

Abstract
Background
Active rehabilitation involving subsymptom threshold exercise combined with education and support promotes recovery in youth with concussion but is typically delivered in person, which may limit accessibility for families because of a lack of services in their communities or logistical challenges to attending in-person sessions.
Objective
This paper describes the evidence-based and theory-informed development of the Tele-Active Rehabilitation (Tele-AR) intervention for pediatric concussion, which was specifically designed for remote service delivery.
Methods
The intervention was designed by clinician-researchers with experience in pediatric concussion rehabilitation following the Medical Research Council guidance for developing complex interventions. Development involved a critical review of the literature to identify existing evidence, the expansion of the theoretical basis for active rehabilitation, and the modeling of the intervention process and outcomes.
Results
Tele-AR is a 6-week home exercise and education and support program facilitated through weekly videoconferencing appointments with a clinician. Exercise consists of low- to moderate-intensity subsymptom threshold aerobic activity and coordination drills that are individualized to participant needs and interests (prescribed for 3 days per week). Education includes the evidence-supported Concussion & You self-management program, which covers topics related to energy management, nutrition, hydration, sleep hygiene, and return to activity. Elements of self-determination theory are incorporated to support motivation and engagement. We present a logic model describing predicted intervention effects using a biopsychosocial conceptualization of outcomes after concussion.
Conclusions
The Tele-AR intervention may help to increase access to care that improves recovery and promotes a timely return to activity in youth with concussion. Future research is needed to evaluate the feasibility and efficacy of this approach.
Keywords: concussion, pediatrics, active rehabilitation, telehealth, exercise, mobile phone
Introduction
Overview
Concussion is a common injury among children and adolescents that may result in physical, cognitive, emotional, or sleep-related symptoms [1-3]. Although many youth with concussion achieve symptom resolution within 2 to 4 weeks after injury, approximately 30% continue to experience persistent symptoms beyond 4 weeks [3]. Youth experiencing persistent concussion symptoms report lower quality of life [4] and higher incidence of mental health disturbances [5] than noninjured peers.
Occupational Performance and Participation in Youth With Concussion
Occupational performance, which refers to the ability to choose, organize, and satisfactorily perform meaningful occupations [6], is often impaired in youth with concussion [7]. Qualitative studies highlight that concussion symptoms limit performance in meaningful activities such as school, physical activity or sport, and social activities [8,9]. Youth with concussion report diverse occupational performance issues in the domains of self-care, productivity, and leisure that can be improved after rehabilitation, underscoring the utility of occupational performance as a measure of functional recovery [7]. Youth may also experience limitations in participation, defined as involvement in a life situation [10]. Although activities and participation generally improve within the first few months after concussion, a substantial portion (30%-60%) of youth continue to report lower participation than their peers at 6 months after injury [10]. Continued limitations in activities and participation may lead to physical deconditioning or threats to psychological well-being, including anxiety, depression, and social isolation [11,12].
Currently, recovery from concussion among children and adolescents is being reconceptualized to emphasize resumption of everyday activities and general well-being, rather than solely the resolution of postconcussion symptoms [13]. Evaluating occupational performance can help to identify limitations and inform active rehabilitation strategies to support youth in gradual resumption of meaningful activities, thus decreasing the impact of the injury and reducing risk for persistent sequelae [14,15].
Active Rehabilitation for Youth With Concussion
Growing evidence supports an active approach to concussion rehabilitation involving guided physical activity. Several studies demonstrate the efficacy of subsymptom threshold aerobic exercise for reducing postconcussion symptoms [16-24]. Some active rehabilitation programs for youth have also included other components such as sport-specific coordination drills [25-31], balance training [32], visualization and relaxation [25-31], and education and support [25-31]. Results from these studies show that active rehabilitation reduces postconcussion symptoms and improves recovery [25-32].
The rationale for an active approach to concussion rehabilitation has been rooted in the benefits of physical exercise to promote biological recovery (ie, improve cerebrovascular autoregulation and increase neuroplasticity) and psychological well-being (ie, increase self-efficacy and improve mood) [28,33-35]. To date, outcome measurement has predominantly focused on changes in postconcussion symptoms [36]. However, evidence indicates that although concussion symptoms initially arise because of physiological changes, including metabolic and cerebral autoregulatory dysfunction, the strength of the relationship between the neurobiology of the injury and ongoing symptom experience diminishes over time, with noninjury factors playing an important role in the persistence of symptoms [37]. Recovery from concussion is therefore best understood through a biopsychosocial model in which psychological and social factors, including activity restriction, emotional reaction, and coping styles, interact with biological factors to maintain symptoms and functional limitation after concussion [13,38-40]. Accordingly, an active rehabilitation approach should aim to restore performance in daily activities in addition to reducing postconcussion symptoms.
The theoretical model of active rehabilitation described by Gagnon et al [28] endorses a biopsychosocial perspective by emphasizing the physiological, psychological, and social benefits of controlled exercise in combination with education and motivation. However, although the biopsychosocial model helps to identify targets for intervention, it does not address how to support motivation, which is an important determinant of outcomes in pediatric rehabilitation [41] and is often reduced after brain injury [42]. Motivation is particularly important during active rehabilitation because the intervention typically involves a home program that youth complete independently. Extending the theoretical rationale for active rehabilitation could help to guide how to promote motivation and further address the impact of such interventions on performance of daily activities and general well-being.
Barriers to Accessing Active Rehabilitation
To date, active rehabilitation has typically been conducted through in-person sessions at a specialty clinic or research facility [27,28,30,31]. However, access to specialty health care is often limited for youth in Canada because of a lack of specialty services in their geographic region, as well as financial and logistical barriers to parental accompaniment [43,44]. Telerehabilitation has emerged as an effective method of service delivery that may address challenges in access. In a systematic review, clinical outcomes from telerehabilitation were found to be similar to, or better than, those from traditional in-person interventions for a variety of conditions [45]. Measures of clinical process, including attendance, compliance, and satisfaction, were also generally high [45]. Among youth, reviews highlight telerehabilitation as an appropriate method of service delivery [46,47] that may be especially effective when targeting behavioral function using a coaching approach and exercise program [46]. The role of telemedicine in concussion care is currently expanding [48,49] but has yet to be explored in the delivery of an active rehabilitation intervention.
This paper describes the evidence-based development of, and theoretical rationale for, the Tele-Active Rehabilitation (Tele-AR) intervention for youth with concussion, which was specifically designed to promote return to activity in a remote service delivery format. A detailed overview of the intervention is also provided.
Methods
Ethical Approval
This study was approved by the University of Toronto Health Sciences Research Ethics Board (REB reference number 00039179). Participants provided informed written consent to participate in the study.
Intervention Development Process
The Tele-AR intervention was designed by a team of clinician-researchers (kinesiologists and occupational therapists) with experience in pediatric concussion rehabilitation, based on clinical experience and a critical review of published literature. The Medical Research Council (MRC) framework for developing and evaluating complex interventions [50,51] guided the development process.
According to the MRC framework, intervention development is an iterative process involving integration of current evidence and appropriate theory, followed by a phased testing approach involving a series of pilot studies before a definitive evaluation [50]. The development stage involves the following three key processes: (1) identifying the existing evidence base, (2) identifying or developing appropriate theory, and (3) modeling process and outcomes.
Key Tasks
We drew on guidance from Campbell et al [52] and Faes et al [53] regarding key tasks for each of the MRC development processes. According to Campbell et al [52], existing evidence should be used to develop an understanding of the problem and target context to identify opportunities for intervention. Key tasks include defining and quantifying the target population most likely to benefit, defining the health outcome and appropriate measures, understanding pathways that cause and sustain the problem, identifying similar interventions, and predicting barriers or design challenges [53]. Integrating appropriate theory involves specifying theory-based determinants of change and describing how the intervention will affect them [53]. Finally, the development of a conceptual or logic model is recommended to define intervention components and clarify anticipated mechanisms linking components to desired targets for change [52]. Textbox 1 shows the application of the MRC framework and key tasks to development of the Tele-AR intervention.
Application of key tasks from the Medical Research Council framework to the development of the Tele-Active Rehabilitation intervention.
Identifying existing evidence
-
Define and quantify target population
Review of concussion epidemiology among youth
Project team consultation to determine target population
-
Define health outcome and outcome measures
Review of current consensus definition of recovery from concussion
Identification of appropriate measurement tools
-
Understand factors that cause and sustain the problem
Review of factors that influence concussion recovery in youth
Identification of existing biopsychosocial models of concussion
-
Identify similar interventions
Critical review of literature pertaining to active rehabilitation interventions for youth with concussion
Review of best practice recommendations for telerehabilitation and telehealth self-management interventions
-
Define target context
Review of guidelines for telemedicine in concussion management
Identifying appropriate theory
Review of existing theoretical rationales for active rehabilitation
Review of health behavior change theories
Integration of health behavior change theory in the intervention
Modeling process and outcomes
Project team consultation to design intervention components
Development of logic model to describe anticipated effects of intervention components
Results
Developing the Intervention
Results from the development stage are described in the following sections, organized according to the MRC headings and key tasks identified in the Methods section.
Identifying Existing Evidence
Define and Quantify Target Population
The Tele-AR intervention targets adolescents (aged 13-17 years) who continue to experience symptoms at least 2 weeks after concussion. All mechanisms of injury are considered, including sport, falls, and motor vehicle accidents.
In recent decades, health care usage for pediatric concussion has increased substantially in Canada [1] and the United States [54]. In Ontario, this increase has been most pronounced among adolescents [1], for whom the average annual incidence of physician-diagnosed concussion was approximately 1500 per 100,000 from 2008 to 2016 [55]. Adolescents are also known to be at high risk for prolonged recovery [56]. According to a Canadian multicenter prospective study, a substantial subset of adolescents, approximately 30%, continue to experience symptoms beyond 1 month after concussion [3], which may lead to mood disturbances [5], reduced quality of life [4], and impaired activity performance [7]. Results from the same multicenter study also indicate that symptom improvement occurs primarily within the first 2 weeks of injury and levels off 2 to 4 weeks after injury [57]. Exercise-based active rehabilitation programs initiated in the subacute phase of recovery (1-2 weeks after injury) are feasible and may reduce the risk of persistent symptoms [19,20,24,26]. The Tele-AR intervention therefore targets adolescents continuing to experience symptoms beyond 2 weeks after concussion who are at risk for developing secondary consequences related to mood, activity performance, and quality of life.
Define Health Outcome and Outcome Measures
Primary health outcomes for the Tele-AR intervention include postconcussion symptoms and perceived occupational performance, a measure of performance in daily activities.
The most recent (2016) international consensus statement on sports-related concussion defines recovery as the resolution of concussion symptoms and return to normal activities, including school, work, and sport [2]. Self-reported concussion symptoms remain the most common measure of recovery from concussion [58] and are measured in adolescents using an age-appropriate symptom scale such as the Postconcussion Symptom Inventory [59]. However, there is growing recognition that symptom reports do not always accurately reflect recovery [13]. Concussion-like symptoms (eg, fatigue, headache, and dizziness) are common in individuals without a history of concussion, and symptom reporting is influenced by a variety of noninjury factors such as personality, comorbid mood disorders, and familial factors [12]. Activity limitations are common among adolescents with concussion [7-9]; therefore, a measure of performance in daily activities (ie, occupational performance) is beneficial for evaluating recovery. The Canadian Occupational Performance Measure has been identified as a useful tool for measuring functional recovery among youth participating in active rehabilitation [7]. Concurrent measurement of symptoms and occupational performance can provide a more complete assessment of recovery than symptom reduction alone.
Factors That Cause and Sustain the Problem
Current evidence indicates that persistent symptoms and activity limitations after concussion are best understood through a biopsychosocial perspective [38,39,60]. A key tenet of the biopsychosocial model is that the interaction among biological, psychological, and social factors determines health outcomes and that these factors must therefore not be addressed in isolation [61].
Biological or physiological factors after concussion include autonomic nervous system and cerebral autoregulatory dysfunction [35], impaired balance and coordination [62], visual and vestibular dysfunction [63], sleep disturbances, and fatigue [64]. Exercise intolerance, which reflects autonomic and cerebrovascular dysfunction, is a prognosticator of recovery [65], as are visual and vestibular dysfunction [63].
There is growing recognition that psychological mechanisms related to cognitive, behavioral, and emotional reactions to concussion influence outcomes [39]. Negative illness perceptions, including beliefs about injury timelines, consequences, and level of control, are associated with poor outcomes [60,66]. Various cognitive biases may precipitate negative illness perceptions, including causal misattribution (ie, misattribution of common benign symptoms to concussion), catastrophizing (ie, misinterpretation of symptoms as dangerous), good-old-days bias (ie, tendency to overestimate preinjury health or function), and the nocebo effect (ie, concussion outcomes shaped by the expectations of illness or dysfunction after the injury) [39]. Negative illness perceptions often lead to maladaptive coping behaviors such as fear avoidance (ie, fear of provoking symptoms leads to avoidance of activities), endurance (ie, pushing through symptoms), or all-or-nothing behavior (ie, alternating between periods of extremely low and extremely high levels of activity) [60,67]. Emotional responses such as stress, anxiety, and depression can result from, or reinforce, negative perceptions and behaviors and have been shown to influence outcomes [68]. In youth, self-efficacy is also reduced after concussion [69], and lower levels of self-efficacy predict greater symptom burden [70]. Cognitive, behavioral, and emotional factors interact to form vicious cycles that maintain the experience of symptoms and functional limitation.
The social influences of concussion are poorly understood. Adolescents with concussion report limitations in school function and social activities [7-9]. Qualitative studies show that concussion has adverse effects on the interpersonal relationships of youth and that the influence of relationships on recovery can be positive or negative [8,71]. In the study by Kita et al [72], female adolescents with concussion identified their friends, parents, clinicians, and peers with personal histories of concussion as key providers of social support that mitigates various challenges in their recovery. Among collegiate athletes, greater satisfaction with social support has been associated with lower postconcussion anxiety [73].
Access to appropriate clinical care may influence how these biological, psychological, and social factors are experienced by the individual and, in turn, their effects on recovery. A systematic review found several studies showing that earlier initiation of clinical care after concussion leads to quicker recovery [74]. Timely access to care allows for early initiation of supervised subsymptom threshold aerobic exercise [33,34]. Conversely, those without guidance may continue to rest until achieving spontaneous symptom resolution, which increases their risk for physical deconditioning and mood disturbances [11,12] or for engaging in levels of activity that may be harmful for recovery. Early education and reassurance from a health care provider can reduce unfavorable psychological responses to injury [75], whereas poor access to care may itself contribute to negative injury perceptions. Communication with a health care provider can also build the capacity of youth to seek social support by providing information about appropriate school accommodations, helping youth to communicate the nature of their injury and encouraging youth to engage those around them to support their recovery [72].
There are currently significant challenges to accessing timely appropriate care for concussion in Canada [49]. Studies have identified knowledge gaps regarding concussion management among primary care providers [76,77]. Access to specialized concussion care is also limited in Canada, especially among individuals in remote communities who may experience significant geographic or socioeconomic barriers and youth who are reliant on caregiver accompaniment. Studies from the United States reveal barriers to accessing pediatric concussion care among families in rural communities, including higher health care expenses [78] and indirect costs related to transportation and lost productivity [79]. Delayed access to care is problematic because it increases the risk of premature return to activity and potential reinjury or development of persistent symptoms and functional limitation.
Identifying Similar Interventions
A critical review of the literature describing active rehabilitation approaches to concussion was performed in the fall of 2019. Key articles were located through search in Google Scholar and PubMed using keywords that included active rehabilitation, exercise, physical activity, concussion, mild traumatic brain injury, youth, and adolescents. Additional pertinent literature was identified through forward and backward searching of reference lists as well as literature previously known to the authors. Intervention characteristics among the studies included in the review are detailed in Multimedia Appendix 1 [7,16-21,24-30,32,80] and briefly summarized in the following paragraphs.
Findings from the review indicated that active rehabilitation interventions typically last 6 weeks and involve a variety of components, including aerobic exercise [7,16,19,20,24-30,32,80-84], sport coordination drills [25-30,32,80,82,83], balance training [32], visualization or relaxation [25-30,80-83], and education and support [25-30,80-83]. The 6-week timeline was established by Gagnon et al [29], who found that a mean intervention duration of 4.4 (SD 2.6) weeks was required to achieve symptom resolution. All the studies identified implemented individual interventions. Active rehabilitation has typically been evaluated through changes in postconcussion symptoms [16-18,24-30,32,82,84]. Improved mood [29,30,80], quality of life [17,30], and occupational performance [7] have also been reported.
Although key components are not fully understood, a study of multimodal active rehabilitation found that youth identified the education, aerobic exercise, and sport coordination drills as most helpful [81]. A combination of education regarding energy management and engagement in supervised physical activity is therefore essential to the approach [81]. Future iterations of active rehabilitation should consider a focus on self-management through education and supervised physical activity involving aerobic and coordination exercise.
Published active rehabilitation interventions typically involve a home exercise program performed several (3-7) days per week and weekly appointments with a clinician. Appointments have occasionally been conducted by telephone [17,31,32], which was reportedly appreciated by participants because the telephone appointments reduced travel requirements [17]. The identified studies required participants to attend in-person appointments for pre- and postintervention assessments, indicating an opportunity to explore interventions designed to be delivered entirely remotely and requiring no in-person appointments.
Systematic reviews of telerehabilitation [45-47] and remote self-management programs [85,86] were consulted to identify best practice recommendations regarding the remote service delivery model for the Tele-AR intervention. Consistent communication with a health care provider was identified as key to promoting retention and positive outcomes among remotely delivered self-management interventions [85]. Ongoing individualized education, lifestyle intervention, adherence support, and clinical review with feedback were also identified as important components [86].
The aforementioned literature provided the foundations for the design of the Tele-AR intervention. On the basis of this literature, it was determined that the intervention should be a 6-week program comprising aerobic exercise, coordination drills, and comprehensive individually tailored education and support to train self-management skills. Telehealth literature indicated that weekly appointments should involve a review of symptoms and activity performance with provider feedback, continued education regarding symptom management strategies, and support to promote motivation and adherence to the home program [85,86].
Defining Target Context
Tele-AR could be an accessible intervention to reduce the burden of pediatric concussion, especially among those identified as high risk for prolonged recovery [3]. It complements ongoing telemedicine initiatives to improve access to pediatric concussion care in rural and remote Canadian communities [48,49].
Recommendations for the use of telemedicine in concussion management specify the need for initial in-person medical assessment to confirm the diagnosis of concussion as well as regular medical follow-up [49,87]. Tele-AR is therefore designed to serve as an adjunct intervention for youth who have previously undergone in-person medical assessment and continue to receive medical follow-up, including appropriate referral for targeted treatments such as cervical or vestibular therapy. Although there is evidence that earlier initiation of supervised exercise (after 24-48 hours of initial rest) leads to quicker recovery [88], many without access to care continue to rest until symptom resolution, which may contribute to delayed recovery [12]. Remote delivery of active rehabilitation could increase access to care that enables earlier resumption of supervised physical activity and contributes to quicker recovery.
Identifying and Applying Theory
Supporting Motivation During Active Rehabilitation
We drew on self-determination theory (SDT) to expand the theoretical foundation for active rehabilitation to address motivation, a key determinant of engagement and outcomes in rehabilitation [41,89]. Motivation is a key facilitator of participation after childhood traumatic brain injury [90] but is often reduced among individuals with a brain injury [42]. Existing theoretical underpinnings of active rehabilitation recognize the importance of motivation [28] but do not address how to promote motivation.
SDT has been identified as a useful framework for conceptualizing motivation in pediatric rehabilitation [41]. SDT is a theory of human motivation that describes the influence of social and cultural factors on an individual’s sense of volition (self-determination), performance, and well-being [91]. According to SDT, three psychological needs foster intrinsic motivation: competence (feeling mastery and success), autonomy (feeling of being able to choose one’s own actions), and relatedness (feeling positive relationships with others) [91]. Systematic reviews demonstrate that health interventions designed using SDT can increase satisfaction of psychological needs, leading to improvements in physical and mental health outcomes [91,92]. Previous articles have highlighted the utility of SDT to identify factors that influence motivation during brain injury rehabilitation [42]. In adults, mild traumatic brain injury reduces fulfillment of psychological needs, suggesting that rehabilitation should address these variables [93].
The Tele-AR intervention is designed to support the 3 psychological needs outlined in SDT to promote motivation and engagement in the program and regular daily activities. Each element is briefly described in the following sections. Table 1 provides examples of how the psychological needs are addressed in the Tele-AR intervention, using the SDT taxonomy from Teixeira et al [94].
Table 1.
Self-determination theory (SDT) strategies in the Tele-Active Rehabilitation (Tele-AR) intervention.
| SDT strategy | Application to Tele-AR intervention | |
| Autonomy support | ||
|
|
MBCTa 1: Elicit perspectives on condition or behavior |
|
|
|
MBCT 3: Use noncontrolling, informational language |
|
|
|
MBCT 5: Providing meaningful rationale |
|
|
|
MBCT 6: Provide choice |
|
| Relatedness support | ||
|
|
MBCT 8: Acknowledge and respect perspectives and feelings |
|
|
|
MBCT 9: Encourage asking questions |
|
|
|
MBCT 10: Show unconditional regard |
|
|
|
MBCT 11: Demonstrate interest in the person |
|
|
|
MBCT 12: Use empathic listening |
|
|
|
MBCT 13: Provide opportunities for ongoing support |
|
|
|
MBCT 14: Prompt identification and seek available social support |
|
| Competence support | ||
|
|
MBCT 15: Address obstacles to change |
|
|
|
MBCT 17: Assist in setting optimal challenge |
|
|
|
MBCT 18: Offer constructive, clear, and relevant feedback |
|
|
|
MBCT 19: Help develop a clear and concrete plan of action |
|
|
|
MBCT 20: Promote self-monitoring |
|
|
|
MBCT 21: Explore ways of dealing with pressure |
|
aMBCT: motivation and behavior change technique (according to the self-determination theory taxonomy developed by Teixeira et al [94]).
Competence
The Tele-AR intervention aims to promote a sense of competence by helping adolescents set optimal challenges and increase self-efficacy. This involves gradually increasing experiences of success through participation in school, exercise, and other meaningful activities. An action plan is developed with each participant to identify how they will implement strategies to support recovery (eg, energy management and relaxation). Second, participants are taught to self-monitor exertion during activities to prevent significant symptom exacerbation. They are encouraged to monitor the time during which they engage in activities such as schoolwork and screen use to facilitate gradual progression. Third, the clinician provides feedback and encouragement during appointments using a strengths-based approach, whereby participants are prompted to discuss what has gone well and which strategies they used to support success. An opportunity is provided for participants to identify barriers they are encountering and explore potential solutions with the clinician. Finally, strategies are discussed for dealing with stressful situations that could undermine competence, such as relaxation techniques (eg, deep breathing, muscle relaxation, and visualization) and seeking help.
Autonomy
Autonomy is supported by providing meaningful rationales for active rehabilitation, integrating participant perspectives in program development, and providing choice. The rationale for the active rehabilitation approach is explained to participants at the beginning of the intervention. Education is provided using nonjudgmental language integrating participant perspectives and emphasizing freedom of choice (ie, which strategies to use and how to use them). Participants are engaged in coconstructing the home program based on their needs and interests, including choice about specific exercises. The Tele-AR intervention is designed to empower youth to take responsibility for their recovery through self-management and coping skills. In a previous study, parents reported that active rehabilitation helped their children become more accountable for their recovery by teaching them to self-monitor their condition [81]. Remote service delivery may further enhance the accountability of youth by eliminating the need for parental accompaniment to appointments.
Relatedness
Relatedness (ie, feeling positive relationships with others) is fostered by the clinician through active listening, expressing empathy, and encouraging perspectives and questions from the participant. Studies from a variety of rehabilitation disciplines, including physiotherapy [95], occupational therapy [96], and psychology [97], demonstrate that therapeutic alliance can be developed effectively through videoconferencing. Weekly appointments foster a strong therapeutic relationship, which has been shown to influence adherence to home exercise programs [98]. In addition, the clinician encourages social support seeking from parents, teachers, coaches, and friends using strategies identified by Kita et al [72]. For example, because of the invisible nature of concussion, some adolescents report being called “fakers” by peers [9]. Participants may therefore be taught metaphors to help communicate their invisible injury, such as comparing energy levels to a cellphone battery [72]. Participants are also encouraged to involve friends in the exercise program where possible, such as having a friend join their walk or including a teammate in sport-specific coordination drills.
Modeling Process and Outcomes
Modeling aims to define intervention components, explain how they relate to each other, and describe the mechanism through which they influence desired intervention outcomes [51]. Figure 1 presents a logic model for the Tele-AR intervention. It describes the predicted effects of intervention components (ie, aerobic exercise, coordination drills, and education and support) based on the review by Gagnon et al [28] and published biopsychosocial models of concussion [38,39]. Descriptions of anticipated outcomes from each intervention component are provided in the following paragraphs.
Figure 1.
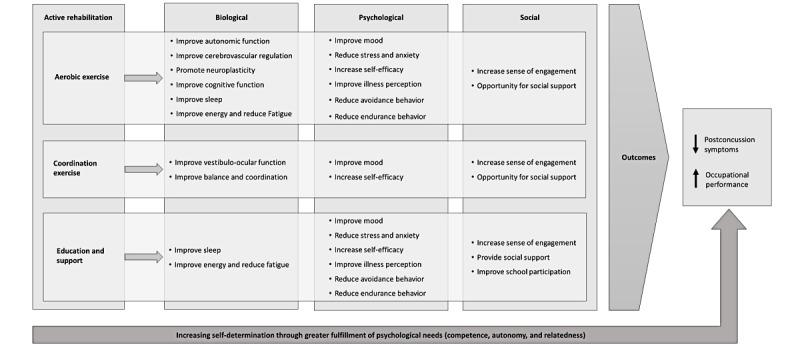
Logic model for the Tele-Active Rehabilitation intervention.
Several reviews demonstrate the efficacy of aerobic exercise for reducing postconcussion symptoms [22,23]. Progressive subsymptom threshold aerobic exercise improves autonomic function and cerebral blood flow regulation, which are impaired after concussion [33-35]. Aerobic activity also facilitates neurological recovery by promoting neuroplasticity [99]. Cardiovascular fitness improves with aerobic training, which can reduce fatigue and improve energy levels [100]. The psychological benefits of aerobic activity include stress reduction, elevated mood, and increased self-efficacy [101]. Supervised exercise may also reduce avoidance and endurance behaviors, both associated with poor outcomes [67]. Graded and supervised subsymptom threshold aerobic exercise builds mastery experiences that challenge catastrophic assumptions about symptoms and activity, which may improve illness perception and reduce activity avoidance [17]. Teaching those who display endurance behavior to monitor exertion during exercise also supports pacing strategies that facilitate activity performance [15]. For individuals who are experiencing restrictions after concussion, exercise can provide a sense of engagement in meaningful activity and create opportunity for social connection [38,81].
According to Gagnon et al [28], the purpose of coordination exercises is to continue light exercise and reintroduce familiar activities in a successful context to improve mood and increase self-efficacy. Allowing choice in coordination exercises enables youth to participate in familiar meaningful activities. A previous study found that youth enjoy the coordination drills because they allow for gradual reintroduction of meaningful activities and help improve overall fitness [81]. These exercises may also target deficits in balance, coordination, and visual function that may occur after concussion [2]. Finally, sport-specific coordination training provides an opportunity for social connection because participants may complete the drills with a friend or teammate.
Education and support are essential components of concussion management consistently recommended among evidence-based guidelines [102]. Education about the nature of concussion and recovery timelines addresses important psychological variables that predict recovery, such as illness perception [66]. Energy management and sleep hygiene strategies may reduce fatigue and improve energy levels [81]. A cohort of youth who participated in active rehabilitation identified energy management as a key component, which parents believed improved their child’s self-management [81]. Providing support and training in coping strategies may also reduce anxiety and emotional distress, which are common after concussion and predict poor outcomes [66]. Helping youth to identify appropriate accommodations and return-to-learn strategies can improve school participation and has been identified by families as a priority service need [103]. Families may also require assistance modifying other activities to support a gradual return, such as playing an instrument or spending time with friends [7]. Ultimately, education and support may increase self-efficacy for activity performance after concussion, which has been associated with lower symptom severity in children and adolescents [70].
As described in the Identifying and Applying Theory section, the Tele-AR intervention is designed to foster satisfaction regarding competence, autonomy, and relatedness to strengthen motivation and self-determination. Fulfillment of these needs is believed to support participation in the program. It is also hypothesized that increased self-determination through active rehabilitation will directly contribute to symptom reduction and improved occupational performance.
Tele-AR Intervention
Intervention Overview
The Tele-AR intervention is a 6-week home program facilitated through weekly videoconferencing appointments with a rehabilitation clinician (kinesiologist, occupational therapist, or physical therapist). It consists of (1) aerobic exercise, (2) sport coordination drills, and (3) comprehensive concussion education and support. The following sections provide a detailed description of the intervention.
Intervention Timeline
Figure 2 presents an overview of the timeline for the Tele-AR intervention. It begins with assessment and program introduction spread over 2 appointments, each lasting for 1 hour. The first appointment is dedicated to completing the informed consent procedures for the research study and preintervention assessments (see the Assessment section). The second appointment consists of a participative concussion education session and collaborative coconstruction of the home program, integrating the participant’s individual needs and interests within the three components (aerobics, coordination drills, and education and support).
Figure 2.
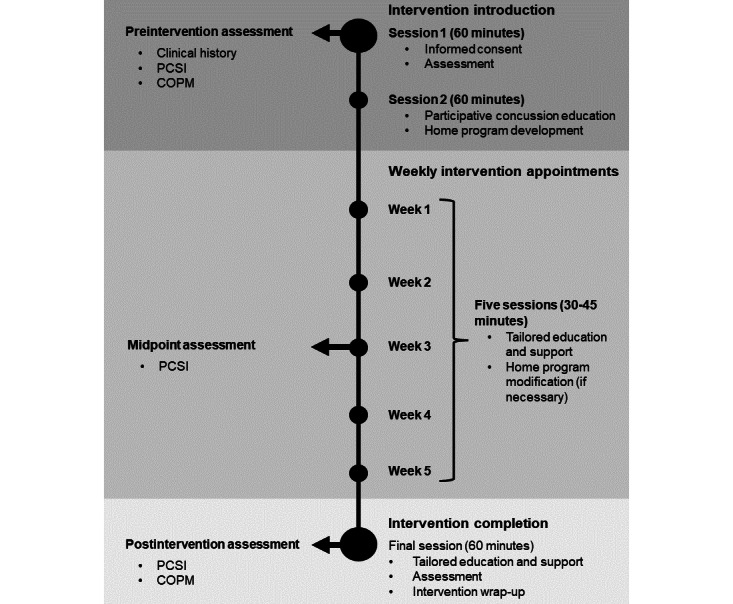
Overview of the Tele-Active Rehabilitation intervention. COPM: Canadian Occupational Performance Measure; PCSI: Postconcussion Symptom Inventory.
During weeks 1 to 6, participants are asked to perform the home exercise program 3 days per week and meet with the research clinician once per week. The purpose of weekly appointments is to provide continued education and support, modify the exercise program as appropriate, and strengthen motivation for engaging in the home program and other daily activities. The week 3 appointment includes symptom reassessment to evaluate interim changes. Significant deterioration at this point could indicate a need for in-person reassessment or referral to other providers [87]. Postintervention assessment occurs in week 6.
Assessment
Preintervention assessment is conducted through a clinical interview with youth and their parents during the first appointment and is used to inform home program prescription. Assessment is repeated in week 6 to evaluate postintervention changes.
Assessment is intentionally targeted to ensure clinical application. It includes clinical history of injury details and factors known to affect recovery (eg, concussion history, medical and mental health history, and social history [3,58]), self-reported symptom rating (Postconcussion Symptom Inventory [59]), and self-perceived occupational performance, a measure of performance in daily activities (Canadian Occupational Performance Measure [104]). These measures reflect current understanding of concussion recovery and call for patient-reported outcome measures in concussion rehabilitation that focus on function and well-being [13,105].
Intervention Components
Overview
The Tele-AR intervention comprises the following components: (1) aerobic exercise, (2) sport coordination drills, and (3) comprehensive concussion education and support. Components are individually tailored to the specific needs of each participant. The exercise program is prescribed for 3 days per week to promote compliance by minimizing disruption to daily activities and to allow for comparison between days with and without exercise. Imhoff et al [32] showed that 3 sessions per week is sufficient to facilitate symptom reduction and was associated with high treatment adherence. A description of each component is provided in the following sections.
Aerobic Exercise
After initial assessment, each participant is prescribed aerobic exercise beginning with 10 minutes of low-intensity activity at level 4 (Just feeling a strain) on the Pictorial Children’s Effort Rating Table (PCERT) [106]. Aerobic exercise may be completed on an exercise machine (treadmill, stationary bike, or elliptical trainer), indoor track, or outdoor space, depending on resources available. Participants are instructed to terminate exercise and rest upon symptom exacerbation (see Safety section); the time to symptom exacerbation becomes the new target duration. Exercise duration and intensity are progressed during weekly appointments if symptoms are well tolerated, following the standardized protocol presented in Table 2.
Table 2.
Aerobic exercise progressiona protocol.
| Week | Duration (minutes) | Intensity (PCERTb level) |
| 1 | 10 | 4 |
| 2 | 15 | 4 |
| 3 | 15 | 5 |
| 4 | 20 | 5 |
| 5 | 20 | 6 |
| 6 | 30 | 6 |
aProgression was only recommended if significant symptom exacerbation did not occur in the previous week.
bPCERT: Pictorial Children’s Effort Rating Table.
The initial aerobic prescription (10 minutes, PCERT level 4) is based on the time to symptom exacerbation reported by Gagnon et al [28] and Dobney et al [26] among youth initiating active rehabilitation. This prescription is consistent with other study protocols [31,107], as well as recommendations from literature reviews and clinical guidelines for exercise after concussion [108,109]. Previous studies demonstrate the utility of perceived exertion as a method for prescribing exercise to youth with concussion [32,110]. The PCERT is a validated tool for assessing effort perception in youth [106] and has been used previously to facilitate the home program in active rehabilitation [26,29-31].
Coordination Drills
Coordination drills are individualized based on participant interests and preintervention assessments. They may target balance, coordination, sport-specific skills, or general health exercises. For example, a basketball player may be given shooting drills first performed stationary and progressed to include dynamic movement. Coordination exercises are performed for up to 10 minutes at the same intensity as the aerobic component and are also terminated at the onset of any new or worsening symptoms. Participants are provided with written instructions outlining the details of their home exercise program.
Education and Support
Individualized education and support regarding symptom management and return to activity are provided to participants throughout the intervention. The education curriculum is based on the evidence-supported Concussion & You self-management program [111], which covers topics that include energy management, relaxation, nutrition, hydration, sleep hygiene, and return to school and sport. Education material is delivered through a participative session and reviewed weekly with specific application to challenges experienced by participants in their daily life. Participants are also provided with the Concussion & You education handbook [112] to consolidate information.
Technology
Appointments in the Tele-AR intervention are conducted through real-time videoconferencing using a secure platform that meets health privacy standards and allows for collaboration features such as screen sharing. The clinician uses a standard laptop or desktop computer, and participants may engage in the videoconferencing appointments using a computer, tablet, or smartphone.
Videoconferencing is believed to facilitate therapeutic rapport and is the most common method of communication in telerehabilitation for children [46]. Mental health support for youth is acceptable and effective when delivered through videoconferencing [113], and a study in adolescents with concussion found similar ratings of therapeutic alliance and satisfaction between face-to-face and video telehealth visits [114]. Although some individuals with concussion experience screen sensitivity, current evidence does not indicate that strict avoidance of screens improves recovery [115], supporting instead an individualized approach to screen use within tolerable limits. Other screen-based interventions for concussion have been tolerated well, with no screen sensitivity issues reported [116,117]. Subsequent feasibility testing of this intervention will assess participant perceptions and experiences engaging in video-based appointments.
Safety
Special attention must be paid to ensure safety in telehealth interventions. Safety considerations for the Tele-AR intervention are summarized in Textbox 2.
Safety considerations for the Tele-Active Rehabilitation intervention.
Symptom exacerbation considerations
Education regarding activity-related symptom exacerbation and appropriate response
Participants instructed to terminate exercise and rest upon significant symptom exacerbation (an increase of ≥3 points on a 10-point visual analog scale)
Suspension of exercise program pending medical clearance if symptom exacerbation occurs during 3 consecutive sessions despite exercise modification
Participants instructed to contact the research team in the event of exercise-induced symptom exacerbation that does not subside within 24 hours of rest or exercise-induced symptom exacerbation during consecutive exercise sessions
Exercise safety considerations
Preparticipation screening of contraindications to exercise
Ensuring an open space for exercise free from tripping hazards
Advising on use of support for balance (if needed)
Considering parental supervision during exercise sessions
General telehealth considerations
Confirming participant location, emergency contact information, and alternative methods of communication before appointment commencement
Development of safety protocol in case of acute medical or mental health emergency
Education regarding activity-related symptom exacerbation and the appropriate response is provided during program prescription. Evidence suggests that activity-related symptom exacerbations are transient and not detrimental to recovery [118]. Exercise-related symptom exacerbation generally resolves within 1 hour of rest [17,25,26]. Participants are instructed to terminate exercise upon significant symptom exacerbation, which is operationalized according to the definition from Leddy et al [119] as an increase of ≥3 points on a 10-point visual analog scale (VAS) [119]. Participants are familiarized with the Wong-Baker FACES pain rating VAS for symptoms [119]. The VAS is used by participants to rate their current overall symptom experience before exercise and monitor for any increase during the activity. Participants are instructed to contact the research team if any of the following occurs: (1) exercise-induced symptom exacerbation that does not subside within 24 hours of rest, (2) exercise-induced symptom exacerbation experienced during consecutive exercise sessions, and (3) the participant has concerns about exercise. In these scenarios, the research team provides appropriate support, discusses potential exercise program modification, and considers referral to the primary care provider or other providers. The stopping rule described by Dobney et al [26] is used, whereby the exercise program is suspended if symptom exacerbation occurs during 3 consecutive sessions despite exercise modification.
Discussion
Contributions
In this paper, we describe the development and theoretical foundation of the Tele-AR intervention for youth with concussion, specifically designed for remote service delivery. Development was guided by the MRC framework for complex interventions, involving the integration of existing evidence with appropriate theory [50]. Although growing evidence supports an active approach to concussion rehabilitation involving closely monitored progressive exercise combined with education and support, families often face several barriers that limit engagement in such care. The Tele-AR intervention was created to address these barriers. Intervention development is an iterative process, and results from an ongoing mixed methods feasibility study will inform further improvements.
The Tele-AR intervention builds on previous work advocating for a holistic approach to concussion care that emphasizes function and general well-being [13]. It is among the first interventions designed to improve activity and participation among youth with concussion [120]. Components are designed to concurrently address biological, psychological, and social aspects of concussion in a remote service delivery format. We emphasize education and support as essential to the intervention and expand the notion of active rehabilitation to facilitate motivation and performance in activities that are meaningful to the individual.
Further Study
The logic model presented here requires further study. Evaluating changes in identified biopsychosocial constructs may improve clinical delivery of active rehabilitation. Continued efforts to reconceptualize recovery from concussion through a biopsychosocial lens with an emphasis on function and participation may also identify new targets for change in rehabilitation and inform a stronger theoretical framework [13]. The qualitative exploration of youth and parent perspectives regarding perceived needs from the Tele-AR intervention is addressed in the feasibility study, and it will help refine intervention components and delivery.
The development process involved extensive review of the literature to integrate current evidence. However, the literature review methodology was not systematic and thus may be subject to selection bias or missed publications. In addition, most of the literature was reviewed before the COVID-19 pandemic when telehealth use and scholarship rapidly increased. Given the breadth of active rehabilitation approaches described in the literature and rapid growth of research in this field, future work using a more intentional review methodology and original investigation is warranted to determine optimal intervention approaches. All studies identified in the review implemented individual interventions. Group interventions may foster a greater sense of relatedness and social support and should be explored in this population.
Conclusions
Tele-AR complements ongoing telemedicine initiatives to improve access to concussion care [49] and may represent an accessible proactive intervention for those identified as high risk for prolonged recovery. The literature reviewed here may also be helpful to clinicians and families of youth with concussion to inform remote care during the COVID-19 pandemic. Research to evaluate the feasibility of this intervention is underway, and if warranted, more rigorous study should be undertaken to determine intervention effects and contribute to identifying best practices for telehealth concussion services that support youth in a timely return to activity.
Acknowledgments
This research was supported by the Canadian Institutes of Health Research (Frederick Banting and Charles Best Canada Graduate Scholarship Master’s Awards), Ontario Graduate Scholarship, and the Hilda and William Courtney Clayton Pediatric Fund. The authors thank the Outcomes, Advocacy and Knowledge (OAK) Concussion Lab team (University of Toronto) for their assistance in preparing this manuscript.
Abbreviations
- MRC
Medical Research Council
- PCERT
Pictorial Children’s Effort Rating Table
- SDT
self-determination theory
- Tele-AR
Tele-Active Rehabilitation
- VAS
visual analog scale
Intervention characteristics among studies included in the review.
Footnotes
Conflicts of Interest: NR is a holder of a Canada Research Chair (Tier 2) in Pediatric Concussion and reports receiving grants and research funding from the Canadian Institutes of Health Research, Ontario Neurotrauma Foundation, Public Health Agency of Canada, Parachute Canada, Special Olympics Canada, Greater Toronto Hockey League, Dr Tom Pashby Sport Safety Fund, Holland Bloorview Kids Rehabilitation Hospital, and Scotiabank. NR is an investigator in a multicenter study funded by the National Football League Scientific Advisory Board; NR does not receive any research funding or financial benefit. NR is a minority shareholder in 360 Concussion Care, an interdisciplinary concussion clinic.
References
- 1.Zemek RL, Grool AM, Rodriguez Duque D, DeMatteo C, Rothman L, Benchimol EI, Guttmann A, Macpherson AK. Annual and seasonal trends in ambulatory visits for pediatric concussion in Ontario between 2003 and 2013. J Pediatr. 2017;181:222–8.e2. doi: 10.1016/j.jpeds.2016.10.067.S0022-3476(16)31201-X [DOI] [PubMed] [Google Scholar]
- 2.McCrory P, Meeuwisse W, Dvořák J, Aubry M, Bailes J, Broglio S, Cantu RC, Cassidy D, Echemendia RJ, Castellani RJ, Davis GA, Ellenbogen R, Emery C, Engebretsen L, Feddermann-Demont N, Giza CC, Guskiewicz KM, Herring S, Iverson GL, Johnston KM, Kissick J, Kutcher J, Leddy JJ, Maddocks D, Makdissi M, Manley GT, McCrea M, Meehan WP, Nagahiro S, Patricios J, Putukian M, Schneider KJ, Sills A, Tator CH, Turner M, Vos PE. Consensus statement on concussion in sport-the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med. 2017;51(11):838–47. doi: 10.1136/bjsports-2017-097699.bjsports-2017-097699 [DOI] [PubMed] [Google Scholar]
- 3.Zemek R, Barrowman N, Freedman SB, Gravel J, Gagnon I, McGahern C, Aglipay M, Sangha G, Boutis K, Beer D, Craig W, Burns E, Farion KJ, Mikrogianakis A, Barlow K, Dubrovsky AS, Meeuwisse W, Gioia G, Meehan 3rd WP, Beauchamp MH, Kamil Y, Grool AM, Hoshizaki B, Anderson P, Brooks BL, Yeates KO, Vassilyadi M, Klassen T, Keightley M, Richer L, DeMatteo C, Osmond MH, Pediatric Emergency Research Canada (PERC) Concussion Team Clinical risk score for persistent postconcussion symptoms among children with acute concussion in the ED. JAMA. 2016;315(10):1014–25. doi: 10.1001/jama.2016.1203.2499274 [DOI] [PubMed] [Google Scholar]
- 4.Valovich McLeod T, Bay RC, Lam KC, Snyder Valier AR. The association between length of recovery following sport-related concussion and generic and specific health-related quality of life in adolescent athletes: a prospective, longitudinal study. J Head Trauma Rehabil. 2019;34(1):E1–9. doi: 10.1097/HTR.0000000000000394. [DOI] [PubMed] [Google Scholar]
- 5.Howell DR, Wilson JC, Kirkwood MW, Grubenhoff JA. Quality of life and symptom burden 1 month after concussion in children and adolescents. Clin Pediatr (Phila) 2019;58(1):42–9. doi: 10.1177/0009922818806308. [DOI] [PubMed] [Google Scholar]
- 6.Townsend EA, Polatajko HJ. Enabling occupation II: advancing an occupational therapy vision for health, well-being, & justice through occupation. Ottawa, Canada: Canadian Association of Occupational Therapists; 2007. [Google Scholar]
- 7.Sang RC, Vawda Y, Greenspoon D, Reed N, Hunt AW. An innovative approach to measuring youth concussion recovery: occupational performance. Br J Occup Ther. 2019;83(4):220–7. doi: 10.1177/0308022619851415. [DOI] [Google Scholar]
- 8.Iadevaia C, Roiger T, Zwart MB. Qualitative examination of adolescent health-related quality of life at 1 year postconcussion. J Athl Train. 2015;50(11):1182–9. doi: 10.4085/1062-6050-50.11.02. https://meridian.allenpress.com/jat/article-lookup/doi/10.4085/1062-6050-50.11.02 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Valovich McLeod TC, Wagner AJ, Bacon CE. Lived experiences of adolescent athletes following sport-related concussion. Orthop J Sports Med. 2017;5(12):2325967117745033. doi: 10.1177/2325967117745033. https://journals.sagepub.com/doi/10.1177/2325967117745033?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed .10.1177_2325967117745033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Renaud MI, van de Port IG, Catsman-Berrevoets CE, Jellema K, Lambregts SA, van Heugten CM. Activities and participation in the first 6 months after mild traumatic brain injury in children and adolescents. J Head Trauma Rehabil. 2020;35(6):E501–12. doi: 10.1097/HTR.0000000000000584.00001199-202011000-00013 [DOI] [PubMed] [Google Scholar]
- 11.DiFazio M, Silverberg ND, Kirkwood MW, Bernier R, Iverson GL. Prolonged activity restriction after concussion: are we worsening outcomes? Clin Pediatr (Phila) 2016;55(5):443–51. doi: 10.1177/0009922815589914.0009922815589914 [DOI] [PubMed] [Google Scholar]
- 12.Silverberg ND, Iverson GL. Is rest after concussion "the best medicine?": recommendations for activity resumption following concussion in athletes, civilians, and military service members. J Head Trauma Rehabil. 2013;28(4):250–9. doi: 10.1097/HTR.0b013e31825ad658. [DOI] [PubMed] [Google Scholar]
- 13.Gagnon I. Determining outcome in children and adolescents after concussion: viewing things more holistically. J Orthop Sports Phys Ther. 2019;49(11):855–63. doi: 10.2519/jospt.2019.8918. [DOI] [PubMed] [Google Scholar]
- 14.Harris MB, Rafeedie S, McArthur D, Babikian T, Snyder A, Polster D, Giza CC. Addition of occupational therapy to an interdisciplinary concussion clinic improves identification of functional impairments. J Head Trauma Rehabil. 2019;34(6):425–32. doi: 10.1097/HTR.0000000000000544.00001199-201911000-00009 [DOI] [PubMed] [Google Scholar]
- 15.Paniccia MJ, Reed NP. Dove and hawk profiles in youth concussion: rethinking occupational performance. Can J Occup Ther. 2017;84(2):111–8. doi: 10.1177/0008417416688302. [DOI] [PubMed] [Google Scholar]
- 16.Kurowski BG, Hugentobler J, Quatman-Yates C, Taylor J, Gubanich PJ, Altaye M, Wade SL. Aerobic exercise for adolescents with prolonged symptoms after mild traumatic brain injury: an exploratory randomized clinical trial. J Head Trauma Rehabil. 2017;32(2):79–89. doi: 10.1097/HTR.0000000000000238. http://europepmc.org/abstract/MED/27120294 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chrisman SP, Whitlock KB, Mendoza JA, Burton MS, Somers E, Hsu A, Fay L, Palermo TM, Rivara FP. Pilot randomized controlled trial of an exercise program requiring minimal in-person visits for youth with persistent sport-related concussion. Front Neurol. 2019;10:623. doi: 10.3389/fneur.2019.00623. doi: 10.3389/fneur.2019.00623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Chrisman SP, Whitlock KB, Somers E, Burton MS, Herring SA, Rowhani-Rahbar A, Rivara FP. Pilot study of the sub-symptom threshold exercise program (SSTEP) for persistent concussion symptoms in youth. NeuroRehabilitation. 2017;40(4):493–9. doi: 10.3233/NRE-161436.NRE1436 [DOI] [PubMed] [Google Scholar]
- 19.Leddy JJ, Haider MN, Ellis MJ, Mannix R, Darling SR, Freitas MS, Suffoletto HN, Leiter J, Cordingley DM, Willer B. Early subthreshold aerobic exercise for sport-related concussion: a randomized clinical trial. JAMA Pediatr. 2019;173(4):319–25. doi: 10.1001/jamapediatrics.2018.4397. http://europepmc.org/abstract/MED/30715132 .2723523 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Leddy JJ, Haider MN, Hinds AL, Darling S, Willer BS. A preliminary study of the effect of early aerobic exercise treatment for sport-related concussion in males. Clin J Sport Med. 2019;29(5):353–60. doi: 10.1097/JSM.0000000000000663. http://europepmc.org/abstract/MED/30239422 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Leddy JJ, Kozlowski K, Donnelly JP, Pendergast DR, Epstein LH, Willer B. A preliminary study of subsymptom threshold exercise training for refractory post-concussion syndrome. Clin J Sport Med. 2010;20(1):21–7. doi: 10.1097/JSM.0b013e3181c6c22c.00042752-201001000-00004 [DOI] [PubMed] [Google Scholar]
- 22.Langevin P, Frémont P, Fait P, Dubé MO, Bertrand-Charette M, Roy JS. Aerobic exercise for sport-related concussion: a systematic review and meta-analysis. Med Sci Sports Exerc. 2020;52(12):2491–9. doi: 10.1249/MSS.0000000000002402.00005768-202012000-00001 [DOI] [PubMed] [Google Scholar]
- 23.Lal A, Kolakowsky-Hayner SA, Ghajar J, Balamane M. The effect of physical exercise after a concussion: a systematic review and meta-analysis. Am J Sports Med. 2018;46(3):743–52. doi: 10.1177/0363546517706137. [DOI] [PubMed] [Google Scholar]
- 24.Willer BS, Haider MN, Bezherano I, Wilber CG, Mannix R, Kozlowski K, Leddy JJ. Comparison of rest to aerobic exercise and placebo-like treatment of acute sport-related concussion in male and female adolescents. Arch Phys Med Rehabil. 2019;100(12):2267–75. doi: 10.1016/j.apmr.2019.07.003. http://europepmc.org/abstract/MED/31377190 .S0003-9993(19)30505-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chan C, Iverson GL, Purtzki J, Wong K, Kwan V, Gagnon I, Silverberg ND. Safety of active rehabilitation for persistent symptoms after pediatric sport-related concussion: a randomized controlled trial. Arch Phys Med Rehabil. 2018;99(2):242–9. doi: 10.1016/j.apmr.2017.09.108.S0003-9993(17)31251-0 [DOI] [PubMed] [Google Scholar]
- 26.Dobney DM, Grilli L, Beaulieu C, Straub M, Galli C, Saklas M, Friedman D, Dubrovsky AS, Gagnon IJ. Feasibility of early active rehabilitation for concussion recovery in youth: a randomized trial. Clin J Sport Med. 2020;30(6):519–25. doi: 10.1097/JSM.0000000000000671.00042752-202011000-00001 [DOI] [PubMed] [Google Scholar]
- 27.Dobney DM, Grilli L, Kocilowicz H, Beaulieu C, Straub M, Friedman D, Gagnon I. Evaluation of an active rehabilitation program for concussion management in children and adolescents. Brain Inj. 2017;31(13-14):1753–9. doi: 10.1080/02699052.2017.1346294. [DOI] [PubMed] [Google Scholar]
- 28.Gagnon I, Galli C, Friedman D, Grilli L, Iverson GL. Active rehabilitation for children who are slow to recover following sport-related concussion. Brain Inj. 2009;23(12):956–64. doi: 10.3109/02699050903373477.10.3109/02699050903373477 [DOI] [PubMed] [Google Scholar]
- 29.Gagnon I, Grilli L, Friedman D, Iverson GL. A pilot study of active rehabilitation for adolescents who are slow to recover from sport-related concussion. Scand J Med Sci Sports. 2016;26(3):299–306. doi: 10.1111/sms.12441. [DOI] [PubMed] [Google Scholar]
- 30.Gauvin-Lepage J, Friedman D, Grilli L, Sufrategui M, De Matteo C, Iverson G, Gagnon I. Effectiveness of an exercise-based active rehabilitation intervention for youth who are slow to recover after concussion. Clin J Sport Med. 2020;30(5):423–32. doi: 10.1097/JSM.0000000000000634.00042752-202009000-00001 [DOI] [PubMed] [Google Scholar]
- 31.Reed N, Greenspoon D, Iverson GL, DeMatteo C, Fait P, Gauvin-Lepage J, Hunt A, Gagnon IJ. Management of persistent postconcussion symptoms in youth: a randomised control trial protocol. BMJ Open. 2015;5(7):e008468. doi: 10.1136/bmjopen-2015-008468. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=26231756 .bmjopen-2015-008468 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Imhoff S, Fait P, Carrier-Toutant F, Boulard G. Efficiency of an active rehabilitation intervention in a slow-to-recover paediatric population following mild traumatic brain injury: a pilot study. J Sports Med (Hindawi Publ Corp) 2016;2016:5127374. doi: 10.1155/2016/5127374. doi: 10.1155/2016/5127374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Leddy JJ, Baker JG, Willer B. Active rehabilitation of concussion and post-concussion syndrome. Phys Med Rehabil Clin N Am. 2016;27(2):437–54. doi: 10.1016/j.pmr.2015.12.003.S1047-9651(15)00125-4 [DOI] [PubMed] [Google Scholar]
- 34.Leddy JJ, Haider MN, Ellis M, Willer BS. Exercise is medicine for concussion. Curr Sports Med Rep. 2018;17(8):262–70. doi: 10.1249/JSR.0000000000000505. http://europepmc.org/abstract/MED/30095546 .00149619-201808000-00005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Leddy J, Baker JG, Haider MN, Hinds A, Willer B. A physiological approach to prolonged recovery from sport-related concussion. J Athl Train. 2017;52(3):299–308. doi: 10.4085/1062-6050-51.11.08. https://meridian.allenpress.com/jat/article-lookup/doi/10.4085/1062-6050-51.11.08 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Carter KM, Pauhl AN, Christie AD. The role of active rehabilitation in concussion management: a systematic review and meta-analysis. Med Sci Sports Exerc. 2021;53(9):1835–45. doi: 10.1249/MSS.0000000000002663.00005768-202109000-00005 [DOI] [PubMed] [Google Scholar]
- 37.Bernard CO, Ponsford JA, McKinlay A, McKenzie D, Krieser D. Predictors of post-concussive symptoms in young children: injury versus non-injury related factors. J Int Neuropsychol Soc. 2016;22(8):793–803. doi: 10.1017/S1355617716000709.S1355617716000709 [DOI] [PubMed] [Google Scholar]
- 38.Register-Mihalik JK, DeFreese JD, Callahan CE, Carneiro K. Utilizing the biopsychosocial model in concussion treatment: post-traumatic headache and beyond. Curr Pain Headache Rep. 2020;24(8):44. doi: 10.1007/s11916-020-00870-y.10.1007/s11916-020-00870-y [DOI] [PubMed] [Google Scholar]
- 39.Silverberg ND, Iverson GL. Etiology of the post-concussion syndrome: physiogenesis and psychogenesis revisited. NeuroRehabilitation. 2011;29(4):317–29. doi: 10.3233/NRE-2011-0708.D622320H7H5154K1 [DOI] [PubMed] [Google Scholar]
- 40.Gagnon I, Friedman D, Beauchamp MH, Christie B, DeMatteo C, Macartney G, McFadyen BJ, Sirois K, Taneja C, Zabjek K, Zemek R, Mrazik M. The Canadian pediatric mild traumatic brain injury common data elements project: harmonizing outcomes to increase understanding of pediatric concussion. J Neurotrauma. 2018;35(16):1849–57. doi: 10.1089/neu.2018.5887. [DOI] [PubMed] [Google Scholar]
- 41.Meyns P, Roman de Mettelinge T, van der Spank J, Coussens M, Van Waelvelde H. Motivation in pediatric motor rehabilitation: a systematic search of the literature using the self-determination theory as a conceptual framework. Dev Neurorehabil. 2018;21(6):371–90. doi: 10.1080/17518423.2017.1295286. [DOI] [PubMed] [Google Scholar]
- 42.Kusec A, Velikonja D, DeMatteo C, Harris JE. Motivation in rehabilitation and acquired brain injury: can theory help us understand it? Disabil Rehabil. 2019;41(19):2343–9. doi: 10.1080/09638288.2018.1467504. [DOI] [PubMed] [Google Scholar]
- 43.Young TK, Chatwood S, Marchildon GP. Healthcare in Canada's north: are we getting value for money? Healthc Policy. 2016;12(1):59–70. http://europepmc.org/abstract/MED/27585027 . [PMC free article] [PubMed] [Google Scholar]
- 44.Huot S, Ho H, Ko A, Lam S, Tactay P, MacLachlan J, Raanaas RK. Identifying barriers to healthcare delivery and access in the circumpolar north: important insights for health professionals. Int J Circumpolar Health. 2019;78(1):1571385. doi: 10.1080/22423982.2019.1571385. http://europepmc.org/abstract/MED/30696379 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kairy D, Lehoux P, Vincent C, Visintin M. A systematic review of clinical outcomes, clinical process, healthcare utilization and costs associated with telerehabilitation. Disabil Rehabil. 2009;31(6):427–47. doi: 10.1080/09638280802062553.901523878 [DOI] [PubMed] [Google Scholar]
- 46.Camden C, Pratte G, Fallon F, Couture M, Berbari J, Tousignant M. Diversity of practices in telerehabilitation for children with disabilities and effective intervention characteristics: results from a systematic review. Disabil Rehabil. 2020;42(24):3424–36. doi: 10.1080/09638288.2019.1595750. [DOI] [PubMed] [Google Scholar]
- 47.dos Santos MT, Moura SC, Gomes LM, Lima AH, Moreira RS, Silva CD, Guimarães EM. Telehealth application on the rehabilitation of children and adolescents. Rev Paul Pediatr. 2014;32(1):136–43. doi: 10.1590/s0103-05822014000100020. https://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-05822014000100136&lng=en&nrm=iso&tlng=en .S0103-05822014000100136 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ellis MJ, Boles S, Derksen V, Dawyduk B, Amadu A, Stelmack K, Kowalchuk M, Russell K. Evaluation of a pilot paediatric concussion telemedicine programme for northern communities in Manitoba. Int J Circumpolar Health. 2019;78(1):1573163. doi: 10.1080/22423982.2019.1573163. http://europepmc.org/abstract/MED/30714513 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Ellis MJ, Russell K. The potential of telemedicine to improve pediatric concussion care in rural and remote communities in Canada. Front Neurol. 2019;10:840. doi: 10.3389/fneur.2019.00840. doi: 10.3389/fneur.2019.00840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M, Medical Research Council Guidance Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337:a1655. doi: 10.1136/bmj.a1655. http://europepmc.org/abstract/MED/18824488 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Campbell M, Fitzpatrick R, Haines A, Kinmonth AL, Sandercock P, Spiegelhalter D, Tyrer P. Framework for design and evaluation of complex interventions to improve health. BMJ. 2000;321(7262):694–6. doi: 10.1136/bmj.321.7262.694. http://europepmc.org/abstract/MED/10987780 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Campbell NC, Murray E, Darbyshire J, Emery J, Farmer A, Griffiths F, Guthrie B, Lester H, Wilson P, Kinmonth AL. Designing and evaluating complex interventions to improve health care. BMJ. 2007;334(7591):455–9. doi: 10.1136/bmj.39108.379965.BE. http://europepmc.org/abstract/MED/17332585 .334/7591/455 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Faes MC, Reelick MF, Esselink RA, Rikkert MG. Developing and evaluating complex healthcare interventions in geriatrics: the use of the medical research council framework exemplified on a complex fall prevention intervention. J Am Geriatr Soc. 2010;58(11):2212–21. doi: 10.1111/j.1532-5415.2010.03108.x. [DOI] [PubMed] [Google Scholar]
- 54.Waltzman D, Womack LS, Thomas KE, Sarmiento K. Trends in emergency department visits for contact sports-related traumatic brain injuries among children - United States, 2001-2018. MMWR Morb Mortal Wkly Rep. 2020;69(27):870–4. doi: 10.15585/mmwr.mm6927a4. doi: 10.15585/mmwr.mm6927a4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Langer L, Levy C, Bayley M. Increasing incidence of concussion: true epidemic or better recognition? J Head Trauma Rehabil. 2020;35(1):E60–6. doi: 10.1097/HTR.0000000000000503.00001199-202001000-00016 [DOI] [PubMed] [Google Scholar]
- 56.Davis GA, Anderson V, Babl FE, Gioia GA, Giza CC, Meehan W, Moser RS, Purcell L, Schatz P, Schneider KJ, Takagi M, Yeates KO, Zemek R. What is the difference in concussion management in children as compared with adults? A systematic review. Br J Sports Med. 2017;51(12):949–57. doi: 10.1136/bjsports-2016-097415.bjsports-2016-097415 [DOI] [PubMed] [Google Scholar]
- 57.Ledoux AA, Tang K, Yeates KO, Pusic MV, Boutis K, Craig WR, Gravel J, Freedman SB, Gagnon I, Gioia GA, Osmond MH, Zemek RL, Pediatric Emergency Research Canada (PERC) Concussion Team Natural progression of symptom change and recovery from concussion in a pediatric population. JAMA Pediatr. 2019;173(1):e183820. doi: 10.1001/jamapediatrics.2018.3820. http://europepmc.org/abstract/MED/30398522 .2712363 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Iverson GL, Gardner AJ, Terry DP, Ponsford JL, Sills AK, Broshek DK, Solomon GS. Predictors of clinical recovery from concussion: a systematic review. Br J Sports Med. 2017;51(12):941–8. doi: 10.1136/bjsports-2017-097729. http://bjsm.bmj.com/lookup/pmidlookup?view=long&pmid=28566342 .51/12/941 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Sady MD, Vaughan CG, Gioia GA. Psychometric characteristics of the postconcussion symptom inventory in children and adolescents. Arch Clin Neuropsychol. 2014;29(4):348–63. doi: 10.1093/arclin/acu014. http://europepmc.org/abstract/MED/24739735 .acu014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Hou R, Moss-Morris R, Peveler R, Mogg K, Bradley BP, Belli A. When a minor head injury results in enduring symptoms: a prospective investigation of risk factors for postconcussional syndrome after mild traumatic brain injury. J Neurol Neurosurg Psychiatry. 2012;83(2):217–23. doi: 10.1136/jnnp-2011-300767.jnnp-2011-300767 [DOI] [PubMed] [Google Scholar]
- 61.Wade DT, Halligan PW. The biopsychosocial model of illness: a model whose time has come. Clin Rehabil. 2017;31(8):995–1004. doi: 10.1177/0269215517709890. [DOI] [PubMed] [Google Scholar]
- 62.Valovich McLeod TC, Hale TD. Vestibular and balance issues following sport-related concussion. Brain Inj. 2015;29(2):175–84. doi: 10.3109/02699052.2014.965206. [DOI] [PubMed] [Google Scholar]
- 63.Master CL, Master SR, Wiebe DJ, Storey EP, Lockyer JE, Podolak OE, Grady MF. Vision and vestibular system dysfunction predicts prolonged concussion recovery in children. Clin J Sport Med. 2018;28(2):139–45. doi: 10.1097/JSM.0000000000000507. [DOI] [PubMed] [Google Scholar]
- 64.Gerst EH, D S, Gioia GA. Fatigue after concussion: do children and their parents report the same changes? Arch Clin Neuropsychol. 2019;34(5):772. doi: 10.1093/ARCLIN/ACZ026.42. [DOI] [Google Scholar]
- 65.Leddy JJ, Hinds AL, Miecznikowski J, Darling S, Matuszak J, Baker JG, Picano J, Willer B. Safety and prognostic utility of provocative exercise testing in acutely concussed adolescents: a randomized trial. Clin J Sport Med. 2018;28(1):13–20. doi: 10.1097/JSM.0000000000000431. http://europepmc.org/abstract/MED/29257777 .00042752-201801000-00002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Snell DL, Siegert RJ, Hay-Smith EJ, Surgenor LJ. Associations between illness perceptions, coping styles and outcome after mild traumatic brain injury: preliminary results from a cohort study. Brain Inj. 2011;25(11):1126–38. doi: 10.3109/02699052.2011.607786. [DOI] [PubMed] [Google Scholar]
- 67.Silverberg ND, Panenka WJ, Iverson GL. Fear avoidance and clinical outcomes from mild traumatic brain injury. J Neurotrauma. 2018;35(16):1864–73. doi: 10.1089/neu.2018.5662. [DOI] [PubMed] [Google Scholar]
- 68.Sandel N, Reynolds E, Cohen PE, Gillie BL, Kontos AP. Anxiety and mood clinical profile following sport-related concussion: from risk factors to treatment. Sport Exerc Perform Psychol. 2017;6(3):304–23. doi: 10.1037/spy0000098. http://europepmc.org/abstract/MED/29130023 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Gagnon I, Swaine B, Friedman D, Forget R. Exploring children's self-efficacy related to physical activity performance after a mild traumatic brain injury. J Head Trauma Rehabil. 2005;20(5):436–49. doi: 10.1097/00001199-200509000-00005.00001199-200509000-00005 [DOI] [PubMed] [Google Scholar]
- 70.Ramsey KA, Vaughan C, Wagner BM, McGuire JF, Gioia GA. Impact of self-efficacy and affective functioning on pediatric concussion symptom severity. J Int Neuropsychol Soc. 2021;27(9):875–82. doi: 10.1017/S1355617720001320.S1355617720001320 [DOI] [PubMed] [Google Scholar]
- 71.Davies SC, Bernstein ER, Daprano CM. A qualitative inquiry of social and emotional support for students with persistent concussion symptoms. J Educ Psychol Consult. 2020;30(2):156–82. doi: 10.1080/10474412.2019.1649598. [DOI] [Google Scholar]
- 72.Kita H, Mallory KD, Hickling A, Wilson KE, Kroshus E, Reed N. Social support during youth concussion recovery. Brain Inj. 2020;34(6):782–90. doi: 10.1080/02699052.2020.1753243. [DOI] [PubMed] [Google Scholar]
- 73.Covassin T, Crutcher B, Bleecker A, Heiden EO, Dailey A, Yang J. Postinjury anxiety and social support among collegiate athletes: a comparison between orthopaedic injuries and concussions. J Athl Train. 2014;49(4):462–8. doi: 10.4085/1062-6059-49.2.03. https://meridian.allenpress.com/jat/article-lookup/doi/10.4085/1062-6059-49.2.03 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Barnhart M, Bay RC, Valovich McLeod TC. The influence of timing of reporting and clinic presentation on concussion recovery outcomes: a systematic review and meta-analysis. Sports Med. 2021;51(7):1491–508. doi: 10.1007/s40279-021-01444-7.10.1007/s40279-021-01444-7 [DOI] [PubMed] [Google Scholar]
- 75.Snell DL, Surgenor LJ, Hay-Smith EJ, Siegert RJ. A systematic review of psychological treatments for mild traumatic brain injury: an update on the evidence. J Clin Exp Neuropsychol. 2009;31(1):20–38. doi: 10.1080/13803390801978849.792843407 [DOI] [PubMed] [Google Scholar]
- 76.Zemek R, Eady K, Moreau K, Farion KJ, Solomon B, Weiser M, Dematteo C. Knowledge of paediatric concussion among front-line primary care providers. Paediatr Child Health. 2014;19(9):475–80. doi: 10.1093/pch/19.9.475. http://europepmc.org/abstract/MED/25414583 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Mann A, Tator CH, Carson JD. Concussion diagnosis and management: knowledge and attitudes of family medicine residents. Can Fam Physician. 2017;63(6):460–6. http://www.cfp.ca/cgi/pmidlookup?view=long&pmid=28615399 .63/6/460 [PMC free article] [PubMed] [Google Scholar]
- 78.Graves JM, Mackelprang JL, Moore M, Abshire DA, Rivara FP, Jimenez N, Fuentes M, Vavilala MS. Rural-urban disparities in health care costs and health service utilization following pediatric mild traumatic brain injury. Health Serv Res. 2019;54(2):337–45. doi: 10.1111/1475-6773.13096. http://europepmc.org/abstract/MED/30507042 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Graves JM, Moore M, Kehoe L, Li M, Chan A, Conrick K, Williams-Gilbert W, Vavilala MS. Family hardship following youth concussion: beyond the medical bills. J Pediatr Nurs. 2020;51:15–20. doi: 10.1016/j.pedn.2019.11.016. http://europepmc.org/abstract/MED/31838221 .S0882-5963(19)30229-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Hunt AW, Agnihotri S, Sack L, Tint A, Greenspoon D, Gauvin-Lepage J, Gagnon I, Reed N, Scratch S. Mood-related changes in children and adolescents with persistent concussion symptoms following a six-week active rehabilitation program. Brain Inj. 2020;34(8):1068–73. doi: 10.1080/02699052.2020.1776396. [DOI] [PubMed] [Google Scholar]
- 81.Hunt AW, Laupacis D, Kawaguchi E, Greenspoon D, Reed N. Key ingredients to an active rehabilitation programme post-concussion: perspectives of youth and parents. Brain Inj. 2018;32(12):1534–40. doi: 10.1080/02699052.2018.1502894. [DOI] [PubMed] [Google Scholar]
- 82.Dobney DM, Grilli L, Kocilowicz H, Beaulieu C, Straub M, Friedman D, Gagnon IJ. Is there an optimal time to initiate an active rehabilitation protocol for concussion management in children? A case series. J Head Trauma Rehabil. 2018;33(3):E11–7. doi: 10.1097/HTR.0000000000000339. [DOI] [PubMed] [Google Scholar]
- 83.Gauvin-Lepage J, Friedman D, Grilli L, Gagnon I. Effect of sex on recovery from persistent postconcussion symptoms in children and adolescents participating in an active rehabilitation intervention. J Head Trauma Rehabil. 2019;34(2):96–102. doi: 10.1097/HTR.0000000000000402. [DOI] [PubMed] [Google Scholar]
- 84.Micay R, Richards D, Hutchison MG. Feasibility of a postacute structured aerobic exercise intervention following sport concussion in symptomatic adolescents: a randomised controlled study. BMJ Open Sport Exerc Med. 2018;4(1):e000404. doi: 10.1136/bmjsem-2018-000404. doi: 10.1136/bmjsem-2018-000404.bmjsem-2018-000404 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Guo Y, Albright D. The effectiveness of telehealth on self-management for older adults with a chronic condition: a comprehensive narrative review of the literature. J Telemed Telecare. 2018;24(6):392–403. doi: 10.1177/1357633X17706285. [DOI] [PubMed] [Google Scholar]
- 86.Hanlon P, Daines L, Campbell C, McKinstry B, Weller D, Pinnock H. Telehealth interventions to support self-management of long-term conditions: a systematic metareview of diabetes, heart failure, asthma, chronic obstructive pulmonary disease, and cancer. J Med Internet Res. 2017;19(5):e172. doi: 10.2196/jmir.6688. https://www.jmir.org/2017/5/e172/ v19i5e172 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Reed N, Zemek R, Dawson J, Ledoux AA, Provvidenza C, Paniccia M. Living guideline for diagnosing and managing pediatric concussion. Ontario Neutrauma Foundation. 2019. [2021-01-20]. https://islandscholar.ca/islandora/object/ir%3A23211/datastream/PDF/view .
- 88.Lawrence DW, Richards D, Comper P, Hutchison MG. Earlier time to aerobic exercise is associated with faster recovery following acute sport concussion. PLoS One. 2018;13(4):e0196062. doi: 10.1371/journal.pone.0196062. https://dx.plos.org/10.1371/journal.pone.0196062 .PONE-D-18-05312 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Maclean N, Pound P. A critical review of the concept of patient motivation in the literature on physical rehabilitation. Soc Sci Med. 2000;50(4):495–506. doi: 10.1016/s0277-9536(99)00334-2.S0277953699003342 [DOI] [PubMed] [Google Scholar]
- 90.Thompson M, Elliott C, Willis C, Ward R, Falkmer M, Falkmer T, Gubbay A, Girdler S. Can, Want and Try: parents' viewpoints regarding the participation of their child with an acquired brain injury. PLoS One. 2016;11(7):e0157951. doi: 10.1371/journal.pone.0157951. https://dx.plos.org/10.1371/journal.pone.0157951 .PONE-D-15-41531 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Ng JY, Ntoumanis N, Thøgersen-Ntoumani C, Deci EL, Ryan RM, Duda JL, Williams GC. Self-determination theory applied to health contexts: a meta-analysis. Perspect Psychol Sci. 2012;7(4):325–40. doi: 10.1177/1745691612447309.7/4/325 [DOI] [PubMed] [Google Scholar]
- 92.Gillison FB, Rouse P, Standage M, Sebire SJ, Ryan RM. A meta-analysis of techniques to promote motivation for health behaviour change from a self-determination theory perspective. Health Psychol Rev. 2019;13(1):110–30. doi: 10.1080/17437199.2018.1534071. [DOI] [PubMed] [Google Scholar]
- 93.Auclair-Pilote J, Lalande D, Tinawi S, Feyz M, de Guise E. Satisfaction of basic psychological needs following a mild traumatic brain injury and relationships with post-concussion symptoms, anxiety, and depression. Disabil Rehabil. 2021;43(4):507–15. doi: 10.1080/09638288.2019.1630858. [DOI] [PubMed] [Google Scholar]
- 94.Teixeira PJ, Marques MM, Silva MN, Brunet J, Duda JL, Haerens L, La Guardia J, Lindwall M, Lonsdale C, Markland D, Michie S, Moller AC, Ntoumanis N, Patrick H, Reeve J, Ryan RM, Sebire SJ, Standage M, Vansteenkiste M, Weinstein N, Weman-Josefsson K, Williams GC, Hagger MS. A classification of motivation and behavior change techniques used in self-determination theory-based interventions in health contexts. Motiv Sci. 2020;6(4):438–55. doi: 10.1037/mot0000172. [DOI] [Google Scholar]
- 95.Kairy D, Tousignant M, Leclerc N, Côté AM, Levasseur M, Researchers TT. The patient's perspective of in-home telerehabilitation physiotherapy services following total knee arthroplasty. Int J Environ Res Public Health. 2013;10(9):3998–4011. doi: 10.3390/ijerph10093998. https://www.mdpi.com/resolver?pii=ijerph10093998 .ijerph10093998 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Kessler D, Anderson ND, Dawson DR. Occupational performance coaching for stroke survivors delivered via telerehabilitation using a single-case experimental design. Br J Occup Ther. 2021;84(8):488–96. doi: 10.1177/0308022620988471. https://journals.sagepub.com/doi/10.1177/0308022620988471?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed .10.1177_0308022620988471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Simpson SG, Reid CL. Therapeutic alliance in videoconferencing psychotherapy: a review. Aust J Rural Health. 2014;22(6):280–99. doi: 10.1111/ajr.12149. [DOI] [PubMed] [Google Scholar]
- 98.Wright BJ, Galtieri NJ, Fell M. Non-adherence to prescribed home rehabilitation exercises for musculoskeletal injuries: the role of the patient-practitioner relationship. J Rehabil Med. 2014;46(2):153–8. doi: 10.2340/16501977-1241. https://www.medicaljournals.se/jrm/content/abstract/10.2340/16501977-1241 . [DOI] [PubMed] [Google Scholar]
- 99.El-Sayes J, Harasym D, Turco CV, Locke MB, Nelson AJ. Exercise-induced neuroplasticity: a mechanistic model and prospects for promoting plasticity. Neuroscientist. 2019;25(1):65–85. doi: 10.1177/1073858418771538. [DOI] [PubMed] [Google Scholar]
- 100.Hassett L, Moseley AM, Harmer AR. Fitness training for cardiorespiratory conditioning after traumatic brain injury. Cochrane Database Syst Rev. 2017;12(12):CD006123. doi: 10.1002/14651858.CD006123.pub3. http://europepmc.org/abstract/MED/29286534 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Mikkelsen K, Stojanovska L, Polenakovic M, Bosevski M, Apostolopoulos V. Exercise and mental health. Maturitas. 2017;106:48–56. doi: 10.1016/j.maturitas.2017.09.003.S0378-5122(17)30856-3 [DOI] [PubMed] [Google Scholar]
- 102.Silverberg ND, Iaccarino MA, Panenka WJ, Iverson GL, McCulloch KL, Dams-O'Connor K, Reed N, McCrea M, American Congress of Rehabilitation Medicine Brain Injury Interdisciplinary Special Interest Group Mild TBI Task Force Management of concussion and mild traumatic brain injury: a synthesis of practice guidelines. Arch Phys Med Rehabil. 2020;101(2):382–93. doi: 10.1016/j.apmr.2019.10.179. https://linkinghub.elsevier.com/retrieve/pii/S0003-9993(19)31305-X .S0003-9993(19)31305-X [DOI] [PubMed] [Google Scholar]
- 103.Gagnon I, Swaine B, Champagne F, Lefebvre H. Perspectives of adolescents and their parents regarding service needs following a mild traumatic brain injury. Brain Inj. 2008;22(2):161–73. doi: 10.1080/02699050701867381.790204300 [DOI] [PubMed] [Google Scholar]
- 104.Carswell A, McColl MA, Baptiste S, Law M, Polatajko H, Pollock N. The Canadian occupational performance measure: a research and clinical literature review. Can J Occup Ther. 2004;71(4):210–22. doi: 10.1177/000841740407100406. [DOI] [PubMed] [Google Scholar]
- 105.Williams RM, Johnson RS, Snyder Valier AR, Curtis Bay R, Valovich McLeod TC. Evaluating multiple domains of health in high school athletes with sport-related concussion. J Sport Rehabil. 2020;30(4):545–51. doi: 10.1123/jsr.2019-0517.jsr.2019-0517 [DOI] [PubMed] [Google Scholar]
- 106.Roemmich JN, Barkley JE, Epstein LH, Lobarinas CL, White TM, Foster JH. Validity of PCERT and OMNI walk/run ratings of perceived exertion. Med Sci Sports Exerc. 2006;38(5):1014–9. doi: 10.1249/01.mss.0000218123.81079.49.00005768-200605000-00028 [DOI] [PubMed] [Google Scholar]
- 107.Ledoux AA, Barrowman NJ, Boutis K, Davis A, Reid S, Sangha G, Farion KJ, Belanger K, Tremblay MS, Yeates KO, DeMatteo C, Reed N, Zemek R, Pediatric Emergency Research Canada PedCARE team Multicentre, randomised clinical trial of paediatric concussion assessment of rest and exertion (PedCARE): a study to determine when to resume physical activities following concussion in children. Br J Sports Med. 2019;53(3):195. doi: 10.1136/bjsports-2017-097981.bjsports-2017-097981 [DOI] [PubMed] [Google Scholar]
- 108.Worts PR, Burkhart SO, Kim JS. A physiologically based approach to prescribing exercise following a sport-related concussion. Sports Med. 2019;49(5):683–706. doi: 10.1007/s40279-019-01065-1.10.1007/s40279-019-01065-1 [DOI] [PubMed] [Google Scholar]
- 109.Reed N, Silverberg ND, Iaccarino MA, McCrea M, McCulloch KL, Panenka W, Gregory E, Dams-O'Connor K, Iverson GL, Weyer Jamora C, Belanger H, McKinney G, Cogan AM, Provvidenza C. Returning to activity after a concussion. Arch Phys Med Rehabil. 2019;100(4):789–91. doi: 10.1016/j.apmr.2018.11.022.S0003-9993(18)31591-0 [DOI] [PubMed] [Google Scholar]
- 110.Maerlender A, Rieman W, Lichtenstein J, Condiracci C. Programmed physical exertion in recovery from sports-related concussion: a randomized pilot study. Dev Neuropsychol. 2015;40(5):273–8. doi: 10.1080/87565641.2015.1067706. [DOI] [PubMed] [Google Scholar]
- 111.Hunt AW, De Feo L, Macintyre J, Greenspoon D, Dick T, Mah K, Paniccia M, Provvidenza C, Reed N. Development and feasibility of an evidence-informed self-management education program in pediatric concussion rehabilitation. BMC Health Serv Res. 2016;16(1):400. doi: 10.1186/s12913-016-1664-3. https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-016-1664-3 .10.1186/s12913-016-1664-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Holland Bloorview Kids Rehabiltiation Hospital. [2021-07-14]. https://hollandbloorview.ca/concussion-handbook .
- 113.Gloff NE, LeNoue SR, Novins DK, Myers K. Telemental health for children and adolescents. Int Rev Psychiatry. 2015;27(6):513–24. doi: 10.3109/09540261.2015.1086322. [DOI] [PubMed] [Google Scholar]
- 114.Elbin RJ, Stephenson K, Lipinski D, Maxey K, Womble MN, Reynolds E, Covert K, Kontos AP. In-person versus telehealth for concussion clinical care in adolescents: a pilot study of therapeutic alliance and patient satisfaction. J Head Trauma Rehabil (forthcoming) 2021:-. doi: 10.1097/HTR.0000000000000707.00001199-900000000-99236 [DOI] [PubMed] [Google Scholar]
- 115.Mckinnon K, Hunt A, Knight K. Does screen time affect recovery from concussion in adolescents? Arch Dis Child. 2021;106(7):720–2. doi: 10.1136/archdischild-2020-320767.archdischild-2020-320767 [DOI] [PubMed] [Google Scholar]
- 116.Kurowski BG, Wade SL, Dexheimer JW, Dyas J, Zhang N, Babcock L. Feasibility and potential benefits of a web-based intervention delivered acutely after mild traumatic brain injury in adolescents: a pilot study. J Head Trauma Rehabil. 2016;31(6):369–78. doi: 10.1097/HTR.0000000000000180. http://europepmc.org/abstract/MED/26360000 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Babcock L, Kurowski BG, Zhang N, Dexheimer JW, Dyas J, Wade SL. Adolescents with mild traumatic brain injury get SMART: an analysis of a novel web-based intervention. Telemed J E Health. 2017;23(7):600–7. doi: 10.1089/tmj.2016.0215. http://europepmc.org/abstract/MED/28112591 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Silverberg ND, Iverson GL, McCrea M, Apps JN, Hammeke TA, Thomas DG. Activity-related symptom exacerbations after pediatric concussion. JAMA Pediatr. 2016;170(10):946–53. doi: 10.1001/jamapediatrics.2016.1187.2537267 [DOI] [PubMed] [Google Scholar]
- 119.Leddy JJ, Willer B. Use of graded exercise testing in concussion and return-to-activity management. Curr Sports Med Rep. 2013;12(6):370–6. doi: 10.1249/JSR.0000000000000008.00149619-201311000-00008 [DOI] [PubMed] [Google Scholar]
- 120.van Heugten C, Renaud I, Resch C. The role of early intervention in improving the level of activities and participation in youths after mild traumatic brain injury: a scoping review. Concussion. 2017;2(3):CNC38. doi: 10.2217/cnc-2016-0030. https://www.futuremedicine.com/doi/abs/10.2217/cnc-2016-0030?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Intervention characteristics among studies included in the review.