

ABSTRACT
Introduction
Upper Gastrointestinal Endoscopy is a frequently advised investigation for upper abdominal symptoms. Studies have questioned the appropriateness of indications for upper gastrointestinal endoscopy and have shown that inappropriate indications range from 5% to 49%. The unnecessary upper gastrointestinal endoscopy expose patients to the risk. The number of upper gastrointestinal endoscopy is rising in our region and we assume so is the number of unnecessary upper gastrointestinal endoscopy. With an aim to find out the appropriateness of the indications of upper gastrointestinal endoscopy and compare its association with positive findings, we conducted a cross-sectional descriptive study.
Methods
All patients undergoing diagnostic upper gastrointestinal endoscopy during study period were included in the study. Appropriateness of indications for upper gastrointestinal endoscopy was defined as per American Society for Gastrointestinal Endoscopy criteria as “appropriate” and “inappropriate”. Upper gastrointestinal endoscopy findings were classified as “significant” and “insignificant” based on endoscopy findings. The extent of this association between appropriateness of indications and upper gastrointestinal endoscopy findings was expressed as the odds ratio of finding a relevant diagnosis in patients with an “appropriate” indication compared with those with an ‘inappropriate'’ indication.
Results
Seventy-nine patients were included in the study. Fifty- two (65.8%) of the indications were considered appropriate as per American Society for Gastrointestinal Endoscopy guidelines. Thirty-three (63.5%) of the appropriate indications has clinically significant finding as compared to seven (25.9%) of inappropriate indication with an odds ratio of 4.962 (95% CI:1.773 – 13.890, P=0.002) which is statistically significant.
Conclusions
Appropriate indications have significantly higher rates of clinically significant findings. Use of guidelines may decrease the number of unnecessary procedures.
Keywords: appropriateness, endoscopy, guidelines, indications
INTRODUCTION
Upper Gastrointestinal Endoscopy (UGIE) is a useful investigation. It is frequently advised investigations for upper abdominal symptoms. UGIE is an invasive procedure with risks and complications. Studies have questioned the appropriateness of indications for UGIE and have shown that inappropriate indications range from 5% to 49%.1–3
These unnecessary UGIE expose patients to the risks of the procedure and results in increased waiting period and increased health care expenses. The American Society for Gastrointestinal Endoscopy (ASGE) guidelines have been used to define the appropriateness of the indications.4–9 The number of UGIE is rising in our region and we assume so is the number of unnecessary UGIE. To the best of our knowledge, there are no studies regarding the appropriateness of UGIE indication in our country.
With an aim to find out the appropriateness of the indications of UGIE and compare its association with positive findings, we conducted a cross-sectional descriptive study.
METHODS
This is a cross-sectional study conducted in, Department of Surgery, Kathmandu Medical College Teaching Hospital, Sinamangal, Kathmandu from February 2017 to May 2017.
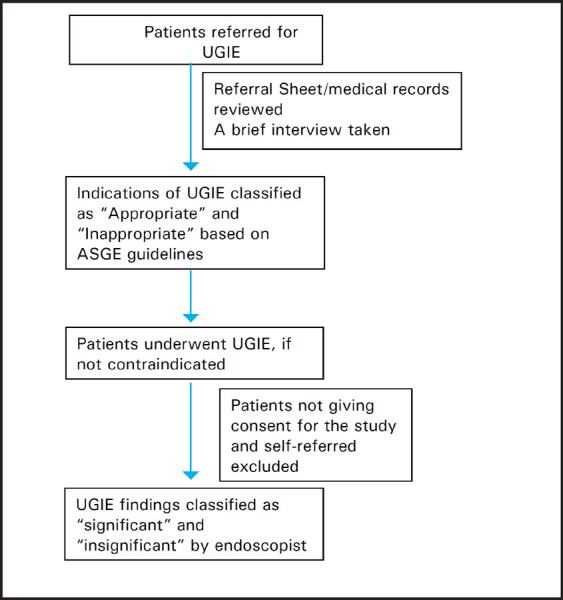
All the patient referred and undergoing diagnostic UGIE at Endoscopy unit, Kathmandu Medical College Teaching Hospital on scheduled day of the author and co-authors were included in the study. Patients not giving consent for the study and self-referred patients for UGIE were excluded from the study. Informed written consent was taken from the patient for the study.
Patients referral sheet or the medical records, history and physical examination were reviewed before the procedure. A brief interview was taken before the procedure to evaluate the indications and rule out contraindications for the procedure. The indication for the UGIE based on information provided by referring physician and brief interview before the procedure was studied and compared with ASGE guidelines. If the information provided by referring doctor is not clear or did not match to the history provided by patient, the indication was confirmed based on the brief interview. The indications of UGIE were classified as “appropriate” if the indication is included in the generally indicated category of ASGE guidelines and “inappropriate” if the indication is included in generally not indicated category or not mentioned anywhere of ASGE guidelines. Appropriateness of the indication was classified before initiating the procedure. UGIE was performed in all patients if not contraindicated. UGIE was performed by the experienced endoscopists or trainee residents under the supervision of the endoscopist according to predefined weekly schedules. All procedures were performed using forward viewing upper gastrointestinal endoscope under topical anaesthesia. UGIE was reported as per Atlas of Gastrointestinal Endoscopy and Related Pathology.10 UGIE diagnosis was classified as “significant” and “insignificant” based on the findings by the endoscopist. In the case of doubt, the significance of the UGIE finding was classified on the consensus of two endoscopists. Patients age, sex, referring department or hospital (if referred from another hospital), an indication of UGIE, appropriateness of the indications as per ASGE guidelines, endoscopic diagnosis and significance of UGIE findings were noted in case report form.
Figure 1. Flowchart of study design.
Approval was taken from the institutional review board.
With a 95% confidence interval, the error of 10% and 27% proportion of inappropriate indications following formula was used to calculate sample size.
Continuous data are presented as median (range). Dichotomous data and counts are presented as frequencies. The significant and insignificant UGIE findings were compared with that of appropriate and inappropriate indications. Association between significant UGIE diagnosis in patients with appropriate indication was compared with that of inappropriate indications. The extent of this association was expressed as the odds ratio (OR) of finding a relevant diagnosis in patients with an “appropriate” indication compared with those with an ‘inappropriate'’ indication. The x2 test was used for analysis of nominal data. Considering appropriate indication as diagnostic test sensitivity and specificity was calculated. P<0.05 was considered statistically significant. Statistical analysis was done using SPSS® version 20 (IBM, Armonk, New York, USA).
RESULTS
Eighty-eight patients were referred for diagnostic UGIE during the study period to the scheduled days of author and co-authors. Four patients were unfit for the procedure. Out of four patients, 2 patients were hypotensive even with inotrope support and 2 patients had dyspnea at rest. Eighty-four diagnostic UGI endoscopies were done. Five patients were self-referred, hence excluded from the study. Seventy-nine patients were included in the study.
The median age of the patients was 48 years (standard deviation- 19.038). There were 47 (59.5%) male and 32 (40.5%) female patients. 55 (69.6%) patients were referred from medicine department (Table 1).
Table 1. Patient's referral according to the speciality.
| Department | Frequency (Percentage) n (%) |
|---|---|
| Medicine | 55 (69.6%) |
| Surgery | 17 (21.5%) |
| Emergency | 2 (2.5%) |
| ENT | 2 (2.5%) |
| Psychiatry | 2 (2.5%) |
| Paediatrics | 1 (1.3%) |
Fifty- two (65.8%) of the indications were considered appropriate and 27 (34.2%) as per ASGE guidelines. Most common indication in the “appropriate indication group” was upper abdominal symptoms or dyspepsia that persist despite an appropriate trial of therapy with two weeks of proton pump inhibitor and most common indication in the “inappropriate indication group” was upper abdominal symptoms or dyspepsia without an appropriate trial of therapy (Table 2).
Table 2. UGIE Indications according to appropriateness as per ASGE guidelines.
| Appropriate Indication Group | Inappropriate Indication Group | ||
|---|---|---|---|
| Indications | appropriate) n (%) | Indications | inappropriate n (%) |
| Upper abdominal symptoms/ dyspepsia that persists despite an appropriate trial of therapy | 23 (44.2%) | Upper abdominal symptoms/dyspepsia without an appropriate trial of therapy | 20 (74.1%) |
| Metastatic carcinoma of unknown | |||
| UGI bleeding | 11 (21.2%) | primary site when the results will not alter management | 1 (3.7%) |
| Chronic Liver Disease with suspected portal hypertension | 7 (13.5%) | Persistent Throat Pain | 1 (3.7%) |
| Upper abdominal symptoms associated with other symptoms or signs suggesting structural disease | 4 (7.7%) | Follow up for benign condition | 2 (7.4%) |
| Persistent Vomiting of Unknown Cause | 2 (3.8%) | Cholelithiasis in elderly for evaluation before cholecystectomy | 1 (3.7%) |
| Dysphagia | 3 (5.8%) | Evaluation of chronic abdominal pain | 2 (7.4%) |
| Follow up for malignant disease | 1 (1.9%) | ||
| Iron Deficiency Anemia | 1 (1.9%) | ||
| Total | 52 (100%) | Total | 27 (100%) |
Most common diagnosis in the “appropriate indication group” was erosive gastritis whereas in “inappropriate indication group” it was normal UGIE as expected (Table 3). There were two patients diagnosed with oesophagal malignancy and both were in “appropriate indication group”.
Table 3. UGIE diagnosis according to appropriateness.
| Appropriateness as per ASGE guidelines | ||
|---|---|---|
| UGIE Diagnosis | Appropriate n (%) | Inappropriate n (%) |
| Erosive Gastritis | 20 (38.5%) | 5 (18.5%) |
| Duodenitis | 2 (3.8%) | 2 (7.4%) |
| Esophageal Varices | 5 (9.6%) | 0 (0.0%) |
| Esophagitis | 4 (7.7%) | 0 (0.0%) |
| Malignancy | 2 (3.8%) | 0 (0.0%) |
| Hiatus Hernia | 1 (1.9%) | 0 (0.0%) |
| Duodenal Ulcer | 2 (3.8%) | 0 (0.0%) |
| Normal | 16 (30.8%) | 20 (74.1%) |
| Total | 52 (100%) | 27 (100%) |
Thirty-three (63.5%) patients in “appropriate indication group” had clinically “significant” finding at UGIE whereas 7 (25.9%) in “inappropriate indication group” had a clinically “significant” diagnosis. (Table 5). Appropriateness of the indication had sensitivity of 82.5% and specificity of 51.3% to predict a clinical significant diagnosis in UGIE with odds ratio of 4.962 (95% CI: 1.773 – 13.890, p =0.002) and relative risk of getting clinically significant diagnosis of 2.448 (95% CI: 1.252 - 4.784) (Table 4).
Table 4. Clinical Significant diagnosis according to appropriateness of indications.
| Clinical Significance | Odds Ratio (95% CI) | |||
|---|---|---|---|---|
| Appropriateness of indication as per ASGE guidelines | Clinically Significant | Clinically Insignificant | Total | |
| n (%) | n (%) | |||
| Appropriate | 33 (63.5%) | 19 (36.5%) | 52 (100%) | 4.962 (1.77313.890), P =0.002) |
| Inappropriate | 7 (25.9%) | 20 (74.1%) | 27 (100%) | P =0.002* |
Chi-square Test
DISCUSSION
Upper gastrointestinal endoscopy (UGIE) is a useful and popular tool to diagnose or rule out pathology related to the esophagus, stomach, first and second part of the duodenum. It is one of the frequently advised investigations by the physicians, surgeons and other specialist for a wide range of symptoms. It is well known among the general public as a safe and effective procedure to diagnose or rule out upper gastrointestinal diseases including cancer. Sometimes patient demand for the procedure for related and unrelated symptoms. UGIE is relatively safe procedure but it is an invasive procedure with potential complications. Though rare, complications of UGIE includes cardiopulmonary complications, bleeding, perforations, infectious complication including iatrogenic infection and rarely death.11–14
Open access endoscopy is in practice at many centres worldwide which do not require specialist consultation for scheduling UGIE. This has reduced the number of patients visiting specialist but has increased the number of UGIE procedures prescribed.15–17 Literature suggests that this has resulted in an increase in a number of unnecessary procedures which range from 5 to 49%.1–3 About half of the patients are undergoing unnecessary invasive procedure which has potential complications. Unnecessary extra procedure results in an increase in the cost of treatment, longer waiting time for the procedure and delay in diagnosis of the patient with the actual disease, rush and increased workload in endoscopic units which may result in inefficiency at work. Our endoscopy unit also operates similarly to open access endoscopy units where any physicians or surgeon or any other specialist from any department within the hospital and from another hospital can ask for UGIE. Sometimes patients themselves also request for UGIE for their symptoms.
The current study reports 34.2% of the endoscopic procedure were done for the inappropriate indications as per ASGE guidelines. This is comparable to 31.3% of inappropriate indications reported in a retrospective study by Aljebreen et al using ASGE criteria.5 This finding is also comparable to Froehlich et al from Switzerland who has reported 40% inappropriate indications.3 65.8% of appropriate indication is slightly less than reported by Hassan et al who reported 77.1% appropriate indications.6 Similarly, our appropriate rate of indication was also less than reported by Mudwai et al, Chan et al, Keren et al and Rossi et al's report of 86%, 88.3%, 84.1% and 88.4% appropriate indications respectively.2,7,18,19 A meta-analysis of 13856 patients also reported 88% of appropriate indications which is also higher than our rate of appropriate indications.9
The current study showed that 63.5% of the appropriate indications has clinically significant finding as compared to 25.9% of inappropriate indication with an odds ratio of 4.962 (95% confidence interval: 1.773-13.890, p = 0.002) which is statistically significant. These findings collaborate with the large prospective Italian multicenter study with 7270 patients across 44 centres which reported odds ratio of 2.65 (99% confidence interval [CI] 2.23-3.20; P<.01) for appropriate indications compared to the inappropriate indication.6 Though seven (25.9%) patients in the appropriate group had positive findings on UGIE, but it was limited to erosive gastritis and duodenitis, none of the patients in “appropriate indication” group had a serious illness like oesophagal varices, esophagitis, ulcers or malignancy. This is comparable to Hassan et al report of 1 (0.07%) malignant case in inappropriate indication group out of 133 (2.7%) malignant cases detected in the study.6 However, in a large retrospectiive study of nine years audit with 20,620 patients, Keren et al found 284 patients (1.38%) esophageal malignancies out of which 263 (1.28%) had an appropriate indication and 21 (0.10%) had inappropriate indication as per ASGE guidelines.19 Similarly they also found 440 (2.13%) gastric malignancies out of which 392 (1.90%) had appropriate indication and 48 (0.23%) had inappropriate indications.19 The difference from our findings with this large study may be due to small sample size in our study. Hence, guidelines should be used cautiously in order not to miss important diagnosis and the clinical suspician and clinical judgements should always come before the guidelines.
The role of negative endoscopic findings on the reassurance of patients, their satisfaction and quality of life after exclusion of serious diseases cannot be undermined for patients even with the inappropriate indication.20,21 In a study on the positive impact of negative endoscopy on the quality of life in dyspepsia, Wiklunds and colleagues found that there was an improvement in the quality of life including sleep score and physical activity despite the change in symptoms.22 Similarly in a retrospective study it was found that 333 (69)% of endoscopies had positive findings but when the result of endoscopies were classified as helpful and unhelpful, 404 (84%) findings were judged helpful in the sense of influencing management.23
Sensitivity and specificity of appropriate indication for diagnosis of clinically significant pathology at UGIE are 82.5% and 51.3% in this study. This is comparable to Buri et al who reported sensitivity 88% and specificity 35% but higher than Aljebreen et al report of 70.3% and 35%.5,24
Most common indication in current study was upper abdominal symptoms/dyspepsia that persists despite an appropriate trial of therapy which is similar to study from Malaysia and Saudi Arab.25 It is different from the study from Sudan which reports most common indication as upper abdominal symptoms associated with other symptoms or signs suggesting serious organic disease (e.g., anorexia and weight loss) or in patients over 45 years of age.7
It is apparent that adherence to the guidelines for appropriate indications increases the diagnostic yield of UGIE and decreases unnecessary procedures resulting in a decrease in cost, decrease in the waiting period for actual needy patients. However, the guidelines developed for the western world may not be applicable as it is to our region with different geography, population, a different pattern of diseases and non-availability of endoscopes in remote areas. The guidelines need to be developed or modified for our region in order to rationalise the use of limited resources.
This study has certain limitations. This is a single centre study and the findings may not be generalised although it is expected that there would be similar scenario at other tertiary centres of this region. As the endoscopists were not blinded from the appropriateness of the indications, performance and reporting bias cannot be ruled out.
CONCLUSIONS
Appropriate indications of UGIE have significantly higher rates of clinically significant findings. Use of appropriate guidelines for indications of UGIE may decrease the number of unnecessary procedures. However, clinical suspicion and clinical judgement should come before the guidelines to get maximum benefits for the patients and avoid unnecessary procedures.
Conflict of Interest
None.
REFERENCES
- 1.Mahajan RJ, Barthel JS, Marshall JB. Appropriateness of referrals for open-access endoscopy. How do physicians in different medical specialties do? Arch Intern Med. 1996 Oct 14;156(18):2065–9. [PubMed] [Google Scholar]
- 2.Chan Y-M, Goh K-L. Appropriateness and diagnostic yield of EGD: a prospective study in a large Asian hospital. Gastrointest Endosc. 2004 Apr;59(4):517–24. doi: 10.1016/s0016-5107(04)00002-1. [DOI] [PubMed] [Google Scholar]
- 3.Froehlich F, Burnand B, Pache I, Vader JP, Fried M, Schneider C, et al. Overuse of upper gastrointestinal endoscopy in a country with open-access endoscopy: a prospective study in primary care. Gastrointest Endosc. 1997 Jan;45(1):13–9. [PubMed] [Google Scholar]
- 4.Early DS, Ben-Menachem T, Decker GA, Evans JA, Fanelli RD, Fisher DA, et al. Appropriate use of GI endoscopy. Gastrointest Endosc. 2012;75(6):1127–31. doi: 10.1016/j.gie.2012.01.011. [DOI] [PubMed] [Google Scholar]
- 5.Aljebreen AM, Alswat K, Almadi MA, Aljebreen AM, Alswat K. Appropriateness and Diagnostic Yield of Upper Gastrointestinal Endoscopy in an Open-Access Endoscopy System. Saudi J Gastroenterol. 2013;19(5):219–22. doi: 10.4103/1319-3767.118128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hassan C, Bersani G, Buri L, Zullo A, Anti M, Bianco MA, et al. Appropriateness of upper-GI endoscopy : an Italian survey on behalf of the Italian Society of Digestive Endoscopy. Gastrointest Endosc. May 2007;65(6):767–74. doi: 10.1016/j.gie.2006.12.058. [DOI] [PubMed] [Google Scholar]
- 7.Mudawi HMY, Khogalie AA, El MA, Mohamed HME. Appropriate use and diagnostic yield of upper gastrointestinal endoscopy in a tertiary referral hospital. Arab J Gastroenterol. 2012;13(3):145–7. doi: 10.1016/j.ajg.2012.08.009. [DOI] [PubMed] [Google Scholar]
- 8.Froehlich F, Repond C, Müllhaupt B, Vader JP, Schneider C, Pache I, et al. Is the diagnostic yield of upper GI endoscopy improved by the use of explicit panel-based appropriateness criteria? Gastrointest Endosc. 2000 Sep;52(3):333–41. doi: 10.1067/mge.2000.107906. [DOI] [PubMed] [Google Scholar]
- 9.Di Giulio E, Hassan C, Marmo R, Zullo A, Annibale B, Giulio E Di, et al. Appropriateness of the indication for upper endoscopy : A meta-analysis. Dig Liver Dis. 2010 Feb;42(2):122–6. doi: 10.1016/j.dld.2009.04.019. [DOI] [PubMed] [Google Scholar]
- 10.Schiller KFR, Cockel R, Hunt RH, Warren BF, editors. Atlas of Gastrointestinal Endoscopy and Related Pathology. 2nd. Massachusetts: Blackwell Science Ltd; 2002. [Google Scholar]
- 11.Ben-Menachem T, Decker GA, Early DS, Evans J, Fanelli RD, Fisher DA, et al. Adverse events of upper GI endoscopy. Gastrointest Endosc. 2012 Oct;76(4):707–18. doi: 10.1016/j.gie.2012.03.252. [DOI] [PubMed] [Google Scholar]
- 12.Froehlich F, Gonvers JJ, Vader JP, Dubois RW, Burnand B, Froehlich F, et al. Appropriateness of Gastrointestinal Endoscopy : Risk of Complications. Endoscopy. 1999;31(8):684–6. doi: 10.1055/s-1999-130. [DOI] [PubMed] [Google Scholar]
- 13.Hart R, Classen M. Complications of Diagnostic Gastrointestinal Endoscopy. Endoscopy. 1990 Sep 17;22(5):229–33. doi: 10.1055/s-2007-1010734. [DOI] [PubMed] [Google Scholar]
- 14.Guidelines on Complications of Gastrointestinal Endoscopy | Endoscopy | Clinical Guidelines.
- 15.Silcock JG, Bramble MG. Open access gastroscopy: second survey of current practice in the United Kingdom. Gut. 1997 Feb;40(2):192–5. doi: 10.1136/gut.40.2.192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hughes-Anderson W, Rankin SL, House J, Aitken J, Heath D, House AK. Open access endoscopy in rural and remote Western Australia: Does it work? ANZ J Surg. 2002 Oct;72(10):699–703. doi: 10.1046/j.1445-2197.2002.02535.x. [DOI] [PubMed] [Google Scholar]
- 17.Marshall JB. Open access endoscopy in Britain: a service in evolution. Gastrointest Endosc. 1998 Dec;48(6):653–8. [PubMed] [Google Scholar]
- 18.Rossi A, Bersani G, Ricci G, Defabritiis G, Pollino V, Suzzi A, et al. ASGE guidelines for the appropriate use of upper endoscopy: association with endoscopic findings. Gastrointest Endosc. 2002 Nov;56(5):714–9. doi: 10.1067/mge.2002.129222. [DOI] [PubMed] [Google Scholar]
- 19.Keren D, Rainis T, Stermer E, Lavy AA, Keren D, Rainis T, et al. A nine-year audit of open-access upper gastrointestinal endoscopic procedures : Results and experience of a single centre. Can J Gastroenterol. 2011;25(2):83–8. doi: 10.1155/2011/379014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chan Y, Goh K-L. Appropriateness and diagnostic yield of EGD : a prospective study in a large Asian hospital. Gastrointest Endosc. 2004 Apr;59(4):517–24. doi: 10.1016/s0016-5107(04)00002-1. [DOI] [PubMed] [Google Scholar]
- 21.Rabeneck L, Wristers K, Souchek J, Ambriz E. Impact of upper endoscopy on satisfaction in patients with previously uninvestigated dyspepsia. Gastrointest Endosc. 2003 Mar;57(3):295–9. doi: 10.1067/mge.2003.122. [DOI] [PubMed] [Google Scholar]
- 22.Wiklund I, Glise H, Jerndal P, Carlsson J, Talley NJ. Does endoscopy have a positive impact on quality of life in dyspepsia? Gastrointest Endosc. 1998 Jun;47(6):449–54. doi: 10.1016/s0016-5107(98)70243-3. [DOI] [PubMed] [Google Scholar]
- 23.Naji SA, Brunt PW, Hagen S, Mowat NA, Russell IT, Sinclair TS, et al. Improving the selection of patients for upper gastrointestinal endoscopy. Gut. 1993 Feb;34(2):187–91. doi: 10.1136/gut.34.2.187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Buri L, Hassan C, Bersani G, Anti M, Bianco MA, Cipolletta L, et al. Appropriateness Guidelines and Predictive Rules to Select Patients for Upper Endoscopy : A Nationwide Multicenter Study. Am J Gastroenterol. 2009;105(6):1327–37. doi: 10.1038/ajg.2009.675. [DOI] [PubMed] [Google Scholar]