

Abstract
We report the case of a young woman with CMV infection, high level of creatine kinase and myopathy. Electromyography showed a myopathic pattern. Muscle biopsy showed a marked increase of NADH enzymatic activity in the central area of almost all type I fibres, few degenerative and necrotic fibres and scattered mononuclear cell infiltrates. Ultrastructural analysis showed a marked disarrangement of sarcomeric structure and large inclusions of thin filaments in some fibres, while immunohistochemistry evidenced alteration in desmin, actin and αB-crystallin protein signals. PCR for CMV detection on muscle sections was negative. Histological, immunological and ultrastructural evaluations were compatible with a necrotic inflammatory myopathy. The correlations between CMV liver infection and the myopathic pattern are discussed. This case underscores the need to consider CMV infection in the differential diagnosis of myopathy with undetermined aetiology, quickly providing directions for a targeted muscle pharmacological intervention.
Key words: CMV, muscle biopsy, myofibrillar disorganization, Z-band streaming
Introduction
Viral infections have been frequently reported in association with development of secondary myopathies characterized by different forms of muscle involvement that can vary from mild to severe inflammatory myopathy. Literature reported evidences of nemaline myopathy and myositis after human immunodeficiency infection (HIV) 1, myositis after infection by hepatitis B and C 2, Epstein-Barr virus 3, herpes simplex virus 4 and, less frequently, cytomegalovirus (CMV) 5. Few cases of severe rhabdomyolysis in association with CMV infection 6,7, and a case of polymyositis associated with primary CMV infection were reported 5.
Herein, we describe the case of a young woman with hepatitis by primary CMV infection, muscle weakness, myalgia, oedema and increased serum creatine kinase (CK) levels associated with severe and marked structural alterations in skeletal muscle, whose symptoms improved after immunomodulatory treatment (intravenous immunoglobulin followed by steroid).
Materials and methods
Case history
A 29-year-old female, with a medical history of asymptomatic SARS-CoV-2 infection (September 2020) and Raynaud’s syndrome, was hospitalized in February 2021 because of a CMV hepatitis associated with asymmetrical upper limb muscle weakness. She reported a three-week history of asthenia, myalgia, local swelling, marked oedema in the upper limbs and low-grade fever without any dyspnoea or dysphagia. Needle electromyography (EMG) showed myopathic pattern in the proximal and distal muscles of the four limbs with abundant signs of denervation in the active phase. During hospitalization, haematological analyses showed a progressive macrocytic anemia (up to a Hb 8.8 g/dL, MCV 99.7), reduced blood cell count (leukocyte 3.200/μL, platelets 162.000/μL), and high levels of D-dimer, most likely attributable to a systemic inflammatory state. No myoglobinuria was detected.
Laboratory examinations showed an increase in CK (3371 U/L, n.v. = 26-192) and lactate dehydrogenase (LDH = 536 U/L, n.v. = 125-250) levels and a deranged liver function (ALT = 220 U/L and AST = 549 U/L). Renal function was normal. A full body CT-scan indicated a slightly enlarged spleen.
The serological viral panel for CMV, EBV, HCV, HIV showed positivity for CMV (anti-CMV IgG 80.00 U/mL, IgM 53.70 U/mL). RT-PCR investigation for CMV in skeletal muscle was negative. The screening for autoantibodies (ASMA, AMA, ANA, ANCA, ENA, anti CCP, anti ds-DNA, anti-beta2 glycoprotein and rheumatoid factor) was negative and so was the screening for autoimmune myositis (antibodies anti-PL-7, PL-12, SRP, Mi-2, EJ, MDA-5, TIF-g, SAE1, SAE2, NXP-2). There were no skin lesions suggesting dermatomyositis.
The patient was treated with intravenous immunoglobulins 0.4 mg/kg for 5 days and with steroid therapy (methylprednisolone 500 mg intravenous for 5 days followed by oral prednisone 50 mg daily) with progressive improvement of asthenia and normalization of CK levels (58 U/L).
At the follow-up two months after discharge, the patient reported an almost complete recovery, with normal walking also possible on toes and heels. Haematological analyses were within normal range except for platelets (141.000/μL). A control EMG three months after dismissal showed regression of spontaneous activity in both proximal and distal muscles of four limbs, only modest myopathic signs being evident in the right ileopsoas muscle.
Muscle biopsy
Skeletal muscle biopsy from left quadriceps was performed at the Neurologia-Stroke Unit of Lecco Hospital and sent to our Neuromuscular and Rare Disease Unit for histological, immunohistochemical and electron microscopy evaluations.
Muscle sections from patients without any detectable muscle diseases were used as normal controls while muscle sections from three patients with diagnosed inflammatory myopathy served as pathological controls (all patients had signed written informed consent when they had undergone muscle biopsy).
Tissue specimen was frozen in isopentane-cooled liquid nitrogen and processed according to standard techniques, as previously described 8. For histological analysis, 8 μm-thick cryosections were picked and processed for routine staining with Haematoxylin and Eosin (H&E), Modified Gomori Trichrome (MGT), myosin ATPase (pH 9.4-4.6-4.3), cytochrome c oxidase (COX), succinate dehydrogenase (SDH), phosphatase acid (PA), NADH, Oil Red O, Periodic Acid Schiff (PAS) and Congo Red.
Electron microscopy
For ultrastructural examination, a small part of muscle sample was fixed in 2.5% glutaraldehyde (pH 7.4), post fixed in 2% osmium tetroxide and then, after dehydration in a graded series of ethanol, embedded in Epon’s resin. Finally, ultrathin sections were stained with lead citrate and uranyl acetate and examined with Zeiss EM109 transmission electron microscope.
Immunofluorescence
Immunohistochemical staining was performed for evaluation of inflammatory component using the following mouse monoclonal antibodies: anti-HLA-ABC Antigen/RPE (1:10), anti-MAC (1:50), anti-CD4 (1:50), anti-CD8 (1:10) and anti-CD68 (1:50), all from Dako Agilent (Santa Clara, CA, USA). Mouse monoclonal anti-cytomegalovirus antibody (not diluted, clone CCH2+DDG9; Dako) was used to detect the presence of virus in muscle sections.
For muscle structural evaluation the following antibodies were tested: actin (1:500 rabbit polyclonal; ThermoFisher, Rockford, IL, USA), myotilin (1:10 mouse monoclonal; Novocastra Laboratories, Newcastle upon Tyne, UK), desmin (1:100 mouse monoclonal; Chemicon, Millipore, Billerica, MA, USA), αB-crystallin (1:100 rabbit polyclonal; Chemicon). Slides were then incubated with the appropriate secondary antibody conjugated to Alexa 488 or Alexa 568 (1:200, Invitrogen Life Technologies, Carlsbad, CA, USA).
Results
Light microscopy
The outstanding feature of muscle biopsy was the strong increase of NADH enzymatic activity in the central area of almost all type I fibres while subsarcolemmal areas of reduced enzymatic activity were appreciated in rare type I fibres (Fig. 1D). H&E and MGT stains showed a few degenerative and necrotic fibres and scattered mononuclear infiltration (Figs. 1A-B). No centronucleated fibres were observed. Fibres were normal in shape with a physiological variability in size. Endomysial and perimysial connective tissue was normal. Rare splitting fibres were also observed. ATP-ase staining showed a normal distribution of type I and type II fibres. Diffuse and moderate increase in acid phosphatase activity in necrotic fibres and in the interstitial tissue were detected (Fig. 1C). COX activity was reduced in scattered fibres with normal SDH (Figs. 1E-F). No changes in glycogen and lipid content were observed.
Figure 1.
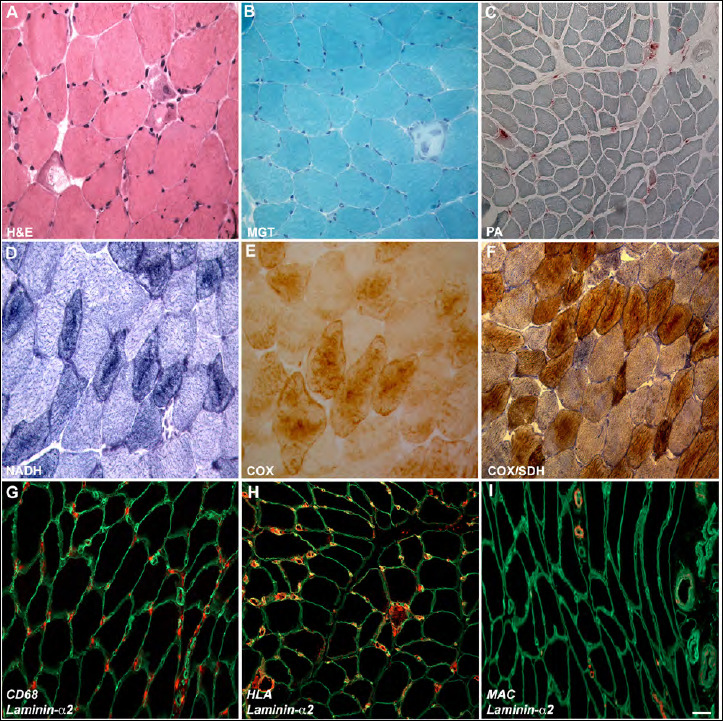
Light microscopy observations. H&E (A) and MGT (B) show few degenerative and necrotic fibres and normal connective tissue (magnification 400 x). Acid phosphate reaction (C) is positive in necrotic fibres and at interstitial level (magnification 200 x). NADH (D) signal is increased in type I fibres, COX (E) and COX-SDH (F) reactions show COX signal reduction in some scattered fibres with normal SDH activity (magnification 400 x). Immunohistochemistry shows CD68 (macrophage) positivity (G), HLA positivity at membrane level and in the cytoplasm of necrotic fibres (H) and MAC positivity in capillaries (I). Laminin-α2 (green) was used for membrane counterstaining (magnification 400 x).
Electron microscopy
Ultrastructural examination showed alteration of sarcomeric structure in several muscle fibres. In particular, we observed three main types of structural changes. In a fair number of fibres, we found thin filamentous inclusions, localized either in the sarcoplasm or at subsarcolemmal level (Figs. 2B, and E). Also, we detected focal areas of myofibrillar disorganization in the centre of otherwise normal muscle fibres (Figs. 2A, C and F). Lastly, as shown in figure 2D, in some areas we observed a disruption of the Z-bands with longitudinal streaming of Z-band material along the sarcomere. Additional observations include a slight increase in lipid droplets (Fig. 2D) and rare lipofuscines (Fig. 2E). Nuclei showed a normal aspect with the exception of those located in the necrotic fibres.
Figure 2.
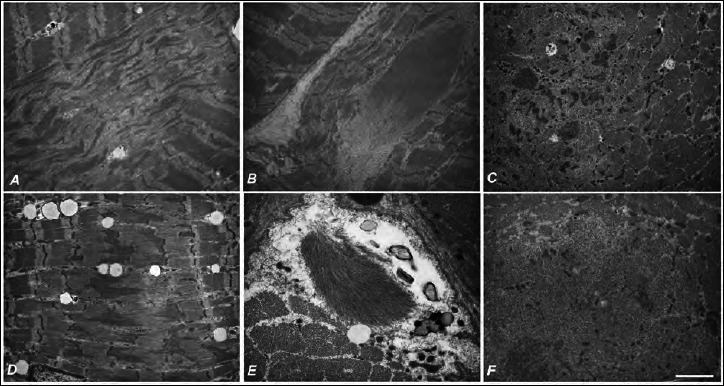
Ultrastructural observation. Central areas of myofibrillar disorganization (A, C, F). Inclusion of thin filaments in the sarcoplasm and in the subsarcolemmal region (B, E). Disruption of the Z-bands with longitudinal streaming of Z-band material, and a slight increase in lipid droplets (D). Scale bar: 2270 nm (A-D), 1420 nm (E, F).
Immunofluorescence
Infiltrating cells were predominantly CD68-positive (Fig. 1G), while rare positivity was observed for CD4 and CD8. Anti-MAC stained some capillaries and anti-HLA showed positivity at the sarcolemma of nearly all muscle fibres and in the cytoplasm of necrotic fibres. Sarcoplasmic HLA-positivity was occasionally observed in some non-necrotic fibres (Figs. 1H-I). No positivity was observed in muscle biopsy tissue from controls.
In addition, several other alterations in fluorescent signals were detected compared to control muscles. In particular, anti-desmin staining showed a discontinuous signal at membrane level as well as a diffuse cytoplasmic signal mostly localized in the central area of several fibres. This positivity was different from the vacuolar staining observed in diagnosed inflammatory myopathies. In control muscles desmin staining was localized only at membrane level (Fig. 3).
Figure 3.
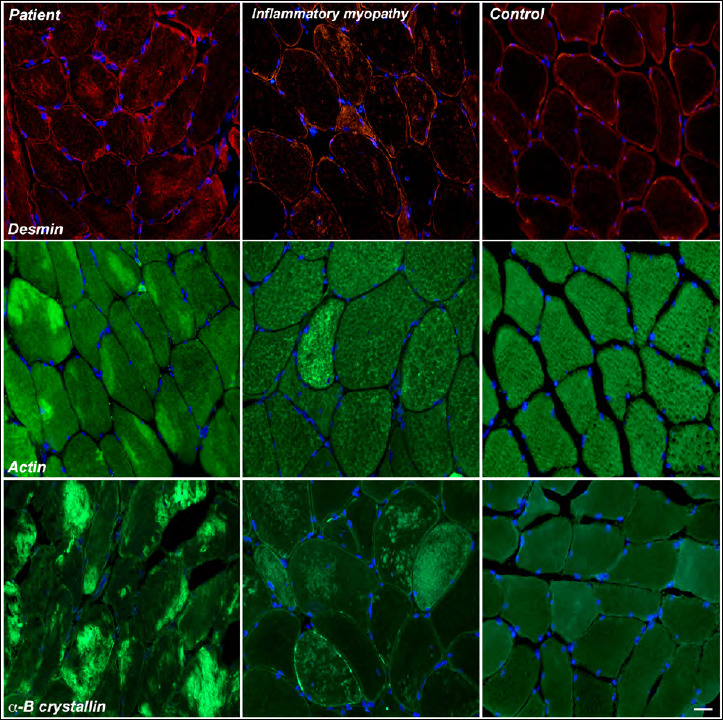
Desmin, actin and αB-crystallin staining in our patient, in diagnosed inflammatory myopathy and in control muscle. Nuclei were detected with DAPI. Magnification 400 x.
Anti-actin staining showed areas of strong positivity in a discrete number of fibres, mainly localized at subsarcolemmal level. No alterations were detectable in both control muscles and in inflammatory myopathy specimens (Fig. 3).
With αB-crystallin staining, many fibres showed a diffuse strong positivity in aggregate-like structures, in some other fibres, however, the staining was localized either in subsarcolemmal areas, or extended to the almost totality of the cytoplasm. This pattern is totally different from what we see in inflammatory myopathies (Fig. 3).
Conclusions
We report the case of a young woman, hospitalized because of a CMV hepatitis and muscle weakness, discharged with a diagnosis of autoimmune myositis. Routine muscle histology was suggestive of a primary necrotizing inflammatory myopathy with peculiar central areas of increased NADH activity in type I fibres. Further investigation by ultrastructural analysis showed, in several fibres, large inclusions of thin filaments, focal areas of myofibrillar disorganization and disruption of the Z-bands with longitudinal streaming of Z-band material along the sarcomere. Immunofluorescence showed marked alterations in desmin, actin and αB-crystallin expression and localization in several fibres.
These findings are quite unique for a primary myositis and, to our knowledge, no cases of similar “secondary myopathies” have ever been associated with CMV hepatitis. A previous single case of muscle weakness, diffuse myalgia with rhabdomyolysis and acute respiratory paralysis probably associated with CMV infection was reported 7.
Although the presence of viral particles has not been confirmed in skeletal muscle by real-time PCR or immunohistochemistry, and the mechanism through which the virus could affect skeletal muscle is still unknown, we can hypothesize that the CMV infection has caused the observed alterations in skeletal muscle as an indirect host-derived effect. Indeed, besides the direct viral liver infection, indirect effects probably mediated by the immunological response can cause detrimental consequences including skeletal muscle alterations 9. However, a possible direct viral muscle infection cannot be completely excluded. Indeed, viral count could have remained below threshold detection level due to methodological limits and/or very low (latent) viral activity when PCR was performed. Ultrastructural changes have been reported in different types of CMV-infected cells as direct effects: in human bone marrow fibroblasts, mitochondrial enlargement, production of dense bodies and cytoplasmic accumulation were observed 10. During in vitro CMV infection, a rapid and progressive alteration of actin, microfilaments and cytoskeleton was observed in both human embryo and lung fibroblasts 11, however what happens in cells and tissues not directly invaded by the virus is still poorly understood.
The clear improvement of the electromyographic pattern following the acute phase, confirms the non-primary nature of the myopathy.
To summarize, several issues – clinical presentation, serological and neurophysiological evidence, skeletal muscle findings and progressive improvement of clinical and instrumental parameters after therapy – favour the hypothesis of an autoimmune/inflammatory myopathy. We could not demonstrate the presence of viral particles in skeletal muscle, but, as explained, an indirect host-derived effect is likely implicated, not to mention concomitance between liver infection and onset of myopathic symptoms.
The study of this case has an important implication for the medical internist approach towards primary CMV viral infection; indeed, the presence of symptoms induced by viral hepatitis could cause underestimation of severe effects on other tissues/organs including skeletal muscle.
Also, our report underscores the need to consider CMV infection in the differential diagnosis of myopathy with undetermined aetiology, providing directions for a targeted muscle pharmacological intervention.
Acknowledgements
This work is promoted within the European Reference Network for Neuromuscular Diseases (ERN-NMD), MS as HCP Representative for the Italian ERN-NMD.
We also thank the “Bank of muscle tissue, peripheral nerve, DNA and cell culture”, member of Telethon network of Genetic Biobanks, at Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico, Milano, Italy and the Associazione Amici del Centro Dino Ferrari.
We thank Patrizia Ciscato, BSc, for performing histology-histochemistry reactions. We thank Prof. G. P. Comi, Dr M. Moggio, Dr A. Rigamonti and Dr A. Salmaggi for contribution to discussion.
Figures and tables
Footnotes
Conflict of interest statement
The Authors declare no conflict of interest
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors’ contributions
MR and SZ wrote the manuscript, MR, LN, MS, SZ interpreted the results, revised the literature and revised the manuscript. VM performed clinical evaluation.
Ethical consideration
All procedures were in accordance with the standards of the bioethical committee and the Declaration of Helsinki.
References
- 1.Johnson RW, Williams FM, Kazi S, et al. Human immunodeficiency virus-associated polymyositis: a longitudinal study of outcome. Arthritis Rheum 2003;49:172-178. https://doi.org/10.1002/art.11002 10.1002/art.11002 [DOI] [PubMed] [Google Scholar]
- 2.Nojima T, Hirakata M, Sato S, et al. A case of polymyositis associated with hepatitis B infection. Clin Exp Rheumatol 2000;18:86-88. [PubMed] [Google Scholar]
- 3.Uchiyama T, Arai K, Yamamoto-Tabata T, et al. Generalized myositis mimicking polymyositis associated with chronic active Epstein-Barr virus infection. J Neurol 2005;252:519-525. https://doi.org/10.1007/s00415-005-0679-1 10.1007/s00415-005-0679-1 [DOI] [PubMed] [Google Scholar]
- 4.Schlesinger JJ, Gandara D, Bensch KG. Myoglobinuria associated with herpes-group viral infections. Arch Intern Med 1978;138:422-424. [PubMed] [Google Scholar]
- 5.Maeda M, Maeda A, Wakiguchi H, et al. Polymyositis associated with primary cytomegalovirus infection. Scand J Infect Dis 2000;32:212-214. https://doi.org/10.1080/003655400750045367 10.1080/003655400750045367 [DOI] [PubMed] [Google Scholar]
- 6.Hughes GS, jr., Hunt R. Cytomegalovirus infection with rhabdomyolisis and myoglobinuria. Ann Intern Med 1984;101:276-277. https://doi.org/10.7326/0003-4819-101-2-276_2 10.7326/0003-4819-101-2-276_2 [DOI] [PubMed] [Google Scholar]
- 7.Hirohama D, Shimizu T, Hashimura K, et al. Reversibile respiratory failure due to rhabdomyolysis associated with cytomegalovirus infection. Inter Med 2008;47:1743. https://doi.org/10.2169/internalmedicine.47.1349 10.2169/internalmedicine.47.1349 [DOI] [PubMed] [Google Scholar]
- 8.Napoli L, Crugnola V, Lamperti C, et al. Ultrastructural mitochondrial abnormalities in patients with sporadic amyotrophic lateral sclerosis. Arch Neurol 2011;68:1612-1613. https://doi.org/10.1001/archneur.68.12.1612 10.1001/archneur.68.12.1612 [DOI] [PubMed] [Google Scholar]
- 9.Freeman RB, Jr. The ‘indirect’ effects of cytomegalovirus infection. Am J Transplantation 2009;9:2453-2458. https://doi.org/10.1111/j.1600-6143.2009.02824.x 10.1111/j.1600-6143.2009.02824.x [DOI] [PubMed] [Google Scholar]
- 10.Gilloteaux J, Nassiri MR. Human bone marrow fibroblasts infected by cytomegalovirus: ultrastructural observations. J Submicrosc Cytol Pathol 2000;32:17-45. [PubMed] [Google Scholar]
- 11.Jones NL, Lewis JC, Kilpatrick B. Cytoskeletal disruption during human cytomegalovirus infection of human lung fibroblasts. Eur J Cell Biol 1986;41:304-312. [PubMed] [Google Scholar]