

Abstract
This study examined the developmental pathways from fathers’ psychopathology in early childhood to child peer victimization (bullying and cyber victimization) in late adolescence via family relationships and early adolescent psychosocial functioning (anxiety, emotion regulation, social problems). A conceptual model with pathways through inter-parental aggression and fathers’ parenting (harshness and sensitivity) was tested. Participants were 227 families (51% female children recruited as infants) who participated in a longitudinal study examining the role of parental alcohol problems and associated risks on developmental and family processes from infancy to late adolescence. Multi-method (observational, parent report, adolescent report) assessments of family processes and child outcomes were conducted across all time points. Fathers’ alcohol problems and depressive symptoms in early childhood was prospectively associated with inter-parental aggression in middle childhood and social problems in early adolescence. For boys only, early adolescent social problems were predictive of bullying victimization. Fathers’ antisocial behavior in early childhood was associated with less sensitive parenting in middle childhood. Fathers’ sensitivity in middle childhood was protective, being associated with lower cyber victimization in late adolescence. Fathers’ sensitivity was also associated with higher emotion regulation in early adolescence; however, counter to expectations, higher emotion regulation was associated with more bullying and cyber victimization. Findings shed light on differences in the etiological pathways to bullying and cyber victimization, as well as how distinct forms of paternal psychopathology in early childhood associate with family relationships, child adjustment, and vulnerability to peer victimization in late adolescence.
Keywords: Fathers, Parenting, Adolescents, Peer Victimization, Etiology, Cyber Victimization
Peer victimization is highly prevalent in adolescence and includes verbal aggression (name-calling, put-downs), physical aggression (hitting, kicking, shoving), social manipulation (spreading rumors, exclusion) and property attacks (stealing, damaging property; Mynard & Joseph, 2000; Olweus, 1996). These behaviors can be perpetrated in-person through bullying or electronically through cyber victimization (Betts, Houston, & Steer 2015; Ybarra, Boyd, Korchmaros, & Oppenheim, 2012). The social and psychological toll of peer victimization may be especially harmful in adolescence due to adolescents’ heightened sensitivity to peer approval and acceptance (Steinberg, 2014). Indeed, adolescent peer victimization is associated with a host of maladaptive outcomes including internalizing problems (i.e., anxiety, depression; Farrington, Loeber, Stallings, & Ttofi, 2011; Reijntjes, Kamphuis, Prinzie, & Telch, 2010); delinquency (Wong & Schonlau, 2013); substance use (Earnshaw, Elliott, Reisner, Mrug,Windle, & Tortolero Emery, et al. 2017; Lee & Kim, 2017); and involvement in other types of violence and victimization (e.g. dating violence; Espelage & Holt, 2007; Lereya, Samara, & Wolke, 2013; Yahner, Dank, Zweig, & Lachman, 2015). Literature on the etiological pathways to peer victimization is mostly limited to in person bullying victimization and to restricted time scales (e.g., middle childhood – adolescence). Many of these studies highlight the importance of parent-child relationships as a significant etiological factor (Espelage, Low, Rao, Hong, & Little, 2014; Hong & Espelage, 2012; Lereya, Samara, & Wolke, 2013) but few have focused specifically on the role of fathers and father-child relationships in the etiological pathway to peer victimization. Those studies that have considered the unique influence of fathers on their children’s vulnerability to peer victimization have shown that poor quality father-child communication was associated with both bullying and cyber victimization (Buelga, Martínez–Ferrer, & Cava, 2017; Cunningham, Goff, Bagby, Stewart, Larocque, Mazurka, et al. 2019; Estévez, Musitu, & Herrero, 2005). However, the mechanisms through which father-child relationships increase vulnerability to, or protect children from, peer victimization have yet to be elucidated.
Theoretical models explaining the development of adolescent risk such as the dynamic cascade model of development (Dodge, Malone, Lansford, Miller-Johnson, Pettit, & Bates, 2009) suggest cascade effects from infancy with risk and protective factors at each stage of development playing a critical role in setting up pathways to risk and resilience. Consistent with this, Hong et al. (2011) proposed a theoretical framework to explain the processes through which early life experiences can contribute to involvement in peer victimization. According to Hong and colleagues, adverse childhood experiences including abuse, neglect, and exposure to family violence, negatively impact children’s psychosocial functioning, thereby contributing to problematic peer relationships and increased vulnerability to peer victimization. This framework also allows for the consideration of protective factors, such as positive parenting, that can reduce risk of peer victimization. The current study uses the theoretical framework suggested by Hong and Espelage (2012) to examine a conceptual model of the association between fathers’ psychopathology in early childhood to peer victimization in late adolescence via family relationships (family aggression, father-child interactions) in middle childhood and child anxiety, emotion dysregulation, and social problems in early adolescence.
Fathers’ Psychopathology
Three inter-related aspects of fathers’ psychopathology were included in this study: fathers’ alcohol problems, antisocial behavior, and depression. Fathers’ alcohol problems often co-occur with other comorbid disorders, particularly antisocial personality disorder (Cloninger, Sigvardsson, & Bohman, 1988; Hussong, Wirth, Edwards, Curran, Chassin, & Zucker, 2007; Hussong, Bauer, & Chassin, 2008) and depressive symptoms (for a review, see Fitzgerald & Eiden, 2007). Antisocial behaviors may include engagement in behaviors for personal gain or power, or behaviors based on exploitation, coercion, or intimidation; lack of inhibition, and being manipulative, deceitful, callous, or hostile in interactions with others (Godleski & Eiden, 2020). The role of comorbid antisocial behavior has been well studied in the alcohol literature as an important explanatory variable for heterogeneity in risk processes as described below. Similarly, it is increasingly recognized that significant levels of depressive symptoms reflecting sadness, low energy, feelings of worthlessness, and loss of enjoyment of activities are common among both mothers and fathers (Keller, Cummings, Peterson, & Davies, 2009). Fathers’ depressive symptoms in the context of an alcohol disorder may also represent the affective impact of heavy drinking and alcohol problems, and account for unique variance in child outcomes (Eiden, Lessard, Colder, Livingston, Casey & Leonard, 2016). Results from papers examining risk trajectories of children from 2 to 17 years of age and pooling data across multiple studies indicate significant increases in risk for internalizing and externalizing symptoms when parent alcohol problems were comorbid with antisocial behavior or depressive symptoms, or children had two parents with alcohol problems (Hussong, Wirth, Edwards, Curran, Chassin, & Zucker, 2007; Hussong, Bauer, & Chassin, 2008).
Fathers’ psychopathology and partner aggression
Fathers’ alcohol problems are also robustly associated with higher father to mother and mother to father aggression across a number of studies and developmental periods (e.g., Finger, Kachadourian, Molnar, Eiden, Edwards, & Leonard, 2010a; Foran & O’Leary, 2008; Marshal, 2003; O’Farrell, Murphy, Neavins, & Van Hutton, 2000). Heavy alcohol use lowers impulse control and self-regulation increasing risk for conflictual interactions becoming aggressive, an association that has been reported with higher frequency among men compared to women (Foran & O’Leary, 2008). One explanation for these associations may be the role of fathers’ depressive symptoms and antisocial behavior in negatively impacting family relationships. Fathers’ depressive symptoms is associated with problems across family relationships including father-child relationships (Cheung & Theule, 2019; deMontigny, Girard, Lacharite, Dubeau, & Devault, 2013) and marital quality (Nelson, O’Brien, Blankson, Calkins, & Keane, 2009), including greater partner conflict (Kouros, Merrilees, & Cummings, 2008). Indeed, meta-analytic reviews indicate significant moderate associations between fathers’ depressive symptoms and lower marital quality (Cheung & Theule, 2019; Cheung, Theule, Hiebert-Murphy, & Piotrowski, 2019). Similarly, studies have reported an indirect path from father’s antisocial behavior via family and parent-child conflict on externalizing behavior problems among children of fathers with alcohol problems (Loukas et al., 2001). In addition, although there is genetic risk for intergenerational transmission of antisocial behavior, additive and exacerbated risk from the caregiving or environmental context is also critical (Harold et al., 2012; Jaffee et al., 2003). Taken together, results indicate that the inter-related problems of fathers’ alcohol problems, depressive symptoms, and antisocial behavior in early childhood may be prospectively associated with higher risk for negative partner interactions and aggression.
Fathers’ Psychopathology and Parenting
Results from earlier waves of the current sample indicated significant concurrent (Eiden, Chavez, & Leonard, 1999) and prospective associations between fathers’ psychopathology (alcohol problems, depressive symptoms, and antisocial behavior) and lower paternal sensitivity and higher harshness during play interactions with their children in infancy and toddler age (see Eiden, 2018; Godleski, Eiden, Shisler, & Livingston, 2020). Similarly, results from studies of older children indicate father to child hostility as a primary mediator of associations between fathers’ antisocial behavior and child outcomes (Harold, Elam, Lewis, Rice, & Thapar, 2012). However, in many of these analyses across ages, fathers’ antisocial behavior did not account for unique variance in fathers’ parenting behaviors or child outcomes when analytic models included fathers’ alcohol problems, depressive symptoms, and other family risk factors (Eiden, Chavez, & Leonard, 1999; Eiden, Colder, Edwards, & Leonard, 2009a; Eiden, Edwards, & Leonard, 2007). Results from meta-analyses also indicate significant associations between fathers’ depressive symptoms and lower parenting quality (Cheung & Theule, 2019; Cheung, Theule, Hiebert-Murphy, & Piotrowski, 2019). In one of the few studies examining the association between fathers’ depressive symptoms and children’s emotion regulation using a longitudinal design, father-child conflictual relationship was a prospective mediator of the association between fathers’ depressive symptoms and child emotion regulation (Nath, Russell, Kuyken, Psychogiou, & Ford, 2016) – highlighting the potential role of parenting as an etiological pathway.
Family relationships, and child anxiety, emotion regulation, and social problems
There are robust linkages between family relationships that include inter-parental aggression and parenting quality and child outcomes such as anxiety, emotion regulation, and social problems. Several theoretical frameworks are supportive of associations between inter-parental aggression and children’s social functioning. For instance, social learning theories emphasize that children first gain social skills by observing their parents interacting with each other, and observations of inter-parental aggression teach children to resolve conflicts using aggression, resulting in greater social problems (Bauer, Herrenkohl, Lozano, Rivara, Hill, & Hawkins, 2006; Stocker & Youngblade, 1999). The emotional security theory suggests that the context of inter-parental aggression creates a toxic environment and maintaining safety within this context becomes a primary goal for children (Davies & Cummings, 1994; Davies & Martin, 2013). Some children may react to this toxic environment by increased emotional distress or anxiety and difficulties regulating emotions instead of imitative behavior, which in turn may increase risk for peer victimization. Similarly, there are strong theoretical and empirical linkages between parent-child relationships and peer relationships (see Hong, Espelage, Grogan-Kaylor, & Allen-Meares, 2012; Lereya, Samara, & Wolke, 2013;). Evidence indicates that children who experience greater parental harshness are less likely to defend themselves in peer contexts and are more likely to be victimized by their peers (Shields & Cicchetti, 2001). In contrast, high levels of parental sensitivity may be protective and be prospectively associated with more positive child outcomes in adolescence. Indeed, in previous waves of the current sample, there was a direct association between fathers’ warmth and sensitivity and family aggression in early childhood and children’s social competence as reported by teachers at early school age (Finger, Eiden, Edwards, & Leonard, 2010b). One goal of the current study was to examine if these prospective associations would continue into middle childhood and adolescence.
Child Outcomes
The theoretical model proposed by Hong et al (2012) highlights the importance of problematic family dynamics in early childhood as a risk factor for children’s involvement in peer victimization. Based on this model, psychosocial factors such as emotional dysregulation, social problems, and internalizing problems may serve as proximal mediators of the association between family relationships and peer victimization. The literature linking children’s emotion regulation to peer victimization is small, but consistent in indicating robust associations between greater emotion regulation and lower risk for bullying victimization (Godleski, Kamper, Ostrov, Hart, & Blakely-McClure, 2014; Shields, Dickstein, Seifer, Giusti, Dodge Magee, & Spritz, 2001). In cross-sectional studies and longitudinal studies, global measures of emotion regulation were associated with lower peer victimization across middle childhood (Garner & Waajid, 2019), in adolescence (Riley, Sullivan, Hinton, & Kliewer, 2019), and children’s emotional dysregulation (by suppression of emotional reactions) was associated with greater peer victimization in high school (Chervonsky & Hunt, 2018). In one of the few studies examining the role of emotion regulation as a prospective mediator of the association between parenting and peer relationships, Dickson et al. (2019) found that high parental engagement in belittling children in early adolescence was associated with increases in adolescent emotional dysregulation a year later. This emotional dysregulation in turn was associated with increased peer victimization the year after.
Similarly, children’s internalizing problems (e.g., anxiety) have prospective associations with victimization experiences, in addition to being a consequence of peer victimization (Hong & Espelage, 2012; McLaughlin, Hatzenbuehler, & Hilt, 2009; Reijntjes, Kamphuis, Prinzie, & Telch, 2010). Children who are anxious or depressed may be targeted for peer aggression because they are perceived as vulnerable and unlikely to defend themselves (Fekkes, Pijpers, Fredriks, Vogels, & Verloove-Vanhorick, 2006). Not surprisingly, youth who struggle with internalizing problems are also likely to have social skills deficits, contributing to poor peer relationships, social withdrawal, and friendlessness (Bornstein, Hahn, & Hayens, 2010). In addition to perceptions that these youth will not defend themselves, there may also be a perception that they are less likely to be defended by others, and that there will be few if any social repercussions for attacking them (Kljakovic & Hunt, 2016).
Few have examined the role of these child emotional and relational processes as mediators of the association between family relationships (inter-parental aggression and parenting) and peer victimization, and none have included cyber victimization in these models. Although it shares some common features with in-person bullying victimization, cyber victimization is unique in that the attacks can be reproduced, widely disseminated, and available for viewing indefinitely. Cyber victimization is also more difficult to escape; the perpetrators can be anonymous; and the attacks can occur whether or not the target is present online (Baldry, Farrington, & Sorrentino, 2015; Landoll, La Greca, Lai, Chan, & Herge, 2015; Tokunaga, 2010). In these respects, cyber victimization has the potential to be especially insidious and harmful (Landoll, La Greca, Lai, Chan, & Herge, 2015; Tokunaga, 2010). Individuals who experience cyber victimization are also highly likely to be victimized in person, although the reverse is not necessarily true (Tokunaga, 2010). Cyber victimization and bullying victimization share common risk factors including poor social skills, poor emotional control, and anxiety (see Baldry, Farrington, & Sorrentino, 2015 for a review). Nonetheless, there is a dearth of longitudinal, theoretically informed research to document the etiology of cyber victimization and to determine whether the etiology differs from that of in-person peer victimization (Baldry, Farrington, & Sorrentino, 2015).
The current study tested a conceptual model of the etiology of peer victimization from infancy to adolescence, based on the theoretical framework proposed Hong and Espelage (2012). Specifically, we sought to determine whether children exposed to paternal psychopathology (i.e., alcohol problems, antisocial behaviors, depressive symptoms) in early childhood were at risk for peer victimization in late adolescence via psychosocial factors. Two etiological pathways were considered. The first pathway was via the parental relationship, whereby, consistent with prior research (e.g., Finger, et al. 2010a), we anticipated that fathers’ psychopathology in early childhood would be predictive of intimate partner aggression among parents in middle childhood, which in turn would be positively associated with anxiety and social problems, and negatively associated with emotional regulation in early adolescence. The second pathway was via parenting behaviors. Based on prior research (e.g., Eiden et al., 2009a; Eiden et al., 2016), in this second pathway, we expected that fathers’ psychopathology would be positively associated with harsh parenting and negatively associated with sensitivity towards their child in middle childhood. In turn, we hypothesized that fathers’ harsh parenting in middle childhood would be positively associated with anxiety and social problems and inversely associated with emotion regulation in early adolescence. In contrast, we expected that fathers’ sensitivity in middle childhood would be a protective influence, and as such, it would be inversely associated with anxiety and social problems, and positively linked to emotion regulation. For both pathways, we hypothesized that anxiety and social problems in early adolescence would be positively related to peer victimization, and that emotion regulation would be negatively associated with peer victimization in late adolescence.
Another goal of the study was to determine whether the etiological pathways differed for in-person bullying and cyber forms of peer victimization. Although the two forms of peer victimization are highly related, they are also distinct in terms of how they are perpetrated and by whom (Landoll, La Greca, Lai, Chan, & Herge, 2015: Tokunga, 2010). However, given the dearth of research on the etiology of cyber victimization and the overlapping risk factors with bullying victimization, we did not have specific hypotheses about how they may differ etiologically. In addition, because there are often differences in both the in-person and cyber victimization experiences of males and females (see Baldry et al. 2015), we examined whether the pathways differed by gender. No specific hypotheses about gender were generated, given mixed findings in the research literature. To summarize, the two overall goals of the study was to 1) examine a conceptual model linking fathers’ psychopathology in early childhood to peer victimization in late adolescence, and 2) to examine this model for both in-person bullying victimization and cyber victimization.
Method
Participants
The initial sample consisted of 227 families with 12-month-old infants (116 females, 111 males) who were recruited to participate in a longitudinal study of parenting and infant development. Families were classified as being in one of two groups: the non-alcohol-problem or control group in which both parents had no or few alcohol problems since the child’s birth (n = 102) and the father alcohol problem group with families in which the father met diagnostic criteria for alcohol abuse or dependence (n = 125). Within the father alcohol problem group, 95 mothers were light drinkers or abstainers, and 30 mothers were heavy drinkers or had current alcohol problems. Given the low number of mothers who met criteria for problem drinking and the fact that in the majority of cases where mother was a problem drinker, father was also a problem drinker, classification was made on the basis of father’s alcohol status.
The majority of parents in the study were European American (94% of mothers and 87% of fathers); approximately 5% of mothers and 7% of fathers were African American and 2% of parents were Hispanic/Latino, Native American, or other. Parental education ranged from less than a high school degree to postgraduate degree, with a majority of mothers (59%) and fathers (54%) having completed at least some post-high school education. Annual family income ranged from $4,000 to $95,000 at recruitment (M = $41,824; SD = $19,423). All mothers and fathers were residing together with the target child at recruitment, and 88% of the parents were married to each other. Mothers’ and fathers’ ages at recruitment ranged from 19 to 41 years (M = 30.7, SD = 4.5) and 21 to 58 years (M = 33.0, SD = 5.9), respectively.
At the time of the current assessment, participants were adolescents whose ages ranged from 15 to 19 (M = 17.68, SD = 1.89). The majority of the adolescents identified as European American (91.9%), 2.7% identified as African American, and 5.4% as multiracial. Slightly less than 2% of the sample identified as being Hispanic/Latino. The majority of participants were in 11th (35.1%) or 12th grades (42.5%), although 18.3% were enrolled in post high school education (college or trade school) and 2.2% had dropped out before completing high school.
Procedure
Recruitment for Initial Study
The names and addresses of participating families were obtained from the New York State birth records for Erie County (see Eiden et al., 2007, for procedural details). Families that met basic eligibility criteria were sent an introductory letter. Those who returned the enclosed form indicating interest in the study were screened for eligibility over the telephone. To be eligible, parents had to be primary caregivers and cohabiting since the infant’s birth; mothers were between 18 and 40 years old at the time of the child’s birth, mothers could not have used drugs during pregnancy or in the past year (except for less than two instances of marijuana use), mothers’ average drinking was less than one drink a day during pregnancy and mothers did not drink five or more drinks on a single occasion during pregnancy. During the phone screen, the Family History Research Diagnostic Criteria for alcoholism was administered to mothers with regard to their partners’ drinking (Andreasen, John, Jean, Theodore, & William, 1986), and fathers were screened with regard to their alcohol use, problems and treatment. Because of the large pool of families potentially eligible for the control group, alcohol problem and control families were matched on race/ethnicity, maternal education, child gender, parity, and marital status.
Family lab assessments were conducted at 10 different child ages, in infancy (12 months) and early childhood (18, 24, 36, and 48 months), at kindergarten age (5–6 years of age), in middle childhood (fourth grade, about 9–10 years of age and sixth grade, about 11–12 years of age), in early adolescence (eighth grade, 13–14 years of age) and in later adolescence (11th/12th grades, 15–19 years of age). Mother-child visits were conducted first followed by father-child visits 1–2 weeks later. A parental questionnaire assessment was also conducted at 48 months. Assessments took place through parental self-reports and laboratory observations from infancy to early adolescence. Children completed interviews and questionnaires from middle childhood to late adolescence. Procedures for each wave of the study were approved by the University Institutional Review Board. Informed written consents were obtained from both parents and child assents were obtained from kindergarten-age and older children. Participants who had reached their 18th birthday by the late adolescent assessment provided informed consent. Data from infancy (12-months), early childhood (24- and 36-months), kindergarten, middle childhood (fourth and sixth grade), early adolescence (eighth grade) and late adolescence (11th - 12th grade) were used in the current analyses.
Measures
Fathers’ Alcohol Use
An adapted, self-report measure of The University of Michigan Composite International Diagnostic Interview (Anthony, Warner, & Kessler, 1994; Kessler, McGonagle, Zhao, Nelson, Hughes, & Eshleman et al, 1994) was used to assess paternal alcohol abuse and dependence when infants were 12 months old. Questions were reworded to inquire as to “how many times” problems had been experienced, as opposed to whether it happened “very often.”
In addition to the screening criteria, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV; American Psychiatric Association, 2000) criteria for alcohol abuse and dependence diagnoses for current alcohol problems (in the past year) were used to assign final diagnostic group status. In order to meet alcohol abuse criteria, recurrent alcohol problems were those occurring at least 3–5 times in the past year or 1–2 times in three or more problem areas. Families in which parents met diagnostic criteria on the screener and questionnaire were assigned to the alcohol problem group at the first assessment.
Fathers’ Depressive Symptoms
The Center for Epidemiological Studies Depression scale (CES-D; Radloff, 1977) was used to measure fathers’ depressive symptoms at 4 time points (12, 18, 24, and 36 months of child age). The CES-D is a scale designed to measure depressive symptoms in community populations. It is a widely used, self-report measure with high internal consistency and strong test–retest reliability (Boyd, Weissman, Thompson, & Myers, 1982). Paternal depressive symptoms were fairly stable, with across time correlations ranging from 0.49 to 0.72. Fathers’ scores on this measure were averaged across time and the internal consistency of this final composite variable was high (Cronbach’s α = .88).
Fathers’ Antisocial Behavior
Paternal antisocial behavior was assessed using a modified, 28-item version on the Antisocial Behavior Checklist (Ham, Zucker, & Fitzgerald, 1993; Zucker and Noll, 1980) at the 12-month visit. Because it is a measure of lifetime antisocial behavior, this assessment was used at only one time point. Fathers rated the frequency with which they engaged in a variety of antisocial and aggressive behaviors (e.g., resisting arrest or being fired). Scores for each item range from 1 “Never” to 4 “Often” with higher scores reflecting more antisocial behavior. Possible scores range from 28 to 112 and scores for the current sample ranged from 29 to 86. The internal consistency for the current sample was quite high (Cronbach’s α = .82). The scores were skewed and transformed using square root transformations.
Inter-Parental Aggression
Mothers and fathers reported on physical and verbal intimate partner aggression measured during the kindergarten and fourth grade assessments. Physical aggression was measured using the Conflict Tactics Scale (CTS; Straus, 1979). In the current study, items focusing on moderate (e.g., push, grab, or shove) to severe (e.g., hit with fist) physical aggression, but not very severe items (e.g., burnt or scalded, use of weapons), were included. The severe items of the CTS were excluded because our pilot study indicated that the base rates of these behaviors in community recruited sample of new parents was extremely low (none were endorsed) and we were concerned about participant burden given the length of the questionnaires. The Pearson correlation coefficients between mother and fathers reports on the CTS ranged from r = .34, p = .00 to r = .88, p = .00. Parents reported the frequency of their own and their partners’ physical aggression toward one another over the past 12 months on a seven-item scale ranging from 0 “0 times” to 6 “20 or more times.” Due to under-reporting of aggressive behaviors, especially by men (Archer, 2002), indicators of each variable were created by taking the maximum of the mother and father reports (Cronbach’s αs = .82, .86).
Fathers’ Sensitivity
During the kindergarten assessment, fathers were asked to decorate a picture frame with their children for 20 minutes. This interaction was coded using the Iowa Family Interaction Rating Scales (Melby, Conger, Book, Rueter, Lucy, & Repinski et. al, 1998). These rating scales were designed to measure both verbal and non-verbal behaviors as well as affective aspects of the interactions along nine-point rating scales. The sensitivity composite included items such as positive reinforcement, sensitive child centered behaviors, humor, positive mood, warmth-support, prosocial behaviors, and physical affection. The internal consistency for this composite scale was quite high (Cronbach’s α = .94).
Two sets of coders blind to group membership scored the father-child interactions. Coders were trained on both scales until they achieved at least 80% reliability, with observations selected at random for inter-rater reliability checks. Inter-rater reliability was calculated for 12% of the sample at kindergarten age (n = 22) and the Intra-class correlation coefficient was .90.
Fathers’ Harshness
Paternal harshness was also measured during the picture frame task at the kindergarten assessment using the Iowa Family Interaction Rating Scales (Melby, Conger, Book, Rueter, Lucy, & Repinski et. al, 1998). The harsh parenting composite at kindergarten age included items such as intrusiveness, angry coercion, hostility, and antisocial behavior from father to child. The internal consistency for this composite scale was adequate (Cronbach’s α = .74).
Two sets of coders blind to group membership scored the father-child interactions. Coders were trained on both scales until they achieved at least 80% reliability, with observations selected at random for inter-rater reliability checks. Intra-class correlation coefficient was calculated to assess inter-rater reliability, calculated for 12% of the sample at kindergarten age (n = 22) and was .90.
Child Anxiety Symptoms
A composite score for child anxiety symptoms was computed from the Revised Manifest Anxiety Scale – 2 (RCMAS; Reynolds & Richmond, 1978). During the eighth-grade assessment, children responded to 37 items with “yes” or “no” answers. Questions were divided into four subscales including physiological anxiety, worry/oversensitivity, concentration/social concerns, and the lie scale. The number of “yes” items given was calculated for each scale and combined to provide a total score for anxiety symptoms. This composite had high internal consistency (Cronbach’s α = .89).
Emotion Regulation
Child emotion regulation was measured in early adolescence during the eighth-grade assessment. Emotion regulation was computed by taking the average of mother and father reports of child Emotion Regulation (ER) subscale from the Emotion Regulation Checklist (Shields & Cicchetti, 1997). The ER subscale measures the occurrence of situationally appropriate affective displays, child empathy, and child emotion self-awareness. Parents rated 12 items using a Likert-like scale with 1 indicating that a behavior “Never” happened and 4 indicating that a behavior “Almost Always” happened. This subscale includes items such as “Is empathic toward others,” and “Can say when s/he is feeling sad, angry or mad, fearful or afraid.” The internal consistency of this composite was Cronbach’s α = .75.
Social Problems
A measure of child social problems was created using the child social problems subscale from the Youth Self-Report (Achenbach & Rescorla, 2001). During the eighth-grade assessment, adolescents reported on the frequency of social interaction problems arising in the previous six months. Adolescents responded to 11 items using a 3-point Likert-like scale with 0 indicating the item was “Not true” and 2 indicating the item was “Very true or often true.” Items in this subscale included statements such as “I am too dependent on others” and “I don’t get along with my peers.” The internal consistency of this composite was Cronbach’s α = .78
Cyber Victimization
At the 12th grade assessment, participants reported experiences of internet harassment and sexual solicitation occurring during the school year using six items from Ybarra, Espelage, & Mitchell (2007). For each item, participants indicated the frequency (0 ‘Never’ to 4 ‘7 or more times’) with which they experienced someone making rude comments, spreading rumors, making threats, and asking them to talk about sex, provide sexual information, or do something sexual when they did not want to. For the analyses, each item was re-coded into a dichotomous variable with 0 indicating ‘no victimization’ and 1 indicating ‘victimization reported’ and then summed to create a composite total cyber victimization score. The composite variable had values ranging from 0 to 5 with adequate reliability (Cronbach’s α = .67).
Bullying Victimization
Late adolescent bullying victimization was measured at the 12th grade assessment. The bullying victimization scale was comprised of six items from the Revised Olweus Bullying/Victimization Questionnaire (Olweus, 1996). Participants indicated how often in the past two months they had experienced each of the following: been called names, made fun of, or teased; left out or excluded; hit, kicked, or shoved; had someone spread rumors or tell lies about them; had money or things taken or stolen; and were threatened or forced to do something they did not want to do. Responses were on a scale from 0 ‘Never happened in the past two months,’ to 4 ‘Several times per week.’ For the analyses, each item was re-coded into a dichotomous variable with 0 indicating ‘no victimization’ and 1 indicating ‘victimization reported’ and then summed to create a continuous composite total bullying/victimization score. The composite variable had values ranging from 0 to 5 and had good internal consistency (Cronbach’s α = .75).
Results
Missing Data
As would be expected of any longitudinal study involving multiple family members, there were incomplete data for some participants at one or more of the eight waves of data included in these analyses. There were no missing data for fathers’ alcohol group status and fathers’ antisocial behavior (n = 227). Data for father’ depressive symptoms were averaged over the early childhood waves (12, 18, 24, and 36 months) into the early childhood composite for fathers’ depressive symptoms and this resulted in no missing data for fathers’ depressive symptoms (all fathers provided this data at 12 and 18 months, 96% at 24 months, and 85% at 36 months). The middle childhood wave for inter-parental aggression reflected a composite from the kindergarten and 4th grade waves of data collection, with 81.5% of the families having data on this composite variable (185 (81.5%) of mothers and 174 fathers (76.7%) with kindergarten data; 168 (74.0%) mothers, 157 (69.2%) fathers with data at 4th grade wave). Father-child play interaction variables were available for 150 (66%) of the families in middle-childhood. In EA 162 (71.4%) children provided data and 186 (81.9%) children provided data in late adolescence.
Among the 227 families, 11% (n = 25) had missing late adolescent data because we were unable to locate them. Among the 202 families who were contacted for the late adolescent wave, 2.4% (n = 5) of the parents refused participation, and 5% (n = 11) had passive refusals (did not complete assessments despite repeated reminders and scheduling). There were no significant group differences between families with missing versus complete data on any of the alcohol variables, depressive symptoms, or parenting.
Among fathers, 77% of those with missing data at toddler age, and 62% of those with missing data at kindergarten age were in the alcohol problem group. There was no significant association between mothers’ missing data and alcohol group status (p > .10). The association between missingness and father alcohol problem status was marginally significant at 24 months, χ2(1) = 2.66, p = .10, and nonsignificant at kindergarten age.
With regard to child outcome data, 52% of those with missing data in early adolescence and 51% of those with missing data in later adolescence were in the alcohol group. There were no associations between missing on child outcome versus not missing and fathers’ alcohol group status or depressive symptoms. However, families with missing child data had fathers who reported higher antisocial behavior compared with those who had complete data (Ms = 37.78 and 43.64, SDs = 7.54 and 12.27, respectively). Thus, the data were not missing completely at random, but fathers’ antisocial behavior was included as an exogenous variable in the model and data did meet criteria for missing at random (Little & Rubin, 1989).
Data Analytic Plan
The correlations among the main variables included in the conceptual model were examined first. Structural Equation Modeling (SEM) was used next to test the conceptual model depicted in Figure 1. Modification indices were examined next to see if there were additional paths from earlier waves that would account for additional variance in peer victimization variables. Theoretically supported paths indicated by modification indices were added one at a time and nested models were compared to test improvement in fit. All SEM analyses were conducted using Mplus (Version 8; Muthén & Muthén, 1998–2013). Full information maximum likelihood estimates were used to handle missing data (Arbuckle, Marcoulides, & Schumacker, 1996). The goodness of model fit was examined by using the comparative fit index (CFI) and the root mean-square error of approximation (RMSEA). We conducted exploratory analyses to examine sex differences. Given the limits of sample size, we did not examine if the full etiological model was different for boys and girls, but rather, examined if the specific direct paths to peer victimization in late adolescence were different for boys and girls using multiple group analysis.
Figure 1:
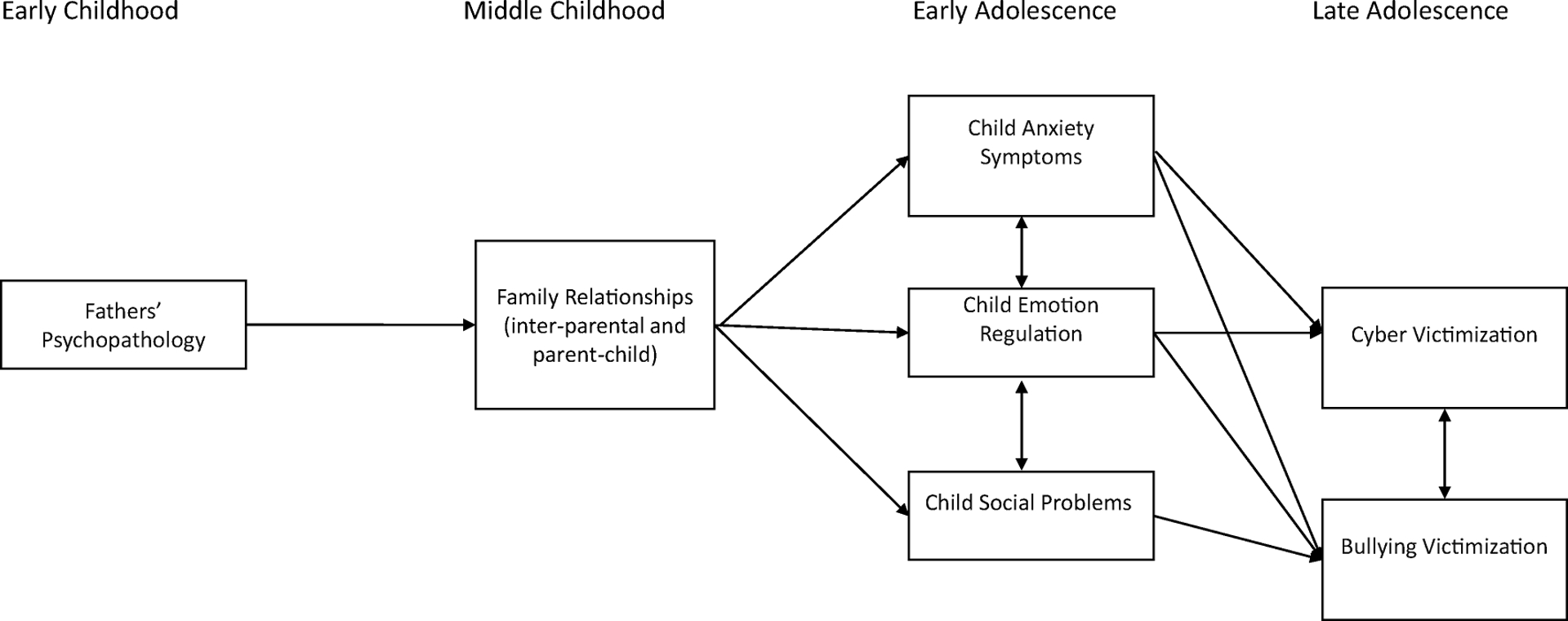
Father Pathways to Peer Victimization - Initial Conceptual Model
Descriptive and Correlational Analyses
The correlations among study variables and descriptive information are presented in Table 1. As noted in this table, fathers’ alcohol group status and depressive symptoms were associated with each other and both alcohol problems and depressive symptoms were associated with higher partner aggression in middle childhood. Higher paternal antisocial behavior was associated with lower paternal sensitivity in middle childhood and lower emotion regulation in early adolescence. Father’ sensitivity in middle childhood was associated with higher emotion regulation in early adolescence and lower cyber victimization in late adolescence. Higher anxiety symptoms in early adolescence was associated with higher social problems at the same time point and higher cyber and bullying victimization in late adolescence. Higher social problems and emotion regulation in early adolescence were also associated with higher cyber and bullying victimization in late adolescence.
Table 1:
Correlations Among Paternal Psychopathology, Middle Child Parenting Variables, and Late Adolescence Peer Outcomes.
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | F Alcohol group status EC | – | ||||||||||
| 2. | F Depression EC | .14* | – | |||||||||
| 3. | F ASB EC | .37** | .30* | – | ||||||||
| 4. | Partner aggression MC | .18** | .27* | .12 | – | |||||||
| 5. | F warmth/sensitivity MC | −.13 | −.05 | −.23* | −.11 | – | ||||||
| 6. | F harshness MC | .01 | −.06 | .09 | .04 | −.43* | – | |||||
| 7. | Child anxiety EA | .11 | .07 | .08 | .09 | −.04 | −.10 | – | ||||
| 8. | Emotion regulation EA | −.08 | −.11 | −.25* | −.08 | .28* | −.10 | −.02 | – | |||
| 9. | Social Problems EA | .09 | −.02 | .07 | .14 | −.16 | .14 | .46* | .05 | – | ||
| 10. | Cyber victimization LA | −.00 | −.01 | .07 | .07 | −.29** | .18* | .24* | .16* | .26** | – | |
| 11. | Bully victimization LA | −.02 | .05 | .02 | .07 | .07 | −.08 | .28** | .16* | .30** | .36** | – |
| Mean | .55 | 6.96 | 39.75 | .81 | 5.08 | 1.96 | 6.03 | 26.34 | 1.90 | .68 | 1.36 | |
| Standard Deviation | .50 | 5.92 | 8.87 | 1.115 | .94 | .83 | 5.62 | 3.01 | 1.74 | 1.11 | 1.43 | |
Note: n = 227; ASB: Antisocial Behavior; F: Father; EC: Early Childhood; MC: Middle childhood; EA: Early Adolescence; LA: Later Adolescence.
p < .05
p < .01
Testing the Conceptual Model
We first tested the conceptual model displayed in Figure 1. As indicated in the figure, this model included paths from fathers’ alcohol group status, depressive symptoms, and antisocial behavior in early childhood to intimate partner aggression; fathers’ sensitivity and harshness in middle childhood; paths from these middle childhood variables to child anxiety symptoms, emotion regulation, and social problems in early adolescence, and paths from these early adolescence variables to cyber and bullying victimization in late adolescence. The model also included causal paths from partner aggression to paternal sensitivity and harshness. In addition to these causal paths, the model included all the within time covariances among variables measured at the same time point.
Results indicated that this conceptual model fit the data adequately χ2 (21) = 36.08, p = .02, CFI = .91, RMSEA = .06 (.00, .09); SRMR = .06. Fathers with alcohol problems had higher inter- parental aggression in middle childhood. Fathers’ depressive symptoms in early childhood was also associated with higher inter-parental aggression in middle childhood, and fathers’ antisocial behavior in early childhood was a proximal predictor of lower paternal sensitivity during play interactions with their children in middle childhood. Among the middle childhood variables, inter-partner aggression accounted for unique variance in child social problems and fathers’ sensitivity accounted for unique variance in children’s emotion regulation in early adolescence. All three early adolescent variables of anxiety symptoms, emotion regulation, and social problems were proximal predictors of cyber and bullying victimization in late adolescence. Examination of modification indices indicated that the addition of a direct path from fathers’ sensitivity in middle childhood to cyber victimization in late adolescence would substantially improve model fit, Δχ2 (1) = 19.07, p < .001. This path was theoretically well justified and was added to the model. The final model with the addition of this path fit the data well, χ2 (20) = 17.01, p = .65, CFI = .99, RMSEA = .00 (.00, .06); SRMR = .04. This final model is depicted in Figure 2. For ease of presentation, only the significant pathways are depicted.
Figure 2: Final Model Including Direct Path from Fathers’ Sensitivity to Cyber Victimization.
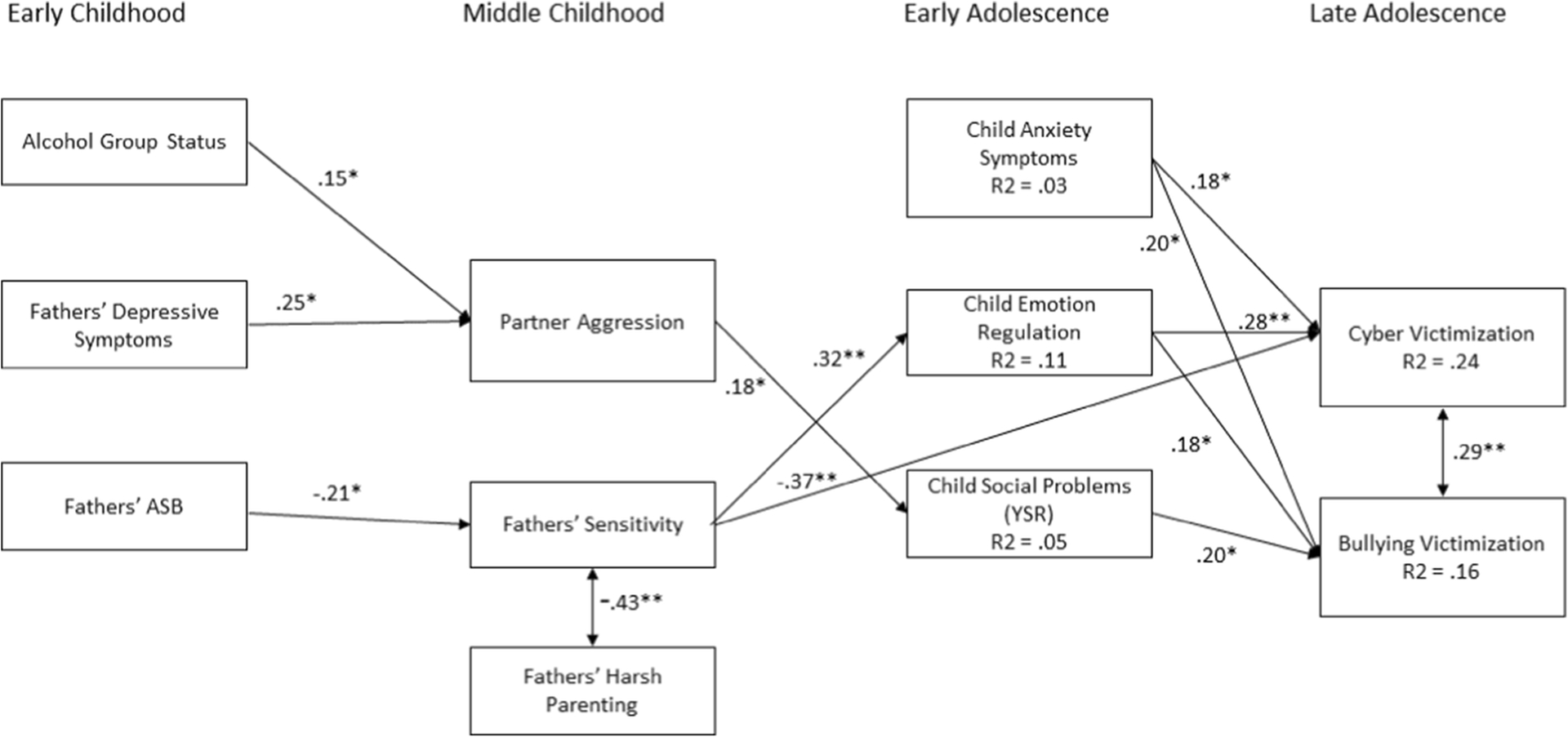
Note. Figure 2. The final model. The numbers represent standardized path coefficients. Nonsignificant paths are not depicted for ease of presentation. Also not included are the error terms and covariances between child social problems and emotion regulation (r = .13, p > .05), between child anxiety and emotion regulation (r = .01, p > .05), and between child anxiety and social problems (r = .46, p = 0.001). High scores on emotion regulation reflect higher emotion regulation, high scores on anxiety, social problems, and victimization variables reflect higher levels on these variables. ASB = Antisocial behaviorPsychology, Michigan State University, 1980, unpublished instrument.
Sex Differences
To examine if the paths from early to late adolescent variables and from fathers’ sensitivity to cyber victimization varied for girls and boys, we conducted a multiple-group SEM testing each of these paths individually, comparing a model with one of the paths constrained to be equal to a fully unconstrained model. Results indicated that the path from social problems to bullying victimization was significantly different for girls and boys Δχ2 (1) = 6.54, p < .01. Examination of the path coefficients indicated that this path was significant for boys but not girls.
Discussion
The results of this study provide empirical support for Hong and Espelage’s (2012) theoretical framework, whereby fathers’ psychopathology in early life disrupted family relationships in middle childhood, which in turn had adverse associations with children’s psychosocial functioning in early adolescence and was associated with risk for peer victimization in late adolescence. Although there was overall support for the conceptual model, not all of the individual hypothesized paths were significant. Notably, although the presence of anxiety symptoms in early adolescence was a significant risk factor for both bullying and cyber victimization in late adolescence, it was unrelated to any of the early life family characteristics included in this model. An additional unexpected finding was that the two hypothesized pathways to peer victimization (i.e., via inter-parent aggression and parenting) were driven by different types of paternal psychopathology. Finally, the study revealed that there were similarities and differences in the respective etiological pathways for bullying and cyber victimization.
The first pathway through which paternal psychopathology was expected to influence peer victimization was through the parental relationship. Based on prior research conducted with the sample at younger ages (e.g., Eiden, Molnar, Edwards, & Leonard, 2009b; Eiden et al., 2007; Finger et al., 2010b), we hypothesized that father’s psychopathology would be associated with inter-parental aggression in middle childhood, which would be associated with children’s anxiety symptoms, social problems, and poor emotion regulation in adolescence, ultimately predicting peer victimization. This hypothesis was partially supported. Results indicated that inter-parental aggression in middle childhood was predicted by fathers’ alcohol problems and depressive symptoms, but not antisocial behavior. This is surprising given that fathers’ alcohol problems and antisocial behavior tend to be comorbid and are related to intimate partner aggression (Finger et al., 2010a). Perhaps the community-recruited sample of mostly well-functioning fathers with alcohol problems who were not selected for high levels of antisocial behavior (e.g., drunk driving) may have accounted for the lack of prospective associations from fathers’ antisocial behavior in early childhood to family relationships in middle childhood.
Inter-parental aggression in middle childhood predicted social problems in early adolescence, which in turn was linked to bullying victimization in late adolescence; however, this path was only significant for boys. Boys exposed to parental alcohol problems and inter-parental aggression are more likely than those who are not to engage in aggressive behavior including bullying and fighting (Espelage, Low, Rao, Hong, & Little, 2014; Fuller, Chermack, Cruise, Kirsch, Fitzgerald, & Zucker, 2003). Youth who are aggressive in peer interactions are likely to have social problems and to be involved in peer aggression as both a perpetrator and a victim (Espelage, Low, Rao, Hong, & Little, 2014; Fox & Boulton, 2006). Contrary to expectations, however, inter-parental aggression in middle childhood did not account for unique variance in anxiety symptoms or emotion regulation in early adolescence. These findings are contrary to those obtained in earlier waves of the current sample where inter-parental aggression across early childhood (infancy to school age) was robustly associated with higher child anxiety symptoms in middle childhood (Eiden et al., 2009b). It is possible that more chronic exposure to intimate partner aggression may have enduring effects on child anxiety symptoms rather than within a narrower developmental period. Another explanation may be that exposure in early childhood when children spend more time with their families rather than at school resulted in more exposure to intimate partner aggression. Future studies with measurement of child exposure to intimate partner aggression may be better able to address this issue.
The model also supported a second pathway from paternal antisocial behavior (but not alcohol problems or depressive symptoms) in early childhood to late adolescent peer victimization, via parenting behavior. Antisocial fathers were less sensitive towards their child in middle childhood. Parental sensitivity has been identified as an important protective factor against peer victimization and other forms of aggression through its positive effects on children’s emotional regulation (Lereya, Samara, & Wolke, 2013; Hong, Espelage, Grogan-Kaylor, & Allen-Meares, 2011). Parents who are warm and sensitive are better able to respond to their children and to teach them appropriate ways of managing negative affect. Their children also tend to be more secure and able to regulate their emotions. Interestingly, although parental sensitivity was inversely associated with harsh parenting, paternal psychopathology did not predict harsh parenting in middle childhood. This is counter to prior research that has shown paternal psychopathology is prospectively associated with harsh parenting behavior at earlier ages (e.g. Eiden et al., 2009a; Eiden et al., 2016). Further, fathers’ harsh parenting was unrelated to any of the psychosocial outcomes. Prior research indicates that parental harshness contributes to child distress and insecurity, making it difficult for them to manage their emotions (Eisenberg, Zhou, Spinrad, Valiente, Fabes, & Liew, 2005; Godleski, Eiden, Shisler, & Livingston, 2020), although there is some evidence that this influence may be stronger for mothers than for fathers (Chang, Schwartz, Dodge, & McBride-Chang, 2003). One explanation may be that mothers were the primary caregivers for the majority of these children and mitigated the potential effects of fathers’ harshness. In addition, the lack of associations between fathers’ harsh parenting and psychosocial outcomes may also be due to the short duration of the observational assessment period, or the use of a community (vs. a clinical or treatment) sample.
In this study, we found fathers’ sensitivity in middle childhood was both directly and indirectly related to peer victimization in late adolescence. Consistent with prior research indicating that warm and sensitive parenting is protective against peer victimization (Lereya, Samara, & Wolke, 2013), fathers’ sensitivity in this study was directly and inversely associated with cyber victimization in late adolescence. As predicted, fathers’ sensitive parenting in middle childhood also was positively associated with emotion regulation in early adolescence. However, counter to expectations, there was a positive association between emotion regulation in early adolescence and both bullying and cyber victimization in late adolescence, suggesting that higher emotion regulation increased risk for peer victimization.
The regulation of emotion is a cognitively complex task that involves the management of both the internal experience of the emotion as well as its expression. There is evidence indicating that discrete emotions are associated with different regulatory processes, that there are individual differences in ability to regulate specific emotions, and these have different associations with peer victimization experiences (Garner & Waajid, 2019). Our measure of emotion regulation was broad and was not specific to particular emotions, thus it may not adequately have captured the relevant processes. Another possibility is that the positive association between emotion regulation and peer victimization that was observed in this study may reflect the suppression of the expression of emotion, rather than management of the subjective experience of the emotion. Strategies such as re-appraisal that aim to reduce the subjective impact of the event so that it becomes less distressing tend to be more adaptive than efforts to suppress or overcontrol the expression of the emotion (Chervonsky & Hunt, 2018). Individuals who control their emotional responses through suppression tend to be less expressive and more neurotic (Webb, Miles, & Sheeran, 2012), which may interfere with social relationships and make them targets for peer victimization (Chervonsky & Hunt, 2018). Findings also showed that bullying and cyber victimization shared common proximal risk factors including anxiety symptoms and emotion regulation, yet their etiological pathways were not identical. In this study, fathers’ sensitivity was protective against cyber victimization as evidenced by their direct negative relationship. It may be that fathers who are sensitive to their children engage in higher levels of monitoring and supervision, including supervision of on-line activities, which have been shown to be protective against cyber victimization (Baldry, Sorrentino, & Farrington, 2019). Social problems, which were predicted from paternal psychopathology via inter-parental aggression, were related to boys’ involvement in bullying victimization but not cyber victimization. Cyber victimization tends to involve relational aggression, whereas bullying victimization can also include overt and physical aggression. Youth, especially boys, exposed to negative parenting and inter-parental aggression tend to engage in aggressive and externalizing behaviors that create social problems with peers (Espelage, Low, Rao, Hong, & Little, 2014). This aggressive behavior may provoke overt, in-person aggression from peers.
Limitations and Future Directions
Limitations of the study include the use of a relatively small community sample comprised of predominantly White, heterosexual parent participants. To be eligible for the study, the child’s biological parents had to be cohabitating from the time of the child’s birth through recruitment when the child was 12 months of age. This may have resulted in a more homogeneous, stable sample and thus, results may not be generalizable to other populations. Another limitation is that child’s aggressive behavior was not included in the model. Given that boys exposed to inter-parental aggression and paternal harsh parenting (Chang et al., 2003; Espelage et al., 2014) tend to be aggressive in their interactions with peers, it is possible that some of the victims were provocative victims. That is, their aggressive behavior towards others may elicit aggressive, retaliatory responses. In addition, compared with those reported in other studies (e.g., Ybarra et al., 2007), the internal consistency of the cyber victimization scale was low. This may be due to the use of a small sample of older adolescents and relatively low rates of endorsement of the cyber victimization items, particularly those items reflecting sexual cyber harassment. Finally, , we used a global measure of emotion regulation based on parent reports that may not have captured the processes that could protect adolescents from peer victimization. Future research should consider a more nuanced assessment of emotional regulation.
In spite of these limitations, the study offered an opportunity to examine the unique influence of fathers on child developmental outcomes from infancy through late adolescence. The unique influence of fathers on their children’s development over time is understudied. Given the paucity of research examining the effects of specific types of paternal psychopathology on child outcomes, the findings from the current study help to elucidate the ways in which paternal psychopathology affects family dynamics and child risk factors. Findings from this study add to a growing body of literature that show that paternal psychopathology in early childhood adversely affects children’s psychosocial development, placing them at risk for negative outcomes such as substance use and victimization (Eiden et al., 2016; Eiden, Shisler, Granger, Schuetze, Colangelo, & Huestis, 2020; Livingston, Eiden, Lessard, Casey, Henrie, & Leonard, 2018). This underscores the need for early, family-based interventions to strengthen both inter-parental and parent-child relationships. The results also show the importance of fathers’ sensitivity in protecting adolescents from on-line cyber victimization. However, the mechanisms through which fathers’ sensitivity protects against cyber victimization need to be further elucidated. Additional research is needed to shed light on the complex relation between emotion regulation and peer victimization, with attention to understanding distinctions in the management of the expression and subjective experiencing of different types of emotion.
Conclusions
The results of this study highlight the unique and important role fathers play in the psychosocial development of their children. As proposed by Hong et, al. (2011), risk for peer victimization has its roots in maladaptive family relationships. Intervening to provide support for families affected by fathers’ psychopathology, including substance abuse treatment, relationship counseling, and parenting skills may help to stabilize family relationships. This may have the added benefit of improving adolescent psychosocial outcomes and reducing involvement in peer victimization.
Funding:
This research was supported by Award 2012-W9-BX-0001, awarded by the National Institute of Justice, Office of Justice Programs, U.S. Department of Justice and by the National Institute of Alcoholism and Alcohol Abuse of the National Institutes of Health R01 AA010042 and R21AA021617. The opinions, findings and conclusions or recommendations expressed in this exhibition are those of the authors and do not necessarily reflect those of the Department of Justice or the National Institutes of Health. We are grateful to families who were part of this longitudinal study and to research staff and students who conducted family assessments and project management.
Footnotes
Conflict of Interest: The authors have no conflict of interest to declare.
Availability of Data: Data available upon request from authors.
Code Availability: Not applicable.
References
- Achenbach TM, & Rescorla L (2001). Manual for the ASEBA school-age forms & profiles: An integrated system of multi-informant assessment. Research Center for Children, Youth, and Families. [Google Scholar]
- American Psychiatric Association. (2000). Diagnostic criteria from dsM-iV-tr. American Psychiatric Pub. https://behavenet.com/apa-diagnostic-classification-dsm-iv-tr [Google Scholar]
- Andreasen NC, John R, Jean E, Theodore R, & William C (1986). The family history approach to diagnosis: how useful is it? Archives of General Psychiatry, 43(5), 421–429. 10.1001/archpsyc.1986.01800050019002 [DOI] [PubMed] [Google Scholar]
- Anthony JC, Warner LA, & Kessler RC (1994). Comparative epidemiology of dependence on tobacco, alcohol, controlled substances, and inhalants: Basic findings from the National Comorbidity Survey. Experimental and Clinical Psychopharmacology, 2(3), 244–268. 10.1037/1064-1297.2.3.244 [DOI] [Google Scholar]
- Arbuckle JL, Marcoulides GA, & Schumacker RE (1996). Full information estimation in the presence of incomplete data. Advanced structural equation modeling: Issues and techniques, 243, 277. [Google Scholar]
- Archer J (2002). Sex differences in physically aggressive acts between heterosexual partners. Aggression and Violent Behavior, 7(4), 313–351. 10.1016/s1359-1789(01)00061-1 [DOI] [Google Scholar]
- Baldry AC, Farrington DP, & Sorrentino A (2015). ‘Am I at risk of cyberbullying’? A narrative review and conceptual framework for research on risk of cyberbullying and cybervictimization: The risk and needs assessment approach. Aggression and Violent Behavior, 23, 36–51. [Google Scholar]
- Baldry AC, Sorrentino A, & Farrington DP (2019). Cyberbullying and cybervictimization versus parental supervision, monitoring and control of adolescents’ online activities. Children and Youth Services Review, 96, 302–307. [Google Scholar]
- Bauer NS, Herrenkohl TI, Lozano P, Rivara FP, Hill KG, & Hawkins JD (2006). Childhood Bullying Involvement and Exposure to Intimate Partner Violence. PEDIATRICS, 118(2), e235–e242. 10.1542/peds.2005-2509 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Betts LR, Houston JE, & Steer OL (2015). Development of the Multidimensional Peer Victimization Scale–Revised (MPVS-R) and the Multidimensional Peer Bullying Scale (MPVS-RB). The Journal of Genetic Psychology: Research and Theory on Human Development, 176(2), 93–109. [DOI] [PubMed] [Google Scholar]
- Bornstein MH, Hahn C-S,Hayens OM (2010). Social competence, externalizing, and internalizing behavioral adjustment through early adolescence: Developmental cascades. Developmental Psychopathology, 22, 717–735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boyd JH, Weissman MM, Thompson WD, & Myers JK (1982). Screening for depression in a community sample: Understanding the discrepancies between depression symptom and diagnostic scales. Archives of general psychiatry, 39(10), 1195–1200. 10.1001/archpsyc.1982.04290100059010 [DOI] [PubMed] [Google Scholar]
- Buelga S, Martínez–Ferrer B, & Cava M (2017). Differences in family climate and family communication among cyberbullies, cybervictims, and cyber bully–victims in adolescents. Computers in Human Behavior, 76, 164–173. 10.1016/j.chb.2017.07.017 [DOI] [Google Scholar]
- Chang L, Schwartz D, Dodge KA, & McBride-Chang C (2003). Harsh parenting in relation to child emotion regulation and aggression. Journal of Family Psychology, 17, 598–606. 10.1037/0893-3200.17.4.598 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chervonsky E, & Hunt C (2018). Emotion suppression and reappraisal associated with bullying involvement and other social outcomes in young adults. Social Psychology of Education: An International Journal, 21(4), 849–873. 10.1007/s11218-018-9440-3 [DOI] [Google Scholar]
- Cheung K, & Theule J (2019). Paternal Depressive Symptoms and Parenting Behaviors: An Updated Meta-Analysis. Journal of Child and Family Studies, 28(3), 613–626. 10.1007/s10826-018-01316-1 [DOI] [Google Scholar]
- Cheung K, Theule J, Hiebert-Murphy D, & Piotrowski C (2019). Paternal Depressive Symptoms and Marital Quality: A Meta-Analysis of Cross-Sectional Studies. Journal of Family Theory & Review. 10.1111/jftr.12341 [DOI] [Google Scholar]
- Cloninger CR, Sigvardsson S, & Bohman M (1988). Childhood Personality Predicts Alcohol Abuse in Young Adults. Alcoholism: Clinical and Experimental Research, 12(4), 494–505. 10.1111/j.1530-0277.1988.tb00232.x [DOI] [PubMed] [Google Scholar]
- Cunningham S, Goff C, Bagby RM, Stewart JG, Larocque C, Mazurka R, Harkness KL (2019). Maternal- versus paternal-perpetrated maltreatment and risk for sexual and peer bullying revictimization in young women with depression. Child Abuse Negl, 89, 111–121. 10.1016/j.chiabu.2018.12.017 [DOI] [PubMed] [Google Scholar]
- Davies PT, & Cummings EM (1994). Marital conflict and child adjustment: An emotional security hypothesis. Psychological Bulletin, 116(3), 387–411. 10.1037/0033-2909.116.3.387 [DOI] [PubMed] [Google Scholar]
- Davies PT, & Martin MJ (2013). The reformulation of emotional security theory: The role of children’s social defense in developmental psychopathology. Development and psychopathology, 25(4pt2), 10.1017/s0954579413000709 [DOI] [PMC free article] [PubMed] [Google Scholar]
- deMontigny F, Girard ME, Lacharite C, Dubeau D, & Devault A (2013). Psychosocial factors associated with paternal postnatal depression. Journal of affective disorders, 150(1), 44–49. 10.1016/j.jad.2013.01.048 [DOI] [PubMed] [Google Scholar]
- Dickson DJ, Laursen B, Valdes O, & Stattin H (2019). Derisive Parenting Fosters Dysregulated Anger in Adolescent Children and Subsequent Difficulties with Peers. Journal of Youth and Adolescence, 48(8), 1567–1579. 10.1007/s10964-019-01040-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dodge KA, Malone PS, Lansford JE, Miller-Johnson S, Pettit GS, & Bates JE (2006). Toward a Dynamic Developmental Model of the Role of Parents and Peers in Early Onset Substance Use. Families Count, 104–132. 10.1017/cbo9780511616259.006 [DOI] [Google Scholar]
- Earnshaw VA, Elliott MN, Reisner SL, Mrug S, Windle M, Tortolero Emery S, Peskin MF, Schuster MA (2017). Peer Victimization, Depressive Symptoms, and Substance Use: A Longitudinal Analysis. Pediatrics,139(6), 10.1542/peds.2016-3426 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiden RD, Chavez F, & Leonard KE (1999). Parent-infant interactions among families with alcoholic fathers. Development and Psychopathology, 11, 745–762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiden RD, Colder C, Edwards EP, & Leonard KE (2009). A longitudinal study of social competence among children of alcoholic and nonalcoholic parents: Role of parental psychopathology, parental warmth, and self-regulation. Psychology of Addictive Behaviors, 23(1), 36–46. 10.1037/a0014839 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiden RD, Edwards EP, & Leonard KE (2007). A conceptual model for the development of externalizing behavior problems among kindergarten children of alcoholic families: role of parenting and children’s self-regulation. Developmental Psychology, 43(5), 1187–1201. 10.1037/0012-1649.43.5.1187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiden RD, Colder C, Edwards EP, & Leonard KE (2009a). A longitudinal study of social competence among children of alcoholics: Role of parental psychopathology, parental warmth, and self-regulation. Psychology of Addictive Behaviors, 23, 36–46. 10.1037/a0014839 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiden RD, Molnar D, Colder C, Edwards EP, Leonard KE (2009b). A conceptual model predicting internalizing problems in middle childhood among children of alcoholic and non-alcoholic fathers: The role of marital aggression. Journal Studies on Alcohol and Drugs, 70, 741–750. 10.15288/jsad.2009.70.741 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiden RD, Lessard J, Colder CR, Livingston J, Casey M, & Leonard KE (2016). Developmental cascade model for adolescent substance use from infancy to late adolescence. Developmental Psychology, 52(10), 1619–1633. 10.1037/dev0000199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiden RD, Shisler S, Granger DA, Schuetze P, Colangelo J, & Huestis MA (2020). Prenatal Tobacco and Cannabis Exposure: Associations with Cortisol Reactivity in Early School Age Children. International Journal of Behavioral Medicine, 27(3), 343–356. 10.1007/s12529-020-09875-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, Zhou Q, Spinrad TL, Valiente C, Fabes RA, & Liew J (2005). Relations Among Positive Parenting, Children’s Effortful Control, and Externalizing Problems: A Three-Wave Longitudinal Study. Child Development, 76(5), 1055–1071. 10.1111/j.1467-8624.2005.00897.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Espelage DL, & Holt MK (2007). Dating violence & sexual harassment across the bully-victim continuum among middle and high school students. Journal of Youth and Adolescence, 36(6), 799–811. 10.1007/s10964-006-9109-7 [DOI] [Google Scholar]
- Espelage DL, Low S, Rao MA, Hong JS, & Little TD (2014). Family violence, bullying, fighting, and substance use among adolescents: A longitudinal mediational model. Journal of Research on Adolescence, 24(2), 337–349. 10.1111/jora.12060 [DOI] [Google Scholar]
- Estévez E, Musitu G, & Herrero J (2005). The influence of violent behavior and victimization at school on psychological distress: The role of parents and teachers. Adolescence, 40(157), 183–196. [PubMed] [Google Scholar]
- Farrington DP, Loeber R, Stallings R, & Ttofi MM (2011). Bullying perpetration and victimization as predictors of delinquency and depression in the Pittsburgh Youth Study. Journal of Aggression, Conflict, and Peace Research, 3,74–81. http://doi10.1108/17596591111132882 [Google Scholar]
- Fekkes M, Pijpers FIM, Fredriks AM, Vogels T, & Verloove-Vanhorick SP (2006). Do bullied children get ill, or do ill children get bullied? A prospective cohort study on the relationship between bullying and health-related symptoms. Pediatrics, 117(5), 1568–1574. 10.1542/peds.2005-0187 [DOI] [PubMed] [Google Scholar]
- Finger B, Eiden RD, Edwards EP, & Leonard KE (2010b). Marital aggression and child social competence: A comparison of three conceptual models. Personal Relationships, 17, 357–376. 10.1111/j.1475-6811.2010.01284.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finger B, Kachadourian LK, Molnar DS, Eiden RD, Edwards EP, & Leonard KE (2010a). Alcoholism, associated risk factors, and harsh parenting among fathers: Examining the role of marital aggression. Addictive Behaviors, 35(6), 541–548. 10.1016/j.addbeh.2009.12.029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fitzgerald HE, & Eiden RD (2007). Paternal Alcoholism, Family Functioning, and Infant Mental Health. Zero to Three, 27(4), 11–18. [Google Scholar]
- Foran HM, & O’Leary KD (2007). Problem drinking, jealousy, and anger control: Variables predicting aggression against a partner. Journal of Family Violence, 23, 141–148. https://doi/10.1007/s10896-007-9136-5 [Google Scholar]
- Fox CL, & Boulton MJ (2006). Friendship as a moderator of the relationship between social skills problems and victimization. Aggressive Behavior, 32, 110–121. 10.1002/ab.20114 [DOI] [Google Scholar]
- Fuller BE, Chermack ST, Cruise KA, Kirsch E, Fitzgerald HE, & Zucker RA (2003). Predictors of aggression across three generations among sons of alcoholics: Relationships involving grandparental and parental alcoholism, child aggression, marital aggression and parenting practices. Journal of Studies on Alcohol and Drugs, 64(4), 472–483. 10.15288/jsa.2003.64.472 [DOI] [PubMed] [Google Scholar]
- Garner PW, & Waajid B (2018). Sociodemographic variations in the linkage between emotion regulation and peer victimization. Journal of School Violence, 18(1), 121–133. 10.1080/15388220.2017.1418670 [DOI] [Google Scholar]
- Godleski SA, Eiden RD, Shisler S, & Livingston JA (2020). Parent socialization of emotion in a high-risk sample. Developmental psychology, 56(3), 489. 10.1037/dev0000793 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Godleski SA & Eiden RD (2020). Fathers, antisocial behavior, and very young children. In Fitzgerald HE, Kai von Klitzing KV, Carbrara N, Skjothaug T, & Scarano de Mendonca J (Eds.), Handbook of Fathers and Child Dveelopment. Springer Press. [Google Scholar]
- Godleski SA, Kamper KE, Ostrov JM, Hart EJ, & Blakely-McClure SJ (2014). Peer Victimization and Peer Rejection During Early Childhood. Journal of Clinical Child & Adolescent Psychology, 4(3), 380–392. 10.1080/15374416.2014.940622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ham HP, Zucker RA, & Fitzgerald HE (1993, August). Assessing antisociality with the Antisocial Behavior Checklist: Reliability and validity studies. Poster presented at the annual meeting of the American Psychological Society, Chicago. [Google Scholar]
- Harold GT, Elam KK, Lewis G, Rice F, & Thapar A (2012). Interparental conflict, parent psychopathology, hostile parenting, and child antisocial behavior: Examining the role of maternal versus paternal influences using a novel genetically sensitive research design. Development and Psychopathology, 24(4), 1283–1295. 10.1017/s0954579412000703 [DOI] [PubMed] [Google Scholar]
- Hong JS, & Espelage DL (2012). A review of research on bullying and peer victimization in school: An ecological system analysis. Aggression and Violent Behavior, 17(4), 311–322. 10.1016/j.avb.2012.03.003 [DOI] [Google Scholar]
- Hong JS, Espelage DL, Grogan-Kaylor A, & Allen-Meares P (2011). Identifying Potential Mediators and Moderators of the Association Between Child Maltreatment and Bullying Perpetration and Victimization in School. Educational Psychology Review, 24(2), 167–186. 10.1007/s10648-011-9185-4 [DOI] [Google Scholar]
- Hussong A, Bauer D, & Chassin L (2008). Telescoped trajectories from alcohol initiation to disorder in children of alcoholic parents. Journal of Abnormal Psychology, 117(1), 63–78. 10.1037/0021-843x.117.1.63 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hussong AM, Wirth RJ, Edwards MC, Curran PJ, Chassin LA, & Zucker RA (2007). Externalizing symptoms among children of alcoholic parents: Entry points for an antisocial pathway to alcoholism. Journal of abnormal psychology, 116(3), 529. 10.1037/0021-843x.116.3.529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jaffee SR, Moffitt TE, Caspi A, & Taylor A (2003). Life with (or without) father: The benefits of living with two biological parents depend on the father’s antisocial behavior. Child Development, 74(1), 109–126. 10.1111/1467-8624.t01-1-00524 [DOI] [PubMed] [Google Scholar]
- Keller PS, Cummings EM, Peterson KM, & Davies PT (2009). Marital conflict in the context of parental depressive symptoms: Implications for the development of children’s adjustment problems. Social Development, 18(3), 536–555. 10.1111/j.1467-9507.2008.00509.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen H-U, & Kendler KS (1994). Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Archives of general psychiatry, 51(1), 8–19. [DOI] [PubMed] [Google Scholar]
- Kljakovic M, & Hunt C (2016). A meta-analysis of predictors of bullying and victimisation in adolescence. Journal of Adolescence, 49, 134–145. 10.1016/j.adolescence.2016.03.002 [DOI] [PubMed] [Google Scholar]
- Kouros CD, Merrilees CE, & Cummings EM (2008). Marital Conflict and Childrens Emotional Security in the Context of Parental Depression. Journal of Marriage and Family, 70(3), 684–697. 10.1111/j.1741-3737.2008.00514.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landoll RR, La Greca AM, Lai BS, Chan SF, & Herge WM (2015). Cyber victimization by peers: Prospective associations with adolescent social anxiety and depressive symptoms. Journal of Adolescence, 42, 77–86. 10.1016/j.adolescence.2015.04.002 [DOI] [PubMed] [Google Scholar]
- Lee Y, & Kim J (2017). Developmental patterns of substance use by gender and their relation to individual, parental, and peer factors. Criminal justice and behavior, 44(11), 1413–1443. https://doi.org/10.1177%2F0093854817717291 [Google Scholar]
- Lereya ST, Samara M, & Wolke D (2013). Parenting behavior and the risk of becoming a victim and a bully/victim: A meta-analysis study. Child Abuse & Neglect, 37(12), 1091–1108. 10.1016/j.chiabu.2013.03.001 [DOI] [PubMed] [Google Scholar]
- Livingston JA, Eiden RD, Lessard J, Casey M, Henrie J, & Leonard KE (2018). Etiology of Teen Dating Violence among Adolescent Children of Alcoholics. Journal of Youth and Adolescence, 47(3), 515–533. 10.1007/s10964-017-0730-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP (2003). For better or for worse? The effects of alcohol use on marital functioning. Clinical psychology review, 23(7), 959–997. 10.1016/j.cpr.2003.09.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Hatzenbuehler ML, & Hilt LM (2009). Emotion dysregulation as a mechanism linking peer victimization to internalizing symptoms in adolescents. Journal of Consulting and Clinical Psychology, 77(5), 894–904. 10.1037/a0015760 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Melby JN, Conger RD, Book R, Rueter R, Lucy L, Repinski D, Rogers S, Rogers B, & Scaramella L (1998). The Iowa family interaction rating scales (5th edn). Institute for Social and Behavioral Research Iowa State University. Ames, IA. [Google Scholar]
- Muthén LK, & Muthén BO BO (1998–2013). Mplus user’s guide. Los Angeles, CA: https://www.statmodel.com/download/usersguide/MplusUserGuideVer_7.pdf [Google Scholar]
- Mynard H, & Joseph S (2000). Development of the multidimensional peer-victimization scale. AGGRESSIVE BEHAVIOR, 26(2), 169–178. [DOI] [Google Scholar]
- Nath S, Russell G, Kuyken W, Psychogiou L, & Ford T (2016). Does father–child conflict mediate the association between fathers’ postnatal depressive symptoms and children’s adjustment problems at 7 years old?. Psychological medicine, 46(8), 1719–1733. 10.1017/S0033291716000234 [DOI] [PubMed] [Google Scholar]
- Nelson JA, O’Brien M, Blankson AN, Calkins SD, & Keane SP (2009). Family stress and parental responses to children’s negative emotions: Tests of the spillover, crossover, and compensatory hypotheses. Journal of Family Psychology, 23(5), 671. 10.1037/a0015977 [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Farrell TJ, Murphy CM, Neavins TM, & Van Hutton V (2000). Verbal Aggression Among Male Alcoholic Patients and Their Wives in the Year Before and Two Years After Alcoholism Treatment. Journal of Family Violence, 15(4), 295–310. 10.1023/a:1007503411845 [DOI] [Google Scholar]
- Olweus D (1996). Revised Olweus bully/victim questionnaire. British Journal of Educational Psychology. 10.1037/t09634-000 [DOI] [Google Scholar]
- Radloff LS (1977). The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological Measurement, 1(3), 385–401. 10.1177/014662167700100306 [DOI] [Google Scholar]
- Reijntjes A, Kamphuis JH, Prinzie P, & Telch MJ (2010). Peer victimization and internalizing problems in children: a meta-analysis of longitudinal studies. Child Abuse & Neglect, 34(4), 244–252. [DOI] [PubMed] [Google Scholar]
- Reynolds CR, & Richmond BO (1978). What I think and feel: A revised measure of children’s manifest anxiety. Journal of abnormal child psychology, 6(2), 271–280. 10.1007/BF00919131 [DOI] [PubMed] [Google Scholar]
- Shields A, & Cicchetti D (1997). Emotion Regulation Q-Scale. PsycTESTS Dataset. 10.1037/t04297-000 [DOI] [Google Scholar]
- Riley TN, Sullivan TN, Hinton TS, & Kliewer W (2019). Longitudinal relations between emotional awareness and expression, emotion regulation, and peer victimization among urban adolescents. Journal of adolescence, 72, 42–51. 10.1016/j.adolescence.2019.02.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shields A, & Cicchetti D (2001). Parental Maltreatment and Emotion Dysregulation as Risk Factors for Bullying and Victimization in Middle Childhood. Journal of Clinical Child & Adolescent Psychology, 30(3), 349–363. 10.1207/s15374424jccp3003_7 [DOI] [PubMed] [Google Scholar]
- Shields A, Dickstein S, Seifer R, Giusti L, Dodge Magee K, & Spritz B (2001). Emotional Competence and Early School Adjustment: A Study of Preschoolers at Risk. Early Education & Development, 12(1), 73–96. 10.1207/s15566935eed1201_5 [DOI] [Google Scholar]
- Steinberg L (2014). Age of opportunity: Lessons from the new science of adolescence. New York: Mariner Books. [Google Scholar]
- Stocker CM, & Youngblade L (1999). Marital conflict and parental hostility: Links with children’s sibling and peer relationships. Journal of Family Psychology, 13(4), 598–609. 10.1037/0893-3200.13.4.598 [DOI] [Google Scholar]
- Straus MA (1979). Conflict Tactics Scales. PsycTESTS Dataset. 10.1037/t02125-000 [DOI] [Google Scholar]
- Tokunaga RS (2010). Following you home from school: A critical review and synthesis of research on cyberbullying victimization. Computers in Human Behavior, 26(3), 277–287. 10.1016/j.chb.2009.11.014 [DOI] [Google Scholar]
- Webb TL, Miles E, & Sheeran P (2012). Dealing with feeling: A meta-analysis of the effectiveness of strategies derived from the process model of emotion regulation. Psychological Bulletin, 138(4), 775–808. 10.1037/a0027600 [DOI] [PubMed] [Google Scholar]
- Wong JS, & Schonlau M (2013). Does bully victimization predict future delinquency?: A propensity score matching approach. Criminal Justice and Behavior, 40(11), 1184–1208. https://doi.org/10.1177%2F0093854813503443 [Google Scholar]
- Yahner J, Dank M, Zweig JM, & Lachman P (2015). The co-occurrence of physical and cyber dating violence and bullying among teens. Journal of Interpersonal Violence, 30(7), 1079–1089. https://doi.org/10.1177%2F0886260514540324 [DOI] [PubMed] [Google Scholar]
- Ybarra ML, Boyd D, Korchmaros JD, & Oppenheim J (2012). Defining and measuring cyberbullying within the larger context of bullying victimization. Journal of Adolescent Health, 51(1), 53–58. 10.1016/j.jadohealth.2011.12.031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ybarra ML, Espelage DL, & Mitchell KJ (2007). The Co-occurrence of internet harassment and unwanted sexual solicitation victimization and perpetration: Associations with psychosocial indicators. Journal of Adolesc Health, 41, S31–S41. https://doi-org/10.1016/j.jadohealth.2007.09.010 [DOI] [PubMed] [Google Scholar]; Zucker RA & Noll RB The Antisocial Behavior Checklist, East Lansing,MI: Department of Psychology, Michigan State University, 1980, unpublished instrument. [Google Scholar]