

Abstract
Background and aims
Despite its illegality among adolescents, online gambling is a common practice, which puts their mental health and well-being at serious risk. This systematic review summarises international scientific literature from the last 20 years on problematic online gambling among adolescents (11–21 years old) to determine its prevalence and to analyse related measurement issues.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed and a protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO, IC: CRD42020162932). Five academic databases were consulted, which resulted in an initial sample of 658 papers.
Results
Sixteen studies met the inclusion criteria for this review. All studies were cross-sectional and targeted students from elementary school, secondary school or university. Most followed a convenience sampling procedure. The primary measurement instruments used were the DSM-IV-MR-J and SOGS-RA. Between 0.77% and 57.5% of adolescents present some degree of problematic online gambling (problem, pathological or disordered) depending on the instruments used, the study samples and the timeframe analysed. Between 0.89% and 1% of adolescents exhibited an online gambling disorder.
Discussion and conclusion
There is a great heterogeneity in the methodology of the reviewed studies (samples, measurement instruments, cut-off points and criteria applied). The limited number of studies and the limited generalizability of their results suggest the need for further research and for development of specific instruments to assess different levels of problematic online gambling in representative samples of adolescents based on clinical ‘gold standard’ criteria and more accurate cut-off points.
Keywords: online gambling, adolescents, disorder, pathological, problem, systematic review
Introduction
Gambling is usually defined as the activity or practice of playing a game of chance for money or other stakes and online gambling refers to a range of wagering and gaming activities offered through Internet-enabled devices (Gainsbury, 2015). Many adolescents worldwide are involved in gambling—both online and offline—despite being below the legal gambling age (between 16 and 21 years, depending on the country and type of game) (Emond & Griffiths, 2020). In general, online gambling is less prevalent than offline gambling. However, due to its progressive legalisation and promotion alongside the expansion of technology, online gambling is becoming increasingly popular, especially among young people (Gómez, Feijóo, Braña, Varela, & Rial, 2019; Hollén, Dörner, Griffiths, & Emond, 2020; Molinaro et al., 2018). According to a recent review of international studies, 5–15% of adolescents gamble online and 40–70% gamble offline, with large differences between countries (King, Russell, & Hing, 2020).
Gambling behaviour can be located at different points on a continuum ranging from occasional, recreational, non-problematic or social gambling to at-risk gambling and then to problem, pathological, compulsive or disordered gambling (Floros, 2018). The terms ‘problem’ and ‘pathological’ gambling are often used interchangeably, but the term ‘problem gambling’ describes an intermediate or subclinical form of the disorder (Lorains, Cowlishaw, & Thomas, 2011). ‘Pathological gambling’ was used in the third and fourth editions of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III and DSM-IV) and in the 10th edition of the International Classification of Diseases (ICD-10) to designate an impulse control disorder. In the fifth edition, the DSM-5, this disorder is renamed ‘gambling disorder’ and is considered an addictive disorder which can comprise three levels of severity—mild, moderate and severe—based on the number of criteria (American Psychiatric Association, 2013). In essence, gambling disorder constitutes a behavioural addiction characterised by persistent and recurrent problematic gambling behaviour that leads to clinically significant deterioration or distress, including social functioning problems, financial problems or even comorbidity with mental and physical illnesses (American Psychiatric Association, 2013). This relevant change was based on their similarities with addictive disorders, not only in terms of diagnostic, clinical and neurological variables, but also in their treatment and comorbidities (Petry et al., 2014). For its part, in the 11th revision of the ICD (ICD-11) (World Health Organization, 2018), ‘gambling disorder’ (6C50) also appears and includes the important distinction of the disorder consisting of ‘predominantly online gambling’ (6C50.1). This study employs the term ‘problematic online gambling’ in a broad sense with the aim to comprehend the entire spectrum of problems related to online gambling (problem, pathological and disordered).
Multiple tools have been developed to evaluate and diagnose problematic gambling in adults, such as the South Oaks Gambling Screen (SOGS) (Lesieur & Blume, 1987), the Massachusetts Gambling Screen (MAGS) (Shaffer, LaBrie, Scanlan, & Cummings, 1994), and the Canadian Problem Gambling Index (CPGI) (Ferris & Wynne, 2001). Many of these instruments have been adapted to the adolescent population by modifying items, timeframes or the number of items required to establish a clinical diagnosis. According to a systematic review by King et al. (2020), the most used instruments for the adolescent age group are the DSM-IV-Multiple Response-Juvenile (DSM-IV-MR-J) (Fisher, 2000), the Problem Gambling Severity Index (PGSI) (Ferris & Wynne, 2001) and the South Oaks Gambling Screen–Revised for Adolescents (SOGS-RA) (Winters, Stinchfield, & Fulkerson, 1993). However, in light of the new types of gambling opportunities (i.e. online) the reliability, validity and suitability of the aforementioned instruments must be re-evaluated (Potenza et al., 2019).
While the available scientific literature on problematic online gambling is still limited (Lawn et al., 2020), it highlights how it can lead to significant consequences. For instance, numerous mental health problems, including depression, stress and anxiety (González-Cabrera et al., 2020), as well as drug use (Effertz, Bischof, Rumpf, Meyer, & John, 2018), problematic Internet use (Andrie et al., 2019; Baggio, Gainsbury, Berchtold, & Iglesias, 2016; Gómez et al., 2019) and Internet gaming disorder (Beranuy et al., 2020). Mainly, however, online gambling has been associated with problem and pathological gambling (Lawn et al., 2020). Some authors suggest the greater addictive potential of online gambling over traditional gambling, especially for young problem gamblers (Effertz et al., 2018; Yazdi & Katzian, 2017). In this regard, various studies note that online gamblers are three to eight times more likely to exhibit problematic gambling than those who do not gamble online (Chóliz, Marcos, & Lázaro-Mateo, 2019; Effertz et al., 2018; Griffiths, Wardle, Orford, Sproston, & Erens, 2009; Volberg, McNamara, & Carris, 2018). However, there are discrepancies in the possible explanation of this phenomenon. Some authors attribute the greater addictive potential of online gambling to situational and structural aspects, such as availability, accessibility, immediacy of reinforcement or speed and frequency of gambling (Chóliz, 2016; Griffiths, 2003). In this sense, the Internet offers several “advantages” for the individual compared to offline or land-based gambling such as high accessibility of gambling, even at home or at the workplace, at low costs and with a high level of convenience (Gainsbury, 2015; Griffiths, 2003). The Internet also allows anonymity for those who do not want to be recognized as gamblers, and multi-simultaneous gambling experiences (Effertz et al., 2018). Online gambling could be a largely automated activity that could be conducted in private, at any time and location, using highspeed Internet connections enabling rapid placement of bets and notification of outcomes (Gainsbury, 2015). On the other hand, the marketing recruitment and maintenance strategies developed by gambling operators (e.g. promotions in Social Media), seem to be very effective, especially among problem gamblers (Gainsbury et al., 2016).
However, other authors argue that online gambling is not in itself more problematic, but that other variables are involved. For example, evidence indicates that those who are already problem gamblers are more involved in online gambling (Emond, Griffiths, & Hollén, 2020; Wijesingha, Leatherdale, Turner, & Elton-Marshall, 2017; Yazdi & Katzian, 2017), which may explain the higher prevalence of problem gambling among online gamblers. Also, some studies report lower rates of gambling problems in ‘pure online gamblers’ than in ‘pure offline gamblers’ (e.g. Gainsbury, 2015). In many cases, online gamblers are also involved in other traditional gambling activities (mixed gamblers), which can influence the relationship between online gambling and gambling problems (Baggio et al., 2017). In addition, among online gamblers, there are specific gambling activities more associated with disordered gambling (e.g. online and land-based Electronic Gaming Machines) than others (Gainsbury, Angus, & Blaszczynski, 2019), and high overall gambling engagement is an important predictor of gambling-related harms (Baggio et al., 2017; Gainsbury et al., 2019).
Other key aspects of problem gambling are sex and age variables as risk factors for developing problematic online gambling. Just as it has been observed that adolescents are particularly vulnerable to developing offline gambling problems (American Psychiatric Association, 2013; Caillon, Grall-Bronnec, Bouju, Lagadec, & Vénisse, 2012; Calado, Alexandre, & Griffiths, 2017), they are also vulnerable to developing online gambling problems (Gainsbury, 2015; Hubert & Griffiths, 2018). This general vulnerability can be explained by the developmental characteristics of adolescence, which is a period of particular vulnerability to engage in multiple forms of risky behaviours (Jessor, 1991) and develop addiction problems due to its immature self-regulation capacity, impulsivity, external locus of control and susceptibility to contextual factors (Hollén et al., 2020). Adolescents' online vulnerability could be due to their overall increased use of the Internet for gambling (Chóliz et al., 2019; King et al., 2020) thanks to the fact that they have grown up in a society where gambling is generally accepted, heavily available, and widely promoted through Internet (Volberg, 2010). They may be lured by the pop up gambling advertisements, offers of gifts and free play, tempting easy win messages, thrill of many online games, and visually exciting graphics and photos presented with the games (Derevensky & Gupta, 2007). In addition, adolescents can gamble with a small cost per session, using prepaid debit cards issued more easily and with fewer safeguards than the credit cards, or online intermediaries like PayPal (Floros, Siomos, Fisoun, & Geroukalis, 2013; Wong, 2010). In sum, the accessibility, affordability, convenience and anonymity of internet gambling may serve as a good mean for young people to engage in gambling activities without age verification and parental supervision (Elton-Marshall, Leatherdale, & Turner, 2016). This fact is specially worrying since several studies show that the lower the age of online gambling onset, the higher the probability of developing problematic online gambling and the more severe the psychosocial consequences are (Potenza et al., 2011; Wong, 2010).
Regarding sex differences, the evidence is not as conclusive. Multiple studies suggest that being male is a robust risk factor, especially during adolescence (American Psychiatric Association, 2013; Dowling et al., 2017; Emond et al., 2020). However, recent studies have demonstrated a significant increase in online gambling behaviour among women, as well as changing trends in online gambling problem development (Hollén et al., 2020; McCormack, Shorter, & Griffiths, 2014; Volberg et al., 2018).
The past two decades have seen growing concern and research about online gambling in adolescents (Calado et al., 2017; Griffiths, 2003; Griffiths & Parke, 2010; King et al., 2020), and empirical studies about problematic online gambling have increased substantially. Some reviews have been published that make important contributions to the literature (e.g. Gainsbury, 2015) despite not including the most recent studies or discussing the prevalence of problematic online gambling itself. Therefore, this review aims to systematically synthesise research trends in studies about problematic online gambling in adolescents and answer the following research questions, which were derived from the PICO (Population, Intervention, Comparator and Outcomes) format (Shamseer et al., 2015): (a) How is online gambling prevalence being operationalised?; (b) What instruments are being used to evaluate problematic online gambling in adolescents, including its cut-off points, criteria and characteristics such as if they are they diagnostic instruments, and do they evaluate online and/or traditional gambling?; and (c) What is the prevalence of problematic online gambling in adolescents at different levels of severity (problem, pathological and disordered gambling), and are there significant differences according to sex or age?
Methods
This systematic review adhered to the systematic search protocol recommended in the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-P; Shamseer et al., 2015). To ensure quality, a protocol was designed and registered with the International Prospective Register of Systematic Reviews (PROSPERO, ID: CRD42020162932).
Inclusion criteria
The scope of this review included quantitative studies about problematic online gambling in adolescents aged 11–21 years published in peer-reviewed academic journals in the past two decades (2000–2020). This age range was chosen because it accords with Salmela-Aro's (2011) proposal regarding the stages of adolescence, and 21 is the age before which online gambling is illegal in several countries.
Studies had to meet five inclusion criteria: (C1) evaluates some level of problematic online gambling (problem, pathological or disordered) through psychometric instruments that allow to establish different groups of gamblers; (C2) includes a study sample consisting of adolescents between 11 and 21 years; (C3) is published in either English or Spanish; (C4) is a quantitative empirical study with original data; and (C5) provides results on the prevalence of problematic online gambling.
The following exclusion criteria were also applied: (1) studies that analysed exclusively traditional gambling (‘offline’ or ‘land-based’) or forms not legally recognised as online gambling (loot boxes, simulated gambling, etc.); (2) studies whose samples consisted exclusively of persons over the age of 21; and (3) thesis works, qualitative studies, reports, case studies and theoretical reviews.
Identification of studies
An initial systematic and comprehensive search of the following electronic databases was carried out from February to April 2020 (inclusive): SCOPUS, Web of Science, PubMed, PsycINFO and Google Scholar. Searches included studies published between January 1, 2000 and April 30, 2020, which were found using the following Medical Subject Heading (MeSH) terms: ‘online gambling’ OR ‘internet gambling’ OR ‘digital gambling’ OR ‘online bet*’ OR ‘internet bet*’, AND ‘adolesc*’ OR ‘child*’ OR ‘kid’ OR ‘teen*’, AND ‘patholog*’ OR ‘problem*’ OR ‘disorder*’ OR ‘disease’ OR ‘excessive’. Searches were re-run on June 30, 2020 and on October 30, 2020, but no newly published study met the five inclusion criteria. The reference lists of qualitative and review studies were also reviewed manually. Full search results and reference listings for each database consulted are available from any of the authors.
Study selection process
Figure 1 presents a flow diagram of the process of identifying, screening, selecting and including studies in the review. After removing all results other than academic articles, 641 manuscripts were identified in the five databases consulted. Seventeen manually identified articles were added from the list of references of review and qualitative studies. All references (n = 658) were imported to Zotero. The removal of duplicates produced 401 items for the screening phase. To minimise potential errors and bias in the selection process (Whiting et al., 2016), two independent researchers evaluated the titles, keywords and abstracts of all items to pre-select articles that could meet the eligibility criteria. Consequently, 308 articles were excluded. Kappa's concordance rate among the researchers at this screening phase was good (κ = 0.795). The first researcher (IM) evaluated the remaining 93 full texts according to the defined eligibility criteria, while the second researcher (JOB) reviewed the application of the criteria to these publications. When there was any discrepancy, the other manuscript authors were consulted until an agreement was reached. Finally, 16 articles were included in the qualitative synthesis. At this stage, Kappa's concordance index among the researchers for eligibility criteria application and final study selection was excellent (κ = 0.838).
Fig. 1.
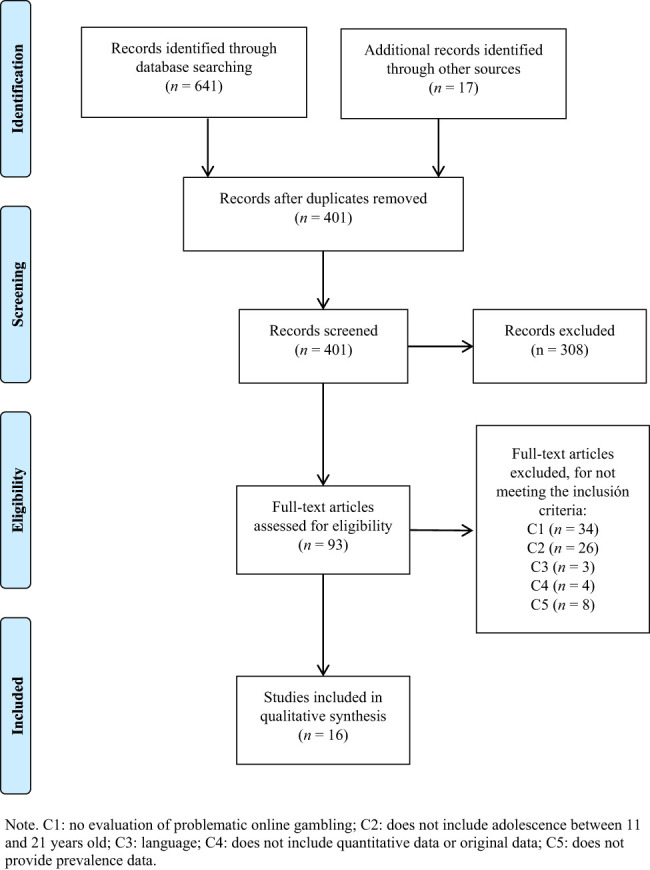
PRISMA Flow diagram of study selection
Data extraction
Table 1 provides a summary of all the information extracted from the sixteen articles selected for review. The data include authors and publication dates; sample countries; final sample size, age and sex of participants (mean, standard deviation and range); terminology used to refer to problematic online gambling (problem, pathological, disordered); measurement instruments and cut-off points used to classify gamblers; reliability data; results on prevalence; and, when analysed in the study, sex and age differences. Following the recommendations of Whiting et al. (2016) for minimising possible errors and bias in data collection, the first researcher (IM.) performed complete data extraction while a second researcher (JOB.) extracted data from 50% of the studies independently to detect and solve any inaccuracies.
Table 1.
Summary of selected international studies (n = 16) about problematic online gambling in adolescents
| Author and location | Final sample | Online gambling | Measurement tools (α) | Terminology | Tipology of gamblers and cut-off criteria | Results about prevalence of problem, pathological or online gambling disorder | Sex and/or age differences |
| Andrie et al. (2019) | 13,284 students of 14–18 y/o (7,000 ♀; 6,284 ♂; 61.4% 14–15.9 y/o). Representative sample. | 6% reported gambling online (any form) in the last year, 10% offline, and 12.5% of the study sample reported having gambled in any environment. | SOGS-RA | At-risk/Problem gambling | (1) 0–1: no problem gambling; (2) ≥2: as at-risk or problem gamblers (ARPG). | At-risk or problem gambling was reported by 3.6% of the whole sample, by 28% of those who gamble (either online or offline), by 48.4% of internet gamblers, and by 26.5% of gamblers in an offline venue. | ♂ (6.6%) > ARPG than ♀ (1%). 16–17.9 y/o (4.5%) > ARPG 14–15.9 y/o (3%). |
| Germany, Greece, Iceland, The Netherlands, Poland, Romania and Spain. | |||||||
| Aricak (2019) | 6,116 students of 12–18 y/o. | 12.4% of adolescents reported that they play online betting. | SOB and IAS | Problematic online betting | Range score 35–175. A median (68.50) plus two standard deviations (SD = 18,125) as a cut-off point (105) for Problematic internet user for Betting. | 2.9% of the whole sample and 23.3% of online bettors were problematic Internet users for betting. | 85.2% of problematic Internet users for betting were ♂. Mage was 15.30 ± 1.84. 8.5% were 12 y/o, 11.9% were 13 y/o, 13.6% were 14 y/o, 17.6% were 15 y/o, 16.5% were 16 y/o, 18.8% were 17 y/o, and 13.1% were 18 y/o. 34.7% were studying in middle school, and 65.3% were studying in high school. |
| Istanbul (Turkey). | |||||||
| Brunelle et al. (2012) | 1,870 students of 14–18 y/o (♂ 45.9%; ♀ 54.1%; Mage 15.43 ± 0.97). | 3.5% Internet Gamblers, 38.1% non-internet gamblers. Internet gamblers had to have gambled online at least once in the past year with actual money (any form of game). | DSM-IV-MR-J | Pathological online gambling | (1) 0–1: no problem gambling (NPG); (2) 2–3: at risk gambling (ARG); (3) ≥4: probable pathological gambling (PPG). | 15.4% of internet gamblers were PPG and 26.1% were ARG (vs. 1.7% and 6.6%, respectively, of non-internet gamblers). The proportion of Internet gamblers in ARG and PPG is five times higher than non-internet gamblers (41.6% vs. 8.3%). | |
| Quebec (Canada). | (α = 0.75) + (with Internet-specific component). | ||||||
| Canale et al. (2016) | 14,778 students of 15–19 y/o (63% ♂; Mage 17.26 ± 1.41). Representative sample. | 15.6% were online gamblers, defined as anyone who has participated in online gambling at least once in the past 12 months. | SOGS-RA Italian version | Problem gambling | Range score 0–12. Three categories: (1) 0–1: no problem; (2) 2–3: at-risk gambling; (3) ≥4: problem gambling. | Problem gambling prevalence rate was 4%; the rate among online gamblers was five times higher at 21.9%; more than 20% of online gamblers were at-risk gamblers (vs. less than 10% of non-online gamblers). Online gamblers were twice as likely to experience gambling problems compared to non-online gamblers. | |
| Italy. | (α = 0.78–0.79) | ||||||
| Elton-Marshall et al. (2016) | 10,035 students from 9th to 12th grade (49.3% ♂, 50.7% ♀; Mage 16.5 ± 0.10). Representative sample. | 9.4% of adolescents had gambled online (poker, sports pools and/or slot machines) in the past 3 months (3.7% of ♀s and 15.3% of ♂s). They had gambled money or something of value. Only 1.8% gamble online exclusively and 20.6% of those had participated in both online and land-based gambling. | GPSS/CAGI | Problem gambling | Classifies the severity of gambling as no problem, low to moderate, and high. | 17.4% of online gamblers scored “high” and 18.2% scored “low to moderate” in gambling severity (vs. 1.2% and 7.2% of land-based only gamblers, respectively). | |
| Canada: Newfoundland and Labrador, Ontario and Saskatchewan | |||||||
| Floros et al. (2013) | 2,017 students of 12–19 y/o (51.8% ♂ with Mage 15.05 ± 0.05; 48.2% ♀ with Mage 15.08 ± 0.05). Representative sample. | 37.2% reported having had some experience with Internet gambling (Mage 14.9 ± 0.06). | DSM-IV-MR-J Greek adaptation (α = 0.91) | Pathological gambling and addicted gambler | ≥4 out of 9 categories is indicative of pathological gambling (addict gamblers). | 11.1% of internet gamblers (n = 83) were classified as demonstrating addictive symptomatology (4.1% of the total student sample). | Sixty-nine of internet gamblers classified as demonstrating addictive symptomatology were ♂s (83%) and 14 ♀s (17%). Age distribution did not differ significantly between the groups. |
| Island of Kos (Greece). | |||||||
| Floros et al. (2015) | 2,684 students of 12–16 y/o (48.5% ♂ with Mage 13.67 ± 0.04; 51.5% ♀ with Mage 13.63 ± 0.04). Representative sample. | 19.1% reported having had some experience with Internet gambling during the past 3 months. | DSM-IV-MR-J Greek adaptation (α = 0.91) | Pathological gambling and addicted gambler | ≥4 out of 9 categories is indicative of pathological gambling (addict gamblers). | 13.8% of those who had had gambling experience and 18.1% among online gamblers (n = 63) demonstrated addictive symptomatology (2.5% of the total student sample). | 88% of internet gamblers classified as demonstrating addictive symptomatology were ♂s and 12% ♀s. Mage 13.92 ± 0.19 addicted gamblers > no gamblers. |
| Cyprus. | |||||||
| González-Cabrera et al. (2020) | 2,691 students of 11–19 y/o (602 ♂, 281 ♀; Mage 14.25 ± 1.55) | 32.8% reported having some experience in online gambling in the last twelve months. | OGD-Q (specific for online gambling) | Online gambling disorder | (1) ≥4 in the last 12 months: Online Gambling Disorder (OGD); (2) ≥4 over a period of 6–12 months: problem of online gambling; (3) ≥4 in a period of less than 6 months: at risk for online gambling problems. | 2% of the total sample and almost 7% of online gamblers had problematic situations with online gambling. OGD reached 0.89% of the total sample and 2.71% of online gamblers. “Problem with online gambling” represent 0.77% of the total sample and 2.38% of online gamblers. “At risk for problem online gambling” made up 0.56% of the total sample and 1.7% of online gamblers. | Of the 60 adolescents who were problematic or at risk, 50 were boys and 10 were girls. |
| Spain. | (α = 0.95) | ||||||
| González-Roz et al. (2017) | 1,267 students of 14–18 y/o (55% ♂; Mage 15.11± 0.73). | 0.6% online-based gamblers, 34.7% land-based gamblers and 3.9% mixed mode. Any game that involves betting with money in the past year (bingo, poker, other casino games, sports betting, lottery, scratch-tickets, and electronic gambling machines). | SOGS-RA Spanish adaptation | Problem gambling | Range score 0–12. Three categories: (1) 0–1: no problem; (2) 2–3: at-risk gambler; (3) ≥4: problem gambler. | None of the online bettors were problem gamblers but 25% were at-risk gamblers; 2.3% of land-based gamblers were problem gamblers and 8.6% were at-risk, while 10.2% of mixed-mode were problem gamblers and 22.4% were at-risk. | |
| Spain. | |||||||
| Griffiths and Wood (2007) | 8,017 young people of 12–15 y/o | 8% had ever played National Lottery products online (Instant win games for money, free Instant win games, lotto or one of the other draw games) (10% ♂s and 6% ♀s). | DSM-IV-MR-J | Pathological gambling/Problem gambling | (1) ≤3 in the past year: social gambler; (2) ≥4 in the past year: problem gambler. | 33% of online gamblers were classified as problem gamblers and 9% were classified as social gambler. | |
| United Kingdom. | |||||||
| Kang et al. (2019) | 14,011 students of 13–17 y/o (52.5% ♂, 47.5% ♀, Mage 14.9 ± 1.4). Representative sample. | 8.1% had gambled online in past 3 months (cards or hwatu using Hangame or Netmarble, wagering, lottery purchases, sports betting using bet-man, illegal sports betting, and internet casinos). | GPSS/CAGI | Problem gambling | Range score 0–27, three categories: (1) 0–1: no problem gambling (“Green light”), (2) 2–5: low to moderate severity (“Yellow light”); (3) ≥6: high severity (“Red light”). | 17.8% of online gamblers were classified as red light (1.1% of the total sample), 25.5% as yellow lights (4% of the total sample) and 56.7% as green light (vs. 3.3%, 15.8% and 80.9% of offline gamblers). | |
| Korea. | (α = 0.85) | ||||||
| Matthews et al. (2009) | 127 university students online gamblers (86 ♂, 41 ♀, Mage 20.8 ± 1.9) | All participants were self-defined online gamblers who had participated in at least one online gambling experience in their lifetime. | SOGS | Pathological gambling | (1) 1–2: non-problem gamblers; (2) 3–4: problem gamblers; (3) ≥5: probable pathological gamblers. | 19% of the sample (online gamblers) were classified as probable pathological gamblers. A further 18% were classified as potential pathological gamblers (problem gamblers), and 63% were defined as non–problem gamblers. | |
| Midlands (UK) | |||||||
| Mcbride and Derevensky (2012) | 465 university students of 18–20 y/o (305 ♂, 160 ♀). | 8% had gambled on the Internet in the past year (13–15 potential gambling activities). Gambling is wagering money on activities with a chance of winning or losing money. | DSM-IV criteria | Problem gambling | (1) 0: Non-gambler; (2) 1–2: social gambler; (3) ≥3: problem gambler. | 16.2% among internet gamblers are classified as problem gamblers (vs. 2.6% of non-internet gamblers). Students who had gambled on the Internet have nearly four times the problem gambling rate found in the entire sample and had higher risk-approach scores. Also, they have have six times the problem gambling rate found in non-internet gamblers. | |
| Canada. | |||||||
| Olason et al. (2011) | 1,537 students of 13–18 y/o (786 ♂, 747 ♀). Representative sample. | 24.3% had gambled on the Internet in the past 12 months. 1.7% of gamblers were land-based and Internet gamblers. | DSM-IV-MR-J | Pathological gambling/Problem gambling | (1) 0–1: no problem; (2) 2–3: at-risk gambling; (3) ≥4: problem gambling. | 2.7% of the entire sample were at-risk gamblers and 2.2% were problem gamblers. Internet gamblers were more likely to be classified as problem gamblers (7.5%) than non-Internet gamblers (1.1%). Problem gambling is predominantly found among those students who gamble on the Internet and land-based (7.7% were problem gamblers and 10.6% were at-risk gamblers). | |
| Hafnarfjörður (Iceland). | |||||||
| Potenza et al. (2011) | 2006 past-year gamblers of 14–18 y/o. | 20.5% reported internet gambling in the past year. Gambling is any game you bet on for money OR anything else of value. | MAGS DSM-IV Subescale | At-risk/Problem gambling | (1) Low-risk gamblers (LRGers): past-year gambling but any DSM-IV criteria; (2) At-risk/problem gamblers (ARPGers): ≥1 DSM-IV criteria. | Among internet gamblers, 57.5% were classified as ARPGers and 42.5% as LRGers (vs. non-internet gamblers: 27.7% and 72.3%, respectively). | 188 out of 237 ARPG are ♂s (81.39%) and 43 ♀s (18.61%), generating a significant difference by sex but not by grade or age. |
| Connecticut (USA) | |||||||
| Wong and So (2014) | 1,004 students (59.5% ♂, 40.5% ♀; Mage 14.7 ± 2.1) | 3.5% gambled online with money in the past year (any form). | DSM-IV-MR-J. (in reference to offline and online gambling) | Pathological gambling/problematic internet gambling | (1) 0–1: social gambling; (2) 2–3: at risk gambling; (3) ≥4: probable pathological gambling. | 1% of the entire sample and 28.6% of the online gamblers exhibited symptoms of problematic gambling. 22.9% and 5.7% of online gamblers were at-risk gamblers and pathological gamblers, respectively (vs. 7.1% and 3.9% of offline gamblers). Online gamblers are 1.5 and 3.2 times more likely to develop pathological and at-risk gambling than non-Internet gamblers. | Problematic Internet gambling was significantly associated with ♂s and school grades. |
| Hong-Kong. |
Note: y/o = years old; M age = arithmetic mean age; ♂ = boys; ♀ = girls; M = arithmetic mean; SD = standard deviation.
NPG = non-problem gambling; ARG = at-risk gambling; PPG = probable pathological gambling; ARPG = at-risk and/or problem gambling.
Table 2 presents the various assessment instruments used in the 16 studies, their main characteristics (number of items, response format and timeframe), psychometric properties such as reliability and validity and defined cut-off points for classifying participants. They are ordered according to the clinical criteria on which they are based, starting with the most current ones (DSM-5 and ICD-11).
Table 2.
Summary of instruments used for measuring problematic online gambling in adolescents, in selected studies (n = 16)
| Clinical criteria | Measurement tool | Studies | Main characteristics of measurement instrument | Items, response format and time frame | Cut-off points | Reliability and validity |
| DSM-5 and ICD-11 | Online Gambling Disorder Questionnaire (OGD-Q; González-Cabrera et al., 2020) | González-Cabrera et al. (2020) | Diagnostic instrument designed by adapting the criteria for the traditional gambling disorder of the DSM-5 (312.31) to the online context, the ICD-11 criteria to predominantly online gambling disorder (6C50.1), and the recommendations of several experts. Designed specifically to assess Online Gambling Disorder in adolescent online gamblers. | 11 items. | Score range 11–55. (1) ≥4 in the last 12 months: Online Gambling Disorder (OGD); (2) ≥4 over a period of 6–12 months: problem of online gambling; (3) ≥4 in a period of less than 6 months: at risk for online gambling problems. | It yielded adequate indicators of validity and reliability with high internal consistency in adolescent online gamblers (α = 0.94; ɷ= 0.95). Factor analysis confirmed a single factor with adequate goodness of fit, and there were also high item-total correlations and satisfactory factor loadings on all items. |
| 5-point scale (1: never; 5: (every day). | ||||||
| From less than a month to more than 12 months | ||||||
| DSM-IV-TR | Checklist of the DSM-IV-TR criteria for problem gambling (Stinchfield, 2003) | Mcbride and Derevensky (2012) | Ten-item checklist of the DSM-IV criteria for diagnosing pathological gambling in adults (Illegal acts committed, reliance on others for financial purposes, disrupted familial relationships, salience, tolerance, withdrawal symptoms, chasing losses, impaired control over gambling, escalation). | 19 items. | Score range 0–10. (1) 0–2: social gamblers; (2) 3–4: at-risk gamblers; (3) ≥5: pathological gamblers. | It has demonstrated satisfactory reliability (α = 0.77–0.98), validity and classification accuracy. However, with the 5-cut-off score, there was a false negative rate of 17%. It was reduced to 7% by lowering the cut score to 4 items, and to 6% by assigning weights to diagnostic items (Stinchfield et al., 2005). |
| Yes/No | ||||||
| Last 12 months | ||||||
| DSM-IV (9 out 10) | DSM-IV-MR-J (Fisher, 2000) | Brunelle et al. (2012), Floros et al. (2013, 2015), Griffiths and Wood (2007), Olason et al. (2011), Wong and So (2014) | Clinical screening tool to identify adolescents with problem gambling in non-clinical populations (Fisher, 2000). Its items were adapted from criteria for diagnosis of adult pathological gambling (progression and preoccupation, tolerance, withdrawal, loss of control, escape, chasing, lies and deception, illegal or unsocial acts, family/school disruption). | 12 items (9 categories). | Score range 0–9; (1) 0–3: Non problem gambling or social gambling; (2) ≥4: problem gambling. | It yielded satisfactory internal consistency reliability (α = 0.75) and convergent validity (r = 0.69) in a sample of 12–15 y/o fruit machine players. One or two-component structure was possible (Fisher, 2000). There is insufficient evidence of validity and classification accuracy (Stinchfield, 2010). |
| 4 response options: never, once or twice, sometimes or often. Yes/No | ||||||
| Past year | ||||||
| DSM-IV | Massachusets Gambling Screen (MAGS), MAGS-7 and DSM-IV Subscale (Shaffer et al., 1994) | Potenza et al. (2019) | Brief clinical screening instrument (survey or interview) for adolescents and adults, that measures the biological, psychological, and social problems in excessive gamblers. It has 2 stand-alone subscales: the 12-item DSM-IV subscale and the 14-item MAGS subscale based on the Short Michigan Alcoholism Screening Test. 7 items were selected as the best discriminators between pathological/non-pathological gamblers (MAGS-7). | MAGS-7: 7 items. | (1) 0–1: Nonpathological Gambling"; (2) 2–3: Transitional Gambling; (3) ≥4: Pathological Gambling. Each item score is multiplied by a weight and then summed along with constant using a weighted scoring algorithm derived from a discriminant function analysis. | The MAGS, the MAGS-7 and the DSM-IV subscale have demonstrated adequate internal consistency with adolescent samples (α = 0.86; α = 0.83; α = 0.87). The validity of the criteria is not equivalent between genders (Edgren et al., 2016). MAGS-7 correctly classified 96% of adolescents when using the DSM-IV as a reference, but it yielded high false negatives (Shaffer et al., 1994). |
| Yes/No. | ||||||
| Past year | ||||||
| DSM-III-R | South Oaks Gambling Screen-Revised for Adolescents (SOGS-RA; Winters et al., 1993) | Andrie et al. (2019), Baggio et al. (2016), Canale et al. (2016), González-Roz et al. (2017) | Screening instrument for adolescents adapted from SOGS, to measure problem severity and other gambling characteristics (onset, attitudes about legal age limit and odds of winning, money gambled, reasons for gambling, loss of control, chasing losses, interference with family, school, and relational life, guilt feelings and consequences of gambling). 4 additional items provide insight to an individual's gambling, but not used in scoring (gambling participation, expenditure, and parental gambling). | 12 items. | Broad criteria: problem gambler gambles at least weekly and obtain a SOGS-RA score of ≥2; or gamble daily, regardless of SOGS-RA score (in disuse). Narrow criteria: (1) 0–1: non-problem gambler; (2) 2–3: at-risk gambler; (3) ≥4: problem gambler (recommended) (Stinchfield, 2010) | Original version demonstrated acceptable reliability (α = 0.80), temporal stability (κ = 0.57), good concurrent validity and criterion validity in a sample of older male adolescents (15–18 y/o) (Winters et al., 1993). There is no consensus about its factorial structure (Stinchfield, 2010) and it seems to present gender and sociocultural differences (Edgren et al., 2016). |
| Yes/No. | ||||||
| Last 12 months. | ||||||
| SOGS: DSM-III; SOGS-R: DSM-III-R | South Oaks Gambling Screen (SOGS; Lesieur & Blume, 1987) | Matthews et al. (2009) | Screening instrument to identify pathological gambling in adults in clinical settings. Questions on gambling behaviour, respondent's feelings about gambling, consequences of gambling and borrowing money. The SOGS can be administered either in self-reports format or via face-to-face or telephone interview. | SOGS: 13 items and life-time. | Score range 0–20; (1) 1–2: non-problem gamblers; (2) 3–4: problem gamblers; (3) ≥5: probable pathological gamblers. | It yielded satisfactory reliability (α = 0.86–0.97) and convergent validity with clinician-administered interviews (r = 0.86–0.94). The self-report version had good overall classification accuracy (0.96), with better sensitivity (0.99) than specificity (0.75), suggesting in turn that in community prevalence studies it may yield high false positive rate (Stinchfield, 2002). |
| SOGS-R: 20 items and last 6 or 12 months. | ||||||
| Yes/No | ||||||
| Not specified | Gambling Problem Severity Subscale (GPSS) of the Canadian Adolescent Gambling Inventory (CAGI; Tremblay et al., 2010) | Elton-Marshall et al. (2016; Kang et al. (2019) | The GPSS was designed to provide a continuum of problem gambling severity among adolescents between 13 and 17 y/o., as part of the Canadian Adolescent Gambling Inventory (CAGI). Problem gambling severity is measured through items from the three consequences subscales (psychological, social, and financial) and the loss of control subscale. | 9 items | Score range 0–27; (1) 0–1 no problem gambling (“Green light”), (2) 2–5 low-to-moderate severity (“Yellow light”); (2) 6+ high severity (“Red light”). | The CAGI was found to yield satisfactory estimates of reliability (α = 0.83–0.90), validity and classification accuracy in adolescent clinical and population-based samples (Tremblay et al., 2010; Turner et al., 2017). The GPSS provided a good classification accuracy for a cut-off point of 6, with a sensitivity of 0.97 and specificity of 0.93. |
| 4-point scale (no: 0; 1–3 times: 1; 4–6 times: 2; 7 times or +: 3). | ||||||
| Last 3 months | ||||||
| Not specified | Survey for Online Betting (SOB) and Turkish version of Internet Addiction Scale (IAS; Gunuc & Kayri, 2010) | Aricak (2019) | The IAS was developed to measure general IA in Turkey. Some SOB questions were open ended questions (e.g. onset, feelings) and some were close ended questions (“Who were the most influential characters on you to bet first time?” and “Do you have VIP membership in online betting web sites?). | 35 + 36 | IAS Range score 35–175. A higher score indicates a higher possible IA level. A median plus two standard deviations as a cut-off point for problematic internet users for betting. | It yielded good internal consistency in paper and pencil (α = 0.89–0.91) and online versions (α = 0.83–0.91). |
| 5-points-scale (from Strongly agree to Strongly disagree). | ||||||
| Last 6 months. |
Synthesis of results
A synthesis of the results concerning prevalence data was carried out following an ad hoc categorisation based on instrument type (diagnostic, screening or severity scale) and whether online or offline gambling was evaluated. This categorization was used because the instruments employed in the reviewed studies shared certain underlying elements (i.e. family and school problems or loss of control), but their goals, contexts and criteria were different (Derevensky & Gupta, 2006). Even the dimensions assessed by the instruments and their approaches were different and not always clinical. Diagnostic instruments are designed to assess the presence of a clinical disorder following diagnostic criteria from APA (DSM-5) or WHO (ICD-11) and allow us to conclude whether a person meets that diagnostic and therefore presents the disorder or the absence of it (e.g. the Online Gambling Disorder Questionnaire -OGD-Q- or DSM-IV-MR-J). Instead, screening instruments are designed to identify the potential presence of a particular problem and they are typically used as a preliminary step in assessment (e.g. the SOGS-RA), as a way of determining if further, more comprehensive assessment is necessary (Waldron, 1998). On the other hand, some scales have been designed to measure the severity of the problem, not based on clinical criteria but psychological, social and financial consequences of gambling behaviours, that allow a score to be obtained on a continuous scale of severity ranging from low, to medium or high (e.g. the Gambling Problem Severity Subescale -GPSS-). Furthermore, an instrument developed to measure problem gambling in a clinical sample, where the base rate is fairly high, would have weaker classification accuracy when applied to the general population, where the base rate is extremely low (Stinchfield, 2010). Also, in many studies it has been observed that prevalence rates tend to be higher when measured with instruments such as the South Oaks Gambling Screen (SOGS), its adolescent version (SOGS-RA) or the Problem Gambling Severity Index (PGSI; Ferris & Wynne, 2001) and lower with clinical DSM criteria (Calado & Griffiths, 2016; Floros, 2018). As these aspects can influence prevalence outcomes and make comparison between them inappropriate (Edgren et al., 2016; Floros, 2018; Stinchfield, 2010), we decided to differentiate them in the narrative synthesis for didactic and presentation purposes.
Thus, this categorisation allowed for distinguishing (a) the prevalence of problem, pathological and disordered online gambling based on diagnostic instruments that address online gambling specifically (e.g. the Online Gambling Disorder Questionnaire [OGD-Q]) or ones that do not (e.g. DSM-IV, MAGS); (b) the prevalence of problem gambling based on the SOGS-RA and SOGS screening instruments, (both of which omit online gambling elements); and (c) the prevalence of high and low to moderate severity of problems using a severity scale such as the Gambling Problem Severity Subscale (GPSS) of the Canadian Adolescent Gambling Inventory (CAGI), which do not have online gambling elements.
Ethics statement
The writing of this manuscript did not involve the use of any procedures on human or animal participants.
Results
Characteristics of the studies
Most of the studies were conducted in Europe (n = 9), with the United Kingdom and Spain standing out with two studies in each country; followed by North America (n = 4), with Canada presenting three studies; and Asia (n = 3). They were all in English and had a cross-sectional design (n = 16). The sampling procedures were mostly non-probabilistic, convenience or incidental and non-representative of the whole adolescent population (n = 10), although five studies used international (Andrie et al., 2019) or national probabilistic samples (Canale, Griffiths, Vieno, Siciliano, & Molinaro, 2016; Elton-Marshall et al., 2016; Floros et al., 2015; Kang, Ok, Kim, & Lee, 2019) and two studies included the entire target population in the sample (Floros et al., 2013; Olason et al., 2011). Sample sizes were heterogeneous and ranged from 127 (Matthews, Farnsworth, & Griffiths, 2009) to 14,778 (Canale et al., 2016) adolescents between 11 and 21 years old. All samples consisted of students from elementary school, secondary school or university, and two samples were composed only of adolescent gamblers (Matthews et al., 2009; Potenza et al., 2011). Of these, only one concerned online gamblers exclusively (n = 127; Matthews et al., 2009). The average time between sample collection and publication was 3.6 years (range 1–7 years).
Measurement issues: online gambling operationalisation
The studies operationalised online gambling and identified online gamblers quite heterogeneously. Only four studies specified the need to have gambled with real money (Brunelle et al., 2012; González-Roz, Fernández-Hermida, Weidberg, Martínez-Loredo, & Secades-Villa, 2017; Mcbride & Derevensky, 2012; Wong & So, 2014), whereas two referred to money or ‘anything else of value’ (Elton-Marshall et al., 2016; Potenza et al., 2011). The rest did not specify anything in this regard.
Ten studies asked about any form of gambling or betting on the Internet without specifying any type of gambling (Andrie et al., 2019; Brunelle et al., 2012; Canale et al., 2016; Floros et al., 2013, 2015; González-Cabrera et al., 2020; Matthews et al., 2009; Olason et al., 2011; Potenza et al., 2011; Wong & So, 2014). Six studies specified the online games they were referring to (Aricak, 2019; Elton-Marshall et al., 2016; González-Roz et al., 2017; Griffiths & Wood, 2007; Kang et al., 2019; Mcbride & Derevensky, 2012).
The studies also differed in their time-based criteria for identifying online gamblers. In three studies, participants had to have gambled online in the three months prior to the study (Elton-Marshall et al., 2016; Floros et al., 2015; Kang et al., 2019), whereas in 9 studies, the period under examination was 12 months prior (Andrie et al., 2019; Brunelle et al., 2012; Canale et al., 2016; González-Cabrera et al., 2020; González-Roz et al., 2017; Mcbride & Derevensky, 2012; Olason et al., 2011; Potenza et al., 2011; Wong & So, 2014). Four studies included all those who had ever gambled online in their lives (Aricak, 2019; Floros et al., 2013; Griffiths & Wood, 2007; Matthews et al., 2009). In addition, two studies differentiated between gamblers who exclusively gambled online (online-based gamblers), exclusively offline (land-based gamblers) or online-offline (mixed gamblers) (González-Roz et al., 2017; Olason et al., 2011).
Measurement issues: problem, pathological and disordered online gambling assessment
There was considerable variability in the measurement instruments and cut-off points used. However, self-administered instruments were used in all cases, and in most cases, the defined timeframe was 12 months (see Table 2). Only three studies included specific elements of online gambling in their measuring instruments, while the rest exclusively mentioned items that referred to traditional gambling (Brunelle et al., 2012; González-Cabrera et al., 2020; Wong & So, 2014).
One study validated a new diagnostic instrument, the OGD-Q for adolescents (González-Cabrera et al., 2020), based on diagnostic criteria from the DSM-5 and the ICD-11 and on recommendations from several experts in the field. Eight studies used diagnostic instruments based on criteria from the DSM-IV or its related text revision, the DSM-IV-TR. Six studies used the Diagnostic and Statistical Manual-IV adapted format for Juveniles DSM-IV-MR-J (Fisher, 2000), one used the list of symptoms from the DSM-IV (Stinchfield, 2003) and one used the DSM-IV MAGS subscale (Shaffer et al., 1994).
Three studies used the SOGS-RA screening instrument (Winters et al., 1993) while one used its adult version, the SOGS (Lesieur & Blume, 1987). Both are based on clinical criteria from the DSM-III or its revised version, the DSM-III-R (American Psychiatric Association, 1980, 1987).
Two studies assessed the severity of problem gambling through the continuous GPSS scale, which is part of the CAGI (Tremblay, Stinchfield, Wiebe, & Wynne, 2010).
Conversely, one study combined a scale designed ad hoc to evaluate online betting (Survey of Online Betting), which was developed by a team of experts, with the Internet Addiction Scale (Gunuc & Kayri, 2010), based on the premise that problematic online betting is an example of Specific Problematic Internet Use (SPIU).
In general, the cut-off points in diagnostic and screening instruments were equal to 4 or more satisfied criteria to classify adolescents as probable pathological gamblers and three criteria generally classified them as exhibiting problem or at-risk gambling. However, it is worth noting that not all the instruments used include the same number of items. For example, while the OGD-Q includes 11 items, the DSM-IV-MR-J includes 9 and the SOGS-RA 12. Also, there were more particularities in each study (see Table 2), such as in one study, in addition to defining the cut-off point of 4 criteria, accounted for the duration of symptoms to determine the diagnosis of an online gambling disorder, differentiating it from problem gambling (González-Cabrera et al., 2020), while another study designates a participant as at-risk/problem gambling by fulfilling only one criterion of the DSM-IV (Potenza et al., 2011).
Only six studies analysed the internal consistency of the scales used by means of Cronbach's alpha (Brunelle et al., 2012; Canale et al., 2016; Floros et al., 2013, 2015; González-Cabrera et al., 2020; Kang et al., 2019). In addition, one study performed an in-depth psychometric analysis of the instrument used on a sample of adolescent online gamblers (González-Cabrera et al., 2020) (see Tables 1 and 2).
Prevalence of online gambling and problematic online gambling
There was great inconsistency in the number of adolescents that were found to gamble online, ranging between 0.6% in Spain (González-Roz et al., 2017) and 37.2% on the island of Kos (Floros et al., 2013). Based on the past year's data, the percentage varies from 3.5% of adolescents in Canada (Brunelle et al., 2012) and China (Wong & So, 2014) to 32.8% in Spain (González-Cabrera et al., 2020). If we look only at those studies that used representative samples of adolescents, online gambling past-year prevalence varies between 6% in European adolescents (Andrie et al., 2019) and 15.6% in Italian adolescents (Canale et al., 2016).
In addition, high variability in problematic online gambling prevalence was found in the reviewed studies. The prevalence of different problematic online gambling levels (disordered or pathological and problem gambling) is described below, taking into account samples, the defined timeframe, the type of assessment instrument used—diagnostic, screening or severity scale—and whether the instrument in question addressed online gambling specifically.
Pathological or disordered online gambling in adolescents and pathological gambling among those who gamble online
Based on diagnostic instruments with online gambling elements, the prevalence of pathological online gambling or online gambling disorder during the last year in adolescents ranged from 0.89% in Spain (González-Cabrera et al., 2020) to 1% in China (Wong & So, 2014), while the prevalence among those adolescent who have gambled online ranged from 2.7% in Spain (González-Cabrera et al., 2020) to 15.4% in Canada (Brunelle et al., 2012). However, based on diagnostic instruments used for offline gambling, the past-year prevalence of pathological gambling in adolescent online gamblers varied from 7.5% in Iceland (Olason et al., 2011) to 18.1% in Cyprus (Floros et al., 2015) and the lifetime prevalence of pathological gambling in adolescent online gamblers ranged from 11.1% in Greece (Floros et al., 2013) to 33% in the UK (Griffiths & Wood, 2007).
It should be noted that only three of the seven studies mentioned used a representative sample of the adolescent population. Specifically, Floros et al. (2013), used a sample consisting of all students on the Island of Kos, Floros et al. (2015) used a representative sample of 2,684 Cypriot students aged 12–16 years and Olason et al. (2011) used a sample consisting of almost all adolescents from Hafnarfjörður (Iceland). In all cases, the presence of pathological gambling among adolescents in general (4.1%, 2.5% and 2.2%, respectively) and among online gamblers (11.1%, 18.1% and 7.5%, respectively) was assessed.
Problem online gambling in adolescents and problem gambling among those who gamble online
When a diagnostic instrument including online gambling elements, such as the OGD-Q, was used to evaluate online gambling problems, the past-year prevalence among adolescents in general was reported at 0.77%, and 2.4% among online gamblers (González-Cabrera et al., 2020). However, the latter figure amounted to 16.2% when DSM-IV criteria to diagnose offline problem gambling were used (Mcbride & Derevensky, 2012). Furthermore, when screening instruments designed to evaluate offline problem gambling (such as the SOGS-RA) were used among online gamblers, the prevalence of problem gambling varied between 10.2% in Spain (González-Roz et al., 2017) and 21.9% in Italy (Canale et al., 2016). It should be noted that only the last of the four studies mentioned used a representative sample of the Italian adolescent population of 15–19 years of age to assess problem gambling among adolescents in general (4%) and among online gamblers (21.9%).
At-risk/problem online gambling in adolescents and at-risk/problem gambling among those who gamble online
Using diagnostic instruments that refer to online gambling, the past-year prevalence of at-risk online gambling among adolescents in general was 0.56% in Spain (González-Cabrera et al., 2020). However, among adolescent online gamblers, prevalence varied between 1.7% in Spain (González-Cabrera et al., 2020), 22.9% in China (Wong & So, 2014) and 26.1% in Canada (Brunelle et al., 2012).
In studies where At-Risk and Problem Gambling (ARPG) were measured together prevalence among adolescent online gamblers varied from 48.4% in a cross-national European study using the SOGS-RA (Andrie et al., 2019) to 57.5% in the U.S. state of Connecticut using the MAGS-DSM-IV in a self-selected sample of past-year gamblers (Potenza et al., 2011). It should be noted that only one of the five studies mentioned used a representative sample of the European adolescent population between 14 and 18 years of age to assess at-risk or problem gambling (ARPG) among adolescents in general (3.6%), among adolescent gamblers (28%), online gamblers (48.4%) and only-offline gamblers (26.5%).
Severity of gambling behaviour among adolescents who gamble online
In terms of the severity of gambling behaviour evaluated with the GPSS/CAGI, the prevalence of highly severe problems in the last 3 months among adolescent online gamblers was between 17.4% in Canada (Elton-Marshall et al., 2016) and 17.8% in South Korea (Kang et al., 2019). The prevalence of low to moderate problems was between 18.2% in Canada (Elton-Marshall et al., 2016) and 25.5% in South Korea (Kang et al., 2019). It should be noted that the two studies mentioned used a representative sample of adolescent population. Specifically, Elton-Marshall et al. (2016) used a representative sample of Canadian adolescents and Kang et al. (2019) of Korean students aged 13–17 years.
Sex and age differences in problem, pathological and disordered online gambling
Six studies provided data on sex based differences in prevalence. They all agreed that boys have more online gambling related problems than girls do (Andrie et al., 2019; Aricak, 2019; Floros et al., 2013; González-Cabrera et al., 2020; Potenza et al., 2011; Wong & So, 2014). Three studies provided data on age differences. One found that among all adolescents who participated in the study, the proportion of ARPG was highest in the older age group (4.5% at 16–17.9 years in comparison to 3% at 14–15.9 years, P < 0.001), in which there were a higher proportion of online gamblers (7.6% in comparison to 4.9%, P < 0.001) (Andrie et al., 2019). The other two studies did not find significant differences between the different age groups between 12 and 19 years of age (Floros et al., 2013; Potenza et al., 2011).
Discussion
The main objective of this systematic review was to synthesize the research related to problematic online gambling, including problem, pathological and disordered online gambling in adolescents and among those who gamble online. In particular, it focused on answering several research questions relating to: (a) the operationalisation of online gambling prevalence; (b) the diverse instruments for assessing problematic online gambling in adolescents, their cut-off points/criteria and characteristics; and (c) the international prevalence data of different grades of problematic online gambling. Initially, 658 peer-reviewed papers were identified, of which 16 ultimately met the five eligibility criteria for inclusion in this systematic review.
Concerning the first research question about the operationalisation of online gambling prevalence, there was, as expected, high heterogeneity. This could explain, at least partially, that the proportion of adolescents that gamble online varied between 0.6% (González-Roz et al., 2017) and 37.2% (Floros et al., 2013). However, when representative samples of the adolescent population were used, the prevalence range was between 6% (Andrie et al., 2019) and 15.6% (Canale et al., 2016), in line with the range found in the King et al.'s (2020) review of online gambling in adolescents (5%–15%). The breadth of the range could be explained by at least five reasons. First, the cultural and legal context of the studies may influence gambling behaviours and, consequently, prevalence rates (Volberg et al., 2018). Second, since not all studies specified the need to gamble for real money, some adolescents might have responded with simulated forms of gambling in mind, as these are common at these ages (Elton-Marshall et al., 2016). Third, the specific forms of online gambling referred to were different in each study, some of which were much more frequent than others, such as online betting (Hollén et al., 2020), that has been related with higher risk of problems (McCormack, Shorter, & Griffiths, 2013). Fourth, the timeframe evaluated varied from three months (Elton-Marshall et al., 2016; Floros et al., 2015; Kang et al., 2019) to a lifetime (Aricak, 2019; Floros et al., 2013; Griffiths & Wood, 2007; Matthews et al., 2009). Finally, in all but one of the reviewed studies (González-Roz et al., 2017), online gamblers were considered a homogeneous group, disregarding that a large percentage of them also gamble offline (Elton-Marshall et al., 2016; Olason et al., 2011).
It is important to note that the group made up of online and offline gamblers is known as mixed gamblers and, according to different studies, mixed gambling predicts both at-risk gambling and problematic gambling better than pure online gambling does. This could be because, beyond the characteristics of the internet, mixed gambling implies greater engagement in the behaviour due to the diversity of games, access modes and time spent on them. González-Roz et al. (2017) and Olason et al. (2011) suggested that this could explain the higher prevalence of at-risk and problem gambling found among adolescents who gamble online (and are mixed gamblers) compared to those who gamble offline in numerous studies, including eleven studies of the present review (e.g. Brunelle et al., 2012; Griffiths & Parke, 2010; Griffiths & Wood, 2007; Mcbride & Derevensky, 2012; Olason et al., 2011). In line with this issue, Blaszczynski, Russell, Gainsbury, and Hing (2016) conclude that exclusive online gamblers represent a different subpopulation at lower risk of harm (problem gambling, gambling involvement and consumption of alcohol) compared to gamblers engaging in multiple forms of gambling. This discussion could be compared to that described in the scientific literature on substance abuse about "polydrugs users", that is those who use multiple substances at the same time, who have more negative and severe social and health consequences compared to monosubstance users (Steele & Peralta, 2020).
Concerning the second research question of this review about the measurement instruments and cut-off points/criteria used, there was noteworthy variability as well as limited psychometric analysis. It is also significant that virtually no instrument has been validated for adolescents who gamble online or has been based on updated diagnostic criteria (DSM-5 and ICD-11). In this review, only one study used a specific instrument to assess online gambling disorder based on the most current diagnostic criteria (González-Cabrera et al., 2020) while two others only included some elements of online gambling in the items of the diagnostic instrument used DSM-IV-MR-J (Brunelle et al., 2012; Wong & So, 2014).
The most commonly used instruments in the reviewed studies were the DSM-IV-MR-J and SOGS-RA, that were designed to assess offline gambling problems. The SOGS-RA is a screening instrument designed for the clinical context and is adapted from its adult version (SOGS), which evaluates symptoms of ‘problem gambling’ and negative consequences of gambling, such as the amount of money gambled or the feeling of guilt (Derevensky & Gupta, 2006), but it does not confirm the existence of a mental disorder (Edgren et al., 2016). Meanwhile, the DSM-IV-MR-J is a diagnostic instrument for evaluating ‘pathological gambling’ in adolescents using the diagnostic criteria of the DSM-IV (preoccupation, tolerance, escape, etc.). Although common, this term is outdated because it draws on the old consideration of the problem as an impulse control disorder, and some authors consider it pejorative and inappropriate for referring to adolescents (Petry et al., 2014; Volberg, Gupta, Griffiths, Ólason, & Delfabbro, 2010). This could explain why ‘problem gambling’ is the preferred term when studying adolescent gambling behaviour and why it has been used as an equivalent to pathological gambling in several studies. In spite of its wide use, problem gambling was discarded from the DSM-5 for being too generic, as it incorporates subclinical problems and conditions (Petry et al., 2014).
Furthermore, as noted, the diagnostic criteria on which these tools were based have not been clinically tested on the adolescent population, which calls into question their validity for this population (Edgren et al., 2016; King et al., 2020; Stinchfield, 2010; Volberg et al., 2010). For some instruments, such as the MAGS or SOGS-RA, it has even been suggested that the criterion validity is not equivalent for boys and girls (Edgren et al., 2016). Moreover, none but one of the reviewed instruments has been validated in adolescent online gamblers (González-Cabrera et al., 2020), which could present a validity issue when assessing problematic online gambling in adolescents and in the highest-risk population: online gamblers. In general, there is limited assessment of the psychometric properties of the measurement instruments used in the studies and several authors recommended further research in this regard (Derevensky & Gupta, 2006; Edgren et al., 2016; King et al., 2020; Potenza et al., 2019; Stinchfield, 2010). In this review, only seven studies provided information on reliability using Cronbach's alpha, but it was insufficient (Edgren et al., 2016).
Regarding the third research question on the international prevalence of different levels of problematic online gambling, and sex and age based differences, the results are greatly affected by the type of assessment tool employed. Between 0.89% and 1% of adolescents exhibited an online gambling disorder based on diagnostic assessment which included online elements. However, between 0.77% and 57.5% of adolescents meet some criteria for problematic online gambling, a range much higher than that found by Calado et al. (2017) on problem gambling in adolescents (0.2%–12.3%). Even when we look only at the studies that used representative samples of the adolescent population, we observe that between 1.1% and 48.4% of adolescents presented some degree of problematic online gambling. The breadth of these ranges could be due at least partially to the differences between samples, assessment instruments, cut-offs, and timeframes. For example, using offline gambling based diagnostic instruments, a higher prevalence is obtained than when using specific online gambling diagnostic instruments. Furthermore, when problem gambling screening instruments are used, the prevalence of problem gambling in online gamblers (10.2%–21.9%) is higher to that found in the review by Delfabbro, King, and Derevensky (2016), according to which between 4% and 8% of adolescent gamblers are experiencing significant gambling-related problems. Among the studies that used representative samples of the adolescent population, we observe that the range of prevalence rates of pathological gambling among online gamblers is from 7.5% to 18.1%, while the prevalence of problem gambling is 21.9% and the percentage of adolescents online gamblers with a high severity of problem gambling is between 17.4% and 17.8%.
Regarding the differences found in prevalence according to sex, although only six studies analysed this issue, all of them indicated that boys have more problems related to online gambling than girls do, in line with findings on offline gambling (Calado et al., 2017). These results may have been skewed by the type of gambling included in each study and, therefore, cannot be considered conclusive. For example, boys place more online sports bets than girls do (Hollén et al., 2020; McCormack et al., 2014), which has been significantly associated with problematic online gambling (Olason et al., 2011; Potenza et al., 2011). However, recent studies have seen significant growth in online gambling behaviour in women and some trend changes in the development of online gambling problems (Hollén et al., 2020; McCormack et al., 2014; Volberg et al., 2018), which points to the need for further analysis on gender related differences in online gambling.
Regarding age, only three studies analysed its relationship with problem, pathological or disordered online gambling. As the results were contradictory, a firm conclusion cannot be established. For example, Potenza et al. (2019) and Floros et al. (2013) found no significant differences in age, whereas Andrie et al. (2019) observed a higher proportion of ARPG among older adolescents. In line with this, studies such as that of Hubert and Griffiths (2018), which included adolescents and adults, found that almost half of the pathological online gamblers were between the ages of 16 and 20.
It should be pointed out that most of the studies included in this review utilized non-representative convenience samples, which do not allow generalize their results to the entire adolescent population. Moreover, the methodological differences between studies and the cultural or legal context, also compromise comparability across studies and countries, making the establishment of a general prevalence very difficult, even when this is crucial to advance in the scientific knowledge of this problem.
Recommendations and future directions
These results yield several recommendations for researchers. First, there is a pressing need to clearly operationalise online gambling and the types of gambling included therein in a unified way, as authors such as King et al. (2020) have suggested. In this sense, it would be worth considering the inclusion of some gambling behaviours characteristic of adolescents, such as the use of loot boxes in online video games, simulated gambling (where it is not necessary to bet real money) or skin gambling (the use of virtual goods as virtual currency to bet), as they seem to be associated with problematic online gambling in adolescents (Floros et al., 2013; King, Delfabbro, Kaptsis, Zwaans, 2014; Kristiansen & Severin, 2020; Wardle, 2019; Zendle, Meyer, & Over, 2019). In addition, although loot boxes are not legally regarded as gambling in all countries (Griffiths, 2018), Belgium has already declared them a form of gambling and the Netherlands and Denmark are moving in the same direction (Kristiansen & Severin, 2020).
Second, the findings of this review highlight the need to design new assessment tools specifically for adolescents and online gambling. Researchers should analyse the psychometric properties of these instruments and incorporate timeframes and cut-off points which are based on a ‘gold standard’ diagnostic criterion to differentiate subclinical online gambling problems from the clinical disorder (Stinchfield, 2010). It would also be advisable to test the instruments in population-based and clinical samples and use each one in the context for which it was created (Derevensky & Gupta, 2006; Edgren et al., 2016; Tremblay et al., 2010). Further, given the changing nature of the phenomenon of online gambling and rapid technological evolution, it would be a good practice to ensure that the time between sample collection and publication of the results is as short as possible.
Third, and in line with the above, there is an urgent need to unify the terminology used by the scientific community to refer to different levels of problematic online gambling including online gambling disorder. Accordingly, it would be necessary to discuss in the next revision of the DSM the inclusion of the online version of gambling disorder. The term ‘gambling disorder’ best suits the current classification systems and available scientific evidence (Petry et al., 2014), but the new technological context deserves a place in this classification, as it already has in the ICD-11. This might prompt further study and generate more solid evidence concerning this issue, such as its prevalence and age and sex differences.
Limitations
This review faced some limitations that should be discussed. First, the number of studies included in the review was limited likely due to the relative novelty of the subject and the very strict protocol requiring compliance with the five inclusion criteria. It is, therefore, possible that other studies of potential relevance did not appear in this review. Second, as some of the reviewed studies predate the DSM-5, some inconsistency in the results was expected. Third, the methodology of this review did not provide meta-analytical results owing to the high heterogeneity of information collected. Fourth, the limited representativeness of most of the study samples does not allow generalization of their results to the entire adolescent population. Finally, an ad hoc categorisation of the results was carried out based on the type of instrument used, which may not match the original intention of the authors. This was considered appropriate from an analytical and pedagogical approach to facilitate the organisation and understanding of the narrative synthesis.
Conclusions
Although problematic online gambling in adolescents is an area of increasing research interest, this systematic review highlights several aspects. First, there is great heterogeneity in the operationalisation of online gambling. Second, there is a lack of consensus about the terminology, instruments and cut-off points used to assess problematic online gambling in a broad sense and online gambling disorder in a clinical sense. Third, the need to develop and psychometrically improve measurement instruments, especially for adolescents and online gambling, is noteworthy, to promote early detection and intervention. This leads to a significant disparity in the prevalence outcomes of different levels of problematic online gambling in adolescents and among those who gamble online, as difficulties in establishing firm conclusions about the extent and severity of the problem.
Funding sources
This research was funded by the Spanish Ministry of Economy, Industry and Competitiveness, RTI2018-094212-B-I00: (CIBER-AACC), and by the International University of La Rioja, Project “Cyberpsychology (Triennium 2017–2020)”.
Authors' contributions
All the authors designed the review. IM wrote the protocol, conducted literature searches, analyzed of the records and wrote the first draft of the manuscript. JOB and ABG contributed to the selection of studies and data extraction. JGC and JMM supervised the project, provided feedback and reviewed the manuscript. JGC acquired the financial support for the project leading to this publication. All authors contributed to and approved the final manuscript. All authors had full access to all data in the review and take responsibility for the integrity of the data.
Conflict of interests
The authors declare that are are no financial, industrial or other relationships that may constitute a conflict of interest concerning this work.
References
- American Psychiatric Association . (1980). Diagnostic and statistical manual of mental disorders (DSM-III) (3rd ed.). American Psychiatric Association. 10.1176/appi.books.9780890420188.dsm-iii-r. [DOI] [Google Scholar]
- American Psychiatric Association . (1987). Diagnostic and statistical manual of mental disorders (DSM-III-R) (3rd ed.). American Psychiatric Association. 10.1176/appi.books.9780890420188.dsm-iii-r. [DOI] [Google Scholar]
- American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders (DSM-5) (5th ed.). American Psychiatric Association. [Google Scholar]
- Andrie, E. K. , Tzavara, C. K. , Tzavela, E. , Richardson, C. , Greydanus, D. , Tsolia, M. , & Tsitsika, A. K. (2019). Gambling involvement and problem gambling correlates among European adolescents: Results from the European Network for Addictive Behavior study. Social Psychiatry and Psychiatric Epidemiology , 54(11), 1429–1441. 10.1007/s00127-019-01706-w. [DOI] [PubMed] [Google Scholar]
- Aricak, O. T. (2019). Problematic online betting among Turkish adolescents. Journal of Gambling Studies , 35(1), 31–45. 10.1007/s10899-018-9793-8. [DOI] [PubMed] [Google Scholar]
- Baggio, S. , Dupuis, M. , Berchtold, A. , Spilka, S. , Simon, O. , & Studer, J. (2017). Is gambling involvement a confounding variable for the relationship between Internet gambling and gambling problem severity? Computers in Human Behavior , 71, 148–152. 10.1016/j.chb.2017.02.004. [DOI] [Google Scholar]
- Baggio, S. , Gainsbury, S. M. , Berchtold, A. , & Iglesias, K. (2016). Co-morbidity of gambling and Internet use among Internet and land-based gamblers: Classic and network approaches. International Gambling Studies , 16(3), 500–517. 10.1080/14459795.2016.1242148. [DOI] [Google Scholar]
- Beranuy, M. , Machimbarrena, J. M. , Vega-osés, M. A. , Carbonell, X. , Griffiths, M. D. , Pontes, H. M. , & González-cabrera, J. (2020). Spanish validation of the internet gaming disorder scale–short form (IGDS9-SF): Prevalence and relationship with online gambling and quality of life. International Journal of Environmental Research and Public Health , 17(5). 10.3390/ijerph17051562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blaszczynski, A. , Russell, A. , Gainsbury, S. , & Hing, N. (2016). Mental health and online, land-based and mixed gamblers. Journal of Gambling Studies , 32(1), 261–275. 10.1007/s10899-015-9528-z. [DOI] [PubMed] [Google Scholar]
- Brunelle, N. , Leclerc, D. , Cousineau, M.-M. , Dufour, M. , Gendron, A. , & Martin, I. (2012). Internet gambling, substance use, and delinquent behavior: An adolescent deviant behavior involvement pattern. Psychology of Addictive Behaviors , 26(2), 364–370. 10.1037/a0027079. [DOI] [PubMed] [Google Scholar]
- Caillon, J. , Grall-Bronnec, M. , Bouju, G. , Lagadec, M. , & Vénisse, J.-L. (2012). Pathological gambling in adolescence [Le jeu pathologique à l’adolescence]. Archives de Pediatrie , 19(2), 173–178. 10.1016/j.arcped.2011.11.020. [DOI] [PubMed] [Google Scholar]
- Calado, F. , Alexandre, J. , & Griffiths, M. D. (2017). Prevalence of adolescent problem gambling: A systematic review of recent research. Journal of Gambling Studies , 33(2), 397–424. 10.1007/s10899-016-9627-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calado, F. , & Griffiths, M. D. (2016). Problem gambling worldwide: An update and systematic review of empirical research (2000–2015). Journal of Behavioral Addictions , 5(4), 592–613. 10.1556/2006.5.2016.073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Canale, N. , Griffiths, M. D. , Vieno, A. , Siciliano, V. , & Molinaro, S. (2016). Impact of Internet gambling on problem gambling among adolescents in Italy: Findings from a large-scale nationally representative survey. Computers in Human Behavior , 57, 99–106. 10.1016/j.chb.2015.12.020. [DOI] [Google Scholar]
- Chóliz, M. (2016). The challenge of online gambling: The effect of legalization on the increase in online gambling addiction. Journal of Gambling Studies , 32(2), 749–756. 10.1007/s10899-015-9558-6. [DOI] [PubMed] [Google Scholar]
- Chóliz, M. , Marcos, M. , & Lázaro-Mateo, J. (2019). The risk of online gambling: A study of gambling disorder prevalence rates in Spain. International Journal of Mental Health and Addiction , 19(2), 1–14. 10.1007/s11469-019-00067-4. [DOI] [Google Scholar]
- Delfabbro, P. , King, D. L. , & Derevensky, J. L. (2016). Adolescent gambling and problem gambling: Prevalence, current issues, and concerns. Current Addiction Reports , 3(3), 268–274. 10.1007/s40429-016-0105-z. [DOI] [Google Scholar]
- Derevensky, J. L. , & Gupta, R. (2006). Measuring gambling problems among adolescents: Current status and future directions. International Gambling Studies , 6(2), 201–215. 10.1080/14459790600928702. [DOI] [Google Scholar]
- Derevensky, J. L. , & Gupta, R. (2007). Internet gambling amongst adolescents: A growing concern. International Journal of Mental Health and Addiction , 5(2), 93–101. 10.1007/s11469-007-9057-9. [DOI] [Google Scholar]
- Dowling, N. A. , Merkouris, S. S. , Greenwood, C. J. , Oldenhof, E. , Toumbourou, J. W. , & Youssef, G. J. (2017). Early risk and protective factors for problem gambling: A systematic review and meta-analysis of longitudinal studies. Clinical Psychology Review , 51, 109–124. 10.1016/j.cpr.2016.10.008. [DOI] [PubMed] [Google Scholar]
- Edgren, R. , Castrén, S. , Mäkelä, M. , Pörtfors, P. , Alho, H. , & Salonen, A. H. (2016). Reliability of instruments measuring at-risk and problem gambling among young individuals: A systematic review covering years 2009–2015. Journal of Adolescent Health , 58(6), 600–615. 10.1016/j.jadohealth.2016.03.007. [DOI] [PubMed] [Google Scholar]
- Effertz, T. , Bischof, A. , Rumpf, H.-J. , Meyer, C. , & John, U. (2018). The effect of online gambling on gambling problems and resulting economic health costs in Germany. European Journal of Health Economics , 19(7), 967–978. 10.1007/s10198-017-0945-z. [DOI] [PubMed] [Google Scholar]
- Elton-Marshall, T. , Leatherdale, S. T. , & Turner, N. E. (2016). An examination of internet and land-based gambling among adolescents in three Canadian provinces: Results from the youth gambling survey (YGS). BMC Public Health , 16, 277. 10.1186/s12889-016-2933-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Emond, A. M. , & Griffiths, M. D. (2020). Gambling in children and adolescents. British Medical Bulletin , 136(1), 21–29. 10.1093/bmb/ldaa027. [DOI] [PubMed] [Google Scholar]
- Emond, A. M. , Griffiths, M. D. , & Hollén, L. (2020). Problem gambling in early adulthood: A population-based study. International Journal of Mental Health and Addiction . 10.1007/s11469-020-00401-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferris, J. , & Wynne, H. (2001). The Canadian problem gambling index: Final report . Canadian Centre on Substance Abuse. https://www.greo.ca/Modules/EvidenceCentre/files/Ferris%20et%20al(2001)The_Canadian_Problem_Gambling_Index.pdf. [Google Scholar]
- Fisher, S. (2000). Developing the DSM-IV-DSM-IV criteria to identify adolescent problem gambling in non-clinical populations. Journal of Gambling Studies , 16(2/3), 253–273. 10.1023/A:1009437115789. [DOI] [PubMed] [Google Scholar]
- Floros, G. D. (2018). Gambling disorder in adolescents: Prevalence, new developments, and treatment challenges. Adolescent Health, Medicine and Therapeutics , 9, 43–51. 10.2147/AHMT.S135423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Floros, G. D. , Paradisioti, A. , Hadjimarcou, M. , Mappouras, D. G. , Karkanioti, O. , & Siomos, K. (2015). Adolescent online gambling in Cyprus: Associated school performance and psychopathology. Journal of Gambling Studies , 31(2), 367–384. 10.1007/s10899-013-9424-3. [DOI] [PubMed] [Google Scholar]
- Floros, G. D. , Siomos, K. , Fisoun, V. , & Geroukalis, D. (2013). Adolescent online gambling: The impact of parental practices and correlates with online activities. Journal of Gambling Studies , 29(1), 131–150. 10.1007/s10899-011-9291-8. [DOI] [PubMed] [Google Scholar]
- Gainsbury, S. M. (2015). Online gambling addiction: The relationship between internet gambling and disordered gambling. Current Addiction Reports , 2(2), 185–193. 10.1007/s40429-015-0057-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gainsbury, S. M. , Angus, D. J. , & Blaszczynski, A. (2019). Isolating the impact of specific gambling activities and modes on problem gambling and psychological distress in internet gamblers. BMC Public Health , 19(1), 1372. 10.1186/s12889-019-7738-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gainsbury, S. M. , King, D. L. , Russell, A. M. T. , Delfabbro, P. , Derevensky, J. , & Hing, N. (2016). Exposure to and engagement with gambling marketing in social media: Reported impacts on moderate-risk and problem gamblers. Psychology of Addictive Behaviors , 30(2), 270–276. 10.1037/adb0000156. [DOI] [PubMed] [Google Scholar]
- Gómez, P. , Feijóo, S. , Braña, T. , Varela, J. , & Rial, A. (2019). Minors and online gambling: Prevalence and related variables. Journal of Gambling Studies , 36, 735–745. 10.1007/s10899-019-09923-3. [DOI] [PubMed] [Google Scholar]
- González-Cabrera, J. , Machimbarrena, J. M. , Beranuy, M. , Pérez-Rodríguez, P. , Fernández-González, L. , & Calvete, E. (2020). Design and measurement properties of the online gambling disorder Questionnaire (OGD-Q) in Spanish adolescents. Journal of Clinical Medicine , 9(1), 120. 10.3390/jcm9010120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- González-Roz, A. , Fernández-Hermida, J. R. , Weidberg, S. , Martínez-Loredo, V. , & Secades-Villa, R. (2017). Prevalence of problem gambling among adolescents: A comparison across modes of access, gambling activities, and levels of severity. Journal of Gambling Studies , 33(2), 371–382. 10.1007/s10899-016-9652-4. [DOI] [PubMed] [Google Scholar]
- Griffiths, M. D. (2003). Internet gambling: Issues, concerns, and recommendations. CyberPsychology & Behavior , 6(6), 557–568. 10.1089/109493103322725333. [DOI] [PubMed] [Google Scholar]
- Griffiths, M. D. (2018). Is the buying of loot boxes in video games a form of gambling or gaming? Gaming Law Review , 22(1), 52–54. 10.1089/glr2.2018.2216. [DOI] [Google Scholar]
- Griffiths, M. D. , & Parke, J. (2010). Adolescent gambling on the internet: A review. International Journal of Adolescent Medicine and Health , 22(1), 59–75. [PubMed] [Google Scholar]
- Griffiths, M. D. , Wardle, H. , Orford, J. , Sproston, K. , & Erens, B. (2009). Sociodemographic correlates of internet gambling: Findings from the 2007 British gambling prevalence survey. Cyberpsychology and Behavior , 12(2), 199–202. 10.1089/cpb.2008.0196. [DOI] [PubMed] [Google Scholar]
- Griffiths, M. D. , & Wood. (2007). Adolescent Internet gambling: Preliminary results of a national survey. Education & Health , 25(2), 23–27. [Google Scholar]
- Gunuc, S. , & Kayri, M. (2010). The profile of internet dependency in Turkey and development of internet addiction scale: Study of validity and reliability. Hacettepe University Journal of Education , 39, 220–232. [Google Scholar]
- Hollén, L. , Dörner, R. , Griffiths, M. D. , & Emond, A. (2020). Gambling in young adults aged 17–24 Years: A population-based study. Journal of Gambling Studies , 36(3), 747–766. 10.1007/s10899-020-09948-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hubert, P. , & Griffiths, M. D. (2018). A comparison of online versus offline gambling harm in Portuguese pathological gamblers: An empirical study. International Journal of Mental Health and Addiction , 16(5), 1219–1237. 10.1007/s11469-017-9846-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jessor, R. (1991). Risk behavior in adolescence: A psychosocial framework for understanding and action. Journal of Adolescent Health , 12(8), 597–605. 10.1016/1054-139X(91. [DOI] [PubMed] [Google Scholar]
- Kang, K. , Ok, J. S. , Kim, H. , & Lee, K.-S. (2019). The gambling factors related with the level of adolescent problem gambler. International Journal of Environmental Research and Public Health , 16(12), 2110. 10.3390/ijerph16122110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King, D. L. , Delfabbro, P. H. , Kaptsis, D. , & Zwaans, T. (2014). Adolescent simulated gambling via digital and social media: An emerging problem. Computers in Human Behavior , 31(1), 305–313. 10.1016/j.chb.2013.10.048. [DOI] [Google Scholar]
- King, D. L. , Russell, A. , & Hing, N. (2020). Adolescent land-based and internet gambling: Australian and international prevalence rates and measurement issues. Current Addiction Reports , 7(2), 137–148. 10.1007/s40429-020-00311-1. [DOI] [Google Scholar]
- Kristiansen, S. , & Severin, M. C. (2020). Loot box engagement and problem gambling among adolescent gamers: Findings from a national survey. Addictive Behaviors , 103. 10.1016/j.addbeh.2019.106254. [DOI] [PubMed] [Google Scholar]
- Lawn, S. , Oster, C. , Riley, B. , Smith, D. , Baigent, M. , & Rahamathulla, M. (2020). A literature review and gap analysis of emerging technologies and new trends in gambling. International Journal of Environmental Research and Public Health , 17(3), 744. 10.3390/ijerph17030744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lesieur, H. R. , & Blume, S. B. (1987). The South Oaks gambling screen (SOGS): A new instrument for the identification of pathological gamblers. American Journal of Psychiatry , 144(9), 1184–1188. 10.1176/ajp.144.9.1184. [DOI] [PubMed] [Google Scholar]
- Lorains, F. K. , Cowlishaw, S. , & Thomas, S. A. (2011). Prevalence of comorbid disorders in problem and pathological gambling: Systematic review and meta-analysis of population surveys: Comorbid disorders in pathological gambling. Addiction , 106(3), 490–498. 10.1111/j.1360-0443.2010.03300.x. [DOI] [PubMed] [Google Scholar]
- Matthews, N. , Farnsworth, B. , & Griffiths, M. D. (2009). A pilot study of problem gambling among student online gamblers: Mood states as predictors of problematic behavior. Cyberpsychology and Behavior , 12(6), 741–745. 10.1089/cpb.2009.0050. [DOI] [PubMed] [Google Scholar]
- Mcbride, J. , & Derevensky, J. (2012). Internet gambling and risk-taking among students: An exploratory study. Journal of Behavioral Addictions , 1(2), 50–58. 10.1556/JBA.1.2012.2.2. [DOI] [PubMed] [Google Scholar]
- McCormack, A. , Shorter, G. W. , & Griffiths, M. D. (2013). An examination of participation in online gambling activities and the relationship with problem gambling. Journal of Behavioral Addictions , 2(1), 31–41. 10.1556/JBA.2.2013.1.5. [DOI] [PubMed] [Google Scholar]
- McCormack, A. , Shorter, G. W. , & Griffiths, M. D. (2014). An empirical study of gender differences in online gambling. Journal of Gambling Studies , 30(1), 71–88. 10.1007/s10899-012-9341-x. [DOI] [PubMed] [Google Scholar]
- Molinaro, S. , Benedetti, E. , Scalese, M. , Bastiani, L. , Fortunato, L. , Cerrai, S. , … Urdih Lazar, T. (2018). Prevalence of youth gambling and potential influence of substance use and other risk factors throughout 33 European countries: First results from the 2015 ESPAD study. Addiction (Abingdon, England) , 113(10), 1862–1873. 10.1111/add.14275. [DOI] [PubMed] [Google Scholar]
- Olason, D. T. , Kristjansdottir, E. , Einarsdottir, H. , Haraldsson, H. , Bjarnason, G. , & Derevensky, J. L. (2011). Internet gambling and problem gambling among 13 to 18 Year old adolescents in Iceland. International Journal of Mental Health and Addiction , 9(3), 257–263. 10.1007/s11469-010-9280-7. [DOI] [Google Scholar]
- Petry, N. M. , Blanco, C. , Auriacombe, M. , Borges, G. , Bucholz, K. , Crowley, T. J. , … O’Brien, C. (2014). An overview of and rationale for changes proposed for pathological gambling in DSM-5. Journal of Gambling Studies , 30(2), 493–502. 10.1007/s10899-013-9370-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Potenza, M. N. , Balodis, I. M. , Derevensky, J. , Grant, J. E. , Petry, N. M. , Verdejo-Garcia, A. , & Yip, S. W. (2019). Gambling disorder. Nature Reviews Disease Primers , 5(1), 51. 10.1038/s41572-019-0099-7. [DOI] [PubMed] [Google Scholar]
- Potenza, M. N. , Wareham, J. D. , Steinberg, M. A. , Rugle, L. , Cavallo, D. A. , Krishnan-Sarin, S. , & Desai, R. A. (2011). Correlates of at-risk/problem internet gambling in adolescents. Journal of the American Academy of Child and Adolescent Psychiatry , 50(2), 150–159.e3. 10.1016/j.jaac.2010.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salmela-Aro, K. (2011). Stages of adolescence. En Encyclopedia of adolescence (pp. 360–368). Elsevier. 10.1016/B978-0-12-373951-3.00043-0. [DOI] [Google Scholar]
- Shaffer, H. J. , LaBrie, R. , Scanlan, K. M. , & Cummings, T. N. (1994). Pathological gambling among adolescents: Massachusetts gambling screen (MAGS). Journal of Gambling Studies , 10(4), 339–362. 10.1007/BF02104901. [DOI] [PubMed] [Google Scholar]
- Shamseer, L. , Moher, D. , Clarke, M. , Ghersi, D. , Liberati, A. , Petticrew, M. , … the PRISMA-P Group . (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ , 349(Jan02 1), g7647–g7647. 10.1136/bmj.g7647. [DOI] [PubMed] [Google Scholar]
- Steele, J. L. , & Peralta, R. L. (2020). Are polydrug users more physically and verbally aggressive? An assessment of aggression among mono- versus polydrug users in a university sample. Journal of Interpersonal Violence , 35(21–22), 4444–4467. 10.1177/0886260517715024. [DOI] [PubMed] [Google Scholar]
- Stinchfield, R. (2002). Reliability, validity, and classification accuracy of the South Oaks Gambling Screen (SOGS). Addictive Behaviors , 27(1), 1–19. 10.1016/S0306-4603(00)00158-1. [DOI] [PubMed] [Google Scholar]
- Stinchfield, R. (2003). Reliability, validity, and classification accuracy of a measure of DSM-IV diagnostic criteria for pathological gambling. American Journal of Psychiatry , 160(1), 180–182. 10.1176/appi.ajp.160.1.180. [DOI] [PubMed] [Google Scholar]
- Stinchfield, R. (2010). A critical review of adolescent problem gambling assessment instruments. International Journal of Adolescent Medicine and Health , 22(1), 77–93. [PubMed] [Google Scholar]
- Tremblay, J. , Stinchfield, R. , Wiebe, J. , & Wynne, H. (2010). Canadian adolescent gambling inventory (CAGI) phase III final report . Canadian Centre on Substance Abuse. https://prism.ucalgary.ca. [Google Scholar]
- Turner, N. E. , Elton-Marshall, T. , Shi, J. , Wiebe, J. , Boak, A. , van der Maas, M. , & Mann, R. E. (2018). Cross Validation of the gambling problem severity subscale of the Canadian adolescent gambling index (CAGI/GPSS) on a sample of Ontario high school students. Journal of Gambling Studies , 34(2), 521–537. 10.1007/s10899-017-9731-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Volberg, R. A. , Gupta, R. , Griffiths, M. D. , Ólason, D. T. , & Delfabbro, P. (2010). An international perspective on youth gambling prevalence studies. International Journal of Adolescent Medicine and Health , 22(1), 3–38. 10.1515/IJAMH.2010.22.1.3. [DOI] [PubMed] [Google Scholar]
- Volberg, R. A. , McNamara, L. M. , & Carris, K. L. (2018). Risk factors for problem gambling in California: Demographics, comorbidities and gambling participation. Journal of Gambling Studies , 34(2), 361–377. 10.1007/s10899-017-9703-5. [DOI] [PubMed] [Google Scholar]
- Waldron, H. B. (1998). Substance abuse disorders. En Comprehensive clinical psychology (pp. 539-563). Elsevier. 10.1016/B0080-4270(73)00255-8. [DOI] [Google Scholar]
- Wardle, H. (2019). The same or different? Convergence of skin gambling and other gambling among children. Journal of Gambling Studies , 35(4), 1109–1125. 10.1007/s10899-019-09840-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whiting, P. , Savović, J. , Higgins, J. P. T. , Caldwell, D. M. , Reeves, B. C. , Shea, B. , … Churchill, R. (2016). ROBIS: A new tool to assess risk of bias in systematic reviews was developed. Journal of Clinical Epidemiology , 69, 225–234. 10.1016/j.jclinepi.2015.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wijesingha, R. , Leatherdale, S. T. , Turner, N. E. , & Elton-Marshall, T. (2017). Factors associated with adolescent online and land-based gambling in Canada. Addiction Research and Theory , 25(6), 525–532. 10.1080/16066359.2017.1311874. [DOI] [Google Scholar]
- Winters, K. C. , Stinchfield, R. , & Fulkerson, J. (1993). Toward the development of an adolescent gambling problem severity scale. Journal of Gambling Studies , 9(1), 63–84. 10.1007/BF01019925. [DOI] [Google Scholar]
- Wong, I. L. K. (2010). Internet gambling: A school-based survey among Macau students. Social Behavior and Personality , 38(3), 365–372. 10.2224/sbp.2010.38.3.365. [DOI] [Google Scholar]
- Wong, & So, E. M. (2014). Internet gambling among high school students in Hong Kong. Journal of Gambling Studies/Co-sponsored by the National Council on Problem Gambling and Institute for the Study of Gambling and Commercial Gaming , 30(3), 565–576. 10.1007/s10899-013-9413-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization . (2018). The international classification of diseases (ICD-11), eleventh revision . Agencia Estatal Boletín Oficial del Estado. [Google Scholar]
- Yazdi, K. , & Katzian, C. (2017). Addictive potential of online-gambling. A prevalence study from Austria. Psychiatria Danubina , 29(3), 376–378. 10.24869/psyd.2017.376. [DOI] [PubMed] [Google Scholar]
- Zendle, D. , Meyer, R. , & Over, H. (2019). Adolescents and loot boxes: Links with problem gambling and motivations for purchase. Royal Society Open Science , 6(6). 10.1098/rsos.190049. [DOI] [PMC free article] [PubMed] [Google Scholar]