

Abstract
The Covid‐19 pandemic disrupted medical education, shifting it towards emergency remote delivery. This cross‐sectional study aimed to assess the impact of the pandemic on preclinical medical education and identify predictors of the virtual learning experience and perceived stress. An anonymous survey was delivered electronically to the students of the authors' medical school that attended either histology or pathology. This survey contained two scales, the virtual learning experience (VLE) and the perceived stress scale‐10 (PSS‐10). A total of 173/255 (68%) responded, showing a positive perception towards the remote delivery of both courses. An exploratory factor analysis was performed on the VLE scale items and four new dimensions were formed: “course quality and learning outcomes”, “student motivation”, virtual against F2F learning”, and “virtual laboratory sessions”. The following significant predictors of enhanced VLE, in at least one dimension, were identified: female gender, pathology course, final examination grade >80%, lower perceived stress levels, studying in home country, and holding of another degree before medical school. In addition, the following predictors were significantly associated with higher levels of student perceived stress: female gender, pathology course, studying away from home, and suboptimal internet connection. Notably, the quality of internet connection was significantly associated with the students' final examination performance. Concerning the best mode for future delivery of both courses, most students proposed a blended, rather than an entirely on‐campus or online approach. In conclusion, despite its problems, a high‐quality remote preclinical medical education was possible in the authors' school and offered tremendous opportunities for future improvement.
Keywords: anatomy and histology, digital technology, microanatomy, online education, pathology, stress, virtual microscopy
INTRODUCTION
The coronavirus disease 2019 (Covid‐19), first identified in Wuhan, China (Zhou et al., 2020), is an unprecedented emergency that has caused health, social, and economic disturbance, making “social distancing”, “home isolation”, and other preventive measures the new norm (Cuschieri & Calleja Agius, 2020; Parker et al., 2020; Torda, 2020). Its impact on medical education has been dramatic. Medical schools around the globe closed their premises overnight, while face‐to‐face delivery was halted and replaced by emergency remote teaching both for preclinical and clinical courses (Cuschieri & Calleja Agius, 2020; Longhurst et al., 2020; Torda, 2020).
This abrupt change posed numerous challenges for medical educators, who had to deal with the students' loss of hands‐on experience (Franchi, 2020; Patra et al., 2021), lack of interaction and engagement, in addition to generating new teaching resources for virtual teaching, since transferring the same material and teaching strategies used for F2F teaching would be unsuitable (Evans et al., 2020). Technical limitations, such us the uneven access to digital technology or unreliable internet connection, could also hamper virtual delivery of the courses (Dhawan, 2020). In addition, the pandemic, with its' associated high level of threat, increased the students' anxiety and stress levels (Reuman et al., 2015; Saraswathi et al., 2020; Taylor et al., 2020b). Factors linked with the worsening mental health included the shift to online class delivery, isolation from peers, financial issues, and others (O'Byrne et al., 2021), while students with preexisting mental disease exhibited higher levels of stress during this period (Guo et al., 2021).
Despite the abovementioned challenges, this new situation gave educators the opportunity to use technology to enhance learning experience (Kirkwood & Price, 2014), develop novel teaching resources (Pather et al., 2020), combine synchronous and asynchronous learning, engage students, and support activities that enhance networking (Rhim & Han, 2020). Strategies applied included the development of real‐life online case scenarios (Rahm et al., 2021), the use of “flipped classroom” (Viveka et al., 2017; El Sadik & Al Abdulmonem, 2021; Qian et al., 2021), and social media (Flynn et al., 2015; Katz & Nandi, 2021), aiming to enhance student motivation and improve learning outcomes. Notably, student mentoring programs were re‐organized to be conducted virtually through online platforms, and even the social media with the help of their senior peers (Kazerooni et al., 2020; Zibold et al., 2021)
In the field of anatomical sciences, although the pandemic caused a decline in the use of cadavers and other hands‐on laboratory modalities (Franchi, 2020; Patra et al., 2021), it multiplied virtual teaching resources and facilitated hybrid (synchronous and asynchronous) activities (Harmon et al., 2021; Harrell et al., 2021). For the laboratory instruction of histology and pathology, medical educators relied on virtual microscopy (VM), which is more convenient and does not hamper academic performance compared to light microscopy (Somera Dos Santos et al., 2021). Notably, several authors have shown that VM enhances student active participation and examination scores (Krippendorf & Lough, 2005; Selvig et al., 2015; Yohannan et al., 2019; Lee et al., 2020). Besides enhancing learning and test performance, a study showed VM, when used together with light microscopy (LM), resulted in more excellent and fewer failing scores in histology and pathology, also less score variability, compared to the LM only group (Lee et al., 2020). However, VM requires high‐speed internet connectivity with enough bandwidth, as microscopic image files have a large size, to allow optimal user experience (Evans et al., 2020), while, on the other hand, students have expressed concerns about lacking the skill to operate the light microscope (Somera Dos Santos et al., 2021). In a survey involving a few Chinese medical schools during the pandemic, histology educators responded that they relied to a great extent on VM, active learning, and online assessments (Cheng et al., 2021). Furthermore, in an Australian medical school, online laboratory sessions coupled with VM resulted in enhanced practical examination scores compared to the previous year, when F2F teaching was applied (Caruso, 2021). Of interest, pathology educators in the United States found the opportunity to establish virtual pathology electives; these had high enrollment rates, and were rated favorably by the students; the latter believed they understand the importance of pathology to modern medical practice and consider a potential future career in pathology to a greater extent that the previous years (Parker et al., 2020; Fu et al., 2021).
Shortly after the pandemic onset, the authors' medical school responded rapidly by re‐structuring its program to be delivered remotely, allowing many of its students to return to their home countries. Virtual teaching was applied to all preclinical medical courses, including histology and pathology. As many faculty members and students were new to online education, the school's IT department supported them by organizing training sessions, maintaining the Blackboard Ultra learning management system (Blackboard Inc., Washington, DC), which hosted the school courses, and answering questions through a troubleshooting line.
As the Covid‐19 pandemic triggered unparalleled changes in medical education, this exploratory study aimed to: (1) Present the student perceptions on preclinical emergency remote teaching, focusing on the histology and pathology courses; (2) Identify predictors of the virtual learning experience; and (3) Identify predictors of perceived stress.
MATERIALS AND METHODS
Medical school curriculum
The six‐year MD program follows a spiral, competency‐based curriculum (Figure 1) that allows horizontal and vertical integration of knowledge (Masters & Gibbs, 2007; Bandaranayake, 2017). A “structure and function” (S&F) approach of each body system is followed through the studies, while student‐centered strategies are applied such as team and problem‐based learning and peer‐teaching (Allchin, 2013; Karamaroudis et al., 2020). The curriculum is composed of three phases. Phase I (Foundations of Medicine; Years 1–2) comprises two stages, “S&F: from Molecules to Cells” and “S&F: Body Systems in Health”, and introduces students the normal human body structure and function, also with skills such as history taking, teamwork, and professionalism. Phase II (Foundations of Clinical Practice; Year 3) consists of “S&F: Body Systems in Disease I” (Semester 5) and “S&F: Body Systems in Disease II” (Semester 6); this phase aims to familiarize students with the abnormal human body structure and function, besides physical examination, clinical skills and reasoning. Phases I and II are preclinical and mainly take place in the medical school campus. Basic and advanced skills development is mostly performed in the simulation training complex, which includes high‐fidelity, procedural skills, and simulated outpatient consulting rooms, in addition to a standardized hospital training suite. Lastly, phase III (Clinical Medicine Core) brings the students to the teaching hospitals to apply and gradually built on the concepts learnt during the Phases I and II.
FIGURE 1.
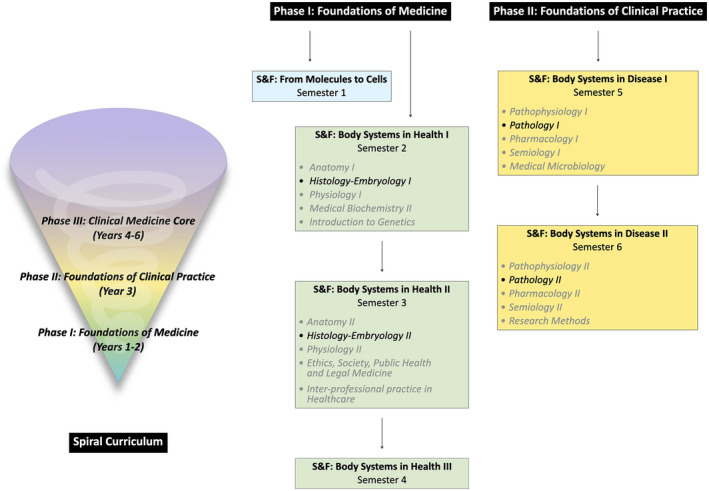
The European University Cyprus medical school follows a spiral, competency‐based curriculum. It consists of three Phases, while a “structure and function” (S&F) approach of each body system is followed through the studies. Histology is taught during the Phase I of the school curriculum (“Histology‐Embryology I” in semester 2; “Histology‐Embryology II” in semester 3), whereas Pathology during the Phase II (“Pathology I” in semester 5; “Pathology II” in semester 6)
Histology and pathology courses description
Histology and Pathology are disciplines that rely on the distinction and interpretation of visual information regarding structure. Histology is taught during the Phase I of the school curriculum (“Histology‐Embryology I” in semester 2; “Histology‐Embryology II” in semester 3), whereas Pathology during the Phase II (“Pathology I” in semester 5; “Pathology II” in semester 6). Weekly activities for both courses include two to three hours of lectures and three to four hours of laboratory sessions (six hours per course for 13 weeks each semester). The same faculty members (C.M., S.C.T., I.P.N.) are involved in the teaching of both histology and pathology courses. Laboratory sessions are conducted in a similar fashion; they start with a description of static microscopic images while integrating structural, functional, and clinical associations, continue with the examination of unknown microscopic slides, and conclude with discussion of one or a few longer cases with clinical relevance. Lectures and laboratory sessions are designed to be interactive and promote active learning by increasing complexity in a stepwise manner (Tian et al., 2014). All student handouts are available prior to the sessions onto the Blackboard Ultra learning management system (Blackboard Inc., Washington, DC). Independent learning includes working on a weekly, tutor‐marked, laboratory assignment that highlights laboratory‐clinical integrations and completing a short multiple‐choice question (MCQ) quiz, with immediate feedback, through Google Forms (Google LLC., Mountain View, CA). The latter revises the knowledge acquired during the lectures and laboratory sessions of each module. Recommended resources include textbooks e.g., Junqueira's Basic Histology: Text and Atlas (Mescher, 2021), Robbins Basic Pathology (Kumar et al., 2017), websites e.g., Michigan Histology and Virtual Microscopy Learning Resources (UMMS, 2021), and YouTube Videos. Online resources become readily available to all students before the sessions begin through weekly laboratory plans. Assessment in both courses takes into account the students' performance on a midterm examination, a final examination, the weekly assignments, and class participation. Each examination consists of 50–60 board style MCQs with and without microscopic images and include questions of diverse difficulty levels, according to Bloom's Taxonomy (Zaidi et al., 2017).
Before the pandemic, all lectures and laboratory sessions were performed F2F on‐campus, while students used a combination of light and virtual microscopy to examine microscopic slides (Figure 2). Sessions were not recorded. However, the pandemic forced an overnight transition to emergency remote teaching (Figure 2). All sessions kept being delivered synchronously, albeit virtually through Blackboard Collaborate (Blackboard Inc., Washington, DC). Virtual microscopy was solely used in the laboratory exercises, a shift not difficult to implement as teaching resources were already prepared before the pandemic. Instructors were able to share their screen and explain microscopic structures at diverse magnifications. Students were allowed to and encouraged to actively engage by using the microphone, chat function, or polling, all of which were available on the platform. The latter also facilitated the tracking of each student's progress. Weekly assignments were performed asynchronously with a submission deadline until the end of the week. Notably, recordings were made readily available some minutes after the completion of each session, offering students flexibility to re‐visit the material. E‐mentoring was provided remotely through the same platform. Lastly, midterm and final examination assessments took place remotely, using online proctoring through the Respondus Lockdown Browser (Respondus Inc., Redmond, WA).
FIGURE 2.
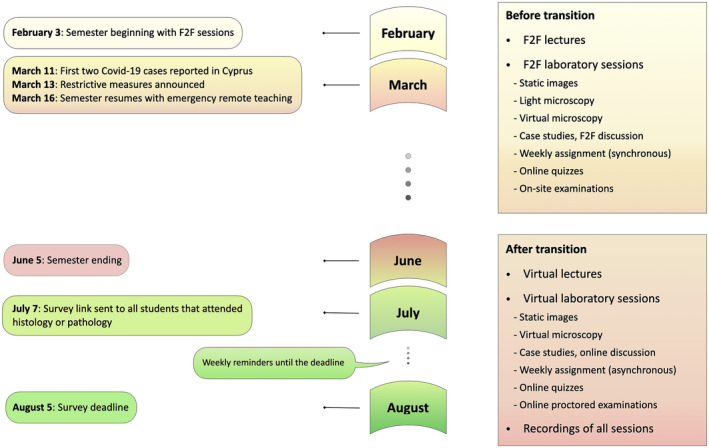
Timeline showing the transition to emergency remote teaching in the authors' medical school, during the 2020 spring semester, and the delivery of the survey to the students, after the semester finished. Similarities and differences in the learning environment of Histology and Pathology courses, before and after the transition, are also presented
Bioethics committee approval
The Cyprus National Bioethics Committee approved the protocol of this research (reference number: 2020.01.139; 24 June 2020). The aim of the survey, besides the fact it was anonymous and optional, were explained to the students before consenting to participate.
Survey details
After the completion of the 2020 spring semester (Figure 2), an e‐survey (Table S1) was sent to the first and third‐year students of the authors' medical school, as well as the second‐year students of the biomedical sciences program. The semester started with on‐campus teaching for a few weeks, yet rapidly shifted towards remote delivery (Figure 2). Histology participants (Histology‐Embryology I; Figure 1) were attending their first microanatomy‐oriented course with only a few weeks of on‐campus experience, before the pandemic hits. In contrast, pathology students (Pathology II; Figure 1) had already completed two conventional courses in histology (Histology‐Embryology I and II) and one in pathology (Pathology I). The same faculty members (C.M., S.C.T., I.P.N.) were involved in the teaching of both histology and pathology courses.
The survey was anonymous and optional and required around 10 min to complete. It was delivered electronically via Google Forms (Google LLC, Mountain View, CA) and comprised background information questions, two scales composed of Likert items, and a few open‐ended questions (Table S1). Examples of background information questions included students' gender, first language, place of living during remote delivery of the classes, familiarity with technology, quality of internet connection, and final examination grade. Students were asked to provide their grade within pre‐defined ranges (<60%; 60%–70%; 70%–80%; 80%–90%; 90%–100%). The first scale was created by the authors, aiming to collect the students' perceptions on their virtual learning experience (VLE scale) while attending the histology and pathology virtual classes. The VLE scale (7‐point scale; strongly disagree‐strongly agree) was composed of 20 Likert items (Figure 3), questioning the quality of the teaching and its comparison with the pre‐pandemic era, the students' perceptions on the importance of these courses, their motivation, and their confidence in the skills they obtained. The second scale used was the perceived stress scale‐10 (PSS‐10), defined by Cohen et al. (1983) and Cohen and Williamson (1988). The PSS‐10 is composed of 10 Likert items (5‐point scale; never‐very often), while its processing gives scores ranging from 0 to 40 [0–13 (low stress); 14–26 (moderate stress); 27–40 (severe stress)], according to the published guidelines.
FIGURE 3.
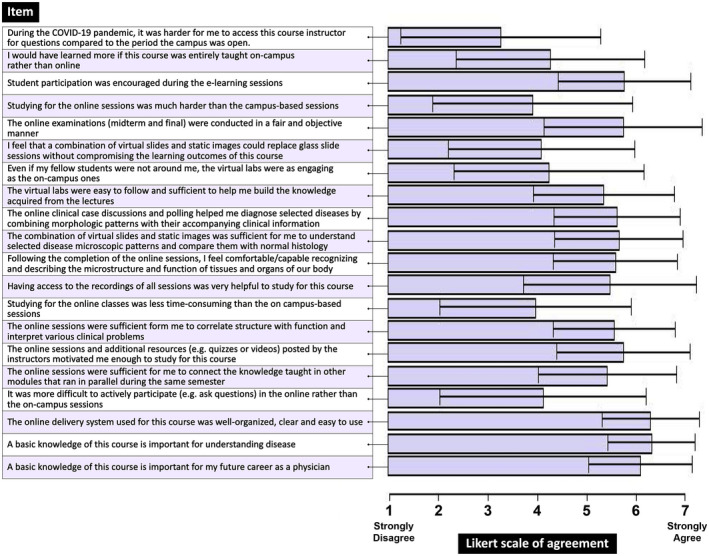
Histology and Pathology students' virtual learning experience (VLE) in the authors' medical school. Results of each VLE item are presented as means with ±standard deviation (±SD). Data were obtained using seven‐point Likert scale (1 = strongly disagree; 2 = disagree; 3 = somewhat disagree; 4 = neither agree nor disagree; 5 = somewhat agree; 6 = agree; 7 = strongly agree)
The survey was open for responses for a four‐week period (Figure 2). Students were notified to participate with weekly emails, also with posts in their WhatsApp year groups by their year student representatives, and their answers were received by the deadline. Data were exported into an Excel program (Microsoft Corporation, Redmond, WA) before processing.
Statistical analysis
Cronbach's a and Kendall's tau B (Tables S2 and S3) were used to assess the reliability of both VLE and PSS‐10 scales of the survey. Categorical variables were compared with the Pearson's chi‐squared test, with results shown as frequencies and percentages. Continuous variables were compared with the independent samples t‐test for normally distributed variables or the Mann‐Whitney test for non‐normally distributed variables, with results shown as means with ±standard deviation (±SD) or medians with interquartile range (IQR). To investigate the construct validity of the VLE questionnaire, an exploratory factor analysis with principal axis factoring was performed and the rotation method used was Varimax with Kaiser Normalization. To confirm that factor analysis was appropriate for the data, we computed the Kaiser‐Meyer‐Olkin measure of sampling adequacy and the Bartlett's test of sphericity. The regression method was used to compute the factor scores of the VLE dimensions resulted from the exploratory factor analysis. The independent samples t‐test was used to compare the factor scores of the VLE dimensions and the Cohens' d effect size was calculated to characterize the strength of the association between VLE dimensions and possible predictors. Lastly, multivariable linear regression models were used to identify significant predictors of VLE and perceived stress, respectively. Multivariable linear regression models include simultaneously several predictor variables in the same model and compute the independent and adjusted effect of each predictor variable to the outcome variable. The standardized regression coefficients of the multivariable linear regression models were the effect sizes of the predictor variables. Statistical analysis was performed with the SPSS statistical package, version 26 (IBM Corp., Armonk, NY) and R statistical software, version 2.12.1 (R Foundation for Statistical Computing, Vienna, Austria). Significance test and confidence intervals were calculated at significance levels of P = 0.05.
RESULTS
Both survey scales were found to have a good reliability. Cronbach's a for the VLE scale was 0.85, after reverse‐coding the negatively keyed items 4, 17, 19, and 20 (Table S1). Cronbach's a for the PSS‐10 was 0.90.
A total of 173/255 (68%) of the enrolled students took part in the survey. More specifically, 89 (51.4%) were histology, while 84 (48.6%) pathology students. Most participants were females (100/173; 57.8%), Greek speakers (103/173; 59.5%), and non‐holders of another degree (147/173; 87%). Students mostly attended the online classes in their home country (145/173; 83.8%) and lived with someone else, such as their family or a fellow student (141/173; 81.5%). The majority perceived their familiarity with technology as expert or advanced (121/173; 69.9%), and around half of them reported having very good (83/173; 48%), rather than average (81/173; 46.8%) or poor (9/173; 5.2%) internet connection during the remote delivery of the classes.
Among the survey participants, the quality of internet connection was significantly associated with the students' final examination performance (Table 1; P = 0.04). Females, students of first language other than English or Greek, holders of another degree prior to medical school, students that attended online classes in their home country, students living with someone else (e.g., their family or a fellow student), and expert/advanced technology users achieved higher scores, but differences were not statistically significant (Table 1).
TABLE 1.
Background characteristics of the students participating in the survey
| Variable | Total (n = 173) | Histology (n = 89) | Pathology (n = 84) | P‐value a | Final examination grade (0–80) (n = 52) | Final examination grade (80–100) (n = 114) | P‐value a |
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Sex | |||||||
| Female | 100 (57.8) | 54 (60.7) | 46 (54.8) | 0.43 | 25 (48.1) | 72 (63.2) | 0.07 |
| Male | 73 (42.2) | 35 (39.3) | 38 (45.2) | 27 (51.9) | 42 (36.8) | ||
| First language | |||||||
| English | 19 (11.0) | 14 (15.7) | 5 (6.0) | 0.05 | 7 (13.5) | 12 (10.5) | 0.59 |
| Greek | 103 (59.5) | 54 (60.7) | 49 (58.3) | 32 (61.5) | 65 (57.0) | ||
| Other | 51 (29.5) | 21 (23.6) | 30 (35.7) | 13 (25.0) | 37 (32.5) | ||
| Holder of another degree | |||||||
| Yes | 22 (13.0) | 7 (8.2) | 15 (17.9) | 0.06 | 6 (12.0) | 16 (14.3) | 0.45 |
| No | 147 (87.0) | 78 (91.8) | 69 (82.1) | 44 (88.0) | 96 (85.7) | ||
| Place of attending online classes | |||||||
| Home country | 145 (83.8) | 79 (88.8) | 66 (78.6) | 0.07 | 40 (76.9) | 98 (86.0) | 0.16 |
| Away from home | 28 (16.2) | 10 (11.2) | 18 (21.4) | 12 (23.1) | 16 (14.0) | ||
| Living situation | |||||||
| With someone else | 141 (81.5) | 78 (87.6) | 63 (75.0) | 0.03 | 40 (76.9) | 95 (83.3) | 0.33 |
| Alone | 32 (18.5) | 11 (12.4) | 21 (25.0) | 12 (23.1) | 19 (16.7) | ||
| Familiarity with technology | |||||||
| Expert | 22 (12.7) | 12 (13.5) | 10 (11.9) | 0.29 | 6 (11.5) | 16 (14.0) | 0.84 |
| Advanced | 99 (57.2) | 55 (61.8) | 44 (52.4) | 29 (55.8) | 65 (57.0) | ||
| Intermediate | 52 (30.1) | 22 (24.7) | 30 (35.7) | 17 (32.7) | 33 (28.9) | ||
| Beginner | – | – | – | – | – | ||
| Quality of internet connection | |||||||
| Very good | 83 (48.0) | 41 (46.1) | 42 (50.0) | 0.39 | 23 (44.2) | 59 (51.8) | 0.04 |
| Average | 81 (46.8) | 45 (50.6) | 36 (42.9) | 29 (55.8) | 46 (40.4) | ||
| Poor | 9 (5.2) | 3 (3.4) | 6 (7.1) | 0 (0.0) | 9 (7.9) | ||
| Device for attending the course | |||||||
| Smartphone | 1 (0.6) | 0 (0.0) | 1 (1.2) | 0.38 | 1 (1.9) | 0 (0.0) | 0.38 |
| Tablet | 14 (8.1) | 9 (10.1) | 5 (6.0) | 3 (5.8) | 8 (7.0) | ||
| Laptop | 152 (87.9) | 76 (85.4) | 76 (90.5) | 47 (90.4) | 101 (88.6) | ||
| Desktop | 6 (3.5) | 4 (4.5) | 2 (2.4) | 1 (1.9) | 5 (4.4) | ||
| Perception for best mode of future course delivery | |||||||
| Entirely on campus | 53 (33.1) | 31 (38.8) | 22 (27.5) | 0.32 | 19 (37.3) | 33 (31.4) | 0.48 |
| Entirely online | 7 (4.4) | 3 (3.8) | 4 (5.0) | 1 (2.0) | 6 (5.7) | ||
| Blended | 100 (62.5) | 46 (57.5) | 54 (67.5) | 31 (60.8) | 66 (62.9) | ||
| Perceived stress (0–40) b | |||||||
| Total perceived stress | 20.1 (8.7) | 18.6 (8.8) | 21.7 (8.5) | 0.03 | 21.0 (8.2) | 19.4 (9.0) | 0.30 |
| Low | 37 (22.7) | 26 (31.3) | 11 (13.8) | 8 (15.4) | 29 (27.1) | 0.13 | |
| Moderate | 85 (52.1) | 40 (48.2) | 45 (56.3) | 33 (63.5) | 51 (47.7) | ||
| High | 41 (25.2) | 17 (20.5) | 24 (30.0) | 11 (21.5) | 27 (25.2) | ||
Significant results are given in Bold.
Chi‐square test or independent samples t‐test.
The tool used to assess the variable “Perceived Stress” was the perceived stress scale‐10 (PSS‐10), which is composed of 10 five‐point Likert scale items where 0 = never and 4 = very often and its processing gives scores ranging from 0 to 40 [0–13 (low stress); 14–26 (moderate stress); 27–40 (severe stress)].
Lastly, when participants were asked about their perception for the best mode of histology and pathology course delivery in the future, most students favored some form of blended learning (57.5% in histology; 67.5% in pathology), while fewer favored entirely on‐campus (38.8% in histology; 27.5% in pathology) or entirely online delivery (3.8% in histology; 5.0% in pathology) (Table 1).
Student perceptions on preclinical emergency remote teaching
Remote delivery of both histology and pathology courses was well‐perceived by the students (Figure 3 and Table S4). In a Likert scale with answers ranging from 1 to 7 (strongly disagree‐strongly agree), participants showed a very positive perception towards the importance of both courses for understanding disease (mean: 6.38 ± 0.91) and their future career as physicians (mean: 6.14 ± 1.09), their remote delivery during the Covid‐19 pandemic (mean: 6.36 ± 1.01), the quality of accompanying resources such as online quizzes or videos (mean: 5.79 ± 1.40), the encouragement of their participation (mean: 5.81 ± 1.39), and the fairness and objectivity of online examinations (mean: 5.78 ± 1.66).
Of interest, students' answers on the negatively keyed items, which compared virtual with traditional F2F instruction, had medians that ranged between 3 (somewhat disagree) to 4 (neither agree nor disagree) (Table S4). More specifically, their answers in the following statements—“It was more difficult to actively participate (e.g., ask questions) in the online rather than the on‐campus sessions” [median: 4 (4.0)], “Studying for the online sessions was much harder than the campus‐based sessions” [median: 4 (4.0)], “I would have learned more if this course was entirely taught on‐campus rather than online” [median: 4 (4.0)], and “During the Covid‐19 pandemic, it was harder for me to access this course instructor for questions compared to the period the campus was open” [median: 3 (4.0)]—is another sign they perceived favorably their remote preclinical education in these particular two courses.
Predictors of virtual learning experience
To give validity on the evidence derived from the VLE scale data, an exploratory factor analysis was performed. The Kaiser‐Olkin measure of sampling adequacy was equal to 0.83, while the P‐value of the Bartlett's test of sphericity equal to 0.001. Four dimensions were formed as a result of this analysis (Table 2):
Course quality and learning outcomes
Student motivation
Virtual against F2F learning
Virtual laboratory sessions
TABLE 2.
Exploratory factor analysis of the virtual learning experience (VLE) scale items
| Items | Factors | ||||
|---|---|---|---|---|---|
| Course quality and learning outcomes | Student motivation | Virtual against F2F learning | Virtual laboratory sessions | Communalities | |
| Item 10 | 0.736 | 0.148 | 0.154 | 0.124 | 0.60 |
| Item 12 | 0.735 | 0.203 | 0.050 | 0.194 | 0.62 |
| Item 11 | 0.694 | 0.237 | 0.104 | 0.141 | 0.57 |
| Item 7 | 0.541 | 0.398 | 0.244 | 0.226 | 0.57 |
| Item 13 | 0.470 | 0.331 | 0.281 | 0.248 | 0.47 |
| Item 9 | 0.317 | −0.081 | 0.024 | −0.048 | 0.11 |
| Item 16 | 0.272 | 0.270 | 0.256 | 0.247 | 0.27 |
| Item 2 | 0.125 | 0.712 | 0.029 | −0.033 | 0.52 |
| Item 3 | 0.136 | 0.583 | 0.400 | 0.077 | 0.53 |
| Item 1 | −0.037 | 0.565 | 0.114 | 0.074 | 0.33 |
| Item 6 | 0.400 | 0.551 | 0.269 | 0.119 | 0.55 |
| Item 18 | 0.193 | 0.433 | 0.074 | 0.221 | 0.57 |
| Item 5 | 0.324 | 0.364 | 0.198 | 0.340 | 0.40 |
| Item 17 reverse | 0.038 | 0.127 | 0.740 | 0.076 | 0.57 |
| Item 19 reverse | 0.148 | 0.055 | 0.696 | 0.335 | 0.62 |
| Item 4 reverse | 0.245 | 0.001 | 0.694 | −0.024 | 0.54 |
| Item 20 reverse | 0.044 | 0.316 | 0.502 | −0.133 | 0.37 |
| Item 15 | 0.152 | 0.074 | −0.045 | 0.864 | 0.78 |
| Item 14 | 0.358 | 0.100 | 0.287 | 0.440 | 0.41 |
| Item 8 | 0.013 | 0.039 | 0.023 | 0.323 | 0.11 |
Extraction Method: Principal Axis Factoring. Rotation Method: Varimax with Kaiser Normalization. Factor loadings with an absolute value > 0.40 are given in Bold.
Abbreviation: F2F, face‐to‐face.
Data were further interpreted using these dimensions (Table 3), also the VLE scale items individually (Table S4). Histology students perceived most dimensions of their VLE less favorably than pathology students (Table 3), specifically “student motivation” (effect size = −0.25; P = 0.001), “virtual laboratory sessions” (effect size = −0.30; P = 0.001), and “course quality and learning outcomes” (effect size = −0.15; P = 0.06). Of interest, they were less convinced than the pathology students that virtual laboratory sessions could replace glass slide sessions without compromising the course learning outcomes [median: 3 (3.0) vs. 5 (2.0); P = 0.001] and that the online sessions were sufficient for them to correlate body structure with function [median: 5 (1.0) vs. 6 (2.0); P = 0.001], while they appreciated more the use of recordings [median: 7 (2.0) vs. 6 (3.0); P = 0.01] (Table S4); the latter could be interpreted as a stronger need to re‐check the materials after the delivery of each session.
TABLE 3.
Virtual learning experience (VLE) of the students according to the course they attended and their final examination grade
| Virtual learning experience | Histology vs. pathology mean difference (95% CI) | d‐value a | P‐value b | Final examination grade (0%–80%) vs. Final exam grade (80%–100%) | d‐value a | P‐value b |
|---|---|---|---|---|---|---|
| Course quality and learning outcomes | −0.26 (−0.53, 0.00) | −0.15 | 0.06 | −0.28 (−0.58, 0.02) | −0.15 | 0.07 |
| Student motivation | −0.44 (−0.69, −0.18) | −0.25 | 0.001 | −0.70 (−1.00, −0.42) | −0.37 | 0.001 |
| Virtual against F2F learning | 0.13 (−0.15, 0.40) | 0.07 | 0.36 | −0.51 (−0.80, −0.23) | −0.27 | 0.01 |
| Virtual laboratory sessions | −0.53 (−0.80, −0.27) | −0.30 | 0.001 | −0.19 (−0.49, 0.10) | −0.10 | 0.20 |
Effect size interpretation: tiny (0–0.05); very small (0.05–0.10); small (0.10–0.20); medium (0.20–0.30); large (0.30–0.40); very large (>0.40). A P‐value ≤ 0.05 was considered statistically significant (bold).
Abbreviation: F2F, face‐to‐face.
Cohen's d effect size.
P‐value of the Independent samples t‐test.
In addition, students that scored less than 80% in their final examination also perceived their VLE less favorably than the ones scoring more than 80% (Table 3), this time in all four dimensions; “course quality and learning outcomes” (effect size = −0.15; P = 0.07), “student motivation” (effect size = −0.37; P = 0.001), “virtual against F2F learning” (effect size = −0.27; P = 0.001), and “virtual laboratory sessions” (effect size = −0.10; P = 0.20). Notably, while examining separately the VLA scale items, these students felt less convinced that basic microanatomy knowledge is important for their future career as physicians [median: 6 (2.0) vs. 7 (1.0); P = 0.001] or to understand disease [median: 6 (1.0) vs. 7 (1.0); P = 0.001], less engaged by the virtual laboratories [median: 3 (3.0) vs. 5 (3.0); P = 0.001]. Furthermore, they considered it harder to study for the online than the previous F2F sessions [median: 5 (2.0) vs. 3 (3.0); P = 0.001], and that they would have learnt more if the course was taught F2F than online [median: 5 (3.0) vs. 4 (4.0); P = 0.001] (Table S4).
Subsequently, a multivariable linear regression model was formed to identify predictors of the four dimensions of the VLE scale (Table 4). Comparable with the previous analysis, the histology course also had a negative effect in three out of four VLE dimensions; “student motivation” [coefficient (95% CI): −0.39 (−0.66, −0.12); effect size = −0.14], “virtual laboratory sessions” [coefficient (95% CI): −0.46 (−0.74, −0.17); effect size = −0.26], and “course quality and learning outcomes” [coefficient (95% CI): −0.46 (−0.76, −0.15); effect size = −0.25]. Better final examination performance (>80%) had a positive effect in three out of four dimensions; “course quality and learning outcomes” [coefficient (95% CI): 0.17 (−0.14, 0.48); effect size = 0.09], “student motivation” [coefficient (95% CI): 0.60 (0.32, 0.88); effect size = 0.31] and “virtual against F2F learning” [coefficient (95% CI): 0.46 (0.17, 0.75); effect size = 0.25]. In addition, a higher perceived stress had a negative effect in three VLE dimensions; “course quality and learning outcomes” [coefficient (95% CI): −0.03 (−0.05, −0.01); effect size = −0.26], “virtual against F2F learning” [coefficient (95% CI): −0.04 (−0.06, −0.02); effect size = −0.38], and “student motivation” [coefficient (95% CI): −0.01 (−0.03, 0.001); effect size = −0.11]. Lastly, male gender had a negative effect in all four dimensions—of them, “student motivation” was significant [coefficient (95% CI): −0.49 (−0.77, −0.22); effect size = −0.27]—while holders of another degree before entering medical school a positive effect in three out of four dimensions—of them, “course quality and learning outcomes” [coefficient (95% CI): 0.45 (0.04, 0.86); effect size = 0.17] and “student motivation” [coefficient (95% CI): 0.34 (0.02, 0.81); effect size = 0.13] were significant.
TABLE 4.
Predictors of the students' virtual learning experience (VLE)
| Variable | Course quality and learning outcomes | Student motivation | Virtual against F2F learning | Virtual laboratory sessions | ||||
|---|---|---|---|---|---|---|---|---|
| Coefficient (95% CI) a | d‐value b | Coefficient (95% CI) a | d‐value b | Coefficient (95% CI) a | d‐value b | Coefficient (95% CI) | d‐value b | |
| Sex | ||||||||
| Female | Ref | Ref | Ref | Ref | ||||
| Male | −0.16 (−0.47, 0.15) | −0.09 | −0.49 (−0.77, −0.22) | −0.27 | −0.18 (−0.47, 0.12) | −0.10 | −0.26 (−0.55, 0.03) | −0.15 |
| Course | ||||||||
| Pathology | Ref | Ref | Ref | Ref | ||||
| Histology | −0.46 (−0.76, −0.15) | −0.25 | −0.39 (−0.66, −0.12) | −0.14 | 0.12 (−0.17, 0.41) | 0.07 | −0.46 (−0.74, −0.17) | −0.26 |
| First language | ||||||||
| Greek | Ref | Ref | Ref | Ref | ||||
| English | 0.28 (−0.22, 0.77) | 0.10 | −0.09 (−0.52, 0.35) | −0.03 | −0.12 (−0.58, 0.34) | −0.04 | −0.43 (−0.89, 0.03) | −0.16 |
| Other | −0.16 (−0.51, 0.19) | −0.08 | −0.15 (−0.46, 0.16) | −0.08 | −0.23 (−0.56, 0.10) | −0.12 | 0.19 (−0.14, 0.52) | 0.10 |
| Holder of another degree | ||||||||
| No | Ref | Ref | Ref | Ref | ||||
| Yes | 0.45 (0.04, 0.86) | 0.17 | 0.34 (0.02, 0.71) | 0.13 | 0.06 (−0.33, 0.45) | 0.04 | 0.00 (−0.39, 0.38) | 0.00 |
| Place of attending online classes | ||||||||
| Away | Ref | Ref | Ref | Ref | ||||
| Home | −0.13 (−0.59, 0.33) | −0.06 | 0.43 (0.03, 0.84) | 0.18 | 0.09 (−0.34, 0.52) | 0.04 | −0.36 (−0.78, 0.06) | −0.16 |
| Living situation | ||||||||
| Alone | Ref | Ref | Ref | Ref | ||||
| With someone else | 0.13 (−0.28, 0.54) | 0.06 | 0.37 (0.00, 0.73) | 0.17 | −0.04 (−0.43, 0.35) | 0.02 | −0.57 (−0.95, −0.19) | −0.26 |
| Familiarity with technology | ||||||||
| Intermediate or Beginner | Ref | Ref | Ref | Ref | ||||
| Expert or Advanced | −0.01 (−0.33, 0.31) | −0.00 | −0.22 (−0.51, 0.06) | −0.12 | −0.12 (−0.42, 0.18) | −0.06 | −0.24 (−0.54, 0.06) | 0.13 |
| Quality of internet connection | ||||||||
| Average or Poor | Ref | Ref | Ref | Ref | ||||
| Very good | −0.14 (−0.44, 0.16) | 0.08 | −0.16 (−0.42, 0.11) | −0.09 | −0.03 (−0.32, 0.25) | −0.02 | 0.18 (−0.10, 0.46) | 0.10 |
| Final examination grade (%) | ||||||||
| 0–80 | Ref | Ref | Ref | Ref | ||||
| 80–100 | 0.17 (−0.14, 0.48) | 0.09 | 0.60 (0.32, 0.88) | 0.31 | 0.46 (0.17, 0.75) | 0.25 | −0.01 (−0.30. 0.28) | −0.01 |
| Perceived stress | −0.03 (−0.05, −0.01) | −0.26 | −0.01 (−0.03, 0.00) | −0.11 | −0.04 (−0.06, −0.02) | −0.38 | 0.00 (−0.02, 0.02) | 0.00 |
Effect size interpretation: tiny (0–0.05); very small (0.05–0.10); small (0.10–0.20); medium (0.20–0.30); large (0.30–0.40); very large (>0.40).
Abbreviations: Ref, reference value; F2F, face‐to‐face.
Regression coefficient of the multivariable linear regression with independent variables the gender, course, first language, holder of another degree, place of attending online classes, living situation, familiarity with technology, quality of internet connection, final examination grade and perceived stress.
Standardized regression coefficients.
To summarize, the following significant predictors of enhanced VLE, in at least one dimension, were identified in this analysis: female gender, pathology course, final examination grade >80%, lower perceived stress levels, studying in home country, and holding of another degree before medical school.
Predictors of perceived stress
To identify significant predictors of perceived stress, a multivariable linear regression model was created (Table 5). The following variables were found to have an independent effect on the student's perceived stress: gender, course, first language, place of attending online classes, and quality of internet connection. Male participants reported lower levels of stress than females (mean difference: −5.1; 95% CI: −7.8, −2.5; P = 0.001), while histology students also had lower levels of perceived stress than pathology students (mean difference: −3.0; 95% CI: −5.7, −0.4; P = 0.001). Students attending the online classes in their home country reported lower levels of stress than students being away from home (mean difference: −3.8; 95% CI: −7.4, −0.1; P = 0.05), while a similar effect was noted on students with very good compared to the ones with poor or average internet connection (mean difference: −4.5; 95% CI: −7.1, −1.9; P = 0.001). In addition, students holding another degree prior to medicine, living with someone else rather than alone, being more familiar with technology, and obtaining a final examination grade >80% reported lower levels of stress, but the differences were not statistically significant (Table 5).
TABLE 5.
Predictors of the students' perceived stress
| Variable | Mean (±SD) | Mean difference (95% CI) | Coefficient (95% CI) | P‐value a |
|---|---|---|---|---|
| Sex | ||||
| Female | 22.2 (±8.5) | |||
| Male | 17.1 (±8.3) | −5.1 (−7.8, −2.5) | −6.0 (−8.6, −3.4) | 0.001 |
| Course | ||||
| Pathology | 21.7 (±8.5) | |||
| Histology | 18.7 (±8.8) | −3.0 (−5.7, −0.4) | −4.1 (−6.7, −1.5) | 0.001 |
| First language | ||||
| Greek | 20.8 (±8.9) | |||
| English | 20.9 (±9.7) | 0.1 (−4.4, 4.7) | 0.39 (−4.0, 4.8) | 0.86 |
| Other | 18.6 (±7.9) | −2.2 (−5.2, 0.9) | −3.7 (−6.7, −0.7) | 0.02 |
| Holder of another degree | ||||
| No | 20.4 (±8.5) | |||
| Yes | 19.4 (±9.8) | −1.1 (−5.1, 3.0) | −1.0 (−4.7, 2.6) | 0.57 |
| Place of attending online classes | ||||
| Away | 23.3 (±7.4) | |||
| Home | 19.5 (±8.9) | −3.8 (−7.4, −0.1) | −4.0 (−8.0, −0.0) | 0.05 |
| Living situation | ||||
| Alone | 22.5 (±8.7) | |||
| With someone else | 19.6 (±8.7) | −2.9 (−6.4, 0.5) | −1.9 (−5.5, 1.8) | 0.32 |
| Familiarity with technology | ||||
| Intermediate or Beginner | 21.2 (±8.4) | |||
| Expert or Advanced | 19.6 (±8.7) | −1.6 (−4.5, 1.3) | 0.2 (−2.6, 3.0) | 0.90 |
| Quality of internet connection | ||||
| Average or Poor | 22.3 (±8.2) | |||
| Very good | 17.8 (±8.8) | −4.5 (−7.1, −1.9) | −4.1 (−6.6, −1.5) | 0.001 |
| Final examination grade (%) | ||||
| 0–80 | 21.0 (±8.2) | |||
| 80–100 | 19.5 (±9.0) | −1.5 (−4.5, 1.4) | −1.4 (−4.2, 1.3) | 0.30 |
The tool used to assess the students' perceived stress was the perceived stress scale‐10 (PSS‐10), which is composed of 10 Likert items [5‐point scale; 0 (never)—4 (very often)] and its processing gives scores ranging from 0 to 40. A total of 173 students (100 females; 73 males) participated in the survey and answered this particular tool. Significant results are given in Bold.
Multivariable linear regression model.
DISCUSSION
Success of emergency remote teaching during the pandemic has been challenged by technical limitations, such as unreliable internet connection, mental fatigue, lack of engagement and hands‐on experience of the students, besides the medical educators' inexperience teaching online or moderating successful virtual small‐group teaching sessions (Cuschieri & Calleja Agius, 2020; Dhawan, 2020; Evans et al., 2020; Pather et al., 2020). However, despite its numerous challenges, this pandemic has given preclinical medical educators a tremendous opportunity to learn, experiment with new ways of learning, and integrate innovative technologies into their courses (Gaur et al., 2020; Parker et al., 2020; Samueli et al., 2020), advancing their leadership and digital skills (Smith & Pawlina, 2021).
This study showed the remote delivery of both histology and pathology courses in the authors' medical school was well‐accepted by most students, who perceived the course outcomes were reached, despite the unprecedented changes induced by the pandemic. Student engaged in the online sessions, making use of the tools provided by the platform that enhance interaction such as the microphone and chat function (Rivera et al., 2021). They also used VM to practice during the laboratory sessions. There are various free VM repositories designed for medical educators, including the Virtual Microscopy Database (Lee et al., 2018), the Iowa Virtual Slidebox (Dee, 2009), and the PathPresenter (Singh, 2021). Research has shown that using VM induces equivalent (Mione et al., 2013; Ordi et al., 2015) or superior learning outcomes (Kuo & Leo, 2019; Lee et al., 2020; Rodrigues‐Fernandes et al., 2020) at the medical school level compared to light microscopy, while LM additionally offers significant advantages, such as enhanced accessibility and collaboration among students, superb image quality, and cost‐effectiveness (Dee, 2009; Saco et al., 2016). Further supporting evidence comes from a recent meta‐analysis, which has shown that e‐learning results in superior learning outcomes in medical education (Pei & Wu, 2019).
This study also demonstrated that, although highly supportive, histology students perceived virtual education with more caution than pathology students. As a similar teaching methodology was employed and the same faculty were involved in the teaching of both courses, these results could be explained on the basis of experience and level of studies. While pathology students had already obtained experience from completing two histology and one pathology conventional courses, first year histology students were attending their first microanatomy‐related course when the pandemic hit (Figure 1). Thus, pathology students possibly found it easier to adjust to the new circumstances forced by the pandemic. In histology and pathology medical courses, images and slides are used as a means to solidify basic processes, understand disease, emphasize basic terminology and laboratory workflow, integrate with other disciplines, promote independent learning and thinking, and educate future physicians of any specialty, rather than train at the level needed for basic scientists or first year pathology residents (Weston, 2018; Parker et al., 2020). These concepts could have been more evident to pathology students, who felt less alarmed by the lack of hands‐on optical microscopy exercises and its potential effect on the quality of their studies, than the histology students. A study by Holaday et al. showed that histology students exhibited a strong preference towards virtual rather than traditional approaches, while this preference increased as the course progressed (Holaday et al., 2013). This study showed a similar trend, albeit during the progression from histology to pathology rather than the histology course itself.
High examination performance was significantly associated with student motivation and adjustment to virtual learning. Indeed, to succeed in online learning, students have to manage their time, plan and regulate their learning effectively, and be critical thinkers (Broadbent & Poon, 2015). Furthermore, our study revealed the quality of internet connection was significantly associated with the students' final examination performance. This is in accordance with the literature, where suboptimal internet connectivity has been shown an important barrier to successful virtual medical education (O'Doherty et al., 2018).
Notably, perceived stress, as defined by Cohen et al. (1983) and Cohen and Williamson (1988), was significantly associated with specific student characteristics. Females reported they experienced higher levels of stress, which is a finding also supported by other studies before (Stegers‐Jager et al., 2020) or during the pandemic (Kannampallil et al., 2020; Salari et al., 2020; Taylor et al., 2020a; Wang et al., 2021). Compared to histology students, pathology students experienced more stress. A recent study reached similar result, reporting higher stress levels during the transitional third year of medical studies (Abdulghani et al., 2020). Indeed, at this stage, medical students are at the crossroads between the preclinical and clinical phase of their medical education. This brings them closer to the realization of the role they are to take at the end of their degree, which could increase their stress levels. Recent studies suggest that medical staff and trainees who have been exposed to patients with Covid‐19 have experienced higher levels of stress and burnout (Kannampallil et al., 2020; Li et al., 2020; Wu et al., 2020). Another study also pointed that residents experienced anxiety more frequently than medical students during this period (Brown et al., 2021). On the other hand, histology students have potentially not yet fully incorporated to the demands of their medical studies and profession and are still in the initial, and more care‐free, adjustment phase. The higher stress levels experienced by those attended the semester away from home could possibly be due to loneliness or lack of support, while in students with native tongue other than Greek or English, it could be implied that cultural factors play a pivotal role. Lastly, students with poor/average internet connection also experienced higher levels of stress at a significant level, as they could be concerned with an additional obstacle to the smooth and successful completion of their studies.
This study and others have shown that emergency remote teaching due to the pandemic has offered educators tremendous opportunities for innovative teaching. However, students lacked the access to the physical university environment, face‐to‐face interactions with faculty and peers, and hands‐on education (Franchi, 2020; Patra et al., 2021). At this point, the main question that arises is what would be about the best delivery mode of histology and pathology courses (or preclinical medical education in general) in the near future, after the pandemic finishes. Could such models be viable in the long term or they were just a short‐term solution? When the students were asked in this study, most proposed some form of blended instruction, rather than solely on‐campus or online. In‐class sessions could provide hands‐on laboratory skills, interactions with peers and educators, professionalism, role‐modeling, and effective teamwork (Smith & Pawlina, 2021). Online sessions could be ideal for introductory lectures and offer a flexible learning environment with innovative teaching solutions, facilitate self‐directed and life‐long learning, and supplement F2F instruction, enhancing students' knowledge acquisition and academic performance (Khalil et al., 2018; Chen et al., 2020; Caruso, 2021). According to the findings of this study, online sessions could be more effective at the late rather than early years of the preclinical medical education, without compromising the quality and lowering the academic standards. Of interest, supportive data come from a recent meta‐analysis, which combined 56 studies from the whole spectrum of health education without a focus on anatomical sciences; this study showed that blended learning exhibits better knowledge outcomes compared to traditional education (Vallée et al., 2020). Therefore, a direction towards blended learning, which will mix traditional on‐campus and online education keeping the best parts of both, could be the way to go in future preclinical medical education.
Limitations of the study
This study has some important limitations. It was a cross‐sectional survey, retrospective in design, and prone to response bias. As it took place after the semester had finished, it was based on student recall. The survey questions were voluntary to complete and a few students did not give an answer to some of them, such as their final examination score. This was a research focused on student perceptions, while two different courses were compared, histology and pathology. Results were solely derived from histology and pathology courses, which means that VLE in other preclinical courses could differ. For example, a recent study about preclinical education revealed negative student perceptions (in contrast to this study) due to absence of hands‐on learning, inability to learn clinical skills, mental exhaustion, and digital fatigue (Shahrvini et al., 2021). Additionally, results of this study came from a single institution. Lastly, there is a possibility of other variables (e.g., study habits) that were not assessed, which could potentially affect the study outcomes.
CONCLUSIONS
This cross‐sectional study aimed to present the student perceptions on preclinical emergency remote teaching and identify predictors of the virtual learning experience and perceived stress. Despite some challenges, it appears that high quality preclinical medical education is possible via virtual learning. While the pandemic forced innovative changes in teaching approaches, histology and pathology online delivery was well‐accepted by most students in the authors' medical school. Pathology students and students with high final examination scores perceived their virtual education more favorably. Lastly, significantly higher levels of stress were noted in females, also in students who attended pathology (rather than histology), had first language other than Greek or English, studied away from their home country, or had a suboptimal internet connection.
CONFLICT OF INTEREST
The authors do not have any conflicts of interest to declare.
Supporting information
Supplementary Material
ACKNOWLEDGMENTS
The authors wish to thank the medical students at the European University Cyprus for participating in this survey and for their continuous support.
Biographies
Ilias P. Nikas, M.D., is an assistant professor of pathology and cytopathology at the School of Medicine, European University Cyprus (EUC), Nicosia, Cyprus. He teaches pathology and histology to medical students and his research interests include cancer diagnostics and medical education.
Demetris Lamnisos, Ph.D., is an associate professor of public health research and health data science in the Department of Health Sciences at the European University Cyprus (EUC), Nicosia, Cyprus. He teaches medical statistics and epidemiology to first‐year medical students and postgraduate students in public health. His research interests are in spatial analysis and geographic health inequalities, trends and forecasts.
Maria Meletiou‐Mavrotheris, Ph.D., is a professor in the Department of Education Sciences, at the European University Cyprus (EUC), Nicosia, Cyprus. She is also Director of the Information Communication Technologies Enhanced Education (ICTEE) Research Laboratory, and Head of Education and Training Services of the Center of Excellence in Innovation and Technology (CERIDES), Nicosia, Cyprus. Her research interests focus on technology‐enabled education, specifically on the use of new and emerging technologies in teaching and learning at the school and higher education level, and in vocational training.
Sophia C. Themistocleous, M.Sc., is a laboratory facilitator at the School of Medicine and special scientist at the School of Sciences, European University Cyprus (EUC), Nicosia, Cyprus. She facilitates in the teaching of laboratory sessions, case studies and occasionally in lectures. She instructs histology/pathology students up to their third‐year of study in biomedical sciences, dentistry and medicine. Her interest in research surrounds forensic science, cancer biology, and genetics.
Chryso Pieridi, Ph.D., is a health/counselling psychologist and a lecturer at the School of Medicine, European University Cyprus (EUC), Nicosia, Cyprus. She teaches medical psychology to second‐year medical students and her research interests include the phenomenology of cancer, as well as the experience of psychotherapeutic processes.
Dimitrios G. Mytilinaios, M.D., Ph.D., is the head of content of the online anatomy platform at Kenhub GmbH in Leipzig, Germany. He taught anatomy and neuroanatomy for several years to first and second‐year students at the University of Athens and the European University Cyprus (EUC). The last few years, he teaches neuroanatomy in various Master Programs in Greece.
Constantinos Michaelides, M.D., is a pathologist and lecturer of histology and embryology at the School of Medicine, European University Cyprus (EUC), Nicosia, Cyprus. He teaches histology and embryology to first and second‐year medical students and pathology to third year medical students. His research interest is in surgical pathology/cytology.
Elizabeth O. Johnson, Ph.D., is a professor of anatomy and Dean of the School of Medicine, European University Cyprus (EUC), Nicosia, Cyprus. She spearheaded anatomical education reform at the Universities of Ioannina (Ioannina, Epirus, Greece) and National and Kapodistrian University of Athens (Athens, Greece), and devised the competency‐based spiral medical curriculum at EUC. She was also a founder of the Laboratory of Education and Research in Neurosciences (LERNs) in the Department of Anatomy, School of Medicine, National and Kapodistrian University of Athens.
Nikas IP, Lamnisos D, Meletiou‐Mavrotheris M, Themistocleous SC, Pieridi C, Mytilinaios DG, Michaelides C, Johnson EO. 2022. Shift to emergency remote preclinical medical education amidst the Covid‐19 pandemic: A single‐institution study. Anat Sci Educ 15:27–41. 10.1002/ase.2159
REFERENCES
- Abdulghani HM, Sattar K, Ahmad T, Akram A. 2020. Association of COVID‐19 pandemic with undergraduate medical students' perceived stress and coping. Psychol Res Behav Manag 13:871–881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allchin D. 2013. Problem‐ and case‐based learning in science: An introduction to distinctions, values, and outcomes. CBE Life Sci Educ 12:364–372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bandaranayake RC. 2017. Integrated learning. In: Dent JA, Harden RM, Hunt D (Editors). A Practical Guide for Medical Teachers. 5th Ed. London, UK: Elsevier Ltd. p 122–127. [Google Scholar]
- Broadbent J, Poon WL. 2015. Self‐regulated learning strategies & academic achievement in online higher education learning environments: A systematic review. Internet High Educ 27:1–13. [Google Scholar]
- Brown A, Kassam A, Paget M, Blades K, Mercia M, Kachra R. 2021. Exploring the global impact of the COVID‐19 pandemic on medical education: An international cross‐sectional study of medical learners. Can Med Educ J 12:28–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caruso MC. 2021. Virtual microscopy and other technologies for teaching histology during Covid‐19. Anat Sci Educ 14:19–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen J, Zhou J, Wang Y, Qi G, Xia C, Mo G, Zhang Z. 2020. Blended learning in basic medical laboratory courses improves medical students' abilities in self‐learning, understanding, and problem solving. Adv Physiol Educ 44:9–14. [DOI] [PubMed] [Google Scholar]
- Cheng X, Chan LK, Cai H, Zhou D, Yang X. 2021. Adaptions and perceptions on histology and embryology teaching practice in China during the Covid‐19 pandemic. Translational Res Anat 24:100115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen S, Williamson GM. 1988. Perceived stress in a probability sample of the United States. In: Spacapan S, Oskamp S (Editors). The Social Psychology of Health. 1st Ed. Newbury Park, CA: Sage Publications, Inc. p 31–67. [Google Scholar]
- Cohen S, Kamarck T, Mermelstein R. 1983. A global measure of perceived stress. J Health Soc Behav 24:385–396. [PubMed] [Google Scholar]
- Cuschieri S, Calleja Agius J. 2020. Spotlight on the shift to remote anatomical teaching during Covid‐19 pandemic: Perspectives and experiences from the University of Malta. Anat Sci Educ 13:671–679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dee FR. 2009. Virtual microscopy in pathology education. Hum Pathol 40:1112–1121. [DOI] [PubMed] [Google Scholar]
- Dhawan S. 2020. Online learning: A panacea in the time of COVID‐19 crisis. J Educ Technol Syst 49:5–22. [Google Scholar]
- El Sadik A, Al Abdulmonem W. 2021. Improvement in student performance and perceptions through a flipped anatomy classroom: Shifting from passive traditional to active blended learning. Anat Sci Educ 14:482–490. [DOI] [PubMed] [Google Scholar]
- Evans DJ, Bay BH, Wilson TD, Smith CF, Lachman N, Pawlina W. 2020. Going virtual to support anatomy education: A STOPGAP in the midst of the COVID‐19 pandemic. Anat Sci Educ 13:279–283. [DOI] [PubMed] [Google Scholar]
- Flynn L, Jalali A, Moreau KA. 2015. Learning theory and its application to the use of social media in medical education. Postgrad Med J 91:556–560. [DOI] [PubMed] [Google Scholar]
- Franchi T. 2020. The impact of the COVID‐19 pandemic on current anatomy education and future careers: A student's perspective. Anat Sci Educ 13:309–312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fu L, Swete M, Selgrade D, Chan CW, Rodriguez R, Wolniak K, Blanco LZ Jr. 2021. Virtual pathology elective provides uninterrupted medical education and impactful pathology education during the COVID‐19 pandemic. Acad Pathol 8:23742895211010275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gaur U, Majumder MA, Sa B, Sarkar S, Williams A, Singh K. 2020. Challenges and opportunities of preclinical medical education: COVID‐19 crisis and beyond. SN Compr Clin Med (in press; 10.1007/s42399-020-00528-1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo AA, Crum MA, Fowler LA. 2021. Assessing the psychological impacts of COVID‐19 in undergraduate medical students. Int J Environ Res Public Health 18:2952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harmon DJ, Attardi SM, Barremkala M, Bentley DC, Brown KM, Dennis JF, Goldman HM, Harrell KM, Klein BA, Ramnanan CJ, Richtsmeier JT, Farkas GJ. 2021. An analysis of anatomy education before and during Covid‐19: May‐August 2020. Anat Sci Educ 14:132–147. [DOI] [PubMed] [Google Scholar]
- Harrell KM, McGinn MJ, Edwards CD, Warren Foster K, Meredith MA. 2021. Crashing from cadaver to computer: Covid‐driven crisis‐mode pedagogy spawns active online substitute for teaching gross anatomy. Anat Sci Educ 14:536–551. [DOI] [PubMed] [Google Scholar]
- Holaday L, Selvig D, Purkiss J, Hortsch M. 2013. Preference of interactive electronic versus traditional learning resources by university of Michigan medical students during the first year histology component. Med Sci Educ 23:607–619. [Google Scholar]
- Kannampallil TG, Goss CW, Evanoff BA, Strickland JR, McAlister RP, Duncan J. 2020. Exposure to COVID‐19 patients increases physician trainee stress and burnout. PLoS One 15:e0237301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karamaroudis S, Poulogiannopoulou E, Sotiropoulos MG, Kalantzis T, Johnson EO. 2020. Implementing Change in neuroanatomy education: Organization, evolution, and assessment of a near‐peer teaching program in an undergraduate medical school in Greece. Anat Sci Educ 13:694–706. [DOI] [PubMed] [Google Scholar]
- Katz M, Nandi N. 2021. Social media and medical education in the context of the COVID‐19 pandemic: Scoping review. JMIR Med Educ 7:e25892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kazerooni AR, Amini M, Tabari P, Moosavi M. 2020. Peer mentoring for medical students during the COVID‐19 pandemic via a social media platform. Med Educ 54:762–763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khalil MK, Abdel Meguid EM, Elkhider IA. 2018. Teaching of anatomical sciences: A blended learning approach. Clin Anat 31:323–329. [DOI] [PubMed] [Google Scholar]
- Kirkwood A, Price L. 2014. Technology‐enhanced learning and teaching in higher education: What is ‘enhanced’ and how do we know? A critical literature review. Learn Media Tech 39:6–36. [Google Scholar]
- Krippendorf BB, Lough J. 2005. Complete and rapid switch from light microscopy to virtual microscopy for teaching medical histology. Anat Rec 285B:19–25. [DOI] [PubMed] [Google Scholar]
- Kuo KH, Leo JM. 2019. Optical versus virtual microscope for medical education: A systematic review. Anat Sci Educ 12:678–685. [DOI] [PubMed] [Google Scholar]
- Kumar V, Abbas AK, Aster JC. 2017. Robbins Basic Pathology. 10th Ed. Philadelphia, PA: Elsevier Inc. 935 p. [Google Scholar]
- Li Y, Wang Y, Jiang J, Valdimarsdóttir UA, Fall K, Fang F, Song H, Lu D, Zhang W. 2020. Psychological distress among health professional students during the COVID‐19 outbreak. Psychol Med 51:1952–1954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Longhurst GJ, Stone DM, Dulohery K, Scully D, Campbell T, Smith CF. 2020. Strength, weakness, opportunity, threat (SWOT) analysis of the adaptations to anatomical education in the United Kingdom and Republic of Ireland in response to the Covid‐19 pandemic. Anat Sci Educ 13:301–311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee BC, Hsieh ST, Chang YL, Tseng FY, Lin YJ, Chen YL, Wang SH, Chang YF, Ho YL, Ni YH, Chang SC. 2020. A web‐based virtual microscopy platform for improving academic performance in histology and pathology laboratory courses: A pilot study. Anat Sci Educ 13:743–758. [DOI] [PubMed] [Google Scholar]
- Lee LM, Goldman HM, Hortsch M. 2018. The virtual microscopy database‐sharing digital microscope images for research and education. Anat Sci Educ 11:510–515. [DOI] [PubMed] [Google Scholar]
- Masters K, Gibbs T. 2007. The spiral curriculum: Implications for online learning. BMC Med Educ 7:52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mescher AL. 2021. Junqueira's Basic Histology: Text and Atlas. 16th Ed. New York, NY: McGraw‐Hill Education. 576 p. [Google Scholar]
- Mione S, Valcke M, Cornelissen M. 2013. Evaluation of virtual microscopy in medical histology teaching. Anat Sci Educ 6:307–315. [DOI] [PubMed] [Google Scholar]
- O'Byrne L, Gavin B, Adamis D, Lim YX, McNicholas F. 2021. Levels of stress in medical students due to COVID‐19. J Med Ethics 47:383–388. [DOI] [PubMed] [Google Scholar]
- O'Doherty D, Dromey M, Lougheed J, Hannigan A, Last J, McGrath D. 2018. Barriers and solutions to online learning in medical education – An integrative review. BMC Med Educ 18:130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ordi O, Bombí JA, Martínez A, Ramírez J, Alòs L, Saco A, Ribalta T, Fernández PL, Campo E, Ordi J. 2015. Virtual microscopy in the undergraduate teaching of pathology. J Pathol Inform 6:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parker EU, Chang O, Koch L. 2020. Remote anatomic pathology medical student education in Washington state. Am J Clin Pathol 154:585–591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pather N, Blyth P, Chapman JA, Dayal MR, Flack NA, Fogg QA, Green RA, Hulme AK, Johnson IP, Meyer AJ, Morley JW, Shortland PJ, Strkalj G, Strkalj M, Valter K, Webb AL, Woodley SJ, Lazarus MD. 2020. Forced disruption of anatomy education in Australia and New Zealand: An acute response to the COVID‐19 pandemic. Anat Sci Educ 13:284–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patra A, Chaudhary P, Ravi KS. 2021. Adverse impact of Covid‐19 on anatomical sciences teachers of India and proposed ways to handle this predicament. Anat Sci Educ 14:163–165. [DOI] [PubMed] [Google Scholar]
- Pei L, Wu H. 2019. Does online learning work better than offline learning in undergraduate medical education? A systematic review and meta‐analysis. Med Educ Online 24:1666538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qian Q, Yan Y, Xue F, Lin J, Zhang F, Zhao J. 2021. Coronavirus disease 2019 (COVID‐19) learning online: A flipped classroom based on micro‐learning combined with case‐based learning in undergraduate medical students. Adv Med Educ Pract 12:835–842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rahm AK, Töllner M, Hubert MO, Klein K, Wehling C, Sauer T, Hennemann HM, Hein S, Kender Z, Günther J, Wagenlechner P, Bugaj TJ, Boldt S, Nikendei C, Schultz JH. 2021. Effects of realistic e‐learning cases on students' learning motivation during COVID‐19. PLoS One 16:e0249425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reuman L, Jacoby RJ, Fabricant LE, Herring B, Abramowitz JS. 2015. Uncertainty as an anxiety cue at high and low levels of threat. J Behav Ther Exp Psychol 47:111–119. [DOI] [PubMed] [Google Scholar]
- Rhim HC, Han H. 2020. Teaching online: Foundational concepts of online learning and practical guidelines. Korean J Med Educ 32:175–183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rivera R, Smart J, Sakaria S, Wray A, Wiechmann W, Boysen‐Osborn M, Toohey S. 2021. Planning engaging, remote, synchronous didactics in the COVID‐19 pandemic era. JMIR Med Educ 7:e25213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodrigues‐Fernandes CI, Speight PM, Khurram SA, Araújo ALD, Perez DE da C, Fonseca FP, Lopes MA, de Almeida OP, Vargas PA, Santos‐Silva AR. 2020. The use of digital microscopy as a teaching method for human pathology: A systematic review. Virchows Arch 477:475–486. [DOI] [PubMed] [Google Scholar]
- Saco A, Bombi JA, Garcia A, Ramírez J, Ordi J. 2016. Current status of whole‐slide imaging in education. Pathobiology 83:79–88. [DOI] [PubMed] [Google Scholar]
- Salari N, Hosseinian‐Far A, Jalali R, Vaisi‐Raygani A, Rasoulpoor S, Mohammadi M, Rasoulpoor S, Khaledi‐Paveh B. 2020. Prevalence of stress, anxiety, depression among the general population during the COVID‐19 pandemic: A systematic review and meta‐analysis. Global Health 16:57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Samueli B, Sror N, Jotkowitz A, Taragin B. 2020. Remote pathology education during the COVID‐19 era: Crisis converted to opportunity. Ann Diagn Pathol 49:151612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saraswathi I, Saikarthik J, Senthil Kumar K, Srinivasan KM, Ardhanaari M, Gunapriya R. 2020. Impact of COVID‐19 outbreak on the mental health status of undergraduate medical students in a COVID‐19 treating medical college: A prospective longitudinal study. PeerJ 8:e10164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Selvig D, Holaday LW, Purkiss J, Hortsch M. 2015. Correlating students' educational background, study habits, and resource usage with learning success in medical histology. Anat Sci Educ 8:1–11. [DOI] [PubMed] [Google Scholar]
- Shahrvini B, Baxter SL, Coffey CS, MacDonald BV, Lander L. 2021. Pre‐clinical remote undergraduate medical education during the COVID‐19 pandemic: A survey study. BMC Med Educ 21:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singh R. 2021. PathPresenter. Mt. Sinai School of Medicine, New York, NY. URL: https://pathpresenter.net [accessed 10 November 2021]. [Google Scholar]
- Smith CF, Pawlina W. 2021. A journey like no other: Anatomy 2020! Anat Sci Educ 14:57. [DOI] [PubMed] [Google Scholar]
- Somera Dos Santos F, Osako MK, Perdoná GD, Alves MG, Sales KU. 2021. Virtual microscopy as a learning tool in Brazilian medical education. Anat Sci Educ 14:408–416. [DOI] [PubMed] [Google Scholar]
- Stegers‐Jager KM, Savas M, Waal J, Rossum EF, Woltman AM. 2020. Gender‐specific effects of raising Year‐1 standards on medical students' academic performance and stress levels. Med Educ 54:538–546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor S, Landry CA, Paluszek MM, Fergus TA, McKay D, Asmundson GJ. 2020a. COVID stress syndrome: Concept, structure, and correlates. Depress Anxiety 37:706–714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor S, Landry CA, Paluszek MM, Fergus TA, McKay D, Asmundson GJ. 2020b. Development and initial validation of the COVID stress scales. J Anxiety Disord 72:102232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tian Y, Xiao W, Li C, Liu Y, Qin M, Wu Y, Xiao L, Li H. 2014. Virtual microscopy system at Chinese medical university: An assisted teaching platform for promoting active learning and problem‐solving skills. BMC Med Educ 14:74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torda A. 2020. How COVID‐19 has pushed us into a medical education revolution. Intern Med J 50:1150–1153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- UMMS . 2021. University of Michigan Medical School. Michigan histology and virtual microscopy learning resources: Histology at the University of Michigan. University of Michigan, Ann Arbor, MI. URL: http://histology.medicine.umich.edu/ [accessed 15 November 2021]. [Google Scholar]
- Vallée A, Blacher J, Cariou A, Sorbets E. 2020. Blended learning compared to traditional learning in medical education: Systematic review and meta‐analysis. J Med Internet Res 22:e16504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Viveka S, Sagar TV, Sudha MJ. 2017. Effectiveness of flipped classroom for teaching anatomy and students' perceptions. Nat J Clin Anat 6:71–81. [Google Scholar]
- Wang J, Liu W, Zhang Y, Xie S, Yang B. 2021. Perceived stress among Chinese medical students engaging in online learning in light of COVID‐19. Psychol Res Behav Manag 14:549–562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weston WW. 2018. Do we pay enough attention to science in medical education? Can Med Educ J 9:e109–e114. [PMC free article] [PubMed] [Google Scholar]
- Wu W, Zhang Y, Wang P, Zhang L, Wang G, Lei G, Xiao Q, Cao X, Bian Y, Xie S, Huang F, Luo N, Zhang J, Luo M. 2020. Psychological stress of medical staffs during outbreak of COVID‐19 and adjustment strategy. J Med Virol 92:1962–1970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yohannan DG, Oommen AM, Umesan KG, Raveendran VL, Sreedhar LSL, Anish TS, Hortsch M, Krishnapillai R. 2019. Overcoming barriers in a traditional medical education system by the stepwise, evidence‐based introduction of a modern learning technology. Med Sci Educ 29:803–817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zaidi NB, Hwang C, Scott S, Stallard S, Purkiss J, Hortsch M. 2017. Climbing Bloom's taxonomy pyramid: Lessons from a graduate histology course. Anat Sci Educ 10:456–464. [DOI] [PubMed] [Google Scholar]
- Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, Si HR, Zhu Y, Li B , Huang CL, Chen HD, Chen J, Luo Y, Guo H, Jiang RD, Liu MQ, Chen Y , Shen XR, Wang X, Zheng XS, Zhao K, Chen QJ, Deng F, Liu LL , Yan B, Zhan FX, Wang YY, Xiao GF, Shi ZL. 2020. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 579:270–273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zibold J, Gernert JA, Reik LJU, Keidel LM, Graupe T, Dimitriadis K. 2021. Adaptations to mentoring and peer mentor training at the medical faculty during the COVID‐19 pandemic. GMS J Med Educ 38:Doc8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material