

Abstract
We report a case of tibial shaft fracture after open‐wedge distal tibial tuberosity osteotomy (OWDTO). The use of a lag screw for a lateral hinge fracture in OWDTO requires careful postoperative rehabilitation and follow‐up. We discuss concerns related to the mechanical strength at the osteotomy site after OWDTO to prevent fracture.
Keywords: distal tibial tuberosity osteotomy, open‐wedge high tibial osteotomy, osteotomy, tibial shaft fracture
The use of a lag screw for a lateral hinge fracture in open‐wedge distal tibial tuberosity osteotomy (OWDTO) requires careful postoperative rehabilitation and follow‐up. Bi‐cortical fixations performed at the distal tibia in OWDTO may be recommended.

1. INTRODUCTION
Medial open‐wedge high tibial osteotomy (OWHTO) is an established treatment for osteoarthritis of varus knees. However, several recent studies have reported that OWHTO negatively impacts the patellofemoral joint by an increase in its pressure and patella infra, which leads to the progression of patellofemoral osteoarthritis. 1 , 2
Therefore, OWHTO with open‐wedge distal tibial tuberosity osteotomy (OWDTO) has been recommended to prevent patella infra, particularly for patients requiring large degrees of valgus correction. 3 In OWDTO, the tibial tuberosity remains attached to the proximal tibia, and the change in patellar height can be minimized. Several studies reported a significant difference in the progression of PF cartilage degradation after OWDTO compared with OWHTO. 4 , 5 While there are advantages of OWDTO, specific complications have been observed. Tibial tuberosity fracture is one of the specific complications of OWDTO, 3 , 6 and it can result in instability of the osteotomy site and delayed union or non‐union. A thinner descending osteotomy can cause tibial tuberosity fractures. On the contrary, a thicker descending osteotomy may increase the risk of fracture at the tibial shaft or lateral hinge. Several authors have reported an increased risk of tibial fracture when they used a technique in which complete tibial tubercle detachment was performed during tibial tuberosity osteotomy. 7 , 8 However, to the best of our knowledge, the biomechanical stability at the osteotomy site after OWDTO has not been much investigated. 9
This report describes a case of tibial shaft fracture at the osteotomy site on the tibial crest after OWDTO, wherein the thickness of the ascending osteotomy was appropriate. However, an additional screw hole used for the compression maneuver of the lateral hinge may have impaired the mechanical strength. The two mono‐cortical screw fixations of the four possible distal screw holes on the locking plate may also have caused insufficient stability when a lateral hinge fracture and an unexpected fracture of the diaphysis occurred. In this report, we discussed concerns related to the mechanical strength at the osteotomy site after OWDTO to prevent fracture.
2. CASE REPORT
A 61‐year‐old man had left knee pain, who did not respond to conservative treatment. The preoperative knee flexion was 145°, and 5° of flexion contracture was noted. His body mass index was 25.7. He had no smoking history. He underwent medial OWDTO with 9° valgus correction. 10 The surgical indication of OWDTO at our institution was as follows: (1) symptomatic medial OA or osteonecrosis, (2) varus malalignment requiring valgus correction of more than 10° by preoperative planning, and (3) patellofemoral joint space narrowing on radiograph or observation of symptoms caused by the joint. In the present case, patellofemoral joint space narrowing was observed on the radiograph; therefore, we performed OWDTO, not OWHTO. For distal tuberosity fixation, the TriS Medial HTO Plate® (Olympus Terumo Biomaterials, Japan) (Figure 1), which has eight screw holes and a 5.5‐mm locking screw, was used. Intraoperatively, a type I lateral hinge fracture was suspected 11 ; hence, an additional lag screw technique by using a 4.5‐mm cortical screw was applied at the distal second screw hole in a distally oblique direction to compress the lateral hinge. We used two bi‐cortical screws at the distal first and second screw holes and two mono‐cortical screws at the distal third and fourth screw holes for locking plate fixation. In addition, bi‐cortical screw fixation from the tuberosity to the posterior tibia was performed to support the descending osteotomy (Figure 2). Postoperative plain radiographs and computed tomography revealed the descending osteotomy with an arc‐shaped osteotomy line at the distal tuberosity that had been performed appropriately. The additional screw hole for the lag screw technique was observed on the lateral tibial wall near the second distal screw and the osteotomy line on the tibial crest. However, no unexpected fracture from the lateral distal edge of the descending osteotomy (arc osteotomy) to the distal second screw hole was observed (Figure 3). Partial weight‐bearing with the patient using two crutches was allowed at 1 week, and full weight‐bearing was started at 4 weeks postoperatively.
FIGURE 1.

TriS medial HTO plate® (Olympus Terumo Biomaterials). This locking plate has screw holes A through D above the osteotomy site and holes 1 through 4 below the osteotomy site. Generally, screw hole 1 or 2 is used to insert a compression lag screw
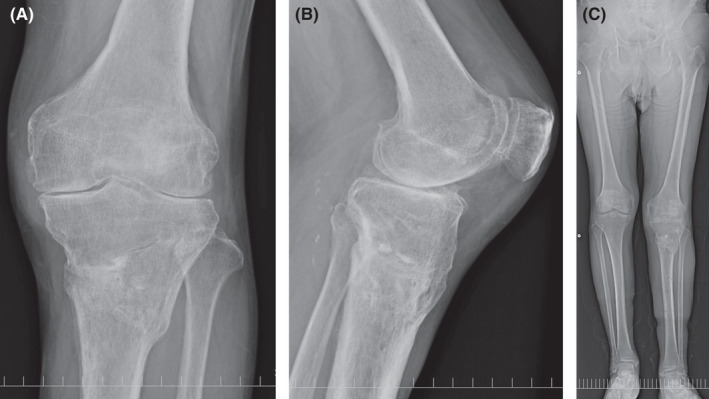
FIGURE 2.
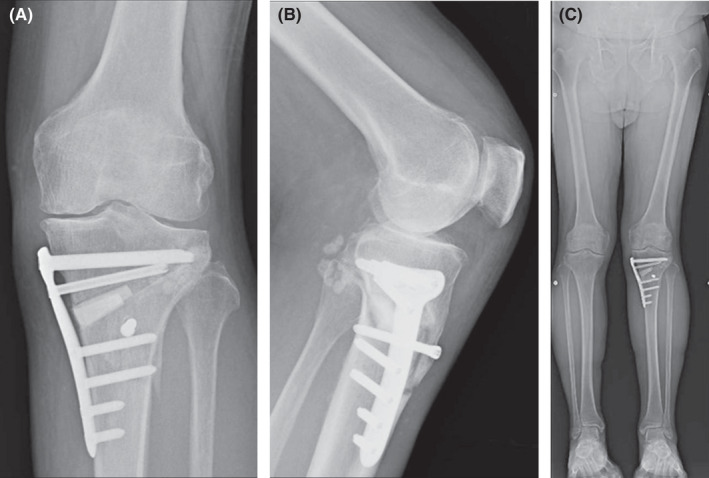
Radiographs after open‐wedge distal tuberosity osteotomy (postoperative 6 weeks). (A) Anteroposterior radiograph. Mono‐cortical screw fixation was performed at screw holes 3 and 4. (B) Lateral radiograph. Additional bi‐cortical screw fixation from the tuberosity to the posterior tibia was performed. (C) Whole‐leg standing radiograph. The hip‐knee‐ankle angle was corrected from 4° varus to 5.6° valgus
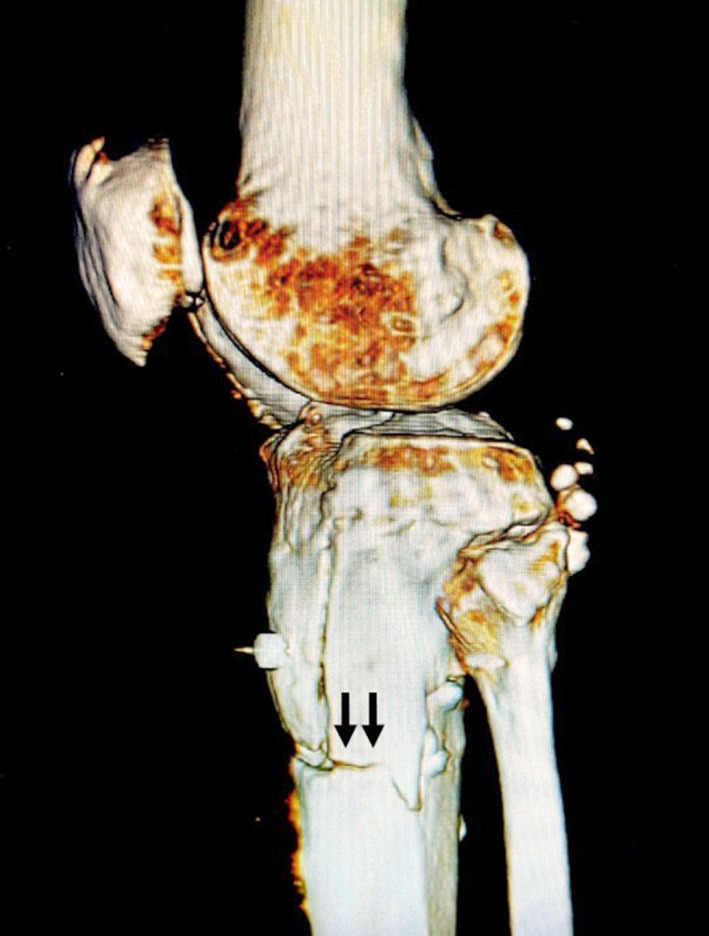
FIGURE 3.

Three‐dimensional computed tomography image after open‐wedge distal tuberosity osteotomy (postoperative 2 months). Asterisk shows the hole of the lag screw. The fracture line can be observed from the hole of the lag screw to screw hole 2 (arrows). No fracture was observed along the edge of the descending osteotomy
Although the bone union had not been observed yet at 2 months after surgery, the osteotomy site had been stable, and the patient's knee pain had reduced. However, severe knee pain recurred after the patient fell 3 months postoperatively, which posed challenges in walking. Upon presentation to the hospital, 1 week after the injury, a hematoma with a late infection around the HTO plate was detected. Moreover, an unexpected fracture from the lateral distal edge of the descending osteotomy (arc osteotomy) to the distal second screw hole was observed (Figure 4). To treat the infection, we immediately debrided the hematoma and assessed the stability of the fracture site. On the intraoperative stress test, the distal fragment was notably unstable because of an additional fracture of the lateral cortex. The two mono‐cortical screws on the locking plate offered unstable support to the distal part of the tibia; thus, we removed the plate (Figure 5). Methicillin‐susceptible Staphylococcus aureus was detected around the plate. Treatment with antibiotics, debridement, and external fixation was performed. After treating the infection, Ilizarov external fixation was performed with using an autologous bone graft (Figure 6). The duration of the external fixation was 7 months, and a low‐intensity pulsed ultrasound was also used. Bone union was achieved 1 year after the fracture, and the patient could walk independently with a cane even with slight knee pain (Figure 7). Postoperative limb alignment was 5.5° valgus, and the range of motion of the knee was from 0° extension to 95° flexion.
FIGURE 4.
Three‐dimensional computed tomography image after open‐wedge distal tuberosity osteotomy immediately prior to the second surgery. An unexpected fracture from the lateral distal edge of the descending osteotomy to the distal second screw hole was observed (arrows)
FIGURE 5.
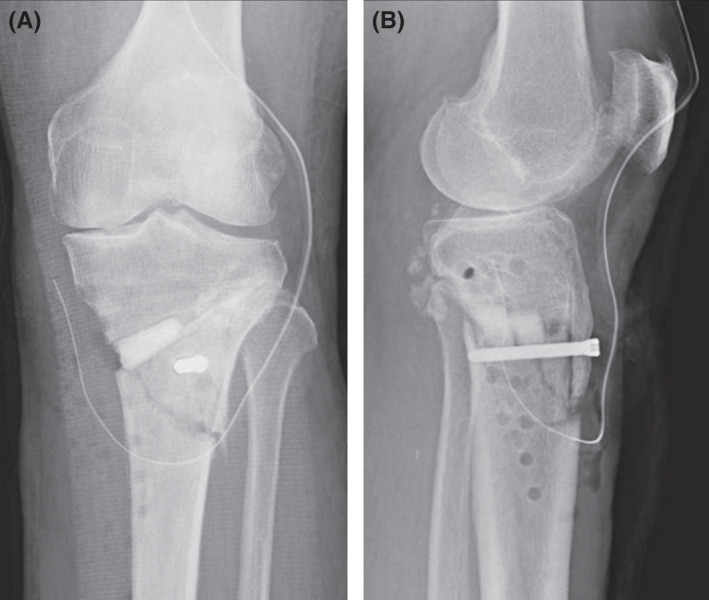
Radiographs obtained 3 months after open‐wedge distal tuberosity osteotomy. The patient was diagnosed with a tibial shaft fracture with surgical site infection triggered by a fall ((A) anteroposterior; (B) lateral)
FIGURE 6.
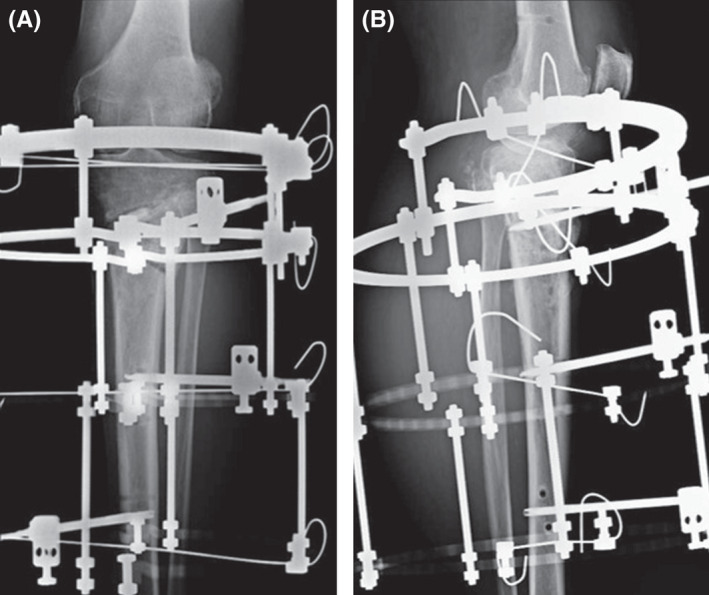
Postoperative radiograph of Ilizarov external fixation with autologous bone graft ((A) anteroposterior; (B) lateral)
FIGURE 7.
Latest follow‐up radiograph. Bone union was obtained 2 years after the tibial shaft fracture ((A) anteroposterior; (B) lateral; (C) standing whole leg). On an anterior‐posterior radiograph, the medial and lateral joint space was slightly narrowed compared with the preoperative radiograph
This case report was approved by the institutional review board of our hospital. The patient was informed that data from the case would be submitted for the publication and gave consent.
3. DISCUSSION
Open‐wedge distal tibial tuberosity osteotomy is advocated as an alternative to OWHTO to prevent patella infra. However, an osteotomy on the tibial crest distal to the descending tuberosity may impair the mechanical strength of the tibial shaft, which can lead to fracture. In the current case, an additional screw hole for the compression lag screw technique close to the osteotomy line may have increased this risk. In addition, it was possible that the two mono‐cortical screws for distal fixation of the locking plate offered insufficient strength to hold the distal fragment when the fracture occurred at the distal tuberosity. Thus, the prolonged bone healing was likely due to the instability of the osteotomy caused by the fracture of the tibial tuberosity.
In this case, a type I hinge fracture was observed intraoperatively, and the cortical screw was inserted in a direction that was different from that of the usual locking screw to compress the lateral hinge. This procedure may have further increased the risk of fracture by creating another hole at the lateral cortex near the distal second screw and the anterior osteotomy site. Although the compression lag screw technique is useful for the reduction of displaced type I hinge fractures, using the same screw hole as one of the locking screws is suggested to avoid creating another screw hole on the lateral cortex of the tibia and to prevent the unexpected fracture. In addition, a type I hinge fracture may provide a more unstable situation in OWDTO compared with OWHTO. The use of a lag screw for a type I hinge fracture in OWDTO requires careful postoperative rehabilitation and follow‐up, and further studies would be required to evaluate the biomechanical effects of lateral hinge fracture in OWDTO.
Mono‐cortical screw fixation for locking plates is performed when there are several screw holes far from the osteosynthesis site, which is also adopted in OWHTO using a long locking plate. Meanwhile, deep peroneal nerve injury has been described as a complication of OWHTO with a locking plate. 12 , 13 To avoid this risk, mono‐cortical fixation of several of the distal screws is recommended. Finite element analysis of mono‐cortical fixation for three distal screws (2, 3, and 4) of the locking plate showed no impairment of biomechanical stability as compared with bi‐cortical fixation for all four distal screws in OWHTO. 14 However, the mechanical properties of the tibia after OWDTO are different from those after OWHTO, particularly the anterior osteotomy line that is located on the diaphysis in OWDTO, while it is located on the metaphysis in OWHTO. To the best of our knowledge, no study has presented any investigation of the stability of mono‐cortical fixation of distal screws in OWDTO. We ascertained that if the descending osteotomy was thicker and the direction of the osteotomy was turned to posterolateral, the lateral distal edge of the descending osteotomy would be closer to the distal second screw, which could present risks for accidental fracture between the two points. When there is a fracture in that area, mechanical stress may be concentrated in the distal third and fourth screws, which is distinctly different from the situation in OWHTO. Mono‐cortical screws in these holes would be insufficient to maintain the stability of the osteotomy site. All of the bi‐cortical fixations for all four distal screws may be recommended in OWDTO. Further biomechanical studies should be conducted to determine the differences in stability between bi‐ and mono‐cortical screws at the distal tibia in OWDTO.
Open‐wedge distal tibial tuberosity osteotomy has been drawing attention as a valuable surgical option for osteoarthritis with varus knee, especially for patients with patella infra or patellofemoral joint degeneration. 4 , 5 , 15 , 16 Its difference from OWHTO is the descending osteotomy at the tibial tuberosity. Concerning the abovementioned complications, if a lateral hinge fracture occurs, the compression lag screw should be inserted in the same direction as the locking screw, and the use of a lag screw in OWDTO requires careful postoperative rehabilitation and follow‐up. Bi‐cortical fixation may be recommended to be performed at the distal tibia in OWDTO. In addition, care must be taken to prevent cutting in the posterolateral direction in the descending osteotomy to preserve space of the lateral tibial cortex for distal bi‐cortical screw fixation.
CONFLICTS OF INTEREST
KO received lecture fees from Olympus Terumo Biomaterials.
AUTHOR CONTRIBUTION
UK involved in the conception and design of the study, or acquisition of data, or analysis and interpretation of data, and drafting the article. MI and JI involved in drafting the article or revising it critically for important intellectual content. KO involved in drafting the article or revising it critically for important intellectual content, and final approval of the version to be submitted. All the authors agree to be accountable for all aspects of the work.
ETHICAL APPROVAL
This study was approved by the Institutional Ethics Commission (No.4578).
CONSENT
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
ACKNOWLEDGEMENTS
None.
Kuwashima U, Itoh M, Itou J, Okazaki K. Tibial shaft fracture after medial open‐wedge distal tibial tuberosity osteotomy: A case report. Clin Case Rep. 2022;10:e05697. doi: 10.1002/ccr3.5697
Funding information
There were no funding sources
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
- 1. Kim KI, Kim DK, Song SJ, Lee SH, Bae DK. Medial open‐wedge high tibial osteotomy may adversely affect the patellofemoral joint. Arthroscopy. 2017;33(4):811‐816. doi: 10.1016/j.arthro.2016.09.034 [DOI] [PubMed] [Google Scholar]
- 2. Goshima K, Sawaguchi T, Shigemoto K, Iwai S, Nakanishi A, Ueoka K. Patellofemoral osteoarthritis progression and alignment changes after open‐wedge high tibial osteotomy do not affect clinical outcomes at mid‐term follow‐up. Arthroscopy. 2017;33(10):1832‐1839. doi: 10.1016/j.arthro.2017.04.007 [DOI] [PubMed] [Google Scholar]
- 3. Gaasbeek RD, Sonneveld H, van Heerwaarden RJ, Jacobs WC, Wymenga AB. Distal tuberosity osteotomy in open wedge high tibial osteotomy can prevent patella infera: a new technique. Knee. 2004;11(6):457‐461. doi: 10.1016/j.knee.2004.02.002 [DOI] [PubMed] [Google Scholar]
- 4. Horikawa T, Kubota K, Hara S, Akasaki Y. Distal tuberosity osteotomy in open‐wedge high tibial osteotomy does not exacerbate patellofemoral osteoarthritis on arthroscopic evaluation. Knee Surg Sports Traumatol Arthrosc. 2020;28(6):1750‐1756. doi: 10.1007/s00167-019-05596-y [DOI] [PubMed] [Google Scholar]
- 5. Ogawa H, Matsumoto K, Yoshioka H, Sengoku M, Akiyama H. Distal tibial tubercle osteotomy is superior to the proximal one for progression of patellofemoral osteoarthritis in medial opening wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2020;28(10):3270‐3278. doi: 10.1007/s00167-019-05836-1 [DOI] [PubMed] [Google Scholar]
- 6. Park H, Kim HW, Kam JH, Lee DH. Open wedge high tibial osteotomy with distal tubercle osteotomy lessens change in patellar position. BioMed Res Int. 2017;2017:4636809. doi: 10.1155/2017/4636809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Luhmann SJ, Fuhrhop S, O’Donnell JC, Gordon JE. Tibial fractures after tibial tubercle osteotomies for patellar instability: a comparison of three osteotomy configurations. J Child Orthop. 2011;5(1):19‐26. doi: 10.1007/s11832-010-0311-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Stetson WB, Friedman MJ, Fulkerson JP, Cheng M, Buuck D. Fracture of the proximal tibia with immediate weightbearing after a Fulkerson osteotomy. Am J Sports Med. 1997;25(4):570‐574. doi: 10.1177/036354659702500422 [DOI] [PubMed] [Google Scholar]
- 9. Zhim F, Laflamme GY, Viens H, Laflamme GH, Yahia L. Biomechanical stability of a retrotubercle opening‐wedge high tibial osteotomy. J Knee Surg. 2006;19(1):28‐32. doi: 10.1055/s-0030-1248073 [DOI] [PubMed] [Google Scholar]
- 10. Akiyama T, Osano K, Mizu‐Uchi H, et al. Distal tibial tuberosity arc osteotomy in open‐wedge proximal tibial osteotomy to prevent patella infra. Arthrosc Tech. 2019;8(6):e655‐e662. doi: 10.1016/j.eats.2019.02.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Takeuchi R, Ishikawa H, Kumagai K, et al. Fractures around the lateral cortical hinge after a medial opening‐wedge high tibial osteotomy: a new classification of lateral hinge fracture. Arthroscopy. 2012;28(1):85‐94. doi: 10.1016/j.arthro.2011.06.034 [DOI] [PubMed] [Google Scholar]
- 12. Itoh M, Itou J, Kuwashima U, Fujieda H, Okazaki K. Deep peroneal nerve injury during plate fixation for medial open‐wedge high tibial osteotomy: a case report and cadaveric study. Clin Case Rep. 2019;7(11):2225‐2230. doi: 10.1002/ccr3.2451 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Itou J, Itoh M, Maruki C, et al. Deep peroneal nerve has a potential risk of injury during open‐wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2020;28(5):1372‐1379. doi: 10.1007/s00167-019-05445-y [DOI] [PubMed] [Google Scholar]
- 14. Itou J, Kuwashima U, Itoh M, Kuroda K, Yokoyama Y, Okazaki K. Monocortical fixation for locking plate distal screws does not impair mechanical properties in open‐wedge high tibial osteotomy. BMC Musculoskelet Disord. 2021;22(1):157. doi: 10.1186/s12891-021-03999-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Erquicia J, Gelber PE, Perelli S, et al. Biplane opening wedge high tibial osteotomy with a distal tuberosity osteotomy, radiological and clinical analysis with minimum follow‐up of 2 years. J Exp Orthop. 2019;6(1):10. doi: 10.1186/s40634-019-0176-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Han C, Li X, Tian X, et al. The effect of distal tibial tuberosity high tibial osteotomy on postoperative patellar height and patellofemoral joint degeneration. J Orthop Surg Res. 2020;15(1):466. doi: 10.1186/s13018-020-01996-w [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.