

Summary
A great number of burns affect the hands, either as part of a more extensive burn or as an isolated injury. These injuries can lead to physical, social and psychological consequences that may reduce quality of life and make difficult the return to work. The goal of this study was to investigate the main epidemiologic characteristics of adult patients with hand burns admitted to a dedicated burn centre, evaluate the outcomes of the treatment, and identify the predictors associated with the worst outcomes. This study found that a considerable amount of burn victims admitted had hand burns (41.5%). Males are more likely to be injured in general, but females are more prevalent in burns by hot liquids. The most common comorbidity was hypertension, followed by dyslipidemia and type II diabetes. Cooking is the activity associated with more accidental victims. Most injuries did not require surgical intervention. Approximately two-thirds of the patients did not have any important sequelae. The most common complications were scar disturbances (26%) and scar contractures (14%). The need for surgery, a higher number of surgeries and higher surface area burn were associated with the worst outcomes. It is imperative to establish a burn prevention education program nationwide, encompassing water temperature control in households, the use of anti-burn equipment, and the replacement of old electrical/ heating equipment.
Keywords: contractures, cooking, fire, surgery, work accident
Abstract
Bon nombre de brûlures touchent les mains, isolément ou dans le cadre de brûlures plus étendues. Elles peuvent entraîner des conséquences physiques, psychologiques et sociales susceptibles d’obérer la qualité de vie et rendre difficile la reprise de l’activité professionnelle. Le but de cette étude était d’évaluer les principales caractéristiques épidémiologiques des brûlures de main chez des adultes admis dans notre CTB, leur évolution et les facteurs prédictifs de mauvaise évolution. Nous avons constaté que 41,5% de nos patients avaient une atteinte de main. Si les hommes étaient plus à risque de brûlures, les brûlures des femmes étaient plus souvent dues à un ébouillantement. Les comorbidités les plus fréquentes étaient l’hypertension artérielle, les dyslipidémies et le diabète de type 2. La cuisine était une activité particulièrement à risque. La plupart des lésions ont cicatrisé spontanément et les 2/3 des patients n’avaient pas de séquelle majeure, les plus fréquentes étant les anomalies cicatricielles (26%) et les brides rétractiles (14%). Les critères de mauvaise évolution étaient la nécessité d’intervention chirurgicale (et leur nombre) ainsi que l’augmentation de la surface brûlée. Il est impératif d’établir un plan national de prévention comprenant la régulation de la température de l’eau aux points de puisage, l’utilisation d’équipements sécurisés et le remplacement des systèmes de chauffage comme des circuits électriques anciens.
Introduction
Burns are one of the most debilitating traumatic events. Even though there has been a substantial improvement in survival rates1 and the prevalence of chronic sequelae2 in the last three decades, burns are still one of the main leading causes of mortality and morbidity worldwide.
More than 80% of burn patients have burns affecting their hands, either as part of a more extensive burn or as an isolated injury.1,3 Despite not being responsible for the patient’s death, hand burns can produce biological, social and psychological consequences that hamper a successful reintegration into society and reduce quality of life.4 Beyond functional restoration, hand aesthetics cannot be undervalued since they are frequently exposed and participate in several social interactions.5 It is estimated that approximately 18 million people worldwide have significant impairment in their daily lives due to hand burns.2
Significant hand burns are classified as a major burn injury, and they should be referred and treated in a specialized Burn Center. Even with the best treatment and rehabilitation available, several patients still develop debilitating contractures, hypertrophic scars and neuropathy.6-8 The goal of this study was to investigate the main epidemiologic characteristics of adult patients with hand burns admitted to a burn center, evaluate the outcomes of the treatment, and identify the predictors associated with the worst outcomes. A secondary goal was to identify groups of individuals with a higher risk of contracting these burns and having poorer outcomes in order to set up prevention strategies.
Materials and methods
We performed a retrospective data analysis of all patients admitted to the Hospital S. José Burn Unit during the period between the first of January 2015 and the thirtieth of December 2017, who had hand burns. This Burn Unit only accepts adult patients, has eight beds, and is one of five specialized Burn Centers in Portugal. From this analysis were excluded all patients admitted who had exclusively first-degree burns of the hands and those suffering from other injuries not associated with burns.
Data were extracted from electronic medical records and included age, gender, length of stay (LOS – in days) for patients with exclusively hand burns, etiology (fire, hot liquids, electrical, flash burn, contact, chemical, abrasion/friction), circumstance of burn (personal accident, work-related, assault), patient occupation, hand surface area (HSA - %) burn, depth of burn (2nd degree superficial, 2nd degree deep and 3rd degree), unilateral vs. bilateral injury, hand burn severity score (HABS)9, number and type of surgeries related to the hand burn, patient comorbidities and outcomes (follow-up ranging from 12-36 months).
Statistical analysis was performed with SPSS, version 22. Descriptive statistics were presented as means (M) and standard deviations (SD) for continuous and symmetrical variables and medians (Mdn) and percentiles P25-P75 for continuous skewed variables. Frequencies (n) and percentages (%) were calculated for categorical variables. Comparisons and associations were performed with qui-square or Fisher tests for categorical variables, t-tests for comparing two groups on continuous normally distributed variables (alternatively Mann-Whitney tests) and ANOVA or the alternative Kruskall-Wallis tests for comparing more than two groups. Significance for rejection of the null hypothesis was p<.05.
Results
General demographics
During the three years analyzed, 337 patients were admitted to the Burn Unit, but only 140 (41.5%) suffered hand burns. Regarding the patients with hand burns, only 16 (11.4%) had exclusively injuries in this anatomical region.
The age of patients ranged from 20 to 93 years old (M=52.96; SD=19.56). Regarding gender, 86 (61.4%) patients were male and 54 (38.6%) were female. The average age of male patients was 48.02 years old (SD=18.73) and female patients 60.83 (SD=18.4).
The median of LOS for the patients with only hand burns was 14.69 days (P25=11; P75=17.5). Eighty patients (57.1%) suffered unilateral burns, and sixty (42.9%) had bilateral injuries.
Circumstance of burn and etiology
The most frequent circumstance of burn was personal accident (n=103; 73.6%), followed by occupational injury (n=36; 25.7%) and assault (n=1; 0.7%). Regarding etiology, most burns were caused by fire (n=89; 63.6%), followed by hot liquids (n=32; 22.9%) and electric flash (n=7; 5%) (Table I).
Table I. Etiology of burns.

Fire burn patients were more often males (64%).
Nineteen of these patients suffered burns in the work environment (23.6%), and one patient tried to kill himself through immolation. The remainder were personal accidents. Regarding work-related injuries, the most common patient occupations were industrial worker (5), cook (3), and mechanic (2) (Table II).
Table II. Occupation of patients with work-related injuries (discriminated by etiology).

Concerning personal accidents, most burns related to barbecue cooking and indoor cooking, with 13 cases each (Table III).
Regarding hot liquid burns, gender distribution was almost the inverse of fire. There were predominantly female patients affected (N=22; 68.8%). The majority were personal accidents (24; 75.1%), but there were also seven work-related burns and one assault. From the 24 personal accidents, 22 happened while cooking in the kitchen, with oil (15) and hot water (7). The remaining two cases happened in the bathtub (hot water), one after a fall (old patient with impaired mobility), and the other after fainting during a shower.
Electric flash was the third most common cause of burn and it only affected male patients. Six out of seven (85.7%) cases were work-related. The electric flash occurred after the explosion of an electric panel (5 cases) or after improper handling of electric cables (2 cases).
Regarding the patients admitted with chemical burns (three men and one woman), only one of them had a work-related injury after being exposed to cement (industrial worker). The other accidental cases were caused by caustic soda (2) and muriatic acid (1).
Electric burns (3 cases) only affected male patients. A single work-related burn occurred in a construction worker. One of the accidental burns occurred during a robbery, trying to remove the copper from the electric cable, and the other happened after the manipulation of electric cables.
Table III. Context of personal accidents resulting in burns.

TBSA, depth of burn, HABS score and comorbidities More than half of the burns were 2nd-degree deep (n=79; 56.4%). Second-degree superficial burns accounted for 34 (24.3%) patients and 27 (19.3%) had 3rd-degree burns. The average HSA burn was 1.55% (SD=1.13), and the average HABS score was 5.97 (SD=4.29).
In our patient sample, the most common comorbidity was hypertension (42; 30%), followed by dyslipidemia (26; 18.6%) and type II diabetes (19; 13.6%) (Table IV).
Table IV. Comorbidities.

Surgery and outcome
During the period studied there were, in total, 84 surgical interventions for the treatment of hand burns. Only 58 patients (41.4%) needed surgery. Of those, 42 (72.4%) were submitted to a single surgery. The most frequent operation was mechanical debridement and split-thickness skin graft (Table V).
Table V. Surgeries.

During hospitalization, 12 patients (8.6%) died. Concerning the remaining 128 patients, 78 had their follow up in other healthcare facilities and their outcomes were not reported. Regarding the 50 patients with follow-up in our department, 33 (66%) did not have any limitations or complaints. Scar disturbances were the most common sequel (n=13; 26%) followed by scar contractures (n=7; 14%) (Table VI).
Table VI. Outcomes.

Associations with LOS, surgery and outcomes
No significant correlations were found for LOS regarding HSA (p=.957), HABS (p=.430), number of surgeries (p=.975), age (p=.931) or any other variable. Surgery probability was associated with older patients (p=.033), increased HSA (p<.001), and higher HABS score (p<.001). An association with depth of burn was also found: 100% of all 3rd-degree burns had surgery, 39.2% (31 patients) of 2nd degree deep burns had surgery, and none of the 2nd degree superficial burns had surgery. Surgery probability was not associated with sex (p=.201), circumstances of burn (p=.063), cause of burn (p=.063), or laterality (p=.085).
The number of surgeries was significantly associated with HSA (rs=.378, p<.001), HABS score (rs=.670, p<.001), and age (rs=.171, p=.043). The number of surgeries was also significantly associated with depth of burn (p<.001), with a higher median for 3rd-degree burns (Mdn=1; P25=1; P75=2) and laterality (p=.034), with a higher median for bilateral burns (Mdn=0.5; P25=0; P75=1). The number of surgeries was not associated with sex (p=.374), circumstances of burn (p=.093), cause of burn (p=.107), or surgery (p=.913).
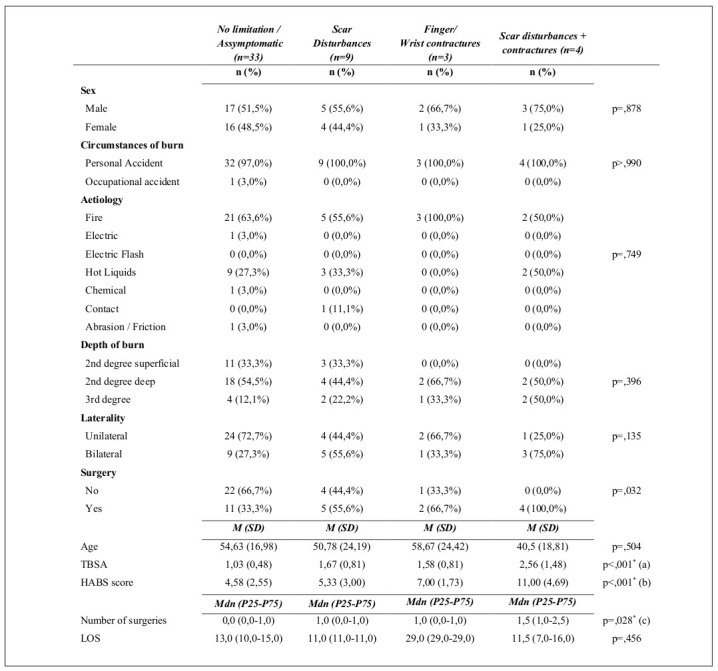
Outcome was then associated with all other variables (Table VII). Results showed significant association of surgery with finger/wrist contractures (66.7%) and scar disturbances + contractures (100%) (p=,032). TBSA and HABS score were also significantly associated with outcome (p<,001). TBSA was lower in the non-symptomatic group (M=1,03; SD=0,48) when compared to the scar disturbances + contractures group (M=2,56; SD=2,48). HABS score was higher in the scar disturbances + contractures group (M=11,00; SD=4,69) compared with no limitations (M=4,58; SD=2,55) and scar disturbances (M=5,33; SD=3,00).
Finally, the number of surgeries was also significantly associated with outcome (p=,028), regarding the comparison of no limitation (Mdn=0,0) vs. scar disturbances + contractures group (Mdn=1,5) (p=,038).
Table VII. Associations of variables with different outcomes.
Finally, the number of surgeries was also significantly associated with outcome (p=,028), regarding the comparison of no limitation (Mdn=0,0) vs. scar disturbances + contractures group (Mdn=1,5) (p=,038).
Discussion
During the period of the study, 41.5% of the patients admitted to the Burn Unit had burns of the hand. This value is lower than several other articles published (54- 90%),1,10-12 but some of them refer to upper limb injuries and not exclusively hands.1,11 Only 11.4% (16 patients) had exclusively hand burns. This value is significantly lower than in a Chinese13 and an Albanian study,14 which had 28.8% and 26.4%, respectively. We believe this difference might be explained by the fact that both studies included children and they are more susceptible to isolated contact burns of the hand. The average age of our patients (52,9) was also substantially higher than in the majority of published studies, in which the average is below 30 years.2,9,14,15 This discrepancy is easily explained by the fact that all these studies include children, and in some they are even the most represented age group.2,9
Interestingly, the study performed by Bache et al.16 in England, which included only patients older than 15 years old, had an average age of the patient sample much similar to the one we obtained, 46.2 years. As expected and following most data in the literature,13-16 males were substantially more affected (61.4%). We found only one exception in a study by Corlew et al.,2 where women were more prevalent. Perhaps the fact that the patients lived exclusively in low and middle-income countries from Sub-Saharan Africa and South Asia where women tend to be in charge of all domestic chores including cooking, the leading cause of burns in that study, explains this finding.
As expected, thermal injury was undisputedly the leading cause of burns.1 Fire was the most prevalent causative agent, followed by hot liquids and electric flash. Chemical, electric, contact and abrasion burns accounted for only 8.5% of the total cases. This causative distribution is in accordance with most published literature.2,16-19 Nevertheless, there are contrasting data available. In the Bache et al.9 study, the most frequent cause was contact, with almost twice the number of flame victims. Importantly, in this study, 40% of the patients were less than 16 years old. Arifi et al.15 report low voltage electrical burns in 36.7% of their patients, the second most prevalent cause after flame.
As pointed out by the author, this high amount of electrical-derived burns may be due to a poor socioeconomic status and inefficient electric energy system in Kosovo. There were substantial gender differences. Men were more affected by flame burns and women by hot liquids. Interestingly, all patients that suffered electric flash or electrical burns were male. We believe this can be attributed to the fact that in most households men are typically in charge of small electrical repairs, and they are substantially more numerous in occupations that deal directly with electric cables or panels such as electricians and industrial workers.
The majority of the burns (72.9%) happened in the context of personal accidents. It was clear that cooking was, by far, the activity that was implicated in the highest number of burns, either in flame or in hot liquids. In the former group, it encompassed 37.7% (26) of the patients and was due to barbecue accidents or poor handling of a blowtorch or stove. In the latter, it was even more impressive, being responsible for 91.7% of the burns. Both Corlew et al.2 and Zikai et al.14 state cooking as the most frequent cause of hand burns.
Accidents with fireplace and candles/lamps were also frequent (10 cases). Of note, 8 of these patients were more than 74 years old. We think this is explained by the fact that some elderly in our country live in ancient houses not equipped with modern heating equipment or proper electrical system installation. Simultaneously, this group of patients has frequently a mobility deficit which increases the probability of burn. Other important causes of flame burns were wildfires and slash burning accidents (5 each). In the last few years, Portugal has been devastated by many wildfires throughout the country with several casualties, so these numbers are not surprising.
Regarding the occupational injuries, cooks are the professionals that suffered more burns, taking into account both fire and hot liquids. Industrial workers (7) and construction workers (3) were also quite prevalent with burns being caused by fire, hot liquids, chemical agents and electricity. Electricians (4 cases in total) were the leading occupational group affected by electrical flash burns. All these jobs are more frequently performed by men in our country, which helps to explain the significantly different prevalence of occupational injuries in each gender (75% of the victims are male). In the study by Zikai et al.,14 this difference was also obtained, with men being much more prevalent in the occupational injuries and the ones occurring outdoors.
Concerning the average surface area injured, most studies report the total body count and not just the hands, so it is difficult to compare with our results. Nonetheless, Wang et al.13 reported 2.03% in their study, which is slightly higher than what we obtained (1.55%). The average HABS we obtained (5.97) was slightly higher than what Bache et al. had published in two previous studies (3.9 and 5.4).9,16 The most frequent burn in our study was 2nd-degree deep accounting for 56.4% and 3rd-degree burns were responsible for only 19.3%. Most studies report higher percentages of 3rd degree burns (22-54%).9,13,15,16-19 One explanation for this might be different timings of burn evaluation. In our study, the categorization was made when the patient was admitted to the Burn Unit. It is possible that some of the more superficial burns became deeper. Another factor to take into account is that in the Chinese13 and Kosovar15 studies, electrical injuries were much more frequent (25.4% and 36.7%). Electrical burns are commonly associated with more profound injuries.1,18
The comorbidities of the patients evaluated do not differ significantly from the rest of the population. Only 8.6% of the patients smoked and only 5.7% had a history of alcoholism. In their series, Knight et al.19 found tobacco abuse in 31.7% and alcohol/non-prescription drug abuse in 22% of the patients. We believe this difference could be explained by some underrepresentation of these comorbidities in our study. Either for legal reasons or potential better healthcare treatment, the patients may have concealed their condition.
In our study, only 41.4% of the patients needed surgical intervention. This value is in accordance with available literature (29-58%).13,14,16,20 The majority of those patients (72.4%) were submitted to only one surgery.
In the group of patients with follow up at our Hospital for at least 12 months (50), there were 66% without any limitations or complaints. The most common sequelae were scar disturbances (24%) and scar contracture (14%). Zikai J. et al.13 had a similar rate of complications in their study, with 30.6% of the patients. Contracture rates in literature vary between 15.8%-23%.21,22 Holavanahalli et al.23 found a poor range of motion in 40% of the patients, but their study included only full-thickness dorsal hand burns with extensor mechanism included. Mohammadi et al.24 state that dorsal contractures are the most common complication of the burned hand. We did not find this to be true in our study as palmar wrist and volar digital contractures were more prevalent.
Higher age, HSA, HABS and deeper burns were associated with a higher probability of surgery. Bache et al.9 also identify a clear association of HABS values with the risk of surgery, with values above or equal to 6 entailing a high surgical risk. Wang et al.,13 besides depth of burn, also found male sex to be a predictor for surgery. In our study, gender was not associated with any of the variables studied (LOS, surgeries, worst outcomes).
Kowalske et al. state that outcomes after hand burns are influenced by several factors, namely depth of burn, edema, pain, neuropathy and compliance with the rehabilitation program.25 In our study, worst outcomes were associated with patients submitted to surgery (being worse with an increasing number of procedures), patients with higher HSA, and HABS. Schneider JC et al.22 indicate that the predictors for hand contractures are the size of the burn, the necessity of surgery, higher LOS, and additional comorbidities. Knight et al.19 refer that depth, TBSA, and pre-morbid health influence outcomes. Interestingly, in this study, the authors found a strong association between female gender and psychiatric disease and worse quality of life after the trauma. Our results seem to corroborate well with the ones obtained by Van der Vlies et al.26 In this paper, the authors found that the factors associated with the need for reconstructive surgery were the existence of surgeries (and their number) in the acute phase, extensive burns, and 3rd-degree burns. Regarding the depth of burn, even though there were differences in the outcomes, the results were not statistically significant.
Taking into account all the data collected, we believe there are several preventive measures and educational programs that need to be implemented in order to reduce the number and severity of the burns. A significant number of flame and hot liquid burns were sustained while cooking. The water temperature should be limited (in every room of the house), all individuals should wear high-temperature resistant gloves while cooking, and the use of alcohol and alcohol-derived products should be strongly contraindicated while having barbecues. We believe another priority should be to avoid the use of lamps/candles and fireplaces in old houses and to implement smoke detectors/alarms. The government should help the elderly population to set up proper electric and heating equipment in their households.
There are several limitations to take into account. Firstly, this is a retrospective study conducted in a single center. Despite the total patient sample being quite large (140), the number of patients with isolated hand burns (16) and with follow-up in our center (50) was much lower. The conclusions regarding some variables were affected by this small number. It is also very likely that there might be other contributing factors for hand function and quality of life after hand burns. The social support and the educational level of the patients seem to be important in the recovery process.4 Patient-reported outcomes are also a vital tool to understand how the patients perceive their recovery, independently of what they have achieved. Future studies should include the results of these types of reports.
Conclusion
This study found that a considerable amount of burn victims admitted to a dedicated burn center had hand burns (41.5%). Males are more likely to be injured in general, but females are more prevalent in burns by hot liquids. Cooking is the activity associated with more accidental victims. Most injuries did not require surgical intervention. Approximately two-thirds of the patients did not have any critical sequelae. The most common complications were scar disturbances (26%) and scar contractures (14%). The need for surgery, a higher number of surgeries, higher HSA and HBSA were associated with the worst outcomes.
It is imperative to establish a burn prevention education program nationwide, encompassing water temperature control in the households and the use of anti-burn equipment. Old or non-existent electrical/heating equipment should be replaced. The governmental regulatory entities should perform constant monitoring of the implementation of safety measures in all workplaces.
References
- 1.Smith MA, Munster MA, Spence RJ. Burns of the hand and upper limb - a review. Burns. 1998;24(6):493–505. doi: 10.1016/s0305-4179(98)00063-1. [DOI] [PubMed] [Google Scholar]
- 2.Corlew DS, McQueen KK. International disease burden of hand burns: perspective from the global health arena. and Clinics. 2017;33(2):399–407. doi: 10.1016/j.hcl.2016.12.010. [DOI] [PubMed] [Google Scholar]
- 3.Soni A, Pham TN, Ko JH. Acute management of hand burns. Hand Clinics. 2017;33(2):229–236. doi: 10.1016/j.hcl.2016.12.001. [DOI] [PubMed] [Google Scholar]
- 4.Johnson SP, Chung KC. Outcomes assessment after hand burns. Hand Clinics. 2017;33(2):389–397. doi: 10.1016/j.hcl.2016.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Edwards J, Mason S. Hand burn management: minimizing pain and trauma at dressing change. British Journal of Nursing. 2013;22(Sup20):S46–S50. doi: 10.12968/bjon.2013.22.Sup20.S46. [DOI] [PubMed] [Google Scholar]
- 6.Kowalske KJ, Greenhalgh DG, Ward SR. Hand burns. J Burn Care Res. 2007;28(4):607–610. doi: 10.1097/BCR.0B013E318093E4B9. [DOI] [PubMed] [Google Scholar]
- 7.Kowalske KJ. Hand burns. Physical medicine and rehabilitation clinics of North America. 2011;22(2):249–259. doi: 10.1016/j.pmr.2011.03.003. [DOI] [PubMed] [Google Scholar]
- 8.Gachie E, Casoli V. Séquelles de brûlures des mains. Annales de chirurgie plastique esthétique. 2011;56(5):454–465. doi: 10.1016/j.anplas.2011.09.003. [DOI] [PubMed] [Google Scholar]
- 9.Bache SE, O’Connor EF, Theodorakopoulou E, Frew Q. The Hand Burn Severity (HABS) Score: a simple tool for stratifying severity of hand burns. Burns. 2017;43(1):93–99. doi: 10.1016/j.burns.2016.07.011. [DOI] [PubMed] [Google Scholar]
- 10.Cartotto R. The burned hand: optimizing long-term outcomes with a standardized approach to acute and subacute care. Clin Plast Surgery. 2005;32(4):515–527. doi: 10.1016/j.cps.2005.05.009. [DOI] [PubMed] [Google Scholar]
- 11.Tredget EE. Management of the acutely burned upper extremity. Hand Clin. 2000;16:187–203. [PubMed] [Google Scholar]
- 12.Luce EA. The acute and subacute management of the burned hand. Clin Plast Surg. 2000;27:49–63. [PubMed] [Google Scholar]
- 13.Wang KA, Sun Y, Wu GS, Wang YR, Xia ZF. Epidemiology and outcome analysis of hand burns: a 5-year retrospective review of 378 cases in a burn center in Eastern China. Burns. 2015;41(7):1550–1555. doi: 10.1016/j.burns.2015.04.004. [DOI] [PubMed] [Google Scholar]
- 14.Zikaj G, Belba G, Xhepa G. Epidemiology of hand burn in Albania 2011-2016. Open access Macedonian Journal of Medical Sciences. 2018;6(5):931–931. doi: 10.3889/oamjms.2018.202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Arifi HM, Duci SB, Zatriqi VK, Ahmeti HR. A retrospective study of 572 patients with hand burns treated at the Department of Plastic Surgery Kosovo during the period 2000-2010. Int J Burns Trauma. 2014;4(1):7–7. [PMC free article] [PubMed] [Google Scholar]
- 16.Bache SE, O’Connor EF, Drake PJ, Philp B, Dziewulski P. Development and validation of the Burnt Hand Outcome Tool (BHOT): a patient-led questionnaire for adults with hand burns. Burns. 2018;44(8):2087–2098. doi: 10.1016/j.burns.2018.07.014. [DOI] [PubMed] [Google Scholar]
- 17.Sheridan RL, Baryza MJ, Pessina MA, O’Neill KM. Acute hand burns in children: management and long-term outcome based on a 10-year experience with 698 injured hands. Ann Surg. 1999;229(4):558–558. doi: 10.1097/00000658-199904000-00016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sheridan RL, Hurley J, Smith MA, Ryan CM. The acutely burned hand: management and outcome based on a ten-year experience with 1047 acute hand burns. J Trauma Acute Care Surg. 1995;39(3):406–411. doi: 10.1097/00005373-199503000-00022. [DOI] [PubMed] [Google Scholar]
- 19.Knight A, Wasiak J, Salway J, O’Brien L. Factors predicting health status and recovery of hand function after hand burns in the second year after hospital discharge. Burns. 2017;43(1):100–106. doi: 10.1016/j.burns.2016.07.025. [DOI] [PubMed] [Google Scholar]
- 20.Williams N, Stiller K, Greenwood J, Calvert P. Physical and quality of life outcomes of patients with isolated hand burns - a prospective audit. J Burn Care Res. 2012;33(2):188–198. doi: 10.1097/BCR.0b013e318242eeef. [DOI] [PubMed] [Google Scholar]
- 21.Antonopulos D, Danikas D, Dotsikas R, Nikolakopoulu G. The treatment of early and late hand contractures following burn injury (1978–1991) Ann MBC. 1992;30:100–101. [Google Scholar]
- 22.Schneider JC, Holavanahalli R, Helm P. Contractures in burn injury part II: investigating joints of the hand. J Burn Care Rehabil. 2008;29(4):606–613. doi: 10.1097/BCR.0b013e31817db8e1. [DOI] [PubMed] [Google Scholar]
- 23.Holavanahalli RK, Helm PA, Gorman AR, Kowalske KJ. Outcomes after deep full-thickness hand burns. Archives of Physical Medicine and Rehabilitation. 2007;88(12):S30–S35. doi: 10.1016/j.apmr.2007.09.010. [DOI] [PubMed] [Google Scholar]
- 24.Mohammadi AA, Mohammadi S. Hand aesthetic, an annoying problem for the burn patients, but commonly overlooked issue by the burn surgeons. Burns. 2017;43(5):1130–1131. doi: 10.1016/j.burns.2017.03.003. [DOI] [PubMed] [Google Scholar]
- 25.Kowalske K. Outcome assessment after hand burns. Hand Clinics. 2009;25(4):557–561. doi: 10.1016/j.hcl.2009.06.003. [DOI] [PubMed] [Google Scholar]
- 26.Van der Vlies CH, de Waard S, Hop J, Nieuwenhuis MK. Indications and predictors for reconstructive surgery after hand burns. J Hand Surgery. 2017;42(5):351–358. doi: 10.1016/j.jhsa.2017.02.006. [DOI] [PubMed] [Google Scholar]