

Key Points
Question
Are T-cell responses to the SARS-CoV-2 Omicron variant conserved in anti-CD20–treated patients with multiple sclerosis after COVID-19 messenger RNA vaccination?
Findings
In this cohort study of 20 patients treated with ocrelizumab, Omicron spike-specific CD4 and CD8 T cells were detectable in approximately half of patients 6 months after the second vaccine dose, and cytotoxic T-cell responses increased following the third dose. Frequencies of T cells specific to the Delta and Omicron variants were lower compared with the vaccine strain, both before and after receiving a booster dose.
Meaning
In this study of anti-CD20–treated patients with multiple sclerosis, the vaccine-induced T-cell responses were little affected by the mutations carried by Omicron and might prevent severe COVID-19 infection, and a third vaccine dose improved cytotoxic T-cell responses against Omicron.
This cohort study evaluates T-cell responses to the Omicron spike protein in anti-CD20–treated patients with multiple sclerosis (MS) before and after a third messenger RNA COVID-19 vaccination.
Abstract
Importance
The SARS-CoV-2 variant B.1.1.529 (Omicron) escapes neutralizing antibodies elicited after COVID-19 vaccination, while T-cell responses might be better conserved. It is crucial to assess how a third vaccination modifies these responses, particularly for immunocompromised patients with readily impaired antibody responses.
Objective
To determine T-cell responses to the Omicron spike protein in anti-CD20–treated patients with multiple sclerosis (MS) before and after a third messenger RNA COVID-19 vaccination.
Design, Setting, and Participants
In this prospective cohort study conducted from March 2021 to November 2021 at the University Hospital Geneva, adults with MS receiving anti-CD20 treatment (ocrelizumab) were identified by their treating neurologists and enrolled in the study. A total of 20 patients received their third dose of messenger RNA COVID-19 vaccine and were included in this analysis.
Interventions
Blood sampling before and 1 month after the third vaccine dose.
Main Outcomes and Measures
Quantification of CD4 and CD8 (cytotoxic) T cells specific for the SARS-CoV-2 spike proteins of the vaccine strain as well as the Delta and Omicron variants, comparing frequencies before and after the third vaccine dose.
Results
Of 20 included patients, 11 (55%) were male, and the median (IQR) age was 45.8 (37.8-53.3) years. Spike-specific CD4 and CD8 T-cell memory against all variants were maintained in 9 to 12 patients 6 months after their second vaccination, albeit at lower median frequencies against the Delta and Omicron variants compared with the vaccine strain (CD8 T cells: Delta, 83.0%; 95% CI, 73.6-114.5; Omicron, 78.9%; 95% CI, 59.4-100.0; CD4 T cells: Delta, 72.2%; 95% CI, 67.4-90.5; Omicron, 62.5%; 95% CI, 51.0-89.0). A third dose enhanced the number of responders to all variants (11 to 15 patients) and significantly increased CD8 T-cell responses, but the frequencies of Omicron-specific CD8 T cells remained 71.1% (95% CI, 41.6-96.2) of the responses specific to the vaccine strain.
Conclusions and Relevance
In this cohort study of patients with MS treated with ocrelizumab, there were robust T-cell responses recognizing spike proteins from the Delta and Omicron variants, suggesting that COVID-19 vaccination in patients taking B-cell–depleting drugs may protect them against serious complications from COVID-19 infection. T-cell response rates increased after the third dose, demonstrating the importance of a booster dose for this population.
Introduction
The SARS-CoV-2 variant B.1.1.529 (Omicron) was designated a variant of concern in November 20211 and is spreading rapidly. The protection provided by current COVID-19 vaccines is not established. Preliminary studies suggest that antibodies neutralizing Omicron, which carries multiple mutations in the spike protein, critically wane in the months following heterologous infection or vaccination.2,3 A third vaccine dose seems to boost neutralizing antibodies, although less efficiently than for the B.1.617.2 (Delta) variant.2 Whether the mutations in Omicron spike protein affect T-cell recognition, which is known to be less affected than antibodies for other variants,4 is still under investigation.
T-cell responses have a role in protection against severe COVID-19, and their importance is further underlined when antibody responses to vaccination are defective. We and others have recently shown that in patients with multiple sclerosis (MS) taking anti-CD20 treatment, 2 doses of COVID-19 messenger RNA (mRNA) vaccines induce suboptimal antibody responses but robust and functional T-cell responses against the vaccine strain.5,6 In the current situation and specifically for this vulnerable population, it is critical to understand if Omicron-specific T cells are elicited by 2 or 3 doses of mRNA vaccine, particularly because monoclonal antibodies that are given to these patients to alleviate symptoms are mainly ineffective against Omicron.3 Here, we report the T-cell responses to Omicron compared with the vaccine strain and Delta variant in anti-CD20–treated patients with MS before and following the third dose of COVID-19 mRNA vaccines.
Methods
This prospective cohort study was initiated in March 2021 at the Geneva University Hospitals, Switzerland, according to the principles of Good Clinical Practice and approved by the Geneva Cantonal Ethics Commission (2021-00430). All study participants provided written informed consent. Participants who received their third dose of mRNA COVID-19 vaccine before November 1, 2021, were included in the analyses, and blood was sampled before and 30 days after vaccination. Study details, methods on peripheral blood mononuclear cells (PBMC) preparation, anti–SARS-CoV-2 nucleoprotein and receptor-binding domain (RBD) antibody measurement, and T-cell assays are found elsewhere5 and in the eMethods in the Supplement. Briefly, specific T cells were measured using the activation-induced marker (AIM) assay. PBMC were stimulated with peptide pools covering the different spike proteins, and specific T cells were identified by the expression of activation surface markers, such as 4-1BB, CD69, and OX40. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Statistical analysis was performed with GraphPad Prism version 8.0.2 (GraphPad). Quantitative variables were compared using Wilcoxon signed rank test either including the entire cohort or responders only, as indicated, and 2-tailed P values less than .05 were considered statistically significant.
Results
Of 20 included patients with MS receiving anti-CD20 monotherapy (ocrelizumab), 11 (55%) were male and 9 (45%) were female, and the median (IQR) age was 45.8 (37.8-53.3) years. A total of 16 patients received a third dose of mRNA-1273 (Moderna; 100 μg) and 4 received a third dose of BNT162b2 (Pfizer-BioNTech), with a median (IQR) interval between the second and third dose of 26.7 (22.3-29.0) weeks. Before the booster dose, 11 patients were seropositive for anti-RBD antibodies, increasing to 13 patients 1 month after the third dose, and antibody levels rose significantly (geometric mean titer, 3.5 U/mL to 57.9 U/mL) (Table; eFigure in the Supplement). One patient had been infected before vaccination as witnessed by detectable anti-nucleoprotein antibodies (Table).
Table. Demographic Details and Serological Results Among Patients With Multiple Sclerosis.
| Characteristic | No. (%) |
|---|---|
| Total, No. | 20 |
| Sex | |
| Female | 9 (45) |
| Male | 11 (55) |
| Age, median (IQR), y | 45.8 (37.8-53.3) |
| Anti-CD20 therapya | |
| Ocrelizumab, 600 mg | 20 (100) |
| History of COVID-19 infection by RT-PCR | 1 (5) |
| Positive antinucleoprotein serology before the third dose | 1 (5) |
| Vaccine | |
| BNT162b2 | 4 (20) |
| mRNA-1273 | 16 (80) |
| Interval between second and third dose, median (IQR), wk | 26.7 (22.3-29.0) |
| Anti-RBD Ig antibody geometric mean titer, mean (SD), U/mL | |
| At third dose | 3.5 (10.2) |
| At 30 d after third dose | 57.9 (83.4) |
| Seropositive >0.8U/mL | |
| At third dose | 11 (55) |
| At 30 d after third dose | 13 (65) |
Abbreviations: RBD, receptor-binding domain; RT-PCR, real-time reverse transcriptase–polymerase chain reaction.
The dose mentioned is the total dose that the individual received in around 2 weeks.
We first measured spike-specific CD8 T cells that have a role in the elimination of SARS-CoV-2–infected cells. These cytotoxic T cells, specific for the vaccine strain and the Delta and Omicron variants, were present before the booster dose in 12, 10, and 9 patients, respectively. Following the booster dose, the number of responders increased to 15 patients for the vaccine strain and to 14 for both variants. The frequencies of specific CD8 T cells were clearly enhanced after the third dose (Figure 1A and B) but were reduced for both variants compared with the vaccine strain before receiving a booster dose (Delta, 83.0%; 95% CI, 73.6-114.5; Omicron, 78.9%; 95% CI, 59.4-100.0) and after receiving a booster dose (Delta, 89.3%; 95% CI, 57.6-100.0; Omicron, 71.1%; 95% CI, 41.6-96.2) (Figure 1C). No difference was observed between levels of Delta-specific and Omicron-specific CD8 T cells (eFigure in the Supplement).
Figure 1. CD8 T-Cell Responses Specific for the Vaccine Strain and Variants Delta and Omicron After the Third Vaccine Dose.
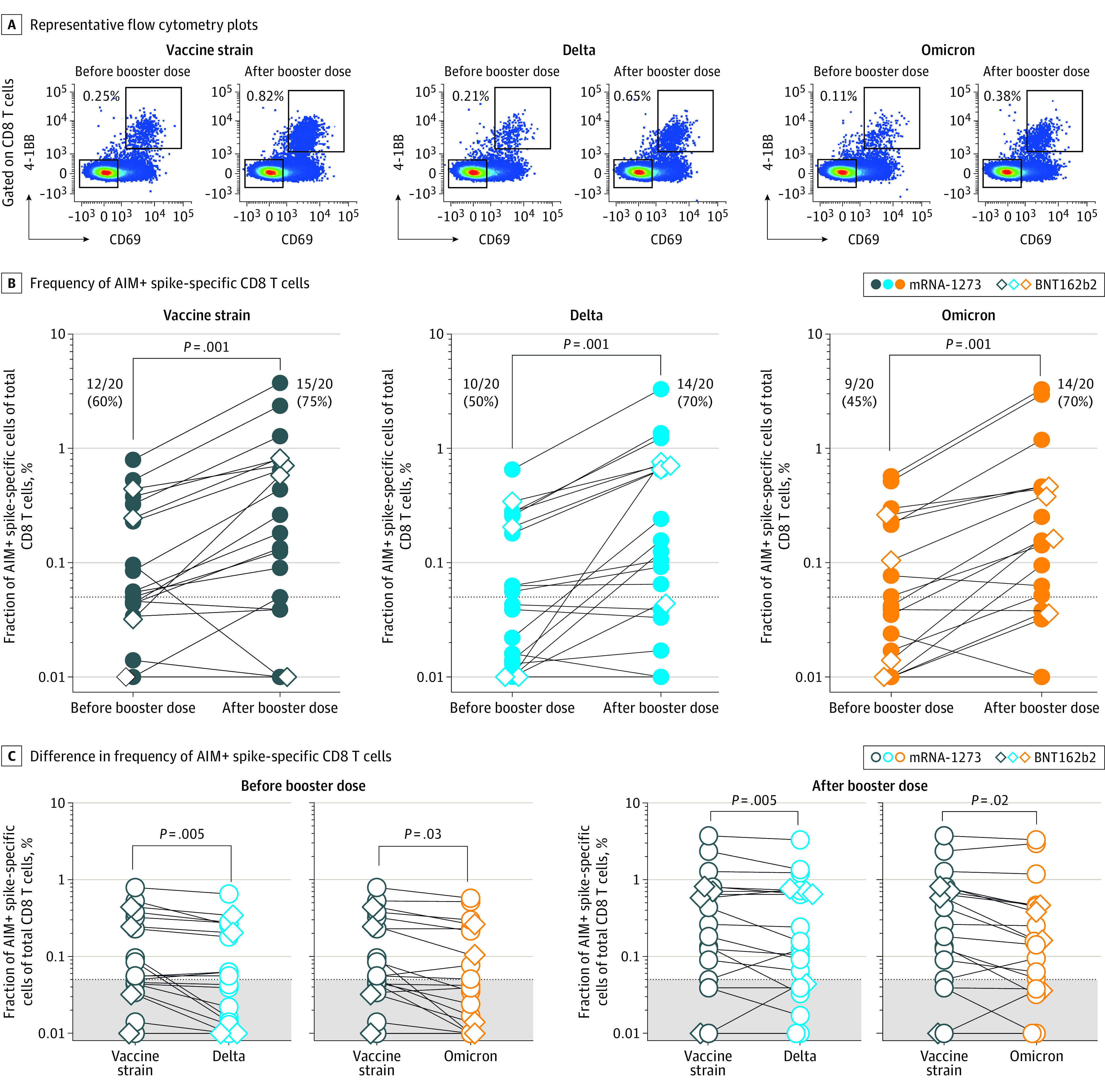
A, Representative flow cytometry plots of CD8 T cells after peripheral blood mononuclear cell stimulation with spike-peptide pools from vaccine strain and the Delta and Omicron variants before and 30 days after the third vaccination. Spike-specific activation-induced marker assay (AIM)–positive CD8 T cells are gated as CD69- and 4-1BB–positive cells. B, Data from 20 ocrelizumab-treated individual patients. Each dot represents 1 patient, and lines connect prebooster and postbooster vaccination frequencies of AIM-positive CD8 T cells specific for SARS-CoV-2 vaccine strain and the Delta and Omicron variants and are background subtracted. The dotted line represents the cutoff limit. Percentages of responders (those with a level above the cutoff limit) are indicated. Patients vaccinated with mRNA-1273 are depicted as closed circles and those with BNT162b2 as open diamonds. The comparison between prebooster and postbooster vaccination was calculated using Wilcoxon signed rank test for all individuals. C, Differences in frequencies of CD8 T cells specific for the spike of vaccine strain vs Delta variant and for the vaccine strain vs Omicron variant in patients before and 30 days after the third vaccine dose. Wilcoxon signed rank test was used on responders to vaccine strain spike to assess differences between variants.
CD4 T cells are known to provide help to B cells, thereby enhancing the production of antibodies with improved neutralizing capacity. Before receiving the booster dose, 9 to 10 patients had detectable memory CD4 T-cell responses, increasing after the booster dose for the vaccine strain (in 15 patients) and for Delta (in 14 patients) but only little for Omicron (in 11 patients). Unlike CD8 T cells, no significant changes in the frequencies of specific CD4 T cells were detected after the booster dose (Figure 2A and B). Delta and Omicron spike-specific CD4 T-cell responses were significantly reduced compared with the vaccine strain to 83.5% (95% CI, 69.4-105.6) for Delta and to 72.3% (95% CI, 53.4-82.7) for Omicron after the booster dose compared with 72.2% (95% CI, 67.4-90.5) and 62.5% (95% CI, 51.0-89.0), respectively, before the booster dose. There was no significant correlation between antibody titers and CD4 or CD8 T-cell levels before or after the booster dose, irrespective of strain specificity (data not shown).
Figure 2. CD4 T-Cell Frequencies Specific for the Vaccine Strain Compared With the Delta and Omicron Variants.
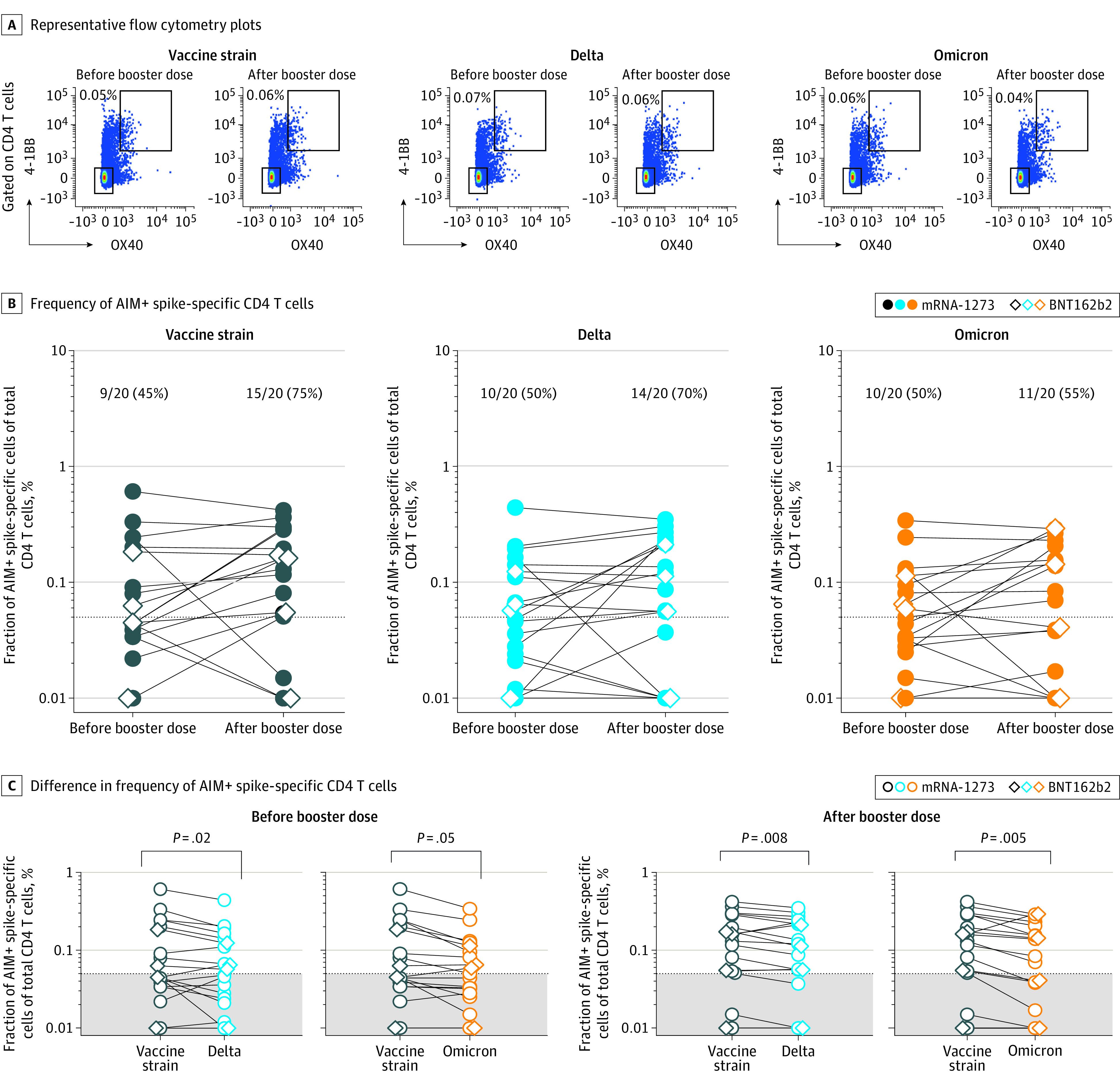
A, Representative flow cytometry plots of CD4 T cells after peripheral blood mononuclear cell stimulation with spike-peptide pools from the vaccine strain and the Delta and Omicron variants before and 30 days after the third vaccination. Spike-specific activation-induced marker assay (AIM)–positive CD4 T cells are gated as OX40- and 4-1BB–positive cells. B, Data from 20 ocrelizumab-treated patients. Each dot represents 1 patient, and lines connect prebooster and postbooster vaccination frequencies of CD4 T cells specific for SARS-CoV-2 vaccine strain and the Delta and Omicron variants and are background subtracted. The dotted line represents the cutoff limit. Percentages of responders (those with a level above the cutoff limit) are indicated. Patients vaccinated with mRNA-1273 are depicted as closed circles and those with BNT162b2 as open diamonds. The comparison between prebooster and postbooster vaccination was calculated using Wilcoxon signed rank test for all individuals. C, Differences in frequencies of CD4 T cells specific for the spike of vaccine strain vs Delta variant and for the vaccine strain vs Omicron variant in patients before and 30 days after the third vaccine dose. Wilcoxon signed rank test was used including only responders to the vaccine strain spike.
Last, we assessed the memory phenotype of spike-specific CD8 and CD4 T cells, as these cells are recalled on encounter with SARS-CoV-2. Spike-specific CD4 and CD8 T cells mostly had an effector phenotype independent of the variant, indicating their capacity to quickly respond in case of infection (eTable in the Supplement).
Discussion
In anti-CD20–treated patients with MS, SARS-CoV-2–specific antibody titers are low or undetectable after 2 doses of mRNA vaccine5,6,7 and are not restored after a third dose, as shown here and for patients with lymphoma.5,8 Antibodies are crucial in the prevention of infection through inhibition of viral entry and in the elimination of infected cells through antibody-mediated killing. Even if antibody responses are largely impaired in anti-CD20–treated patients, T-cell responses after 2 vaccine doses developed similarly to immunocompetent individuals.9 Activated T cells have an important role in the clearance of infected cells and in the control of viral load, which may decrease duration and intensity of symptoms.10 With the emergence of variants such as Omicron that can evade neutralizing antibodies, even at high titers, T-cell responses become even more important, and their presence may still provide protection from the severe forms of COVID-19.
In this study, 6 months after the second vaccine dose, memory T-cell responses to Delta and Omicron were detectable in around half of patients, in line with the durability of the response in healthy individuals.9 The number of responders increased for both CD4 and CD8 T cells after the third vaccine dose, showing that those with undetectable memory response after the primary vaccine series can be boosted. Importantly, a third dose increased the frequency of cytotoxic CD8 T cells, which are particularly important in viral defense, irrespective of the SARS-CoV-2 variant. Yet both before and after the booster dose, their frequencies were lower against Omicron, similar to the moderate decrease observed in healthy individuals 5 to 6 months after 2 doses.11 This could indicate that the recognition of T cells may be partially compromised as mutations accumulate in variants of concern.
Limitations
This study has limitations. The interpretation of our results is limited by the low sample size and the lack of comparison with other treatments or control populations. Given that the level of vaccine-specific T-cell responses in anti-CD20–treated patients with MS is similar to healthy controls after 2 doses, one could expect comparable levels after a third dose. Accordingly, others have reported similar levels of Omicron-specific T cells in healthy individuals.11 Furthermore, the postvaccination follow-up is limited. The monitoring of breakthrough infections in this population is needed to confirm the benefit of vaccination, in particular against Omicron.
Conclusions
In this cohort study of patients with MS treated with ocrelizumab, a COVID-19 mRNA booster vaccination induced robust T-cell responses to both Delta and Omicron. However, their frequencies were lower compared with the vaccine strain, and the clinical implications of these findings need to be assessed.
eMethods.
eFigure. Comparison of anti-RBD antibody and frequencies of Delta- and Omicron-specific T cells.
eTable. Effector memory phenotype of spike-specific CD4 and CD8 T cells in anti-CD20–treated MS patients before and after the third vaccine dose.
References
- 1.World Health Organization . Classification of Omicron (B.1.1.529): SARS-CoV-2 variant of concern. Accessed December 19, 2021. https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern
- 2.Garcia-Beltran WF, St Denis KJ, Hoelzemer A, et al. mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell. 2022;185(3):457-466.e4. doi: 10.1016/j.cell.2021.12.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wilhelm A, Widera M, Grikscheit K, et al. Reduced neutralization of SARS-CoV-2 Omicron variant by vaccine sera and monoclonal antibodies. medRxiv. Preprint posted online December 8, 2021. doi: 10.1101/2021.12.07.21267432 [DOI]
- 4.Tarke A, Sidney J, Methot N, et al. Impact of SARS-CoV-2 variants on the total CD4+ and CD8+ T cell reactivity in infected or vaccinated individuals. Cell Rep Med. 2021;2(7):100355. doi: 10.1016/j.xcrm.2021.100355 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Madelon N, Lauper K, Breville G, et al. Robust T cell responses in anti-CD20 treated patients following COVID-19 vaccination: a prospective cohort study. Clin Infect Dis. 2021;ciab954. doi: 10.1093/cid/ciab954 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Apostolidis SA, Kakara M, Painter MM, et al. Cellular and humoral immune responses following SARS-CoV-2 mRNA vaccination in patients with multiple sclerosis on anti-CD20 therapy. Nat Med. 2021;27(11):1990-2001. doi: 10.1038/s41591-021-01507-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gadani SP, Reyes-Mantilla M, Jank L, et al. Discordant humoral and T cell immune responses to SARS-CoV-2 vaccination in people with multiple sclerosis on anti-CD20 therapy. EBioMedicine. 2021;73:103636. doi: 10.1016/j.ebiom.2021.103636 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Herishanu Y, Rahav G, Levi S, et al. Efficacy of a third BNT162b2 mRNA COVID-19 vaccine dose in patients with CLL who failed standard two-dose vaccination. Blood. 2021;blood.2021014085. doi: 10.1182/blood.2021014085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Goel RR, Painter MM, Apostolidis SA, et al. ; UPenn COVID Processing Unit‡ . mRNA vaccines induce durable immune memory to SARS-CoV-2 and variants of concern. Science. 2021;374(6572):abm0829. doi: 10.1126/science.abm0829 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.de Candia P, Prattichizzo F, Garavelli S, Matarese G. T Cells: warriors of SARS-CoV-2 infection. Trends Immunol. 2021;42(1):18-30. doi: 10.1016/j.it.2020.11.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tarke A, Coelho CH, Zhang Z, et al. SARS-CoV-2 vaccination induces immunological memory able to cross-recognize variants from Alpha to Omicron. bioRxiv. Preprint posted online December 28, 2021. doi: 10.1101/2021.12.28.474333 [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods.
eFigure. Comparison of anti-RBD antibody and frequencies of Delta- and Omicron-specific T cells.
eTable. Effector memory phenotype of spike-specific CD4 and CD8 T cells in anti-CD20–treated MS patients before and after the third vaccine dose.