

Abstract
BACKGROUND:
Triaxial accelerometer output [Vector Magnitude (VM) counts] may better estimate physical activity intensity as reflected in the rate of oxygen uptake (VO2) than the traditional Vertical Axis (VA) counts in adults with Down syndrome (DS). This study examined the accuracy of VM vs. VA counts in estimating V̇O2 in adults with and without DS across different physical activities and sedentary behaviours.
METHODS:
Sixteen adults with DS (10 men; 31 ± 15 years) and 19 adults without DS (10 men; 24 ± 5 years) performed 12 tasks. V̇O2 was measured by portable spirometer (K4b2, Cosmed) and VM and VA with an accelerometer (wGT3X-BT, Actigraph).
RESULTS:
VM and VA were significant predictors of V̇O2 in adults with DS (p<0.001; R2=0.74 and 0.65, respectively) and adults without DS (p<0.001; p<0.001; R2=0.75 and 0.61, respectively). Absolute error of prediction was significantly smaller for VM than VA for sitting, playing app, drawing, sweeping, standing, and basketball (p≤0.005), but smaller for VA than VM for walking at 0.8 m·s−1 (p=0.005). Bland-Altman plots for adults with and without DS indicated narrower limits of agreement for VM than VA (−5.57–5.57 and −6.44–6.44 ml·kg−1.min−1; −6.21–6.17 and −7.75–7.74 ml·kg−1.min−1, respectively).
CONCLUSION:
VM and VA are significant predictors of V̇O2 in adults with and without DS, yet VM more accurately estimated V̇O2 than VA for most tasks. Development of accelerometer-based prediction of physical activity levels in adults with and without DS may improve by utilizing VM counts.
Keywords: disability, Down syndrome, physical activity, sedentary behaviour, accelerometer
Background
Down Syndrome (DS) is the most common genetic chromosomal disorder caused by trisomy of the 21st chromosome (Bull, 2020). It is estimated that more than 250,000 people with DS live in the United States (Presson et al., 2013). Adults with DS have high cardiometabolic risk as indicated by high rates of obesity, cardiovascular disease, and diabetes, and very low cardiovascular fitness (Baynard et al., 2008; Magge et al., 2019; Rafii et al., 2019). These conditions may be alleviated or prevented by increasing physical activity and decreasing sedentary behaviour levels (Paul et al., 2019). Adults with DS exhibit low levels of physical activity and high levels of sedentary behaviour (Agiovlasitis et al., 2020; Oreskovic et al., 2020; Phillips & Holland, 2011). This knowledge base, however, is not conclusive due to methodological concerns with accelerometer-based measurement of physical activity and sedentary behaviour – accelerometers have not been calibrated for adults with DS.
One of the approaches to accelerometer calibration involves the development of cut-points for physical activity intensity based on the association between accelerometer output and the energy expenditure or the rate of oxygen uptake (V̇O2) during activities and sedentary behaviours. Although most present accelerometers provide both triaxial and uniaxial outputs, there are several sets of cut-points for estimating physical activity levels in various populations based on uniaxial output and are still in use. Previous studies, however, have demonstrated that, in people without disabilities, triaxial accelerometer output is more accurate than uniaxial in estimating the energy expenditure of physical activity and sedentary behaviour (Howe et al., 2009; Yamada et al., 2009). One study reported that triaxial output from a hip accelerometer expressed as the vector magnitude (VM) had a stronger association with V̇O2 during walking than the single vertical axis (VA) output in people with, but not without, DS (Leung et al., 2021). The researchers hypothesized that this was due to the greater mediolateral motion of the body center of mass that adults with DS exhibit compared to adults without DS during walking (Agiovlasitis et al., 2009). Indeed, adults with DS demonstrate higher energy expenditure during walking, which has been found associated with gait characteristics (Agiovlasitis et al., 2011, 2015, 2018). Not surprisingly, the relationship between energy expenditure and uniaxial accelerometer output during walking is different between adults with and without DS (Agiovlasitis et al., 2011, 2012). The study by Leung et al. (2021), however, did not evaluate the error of predicting V̇O2 from VM or VA counts in adults with and without DS and examined only walking. More recent research has shown that, across various physical activities and sedentary behaviours, differences between adults with and without DS in the energy expenditure to VM counts relationship are smaller than those shown in past research for VA counts (Agiovlasitis et al., 2011; Allred et al., 2019). Nevertheless, it has not been directly examined if, beyond walking, VM provides better V̇O2 prediction than VA across household, recreational, and occupational physical activities and sedentary behaviour in adults with DS. Examining this issue will advance research on accelerometry in adults with DS and may lead to more accurate measurement of their physical activity and sedentary behaviour levels.
The current study examined whether VM or VA more accurately predict V̇O2 in adults with and without DS. We hypothesized that the triaxial VM would correlate more strongly and thereby offer more accurate estimates of V̇O2 across a range of household, recreational, and occupational physical activities and sedentary behaviour than the uniaxial VA.
Methods
Participants
Sixteen adults with DS (10 males, 6 females; age 31 ± 15 years) and 19 adults without DS (10 males, 9 females; age 24 ± 5 years) were recruited for this study. Participants with DS were from local group homes, Special Olympics, vocational rehabilitation programs, and participants from previous research. Inclusion criteria for the study were: (a) age 18–45 years; (b) being ambulatory without assistance devices; and (c) having the ability to comprehend and adhere to the testing protocol. Participants were excluded if they met the following criteria: (a) using ambulatory assistive devices; and (b) being unable to understand the testing protocol during the consent process or familiarization session. Participants with and without DS provided written informed consent and the legal guardians of participants with DS gave written permission. Participants without DS were recruited from the local community. All testing procedures were approved by an institutional review board at Mississippi State University.
Protocol
Participants attended three sessions. The first session lasted ~1 h and was utilized for familiarization of participants with the personnel and testing equipment and procedures. Data collection occurred in the remaining two sessions; each session lasted ~1.5 h. The data collection procedures were practiced extensively by the research team.
Familiarization Session
During the familiarization session, height (cm) and weight (kg) were measured and informed calculation of body mass index (BMI; kg∙m−2). Participants were then fitted with the accelerometer and portable metabolic system and practiced sitting, standing, and walking at their preferred walking speed for 6 min while wearing all equipment. Next, all equipment was removed, and the participant practiced the remaining activities and sedentary behaviours of the testing procedure for at least 1–2 min. Additional time was allowed for participants who needed more time to become familiar with an activity. The data collection sessions were not concluded until the research team felt confident that the participant fully understood each activity.
Data Collection Sessions
Participants attended two data collection sessions. All equipment was worn by the participant during all activities and sedentary behaviours. Six of the activities were performed during the first session, and the other six were performed during the second session. The tasks selected for the study consisted of sedentary behaviours, household chores, recreational activities, and occupational activities to replicate common daily tasks that participants might perform. Activities were performed for 6-min followed by a 6-min rest period between activities. The rest period was used for recovery of metabolism to resting levels before performing the next activity.
The first data collection session included these activities: (1) standing; (2) walking at the participant’s preferred walking speed; (3) slow walk (1.8 mph); (4) fast walk (3.1 mph); (5) transporting a 3.5 kg box between two carts distanced 6 meters apart; and (6) dribbling, passing, and shooting a basketball. The pacing of the slow and fast walk trials was done by a researcher using a distance-measuring wheel affixed with a cycle computer that instantaneously displayed walking speed. This allowed the researcher to maintain the appropriate speed while the participant walked ~1 m behind the researcher. A second researcher walked with the participant for motivation and to make sure they maintained ~1 m distance from the researcher with the distance wheel.
The second data collection session included: (1) sitting quietly; (2) playing a game on a tablet; (3) drawing with markers; (4) folding clothes; (5) sweeping up shredded paper spread out over an area ~16 m2; and (6) a fitness circuit. The fitness circuit consisted of shoulder raises, bodyweight squats, bicep curls, forward and backwards line jumps, standing rows, and box step-ups. Each exercise was performed for 10 repetitions before moving to the next exercise. Shoulder raises and bicep curls were performed with two light-weight dumbbells (1–2 lbs.). Banded rows were performed using an elastic resistance band. For the remaining exercises, no resistance was used. The circuit was led by a member of the research team demonstrating and the exercises and performing them together with the participant. The exercise circuit was repeated for the entire 6 min. All other activities were performed by the participant at their own pace.
Instruments
Two main measurement instruments were included in this study – the K4b2 (Cosmed, Chicago, IL) portable metabolic system and the wGT3X-BT (Actigraph LLC, Pensacola, FL) triaxial accelerometer. The K4b2 measured V̇O2 during each activity. The K4b2 was worn by the participant on the front of the body with a harness. The participant wore a face mask covering the nose and mouth. This mask was connected to the K4b2 unit through a rotary flow turbine which allowed for measurement of respiratory gas concentration (O2 and CO2) along with flow volumes. The wGT3X-BT accelerometer was used to collect VM and VA counts. VM counts are a triaxial measure of acceleration along the anteroposterior, vertical, and mediolateral axes, while VA counts are a measure of acceleration along the vertical axis only. Participants wore the accelerometer over the non-dominant hip with an elastic belt.
Rate of Oxygen Uptake (V̇O2)
The K4b2 portable spirometer underwent manufacturer recommended calibration before each data collection session. V̇O2 data from the K4b2 were collected during activities and sedentary behaviours. V̇O2, measured in mL∙kg−1∙min−1, was recorded and averaged over the last 3 min of each activity. To ensure that steady state was reached, the first 3 min of each activity were discarded.
Accelerometer Data
The wGTX-BT triaxial accelerometer data were sampled at 100 Hz and processed in 1s epochs using the ActiLife software (version 6.13.3). Accelerometer data were collected during activities and sedentary behaviours. The last 3 minutes for VM and VA were used to calculate rate per min to be used in statistical analysis. The first 3 min of each activity were discarded for the accelerometer output also.
Statistical Analyses
Data were analyzed using the Statistical Package for the Social Sciences (SPSS, version 27.0, Chicago, IL). Two separate multi-level regression models for each group were used to predict V̇O2 from VA or VM. The fit of the models was evaluated with the R2 and accuracy with Bland-Altman plots and absolute percent error which was compared between models across tasks using 3-way (method-by-task-by-group) analysis of variance (ANOVA) and follow-up paired-samples t-tests as warranted.
Results
Both VM and VA significantly predicted V̇O2 in adults with DS in separate models (p < 0.001; R2 = 0.74 and 0.65, respectively; Table 1), as well as adults without DS (p < 0.001; R2 = 0.75 and 0.61, respectively; Table 1). Bland-Altman plots for adults with DS indicated zero mean error for both models; however, the limits of agreement were narrower for the VM than the VA model (−5.57 to 5.57 and −6.44 to 6.44 ml·kg−1.min−1, respectively). Similarly, Bland-Altman plots for adults without DS indicated nearly-zero mean error for VM (−0.02) and VA (−0.01) with narrower limits of agreement for the VM than the VA model (−6.21 to 6.17 and −7.75 to 7.74 ml·kg−1.min−1, respectively). For both DS and Non-DS, limits of agreement from Bland-Altman plots were narrower for VM than VA (Figure 1).
Table 1.
Regression models predicting rate of oxygen uptake (V̇O2) from vertical axis (VA) or vector magnitude (VM) accelerometer counts in adults with Down syndrome (DS) and without Down syndrome (Non-DS).
| Vertical Axis | Vector Magnitude | |||||
|---|---|---|---|---|---|---|
| b | SE | b | SE | |||
| DS | Intercept | 5.937070 | 0.396450 | 4.488373 | 0.440668 | |
| Slope | 0.004332 | 0.000224 | 0.002548 | 0.000098 | ||
| Non-DS | Intercept | 7.336004 | 0.443037 | 5.388516 | 0.444785 | |
| Slope | 0.003518 | 0.000181 | 0.002898 | 0.000100 | ||
Figure 1.
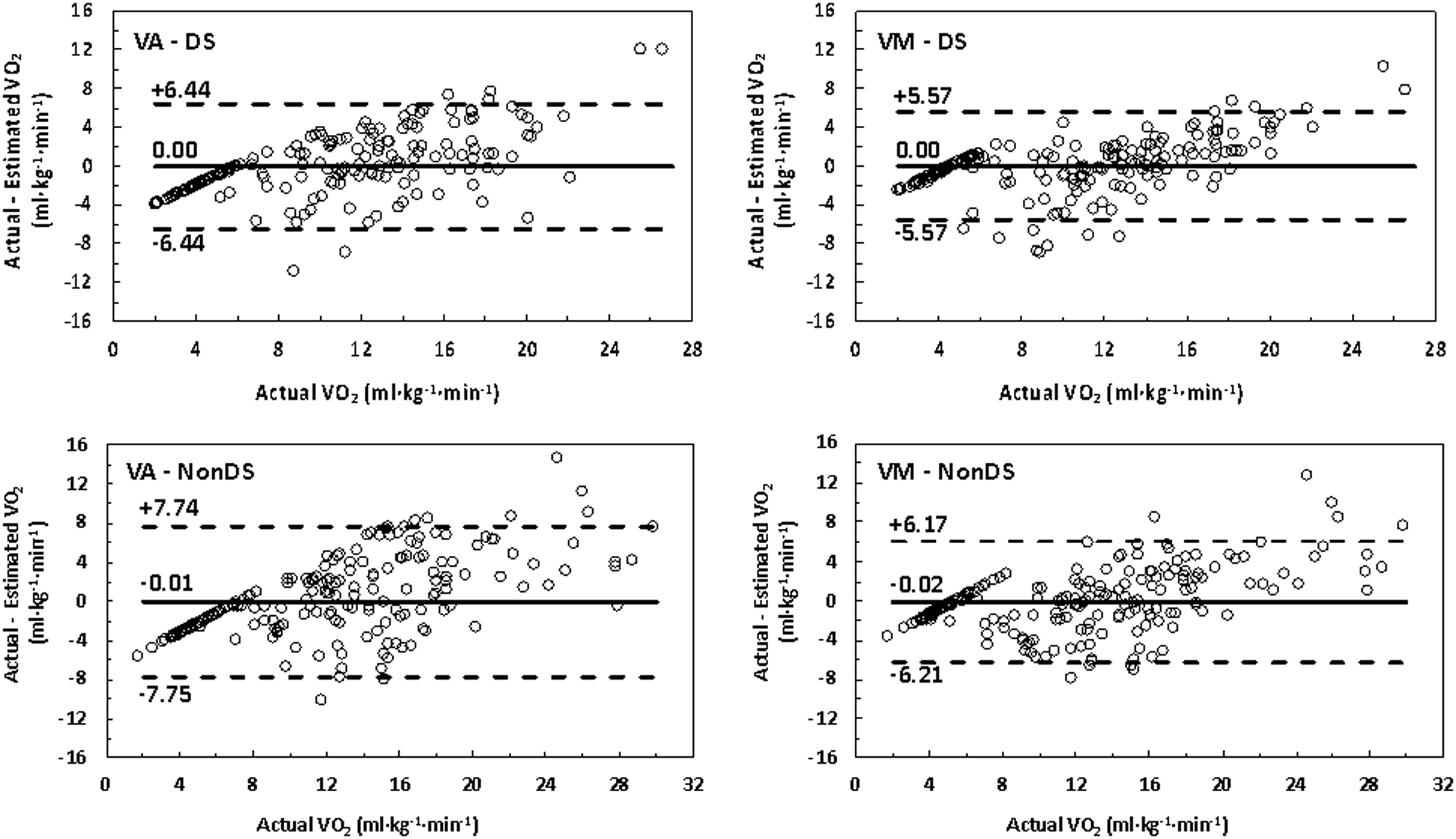
Bland-Altman plots for difference between actual and estimated oxygen uptake (V̇O2) from vertical axis (VA) and vector magnitude (VM) prediction models for adults with Down syndrome (DS) and without Down syndrome (Non-DS)
Mean and standard deviation of absolute percent error for predicting V̇O2 using models developed for VA and VM accelerometer counts across activities between DS and Non-DS are shown in Table 2. Three-way (method-by-task-by-group) ANOVA indicated there were significant main effects of measurement (p < 0.001) and task (p = 0.002), but no significant main effect of group (p = 0.798). A significant method-by-task interaction was present (p < 0.001), but no other interactions were significant (p ≥ 0.397). Follow-up paired samples t-tests indicated that, for both groups combined, absolute error of VA was significantly higher than VM for sitting (p < 0.001), playing app (p < 0.001), drawing (p < 0.001), sweeping (p = 0.005), standing (p < 0.001), and basketball (p = 0.001), whereas absolute error of VM was significantly higher than VA for slow walking (p = 0.005). There were no significant differences between measurements for the remaining tasks.
Table 2.
Mean ± SD of absolute percent error for predicting oxygen uptake (V̇O2) using developed models for Vertical Axis (VA) and Vector Magnitude (VM) accelerometer counts in adults with Down syndrome (DS) and without Down syndrome (Non-DS)
| Vertical Axis | Vector Magnitude | ||||
|---|---|---|---|---|---|
| Absolute Error (%) | Absolute Error (%) | ||||
| DS | Non-DS | DS | Non-DS | ||
| Sitting* | 74.0 ± 51.1 | 77.6 ± 71.3 | 34.4 ± 37.5 | 35.0 ± 50.1 | |
| Playing App* | 52.7 ± 47.6 | 65.2 ± 45.8 | 27.9 ± 28.2 | 29.0 ± 27.6 | |
| Drawing* | 47.2 ± 48.3 | 56.5 ± 72.7 | 26.2 ± 29.3 | 33.1 ± 46.6 | |
| Folding Clothes | 19.0 ± 11.9 | 23.8 ± 12.5 | 19.5 ± 20.7 | 19.6 ± 16.3 | |
| Sweeping* | 28.7 ± 14.3 | 34.7 ± 13.7 | 21.9 ± 29.2 | 22.3 ± 14.4 | |
| Fitness Circuit | 18.8 ± 10.2 | 19.3 ± 14.5 | 17.7 ± 11.8 | 17.6 ± 13.4 | |
| Standing* | 51.1 ± 50.1 | 45.4 ± 28.7 | 29.9 ± 31.3 | 20.3 ± 12.2 | |
| Walking PWS | 24.6 ± 32.1 | 23.5 ± 20.8 | 23.4 ± 32.0 | 22.3 ± 17.1 | |
| Walking Slow § | 18.3 ± 23.5 | 19.5 ± 13.6 | 25.7 ± 33.0 | 26.7 ± 22.2 | |
| Walking Fast | 14.7 ± 20.2 | 26.4 ± 22.9 | 16.4 ± 18.0 | 23.1 ± 19.6 | |
| Moving Box | 25.5 ± 14.6 | 18.3 ± 11.5 | 21.4 ± 18.1 | 17.3 ± 14.1 | |
| Basketball* | 28.1 ± 10.7 | 24.8 ± 11.5 | 20.4 ± 14.5 | 17.2 ± 9.5 | |
significantly higher absolute error for VA than VM (p < 0.05) in paired samples t-test for both groups combined.
significantly higher absolute error for VM than VA (p < 0.05) in paired samples t-test for both groups combined. There were no statistically significant differences between DS and Non-DS
Discussion
In this study, we examined the accuracy of VM and VA counts in estimating V̇O2 in adults with and without DS across various physical activities and sedentary behaviours. The main findings were that both VM and VA counts predicted V̇O2 in adults with and without DS; however, prediction was generally more accurate for VM than VA, especially during sedentary behaviour. These results have relevance for accelerometer-based assessment of physical activity in adults with and without DS.
Both VM and VA were individually significant predictors of V̇O2 in adults with and without DS. This agrees with a large body of previous research demonstrating that both uniaxial and triaxial accelerometer outputs are predictive of energy expenditure (Adolph et al., 2012; Agiovlasitis et al., 2011; Allred et al., 2019; Howe et al., 2009; Kelly et al., 2013; Leung et al., 2021). In the present study, the model with VM was generally more accurate than that with VA for both groups. Notably, the models for VM explained more variance than those for VA (11% and 14% more for adults with and without DS, respectively) and limits of agreement in the Bland-Altman plots were narrower for VM than VA for both groups. These findings agree with past research demonstrating that, overall, VM is a stronger predictor of energy expenditure in adults with and without DS (Howe et al., 2009; Leung et al., 2021; Yamada et al., 2009). This is logical because most movements have three-dimensional components that are likely to be captured by triaxial but not uniaxial accelerometer output. Therefore, triaxial accelerometer output may better predict the energy expenditure of activities and sedentary behaviours in people with and without DS.
The differences in the predictability of the models with VM and VA were dependent on task, as indicated by the significant method-by-task interaction for absolute error. And a closer look at the predictability of the models with VM and VA was provided by examining differences across tasks. For both adults with and without DS, the model with VM was more accurate than that with VA in estimating V̇O2 during sitting, playing an app, drawing, sweeping, standing, and basketball. These findings are consistent with previous research showing that, compared to VA counts, VM counts tend to more accurately estimate energy expenditure of activities of daily living and sedentary behaviour among adults without DS (Howe et al., 2009; Yamada et al., 2009). As it has been previously proposed, differences in the biomechanical characteristics between behaviours may be at play (Howe et al., 2009). Sedentary behaviours and standing have minimal vertical movement, so it is logical that VA counts may have lower ability to explain variance in V̇O2 compared to VM for these tasks. Furthermore, sweeping and basketball involve frequent changes in speed and direction and thus antero-posterior and medio-lateral accelerations are more likely to be captured by VM but not VA counts, resulting in better predictability of V̇O2 for the model with VM. In contrast, VA more accurately estimated V̇O2 than VM for slow walking. This finding cannot be directly explained from the present data. It is possible that VM may vary to a greater extent than VA between strides during slow walking and may thus be less reliable and less predictive of V̇O2; however, this is only a speculation that should be further examined. Overall, accelerometers measure movements with greater error at slower compared to faster walking speeds in individuals with and without DS (Agiovlasitis et al., 2016; Crouter et al., 2006; Pitchford & Yun, 2010), although this does not seem to be the case for step-counts derived from hip-worn Actigraph accelerometers when the low-frequency extension filter is utilized during data collection (Bertapelli et al., 2020). More research is needed to improve the accuracy of accelerometry in predicting physical activity intensity. In summary, the present data and those from previous investigations collectively suggest that triaxial accelerometer output is better than uniaxial in predicting the energy expenditure of physical activities and sedentary behaviours.
There were no significant differences between adults with and without DS in the prediction of V̇O2 by each of the two models. This contrasts with previous research demonstrating that VM had greater association with V̇O2 than VA during walking in adults with DS, but not in adults without DS (Leung et al., 2021). These researchers hypothesized that this was due to greater mediolateral movement during walking in people with DS than without DS (Leung et al., 2021). Indeed, past research has shown an altered gait pattern in people with DS leading to an increase in energy expenditure (Agiovlasitis et al., 2009, 2015). Unlike the research by Lueng et al. (2021) which was limited only to walking at three speeds, our study, included locomotion, household, recreational, and occupational activities, as well as sedentary behaviours. The inclusion of many tasks may have increased the ability of VM to explain variance in V̇O2 for both groups, masking any possible group differences for walking. We should consider here that accelerometers are used to provide an estimate of the degree of engaging in different intensities of physical activity in general and not for specific activities. The bottom line is that VM seems to have greater potential to predict energy expenditure than VA in adults with and without DS.
The present findings, viewed in the context of past research, have implications for accelerometer-based assessment of physical activity and sedentary behaviour in adults with and without DS. Triaxial accelerometer output seems more accurate than uniaxial in estimating energy expenditure and thus physical activity intensity in adults with and without DS; therefore, triaxial accelerometers should be the devices of preference by physical activity researchers and practitioners. Currently, there are no predictive models for estimating levels and patterns of physical activity and sedentary behaviour from large representative samples of adults with DS; the present results indicate that these models should be developed using triaxial and not uniaxial accelerometers. Importantly, predictive models should be derived from research that includes various types of physical activity and sedentary behaviour. Assessment of physical activity and sedentary behaviour is an important component of public health surveillance and provides a basis for the development of interventions to promote physical activity and health in people with and without DS.
Limitations and Strengths
This research had a set of limitations that should be considered in the evaluation of the findings. This study had a small sample size that may not be representative of all adults with and without DS. The physical activities and sedentary behaviours included in our protocol may not represent the daily living of adults with and without DS. The protocol did not include vigorous activities. Furthermore, we evaluated the V̇O2 predictive ability of VM and VA counts which are derived with proprietary algorithms, and not that of raw accelerometer data. Finally, we did not consider more modern approaches to accelerometer-based estimation of physical activity such as machine learning, Euclidean Norm Minus One, and Mean Amplitude Deviation (Staudenmayer et al., 2009; Vähä-Ypyä et al., 2015; van Hees et al., 2013).
Strengths of this study were: (1) the use of a familiarization session known to enhance data reliability in individuals with intellectual disabilities (Rintala et al., 1995); (2) the extensive practice with the protocol by the research team; (3) the inclusion of several physical activity and sedentary behaviours; and (4) the use of multi-level regression which accounts for nesting of observations within participants.
Conclusions
In conclusion, both VA and VM counts predict V̇O2 in adults with and without DS; however, overall prediction is more accurate for VM than VA counts. For this reason, VM counts should be preferred in developing accelerometer-based prediction of physical activity intensity and sedentary behaviour in adults with DS.
Footnotes
Conflict of Interest Statement
The authors declare that they have no competing interests.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, BB, upon reasonable request.
References
- Adolph AL, Puyau MR, Vohra FA, Nicklas TA, Zakeri IF, & Butte NF (2012). Validation of uniaxial and triaxial accelerometers for the assessment of physical activity in preschool children. Journal of Physical Activity and Health, 9, 944–53. 10.1123/jpah.9.7.944 [DOI] [PubMed] [Google Scholar]
- Agiovlasitis S, Beets MW, Lamberth J, Pitetti KH, & Fernhall B (2016). Accuracy of a piezoelectric pedometer in persons with and without Down syndrome. Research in Developmental Disabilities, 59, 73–9. 10.1016/j.ridd.2016.08.003 [DOI] [PubMed] [Google Scholar]
- Agiovlasitis S, Choi P, Allred AT, Xu J, & Motl RW (2020). Systematic review of sedentary behaviour in people with Down syndrome across the lifespan: A clarion call. Journal of Applied Research in Intellectual Disabilities, 33, 146–59. 10.1111/jar.12659 [DOI] [PubMed] [Google Scholar]
- Agiovlasitis S, McCubbin JA, Yun J, Mpitsos G, & Pavol MJ (2009). Effects of Down syndrome on three-dimensional motion during walking at different speeds. Gait & Posture, 30, 345–50. 10.1016/j.gaitpost.2009.06.003 [DOI] [PubMed] [Google Scholar]
- Agiovlasitis S, McCubbin JA, Yun J, Widrick JJ, & Pavol MJ (2015). Gait characteristics of adults with Down syndrome explain their greater metabolic rate during walking. Gait & Posture, 41, 180–4. 10.1016/j.gaitpost.2014.10.004 [DOI] [PubMed] [Google Scholar]
- Agiovlasitis S, Mendonca GV, McCubbin JA, & Fernhall B (2018). Prediction of energy expenditure during walking in adults with down syndrome. Journal of Applied Research in Intellectual Disabilities, 31, 151–6. 10.1111/jar.12392 [DOI] [PubMed] [Google Scholar]
- Agiovlasitis S, Motl RW, Fahs CA, Ranadive SM, Yan H, Echols GH et al. (2011). Metabolic rate and accelerometer output during walking in people with Down syndrome: Medicine & Science in Sports & Exercise, 43, 1322–7. 10.1249/MSS.0b013e31820936c4 [DOI] [PubMed] [Google Scholar]
- Agiovlasitis S, Motl RW, Foley JT, & Fernhall B (2012). Prediction of energy expenditure from wrist accelerometry in people with and without Down syndrome. Adapted Physical Activity Quarterly, 29, 179–90. [DOI] [PubMed] [Google Scholar]
- Allred AT, Choi P, & Agiovlasitis S (2019). Triaxial accelerometer output predicts oxygen uptake in adults with Down syndrome. Disability and Rehabilitation, 1–8. 10.1080/09638288.2019.1706648 [DOI] [PubMed] [Google Scholar]
- Baynard T, Pitetti KH, Guerra M, Unnithan VB, & Fernhall B (2008). Age-related changes in aerobic capacity in individuals with mental retardation: A 20-yr review. Medicine & Science in Sports & Exercise, 1984–9. 10.1249/MSS.0b013e31817fl9al [DOI] [PubMed] [Google Scholar]
- Bertapelli F, Allred AT, Choi P, Pitchford EA, Guerra‐Junior G, & Agiovlasitis S (2020). Predicting the rate of oxygen uptake from step counts using ActiGraph waist‐worn accelerometers in adults with Down syndrome. Journal of Intellectual Disability Research, 64, 602–11. 10.1111/jir.12755 [DOI] [PubMed] [Google Scholar]
- Bull MJ (2020). Down syndrome. New England Journal of Medicine, 382, 2344–52. 10.1056/NEJMra1706537 [DOI] [PubMed] [Google Scholar]
- Crouter SE, Churilla JR, & Bassett DR (2006). Estimating energy expenditure using accelerometers. European Journal of Applied Physiology, 98, 601–12. 10.1007/s00421-006-0307-5 [DOI] [PubMed] [Google Scholar]
- Howe CA, Staudenmayer JW, & Freedson PS (2009). Accelerometer prediction of energy expenditure: Vector magnitude versus vertical axis. Medicine & Science in Sport & Exercise, 2199–206. [DOI] [PubMed] [Google Scholar]
- Kelly LA, McMillan DG, Anderson A, Fippinger M, Fillerup G, & Rider J (2013). Validity of actigraphs uniaxial and triaxial accelerometers for assessment of physical activity in adults in laboratory conditions. BMC Medical Physics, 13, 5. 10.1186/1756-6649-13-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung W, Schuna JM, & Yun J (2021). Comparison of uniaxial and triaxial accelerometer outputs among individuals with and without Down syndrome. Journal of Intellectual Disability Research, 65, 77–85. 10.1111/jir.12792 [DOI] [PubMed] [Google Scholar]
- Magge SN, Zemel BS, Pipan ME, Gidding SS, & Kelly A (2019). Cardiometabolic risk and body composition in youth with Down syndrome. Pediatrics, 144, e20190137. 10.1542/peds.2019-0137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oreskovic NM, Cottrell C, Torres A, Patsiogiannis V, Santoro S, Nichols D et al. (2020). Physical activity patterns in adults with Down Syndrome. Journal of Applied Research in Intellectual Disabilities, 33, 1457–64. 10.1111/jar.12773 [DOI] [PubMed] [Google Scholar]
- Paul Y, Ellapen TJ, Barnard M, Hammill HV, & Swanepoel M (2019). The health benefits of exercise therapy for patients with Down syndrome: A systematic review. African Journal of Disability, 8, a576. 10.4102/ajod.v8i0.576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phillips AC, & Holland AJ (2011). Assessment of objectively measured physical activity levels in individuals with intellectual disabilities with and without Down’s syndrome. PLoS ONE, 6, e28618. 10.1371/journal.pone.0028618 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pitchford EA, & Yun J (2010). The accuracy of pedometers for adults with Down syndrome. Adapted Physical Activity Quarterly, 27, 321–36. 10.1123/apaq.27.4.321 [DOI] [PubMed] [Google Scholar]
- Presson AP, Partyka G, Jensen KM, Devine OJ, Rasmussen SA, McCabe LL et al. (2013). Current estimate of Down syndrome population prevalence in the United States. The Journal of Pediatrics, 163, 1163–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rafii MS, Kleschevnikov AM, Sawa M, & Mobley WC (2019). Down syndrome. Handbook of Clinical Neurology, 167, 321–36. 10.1016/B978-0-12-804766-8.00017-0 [DOI] [PubMed] [Google Scholar]
- Rintala P, McCubbin JA, & Dunn JM (1995). Familiarization process in cardiorespiratory fitness testing for persons with mental retardation. Sports Medicine Training and Rehabilitation, 6, 15–27. [Google Scholar]
- Staudenmayer J, Pober D, Crouter S, Bassett D, & Freedson P (2009). An artificial neural network to estimate physical activity energy expenditure and identify physical activity type from an accelerometer. Journal of Applied Physiology, 107, 1300–7. 10.1152/japplphysiol.00465.2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vähä-Ypyä H, Vasankari T, Husu P, Mänttäri A, Vuorimaa T, Suni J et al. (2015). Validation of cut-points for evaluating the intensity of physical activity with accelerometry-based mean amplitude deviation (MAD). PLoS ONE, 10, e0134813. 10.1371/journal.pone.0134813 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Hees VT, Gorzelniak L, Dean León EC, Eder M, Pias M, Taherian S et al. (2013). Separating movement and gravity components in an acceleration signal and implications for the assessment of human daily physical activity. PLoS ONE, 8, e61691. 10.1371/journal.pone.0061691 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yamada Y, Yokoyama K, Noriyasu R, Osaki T, Adachi T, Itoi A et al. (2009). Light-intensity activities are important for estimating physical activity energy expenditure using uniaxial and triaxial accelerometers. European Journal of Applied Physiology, 105, 141–52. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, BB, upon reasonable request.