, Long JA, Vicinanzo MG, Boyd GL. Safety Comparison of Laryngeal Mask Use With Endotracheal Intubation in Patients Undergoing Dacryocystorhinostomy Surgery. Ophthalmic Plast Reconstr Surg. 2018;34(4):324–8. doi: 10.1097/IOP.0000000000000969. [DOI] [PubMed] [Google Scholar]
- 14.Griffiths B, Lee G, Durward A. Critical airway obstruction in apparently asymptomatic neonates. Pediatric Pulmonology. 2016;52(4) doi: 10.1002/ppul.23564. [DOI] [PubMed] [Google Scholar]
- 15.Safari S, Zali A, Pezeshgi P, Bastanhagh E, Jahangirifard A, Akhlaghdoust M. Neuroprotective strategies in the perioperative period: A systematic review. J Cell Mol Anesth. 2021;6(1):50–65. [Google Scholar]
- 16.Sanatkar M, Goudarzi M, Ebrahim Soltani A. The Comparison of Hemodynamic Responses Following Laryngeal Mask Airway Insertion Versus Tracheal Intubation in Hypertensive Patients Scheduled for Elective Ophthalmic Surgery Under General Anesthesia. Acta Medica Iranica. 2019 doi: 10.18502/acta.v57i5.1863. [DOI] [Google Scholar]
- 17.Zuercher M, Casso G, Krugel V, Potie A, Barry MP, Schoettker P. Tracheal intubation using intubating laryngeal tube iLTS-D and LMA Fastrach in 99 adult patients: A prospective multicentric randomised non-inferiority study. J Clin Anesth. 2022;78:110671. doi: 10.1016/j.jclinane.2022.110671. [DOI] [PubMed] [Google Scholar]
- 18.Naguib TM, Ahmed SA. Evaluation of Flexible Laryngeal Mask Airway((R)) in Tongue Trauma Repair: A Randomized Trial. Anesth Pain Med. 2019;9(4):e92929. doi: 10.5812/aapm.92929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kang SH, Park M. Comparison of early postoperative recovery between laryngeal mask airway and endotracheal tube in laparoscopic cholecystectomy: A randomized trial. Medicine (Baltimore). 2019;98(25):e16022. doi: 10.1097/MD.0000000000016022. [DOI] [PMC free article] [PubMed] [Google Scholar]