

Abstract
Background
Coronary artery disease (CAD) is the single most common cause of death worldwide. Recent technological developments with coronary cardiovascular magnetic resonance angiography (CCMRA) allow high-resolution free-breathing imaging of the coronary arteries at submillimeter resolution without contrast in a predictable scan time of ~ 10 min. The objective of this study was to determine the diagnostic accuracy of high-resolution CCMRA for CAD detection against the gold standard of invasive coronary angiography (ICA).
Methods
Forty-five patients (15 female, 62 ± 10 years) with suspected CAD underwent sub-millimeter-resolution (0.6 mm3) non-contrast CCMRA at 1.5T in this prospective clinical study from 2019–2020. Prior to CCMR, patients were given an intravenous beta blockers to optimize heart rate control and sublingual glyceryl trinitrate to promote coronary vasodilation. Obstructive CAD was defined by lesions with ≥ 50% stenosis by quantitative coronary angiography on ICA.
Results
The mean duration of image acquisition was 10.4 ± 2.1 min. On a per patient analysis, the sensitivity, specificity, positive predictive value and negative predictive value (95% confidence intervals) were 95% (75–100), 54% (36–71), 60% (42–75) and 93% (70–100), respectively. On a per vessel analysis the sensitivity, specificity, positive predictive value and negative predictive value (95% confidence intervals) were 80% (63–91), 83% (77–88), 49% (36–63) and 95% (90–98), respectively.
Conclusion
As an important step towards clinical translation, we demonstrated a good diagnostic accuracy for CAD detection using high-resolution CCMRA, with high sensitivity and negative predictive value. The positive predictive value is moderate, and combination with CMR stress perfusion may improve the diagnostic accuracy. Future multicenter evaluation is now required.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12968-022-00858-0.
Keywords: Coronary imaging, Cardiovascular magnetic resonance angiography, Coronary artery disease
Introduction
Coronary artery disease (CAD) remains the single most common cause of death worldwide. Imaging can be used to assess CAD, which has gained increasing importance given the low yield of CAD identification during routine invasive coronary angiography (ICA) [1]. Coronary computed tomography angiography (CCTA) is the non-invasive reference standard for assessment of anatomical CAD, by means of excellent spatial and temporal resolution that enables sharp delineation of the coronary arteries. The vast diagnostic and prognostic evidence of CCTA have seen it mature into clinical guidelines for routine assessment of CAD [2, 3].
Coronary cardiovascular magnetic resonance angiography (CCMRA) is an attractive alternative to CCTA derive anatomical detail of the coronary arteries [4], which may be advantageous in selected patients as it does not require administration of iodinated contrast or use of ionizing radiation. Furthermore, CMRA may allow simultaneous soft tissue characterization and does not suffer from blooming artefact in heavily diseased coronary arteries, which can make luminal assessment challenging in patients with advanced atheroma [5]. Traditionally, routine implementation of CCMRA into clinical practice has been hampered by long and unpredictable acquisition times, suboptimal spatial resolution and significant patient motion which may degrade image quality. Recently developed methods have been developed to achieve submillimeter resolution CCMRA within a short timeframe with advanced motion correction of non-rigid respiratory-induced motion of the heart and 100% respiratory scan efficiency, which may thereby facilitate implementation into a routine clinical workflow [6, 7].
More recently, this technique shows good diagnostic accuracy against CCTA [8], although the prevalence of CAD was relatively low. Thus, the objective of this study was to prospectively determine the diagnostic accuracy of CCMRA against the gold standard of ICA in patients with suspected CAD.
Methods
Study population
consecutive patients with suspected CAD scheduled for ICA as part of routine clinical care were recruited to this prospective single center study between 2019—2020. Patients were recruited either before (n = 24) or after (n = 21) ICA. For the latter, patients were only included if no revascularization was undertaken in the interval. Exclusion criteria were contraindication to CMR, previous coronary artery bypass graft (CABG) surgery, previous coronary stents, atrial fibrillation or unstable angina. The study was approved by the National Research Ethics Service (15/NW/0778) and written informed consent was obtained from all participants.
CMR protocol
CMR scans were performed on a 1.5 T CMR scanner (MAGNETOM Aera, Siemens Healthineers, Erlangen, Germany) with a dedicated 32-channel spine coil and an 18-channel body coil.
Patient preparation
In order to promote coronary vasodilatation and control heart rate, patients were given sublingual 800 mcg glyceryl trinitrate and intravenous metoprolol (Betaloc ®, AstraZeneca, United Kingdom), titrated in 5 mg aliquots to target a heart rate of 60 bpm.
Image acquisition
A multi-slice survey was performed in the axial, coronal and sagittal planes. A free-breathing 4 chamber cine was acquired using a balanced steady state free precession (bSSFP) sequence, to ascertain the optimal time period during which there was the least cardiac motion, typically the diastolic phase of the cardiac cycle. This acquisition was performed free-breathing to mimic the same conditions of the free-breathing CCMRA acquisition, since breath holds during image acquisition have been shown to alter heart rate [9]. Typical parameters for the cine acquisition included: echo time 1.16 ms, repetition time 2.32 ms, flip angle 50°, voxel size 1.8 × 1.8× 6 mm, segmented acquisition, retrospective gating and 25 phases per cardiac cycle.
The CCMRA acquisition used an electrocardiogram (ECG)-triggered undersampled (threefold acceleration factor) free-breathing 3D whole-heart, bSSFP sequence with a 3D variable density spiral-like Cartesian trajectory with golden-angle rotation, as previously described [7]. Typical parameters included: echo time 1.6 ms, repetition time 3.7 ms, flip angle 90°, bandwidth per pixel 890 Hz and field of view 320 × 320 × 86–115 mm. A low-resolution 2D image-navigator (iNAV) preceded each spiral-like interleave which allows for 100% respiratory scan efficiency, predictable scan time and 2D translational motion correction of the heart on a beat-to-beat basis [10]. A spectrally selective spectral presaturation with inversion recovery (SPIR) fat saturation pulse with a constant flip angle of 130° was used to improve coronary delineation and minimize fat-related artefacts. An adiabatic T2 preparation module (40 ms) was used at each heartbeat in order to enhance the contrast between blood and cardiac muscle, and thereby avoid extracellular contrast agents. The reconstructed voxel size was 0.6 mm3 (acquired isotropic resolution of 0.9 mm3). Acquisition times were recorded.
Motion corrected image reconstruction
This consisted of three main steps as previously described [8], which involves beat-to-beat respiratory binning and intra-bin translational motion correction using 2D iNAV [10], bin-to-bin 3D non-rigid motion correction [11] and 3D patch-based low-rank reconstruction [7].
Image analysis
CCMRA images were analyzed after 3D multiplanar reformatting using Osirix (Pixmeo SARL, Bernex, Switzerland) by two expert readers in both CMR and CCTA with greater than 5 years of experience (PGM and MSN). The presence and degree of CAD was determined based on a visual analysis of DICOM images using a nine segment coronary segmentation model [12]. Analysis was performed on a per-patient level (at least one coronary artery with stenosis ≥ 50%) and per-vessel level. The process was repeated in 10 random cases, six months later to assess observer variation.
Image quality was graded on a per-patient and per-vessel analysis on a 4-point scale (1 = poor, 2 = average, 3 = good and 4 = excellent). The diagnostic quality was determined for each segment (0 = non diagnostic, 1 = diagnostic).
Coronary angiography
Patients underwent ICA at St Thomas’ Hospital, London. Quantitative coronary angiography (QCA) was performed retrospectively on x-ray coronary angiography images offline (Medcon Ltd., Tel Aviv, Israel) by an experienced observer with more than 5 years of experience in coronary angiography. Obstructive CAD was defined by a stenosis in a major artery of ≥ 50% on QCA.
Statistical analyses
Statistical analyses were performed using GraphPad Prism 8 software (version 8.4.1, GraphPad Software, San Diego, California, USA). Continuous variables were expressed as mean ± standard deviation or median and interquartile range according to the distribution. Normality distribution was assessed histograms and using Shapiro-Wilks test. Categorical variables are expressed as frequency (%). On a patient level, CAD was defined by the presence of at least one coronary artery with a lesion of ≥ 50% stenosis. On per territory basis, CAD was defined by presence of a vessel with at least one with stenosis of ≥ 50%. Diagnostic accuracies were calculated for sensitivity, specificity, positive predictive value and negative predictive value and the 95% confidence intervals were computed as previously described [13, 14]. Observer agreement was assessed with Cohen’s Kappa coefficient for categorical data. Two tailed values of p < 0.05 were considered statistically significant.
Results
Two patients could not complete the scan due to claustrophobia, and one scan was excluded due to the presence of an intracoronary cardiac stent. Thus, the final analysis was composed of 45 patients. The prevalence of obstructive CAD was 42%. Median time interval between CCMRA and ICA was 11 (interquartile range 3-35) days. Mean duration of CCMRA imaging was 10.4 ± 2.1 min with 100% respiratory scan efficiency. Baseline patient demographics and cardiovascular risk factors are shown in Table 1 and distribution of CAD is shown in Table 2.
Table 1.
Patient demographics and cardiovascular risk factors (n = 45)
| Demographics | n=45 |
| Age (years) | 62 ± 10 |
| Gender female | 15F (33%) |
| Height (m) | 1.71 ± 0.10 |
| Weight (kg) | 90 ± 19 |
| Body mass index (kg/m2) | 31 ± 6 |
| Cardiovascular risk factors | |
| Hypertension | 35 (78%) |
| Hypercholesterolemia | 31 (69%) |
| Diabetes mellitus | 15 (33%) |
| Smoking history | 17 (38%) |
| Family history of coronary artery disease | 21 (47%) |
| Previous myocardial infarction | 5 (11%) |
| Hemodynamic data | |
| Heart rate during CMRA scan (beats per minute) | 61 ± 8 |
| Resting systolic blood pressure (mmHg) | 126 ± 16 |
| Resting diastolic blood pressure (mmHg) | 73 ± 11 |
Data presented as n (%) and as mean ± standard deviation
Table 2.
Distribution of disease as defined by invasive coronary angiography
| Vessel | n (%) |
|---|---|
| LAD | 13 (29) |
| LCx | 9 (20) |
| RCA | 7 (16) |
| LM | 1 (2) |
| Distribution of disease | |
| Single vessel | 11 (24) |
| Two vessel | 6 (13) |
| Three vessel | 2 (4) |
Obstructive lesions were defined ≥ 50% stenosis on quantitative coronary angiography. LAD left anterior descending coronary artery, LCx left circumflex coronary artery, LM Left main coronary artery, RCA right coronary artery
CMRA image quality
On a per-patient analysis, median score for CCMRA image quality was 3 (interquartile range 2–3). On a per-vessel analysis, median image quality score for the left anterior descending artery (LAD): 3 (interquartile range 2–3), left circumflex (LCx): 3 (interquartile range 2–4) and right coronary artery (RCA): 3 (interquartile range 2–4). On a per segment analysis, diagnostic image quality was achieved in 100% of left main (LM) segment, 92% of LAD segments, 91% of LCx and 93% of RCA segments. Diagnostic image quality was achieved in 98% of proximal, 92% of mid and 87% of distal segments.
Hemodynamic data
Mean dose of intravenous metoprolol administered was 12 ± 6 mg. Mean heart rate during image acquisition was 61 ± 8 beats per minute. Resting systolic blood pressure and diastolic blood pressure for patients were 126 ± 16 and 73 ± 11 mmHg, respectively.
Diagnostic accuracy
On a per-patient analysis, the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) (95% confidence intervals) were 95% (75–100), 54% (36–71), 60% (42–75) and 93% (70–100), respectively.
On a per-vessel analysis the sensitivity, specificity, PPV and NPV (95% confidence intervals) were 80% (63–91), 83% (77–88), 49% (36–63) and 95% (90–98), respectively.
There was a good interobserver agreement from the two reporters (κ = 0.74, p = 0.02).
The full breakdown of the diagnostic accuracies are presented in Table 3. Typical case examples are shown in Figs. 1, 2, 3 and 4 and Additional file 1: Videos S1, Additional file 2: Videos S2 and Additional file 3: Videos S3.
Table 3.
Diagnostic accuracy of high-resolution coronary cardiovascular magnetic resonance angiography (CCMRA) for the detection of obstructive coronary artery disease defined by invasive coronary angiography
| Sensitivity (%) | Specificity (%) | Positive Predictive Value (%) | Negative Predictive Value (%) | |
|---|---|---|---|---|
| Patient level | 95 (75–100) | 54 (36–71) | 60 (42–75) | 93 (70–100) |
| Territory level | 80 (63–91) | 83 (77–88) | 49 (36–63) | 95 (90–98) |
| LAD | 92 (67–100) | 69 (51–82) | 55 (35–73) | 96 (79–100) |
| LCx | 67 (35–88) | 81 (65–90) | 46 (23–71) | 91 (76–97) |
| RCA | 86 (49–100) | 79 (64–89) | 43 (21–67) | 97 (84–100) |
Sensitivity, specificity, positive predictive value and negative predictive value are in %. 95% confidence intervals in brackets
Fig. 1.

3D curved multi-planar reformats of a coronary cardiovascular magnetic resonance angiography (CCMRA) in a patient with chest pain and a history of hypertension, hypercholesterolemia and a family history of coronary artery disease. There is no significant disease in the left anterior descending coronary artery (LAD) A, B or right coronary artery (RCA) (C, D). However, there is an occluded left circumflex artery coronary artery (LCx), red arrows (E, F). These findings were confirmed during invasive coronary angiography (G–I, Additional file 1: Video S1)
Fig. 2.
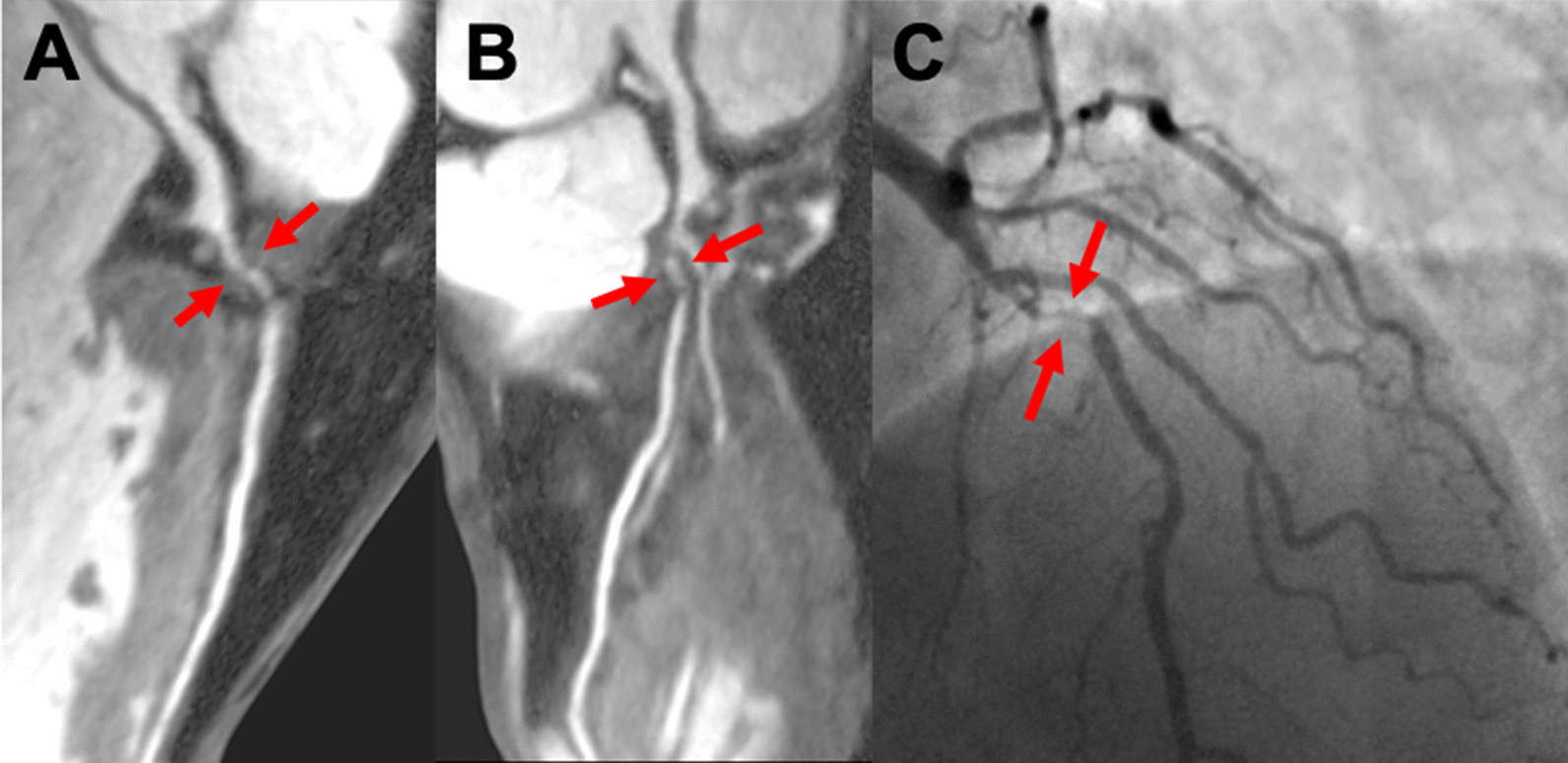
3D curved multi-planar reformat of a CCMRA in a male patient with exertional chest pain with a history of hypertension. There is an obstructive lesion (> 50%) in the LAD (Panel A and B, red arrows). These findings were confirmed during invasive coronary angiography (C and Additional file 2: Video S2)
Fig. 3.
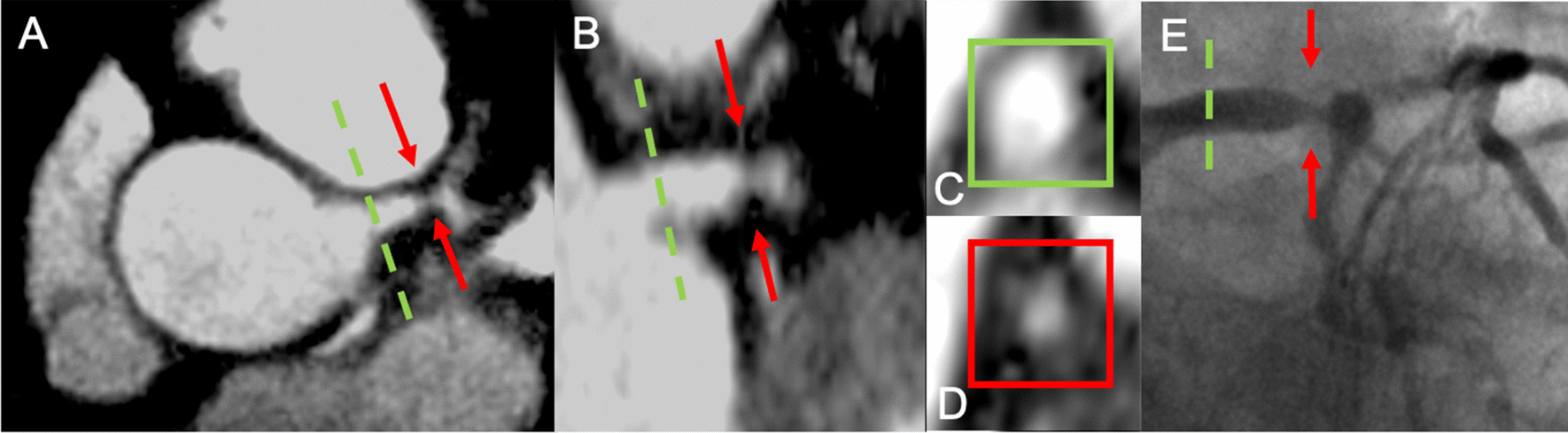
3D multi-planar reformat of a CCMRA in a patient with exertional chest pain on a background of hypertension and type 2 diabetes mellitus. Orthogonal views in Panel A and B, cross section views in Panel C and D. There is no significant disease in the proximal LM (green dashed line), but there is greater than 50% stenosis in the distal left main coronary artery (LM) (red arrow). These findings were confirmed during invasive coronary angiography (Panel E and Additional file 3: Video S3)
Fig. 4.

3D curved multi-planar reformats of a CCMRA in a patient investigated for suspected chest pain with no cardiovascular risk factors showed no obstructive disease. Large dominant RCA (A, B). LAD (C, D). Small non dominant LCx (E, F). These findings were confirmed during invasive coronary angiography (G–I and Additonal file 4: Video S4 and Additional file 5: Video S5)
Discussion
Using non-contrast high-resolution CCMRA, we demonstrated a high diagnostic accuracy with high sensitivity and negative predictive value for detection of CAD compared to the invasive reference standard of ICA in a rapid timeframe of ~ 10 min.
In a preceding study [8], compared to reference standard of CCTA, there was a high sensitivity, specificity, PPV, NPV and diagnostic accuracy of 100% (95% CI: 76–100%), 74% (95% CI: 58–85%), 55% (95% CI: 35–73%), 100% (95% CI: 88–100%) and 80% (95% CI: 67–89%) respectively, for the detection of CAD. However, that study was performed in a cohort of patients with a lower risk of and prevalence of CAD, and the comparator was CCTA, rather than the invasive gold standard of ICA [7]. In this current study, we investigated patients with a comparatively higher prevalence of CAD, and we confirmed that this CCMRA technique has a high sensitivity and a high NPV, suggesting a potential role as a rule out test for CAD. The moderate PPV (60% and 49% at the patient and territory level respectively), may be due to a number of reasons. Firstly, the analysis of degree of stenosis was performed by readers in consensus, and despite blinding to the findings from the coronary angiogram, may have led to inadvertent overestimation of degree of stenosis, in order not to miss clinically relevant CAD lesions. Secondly, the intermediate PPV may relate to the inferior spatial resolution of CMRA (reconstructed to 0.6 mm3) compared to ICA (~ 0.2 mm), which may result in an overestimation in the degree of stenosis. Furthermore, we found that the diagnostic performance in the LCx territory was lower, which may be explained by the lower signal-to-noise ratio due to the greater distance from the coils from the LCx. Furthermore, the beat-to-beat anterior–posterior motion is not corrected for in this proposed approach, which may not correct the motion of the LCx in the lateral plane. Thus, future studies should investigate methods that enhance spatial resolution without compromising the total acquisition time, boosting signal to noise in the LCx and further improving motion correction.
The speed of acquisition of CMR clinical scans is highly relevant for clinical workflow, patient comfort and effective healthcare resource utilization. Often, CMR scans are considered as lengthy scans with variable scan times between patients, although technological developments such as parallel imaging, multichannel coils and compressed sensing have allowed more rapid clinical protocols [15–18]. The average time of acquisition of CCMRA in this study was approximately 10 min, which we feel is acceptable for routine integration for clinical workflow. For instance, the CCMRA acquisition could potentially be acquired after gadolinium contrast injection in a predictable scan time, by which time after 10 min, late gadolinium enhancement (LGE) could be acquired, as performed in routine clinical lists which require LGE imaging. The speed of acquisition has been achieved through the development of advanced motion correction frameworks that allow for 100% respiratory scan efficiency in combination with undersampled reconstruction. However, the acquisition time of CCMRA, typically acquired over several hundred heart beats, is still substantially longer in comparison to that of CCTA, which can be acquired in single heartbeat using modern technology. The longer image acquisition time is critically important, as any significant patient related movement cannot be easily corrected for.
CCMRA for the evaluation of CAD has been established over two decades ago [19, 20], and despite initial promise in multicenter evaluation [21], has not become part of routine clinical assessment in CMR. This may in part relate to the long unpredictable acquisition times and respiratory inefficiency from previous techniques. One recent study used compressed sensing to accelerate image acquisition within a rapid timeframe, although in that study, contrast administration was required [22], and did not compare to the invasive reference standard of ICA as we did in this study. More recently, obstructive CAD seen on CCMRA was found to provide incremental prognostic value over traditional risk factors [23]. One important step to clinical translation in our study is the ability to achieve 100% respiratory scan efficiency and high-resolution imaging with predictable scan times (thus not dependent on the specific subject’s breathing pattern). This is made possible by a 3D non-rigid motion corrected reconstruction framework with golden-step variable density spiral-like Cartesian trajectory with good undersampling properties which allows for 100% scan efficiency.
Whilst the focus of this study was to determine the degree of luminal stenosis compared to ICA, there has been much interest into plaque morphology. For example, there are established imaging biomarkers derived from CCTA which indicate adverse clinical outcomes such low attenuation plaque and positive remodeling [24] and perivascular fat [25]. Using computational fluid dynamics, non-invasive assessment of fractional flow reserve can be derived, which has shown to have high diagnostic accuracy and is associated with prognostic outcome data [26, 27]. There are also features that can be derived from CCMRA that indicate adverse clinical outcome, such as with high intensity plaques from T1-weighted images [28]. These features were not investigated as part of this current study, although the ability to determine the presence of vulnerable plaque and hemodynamic significance of lesions are likely to have incremental benefit beyond that of the degree of stenosis, although future studies are required to determine this.
The assessment of CAD is important for patients so that appropriate medical therapy can be initiated, adverse clinical outcomes can be prevented and revascularization considered for relief of angina symptoms [29]. The integration of high-resolution CMRA into a clinical workflow for assessment of CAD is particularly attractive given the multiparametric nature of CMR, which can be used to derive precise measurements of left ventricular function, viability (derived from regional motion wall abnormalities and LGE) and ischemia (derived from dynamic first pass perfusion imaging or dobutamine stress). The integration of anatomy as part of a multiparametric assessment has the potential to provide a complete assessment of CAD to guide clinical decision making and revascularization from a single exam. We feel that this is particularly important for clinical decision makers; whilst a negative stress perfusion scan is associated with a low risk of adverse outcome [30], from a perfusion scan alone, standard CMR does not derive information on coronary plaques and stenosis. Therefore, using standard CMR techniques may otherwise miss the opportunity to initiate preventative medical therapy based on the presence of coronary plaque with statins and alter clinical outcomes, as has been shown with CCTA [31]. Thus, the integration of high-resolution CCMRA may provide incremental diagnostic and prognostic value over standard CMR methods in patients with suspected CAD, and this will be the focus of our future research, which we hope will benefit our patients.
Limitations
Firstly, this study was performed at a single center, using a single vendor at 1.5T field strength. Secondly, our analysis of CCMRA data was performed based on visual analysis rather than automated analysis of degree of stenosis. Nevertheless, the analysis was performed by two expert CMR readers, with good interobserver agreement. Thirdly, we excluded patients with previous CABG or coronary stents, and therefore the diagnostic performance in these patients is unknown, but is likely to be suboptimal due to the susceptibility artefact from stents and surgical clips. Forthly, we did not undertake intracoronary assessment with intravascular ultrasound or optical coherence tomography for the assessment of coronary artery lesions. Finally, we excluded patients with atrial fibrillation, as the variation of R-R interval would likely result in suboptimal image quality given variation in the acquisition period in the cardiac cycle.
Conclusion
We demonstrate a high diagnostic accuracy of high-resolution non-contrast CCMRA within predictable scan time of ~ 10 min for the diagnosis of CAD. Future work is required through large multicenter evaluation for diagnostic accuracy and clinical outcomes in patients with CAD. CCMRA could be considered for routine integration in CMR protocols combined with stress perfusion and viability imaging, and in turn lead to a comprehensive assessment for the workup of patients with suspected CAD .
Supplementary Information
Additional file 1: Video S1. Invasive s-ray coronary angiography confirms occluded proximal left circumflex coronary artery.
Additional file 2: Video S2. Invasive x-ray coronary angiography confirms severe stenosis in mid left anterior descending coronary artery.
Additional file 3: Video S3. Invasive x-ray coronary angiography confirms severe distal left main coronary arterydisease.
Additional file 4: Video S4. Invasive x-ray coronary angiography confirms no significant obstructive disease in the right coronary artery.
Additional file 5: Video S5. Invasive x-ray coronary angiography confirms no significant obstructive disease in the left coronary artery.
Acknowledgements
The authors would like to thank the radiographers that were involved in the acquisition of images and the patients that participated in this study.
Abbreviations
- bSSFP
Balanced steady state free precession
- CABG
Coronary artery bypass graft surgery
- CAD
Coronary artery disease
- CCMRA
Coronary cardiovascular magnetic resonance angiography
- CCTA
Coronary computed tomography angiography
- ECG
Electrocardiography
- ICA
Invasive coronary angiography
- iNAV
Image navigator
- LAD
Left anterior descending coronary artery
- LCx
Left circumflex coronary artery
- LGE
Late gadolinium enhancement
- LM
Left main coronary artery
- NPV
Negative predictive value
- PPV
Positive predictive value
- QCA
Quantitative coronary angiography
- RCA
Right coronary artery
- SPIR
Spectral presaturation with inversion recovery
Author contributions
MSN, AC, RB and CP conceived the idea of this project. MSN, AB, RH, MY ad VV undertook data acquisition and analysis. MR and PG undertook data analysis. MSN drafted the manuscript. All authors read and approved the final manuscript.
Funding
The authors acknowledge financial support from the Department of Health through the National Institute for Health Research (NIHR) comprehensive Biomedical Research Centre award to Guy’s & St Thomas’ NHS Foundation Trust in partnership with King’s College London and King’s College Hospital NHS Foundation Trust and by the NIHR MedTech Co-operative for Cardiovascular Disease at Guy’s and St Thomas’ NHS Foundation Trust. This paper presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant Reference Number PB-PG-0416-20008). The work was also supported by the EPSRC (EP/P001009/1 and EP/P007619/1) and the Wellcome/EPSRC Centre for Medical Engineering [WT 203148/Z/16/Z]. MSN was funded by a NIHR Clinical Lectureship [CL-2019-17-001]. SP is funded by a BHF Chair [CH/16/2/32089]. The views expressed are those of the authors and not necessarily those of the BHF, the DoH, the EPSRC, the NHS, the NIHR, or the Wellcome Trust.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Dr. Debiao Li served as the JCMR Guest Editor for this manuscript. Declarations
Ethics approval and consent to participate
The study was approved by the National Research Ethics Service (15/NW/0778) written informed consent obtained from all patients.
Consent for publication
All participicants in this study provided written informed consent for the use of their data.
Competing interests
Radhouene Neji and Karl Kunze are employees of Siemens Healthcare. The remaining authors have no relevant disclosures.
Footnotes
Dr. Debiao Li served as the JCMR Guest Editor for this manuscript.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Patel MR, Peterson ED, Dai D, Brennan JM, Redberg RF, Anderson HV, et al. Low diagnostic yield of elective coronary angiography. N Engl J Med. 2010;362(10):886–895. doi: 10.1056/NEJMoa0907272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.National Institute for Health and Care Excellence . Chest pain of recent onset. Assessment and diagnosis of recent onset chest pain or discomfort of suspected cardiac origin (update) London: National Institute for Health and Care Excellence; 2016. [PubMed] [Google Scholar]
- 3.Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: the Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC) Eur Heart J. 2019;41(3):407–477. doi: 10.1093/eurheartj/ehz425. [DOI] [PubMed] [Google Scholar]
- 4.Hajhosseiny R, Bustin A, Munoz C, Rashid I, Cruz G, Manning WJ, et al. Coronary magnetic resonance angiography: technical innovations leading us to the promised land? JACC Cardiovasc Imaging. 2020;13(12):2653–2672. doi: 10.1016/j.jcmg.2020.01.006. [DOI] [PubMed] [Google Scholar]
- 5.Dweck MR, Puntman V, Vesey AT, Fayad ZA, Nagel E. MR imaging of coronary arteries and plaques. JACC Cardiovasc Imaging. 2016;9(3):306–316. doi: 10.1016/j.jcmg.2015.12.003. [DOI] [PubMed] [Google Scholar]
- 6.Bustin A, Ginami G, Cruz G, Correia T, Ismail TF, Rashid I, et al. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn Reson Med. 2019;81(1):102–115. doi: 10.1002/mrm.27354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bustin A, Rashid I, Cruz G, Hajhosseiny R, Correia T, Neji R, et al. 3D whole-heart isotropic sub-millimeter resolution coronary magnetic resonance angiography with non-rigid motion-compensated PROST. J Cardiovasc Magn Reson. 2020;22(1):24. doi: 10.1186/s12968-020-00611-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hajhosseiny R, Rashid I, Bustin A, Munoz C, Cruz G, Nazir MS, et al. Clinical comparison of sub-mm high-resolution non-contrast coronary CMR angiography against coronary CT angiography in patients with low-intermediate risk of coronary artery disease: a single center trial. J Cardiovasc Magn Reson. 2021;23(1):57. doi: 10.1186/s12968-021-00758-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zhang J, Fletcher JG, Scott Harmsen W, Araoz PA, Williamson EE, Primak AN, et al. Analysis of heart rate and heart rate variation during cardiac CT examinations. Acad Radiol. 2008;15(1):40–48. doi: 10.1016/j.acra.2007.07.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Henningsson M, Koken P, Stehning C, Razavi R, Prieto C, Botnar RM. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med. 2012;67(2):437–445. doi: 10.1002/mrm.23027. [DOI] [PubMed] [Google Scholar]
- 11.Cruz G, Atkinson D, Henningsson M, Botnar RM, Prieto C. Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn Reson Med. 2017;77(5):1894–1908. doi: 10.1002/mrm.26274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Henningsson M, Shome J, Bratis K, Vieira MS, Nagel E, Botnar RM. Diagnostic performance of image navigated coronary CMR angiography in patients with coronary artery disease. J Cardiovasc Magn Reson. 2017;19(1):68. doi: 10.1186/s12968-017-0381-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wilson EB. Probable inference, the law of succession, and statistical inference. J Am Stat Assoc. 1927;22(158):209–212. doi: 10.1080/01621459.1927.10502953. [DOI] [Google Scholar]
- 14.Lawrence DB, Cai TT, Anirban D. Interval estimation for a binomial proportion. Stat Sci. 2001;16(2):101–133. doi: 10.1214/ss/1009213285. [DOI] [Google Scholar]
- 15.Lustig M, Donoho D, Pauly JM. Sparse MRI: the application of compressed sensing for rapid MR imaging. Magn Reson Med. 2007;58(6):1182–1195. doi: 10.1002/mrm.21391. [DOI] [PubMed] [Google Scholar]
- 16.Yang Q, Li K, Liu X, Du X, Bi X, Huang F, et al. 3.0T whole-heart coronary magnetic resonance angiography performed with 32-channel cardiac coils: a single-center experience. Circ Cardiovasc Imaging. 2012;5(5):573–579. doi: 10.1161/CIRCIMAGING.112.974972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magn Reson Med. 1999;42(5):952–962. doi: 10.1002/(SICI)1522-2594(199911)42:5<952::AID-MRM16>3.0.CO;2-S. [DOI] [PubMed] [Google Scholar]
- 18.Griswold MA, Jakob PM, Heidemann RM, Nittka M, Jellus V, Wang J, et al. Generalized autocalibrating partially parallel acquisitions (GRAPPA) Magn Reson Med. 2002;47(6):1202–1210. doi: 10.1002/mrm.10171. [DOI] [PubMed] [Google Scholar]
- 19.Stuber M, Botnar RM, Fischer SE, Lamerichs R, Smink J, Harvey P, et al. Preliminary report on in vivo coronary MRA at 3 Tesla in humans. Magn Reson Med. 2002;48(3):425–429. doi: 10.1002/mrm.10240. [DOI] [PubMed] [Google Scholar]
- 20.Weber OM, Martin AJ, Higgins CB. Whole-heart steady-state free precession coronary artery magnetic resonance angiography. Magn Reson Med. 2003;50(6):1223–1228. doi: 10.1002/mrm.10653. [DOI] [PubMed] [Google Scholar]
- 21.Kato S, Kitagawa K, Ishida N, Ishida M, Nagata M, Ichikawa Y, et al. Assessment of coronary artery disease using magnetic resonance coronary angiography: a national multicenter trial. J Am Coll Cardiol. 2010;56(12):983–991. doi: 10.1016/j.jacc.2010.01.071. [DOI] [PubMed] [Google Scholar]
- 22.Hirai K, Kido T, Kido T, Ogawa R, Tanabe Y, Nakamura M, et al. Feasibility of contrast-enhanced coronary artery magnetic resonance angiography using compressed sensing. J Cardiovasc Magn Reson. 2020;22(1):15. doi: 10.1186/s12968-020-0601-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Nakamura S, Ishida M, Nakata K, Ichikawa Y, Takase S, Takafuji M, et al. Long-term prognostic value of whole-heart coronary magnetic resonance angiography. J Cardiovasc Magn Reson. 2021;23(1):56. doi: 10.1186/s12968-021-00749-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Williams MC, Moss AJ, Dweck M, Adamson PD, Alam S, Hunter A, et al. Coronary artery plaque characteristics associated with adverse outcomes in the SCOT-HEART study. J Am Coll Cardiol. 2019;73(3):291–301. doi: 10.1016/j.jacc.2018.10.066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Oikonomou EK, Marwan M, Desai MY, Mancio J, Alashi A, Hutt Centeno E, et al. Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): a post-hoc analysis of prospective outcome data. Lancet. 2018;392(10151):929–939. doi: 10.1016/S0140-6736(18)31114-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Taylor CA, Fonte TA, Min JK. Computational fluid dynamics applied to cardiac computed tomography for noninvasive quantification of fractional flow reserve: scientific basis. J Am Coll Cardiol. 2013;61(22):2233–2241. doi: 10.1016/j.jacc.2012.11.083. [DOI] [PubMed] [Google Scholar]
- 27.Nazir MS, Mittal TK, Weir-McCall J, Nieman K, Channon K, Nicol ED. Opportunities and challenges of implementing computed tomography fractional flow reserve into clinical practice. Heart. 2020;106(18):1387–1393. doi: 10.1136/heartjnl-2019-315607. [DOI] [PubMed] [Google Scholar]
- 28.Noguchi T, Kawasaki T, Tanaka A, Yasuda S, Goto Y, Ishihara M, et al. High-intensity signals in coronary plaques on noncontrast T1-weighted magnetic resonance imaging as a novel determinant of coronary events. J Am Coll Cardiol. 2014;63(10):989–999. doi: 10.1016/j.jacc.2013.11.034. [DOI] [PubMed] [Google Scholar]
- 29.Boden WE, O'Rourke RA, Teo KK, Hartigan PM, Maron DJ, Kostuk WJ, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356(15):1503–1516. doi: 10.1056/NEJMoa070829. [DOI] [PubMed] [Google Scholar]
- 30.Lipinski MJ, McVey CM, Berger JS, Kramer CM, Salerno M. Prognostic value of stress cardiac magnetic resonance imaging in patients with known or suspected coronary artery disease: a systematic review and meta-analysis. J Am Coll Cardiol. 2013;62(9):826–838. doi: 10.1016/j.jacc.2013.03.080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Newby DE, Adamson PD, Berry C, Boon NA, Dweck MR, Flather M, et al. Coronary CT Angiography and 5-Year Risk of Myocardial Infarction. N Engl J Med. 2018;379(10):924–933. doi: 10.1056/NEJMoa1805971. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Video S1. Invasive s-ray coronary angiography confirms occluded proximal left circumflex coronary artery.
Additional file 2: Video S2. Invasive x-ray coronary angiography confirms severe stenosis in mid left anterior descending coronary artery.
Additional file 3: Video S3. Invasive x-ray coronary angiography confirms severe distal left main coronary arterydisease.
Additional file 4: Video S4. Invasive x-ray coronary angiography confirms no significant obstructive disease in the right coronary artery.
Additional file 5: Video S5. Invasive x-ray coronary angiography confirms no significant obstructive disease in the left coronary artery.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Dr. Debiao Li served as the JCMR Guest Editor for this manuscript. Declarations