

Abstract
Objectives:
Rumination is a transdiagnostic risk factor for depression and anxiety, which surge during the adolescent years. Mindfulness training – with its emphasis on metacognitive awareness and present-moment attention – may be effective at reducing rumination. Mindfulness apps offer a convenient, engaging, and cost-effective means for accessing mindfulness training for teens. Despite their increasing popularity among adolescents, no study to date has investigated which teens are well-suited to app-based mindfulness training.
Methods:
Eighty adolescents (M age = 14.01 years, 45% girls) with elevated rumination were enrolled in a 3-week trial of app-based mindfulness training. Repeated daily ecological momentary assessment (EMA) surveys assessed problem-focused and emotion-focused rumination immediately prior to and following each mindfulness exercise. Elastic net regularization (ENR) models tested baseline predictors of “immediate” (post-mindfulness exercise) and “cumulative” (post-3-week intervention) benefit from app-based mindfulness training.
Results:
Ninety percent (72/80) of adolescents completed the 3-week trial, and the mean number of mindfulness exercises completed was 28.7. Baseline adolescent characteristics accounted for 14%–25% of the variance in outcomes (i.e., reduction in problem-focused or emotion-focused rumination). Higher baseline rumination, and lower emotional suppression, predicted better immediate and cumulative outcomes. In contrast, female gender and older age predicted better immediate, but not cumulative, outcomes. Differences in results across outcome timeframes (immediate vs. cumulative) are discussed.
Conclusions:
Findings from this study highlight the potential of data-driven approaches to inform which adolescent characteristics may predict benefit from engaging with an app-based mindfulness training program. Additional research is needed to test these predictive models against a comparison (non-mindfulness) condition.
Keywords: mindfulness, smartphone app, rumination, adolescents, prediction
The adolescent years are a time of profound change, often accompanied by significant stress and emotional turmoil. Symptoms of anxiety and, in particular, depression increase substantially during the adolescent years (Avenevoli et al., 2015; Merikangas et al., 2010). Epidemiological studies indicate that by the end of adolescence approximately 15% of youth have experienced at least one major depressive episode, whereas 32% have developed an anxiety disorder (Avenevoli et al., 2015; Merikangas et al., 2010). Moreover, there is recent evidence that rates of emotional disorders and overall psychological distress among adolescents have increased over the past decade (Twenge et al., 2019).
A growing body of research indicates that rumination (i.e., repetitive and negative self-focused thinking) is a transdiagnostic risk factor involved in the development of depression and anxiety (for reviews see Aldao et al., 2010; Nolen-Hoeksema et al., 2008; Nolen-Hoeksema & Watkins, 2011; Watkins & Roberts, 2020). For example, rumination prospectively predicts the onset of both depressive symptoms (Rood et al., 2009) and depression diagnoses (Abela & Hankin, 2011; Gibb et al., 2012) in youth. Similarly, studies have found that rumination concurrently and prospectively predicts anxiety symptoms in adolescents (e.g., McLaughlin & Nolen-Hoeksema, 2011; Muris et al., 2004). In addition, prior work suggests that rumination not only increases during adolescence (Baiocco et al., 2017; Hampel & Petermann, 2005; Jose & Brown, 2008; Shaw et al., 2019), but exhibits a stronger association with depression in adolescents relative to children (Rood et al., 2009). Gender differences also emerge during adolescence, with girls reporting higher levels of rumination than boys (Hilt et al., 2010; Jose & Brown, 2008; Shaw et al., 2019), which may in part account for similar gender differences in depression which emerge during the same developmental period. Moreover, developmental research indicates that cognitive “response styles” (including rumination) become more stable during the adolescent years (Abela et al., 2004; Shaw et al., 2019). As others have argued (Shaw et al., 2019), rumination may develop into a more consolidated and stable mental habit during the adolescent years as it is repeatedly rehearsed and becomes “well-practiced,” which may help account for its strengthening association with depression in adolescents relative to children (Rood et al., 2009). Given the growing body of research supporting the role of rumination in the development and maintenance of depression and anxiety symptoms during adolescence, it represents an important target for prevention and treatment.
Mindfulness training, with its emphasis on metacognitive awareness and present-moment attention, may be effective at reducing rumination. Mindfulness meditation encourages the cultivation of attentional control and focused attention on the present moment without judgement (Kabat-Zinn, 1994, 2013). In contrast, rumination typically involves a perseverative and passive focus on negative or stressful past events (Shaw et al., 2019; Watkins & Nolen-Hoeksema, 2014). Mindfulness training may alleviate rumination through its focus on the present and emphasis on metacognitive awareness of mental events (i.e., the ability to notice and observe thoughts and feelings as they occur), rather than becoming immersed in them as one does while ruminating (Segal et al., 2012). Indeed, multiple studies indicate that reductions in rumination mediate the therapeutic effects of mindfulness interventions on depressive symptoms, anxiety and distress (Deyo et al., 2009; Gu et al., 2015; Jain et al., 2007; van der Velden et al., 2015). Although promising, these studies focused on adults. Furthermore, it is unclear whether intensive, in-person meditation training (e.g., 8 weeks of mindfulness-based stress reduction (Kabat-Zinn, 2013) or mindfulness-based cognitive therapy (MBCT; Segal et al., 2012)) is required to reduce rumination. Indeed, initial studies indicate that even brief mindfulness interventions significantly reduce rumination. In two studies, one with college students (Villa & Hilt, 2014) and one with younger adolescents (Hilt & Pollak, 2012), an 8-minute guided mindfulness exercise was shown to reduce rumination. These studies highlight the benefit of even brief mindfulness interventions for adolescents.
Mindfulness apps offer a highly scalable, convenient, cost-effective and (potentially) engaging means for teens to access brief mindfulness training via their smartphones. Rates of smartphone ownership among adolescents have soared in recent years. In 2015, 67% of 13–18-year olds owned a smartphone. As of 2019, that number had risen to 84% (Rideout & Robb, 2019). In a recent survey, 11% of adolescents reported using a mindfulness app; however, the number was higher (18%) among those experiencing moderate to severe levels of depressive symptoms (Rideout & Fox, 2018). There are over 260 mindfulness apps available (Mani et al., 2015), and millions of monthly users (Wasil et al., 2020). Despite their increasing popularity among adolescents, no study to date has investigated which teens are well-suited to app-based mindfulness training.
The current study investigated whether adolescent clinical and demographic characteristics can inform which teens are expected to benefit from a mindfulness app. Mindfulness apps typically consist of brief (e.g., 1–10 minute), guided mindfulness exercises, offered daily via “courses” which last for several weeks or longer (e.g., the highly popular Headspace app offers 10-day to 30-day mindfulness courses). Thus, one could examine outcomes across two timeframes: (1) “immediate” reductions in rumination from engaging in a brief (e.g., 1–10 minute) mindfulness exercise (i.e., pre- to post-mindfulness exercise change in rumination) and (2) “cumulative” effects of a multi-week mindfulness app course (i.e., longer-term effects of engaging in daily mindfulness exercises over several weeks). Accordingly, within the context of a 3-week mindfulness app trial, we tested baseline predictors of both “immediate” and “cumulative” outcomes of app-based mindfulness training for adolescents with elevated rumination. We predicted that adolescents with relatively higher levels of rumination would exhibit better outcomes to app-based mindfulness training.
Method
Participants
Participants were 80 early adolescents ages 12–15 (M age = 14.01 years, SD = .99) recruited in 2018–2019 from a moderately sized Midwestern community. Sample size was determined via power analysis for the primary aims focused on testing pre- to post-intervention change in rumination (see Hilt & Swords, 2021; Swords, Breitenstein, Doane, & Hilt, 2021), with pilot data indicating a large effect (Cohen’s d = .88). The present manuscript represents secondary analyses focused on predictions of mindfulness app outcome based on pre-treatment adolescent characteristics. With an alpha = .05 and power = 0.80, the included sample size could detect a medium (r = .31) correlation between individual predictors and outcome. In addition to age (12–15), inclusion criteria required at least moderate trait rumination, which was assessed via phone screen. Participants were eligible if their average score, based on two questions from the rumination subscale of the Children’s Response Styles Questionnaire (Abela et al., 2002; When you feel sad or stressed, do you think about a recent situation, wishing it had gone better? When you feel sad or stressed, do you think “why can’t I handle things better?”), indicating that they ruminate “sometimes,” “often,” or “always.” The sum of these two items is highly correlated with the full rumination subscale from the CRSQ (current sample: r = .82, p < .001) and is associated with depressive symptoms and non-suicidal self-injury (NSSI) in previous work (Hilt et al., 2008). Based on pilot data, an estimated 42% of adolescents were expected to endorse moderate to high levels of rumination based on these two items. Fourteen potential participants were excluded based on this criterion. For a summary of demographic information and baseline measures of psychopathology see Table 1.
Table 1.
Demographic and Clinical Characteristics for the Sample (N = 80).
| N | % | Mean | SD | ||
|---|---|---|---|---|---|
| Gender | |||||
| Boys | 43 | 53.8% | |||
| Girls | 36 | 45.0% | |||
| Chose not to answer | 1 | 1.2% | |||
| Race | |||||
| White | 69 | 86.25% | |||
| Chose not to answer | 7 | 8.75 % | |||
| Native American | 2 | 2.5% | |||
| Black | 1 | 1.25% | |||
| Multi-racial | 1 | 1.25% | |||
| Ethnicity | |||||
| Non-Hispanic | 75 | 93.75% | |||
| Hispanic | 3 | 3.75% | |||
| Chose not to answer | 2 | 2.5% | |||
| Clinical Characteristics | |||||
| ERQ Suppression | 15.15 | 4.23 | |||
| ERQ Reappraisal | 26.29 | 7.59 | |||
| CRSQ Rumination | 13.79 | 7.97 | |||
| CRSQ Distraction | 8.34 | 3.30 | |||
| CRSQ Problem Solving | 5.45 | 2.78 | |||
| FFMQ Observe | 22.51 | 6.80 | |||
| FFMQ Describe | 24.25 | 5.91 | |||
| FFMQ Awareness | 25.79 | 5.91 | |||
| FFMQ Nonjudgement | 29.91 | 6.16 | |||
| FFMQ Nonreactivity | 18.96 | 5.14 | |||
| CDI Total | 9.40 | 7.32 | |||
| MASC Total | 46.55 | 15.48 | |||
| History of NSSI | 10 | 12.5% | |||
| History of Suicidal Ideation | 11 | 13.75% | |||
| Prior mindfulness exposure | 26 | 32.9% |
Procedure
Participants were recruited by word-of-mouth and through letters sent to parents of sixth through ninth grade students enrolled in the local public-school district. During the initial lab visit, adolescents and their guardians provided assent and informed consent, and completed baseline questionnaires. Adolescents then downloaded the CARE app onto their device, or one that they had borrowed from the lab, and were taught to use the app. When adolescents first use the app, they are prompted to enter their wake and sleep times. Based on these inputted times, the app prompts adolescents to use the app three times a day within that time window (i.e., morning, late afternoon, and just before bedtime) through randomized notifications. If adolescents were busy when they received the notification, they were asked to use the app as soon as they were available after a notification. App use was incentivized with a $5 weekly bonus, which adolescents could earn by using the app 21 times or more during each week of the active 3-week intervention period. To help adolescents keep track of their app use, guardians were notified mid-week with an email update. Additionally, guardians were emailed at the end of the week to let adolescents know how many times they used the app and whether they had earned the weekly bonus.
Each time adolescents used the app, they were prompted with an ecological momentary assessment (EMA) survey including items to assess state rumination (i.e., focus on emotions and problems) and state mood (i.e., sadness and anxiety) on a 0 (Not at all) to 100 (Extremely) scale (see Measures below). Mindfulness exercises were randomly assigned 67% of the time, or 85% of the time when negative mood ratings (i.e., sad or anxious) were 90–100 (i.e., the chance of receiving an exercise was greatest when adolescents most needed it). If prompted to complete a guided mindfulness activity, adolescents were first asked to indicate how much time they had available (i.e., about 1, 5 or 10 minutes) and were randomly allocated a mindfulness activity within the available timeframe. One-minute exercises provided written instructions on the screen for focusing on the breath, sounds or physical sensations along with a one-minute timer. All other mindfulness exercises also involved focusing on the breath, sounds or physical sensations, but ranged from 3–12 minutes and were delivered via guided audio instructions. The mindfulness exercises included in the app were selected from free and publicly available mindfulness exercises that represent commonly used practices from mindfulness-based interventions and were appropriate for adolescents based on pilot testing (see Supplement for additional details). Immediately following a mindfulness exercise, participants again completed EMA questions about their current state (including rumination).
Measures
Response styles.
We assessed response styles using the Children’s Response Styles Questionnaire (CRSQ; Abela et al., 2002). In this study, we modified directions to ask participants to report on what they do when they feel sad or stressed, in line with current conceptualizations (Nolen-Hoeksema et al., 2008; Shaw et al., 2019). For each item, participants are asked to indicate how often they respond that way on a 4-point Likert scale (0 = almost never, 1 = sometimes, 2 = often, 3 = almost always). The rumination subscale consists of 13-items that assess a child’s tendency to respond to feelings of distress with rumination. Sample items include: “Why can’t I handle things better” and “Think about a recent situation, wishing it had gone better.” The 7-item distraction subscale assesses engagement in behaviors to avoid feeling distress. Sample items include: “Help someone else with something so you don’t think about your problem” and “Go to your favorite place and get your mind off your feelings.” The 5-item problem-solving subscale assesses solution-focused responses to distress. Sample items include, “Think of a way to make your problem better” and “Ask a friend/parent/teacher to help you solve your problem.” Past research has demonstrated reliability and validity of the CRSQ among adolescents (e.g., Abela et al., 2002). The CRSQ demonstrated excellent reliability for rumination (α = .89), but lower internal consistency for distraction (α = .50) and problem-solving (α = .59).
Trait Mindfulness.
Trait mindfulness was assessed using the Five Facet Mindfulness Questionnaire (FFMQ: Baer et al., 2006). The FFMQ is a 39-item self-report questionnaire that identifies five dimensions of mindfulness. These five facets include: observing (e.g. “I notice the smells and aromas of things.”), describing (e.g.“ I am good at findings words to describe my feelings.”), acting with awareness (e.g. “I find myself doing things without paying attention”), nonjudgement of inner experiences (e.g. “I think some of my emotions are bad or inappropriate and I should not feel them”), and nonreactivity to inner experience (e.g. “I perceive my feelings and emotions without having to react to them”). Items are assessed on a 5-point Likert-scale (1 = never or very rarely true to 5= very often or always true). The reliability for the subscales in the present study were as follows: Observing (α = .82), Describing (α =.79), Awareness (α =.82), Nonjudgment (α =.87) and Nonreactivity (α =.77). The FFMQ has been used in adolescent samples, demonstrating high reliability (see Hambour et al., 2018; Johnstone et al., 2020; Ramler et al., 2016). In addition, parents were also asked (yes/no) whether their child had previous exposure to mindfulness or mindfulness-based concepts.
Emotion Regulation.
We assessed emotion regulation with the Emotion Regulation Questionnaire (ERQ; Gross & John, 2003). The ERQ is a 10-item questionnaire that measures two emotion regulation strategies: suppression (4 items) and reappraisal (6 items). Past research demonstrates that ERQ has high internal consistency, test-retest reliability, and good convergent and discriminant validity (Gross & John, 2003; John & Gross, 2004), including among adolescent samples (Gullone et al., 2010; Hollenstein et al., 2012). In our sample, the reliability for the suppression (α =.66) and reappraisal (α =.89) were adequate.
Depression.
We assessed depression with the Children’s Depression Inventory (CDI; Kovacs, 1992), a 27-item self-report questionnaire that assesses the frequency and severity of depressive symptoms in the last two weeks. Items are scored from 0–2, with higher scores indicating greater clinical severity of depressive symptoms. Past research has demonstrated reliability and validity of the measure among adolescents (Craighead et al.,1995; Klein, et al., 2005). The CDI demonstrated excellent reliability in this study (α = .90).
Anxiety.
We assessed anxiety using the total score from the Multidimensional Anxiety Scale for Children (MASC; March et al. 1997), a 39-item reliable and valid index of anxiety in youth. The MASC assesses for a variety of symptoms including physical (e.g., restlessness), harm avoidance, social (e.g., fear of humiliation and rejection), and separation anxiety. Past research suggests the MASC has good-to-excellent internal reliability (Baldwin & Dadds, 2007) and demonstrates satisfactory-to-excellent test-retest reliability among adolescents (March et al., 1997; March, Sullivan & Parker, 1999). The MASC demonstrated excellent reliability in this study (α=.88).
Self-Injury.
Adolescents completed the Self-Injurious Thoughts and Behaviors Interview Child Self-Report form (SITBI; Nock et al., 2007). In this questionnaire, adolescents are asked whether they have ever engaged in or experienced non-suicidal self-injury, suicidal ideation, suicide plans, and suicide attempts. If so, adolescents are prompted to report the number of occurrences within their lifetime, the past year, and the past week.
EMA State Rumination.
To acquire a more fine-grained and ecologically valid assessment of change in rumination in the daily lives of teens enrolled in the mindfulness app trial, rumination was assessed via repeated daily smartphone-delivered ecological momentary assessment (EMA) surveys. Our assessment distinguished between rumination focused on feelings vs. problems (Moberly & Watkins, 2008). The former aspect of rumination is consistent with Nolen-Hoeksema’s (1991) definition highlighting maladaptive focus on depressive feelings; whereas the latter is based on the aspect of Nolen-Hoeksema’s (1991) definition related to dwelling on the possible causes and consequences of depression, as well as theories linking rumination to perceived problems arising from discrepancies between one’s current reality and goals (Lyubomirsky et al., 1999; Martin & Tesser, 1996). In summary, both the intervention (mindfulness app) and outcome assessments (EMA rumination) were delivered via adolescents’ smartphones.
More specifically, state rumination, the outcome measure, was assessed with two EMA items: focusing on problems and focusing on emotions, adapted from Moberly & Watkins (2008). An example of problem-focused rumination is dwelling on an interpersonal conflict (e.g., “Why do I keep getting into the same arguments?”) and an example of emotion-focused rumination is brooding over depressive feelings (e.g., “Why do I always feel so sad? Why do I keep feeling this way?”). At each EMA timepoint, participants were asked to answer questions based on how they were feeling/thinking “just before” they started answering these questions. The rumination items were, “How much were you focusing on your problems?” and “How much were you focusing on your emotions?” Both items were assessed on a sliding scale from 0 (Not at all) to 100 (Extremely). These items have been used to assess state rumination in other studies with adolescents (e.g., Hilt & Pollak, 2012; Hilt, Sladek, Doane, & Stroud, 2017).
Data Analyses.
The present study investigated baseline (i.e., pre-intervention) predictors of improvement in rumination among adolescents enrolled in a 3-week mindfulness app course. Baseline variables included plausible predictors of change in rumination, including clinical (e.g., severity of depressive and anxiety symptoms) and demographic (e.g., age and gender) characteristics, as well as mindfulness skills/facets (e.g., ability to observe internal experiences, non-judgmental attitude towards internal experience, acting with awareness), response styles (i.e., rumination, distraction and problem-solving) and emotion regulation (reappraisal and suppression) variables. Given the number of predictor variables, and to minimize overfitting (i.e., increase generalizability of the model to new subjects), elastic net regularization (ENR) was implemented for feature selection and to generate predictions of expected outcome (i.e., change in rumination).
Analyses focused on predicting both “immediate” outcomes (i.e., short-term effects of engaging in a 1–12 minute mindfulness exercise) and “cumulative” effects of the 3-week mindfulness app trial (i.e., longer-term effects of engaging in daily mindfulness exercises over the 21-day intervention period) from baseline subject characteristics. Immediate outcomes were computed as the mean change in problem-focused rumination (RumProb) and emotion-focused rumination (RumEmo) during mindfulness exercises (i.e., for each subject, averaging pre- to post-mindfulness exercise rumination change scores). In contrast, cumulative outcomes were computed as the slope of rumination change over the course of the 3-week trial (i.e., derived from subject-specific regressions of rumination scores on intervention day [Day 1- Day 21]). For the latter analyses, we first computed daily means of RumProb and RumEmo representing the mean value of these two variables for each day, for each subject, across the 21-day trial. These means were computed from the RumProb and RumEmo scores assessed immediately prior to (rather than after) each mindfulness exercise, in order not to contaminate analyses focused on cumulative effects of the 3-week intervention with the above tests of the immediate effects of the mindfulness exercises. Baseline predictors in the models included age, gender, response styles (CRSQ subscales: Rumination, Distraction and Problem-Solving), emotion regulation (ERQ subscales: Cognitive Reappraisal and Expressive Suppression), mindfulness skills (FFMQ subscales: Observe, Describe, Awareness, Nonjudgment, Nonreactivity), parent-reported child exposure to mindfulness (yes/no), depression severity (CDI total score), anxiety severity (MASC total score), history of NSSI (yes/no) and history of suicidal ideation (yes/no). Complete data (n = 80) were available for all baseline predictors with the exception of 4 variables, which were each missing one value. These missing values were imputed via the MissForest package in R (Stekhoven & Bühlmann, 2012), which implements a random forest approach to impute missing values for continuous and categorical variables by averaging across regression trees. Outcome variables (RumProb and RumEmo) were not included in the imputation. Prior to analysis, continuous predictors were z-scored (mean = 0 and SD = 1) and categorical variables dummy coded.
To predict immediate outcomes, two ENR models were run: one for predicting change in RumProb and one for RumEmo. Similarly, to predict cumulative outcomes, two ENR models were run: one for predicting the slope of change in RumProb and one for RumEmo. Predictions were generated via 10-fold cross-validation (CV) ENR (glmnet package, Friedman et al., 2010). Tuning of ENR’s alpha and lambda parameters was performed using the CARET package’s resampling grid search (Kuhn, 2008), testing each combination of alpha (from 0 to 1 by 0.05) and lambda (from 0 to 2 by 0.01) (optimal values were selected via minimum cross-validated error criterion). The 10-fold ENR models were each repeated 100 times. Parameter estimates and performance metrics (r-squared and root mean square error [RMSE] values) reported below represent median values across the 100 iterations. Predictor variables that were retained in at least 80% (80/100) of the ENR iterations are reported (see Supplement for additional details on ENR).
Results
Attrition and Adherence
Ninety percent (72/80) of the adolescent participants completed the 3-week trial. The mean number of mindfulness exercises completed over the course of the trials was 28.7 (range 7–47). Adolescents received 1-minute mindfulness exercises most frequently (91% vs. 8% for 5-min and 1% for 10-min mindfulness exercise options). Over half the sample (59%; n=47) received at least one 5-min mindfulness exercise, and 24% received at least one 10-min exercise. Overall outcomes from this trial have been reported elsewhere (see Hilt & Swords, 2021; Swords, Breitenstein, Doane, & Hilt, 2021).
Predicting Immediate vs. Cumulative Benefit of App-based Mindfulness Training
As displayed in Figure 1, there was substantial variability across adolescents in the immediate benefits they derived from the mindfulness exercise with regards to change in RumProb (green distribution; range = −14.5 to 40.0; SD = 11.5) and RumEmo (red distribution; range = −42.6 to 32.3; SD = 15.6). Similarly, as displayed by the distribution of subject-specific slopes in Figure 2 (RumProb) and Figure 3 (RumEmo), there was variability across subjects in cumulative rumination change over the 3-week trial, with some adolescents experiencing reductions in rumination (i.e., negative slope), whereas others experiencing limited or no improvement (or even worsening rumination as reflected by a positive slope)(RumProb: range = −4.3 to 5.3; SD = 1.5; RumEmo: range = −3.5 to 3.0; SD = 1.4). In summary, given the variability between adolescents in immediate and cumulative outcomes, we sought to predict which adolescents are expected to benefit from engaging in app-delivered mindfulness training.
Figure 1.
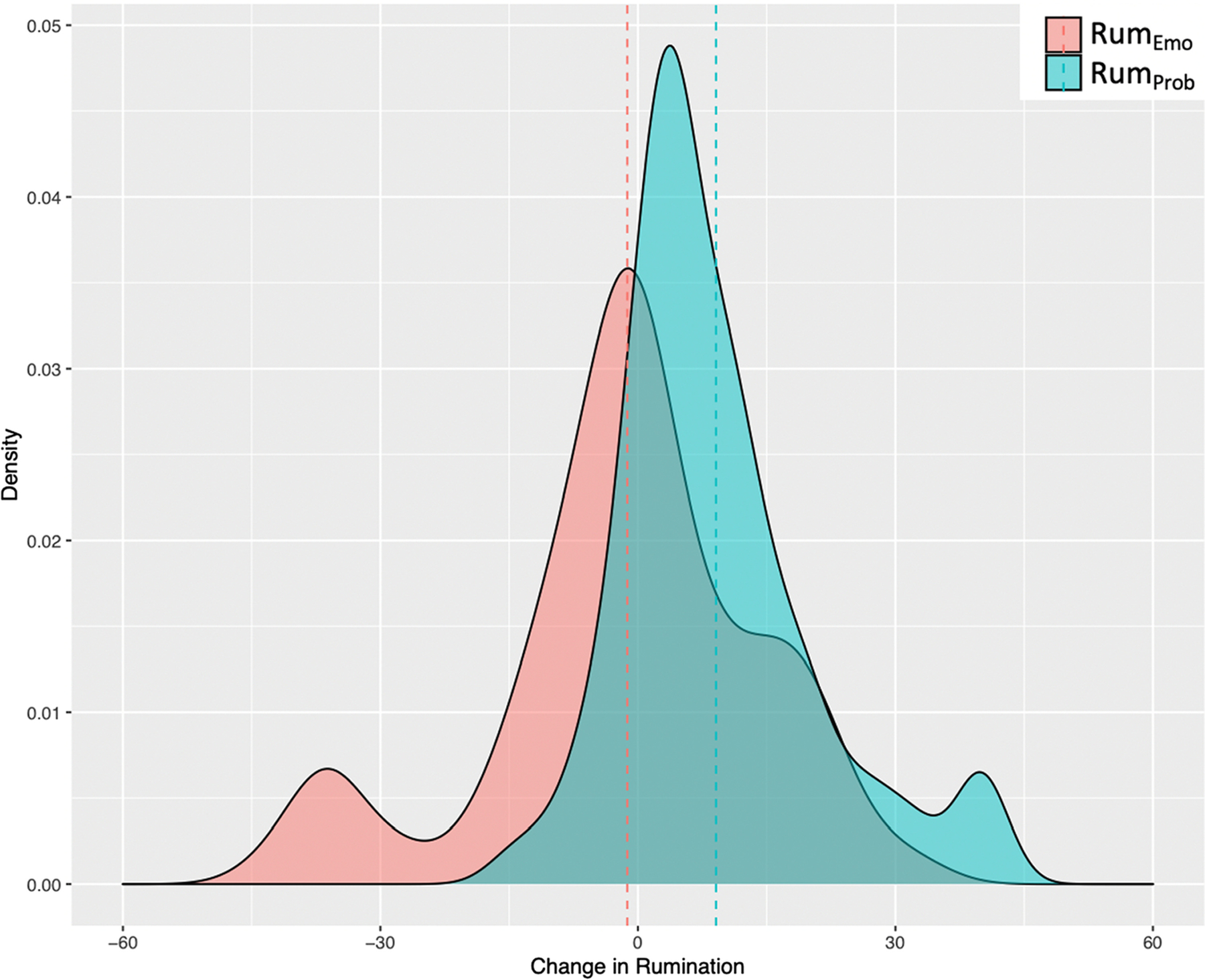
Distribution of “immediate” change in problem-focused rumination (green) and emotion-focused rumination (red) from engaging in brief (1–12 mins) mindfulness exercises across subjects. In this figure, positive values reflect greater reductions. Dotted lines represent means.
Figure 2.
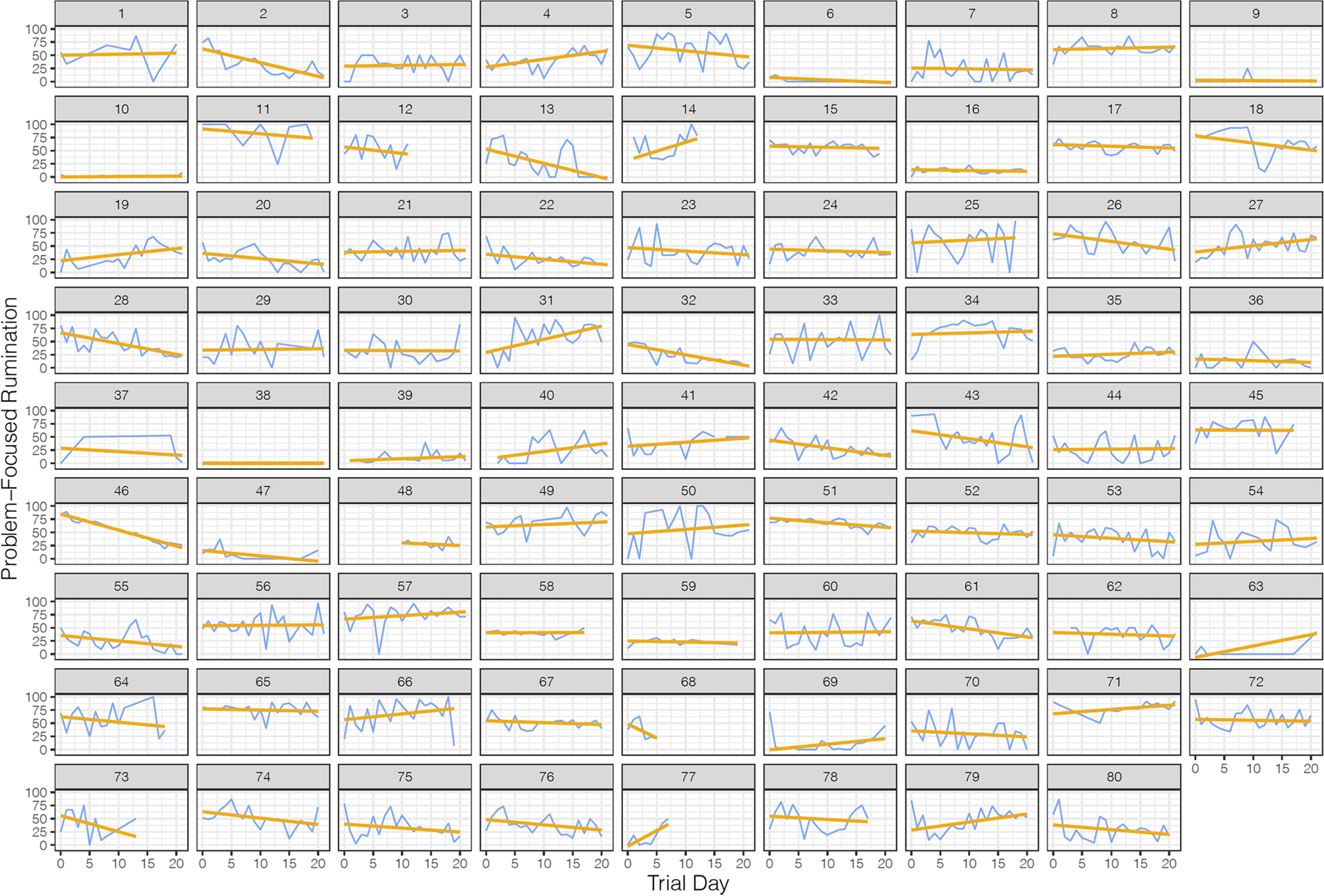
Subject-specific plots of “cumulative” change (blue lines) in problem-focused rumination (RumProb) over the course of the 21-day trial. Gold lines represent regression slopes.
Figure 3.
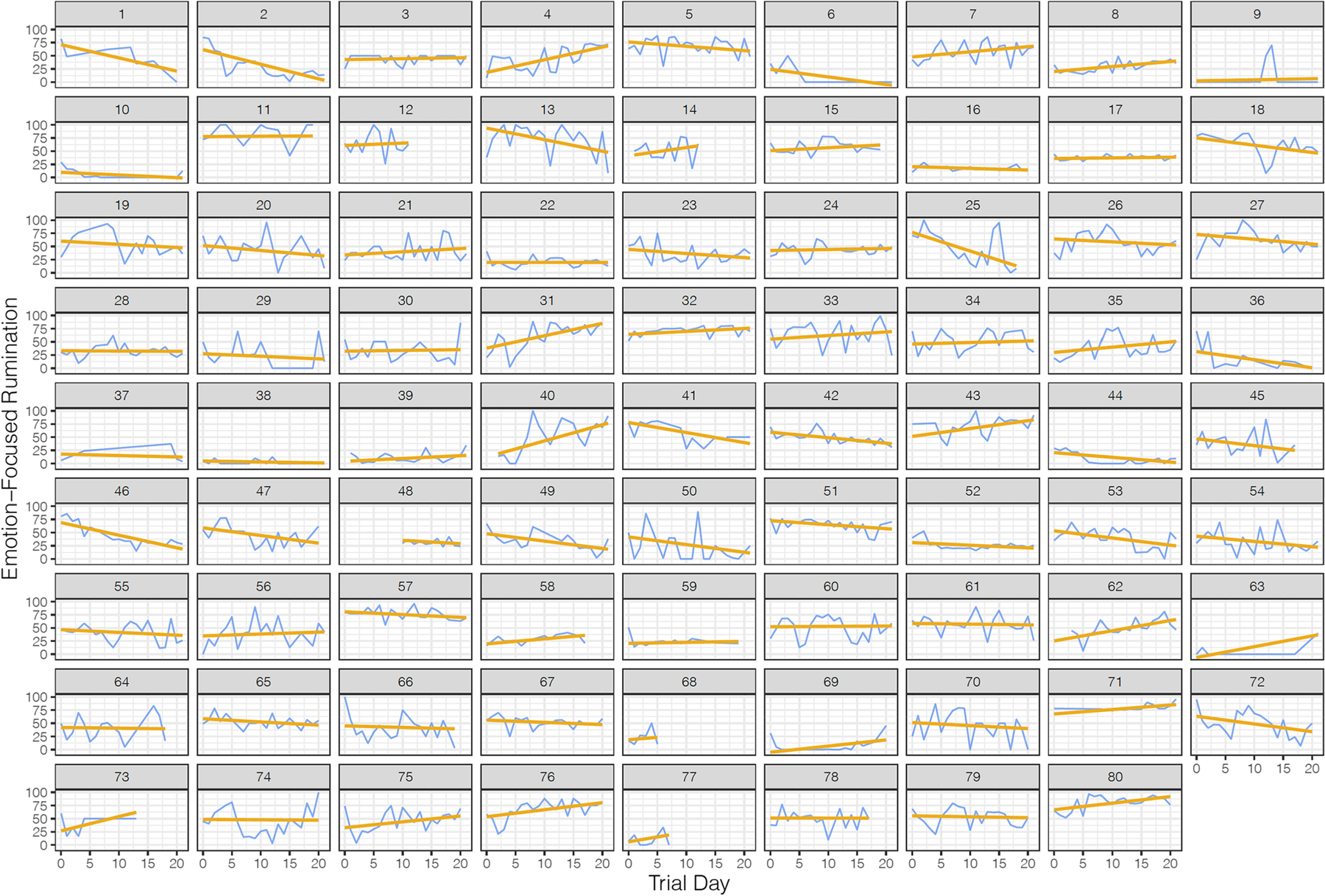
Subject-specific plots of “cumulative” change (blue lines) in emotion-focused rumination (RumEmo) over the course of the 21-day trial. Gold lines represent regression slopes.
ENR models, informed by a combination of baseline adolescent characteristics, accounted for 14%–25% of the variance (R2) in rumination outcomes (see Table 2 for RMSE values). As noted above, the 10-fold CV ENR models were repeated 100 times. The standard deviation (SD) in RMSE and R2 values across iterations was small (e.g., for the slope of change in emotion-focused rumination: RMSE (SD) = .02, R2 (SD) = .04; for problem-focused rumination slope: RMSE (SD) = .02, R2 (SD) = .04). Baseline predictors retained in each ENR model are reported in Table 2. Notably, gender was a predictor of the immediate – but not cumulative – effect of app-based mindfulness training. Specifically, girls experienced greater short-term reductions in both RumProb and RumEmo from engaging in a brief mindfulness exercise, but did not significantly differ from boys in their outcomes over the 3-week trial. Second, a greater tendency towards emotional suppression (ERQ) predicted worse outcome across all measures, with the exception of RumProb (immediate effects). Higher levels of baseline rumination predicted both greater immediate and cumulative reductions in RumEmo. No consistent pattern of prediction emerged for baseline mindfulness skills or clinical measures of depression, anxiety or suicidality. Interestingly, prior exposure to mindfulness was not associated with mindfulness app outcome (see Supplement for secondary analyses).
Table 2.
Results of Elastic Net Regularization Models
|
Immediate Effects of
Mindfulness Exercises |
Cumulative (3-week)
Intervention Effects |
|||
|---|---|---|---|---|
| Predictors | RumProb | RumEmo | RumProb | RumEmo |
| Age | 0.31 | |||
| Gender | 1.29 | 1.50 | ||
| ERQ Suppression | −3.77 | −0.42 | −0.09 | |
| ERQ Reappraisal | −0.92 | 0.19 | ||
| CRSQ Rumination | 2.49 | 0.15 | ||
| CRSQ Distraction | 2.56 | −0.12 | −0.38 | |
| CRSQ Problem Solving | 0.12 | 0.17 | ||
| FFMQ Observe | 1.66 | |||
| FFMQ Describe | −0.20 | |||
| FFMQ Awareness | 0.68 | |||
| FFMQ Nonjudgement | −0.28 | |||
| FFMQ Nonreactivity | −0.80 | 0.22 | ||
| CDI Total | ||||
| MASC Total | 0.05 | |||
| History of NSSI | ||||
| History of Suicidal Ideation | ||||
| Prior mindfulness exposure | ||||
| R-Squared (RMSE) | .14 (10.9) | .22 (14.4) | .25 (1.3) | .17 (1.3) |
Notes. RumProb = Problem-focused rumination; RumEmo = Emotion-focused rumination; ERQ = Emotion Regulation Questionnaire; CRSQ = Children’s Response Styles Questionnaire; FFMQ = Five Facet Mindfulness Questionnaire; CDI = Children’s Depression Inventory; MASC = Multidimensional Anxiety Scale for Children. Positive parameter estimates indicate that higher scores on the predictor variable are associated with better outcome (i.e., reduction in rumination).
Discussion
Smartphone ownership among adolescents has soared over the past decade, and teens are increasingly turning to mental health apps – including mindfulness apps – as a means of reducing stress and negative emotions, often triggered by rumination (Aldao et al., 2010; Nolen-Hoeksema et al., 2008; Nolen-Hoeksema & Watkins, 2011; Rideout & Fox, 2018; Rideout & Robb, 2019; Watkins & Roberts, 2020). Given their emphasis on the development of metacognitive awareness and present-moment attention, app-based mindfulness training programs may be effective at reducing rumination in teens. The purpose of the present study was to test whether baseline participant characteristics could inform which adolescents are likely to benefit from app-based mindfulness training.
There are several notable strengths to the present study. First, mindfulness training was delivered via a smartphone app, which represents a highly scalable, engaging, and convenient means for teens to access mindfulness training (e.g., relative to in-person meditation classes). In addition, the adaptive nature of our mindfulness app (i.e., users had an increased likelihood of receiving a guided mindfulness exercise when reporting higher sadness and/or anxiety ratings) resulted in teens receiving mindfulness exercises when they were more likely to be ruminating and in greater need for improvement in mood. Second, to acquire a more fine-grained and ecologically valid assessment of changes in negative cognitions over the course of the trial, rumination was assessed via repeated daily smartphone-delivered EMA. Third, we distinguished between “immediate” effects of mindfulness exercises vs. longer-term “cumulative” effects of daily practice over 3 weeks. Some adolescent characteristics may predict immediate or short-term benefits, but may not be predictive of longer-term benefit over time (and vice versa). Indeed, gender and age emerged as predictors of immediate – but not cumulative – outcomes. Specifically, girls and older adolescents were more likely to experience immediate – but not longer-term – reductions in rumination from engaging in brief (1–12 minute) mindfulness exercises (gender also predicted engagement with the app; see Supplement). Fourth, we distinguished between rumination focused on personal problems versus emotion-focused rumination, which yielded different findings (see Table 2). Finally, we used a modeling approach (ENR) well-suited to handling a relatively large number of predictor variables and optimized to minimize overfitting (i.e., to increase the generalizability of the predictive model to new adolescents).
Results revealed that predictive models, informed by a combination of baseline adolescent characteristics, accounted for 14%–25% of the variance in rumination outcomes. Notably, higher levels of emotional suppression predicted less improvement in rumination across three out of four outcome measures (Table 2). The ERQ suppression subscale assesses the habitual tendency to inhibit the external expression (e.g., facial expression) of one’s internal emotional state. Adolescents with a habitual tendency to suppress their emotional states may be less likely to benefit from a short-term mindfulness intervention focused on the open and non-judgmental acceptance of internal states (including aversive emotional states). It is important to note that this study only examined brief (1–12 minute) mindfulness exercises over a 3-week period. It may be that more sustained, intensive meditation practice would yield a different pattern of findings. For example, consistent with a “compensatory” model, individuals high in suppression may in fact be particularly well-suited to longer-term or more intensive mindfulness training given that they may learn and gradually internalize a more adaptive, open and receptive relationship with emotional states through the acquisition of mindfulness skills (Tang & Braver, 2020). However, the present findings suggest that adolescents with higher levels of emotional suppression are relatively ill-suited to (at least) brief, app-based mindfulness training.
In contrast, higher levels of baseline rumination (CRSQ) were associated with greater immediate and cumulative reductions in emotion-focused rumination. These findings emerged within a model which simultaneously included associated covariates, including depressive and anxiety symptoms, both which did not emerge as predictors of outcome. The purpose of this trial was specifically to recruit adolescents with elevated rumination, a maladaptive cognitive state defined by repetitive and negative thinking often focused on the past. Given its core focus on the cultivation of present moment attention and metacognitive awareness, mindfulness training may be particularly beneficial for adolescents who struggle to disengage from rumination. It is unclear why findings were specific to emotion-focused rumination. In contrast, no consistent patterns of prediction emerged for baseline levels of mindfulness skills or symptom (e.g., depression and anxiety) severity. More specifically, whether you have low or high levels of mindfulness skills, or depressive or anxiety symptoms, does not seem to be predictive of your likelihood of benefiting from app-based mindfulness training (at least with regards to reduction in rumination).
Limitations and Future Research
Several limitations should be noted. First, the present study lacked a comparison intervention or control group. Specifically, this study identified baseline adolescent characteristics predictive of change in rumination in a single intervention (i.e., app-based mindfulness training). It is not clear whether identified predictors are specific to app-based mindfulness training or instead represent intervention non-specific predictors of outcome. For example, do higher levels of rumination predict better outcome to app-based mindfulness training relative to an alternative (non-mindfulness) intervention? In other words, are the baseline predictors “prescriptive” (i.e., intervention specific) or merely “prognostic” (intervention non-specific) predictors of outcome (Cohen & DeRubeis, 2018; Webb et al., 2018)? Future research testing predictive models while including a comparison condition (e.g., a mood monitoring app) is needed (e.g., Webb et al., 2021). Second, sample size was small for these prediction models. Findings require replication in a larger sample of adolescents (e.g., several hundred participants), as well as including a richer set of baseline adolescent characteristics that may be predictive of response to app-based mindfulness training. For example, the study relied primarily on self-report measures as baseline predictors. Behavioral tasks assessing constructs relevant to meditation (e.g., pre-intervention attentional control skills (Wong et al., 2018; MacLean et al., 2010), for self-report version (Derryberry & Reed, 2002)) could be helpful in informing which adolescents could benefit from a course of app-delivered mindfulness training. In addition, adolescents completed the shortest (1-minute) mindfulness exercises most frequently (91%), which may have influenced results (e.g., limited the benefits they could have derived from app-based mindfulness training). Relatedly, it is unclear to what extent differences in the format of the mindfulness exercises (written text for 1-minute exercises vs. audio-guided for the 3–12-minute exercises) may have influenced results. Furthermore, in contrast to the CRSQ rumination subscale, the distraction and problem-solving subscales had low reliability, which may have influenced prediction results. Finally, we distinguished between problem-focused versus emotion-focused rumination. However, some teens who benefit from mindfulness training may report an increased (adaptive) focus on emotions as a result of engaging in mindfulness exercises. In other words, for at least some adolescent participants, increasing scores on the emotion-focused rumination measure may in fact be adaptive (or inert) rather than reflect maladaptive rumination. These limitations notwithstanding, if these findings are replicated, a predictive model could ultimately inform personalized predictions of benefit from app-based mindfulness training that could be used to objectively communicate expected outcome to users prior to engaging with a mindfulness app (e.g., via a freely-available, web-based prognosis calculator).
Supplementary Material
Funding:
This project was supported by a grant from the American Psychological Foundation to LMH. The first author (CAW) was partially supported by R01 MH116969, the Tommy Fuss Fund and a NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation. The opinions and assertions contained in this article should not be construed as reflecting the views of the sponsors.
Footnotes
Compliance with Ethical Standards
This study was approved by Lawrence University IRB and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Conflict of Interest: The authors declare that they have no conflict of interest.
Informed consent
Informed consent (or assent for participating adolescents) was obtained from all individual participants included in the study.
Data Availability Statement
Data are available upon request from Dr. Hilt and with a Data Use Agreement (DUA).
References
- Abela JR, Vanderbilt E, & Rochon A (2004). A test of the integration of the response styles and social support theories of depression in third and seventh grade children. Journal of Social and Clinical Psychology, 23(5), 653–674. [Google Scholar]
- Abela JRZ, Brozina K, & Haigh EP (2002). An examination of the response styles theory of depression in third- and seventh-grade children: A short-term longitudinal study. Journal of Abnormal Child Psychology, 30(5), 515–527. 10.1023/A:1019873015594 [DOI] [PubMed] [Google Scholar]
- Abela JRZ, & Hankin BL (2011). Rumination as a vulnerability factor to depression during the transition from early to middle adolescence: A multiwave longitudinal study. Journal of Abnormal Psychology, 120(2), 259–271. 10.1037/a0022796 [DOI] [PubMed] [Google Scholar]
- Aldao A, Nolen-Hoeksema S, & Schweizer S (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30(2), 217–237. 10.1016/j.cpr.2009.11.004 [DOI] [PubMed] [Google Scholar]
- Avenevoli S, Swendsen J, He J-P, Burstein M, & Merikangas KR (2015). Major depression in the national comorbidity survey–adolescent supplement: Prevalence, correlates, and treatment. Journal of the American Academy of Child & Adolescent Psychiatry, 54(1), 37–44.e2. 10.1016/j.jaac.2014.10.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baer RA, Smith GT, Hopkins J, Krietemeyer J, & Toney L (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13(1), 27–45. 10.1177/1073191105283504 [DOI] [PubMed] [Google Scholar]
- Baiocco R, Manzi D, Lonigro A, Petrocchi N, Laghi F, Ioverno S, & Ottaviani C (2017). A kid-friendly tool to assess rumination in children and early adolescents: Relationships with mother psychopathology and family functioning. Journal of Child and Family Studies, 26(10), 2703–2715. [Google Scholar]
- Cohen ZD, & DeRubeis RJ (2018). Treatment selection in depression. Annual Review of Clinical Psychology, 14(1), 209–236. 10.1146/annurev-clinpsy-050817-084746 [DOI] [PubMed] [Google Scholar]
- Derryberry D, & Reed MA (2002). Anxiety-related attentional biases and their regulation by attentional control. Journal of Abnormal Psychology, 111(2), 225. [DOI] [PubMed] [Google Scholar]
- Deyo M, Wilson KA, Ong J, & Koopman C (2009). Mindfulness and rumination: Does mindfulness rraining lead to reductions in the ruminative thinking associated with depression? EXPLORE, 5(5), 265–271. 10.1016/j.explore.2009.06.005 [DOI] [PubMed] [Google Scholar]
- Wong F, Massar, S. K,AA, Chee MWL, & Lim J (2018). Towards an objective measure of mindfulness: Replicating and extending the features of the breath-counting task. Mindfulness, 9(5), 1402–1410. 10.1007/s12671-017-0880-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman JH, Hastie T, & Tibshirani R (2010). Regularization paths for generalized linear models via coordinate descent. Journal of Statistical Software, 33(1), 1–22. [PMC free article] [PubMed] [Google Scholar]
- Gibb BE, Grassia M, Stone LB, Uhrlass DJ, & McGeary JE (2012). Brooding Rumination and Risk for Depressive Disorders in Children of Depressed Mothers. Journal of Abnormal Child Psychology, 40(2), 317–326. 10.1007/s10802-011-9554-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gu J, Strauss C, Bond R, & Cavanagh K (2015). How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clinical Psychology Review, 37, 1–12. 10.1016/j.cpr.2015.01.006 [DOI] [PubMed] [Google Scholar]
- Gullone E, Hughes EK, King NJ, & Tonge B (2010). The normative development of emotion regulation strategy use in children and adolescents: A 2‐year follow‐up study. Journal of Child Psychology and Psychiatry, 51(5), 567–574. [DOI] [PubMed] [Google Scholar]
- Hambour VK, Zimmer-Gembeck MJ, Clear S, Rowe S, & Avdagic E (2018). Emotion regulation and mindfulness in adolescents: Conceptual and empirical connection and associations with social anxiety symptoms. Personality and Individual Differences, 134, 7–12. [Google Scholar]
- Hampel P, & Petermann F (2005). Age and gender effects on coping in children and adolescents. Journal of Youth and Adolescence, 34(2), 73–83. 10.1007/s10964-005-3207-9 [DOI] [Google Scholar]
- Hilt LM, McLaughlin KA, & Nolen-Hoeksema S (2010). Examination of the response styles theory in a community sample of young adolescents. Journal of Abnormal Child Psychology, 38(4), 545–556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hilt LM, & Pollak SD (2012). Getting out of rumination: Comparison of three brief interventions in a sample of youth. Journal of Abnormal Child Psychology, 40(7), 1157–1165. 10.1007/s10802-012-9638-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hilt LM, & Swords CM (in press). Acceptability and preliminary effects of a mindfulness mobile application for ruminative adolescents. Behavior Therapy. DOI: 10.1016/j.beth.2021.03.004 [DOI] [PubMed] [Google Scholar]
- Hollenstein T, McNeely A, Eastabrook J, Mackey A, & Flynn J (2012). Sympathetic and parasympathetic responses to social stress across adolescence. Developmental Psychobiology, 54(2), 207–214. [DOI] [PubMed] [Google Scholar]
- Jain S, Shapiro SL, Swanick S, Roesch SC, Mills PJ, Bell I, & Schwartz GER (2007). A randomized controlled trial of mindfulness meditation versus relaxation training: Effects on distress, positive states of mind, rumination, and distraction. Annals of Behavioral Medicine, 33(1), 11–21. 10.1207/s15324796abm3301_2 [DOI] [PubMed] [Google Scholar]
- Johnstone JM, Ribbers A, Jenkins D, Atchley R, Gustafsson H, Nigg JT, Wahbeh H, & Oken B (2020). Classroom-based mindfulness training reduces anxiety in adolescents: Acceptability and effectiveness of a cluster-randomized pilot study. Journal of Restorative Medicine, 10(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jose PE, & Brown I (2008). When does the gender difference in rumination begin? Gender and age differences in the use of rumination by adolescents. Journal of Youth and Adolescence, 37(2), 180–192. [Google Scholar]
- Kabat-Zinn J (1994). Wherever you go, there you are: Mindfulness meditation in everyday life. New York: Hyperion. [Google Scholar]
- Kabat-Zinn J (2013). Full catastrophe living (revised edition): Using the wisdom of your body and mind to face stress, pain, and illness (Revised, Updated edition; ). Bantam. [Google Scholar]
- Kuhn M (2008). Caret package. Journal of Statistical Software, 28(5), 1–26.27774042 [Google Scholar]
- Lyubomirsky S, Tucker KL, Caldwell ND, & Berg K (1999). Why ruminators are poor problem solvers: Clues from the phenomenology of dysphoric rumination. Journal of Personality and Social Psychology, 77(5), 1041. [DOI] [PubMed] [Google Scholar]
- MacLean KA, Ferrer E, Aichele SR, Bridwell DA, Zanesco AP, Jacobs TL, King BG, Rosenberg EL, Sahdra BK, Shaver PR, Wallace BA, Mangun GR, & Saron CD (2010). Intensive meditation training improves perceptual discrimination and sustained attention. Psychological Science, 21(6), 829–839. 10.1177/0956797610371339 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mani M, Kavanagh DJ, Hides L, & Stoyanov SR (2015). Review and evaluation of mindfulness-based iPhone apps. JMIR MHealth and UHealth, 3(3). 10.2196/mhealth.4328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin LL, & Tesser A (1996). Some ruminative thoughts. Advances in Social Cognition, 9, 1–47. [Google Scholar]
- McLaughlin KA, & Nolen-Hoeksema S (2011). Rumination as a transdiagnostic factor in depression and anxiety. Behaviour Research and Therapy, 49(3), 186–193. 10.1016/j.brat.2010.12.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merikangas KR, He J, Burstein M, Swanson SA, Avenevoli S, Cui L, Benjet C, Georgiades K, & Swendsen J (2010). Lifetime prevalence of mental disorders in US adolescents: Results from the national comorbidity study-adolescent supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 49(10), 980–989. 10.1016/j.jaac.2010.05.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moberly NJ, & Watkins ER (2008). Ruminative self-focus and negative affect: An experience sampling study. Journal of Abnormal Psychology, 117(2), 314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muris P, Roelofs J, Meesters C, & Boomsma P (2004). Rumination and worry in nonclinical adolescents. Cognitive Therapy and Research, 28(4), 539–554. 10.1023/B:COTR.0000045563.66060.3e [DOI] [Google Scholar]
- Nolen-Hoeksema S (1991). Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology, 100(4), 569. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, & Watkins ER (2011). A heuristic for developing transdiagnostic models of psychopathology: Explaining multifinality and divergent trajectories. Perspectives on Psychological Science, 6(6), 589–609. 10.1177/1745691611419672 [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Wisco BE, & Lyubomirsky S (2008). Rethinking rumination. Perspectives on Psychological Science, 3(5), 400–424. 10.1111/j.1745-6924.2008.00088.x [DOI] [PubMed] [Google Scholar]
- Ramler TR, Tennison LR, Lynch J, & Murphy P (2016). Mindfulness and the college transition: The efficacy of an adapted mindfulness-based stress reduction intervention in fostering adjustment among first-year students. Mindfulness, 7(1), 179–188. 10.1007/s12671-015-0398-3 [DOI] [Google Scholar]
- Rideout V, & Fox S (2018). Digital health practices among teens and young adults—Hopelab. https://www.hopelab.org/report/a-national-survey-by-hopelab-and-well-being-trust-2018/digital-health-practices/digital-health-practices-among-teens-and-young-adults/
- Rideout V, & Robb MB (2019). The common sense census: Media use by tweens and teens, 2019 | Common Sense Media. https://www.commonsensemedia.org/research/the-common-sense-census-media-use-by-tweens-and-teens-2019
- Rood L, Roelofs J, Bögels SM, Nolen-Hoeksema S, & Schouten E (2009). The influence of emotion-focused rumination and distraction on depressive symptoms in non-clinical youth: A meta-analytic review. Clinical Psychology Review, 29(7), 607–616. 10.1016/j.cpr.2009.07.001 [DOI] [PubMed] [Google Scholar]
- Segal ZV, Williams JMG, & Teasdale JD (2012). Mindfulness-based cognitive therapy for depression, Second Edition (2nd edition). The Guilford Press. [Google Scholar]
- Shaw ZA, Hilt LM, & Starr LR (2019). The developmental origins of ruminative response style: An integrative review. Clinical Psychology Review, 74, 101780. 10.1016/j.cpr.2019.101780 [DOI] [PubMed] [Google Scholar]
- Stekhoven DJ, & Bühlmann P (2012). MissForest—Non-parametric missing value imputation for mixed-type data. Bioinformatics, 28(1), 112–118. 10.1093/bioinformatics/btr597 [DOI] [PubMed] [Google Scholar]
- Swords CM, Breitenstein RS, Doane LD, & Hilt LM (2021). Mechanisms of mindfulness training: Ecological momentary assessment with adolescents. [Manuscript submitted for publication]. Department of Psychology, Lawrence University. [Google Scholar]
- Tang R, & Braver TS (2020). Towards an individual differences perspective in mindfulness training research: Theoretical and empirical considerations. Frontiers in Psychology, 11. 10.3389/fpsyg.2020.00818 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Twenge JM, Cooper AB, Joiner TE, Duffy ME, & Binau SG (2019). Age, period, and cohort trends in mood disorder indicators and suicide-related outcomes in a nationally representative dataset, 2005–2017. Journal of Abnormal Psychology, 128(3), 185–199. 10.1037/abn0000410 [DOI] [PubMed] [Google Scholar]
- van der Velden AM, Kuyken W, Wattar U, Crane C, Pallesen KJ, Dahlgaard J, Fjorback LO, & Piet J (2015). A systematic review of mechanisms of change in mindfulness-based cognitive therapy in the treatment of recurrent major depressive disorder. Clinical Psychology Review, 37, 26–39. 10.1016/j.cpr.2015.02.001 [DOI] [PubMed] [Google Scholar]
- Villa CD, & Hilt LM (2014). Brief instruction in mindfulness and relaxation reduce rumination differently for men and women. International Journal of Cognitive Therapy, 7(4), 320–333. 10.1521/ijct_2014_07_02 [DOI] [Google Scholar]
- Wasil AR, Gillespie S, Shingleton R, Wilks CR, & Weisz JR (2020). Examining the reach of smartphone apps for depression and anxiety. American Journal of Psychiatry, 177(5), 464–465. 10.1176/appi.ajp.2019.19090905 [DOI] [PubMed] [Google Scholar]
- Watkins ER, & Nolen-Hoeksema S (2014). A habit-goal framework of depressive rumination. Journal of Abnormal Psychology, 123(1), 24–34. 10.1037/a0035540 [DOI] [PubMed] [Google Scholar]
- Watkins ER, & Roberts H (2020). Reflecting on rumination: Consequences, causes, mechanisms and treatment of rumination. Behaviour Research and Therapy, 127, 103573. 10.1016/j.brat.2020.103573 [DOI] [PubMed] [Google Scholar]
- Webb CA, Cohen ZD, Beard C, Forgeard M, Peckham AD, & Björgvinsson T (2020). Personalized prognostic prediction of treatment outcome for depressed patients in a naturalistic psychiatric hospital setting: A comparison of machine learning approaches. Journal of Consulting and Clinical Psychology, 88(1), 25–38. 10.1037/ccp0000451 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Webb CA, Swords CM, Lawrence H, & Hilt LM (2021). Which adolescents are well-suited to app-based mindfulness training? A randomized clinical trial and data-driven approach for personalized recommendations. PsyArXiv. 10.31234/osf.io/7gbjd [DOI] [PMC free article] [PubMed] [Google Scholar]
- Webb CA, Trivedi MH, Cohen ZD, Dillon DG, Fournier JC, Goer F, Fava M, McGrath PJ, Weissman M, Parsey R, Adams P, Trombello JM, Cooper C, Deldin P, Oquendo MA, McInnis MG, Huys Q, Bruder G, Kurian BT, … Pizzagalli DA (2018). Personalized prediction of antidepressant v. placebo response: Evidence from the EMBARC study. Psychological Medicine, 1–10. 10.1017/S0033291718001708 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zou H, & Hastie T (2005). Regularization and variable selection via the elastic net. Journal of the Royal Statistical Society: Series B (Statistical Methodology), 67(2), 301–320. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data are available upon request from Dr. Hilt and with a Data Use Agreement (DUA).