

Abstract
Objective
Identifying muscle weakness and probable sarcopenia using strength tests requires reference data. This study aimed to provide age- and sex-specific normative data for grip strength and common variations of the Sit-to-Stand (STS) test: time to complete 5 stands (5x-STS) and number of stands completed in 30 seconds (30s-STS). Predictors of test performance were also explored.
Methods
Dominant hand grip strength was assessed in adults (age = 18–80 years) using a digital dynamometer, and 5x-STS and 30s-STS performance were assessed synchronously during a single 30-second test. Sex-specific centile curves were generated using the lambda-mu-sigma method.
Results
Data from 2301 participants (female = 1682, male = 619) were included. Peak median grip strength occurred in female participants at 33.9 years of age (27.9 kg) and in male participants at 37.6 years of age (47.2 kg). 5x-STS and 30s-STS performance peaked at the youngest age (18.0 years) in both female participants (8.16 seconds and 17.2 repetitions) and male participants (8.02 seconds and 17.7 repetitions). Test performances were lowest for all tests at the oldest age in the database. Predictors of better test performance included lower age and higher self-reported physical functioning and appendicular skeletal muscle mass, to name a few. White participants had better performance than Black participants on the STS tests.
Conclusion
The generated centile curves reveal the pattern of change in muscle strength for tests recommended to identify probable sarcopenia. The curves can be used in rehabilitation to assess an individual’s performance relative to sex- and age-specific norms. To aid use of the data, a downloadable Excel-based calculator is provided to compute participant-specific percentiles, z scores, and t scores for each outcome and plot performance on the centile curves.
Impact
Physical therapists have an important role in identifying and treating individuals with sarcopenia and other causes of muscle weakness. The reference data provided for common clinical muscle strength tests provide therapists an ability to assess an individual’s relative performance.
Lay Summary
Knowing the normal or expected strength for an individual’s age and sex is essential to identifying muscle weakness. This study provides age- and sex-specific normal values for hand grip strength and sit-to-stand tests in adults aged 18 to 80 years.
Keywords: Cachexia, Chair Stand Test, Grip Strength, Normative Data, Sarcopenia, Sit To Stand Test
Introduction
Sarcopenia is a generalized skeletal muscle disorder characterized by accelerated loss of muscle mass and function.1 Historically considered a condition of aging (primary sarcopenia), sarcopenia is now recognized as a sequela in an ever-growing number of disease states (secondary sarcopenia), where it contributes to physical disability, falls, fractures, and mortality.2 According to the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), sarcopenia is probable when low strength is detected, with the diagnosis confirmed by the coexistence of low muscle quantity or quality.2 The identification of low strength with clinically performed muscle strength tests requires the availability of reference data.
Grip strength is the most recognized clinical muscle strength test for identifying probable sarcopenia.2–7 It has predictive validity in terms of falls, disability, impaired quality of life, and hospital length of stays8–10 and is reportedly a stronger predictor of cardiovascular mortality than systolic blood pressure.11 A benefit of grip strength is the availability of normative data across the life span.12–14 However, grip strength may not be a proxy for muscle strength at other sites, such as the lower extremities.15
To clinically assess lower extremity muscle strength and aid in identifying probable sarcopenia, performance on a Sit-to-Stand test (STS; also known as a chair rise or stand test) has been suggested.2,4 Some guidelines3,5 refer to STS tests more as physical performance tests because they are influenced by factors beyond strength; however, their addition as a strength test may aid in identifying sarcopenia in groups distinct from those identified via grip strength.16 Irrespective of the tests’ categorization, poor performance on the 2 most common STS test variations—the time to complete 5 stands from a seated position (5×-STS )17 and the number of stands completed in 30 seconds (30s-STS)18—can be predictive of poor outcomes.19,20
The 5×-STS and 30s-STS tests may identify probable sarcopenia but also have utility in assessing strength and physical performance in alternate disease states commonly seen in physical therapy and during physical training and rehabilitation.21–23 Because their use spans varying stages of life, there is a need for normative data for both STS tests across the life span. Currently available normative data are either prinicipally in older individuals18,24,25 or stratified by blocks of age (usually decades).18,25–29 The former is not consistent with the life course epidemiology framework,30 and the latter does not readily allow the calculation of patient-specific percentiles, z scores, and t scores (ie, performance relative to that of young individuals who are healthy). Landi et al31 and Suetta et al32 recently reported centile curves for 5×-STS and 30s-STS performance across the adult life span, respectively. However, data were obtained in geographically distinct populations, which may not be representative of those living in other regions, and testing procedures were incompletely described.
The purpose of the present study was to provide age- and sex-specific centile curves for grip strength and the 5×-STS and 30s-STS tests across adulthood in a Midwest US population. Normative data for grip strength are well established but were developed in the current sample to assess the comparability of our cohort with others. In contrast, there is a limited availability of reference values over the age span for the STS tests. A secondary purpose was to explore predictors of test performance. The ultimate goal was to use the cumulative data to provide clinicians and researchers a practical calculator to compute patient-specific percentiles, z scores, and t scores for each outcome and plot test performance on the centile curves.
Methods
Study Design and Participants
Data were retrieved from the initial 2594 participants tested between December 2017 and May 2021 within the Musculoskeletal Function, Imaging, and Tissue (MSK-FIT) Resource Core of the Indiana Center for Musculoskeletal Health’s Clinical Research Center (Indianapolis, IN, USA). Participants are recruited to the core by investigators seeking the standardized performance of physical function tests performed by their research participants as well as via self-referral from the local community. The core has institutional review board approval from Indiana University to test all comers who provide written informed consent, irrespective of current or previous health status. To be eligible for inclusion in the current dataset, participants needed to be between 18 and 80 years old and to have completed the STS and dominant hand grip strength tests as described below with pain ≤3 out of 10 on a verbal reporting scale. An upper age limit of 80 years was selected because the MSK-FIT Resource Core cohort currently has a limited number of participants beyond this age, with centile curves being sensitive to low numbers of individuals at the tail of distributions.
Participant Characteristics
Height (to nearest 0.1 cm) and weight (to nearest 0.1 kg) were measured without shoes using a calibrated stadiometer (Seca 264; Seca GmbH & Co, Hamburg, Germany) and scale (MS140–300; Brecknell, Fairmont, MN, USA). Self-reported race was categorized as White, Black or African American, Asian, or Other (including individuals reporting as being multiracial). The physical function (PF) domain of the National Institutes of Health Patient-Reported Outcomes Measurement Information System (PROMIS) computerized adaptive test (CAT) (PROMIS PF CAT; version 1.2) was used to assess self-reported functional health. Appendicular skeletal muscle mass relative to height (ASM/height2; kg/m2) was assessed by whole-body dual-energy x-ray absorptiometry (DXA) (Norland Elite; Norland at Swissray, Fort Atkinson, WI, USA).
Grip Strength Test
Dominant hand grip strength was measured with a Jamar Plus+ digital hand dynamometer (Sammons Preston, Bolingbrook, IL, USA), according to the Southampton Grip-Strength Measurement Protocol9 and using a standardized script and procedure (Suppl. Appendix 1). Dynamometer performance was confirmed weekly by applying known masses. The self-identified most dominant hand was tested in ambidextrous individuals. The dynamometer handle was set in the second smallest position unless deemed uncomfortable by the participant.
For testing, the participant sat upright in a chair with feet flat on the floor, elbow at 90 degrees of flexion, and forearm on the arm rest of the chair. The wrist was over the end of the arm rest with forearm in mid-pronation/supination so the dynamometer was unsupported and held vertical. The participant squeezed as hard as they could for a minimum of 3 seconds, keeping their trunk and arm stationary. The tester instructed the participant to “squeeze, squeeze, squeeze” with a consistent tone and volume. No additional motivational input was provided. The peak reading was recorded and the test repeated twice more with 30-second intervening rest periods. The maximum peak grip strength recorded from the 3 trials was used in analyses. Pain limiting test performance was recorded using a verbal rating scale from 0 to 10.
Sit-to-Stand Test
5×-STS performance and 30s-STS performance were assessed synchronously during a single 30-second test using a prescribed script and procedure (Suppl. Appendix 1). Each test was performed in shoes and with a standardized chair (seat height = 45 cm). Following test demonstration, the participant completed an initial single STS maneuver with their arms folded across their chest. Following satisfactory completion of the initial trial and once the participant was ready, the tester said “Ready, go!” and simultaneously started both a countdown timer set to 30 seconds and a stopwatch. The tester counted aloud with a consistent tone and volume each time the participant stood up. No additional motivational input was provided. If the participant did not complete the STS maneuver correctly (eg, did not come to a full erect stand or arms came away from body), the test was stopped, demonstration repeated, and test restarted after a 1-minute rest. The tester stopped the stopwatch once the participant stood up completely for the fifth time (5×-STS) and continued counting as the participant completed each subequent stand until the 30-second countdown timer expired (30s-STS). If a halfway standing position was reached when time elasped, it was counted as a stand. Pain limiting test performance was recorded using a verbal rating scale from 0 to 10.
Data Analyses
Analyses were performed separately for women and men. Participant characteristics were described according to decade stage of life, with categorical variables summarized by frequencies and percentages, and continuous variables summarized by means (SDs) and/or medians (interquartile ranges).
Grip strength, 5×-STS, and 30s-STS centile curves were generated using the lambda-mu-sigma (LMS) method33 with R package GAMLSS (version 5.2.0).34 In the LMS method, Box-Cox transformation is used to achieve normality at a given age. Nonparametric smooth curves are fit to the parameter values across the age range using penalized likelihood with penalty on the second derivatives. Once parameter curves are estimated, centile curves, z scores, and t scores can be calculated.
As per convention, z scores represent the number of SDs the patient-specific outcome varies from age- and sex-matched median outcomes, whereas t scores represent the number of SDs the patient-specific outcome varies from the best sex-specific median outcome. Because the LMS method to achieve normality constrains maximum obtainable z and t scores, LMS-derived z and t scores are not suited for identifying extreme values. To address this, modified z and t scores are provided in the current dataset for scores greater than +2. In the modified z scores, the outcome of interest is expressed relative to the sex- and age-matched median in units of one-half the distance between 0 and + 2 z scores in accordance with the approach used for growth charts by the Centers for Disease Control and Prevention.35 Modified t scores are expressed in units one-half the distance between 0 and + 2 z scores at the age of best sex-specific median test performance.
Receiver operating characteristic curves were generated using IBM SPSS Statistics (v27; IBM Corp, Armonk, NY, USA), and the areas under the curves (AUCs) were used to assess the ability of the muscle strength tests to discriminate between individuals with and individuals without DXA-identified sarcopenia. DXA-identified sarcopenia was determined based on EWGSOP2-recommended ASM/height2 cutoffs (women: <5.5 kg/m2, men: <7.0 kg/m2).2 AUCs were assigned as nondiscriminatory (0.50), poor (0.51–0.60), acceptable (0.61–0.70), excellent (0.71–0.80), or outstanding (>0.90).36
Multivariable linear regression models were used with SAS 9.4 (SAS Institute, Cary, NC, USA) to build predictive models for test performance. Data were 1:1 randomly split into a training dataset and a validating dataset. Stepwise model selection was used to find the best mode for a given model size using the training dataset. The optimal predicting model was then selected according to prediction errors using the validating dataset from the best models of different sizes. Two-sided P values <.05 were considered statistically significant.
Role of the Funding Source
The funders played no role in the design, conduct, or reporting of this study.
Results
Participant Characteristics
A total of 2301 participants (1682 women, 619 men) from the initial MSK-FIT Resource Core cohort were included. Reasons for exclusion were age <18 years (n = 85) or >80 years (n = 47), STS test not performed and/or nondominant hand grip strength assessed (n = 48), and pain reported at >3 out of 10 during grip strength and/or STS testing (n = 113). Characteristics of included women and men are reported in Table 1 and Table 2, respectively. Women and men ranged in age from 18.0 to 80.0 years and 18.0 to 79.3 years, respectively.
Table 1.
Participant Characteristics and Muscle Strength Test Performance Stratified by Decade of Age for Womena
| Age Group: | ||||||
|---|---|---|---|---|---|---|
| Parameter | 18–29 y | 30–39 y | 40–49 y | 50–59 y | 60–69 y | 70–79 y |
| Participant characteristic | ||||||
| No. of participants | 334 | 236 | 251 | 379 | 358 | 124 |
| Race, no. of participants | ||||||
| White | 271 | 187 | 211 | 316 | 325 | 105 |
| Black | 19 | 22 | 16 | 30 | 23 | 11 |
| Asian | 37 | 24 | 21 | 31 | 10 | 7 |
| Other | 7 | 3 | 3 | 2 | 0 | 1 |
| Age, y | 24.0 (3.1) | 35.0 (3.0) | 45.5 (2.9) | 55.5 (3.0) | 64.4 (2.8) | 74.0 (2.8) |
| Height, m | 1.65 (0.06) | 1.65 (0.06) | 1.64 (0.06) | 1.64 (0.06) | 1.63 (0.06) | 1.60 (0.06) |
| Weight, kg | 69.2 (17.4) | 73.4 (18.8) | 75.4 (20.1) | 74.2 (18.2) | 73.2 (16.6) | 69.8 (14.9) |
| BMI, kg/m2 | 25.4 (5.9) | 27.0 (6.9) | 28.1 (7.3) | 27.7 (6.6) | 27.7 (6.3) | 27.4 (6.1) |
| PROMIS PF CAT, t score | 58.0 (7.4) | 56.1 (7.5) | 54.3 (8.0) | 52.7 (7.4) | 51.2 (6.8) | 49.2 (6.4) |
| ASM/height2, kg/m2 | 7.27 (1.38) | 7.36 (1.50) | 7.33 (1.54) | 7.04 (1.37) | 6.84 (1.17) | 6.72 (1.17) |
| Muscle strength test performance | ||||||
| Hand grip strength, kg | ||||||
| Handle position, 1/2/3,b no. of participants | 4/329/1 | 5/230/1 | 9/242/0 | 6/372/1 | 9/349/0 | 3/121/0 |
| Mean (SD) | 27.7 (6.8) | 28.2 (6.2) | 26.6 (7.0) | 25.2 (5.6) | 24.4 (5.1) | 21.6 (4.6) |
| Median (IQR) | 27.4 (23.0–31.8) |
28.4 (24.6–32.2) |
26.6 (22.0–31.2) |
25.0 (21.5–28.6) |
24.2 (21.1–27.4) |
21.4 (18.4–24.4) |
| 5×-STS, s | ||||||
| Mean (SD) | 8.5 (2.0) | 8.9 (2.1) | 9.2 (2.4) | 10.1 (2.7) | 9.5 (2.2) | 10.6 (2.7) |
| Median (IQR) | 8.3 (6.9–9.7) |
8.4 (7.0–9.9) |
9.0 (7.3–10.7) |
9.7 (7.4–10.1) |
9.3 (8.0–11.4) |
10.3 (8.3–12.3) |
| 30s-STS, no. of stands | ||||||
| Mean (SD) | 17.5 (4.1) | 16.5 (3.9) | 16.3 (4.3) | 15.9 (4.2) | 14.6 (3.8) | 14.0 (3.5) |
| Median (IQR) | 17 (14–20) | 16 (13–19) | 16 (13–19) | 15 (12–18) | 14 (11–17) | 13 (11–16) |
a 30s-STS = 30-s sit-to-stand test; 5×-STS = 5-times sit-to-stand test; ASM = appendicular skeletal muscle mass; BMI = body mass index; IQR = interquartile range; PROMIS PF CAT = physical function domain of the National Institutes of Health Patient-Reported Outcomes Measurement Information System computerized adaptive test.
b Dynamometer handle position during testing: smallest (1) to middle (3); no participant chose larger handle position 4 or 5.
Table 2.
Participant Characteristics and Muscle Strength Test Performance Stratified by Decade of Age for Mena
| Age Group | ||||||
|---|---|---|---|---|---|---|
| Parameter | 18–29 y | 30–39 y | 40–49 y | 50–59 y | 60–69 y | 70–79 y |
| Participant characteristic | ||||||
| No. of participants | 198 | 102 | 52 | 91 | 112 | 64 |
| Race, no. of participants | ||||||
| White | 153 | 85 | 44 | 71 | 96 | 57 |
| Black | 11 | 7 | 2 | 9 | 5 | 2 |
| Asian | 29 | 7 | 5 | 10 | 11 | 5 |
| Other | 5 | 3 | 1 | 1 | 0 | 0 |
| Age, y | 24.4 (3.2) | 34.8 (3.1) | 44.8 (2.6) | 55.0 (3.1) | 64.8 (2.6) | 73.4 (2.5) |
| Height, m | 1.77 (0.07) | 1.77 (0.07) | 1.76 (0.08) | 1.76 (0.08) | 1.76 (0.07) | 1.73 (0.06) |
| Weight, kg | 81.2 (14.5) | 84.3 (16.1) | 89.2 (16.5) | 90.9 (20.9) | 86.2 (15.8) | 85.2 (14.9) |
| BMI, kg/m2 | 25.7 (4.1) | 27.0 (4.7) | 28.8 (5.6) | 29.2 (6.0) | 27.8 (4.3) | 28.3 (4.7) |
| PROMIS PF CAT, T score | 59.9 (7.6) | 58.6 (9.0) | 56.4 (8.6) | 53.1 (8.3) | 53.2 (7.5) | 48.2 (5.8) |
| ASM/height2, kg/m2 | 9.01 (1.38) | 8.78 (1.36) | 9.05 (1.46) | 8.88 (1.66) | 8.51 (1.21) | 8.32 (1.18) |
| Muscle strength test performance | ||||||
| Hand grip strength, kg | ||||||
| Handle position, 1/2/3,b no. of participants | 3/183/12 | 2/95/5 | 0/49/3 | 0/86/5 | 0/99/13 | 0/62/2 |
| Mean (SD) | 45.0 (10.9) | 47.6 (12.0) | 47.9 (11.2) | 42.8 (9.5) | 39.1 (8.6) | 34.8 (9.6) |
| Median (IQR) | 45.5 (38.6–52.5) |
46.2 (37.7–54.8) |
48.7 (41.8–55.6) |
43.2 (38.1–48.3) |
38.3 (32.2–44.2) |
34.1 (27.2–41.0) |
| 5×-STS, s | ||||||
| Mean (SD) | 8.3 (2.0) | 8.0 (2.1) | 8.8 (2.0) | 9.3 (2.4) | 9.7 (3.0) | 11.2 (3.5) |
| Median (IQR) | 8.3 (7.1–9.5) |
7.7 (6.4–9.1) |
8.8 (7.5–10.1) |
9.0 (7.3–10.7) |
9.1 (7.6–10.6) |
10.5 (8.2–12.8) |
| 30s-STS, no. of stands | ||||||
| Mean (SD) | 18.1 (4.4) | 18.7 (4.7) | 16.7 (3.7) | 16.3 (4.6) | 15.7 (4.3) | 13.9 (4.8) |
| Median (IQR) | 17 (15–19) | 18 (15–21) | 16 (14–18) | 15 (12–18) | 15 (13–17) | 13 (10–16) |
a 30s-STS = 30-s sit-to-stand test; 5×-STS = 5-times sit-to-stand test; ASM = appendicular skeletal muscle mass; BMI = body mass index; IQR = interquartile range; PROMIS PF CAT = physical function domain of the National Institutes of Health Patient-Reported Outcomes Measurement Information System computerized adaptive test.
b Dynamometer handle position during testing: smallest (1) to middle (3); no participant chose larger handle position 4 or 5.
Grip Strength
Based on the centile curves fitted to the grip strength data, median grip strength was modeled to be highest (27.9 kg) in women who were 33.9 years old and lowest (20.2 kg) at the maximum age in the dataset (80.0 years) (Fig. 1A). A performance of 21.3 kg at 33.9 years equated to a z score of −1.0, with median performance at 76.1 years equating to a t score of −1. In men, median grip strength was highest (47.2 kg) in those who were 37.6 years old and lowest (32.5 kg) at the maximum age (79.3 years) (Fig. 1B). A performance of 36.4 kg at 37.6 years equated to a z score of −1, with median performance at 70.0 years equating to a t score of −1. Grip strength was predictive of DXA-identified sarcopenia in both women and men, with AUCs of 0.62 (95% CI = 0.58 to 0.67; P < .001) and 0.72 (95% CI = 0.66 to 0.78; P = .001), respectively.
Figure 1.
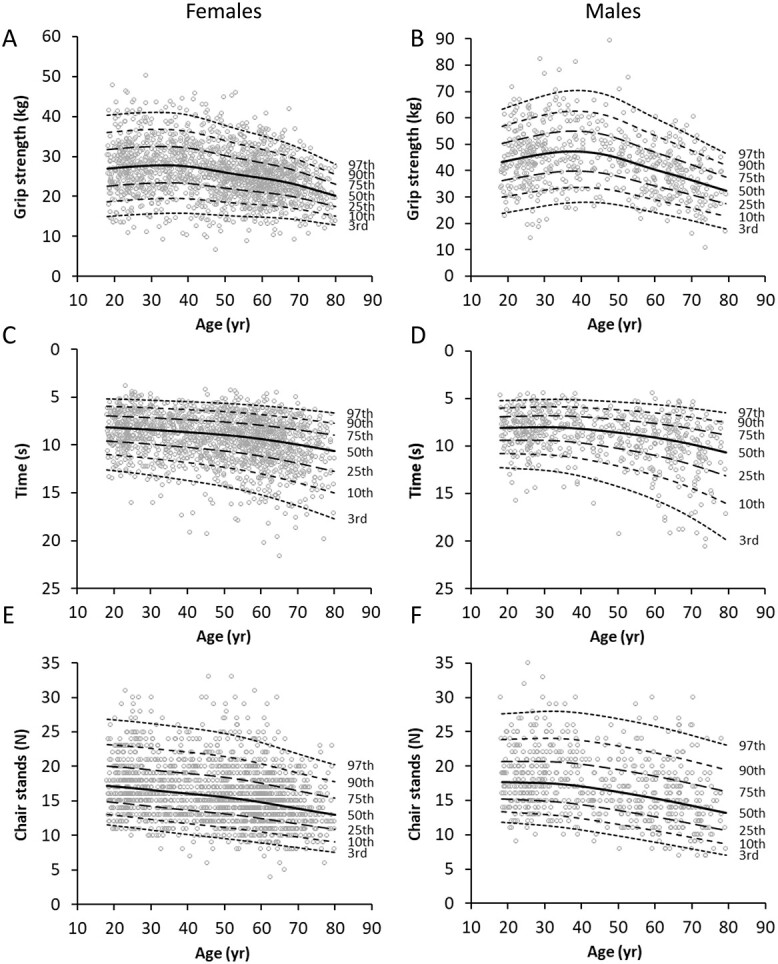
Test performance and centile curves for hand grip strength (A and B), time to complete 5 stands (5×-STS) (C and D), and number of stands completed in 30 seconds (30s-STS) (E and F) in women and men. Centile curves were generated using the lambda-mu-sigma method.
Time to Complete 5×-STS
Women who were 18.0 years old had the fastest median 5×-STS performance (8.16 seconds) based on the fitted centile curves (Fig. 1C). The slowest median performance (10.66 seconds) occurred at the maximum age (80.0 years). A performance of 10.32 seconds at 18.0 years equated to a z score of −1.0, with median performance at 75.2 years equating to a t score of −1. Men who were 29.9 years old had the fastest median 5×-STS performance (8.02 seconds), and men at the maximum age (79.3 years) had the slowest median 5×-STS performance (10.65 seconds) (Fig. 1D). A performance of 10.17 seconds at 29.9 years equated to a z score of −1.0, with median performance at 74.1 years coinciding with a t score of −1. 5×-STS was unable to predict DXA-identified sarcopenia in either women (AUC = 0.51 [95% CI = 0.46 to 0.56], P = .64) or men (AUC = 0.52 [95% CI = 0.43 to 0.60], P = .68).
Number of Stands Completed in 30 Seconds (30s-STS)
The highest (17.2 repetitions) and lowest (13.0 repetitions) median 30s-STS performance results were modeled in women at the youngest (18.0 years) and oldest (80.0 years) ages, respectively (Fig. 1E). A performance of 13.8 repetitions at 18.0 years equated to a z score of −1.0, with median performance at 70.7 years equating to a t score of −1. Men at the youngest age (18.0 years) were modeled to have the highest median 30s-STS performance (17.7 repetitions), and men at the maximum age (79.3 years) were modeled to have the lowest median 30s-STS performance (13.0 repetitions) (Fig. 1F). A performance of 14.2 at 18.0 years equated to a z score of −1.0, with median performance at 70.3 years coinciding with a t score of −1. 30s-STS was unable to predict DXA-identified sarcopenia in either women (AUC = 0.50 [95% CI = 0.45 to 0.55], P = .96) or men (AUC = 0.51 [95% CI = 0.43 to 0.60], P = .77).
Percentile, z Score, and T Score Calculator and Centile Curve Plotter
A downloadable Excel-based calculator (Fig. 2) for computing age- and sex-specific percentiles, z scores, and t scores for an individual’s performance and for plotting performance on centile curves is provided in Supplementary Appendix 2.
Figure 2.

Screenshots of the downloadable Excel (Microsoft Corp, Redmond, WA, USA)-based calculator available in Supplementary Appendix 2. Following test performance and data entry (A), subject-specific percentiles, z scores, and t scores are automatically computed for each outcome, and centile curves are plotted (B). *The authors retain copyright of the Grip Strength and Sit-to-Stand Test Performance Calculator.
Predictors of Muscle Strength Test Performance
Predictors of muscle strength test performance are shown in Table 3. In women, the included predictors explained 31.5%, 30.5%, and 30.5% of the variance in grip strength, 5×-STS performance, and 30s-STS performance, respectively. In men, 38.4%, 24.7%, and 24.7% of the variance in grip strength, 5×-STS, and 30s-STS performance were explained by the predictors, respectively. Performance on all tests was worse with increasing age and better with increasing self-reported physical functioning (PROMIS PF CAT) and performance on the alternate muscle strength test (eg, grip strength or STS test). ASM/height2 improved performance on all tests, except for STS tests in men. Greater height had variable effects across tests, increasing grip strength and decreasing 5×-STS performance in both sexes and decreasing 30s-STS performance in women. Greater weight reduced 5×-STS and 30s-STS performance in women and 30-STS performance in men. There was no influence of race on grip strength; however, women and men identifying as Black had poorer performance on both 5×-STS and 30s-STS than did those identifying as White.
Table 3.
Predictors of Hand Grip Strength and Sit-to-Stand Test Performancea
| Women | Men | |||||||
|---|---|---|---|---|---|---|---|---|
| Muscle Strength Test and Candidate Predictor | Estimate | SE | P | R 2 | Estimate | SE | P | R 2 |
| Hand grip strength, kg | 0.315 | 0.384 | ||||||
| Age, y | −0.028 | 0.009 | .002 | −0.064 | 0.023 | .005 | ||
| Race | ||||||||
| Height, m | 0.362 | 0.022 | <.001 | 0.430 | 0.052 | <.001 | ||
| Weight, kg | ||||||||
| BMI, kg/m2 | ||||||||
| PROMIS PF CAT | 0.097 | 0.020 | <.001 | 0.166 | 0.049 | .001 | ||
| ASM/height2, kg/m2 | 1.110 | 0.098 | <.001 | 2.787 | 0.270 | <.001 | ||
| 5×-STS, sb | ||||||||
| 30s-STS, no. of standsb | 0.369 | 0.036 | <.001 | 0.457 | 0.088 | <.001 | ||
| Constant | −51.052 | 3.866 | <.001 | −71.224 | 9.648 | <.001 | ||
| 5×-STS , s | 0.305 | 0.247 | ||||||
| Age, y | 0.014 | 0.004 | <.001 | 0.023 | 0.006 | <.001 | ||
| Race | <.001 | .001 | ||||||
| Asian vs White | 0.296 | 0.202 | .144 | −0.182 | 0.308 | .554 | ||
| Black vs White | 1.102 | 0.209 | <.001 | 1.606 | 0.392 | <.001 | ||
| Other vs White | −0.418 | 0.497 | .400 | 0.548 | 0.730 | .453 | ||
| Height, m | 0.059 | 0.010 | <.001 | 0.047 | 0.014 | .001 | ||
| Weight, kg | 0.038 | 0.005 | <.001 | |||||
| BMI, kg/m2 | ||||||||
| PROMIS PF CAT | −0.081 | 0.008 | <.001 | −0.084 | 0.012 | <.001 | ||
| ASM/height2, kg/m2 | −0.203 | 0.064 | .002 | |||||
| Hand grip strength, kg | −0.092 | 0.010 | <.001 | −0.051 | 0.009 | <.001 | ||
| Constant | 4.281 | 1.620 | .008 | 6.425 | 2.441 | .009 | ||
| 30s-STS, no. of stands | 0.305 | 0.247 | ||||||
| Age, y | −0.026 | 0.006 | <.001 | −0.029 | 0.010 | .005 | ||
| Race | <.001 | .005 | ||||||
| Asian vs White | −0.131 | 0.343 | .703 | 0.390 | 0.558 | .485 | ||
| Black vs White | −1.828 | 0.352 | <.001 | −2.440 | 0.708 | .001 | ||
| Other vs White | 1.535 | 0.842 | .069 | −0.792 | 1.318 | .548 | ||
| Height, m | −0.120 | 0.016 | .001 | |||||
| Weight, kg | −0.071 | 0.009 | <.001 | −0.111 | 0.025 | <.001 | ||
| BMI, kg/m2 | 0.232 | 0.083 | .006 | |||||
| PROMIS PF CAT | 0.136 | 0.014 | <.001 | 0.124 | 0.023 | <.001 | ||
| ASM/height2, kg/m2 | 0.457 | 0.108 | <.001 | |||||
| Hand grip strength, kg | 0.163 | 0.016 | <.001 | 0.113 | 0.017 | <.001 | ||
| Constant | 27.394 | 2.738 | <.001 | 9.676 | 1.983 | <.001 | ||
a Determined using stepwise linear regression with age forced to stay in the model. 30s-STS = 30-s sit-to-stand test; 5×-STS = 5-times sit-to-stand test; ASM = appendicular skeletal muscle mass; BMI = body mass index; IQR = interquartile range; PROMIS PF CAT = physical function domain of the National Institutes of Health Patient-Reported Outcomes Measurement Information System computerized adaptive test.
b Either the 5×-STS or the 30s-STS was included, depending on which yielded the highest R2 value in the stepwise regression.
Discussion
The present study provides age- and sex-specific normative data for grip strength and the 5×-STS and 30s-STS tests across adulthood (age = 18–80 years) in a Midwest US population acquired using standardized scripts and procedures. From the centile curves fit to the data using the LMS method, an Excel-based calculator was developed and is available for download (Suppl. Appendix 2). The calculator computes patient-specific percentiles, z scores, and t scores for each outcome and plots test performance on the centile curves (Fig. 2). z scores and their associated percentiles can be used to identify individuals underperforming compared with their age- and sex-matched peers, which is relevant to therapists using clinical muscle strength tests to assess general musculoskeletal function and performance in disease and injury states. t scores comparing performance with that of young adults who are healthy may aid in identifying those with possible sarcopenia, such as how t scores are used to identify osteoporosis based on DXA outcomes. However, there is currently no operational definition of sarcopenia based on t scores, although EWGSOP2 recommendations typically have used cutoffs at −2 SDs compared with mean reference values.2
Centile curves for grip strength are widely available because the test is most recommended for clinically identifying probable sarcopenia.2–7 Grip strength was collected in the present study to assess the comparability of our sample. Our grip strength centile curves follow the same pattern as those of Dodds et al,12 who pooled data from 60,803 observations in 12 British studies. They reported women and men reached their peak median grip strength at ages of 26 to 42 years and 29 to 39 years, respectively. These ranges correspond to those in the present study, in which women and men reached peak median grip strengths at 33.9 years and 37.6 years, respectively. Both the study of Dodds et al12 and the present study demonstrated the expected decline in grip strength with advancing age, with the lowest point on the median centile curves occurring at the oldest age in the respective databases. Accordingly, advancing age was a predictor of lower grip strength performance in the present study.
Although our centile curves followed the same pattern as those of Dodds et al,12 they were shifted downward 5% to 10%. The reason(s) for the systematically lower grip strength in our cohort is unknown. Procedural and testing equipment differences may contribute.9 Also, there is evidence of geographical differences in muscle strength.14 However, the median centile curves in both sexes in the present study overlap those recently reported by Landi et al,31 who assessed grip strength in 11,488 Italians. Likewise, grip strength stratified by decade of age in women in the present study are nearly identical to those recently reported in Australian women.37 Most notably, our grip strength outcomes stratified by decade of age in both women and men closely approximate the outcomes reported as part of the US population–based National Institutes of Health Toolbox standardization study.38 The latter suggests that the female and male cohorts we tested are representative of the US population.
The EWGSOP2 recommendations used the data of Dodd et al12 and a conservative t score of −2.5 to define cutoff points of <16 and <27 kg for low grip strength and probable sarcopenia in women and men, respectively.2 Cutoff values have greater clinical utility than t scores because they are in the unit of measure, but there is unlikely a single diagnostic value for identifying sarcopenia. In the present study, there were 84 women (5%) and 37 men (6%) with grip strength outcomes below the EWGSOP2 cutoff points. Only 12 of the women and 7 of the men had DXA-confirmed sarcopenia, as defined by EWGSOP2 cutoff points for ASM/height2 of <5.5 and <7 kg/m2, respectively.2 However, ASM/height2 did contribute to the prediction of grip strength, and grip strength did have some ability to predict DXA-identified sarcopenia, as evidenced by AUCs in the acceptable (0.61–0.70) and excellent (0.71–0.80) ranges in women and men, respectively.
Compared with centile curves for grip strength, centile curves for 5×-STS and 30s-STS performance are not widely available. Suetta et al32 recently published centile curves for 30s-STS performance using data from the Copenhagen Sarcopenia Study. However, the transferability of the data remains unclear, because they reported peak test performances of 27.2 and 27.3 repetitions in women and men, respectively. These values represent 9 or 10 (>50%) more repetitions than those seen in the cohort in the present study and correspond to 1 STS repetition nearly every second.
A real difference in muscle strength may explain the better 30s-STS performance reported by Suetta et al,32 with their cohort also having greater grip strength (4–8 kg, 10%–25%) than reported here and in other recent studies.12,14,31,37,38 However, real differences in muscle strength would be expected to be coupled with muscle quantity measures trending in the same direction. This was not the case, with DXA-derived ASM/height2 in the present study being systematically higher in both sexes than that reported by Suetta et al.32
Differences in test administration are a likely contributor to the differing test performances between the present study and that of Suetta et al.32 Data collection in the latter study followed practice trials (ie, familiarization) and used “strong verbal encouragement,” according to Alcazar et al.39 Both approaches enhance performance,40,41 but multiple practice trials are not typically used clinically because of time constraints, and it is difficult to standardize the timing, content, volume, and tone of verbal encouragement. To promote the clinical utility of our data, we used the widely implemented STS and grip strength testing protocols of the Short Physical Performance Battery17 and the Southampton Grip-Strength Measurement Protocol,9 respectively. The exact protocols and scripts that we used are provided in Supplementary Appendix 1.
Landi et al31 recently published centile curves for 5×-STS performance. They reported peak performances of 6.0 seconds in both sexes—times that were 2.16 seconds (26%) and 2.02 seconds (25%) faster than those of women and men in the present study, respectively. The better test performance existed across age strata, suggesting a systematic difference in 5×-STS performance between cohorts. One possible explanation for the slower test performance in the present study is our synchronous performance of the 5×-STS and 30s-STS tests in a single test. This was undertaken for testing efficacy. Participants may have performed their 5×-STS test repetitions slower to preempt fatigue associated with completing the 30s-STS test. However, this possibility is not considered a major contributor, with times recorded in the present study that were similar to those in other studies.24,26 It is possible that 5×-STS test administration differed between studies; however, the exact script and test procedure performed by Landi et al31 were not provided, negating cross-study comparisons.
STS performance was not a predictor of DXA-identified sarcopenia in either sex (as assessed by AUCs), despite ASM/height2 being a predictor of 5×-STS and 30s-STS performance in women. Also, individuals with and individuals without DXA-identified sarcopenia did not differ on 5×-STS or 30s-STS performance for either women or men (assessed via 1-way analysis of variance with age as a covariate; data not shown). These observations suggest that STS tests may not be useful in identifying sarcopenia. However, the PROMIS PF CAT was an excellent predictor of 5×-STS–identified probable sarcopenia—the latter determined by an EWGSOP2-recommended 5×-STS time of >15 seconds (AUC for women = 0.85 [95% CI = 0.79 to .91], P < .001; AUC for men = 0.83 [95% CI = 0.73 to 0.94], P < .001). Interestingly, the PROMIS PF CAT was a poor predictor of DXA-identified sarcopenia (AUC for women = 0.60 [95% CI = 0.50 to 0.70], P = .03; AUC for men = 0.61 [95% CI = 0.48 to 0.74], P = .11). Thus, 5×-STS is a useful indicator of self-reported PF and may identify probable sarcopenia independent of DXA assessment of muscle quantity. Others have shown that physical performance tests can provide better estimates of mobility impairment and mortality risk than measures of muscle quantity.42,43
Finally, the present study explored predictors of muscle strength test performance. A number have already been discussed, including age, ASM height2, and PROMIS PF CAT. An additional predictor for grip strength in both women and men was greater height, confirming previous reports.44 In contrast, increasing height and weight had negative impacts on STS performance. Additionally, STS performance was also affected by race, with Whites having better performances than Blacks. Visser et al45 previously reported Blacks had lower performance on the 5×-STS despite having greater muscle mass. A possible reason was greater muscle fat infiltration. Our data lend support to this hypothesis, with Blacks having significantly greater weight and whole-body percent body fat despite having greater ALM/height2 than Whites (assessed via 1-way analysis of variance with age as a covariate; data not shown).
Limitations
Our study has several strengths, including the use of a standardized test protocol and script, creation of a normative performance calculator, and generation of normative data across adulthood for the 2 most common versions of the STS test. Despite our study strengths, there are limitations, including the use of cross-sectional data to generate normative curves, which may not represent an individual’s trajectory over time; the inclusion of a relatively small number of male participants; the lack of normative data provided for adults over 80 years of age, who are anticipated to have the poorest test performances; not studying individuals under 18 years of age; synchronous performance of the 5×-STS and 30s-STS tests; and the lack of assessment of the appropriateness of our sample size and sample composition, as recently recommended by Cole.46
Conclusion
The present study provides age- and sex-specific normative data for grip strength and the 5×-STS and 30s-STS tests across adulthood in a Midwest US population. Predictors for test performance, including participant age, race, height, weight, DXA-acquired appendicular lean mass, and self-reported PF, were identified. Using the acquired data, a practical Excel-based calculator was generated. The calculator enables ready computation of patient-specific percentiles, z scores, and t scores for each outcome and plots performance on centile curves. Use of the calculator will enable clinicians and researchers to express outcomes in an individual or population of interest relative to expected values.
Supplementary Material
Contributor Information
Stuart J Warden, Department of Physical Therapy, School of Health and Human Sciences, Indiana University, Indianapolis, Indiana, USA; Indiana Center for Musculoskeletal Health, School of Medicine, Indiana University, Indianapolis, Indiana, USA; La Trobe Sport and Exercise Medicine Research Centre, La Trobe University, Bundoora, Victoria, Australia.
Ziyue Liu, Indiana Center for Musculoskeletal Health, School of Medicine, Indiana University, Indianapolis, Indiana, USA; Department of Biostatistics, School of Medicine, Indiana University, Indianapolis, Indiana, USA.
Sharon M Moe, Indiana Center for Musculoskeletal Health, School of Medicine, Indiana University, Indianapolis, Indiana, USA; Division of Nephrology, Department of Medicine, School of Medicine, Indiana University, Indianapolis, Indiana, USA.
Author Contributions
Concept/idea/research design: S.J. Warden, Z. Liu, S.M. Moe
Writing: S.J. Warden, Z. Liu, S.M. Moe
Data collection: S.J. Warden, S.M. Moe
Data analysis: S.J. Warden, Z. Liu
Project management: S.J. Warden, S.M. Moe
Fund procurement: S.J. Warden
Providing participants: S.J. Warden, S.M. Moe
Providing facilities/equipment: S.J. Warden
Consultation (including review of manuscript before submitting): S.M. Moe
Funding
This study was supported by grants from the National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIH/NIAMS P30 AR072581 and AR077273) and the Indiana Clinical Translational Science Award/Institute (NCATS UL1TR002529–01).
Ethics Approval
This study was approved by the Indiana University Institutional Review Board.
Disclosures
The authors completed the ICMJE Form for Disclosure of Potential Conflicts of Interest and reported no conflicts of interest.
The authors retain copyright of the Grip Strength and Sit-to-Stand Test Performance Calculator in Supplementary Appendix 2.
References
- 1. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393:2636–2646. [DOI] [PubMed] [Google Scholar]
- 2. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48:16–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Beaudart C, Rolland Y, Cruz-Jentoft AJ, et al. Assessment of muscle function and physical performance in daily clinical practice: a position paper endorsed by the European Society for Clinical and Economic Aspects of osteoporosis, osteoarthritis and musculoskeletal diseases (ESCEO). Calcif Tissue Int. 2019;105:1–14. [DOI] [PubMed] [Google Scholar]
- 4. Bauer J, Morley JE, Schols AMWJ, et al. Sarcopenia: a time for action. An SCWD position paper. J Cachexia Sarcopenia Muscle. 2019;10:956–961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Chen L-K, Woo J, Assantachai P, et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21:300–307.e2. [DOI] [PubMed] [Google Scholar]
- 6. Dent E, Morley JE, Cruz-Jentoft AJ, et al. International clinical practice guidelines for sarcopenia (ICFSR): screening, diagnosis, and management. J Nutr Health Aging. 2018;22:1148–1161. [DOI] [PubMed] [Google Scholar]
- 7. Studenski SA, Peters KW, Alley DE, et al. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J Gerontol. 2014;69:547–558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Bohannon RW. Muscle strength: clinical and prognostic value of hand-grip dynamometry. Curr Opin Clin Nutr Metab Care. 2015;18:465–470. [DOI] [PubMed] [Google Scholar]
- 9. Roberts HC, Denison HJ, Martin HJ, et al. A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age Ageing. 2011;40:423–429. [DOI] [PubMed] [Google Scholar]
- 10. Rantanen T, Guralnik JM, Foley D, et al. Midlife hand grip strength as a predictor of old age disability. JAMA. 1999;281:558–560. [DOI] [PubMed] [Google Scholar]
- 11. Leong DP, Teo KK, Rangarajan S, et al. Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet. 2015;386:266–273. [DOI] [PubMed] [Google Scholar]
- 12. Dodds RM, Syddall HE, Cooper R, et al. Grip strength across the life course: normative data from twelve British studies. PLoS One. 2014;9:e113637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Dodds RM, Syddall HE, Cooper R, Kuh D, Cooper C, Sayer AA. Global variation in grip strength: a systematic review and meta-analysis of normative data. Age Ageing. 2016;45:209–216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Leong DP, Teo KK, Rangarajan S, et al. Reference ranges of handgrip strength from 125,462 healthy adults in 21 countries: a prospective urban rural epidemiologic (PURE) study. J Cachexia Sarcopenia Muscle. 2016;7:535–546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Yeung SSY, Reijnierse EM, Trappenburg MC, et al. Handgrip strength cannot be assumed a proxy for overall muscle strength. J Am Med Dir Assoc. 2018;19:703–709. [DOI] [PubMed] [Google Scholar]
- 16. Johansson J, Strand BH, Morseth B, Hopstock LA, Grimsgaard S. Differences in sarcopenia prevalence between upper-body and lower-body based EWGSOP2 muscle strength criteria: the Tromsø study 2015–2016. BMC Geriatr. 2020;20:461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49:M85–M94. [DOI] [PubMed] [Google Scholar]
- 18. Jones CJ, Rikli RE, Beam WC. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res Q Exerc Sport. 1999;70:113–119. [DOI] [PubMed] [Google Scholar]
- 19. Cooper R, Kuh D, Hardy R, Mortality Review G, Falcon THAS. Objectively measured physical capability levels and mortality: systematic review and meta-analysis. BMJ. 2010;341:c4467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332:556–562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Aparicio VA, Carbonell-Baeza A, Ruiz JR, et al. Fitness testing as a discriminative tool for the diagnosis and monitoring of fibromyalgia. Scand J Med Sci Sports. 2013;23:415–423. [DOI] [PubMed] [Google Scholar]
- 22. Dobson F, Hinman RS, Roos EM, et al. OARSI recommended performance-based tests to assess physical function in people diagnosed with hip or knee osteoarthritis. Osteoarthr Cartil. 2013;21:1042–1052. [DOI] [PubMed] [Google Scholar]
- 23. Klokkerud M, Dagfinrud H, Uhlig T, et al. Developing and testing a consensus-based core set of outcome measures for rehabilitation in musculoskeletal diseases. Scand J Rheumatol. 2018;47:225–234. [DOI] [PubMed] [Google Scholar]
- 24. Bohannon RW. Reference values for the five-repetition sit-to-stand test: a descriptive meta-analysis of data from elders. Percept Mot Skills. 2006;103:215–222. [DOI] [PubMed] [Google Scholar]
- 25. Rikli RE, Jones CJ. Functional fitness normative scores for community-residing older adults, ages 60–94. J Aging Phys Act. 1999;7:162–181. [Google Scholar]
- 26. Bergland A, Strand BH. Norwegian reference values for the Short Physical Performance Battery (SPPB): the Tromsø study. BMC Geriatr. 2019;19:216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Bohannon RW, Shove ME, Barreca SR, Masters LM, Sigouin CS. Five-repetition sit-to-stand test performance by community-dwelling adults: a preliminary investigation of times, determinants, and relationship with self-reported physical performance. Isokinet Exerc Sci. 2007;15:77–81. [Google Scholar]
- 28. McKay MJ, Baldwin JN, Ferreira P, Simic M, Vanicek N, Burns J. Reference values for developing responsive functional outcome measures across the lifespan. Neurology. 2017;88:1512–1519. [DOI] [PubMed] [Google Scholar]
- 29. Tveter AT, Dagfinrud H, Moseng T, Holm I. Health-related physical fitness measures: reference values and reference equations for use in clinical practice. Arch Phys Med Rehabil. 2014;95:1366–1373. [DOI] [PubMed] [Google Scholar]
- 30. Ben-Shlomo Y, Kuh D. A life course approach to chronic disease epidemiology: conceptual models, empirical challenges, and interdisciplinary perspectives. Int J Epidemiol. 2002;31:285–293. [PubMed] [Google Scholar]
- 31. Landi F, Calvani R, Martone AM, et al. Normative values of muscle strength across ages in a ‘real world’ population: results from the longevity check-up 7+ project. J Cachexia Sarcopenia Muscle. 2020;11:1562–1569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Suetta C, Haddock B, Alcazar J, et al. The Copenhagen Sarcopenia Study: lean mass, strength, power, and physical function in a Danish cohort aged 20–93 years. J Cachexia Sarcopenia Muscle. 2019;10:1316–1329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med. 1992;11:1305–1319. [DOI] [PubMed] [Google Scholar]
- 34. Rigby RA, Stasinopoulos DM. Generalized additive models for location, scale and shape. J R Stat Soc: Ser C: Appl Stat. 2005;54:507–554. [Google Scholar]
- 35. Centers for Disease Control and Prevention . Modified z-scores in the CDC growth charts. Accessed June 20, 2021. https://www.cdc.gov/nccdphp/dnpa/growthcharts/resources/biv-cutoffs.pdf.
- 36. Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression. 3rd ed. Hoboken, NJ, USA: John Wiley & Sons, Inc; 2013. [Google Scholar]
- 37. Sui SX, Holloway-Kew KL, Hyde NK, et al. Handgrip strength and muscle quality in Australian women: cross-sectional data from the Geelong osteoporosis study. J Cachexia Sarcopenia Muscle. 2020;11:690–697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Wang YC, Bohannon RW, Li X, Sindhu B, Kapellusch J. Hand-grip strength: normative reference values and equations for individuals 18 to 85 years of age residing in the United States. J Orthop Sports Phys Ther. 2018;48:685–693. [DOI] [PubMed] [Google Scholar]
- 39. Alcazar J, Kamper RS, Aagaard P, et al. Relation between leg extension power and 30-s sit-to-stand muscle power in older adults: validation and translation to functional performance. Sci Rep. 2020;10:16337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Jung M-C, Hallbeck MS. The effects of instruction, verbal encouragement, and visual feedback on static handgrip strength. Proceedings of the Human Factors and Ergonomics Society Annual Meeting. 1999;43:703–707. [Google Scholar]
- 41. Schaubert K, Bohannon RW. Reliability of the sit-to-stand test over dispersed test sessions. Isokinet Exerc Sci. 2005;13:119–122. [Google Scholar]
- 42. McLean RR, Shardell MD, Alley DE, et al. Criteria for clinically relevant weakness and low lean mass and their longitudinal association with incident mobility impairment and mortality: the Foundation for the National Institutes of Health (FNIH) Sarcopenia Project. J Gerontol A Biol Sci Med Sci. 2014;69:576–583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Newman AB, Kupelian V, Visser M, et al. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J Gerontol. 2006;61:72–77. [DOI] [PubMed] [Google Scholar]
- 44. Ahmad I, Alam MM, Haque N, Khan AA, Farooq M. Relationship between grip strength and anthropometric variations—a systematic review. In: Muzammil M, Khan AA, Hasan F, eds. Ergonomics for Improved Productivity. Singapore: Springer Singapore; 2021: 409–415. [Google Scholar]
- 45. Visser M, Kritchevsky SB, Goodpaster BH, et al. Leg muscle mass and composition in relation to lower extremity performance in men and women aged 70 to 79: the health, aging and body composition study. J Am Geriatr Soc. 2002;50:897–904. [DOI] [PubMed] [Google Scholar]
- 46. Cole TJ. Sample size and sample composition for constructing growth reference centiles. Stat Methods Med Res. 2021;30:488–507. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.