

Key Points
Question
Are there differences in cerebrospinal fluid (CSF) biomarkers between patients with unipolar depression and healthy control individuals?
Findings
In this systematic review and meta-analysis of 97 studies, CSF levels of interleukin 6, total protein, and cortisol were higher among patients with unipolar depression, whereas levels of homovanillic acid, γ-aminobutyric acid, somatostatin, brain-derived neurotrophic factor, amyloid-β 40, and transthyretin were lower. However, the number of eligible studies was limited for most of the identified biomarkers, and analyses revealed substantial heterogeneity among studies.
Meaning
This study found numerous biomarkers in the CSF were altered in individuals with unipolar depression, indicating a multifactorial pathogenesis implicating several neurocircuits; however, high-quality studies investigating multiple CSF markers are needed.
This systematic review and meta-analysis evaluates differences in cerebrospinal fluid biomarkers among individuals with unipolar depression and healthy control individuals.
Abstract
Importance
Depression has been associated with alterations in neurotransmitters, hormones, and inflammatory and neurodegenerative biomarkers, and biomarkers quantified in the cerebrospinal fluid (CSF) are more likely to reflect ongoing biochemical changes within the brain. However, a comprehensive overview of CSF biomarkers is lacking and could contribute to the pathophysiological understanding of depression.
Objective
To investigate differences in quantified CSF biomarkers in patients with unipolar depression compared with healthy control individuals.
Data Sources
PubMed, EMBASE, PsycINFO, Cochrane Library, Web of Science, and ClinicalTrials.gov were searched for eligible trials from database inception to August 25, 2021.
Study Selection
All studies investigating CSF biomarkers in individuals 18 years and older with unipolar depression and healthy control individuals were included. One author screened titles and abstracts, and 2 independent reviewers examined full-text reports. Studies that did not include healthy control individuals or included control individuals with recent hospital contacts or admissions that might affect CSF biomarker concentrations were excluded.
Data Extraction and Synthesis
Data extraction and quality assessment were performed by 2 reviewers following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) and Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guidelines. Meta-analyses were performed using standardized mean differences (SMDs) calculated with random-effects models. A third investigator was consulted if the 2 reviewers reached different decisions or when in doubt.
Main Outcomes and Measures
Quantifiable CSF biomarkers.
Results
A total of 167 studies met eligibility criteria, and 97 had available data and were included in the meta-analysis. These 97 studies comprised 165 biomarkers, 42 of which were quantified in 2 or more studies. CSF levels of interleukin 6 (7 studies; SMD, 0.35; 95% CI, 0.12 to 0.59; I2 = 16%), total protein (5 studies; SMD, 0.53; 95% CI, 0.35 to 0.72; I2 = 0%), and cortisol (2 studies; SMD, 1.23; 95% CI, 0.89 to 1.57; I2 = 0%) were higher in patients with unipolar depression compared with healthy control individuals, whereas homovanillic acid (17 studies; SMD, −0.26; 95% CI, −0.39 to −0.14; I2 = 11%), γ-aminobutyric acid (4 studies; SMD, −0.50; 95% CI, −0.92 to −0.08; I2 = 55%), somatostatin (5 studies; SMD, −1.49; 95% CI, −2.53 to −0.45; I2 = 91%), brain-derived neurotrophic factor (3 studies; SMD, −0.58; 95% CI, −0.97 to −0.19; I2 = 0%), amyloid-β 40 (3 studies; SMD, −0.80; 95% CI, −1.14 to −0.46; I2 = 0%), and transthyretin (2 studies; SMD, −0.82; 95% CI, −1.37 to −0.27; I2 = 0%) were lower. The remaining 33 biomarkers had nonsignificant results.
Conclusions and Relevance
The findings of this systematic review and meta-analysis point toward a dysregulated dopaminergic system, a compromised inhibitory system, hypothalamic-pituitary-adrenal axis hyperactivity, increased neuroinflammation and blood-brain barrier permeability, and impaired neuroplasticity as important factors in depression pathophysiology.
Introduction
Globally, more than 264 million people experience depression, which is the third leading cause of years lived with disability.1 However, depression pathophysiology is not fully elucidated despite multiple hypotheses. Whereas monoamine depletion forms the background for most antidepressant medication,2 depression has also been associated with imbalances in the glutamatergic and γ-aminobutyric acid (GABA) systems,3 hyperactivity of the hypothalamic-pituitary-adrenal (HPA) axis,4 increased inflammation,5 and reduced neuroplasticity.6 To improve future diagnostics and treatment, it is important to advance insight into the underlying biological mechanisms by identifying quantifiable biomarkers of depression. Cerebrospinal fluid (CSF) reflects ongoing biochemical changes in the brain and is considered a good medium for biomarker research, as it is the material closest to the brain, is easily accessible for clinical investigations, and plays a key role in the exchange and clearance of molecules in the interstitial space of the central nervous system.7 However, previous meta-analyses in this field have been limited to certain specific biomarkers, and to our knowledge, no comprehensive meta-analysis of all CSF biomarkers in unipolar depression exists. Additionally, many earlier meta-analyses do not distinguish unipolar and bipolar depression, and some include both neurological and surgical patients as control individuals.
Here, we conducted what we believe to be the first comprehensive systematic review and meta-analysis primarily investigating differences in all quantified CSF biomarkers from patients with unipolar depression compared with healthy control individuals. We also investigated associations between biomarker levels with psychopathology, prognosis, antidepressant treatment, and levels in blood. This comprehensive and broad approach to investigation of current CSF biomarker research may help advance our understanding of the multifactorial pathogenesis of depression.
Methods
The study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) and Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guidelines for conducting and reporting systematic reviews (eTables 1 and 2 in the Supplement). The study protocol was published on PROSPERO (CRD42020222357).
Search Strategy and Selection Criteria
We included clinical studies fulfilling the following criteria: investigated quantifiable biomarkers in CSF obtained from living human study participants, included patients 18 years and older with a primary diagnosis of unipolar depression according to a diagnostic system (eg, International Classification of Diseases [ICD], DSM, or Research Diagnostic Criteria [RDC]), compared patients with healthy control individuals, had cohorts of 10 or more individuals, were published in peer-reviewed journals, and were published in English. Studies were excluded if they contained previously published data; had a control group of patients admitted to the hospital (eg, for a surgical procedure requiring spinal anesthesia or a neurological examination with lumbar puncture) (eTable 9 in the Supplement) or participants with an inflammatory, psychiatric, or neurological disease that might affect CSF biomarker concentrations; or used methods not directly quantifying biomarkers in the CSF (eg, proton magnetic resonance spectroscopic imaging). No exclusions were made by time period, sex, or race and ethnicity. All publications in PubMed, EMBASE, PsycINFO, Cochrane Library, Web of Science, and ClinicalTrials.gov were included from database inception to August 25, 2021. An information specialist at the Royal Danish Library was consulted to review the query in the respective databases. The search string is presented in eTable 3 in the Supplement.
Data Extraction
One author (I.V.M.) extracted data, and another author (N.V.S.) quality checked all extracted data. To include only individuals with unipolar depression, the following reservations were made. If a diagnosis of major depression or major depressive disorder was given according to DSM-III, DSM-IV, DSM-V, ICD-9, or ICD-10, the study was included, as these diagnostic criteria exclude former manic or hypomanic episodes. If a diagnosis of a major depressive episode had been given, the study was included only when the study excluded previous manic episodes. If a diagnosis of depression was given according to RDC,8 Feighner,9 or the Newcastle Inventory10 the study was excluded, as these diagnoses do not exclude bipolar depression, unless the study specified that only patients with unipolar depression were included. If studies included patients with bipolar and unipolar depression, only data from the patients with unipolar depression were extracted. In all cases of uncertainty or missing data, authors were contacted to provide further information with a reminder in case of no response (eTable 8 in the Supplement).
Our primary outcome was differences between patients with unipolar depression and healthy control individuals in any kind of biomarker measured in the CSF. Where appropriate data were available, we sought to investigate the following secondary outcomes: associations between CSF biomarkers and psychopathology, cognition, or functioning (eg, symptom rating scales, such as Hamilton Depression Score [HAM-D]); changes in biomarker levels after treatment with psychotropic drugs; associations between CSF biomarkers and prognosis; and associations between CSF biomarkers and findings in blood.
Bias Assessment
Two authors (I.V.M. and N.V.S.) conducted bias assessment of included studies according to the Newcastle-Ottawa criteria11 as suggested by Cochrane. For biomarkers quantified in 10 or more studies, the risk of publication bias was assessed with funnel plots. For biomarkers quantified in 5 or more studies, subgroup analyses compared a total score of 4 or higher vs less than 4 on the Newcastle-Ottawa Scale, and publication before and after the year 2000. When quantified in 10 or more studies, meta-regression analyses associating publication year with SMD were presented. To rate the quality of evidence, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) instrument12 was applied for each biomarker quantified in 2 or more studies.
Statistical Analysis
Meta-analyses were performed using standardized mean differences (SMDs). Only results from random-effects models are presented in the article, whereas both random-effects and fixed-effects models are presented in eFigures 2 to 6 in the Supplement. Random-effects meta-analyses were made using the DerSimonian-Laird estimator13 of the between-study variance τ2,14 with the inverse-variance weighting method. Estimates of SMDs were bias-corrected using Hedges g.15,16 χ2 tests for heterogeneity were performed and I2 was calculated to assess heterogeneity.17 The Egger test was used to assess possible publication bias.18 When necessary, means and standard deviations were imputed using information on medians, quartiles, and ranges. Meta-regression was used to associate effect sizes with the average number of participants (harmonic mean) in treatment arms. All statistical analyses were conducted in R version 4.02 (The R Foundation) using the meta-package.19 P values less than .05 were considered statistically significant, and all P values were 2-sided.
To investigate associations between biomarker levels and depression severity across studies, we performed meta-regression associating mean HAM-D score and biomarker level when given in 10 or more studies and subgroup analyses of inpatient or outpatient status when provided in 5 or more studies. To examine whether the length of medication discontinuation before lumbar puncture affected biomarker level, we performed subgroup analyses on studies with 14 days or less compared with more than 14 days of pause when given in 5 or more studies.
Results
We identified 11 926 studies after removal of duplicates, of which 631 full-text articles were assessed for eligibility and 167 met the inclusion criteria (eFigure 1 in the Supplement). Of these, 97 studies comprised data appliable for conducting meta-analyses, either published or sent to us by the authors. For the remaining 70 studies, numeric biomarker levels were not reported and could not be obtained from the authors. The details and characteristics of all 167 studies, including all references, are described in eTable 4 in the Supplement. A total of 165 biomarkers were identified, 42 of which were quantified in 2 or more studies and are presented in Table 1. Forest plots of the significant results are shown in Figure 1,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40 Figure 2,26,29,32,41,42,43,44,45,46 and Figure 3,34,47,48,49,50,51,52,53,54,55,56,57,58,59,60 and the biomarkers’ functions are listed in Table 2.4,5,32,61,62,63,64,65,66,67,68,69,70 All forest plots, including fixed-effects models, are accessible in eFigures 2 through 5 in the Supplement. The remaining 123 biomarkers quantified in only 1 study are presented in eFigure 6 in the Supplement. An overview of the function and association with depression of the 165 biomarkers is provided in eTable 5 in the Supplement. Subgroup, sensitivity, and bias assessment analyses are presented in eFigures 7 through 14 in the Supplement.
Table 1. Biomarkers in the Cerebrospinal Fluid (CSF) in Individuals With Depression Compared With Healthy Control Individuals Measured in 2 or More Studiesa.
| CSF marker | No. of studies | Individuals with depression, No. | Control individuals, No. | SMD (95% CI) | P value | I2, % |
|---|---|---|---|---|---|---|
| Neurotransmitters and their metabolites | ||||||
| HVA | 17 | 684 | 681 | −0.26 (−0.39 to −0.14) | <.001 | 11 |
| 5-HIAA | 15 | 566 | 558 | −0.04 (−0.28 to 0.19) | .72 | 66 |
| MHPG | 14 | 581 | 517 | 0.11 (−0.14 to 0.36) | .38 | 70 |
| GABA | 4 | 180 | 111 | −0.50 (−0.92 to −0.08) | .02 | 55 |
| Glutamate | 4 | 90 | 93 | 0.21 (−0.79 to 1.21) | .68 | 88 |
| Glutamine | 4 | 90 | 94 | 0.33 (−0.15 to 0.82) | .18 | 54 |
| Hormones | ||||||
| Cortisol | 2 | 77 | 81 | 1.23 (0.89 to 1.57) | <.001 | 0 |
| Transthyretin | 2 | 25 | 39 | −0.82 (−1.37 to −0.27) | .003 | 0 |
| CRH | 8 | 169 | 210 | −0.02 (−0.39 to 0.34) | .91 | 62 |
| ACTH | 2 | 39 | 139 | 0.07 (−0.29 to 0.42) | .72 | 0 |
| Oxytocin | 2 | 36 | 39 | −0.34 (−0.79 to 0.12) | .15 | 0 |
| Vasopressin | 2 | 56 | 43 | −0.07 (−0.47 to 0.33) | .74 | 0 |
| Neuropeptides | ||||||
| Somatostatin | 5 | 130 | 113 | −1.49 (−2.53 to −0.45) | .005 | 91 |
| NPY | 5 | 172 | 101 | −0.34 (−1.37 to 0.69) | .52 | 93 |
| Substance P | 2 | 51 | 58 | 0.71 (−0.15 to 1.57) | .11 | 70 |
| CART | 2 | 69 | 30 | −0.42 (−1.04 to 0.20) | .18 | 30 |
| Orexin | 2 | 29 | 22 | −0.25 (−0.81 to 0.31) | .39 | 0 |
| Amino acids and derivates | ||||||
| D-serine | 3 | 55 | 56 | 0.43 (−0.15 to 1.02) | .14 | 52 |
| L-serine | 3 | 55 | 56 | 0.16 (−0.64 to 0.96) | .69 | 75 |
| Serine | 2 | 51 | 64 | 0.60 (−0.36 to 1.57) | .22 | 70 |
| Glycine | 3 | 79 | 83 | 0.07 (−0.38 to 0.52) | .76 | 43 |
| Tryptophan | 2 | 37 | 54 | −0.22 (−0.64 to 0.20) | .30 | 0 |
| Tyrosine | 2 | 56 | 72 | −0.07 (−0.45 to 0.31) | .71 | 9 |
| Aspartate | 2 | 33 | 47 | −0.79 (−2.44 to 0.87) | .35 | 88 |
| Methionine | 2 | 56 | 72 | −0.17 (−0.52 to 0.18) | .35 | 0 |
| Ascorbic acid | 2 | 42 | 36 | 0.40 (−0.67 to 1.48) | .46 | 81 |
| Inflammatory markers | ||||||
| IL-6 | 7 | 156 | 229 | 0.35 (0.12 to 0.59) | .003 | 16 |
| IL-8 | 5 | 234 | 297 | 0.12 (−0.21 to 0.45) | .46 | 66 |
| TNF-α | 2 | 50 | 72 | 0.23 (−0.13 to 0.59) | .21 | 0 |
| White cell count | 3 | 184 | 195 | 0.05 (−0.23 to 0.33) | .72 | 42 |
| MMP-3 | 2 | 141 | 148 | 0.14 (−0.09 to 0.38) | .22 | 0 |
| Blood-brain barrier permeability | ||||||
| Total protein | 5 | 220 | 261 | 0.53 (0.35 to 0.72) | <.001 | 0 |
| Albumin ratio | 2 | 40 | 81 | 0.51 (−0.26 to 1.29) | .19 | 62 |
| Glucose | 2 | 99 | 114 | 0.04 (−0.23 to 0.31) | .78 | 0 |
| Synaptic plasticity | ||||||
| BDNF | 3 | 46 | 62 | −0.58 (−0.97 to −0.19) | .004 | 0 |
| NCAM | 2 | 187 | 229 | −0.11 (−0.31 to 0.08) | .24 | 0 |
| Neurodegeneration | ||||||
| Amyloid-β 40 | 3 | 71 | 81 | −0.80 (−1.14 to −0.46) | <.001 | 0 |
| Total τ | 9 | 153 | 283 | −0.32 (−0.70 to 0.06) | .10 | 66 |
| P-τ 181 | 6 | 114 | 154 | −0.02 (−0.28 to 0.24) | .88 | 0 |
| Amyloid-β 42 | 8 | 140 | 248 | 0.07 (−0.48 to 0.62) | .80 | 82 |
| Neurogranin | 2 | 34 | 63 | −0.17 (−0.65 to 0.32) | .50 | 0 |
| NfL | 2 | 27 | 85 | 0.01 (−1.38 to 1.39) | .99 | 88 |
Abbreviations: ACTH, adrenocorticotropic hormone; BDNF, brain-derived neurotrophic factor; CART, cocaine- and amphetamine-regulated transcript; CRH, corticotropin-releasing hormone; GABA, γ-aminobutyric acid; HIAA, hydroxyindoleacetic acid; HVA, homovanillic acid; IL, interleukin; MHPG, 3-methoxy–4-hydroxyphenylglycol; MMP, matrix metalloproteinase; NCAM, neural cell adhesion molecule; NfL, neurofilament light; NPY, neuropeptide Y; SMD, standard mean difference; TNF, tumor necrosis factor.
The table displays only results from random-effects models.
Figure 1. Neurotransmitters and Their Metabolites: Significant Differences in the Cerebrospinal Fluid in Individuals With Depression Compared With Healthy Control Individuals Measured in 2 or More Studies.
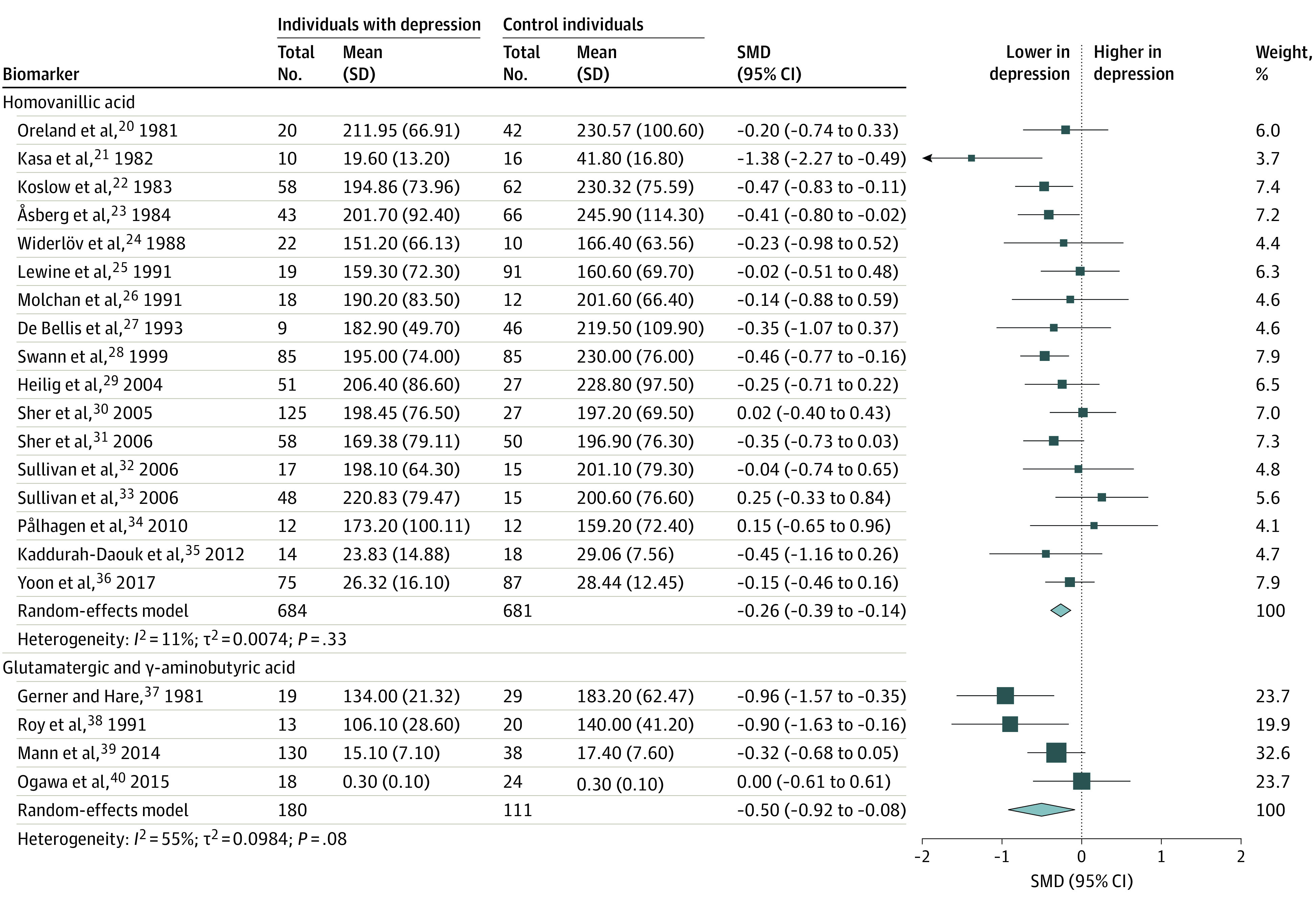
GABA indicates glutamatergic and γ-aminobutyric acid.
Figure 2. Hormones and Neuropeptides: Significant Differences in the Cerebrospinal Fluid in Individuals With Depression Compared With Healthy Control Individuals Measured in 2 or More Studies.
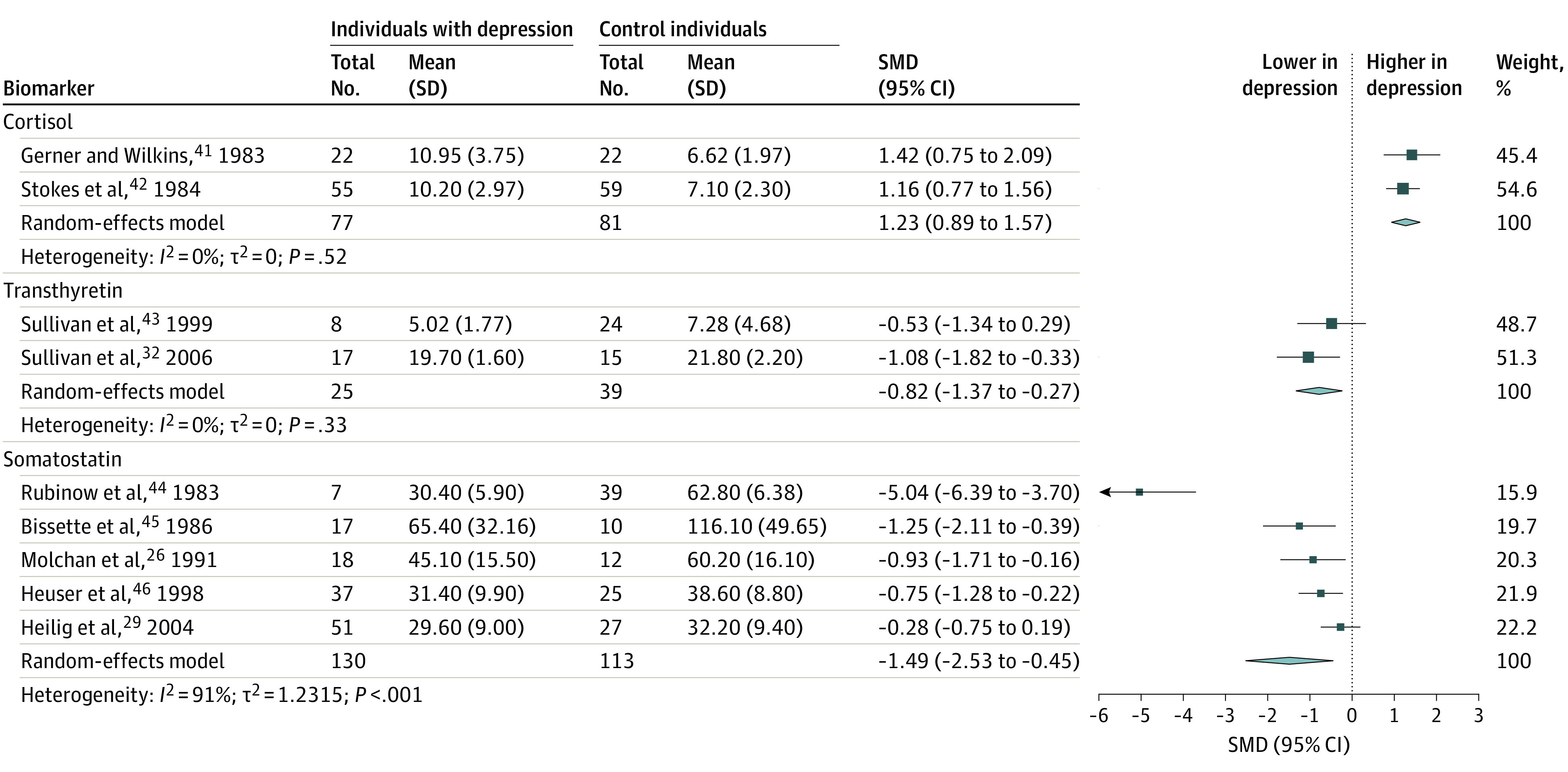
Figure 3. Inflammation, Blood-Brain Barrier Permeability, Neurodegeneration, and Synaptic Plasticity: Significant Differences in the Cerebrospinal Fluid in Individuals With Depression Compared With Healthy Control Individuals Measured in 2 or More Studies.
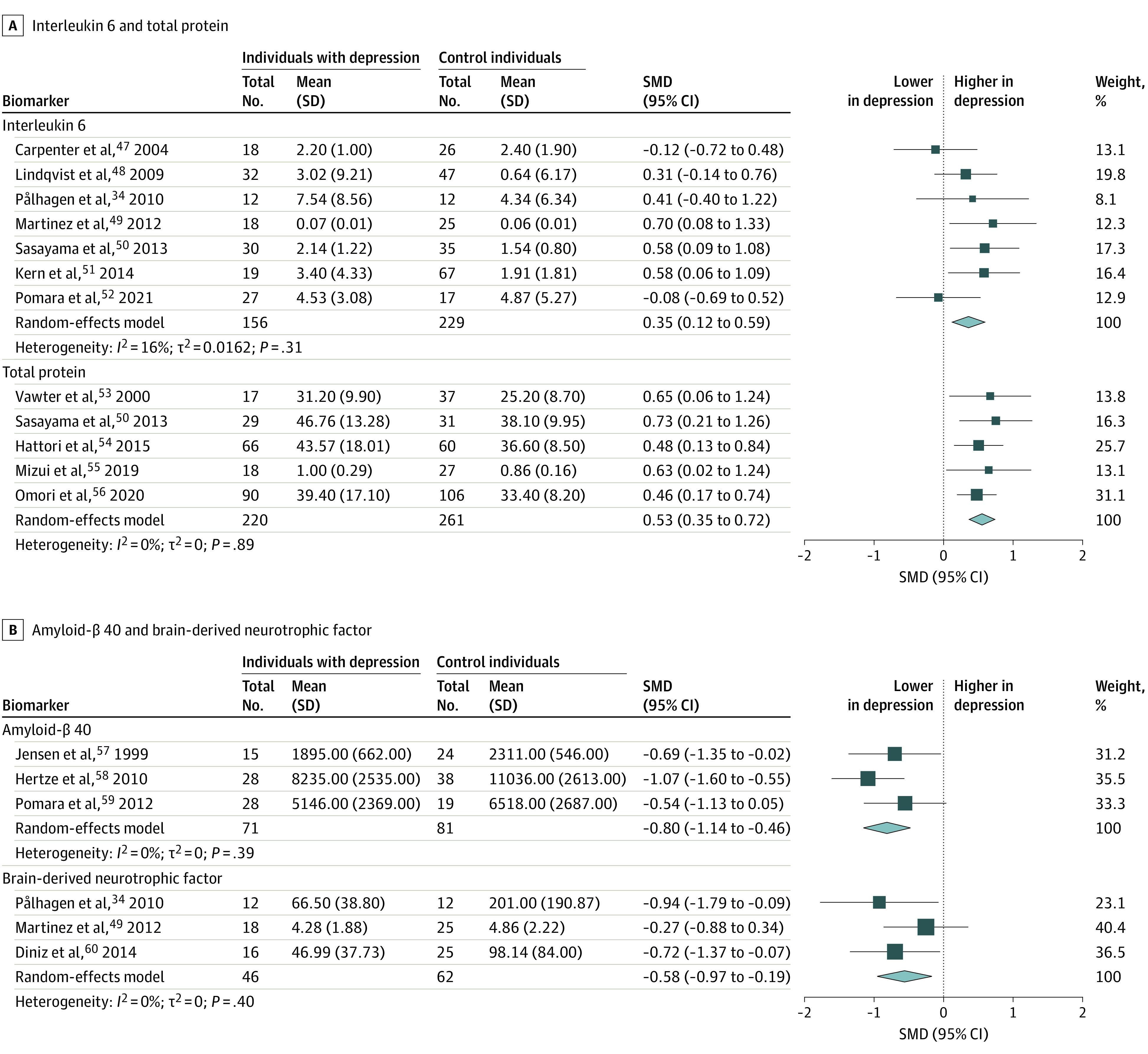
Table 2. Biomarkers in 2 or More Studies That Were Significantly Different in Patients With Depression and a Brief Description of Their Function.
| Biomarker | Description |
|---|---|
| HVA | Dopamine is a neurotransmitter involved in the experience of pleasure, motivation, and reward. Decreased levels have repeatedly been associated with depression. HVA is the final excretion product of dopamine and reflects dopamine levels in the brain.61 |
| GABA | GABA is the major inhibitory neurotransmitter in the CNS suggested to play a vital role in the control of stress and depression. GABA deficiency has repeatedly been observed in patients with depression. This may result in local hyperexcitability leading to compromised neurogenesis and HPA axis hyperactivity; factors also presumed to be important in depression.62 |
| Cortisol | Cortisol is a glucocorticoid secreted from the adrenal cortex on activation of the HPA axis. Prolonged psychological stress can increase levels of cortisol, which repeatedly has been observed in patients with depression. This may affect several systems, including the release of inflammatory markers, increased excitotoxic effects, and reduced neurogenesis.4,63 |
| TTR/prealbumin | TTR or prealbumin is a transport protein synthesized in the choroid plexus. TTR is involved in the transport of T4 across the BBB. Lower levels of CSF TTR have been reported in individuals with depression and is thought to reduce T4 levels in the brain and thus induce depressive symptoms similar to those associated with global hypothyroidism.32 |
| SS | SS is a peptide synthesized both in the endocrine pancreas, the gastrointestinal tract and in the periventricular region of the hypothalamus.64 In the CNS, SS acts as an inhibitory and modulatory neuropeptide often coexpressed and coreleased with GABA.65 SS deficiency has been associated with depression because it can affect physiological and behavioral stress responses and induce serotonin release, is associated with BNDF levels, and exhibits general inhibitory effects.64,65 |
| IL-6 | IL-6 is a part of the group of proinflammatory cytokines that has been suggested to induce sickness behavior in patients with depression, and increased levels in blood and CSF have been repeatedly associated with depression.5 Together with TNF-α, IL-6 is suggested to promote chronic inflammation.66 |
| Total protein | Increased CSF total protein is normally caused by BBB dysfunction and increased BBB permeability.67 Increased BBB permeability has been associated with affective disorders.68 |
| Aβ40 | Aβ is a heterogeneous mix of small peptides (from 36 to 43 amino acids) derived from cleavage of the APP. Aβ is normally secreted from cells and degraded, but in Alzheimer disease an abnormal accumulation in the brain leads to insoluble plaques. Aβ40 is an isotypes of Aβ consisting of 38 amino acids.69 |
| BDNF | BDNF is a secretory protein primarily expressed by neurons in the CNS. It is involved in neurogenesis, synaptic plasticity, and the modulating of neurotransmission and affects neuronal death and survival. Expression of BDNF can be regulated by stress, diet, and physical activity, and lower levels of BNDF in CNS have been repeatedly found in patients with major depression.70 |
Abbreviations: Aβ, amyloid-β; Aβ40, amyloid-β 40; APP, amyloid precursor protein; BBB, blood-brain barrier; BDNF, brain-derived neurotrophic factor; CNS, central nervous system; CSF, cerebrospinal fluid; GABA, γ-aminobutyric acid; HPA, hypothalamic-pituitary-adrenal; HVA, homovanillic acid; IL, interleukin; SS, somatostatin; TNF, tumor necrosis factor; TTR, transthyretin.
Bias Assessment
Of the 97 studies presented here, 40 received fewer than 4 stars on the Newcastle-Ottawa Scale, whereas 57 received 4 or more stars (term definitions are shown in eTable 6 in the Supplement and bias assessment in eTable 7 in the Supplement). Only 1 study71 received the maximum of 8 stars. Most studies had a risk of bias owing to representativeness of cases (86 of 97), ascertainment of exposure (77 of 97), and case definition (60 of 97). A minority of studies had risk of bias owing to the same method of ascertainment (1 of 97) and the definition (26 of 97) and selection (44 of 97) of control individuals. Regarding comparability, 51 studies controlled for both age and sex, 18 for either age or sex, and 28 did not state any controlling factors. As presented in the GRADE evidence profile (eTable 10 in the Supplement), 1 of 42 biomarkers were rated as high quality of evidence whereas 5 of 42, 11 of 42, and 25 of 42 were rated moderate, low, and very low quality, respectively.
Neurotransmitters and Metabolites
Levels were lower in individuals with depression compared with healthy control individuals for homovanillic acid (HVA) (17 studies20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36 including 684 patients and 681 control individuals; SMD, −0.26; 95% CI, −0.39 to −0.14; I2 = 11%) and GABA (4 studies37,38,39,40 including 180 patients and 111 control individuals; SMD, −0.50; 95% CI, −0.92 to −0.08; I2 = 55%). The analyses of 5-hydroxyindoleacetic acid (5-HIAA), 3-methoxy–4-hydroxyphenylglycol (MHPG), glutamate, and glutamine did not differ significantly between groups (Table 1).
Depression severity measured by HAM-D was associated with 5-HIAA (estimate, 0.048; 95% CI, 0.002 to 0.095; P = .04) and MHPG (estimate, 0.068; 95% CI, 0.036 to 0.100; P < .001) in the meta-regression analyses (eFigure 7 in the Supplement). However, the meta-regression analysis was no longer significant when excluding 2 outlying articles.22,36 Likewise, the meta-regression analysis for HVA was not significant (estimate, −0.018; 95% CI, −0.045 to 0.010; P = .21). Inpatient or outpatient status and discontinuation of medication prior to lumbar puncture were not significantly associated with biomarker levels (eFigures 8 and 9 in the Supplement).
Hormones, Neuropeptides, and Amino Acids
We found elevated levels of cortisol in individuals with depression (2 studies41,42 including 77 patients and 81 control individuals; SMD, 1.23; 95% CI, 0.89 to 1.57; I2 = 0%), whereas transthyretin levels were lower in individuals with depression (2 studies32,43 including 25 patients and 39 control individuals; SMD, −0.82; 95% CI, −1.37 to −0.27; I2 = 0%). No significant differences were found for corticotrophin-releasing hormone, adrenocorticotropic hormone, oxytocin, or vasopressin (Table 1). Regarding neuropeptides, the meta-analysis revealed lower levels of somatostatin in patients (5 studies26,29,44,45,46 including 130 patients and 113 control individuals; SMD, −1.49; 95% CI, −2.53 to −0.45; I2 = 91%), whereas there were no significant differences for neuropeptide Y, substance P, cocaine- and amphetamine-regulated transcript, or orexin. We found no significant differences between patients and healthy control individuals for the amino acids and metabolites quantified (Table 1). When examining the association of discontinuation of antidepressant medication before lumbar puncture with differences in biomarker levels between patients and healthy control individuals, no significant findings were found for somatostatin, corticotrophin-releasing hormone, or neuropeptide Y (eFigure 9 in the Supplement).
Immunological Markers
Higher levels of interleukin 6 (IL-6) were found in individuals with depression (7 studies34,47,48,49,50,51,52 including 156 patients and 229 control individuals; SMD, 0.35; 95% CI, 0.12 to 0.59; I2 = 16%), while no significant differences were found for IL-8, tumor necrosis factor α, white cell count, or matrix metalloproteinase-3 (Table 1). Concerning markers of blood-brain barrier permeability, we found elevated levels of total protein in patients (5 studies50,53,54,55,56 including 220 patients and 261 control individuals; SMD, 0.53; 95% CI, 0.35 to 0.72; I2 = 0%), whereas albumin ratio and glucose did not differ significantly between groups (Table 1). Discontinuation of medication prior to lumbar puncture was not significantly associated with levels of IL-6 (eFigure 9 in the Supplement).
Synaptic Plasticity and Neurodegeneration
Regarding markers of synaptic plasticity, brain-derived neurotrophic factor (BDNF) levels were lower in patients (3 studies34,49,60 including 46 patients and 62 control individuals; SMD, −0.58; 95% CI, −0.97 to −0.19; I2 = 0%), whereas levels of neural cell adhesion molecule did not differ significantly (Table 1). Investigating biomarkers of neurodegeneration, we found lower levels of amyloid-β 4057,58,59 (3 studies including 71 patients and 81 control individuals; SMD, −0.80; 95% CI, −1.14 to −0.46; I2 = 0%), whereas no significant differences were found in total τ, p-τ 181, amyloid-β 42, neurogranin, and neurofilament light protein (Table 1).
Biomarkers Only Quantified in 1 Study
Of the 165 biomarkers included in this meta-analysis, 123 were quantified in only 1 study. Of these, 27 displayed significant results when based on extracted summary data (eFigure 6 in the Supplement). The following were elevated in patients compared with healthy control individuals: asparagine (1 study including 42 patients and 54 control individuals; SMD, 0.44; 95% CI, 0.03 to 0.85; P = .03), B-cell–attracting factor/tumor necrosis factor superfamily 13β (1 study including 104 patients and 118 control individuals; SMD, 0.32; 95% CI, 0.06 to 0.59; P = .02), C5 (1 study including 89 patients and 117 control individuals; SMD, 0.59; 95% CI, 0.31 to 0.87; P < .001), corticosterone (1 study including 12 patients and 12 control individuals; SMD, 1.30; 95% CI, 0.41 to 2.20; P = .004), fibrinogen (1 study including 66 patients and 60 control individuals; SMD, 0.52; 95% CI, 0.16 to 0.87; P = .004), hyaluronic acid (1 study including 39 patients and 45 control individuals; SMD, 0.54; 95% CI, 0.10 to 0.98; P = .02), interferon-β (1 study including 104 patients and 118 control individuals; SMD, 0.36; 95% CI, 0.10 to 0.63; P = .007), matrix metalloproteinase-10 (1 study including 90 patients and 106 control individuals; SMD, 0.38; 95% CI, 0.09 to 0.66; P = .009), matrix metalloproteinase-2 (1 study including 90 patients and 106 control individuals; SMD, 0.34; 95% CI, 0.06 to 0.62; P = .02), noradrenalin (1 study including 10 patients and 14 control individuals; SMD, 3.48; 95% CI, 2.13 to 4.83; P < .001), quinolinic acid (1 study including 31 patients and 36 control individuals; SMD, 0.96; 95% CI, 0.45 to 1.46; P < .001), SL000022 (D-dimer) (1 study including 30 patients and 30 control individuals; SMD, 0.54; 95% CI, 0.03 to 1.06; P = .04), SL0000424 (fibrinogen) (1 study including 30 patients and 30 control individuals; SMD, 0.63; 95% CI, 0.11 to 1.15; P = .02), SL003341 (fibrinogen y-chain) (1 study including 30 patients and 30 control individuals; SMD, 0.55; 95% CI, 0.04 to 1.07; P = .04), sorbitol (1 study including 10 patients and 10 control individuals; SMD, 1.36; 95% CI, 0.37 to 2.36; P = .007), and threonine (1 study including 42 patients and 54 control individuals; SMD, 0.45; 95% CI, 0.04 to 0.86; P = .03). The following biomarkers were lower in patients compared with healthy control individuals: amyloid-β 38 (1 study including 28 patients and 38 control individuals; SMD, −0.86; 95% CI, −1.37 to −0.35; P = .001), butyrylcholinesterase (1 study including 27 patients and 17 control individuals; SMD, −0.72; 95% CI, −1.34 to −0.09; P = .03), calcitonin (1 study including 29 patients and 19 control individuals; SMD, −0.79; 95% CI, −1.39 to −0.19; P = .01), carnosine (1 study including 35 patients and 44 control individuals; SMD, −0.48; 95% CI, −0.93 to −0.03; P = .04), ethanolamine (1 study including 42 patients and 54 control individuals; SMD, −1.11; 95% CI, −1.54 to −0.67; P < .001), monocyte chemoattractant protein–4 (1 study including 51 patients and 43 control individuals; SMD, −0.81; 95% CI, −1.23 to −0.39; P < .001), paired helical filaments–τ (1 study including 10 patients and 31 control individuals; SMD, −1.40; 95% CI, −2.18 to −0.62; P < .001), picolinic acid (1 study including 31 patients and 36 control individuals; SMD, −1.31; 95% CI, −1.84 to −0.78; P < .001), soluble amyloid precursor protein β (1 study including 28 patients and 38 control individuals; SMD, −0.51; 95% CI, −1.00 to −0.01; P = .046), soluble triggering receptor expressed on myeloid cells–2 (1 study including 27 patients and 17 control individuals; SMD, −0.63; 95% CI, −1.25 to −0.01; P = .047), and thymus activation-regulated chemokine (1 study including 51 patients and 43 control individuals; SMD, −0.66; 95% CI, −1.08 to −0.24; P = .002).
Sensitivity Analysis
We found no significant differences when comparing studies with a total Newcastle-Ottawa Scale score of 4 and higher vs less than 4 (eFigure 10 in the Supplement). Subgroup analyses of publication year only displayed significant differences for HVA and somatostatin, both becoming insignificant when solely including studies published after 2000 (eFigure 11 in the Supplement). The funnel plots for HVA, 5-HIAA, and MHPG did not indicate publication bias (eFigure 12 in the Supplement). The meta-regression relating group sizes to SMD presented significant associations for 5-HIAA (estimate, −0.009; 95% CI, −0.018 to 0; P = .049) indicating lower levels of serotonin in larger group sizes (eFigure 13 in the Supplement). However, when excluding the only study36 not pausing antidepressant medication, the association was not significant (estimate, −0.003; 95% CI, −0.016 to 0.010; P = .64). None of the meta-regression analyses associating publication year with SMD presented significant results (eFigure 14 in the Supplement).
Discussion
This systematic review and meta-analysis of all CSF studies comparing individuals with unipolar depression with healthy control individuals revealed higher levels of IL-6, total protein, and cortisol and lower levels of HVA, GABA, somatostatin, BDNF, amyloid-β 40, and transthyretin in individuals with depression. To our knowledge, this is the first meta-analysis to reveal alterations in cortisol, total protein, BDNF, somatostatin, amyloid-β 40, and transthyretin in CSF from patients with unipolar depression compared with healthy control individuals. Our meta-analysis supports the hypothesis of a dysregulated dopaminergic system in individuals with depression, while concurrently pointing toward a compromised inhibitory system, hyperactivity of the HPA axis, increased neuroinflammation and blood-brain barrier permeability, and impaired neuroplasticity as possible pathophysiological contributors. To our knowledge, this meta-analysis is also the first to comprise all biomarkers quantified in CSF from patients with unipolar depression compared with healthy control individuals, hereby providing a full overview of the currently available literature.
As the most targeted neurotransmitters in modern antidepressant treatment,72 it is notable that we did not find significant differences between patients and control individuals in the metabolite levels of serotonin and noradrenalin. Despite including more studies, we confirmed the findings of previous meta-analyses,73,74 presenting only lower levels of the dopamine metabolite. However, the nonsignificant findings for 5-HIAA and MHPG could be explained by the substantial heterogeneities revealed in both meta-analyses.
Our analysis on GABA included more studies, validating previous findings of lower levels in patients with unipolar depression.75 Owing to its inhibitory effect, GABA deficiency may result in local hyperexcitability leading to compromised neurogenesis and HPA axis hyperactivity.62 We also found lower levels of somatostatin, a modulatory and inhibitory neuropeptide often colocalized with GABA.65 However, most included studies were from prior decades, indicating a need for novel studies to validate these findings with improved methods. The same applies to the analysis on cortisol only comprising 2 older studies that revealed highly elevated levels in individuals with depression compared with healthy control individuals. Moreover, our meta-analysis revealed lower levels of transthyretin, proposed to be associated with altered thyroid hormone balance in the central nervous system32,43; however, this could also be because of neuroprotective abilities.76
Furthermore, we found lower levels of BDNF in patients with depression, pointing in the same direction as earlier meta-analyses on blood levels.6,77 BDNF is involved in neurogenesis, synaptic plasticity, and modulating of neurotransmission70 and is shown to increase in blood levels in response to antidepressant treatment.6
Another main finding of this meta-analysis was increased IL-6 levels, suggesting chronic inflammation in line with previous findings.78,79 We also found elevated total protein denoting blood-brain barrier dysfunction, which can likewise be indicative of inflammation in the central nervous system.68,80 One meta-analysis previously reported increased total protein in individuals with affective disorders,68 although to our knowledge no meta-analysis has examined individuals with unipolar depression only.
Despite multiple significant findings, most biomarkers displayed no significant differences and many analyses revealed substantial heterogeneity, indicating a considerable variation among studies. There may be several reasons for this. First, the inconsistency in findings may reflect a compromised quality of the included studies and variations in cohorts. Second, quantification of total CSF biomarker concentrations does not reflect local alteration within the central nervous system. Third, the variation could be a result of the existence of subgroups in depression. Such subgroups would not only explain the failure to identify 1 biomarker and thus 1 biological mechanism, but also the diverse symptomatology81 and variability in treatment response.82 The possibility of subgroups identifiable by different biomarkers that might benefit from different types of medication is endorsed by studies showing better effects with anti-inflammatory treatment among patients with high baseline inflammatory markers.83,84 However, many antidepressants seem to affect a variety of biological systems,85,86 and evidence implies a high degree of interaction between different neurocircuits, indicating a highly complex etiology.5,87 Hence, an integrative understanding of depression pathophysiology is most likely needed to identify reliable biomarkers useful in precise treatment of depression.
Limitations
This study has limitations. For most biomarkers, the number of eligible studies was limited, and of 165 biomarkers identified, only 42 were quantified in more than 1 study. Additionally, all studies except 1 had risk of bias on the Newcastle-Ottawa Scale, and most did not adequately address factors possibly affecting biomarker levels, such as age,22,27,88,89 sex,22 and body mass index.90 Although a diagnosis of unipolar depression was required for inclusion in this analysis, studies varied in diagnostic tools, severity of depression, duration of disease, and medication status, if reported. The type of assay and thus sensitivity also varied across studies, and most studies did not report the actual number of samples above the detection limit. By extension, for some biomarkers, the methodology of analyzing CSF has changed over time. Only 28 of 97 studies stated whether the biomarker concentrations were normally distributed or log transformed, despite this being highly relevant when computing standardized mean differences. Only 6 of 97 studies quantified the same biomarker in CSF and blood, and therefore separate analyses on such associations could not be conducted. Moreover, owing to the lack of longitudinal studies, we could not examine the prognostic value of biomarker levels.
Conclusions
This systematic review and meta-analysis provides evidence that numerous biomarkers may be altered in patients with depression, indicating involvement of several neurocircuits. However, many studies had small cohorts and most quantified only a few biomarkers, making it hard to examine potential interactions between biomarkers or identify specific phenotypes of depression. Therefore, novel high-quality studies including larger cohorts with an integrative approach and extensive numbers of biomarkers are needed to validate these potential biomarkers of depression and set the stage for the development of more effective and precise treatments.
eTable 1. PRISMA 2020 Checklist
eTable 2. MOOSE Checklist for Meta-analyses of Observational Studies
eTable 3. Search string
eFigure 1. PRISMA 2020 flow diagram
eTable 4. Baseline characteristics from CSF studies
eFigure 2. Neurotransmitters and their metabolites
eFigure 3. Hormones, neuropeptides and metabolites
eFigure 4. Inflammation and BBB permeability
eFigure 5. Neurodegeneration and synaptic plasticity
eFigure 6. Forest plots of biomarkers quantified in only one study
eTable 5. Presentation of all biomarkers identified for the meta-analysis and a brief description of their function
eFigure 7. Meta-regression analyses of mean biomarker levels in relation to mean HAM-D scores for patients. Performed on biomarkers with data for ≧10 studies
eFigure 8. Hospitalized patients compared to not hospitalized patients for biomarkers with data on ≧5 studies
eFigure 9. Patients off antidepressant treatment for ≦14 days compared to >14 days for biomarkers with data on ≧5 studies
eFigure 10. Studies with a total score of ≧4 compared to <4 on the Newcastle Ottawa Scale (NOS) for biomarkers quantified in ≧5 studies
eFigure 11. Studies published before year 2000 compared to studies published in or after 2000 for biomarkers quantified in ≧5 studies
eFigure 12. Funnel plots of biomarkers examined in ≧10 studies
eFigure 13. Meta-regression analyses of mean group size in relation to standard mean difference (SMD) on biomarkers examined in ≧10 studies
eFigure 14. Meta-regression analyses of publication year in relation to standard mean difference (SMD) on biomarkers examined in ≧10 studies
eTable 6. Definition of terms for bias assessment according to the Newcastle-Ottawa criteria for case-control studies
eTable 7. Bias assessment according to the Newcastle-Ottawa criteria for case-control studies
eTable 8. Studies contacted for data request
eTable 9. Studies that had been included in previous meta-analyses but were excluded due to neurological or surgical controls
eTable 10. GRADE evidence profile for biomarkers quantified in ≧2 studies
References
- 1.GBD 2017 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789-1858. doi: 10.1016/S0140-6736(18)32279-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jayamohananan H, Manoj Kumar MK, T P A. 5-HIAA as a potential biological marker for neurological and psychiatric disorders. Adv Pharm Bull. 2019;9(3):374-381. doi: 10.15171/apb.2019.044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sanacora G, Treccani G, Popoli M. Towards a glutamate hypothesis of depression: an emerging frontier of neuropsychopharmacology for mood disorders. Neuropharmacology. 2012;62(1):63-77. doi: 10.1016/j.neuropharm.2011.07.036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Won E, Kim Y-K. Stress, the autonomic nervous system, and the immune-kynurenine pathway in the etiology of depression. Curr Neuropharmacol. 2016;14(7):665-673. doi: 10.2174/1570159X14666151208113006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Miller AH, Raison CL. The role of inflammation in depression: from evolutionary imperative to modern treatment target. Nat Rev Immunol. 2016;16(1):22-34. doi: 10.1038/nri.2015.5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Brunoni AR, Lopes M, Fregni F. A systematic review and meta-analysis of clinical studies on major depression and BDNF levels: implications for the role of neuroplasticity in depression. Int J Neuropsychopharmacol. 2008;11(8):1169-1180. doi: 10.1017/S1461145708009309 [DOI] [PubMed] [Google Scholar]
- 7.Strittmatter WJ. Bathing the brain. J Clin Invest. 2013;123(3):1013-1015. doi: 10.1172/JCI68241 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Spitzer RL, Endicott J, Williams JBW. Research diagnostic criteria. Arch Gen Psychiatry. 1979;36(12):1381-1383. doi: 10.1001/archpsyc.1979.01780120111013 [DOI] [PubMed] [Google Scholar]
- 9.Feighner JP, Robins E, Guze SB, Woodruff RA Jr, Winokur G, Munoz R. Diagnostic criteria for use in psychiatric research. Arch Gen Psychiatry. 1972;26(1):57-63. doi: 10.1001/archpsyc.1972.01750190059011 [DOI] [PubMed] [Google Scholar]
- 10.Gurney C, Roth M, Garside RF, Kerr TA, Schapira K. Studies in the classification of affective disorders. the relationship between anxiety states and depressive illnesses. II. Br J Psychiatry. 1972;121(561):162-166. doi: 10.1192/bjp.121.2.162 [DOI] [PubMed] [Google Scholar]
- 11.The Cochrane Collaboration . Newcastle-Ottawa Quality Assessment Scale Case Control Studies. Accessed August 19, 2021. http://www.ohri.ca/programs/clinical_epidemiology/nosgen.pdf
- 12.Schünemann H, Brożek J, Guyatt G, Oxman A, eds. GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations. The GRADE Working Group. Accessed January 9, 2022. http://guidelinedevelopment.org/handbook [Google Scholar]
- 13.DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177-188. doi: 10.1016/0197-2456(86)90046-2 [DOI] [PubMed] [Google Scholar]
- 14.Levine SZ, Rabinowitz J, Faries D, Lawson AH, Ascher-Svanum H. Treatment response trajectories and antipsychotic medications: examination of up to 18 months of treatment in the CATIE Chronic Schizophrenia trial. Schizophr Res. 2012;137(1-3):141-146. doi: 10.1016/j.schres.2012.01.014 [DOI] [PubMed] [Google Scholar]
- 15.Hedges LV. Distribution theory for Glass’s estimator of effect size and related estimators. J Educ Behav Stat. 1981;6(2):107-128. doi: 10.3102/10769986006002107 [DOI] [Google Scholar]
- 16.Hedges LV. Estimation of effect size from a series of independent experiments. Psychol Bull. 1982;92(2):490-499. doi: 10.1037/0033-2909.92.2.490 [DOI] [Google Scholar]
- 17.Higgins JPT, Thomas J, Chandler J, et al. , eds. Cochrane Handbook for Systematic Reviews of Interventions. 2nd ed. The Cochrane Collaboration; 2019. doi: 10.1002/9781119536604 [DOI] [Google Scholar]
- 18.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629-634. doi: 10.1136/bmj.315.7109.629 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. 2019;22(4):153-160. doi: 10.1136/ebmental-2019-300117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Oreland L, Wiberg A, Asberg M, et al. Platelet MAO activity and monoamine metabolites in cerebrospinal fluid in depressed and suicidal patients and in healthy control individuals. Psychiatry Res. 1981;4(1):21-29. doi: 10.1016/0165-1781(81)90004-4 [DOI] [PubMed] [Google Scholar]
- 21.Kasa K, Otsuki S, Yamamoto M, Sato M, Kuroda H, Ogawa N. Cerebrospinal fluid γ-aminobutyric acid and homovanillic acid in depressive disorders. Biol Psychiatry. 1982;17(8):877-883. [PubMed] [Google Scholar]
- 22.Koslow SH, Maas JW, Bowden CL, Davis JM, Hanin I, Javaid J. CSF and urinary biogenic amines and metabolites in depression and mania. a controlled, univariate analysis. Arch Gen Psychiatry. 1983;40(9):999-1010. doi: 10.1001/archpsyc.1983.01790080081011 [DOI] [PubMed] [Google Scholar]
- 23.Åsberg M, Bertilsson L, Mårtensson B, Scalia-Tomba G-P, Thorén P, Träskman-Bendz L. CSF monoamine metabolites in melancholia. Acta Psychiatr Scand. 1984;69(3):201-219. doi: 10.1111/j.1600-0447.1984.tb02488.x [DOI] [PubMed] [Google Scholar]
- 24.Widerlöv E, Bissette G, Nemeroff CB. Monoamine metabolites, corticotropin releasing factor and somatostatin as CSF markers in depressed patients. J Affect Disord. 1988;14(2):99-107. doi: 10.1016/0165-0327(88)90051-1 [DOI] [PubMed] [Google Scholar]
- 25.Lewine RRJ, Risch SC, Risby E, et al. Lateral ventricle-brain ratio and balance between CSF HVA and 5-HIAA in schizophrenia. Am J Psychiatry. 1991;148(9):1189-1194. doi: 10.1176/ajp.148.9.1189 [DOI] [PubMed] [Google Scholar]
- 26.Molchan SE, Lawlor BA, Hill JL, et al. CSF monoamine metabolites and somatostatin in Alzheimer’s disease and major depression. Biol Psychiatry. 1991;29(11):1110-1118. doi: 10.1016/0006-3223(91)90253-I [DOI] [PubMed] [Google Scholar]
- 27.De Bellis MD, Geracioti TD Jr, Altemus M, Kling MA. Cerebrospinal fluid monoamine metabolites in fluoxetine-treated patients with major depression and in healthy volunteers. Biol Psychiatry. 1993;33(8-9):636-641. doi: 10.1016/0006-3223(93)90103-K [DOI] [PubMed] [Google Scholar]
- 28.Swann AC, Katz MM, Bowden CL, Berman NG, Stokes PE. Psychomotor performance and monoamine function in bipolar and unipolar affective disorders. Biol Psychiatry. 1999;45(8):979-988. doi: 10.1016/S0006-3223(98)00172-3 [DOI] [PubMed] [Google Scholar]
- 29.Heilig M, Zachrisson O, Thorsell A, et al. Decreased cerebrospinal fluid neuropeptide Y (NPY) in patients with treatment refractory unipolar major depression: preliminary evidence for association with preproNPY gene polymorphism. J Psychiatr Res. 2004;38(2):113-121. doi: 10.1016/S0022-3956(03)00101-8 [DOI] [PubMed] [Google Scholar]
- 30.Sher L, Oquendo MA, Li S, et al. Higher cerebrospinal fluid homovanillic acid levels in depressed patients with comorbid posttraumatic stress disorder. Eur Neuropsychopharmacol. 2005;15(2):203-209. doi: 10.1016/j.euroneuro.2004.09.009 [DOI] [PubMed] [Google Scholar]
- 31.Sher L, Mann JJ, Traskman-Bendz L, et al. Lower cerebrospinal fluid homovanillic acid levels in depressed suicide attempters. J Affect Disord. 2006;90(1):83-89. doi: 10.1016/j.jad.2005.10.002 [DOI] [PubMed] [Google Scholar]
- 32.Sullivan GM, Mann JJ, Oquendo MA, Lo ES, Cooper TB, Gorman JM. Low cerebrospinal fluid transthyretin levels in depression: correlations with suicidal ideation and low serotonin function. Biol Psychiatry. 2006;60(5):500-506. doi: 10.1016/j.biopsych.2005.11.022 [DOI] [PubMed] [Google Scholar]
- 33.Sullivan GM, Oquendo MA, Huang YY, Mann JJ. Elevated cerebrospinal fluid 5-hydroxyindoleacetic acid levels in women with comorbid depression and panic disorder. Int J Neuropsychopharmacol. 2006;9(5):547-556. doi: 10.1017/S1461145705006231 [DOI] [PubMed] [Google Scholar]
- 34.Pålhagen S, Qi H, Mårtensson B, Wålinder J, Granérus AK, Svenningsson P. Monoamines, BDNF, IL-6 and corticosterone in CSF in patients with Parkinson’s disease and major depression. J Neurol. 2010;257(4):524-532. doi: 10.1007/s00415-009-5353-6 [DOI] [PubMed] [Google Scholar]
- 35.Kaddurah-Daouk R, Yuan P, Boyle SH, et al. Cerebrospinal fluid metabolome in mood disorders-remission state has a unique metabolic profile. Sci Rep. 2012;2:667. doi: 10.1038/srep00667 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Yoon HS, Hattori K, Ogawa S, et al. Relationships of cerebrospinal fluid monoamine metabolite levels with clinical variables in major depressive disorder. J Clin Psychiatry. 2017;78(8): e947-e956. doi: 10.4088/JCP.16m11144 [DOI] [PubMed] [Google Scholar]
- 37.Gerner RH, Hare TA. CSF GABA in normal subjects and patients with depression, schizophrenia, mania, and anorexia nervosa. Am J Psychiatry. 1981;138(8):1098-1101. doi: 10.1176/ajp.138.8.1098 [DOI] [PubMed] [Google Scholar]
- 38.Roy A, Dejong J, Ferraro T. CSF GABA in depressed patients and normal control individuals. Psychol Med. 1991;21(3):613-618. doi: 10.1017/S0033291700022248 [DOI] [PubMed] [Google Scholar]
- 39.Mann JJ, Oquendo MA, Watson KT, et al. Anxiety in major depression and cerebrospinal fluid free gamma-aminobutyric acid. Depress Anxiety. 2014;31(10):814-821. doi: 10.1002/da.22278 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ogawa S, Hattori K, Sasayama D, et al. Reduced cerebrospinal fluid ethanolamine concentration in major depressive disorder. Sci Rep. 2015;5:7796. doi: 10.1038/srep07796 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Gerner RH, Wilkins JN. CSF cortisol in patients with depression, mania, or anorexia nervosa and in normal subjects. Am J Psychiatry. 1983;140(1):92-94. doi: 10.1176/ajp.140.1.92 [DOI] [PubMed] [Google Scholar]
- 42.Stokes PE, Stoll PM, Koslow SH, et al. Pretreatment DST and hypothalamic-pituitary-adrenocortical function in depressed patients and comparison groups. a multicenter study. Arch Gen Psychiatry. 1984;41(3):257-267. doi: 10.1001/archpsyc.1984.01790140047006 [DOI] [PubMed] [Google Scholar]
- 43.Sullivan GM, Hatterer JA, Herbert J, et al. Low levels of transthyretin in the CSF of depressed patients. Am J Psychiatry. 1999;156(5):710-715. [DOI] [PubMed] [Google Scholar]
- 44.Rubinow DR, Gold PW, Post RM, et al. CSF somatostatin in affective illness. Arch Gen Psychiatry. 1983;40(4):409-412. doi: 10.1001/archpsyc.1983.01790040063009 [DOI] [PubMed] [Google Scholar]
- 45.Bissette G, Widerlöv E, Walléus H, et al. Alterations in cerebrospinal fluid concentrations of somatostatinlike immunoreactivity in neuropsychiatric disorders. Arch Gen Psychiatry. 1986;43(12):1148-1151. doi: 10.1001/archpsyc.1986.01800120034008 [DOI] [PubMed] [Google Scholar]
- 46.Heuser I, Bissette G, Dettling M, et al. Cerebrospinal fluid concentrations of corticotropin-releasing hormone, vasopressin, and somatostatin in depressed patients and healthy control individuals: response to amitriptyline treatment. Depress Anxiety. 1998;8(2):71-79. doi: [DOI] [PubMed] [Google Scholar]
- 47.Carpenter LL, Heninger GR, Malison RT, Tyrka AR, Price LH. Cerebrospinal fluid interleukin (IL)-6 in unipolar major depression. J Affect Disord. 2004;79(1-3):285-289. doi: 10.1016/S0165-0327(02)00460-3 [DOI] [PubMed] [Google Scholar]
- 48.Lindqvist D, Janelidze S, Hagell P, et al. Interleukin-6 is elevated in the cerebrospinal fluid of suicide attempters and related to symptom severity. Biol Psychiatry. 2009;66(3):287-292. doi: 10.1016/j.biopsych.2009.01.030 [DOI] [PubMed] [Google Scholar]
- 49.Martinez JM, Garakani A, Yehuda R, Gorman JM. Proinflammatory and “resiliency” proteins in the CSF of patients with major depression. Depress Anxiety. 2012;29(1):32-38. doi: 10.1002/da.20876 [DOI] [PubMed] [Google Scholar]
- 50.Sasayama D, Hattori K, Wakabayashi C, et al. Increased cerebrospinal fluid interleukin-6 levels in patients with schizophrenia and those with major depressive disorder. J Psychiatr Res. 2013;47(3):401-406. doi: 10.1016/j.jpsychires.2012.12.001 [DOI] [PubMed] [Google Scholar]
- 51.Kern S, Skoog I, Börjesson-Hanson A, et al. Higher CSF interleukin-6 and CSF interleukin-8 in current depression in older women. results from a population-based sample. Brain Behav Immun. 2014;41(1):55-58. doi: 10.1016/j.bbi.2014.05.006 [DOI] [PubMed] [Google Scholar]
- 52.Pomara N, Bruno D, Plaska CR, et al. Evidence of upregulation of the cholinergic anti-inflammatory pathway in late-life depression. J Affect Disord. 2021;286:275-281. doi: 10.1016/j.jad.2021.03.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Vawter MP, Frye MA, Hemperly JJ, et al. Elevated concentration of N-CAM VASE isoforms in schizophrenia. J Psychiatr Res. 2000;34(1):25-34. doi: 10.1016/S0022-3956(99)00026-6 [DOI] [PubMed] [Google Scholar]
- 54.Hattori K, Ota M, Sasayama D, et al. Increased cerebrospinal fluid fibrinogen in major depressive disorder. Sci Rep. 2015;5:11412. doi: 10.1038/srep11412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Mizui T, Hattori K, Ishiwata S, et al. Cerebrospinal fluid BDNF pro-peptide levels in major depressive disorder and schizophrenia. J Psychiatr Res. 2019;113:190-198. doi: 10.1016/j.jpsychires.2019.03.024 [DOI] [PubMed] [Google Scholar]
- 56.Omori W, Hattori K, Kajitani N, et al. Increased matrix metalloproteinases in cerebrospinal fluids of patients with major depressive disorder and schizophrenia. Int J Neuropsychopharmacol. 2020;23(11):713-720. doi: 10.1093/ijnp/pyaa049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Jensen M, Schröder J, Blomberg M, et al. Cerebrospinal fluid A42 is increased early in sporadic Alzheimer’s disease and declines with disease progression. Ann Neurol. 1999;45(4):504-511. doi: [DOI] [PubMed] [Google Scholar]
- 58.Hertze J, Minthon L, Zetterberg H, Vanmechelen E, Blennow K, Hansson O. Evaluation of CSF biomarkers as predictors of Alzheimer’s disease: a clinical follow-up study of 4.7 years. J Alzheimers Dis. 2010;21(4):1119-1128. doi: 10.3233/JAD-2010-100207 [DOI] [PubMed] [Google Scholar]
- 59.Pomara N, Bruno D, Sarreal AS, et al. Lower CSF amyloid beta peptides and higher F2-isoprostanes in cognitively intact elderly individuals with major depressive disorder. Am J Psychiatry. 2012;169(5):523-530. doi: 10.1176/appi.ajp.2011.11081153 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Diniz BS, Teixeira AL, Machado-Vieira R, et al. Reduced cerebrospinal fluid levels of brain-derived neurotrophic factor is associated with cognitive impairment in late-life major depression. J Gerontol B Psychol Sci Soc Sci. 2014;69(6):845-851. doi: 10.1093/geronb/gbu096 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Dunlop BW, Nemeroff CB. The role of dopamine in the pathophysiology of depression. Arch Gen Psychiatry. 2007;64(3):327-337. doi: 10.1001/archpsyc.64.3.327 [DOI] [PubMed] [Google Scholar]
- 62.Luscher B, Shen Q, Sahir N. The GABAergic deficit hypothesis of major depressive disorder. Mol Psychiatry. 2011;16(4):383-406. doi: 10.1038/mp.2010.120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Yang L, Zhao Y, Wang Y, et al. The effects of psychological stress on depression. Curr Neuropharmacol. 2015;13(4):494-504. doi: 10.2174/1570159X1304150831150507 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Faron-Górecka A, Kuśmider M, Solich J, et al. Involvement of prolactin and somatostatin in depression and the mechanism of action of antidepressant drugs. Pharmacol Rep. 2013;65(6):1640-1646. doi: 10.1016/S1734-1140(13)71525-1 [DOI] [PubMed] [Google Scholar]
- 65.Lin LC, Sibille E. Reduced brain somatostatin in mood disorders: a common pathophysiological substrate and drug target? Front Pharmacol. 2013;4:110. doi: 10.3389/fphar.2013.00110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Gabay C. Interleukin-6 and chronic inflammation. Arthritis Res Ther. 2006;8(suppl 2):S3. doi: 10.1186/ar1917 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Breiner A, Moher D, Brooks J, et al. Adult CSF total protein upper reference limits should be age-partitioned and significantly higher than 0.45 g/L: a systematic review. J Neurol. 2019;266(3):616-624. doi: 10.1007/s00415-018-09174-z [DOI] [PubMed] [Google Scholar]
- 68.Orlovska-Waast S, Köhler-Forsberg O, Brix SW, et al. Cerebrospinal fluid markers of inflammation and infections in schizophrenia and affective disorders: a systematic review and meta-analysis. Mol Psychiatry. 2019;24(6):869-887. doi: 10.1038/s41380-018-0220-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Chen G-F, Xu T-H, Yan Y, et al. Amyloid beta: structure, biology and structure-based therapeutic development. Acta Pharmacol Sin. 2017;38(9):1205-1235. doi: 10.1038/aps.2017.28 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Lima Giacobbo B, Doorduin J, Klein HC, Dierckx RAJO, Bromberg E, de Vries EFJ. Brain-derived neurotrophic factor in brain disorders: focus on neuroinflammation. Mol Neurobiol. 2019;56(5):3295-3312. doi: 10.1007/s12035-018-1283-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Eratne D, Loi SM, Walia N, et al. A pilot study of the utility of cerebrospinal fluid neurofilament light chain in differentiating neurodegenerative from psychiatric disorders: a ‘C-reactive protein’ for psychiatrists and neurologists? Aust N Z J Psychiatry. 2020;54(1):57-67. doi: 10.1177/0004867419857811 [DOI] [PubMed] [Google Scholar]
- 72.Commonly prescribed antidepressants and how they work. NIH MedlinePlus Magazine. Accessed June 3, 2021. https://magazine.medlineplus.gov/article/commonly-prescribed-antidepressants-and-how-they-work
- 73.Pech J, Forman J, Kessing LV, Knorr U. Poor evidence for putative abnormalities in cerebrospinal fluid neurotransmitters in patients with depression versus healthy non-psychiatric individuals: a systematic review and meta-analyses of 23 studies. J Affect Disord. 2018;240(240):6-16. doi: 10.1016/j.jad.2018.07.031 [DOI] [PubMed] [Google Scholar]
- 74.Ogawa S, Tsuchimine S, Kunugi H. Cerebrospinal fluid monoamine metabolite concentrations in depressive disorder: a meta-analysis of historic evidence. J Psychiatr Res. 2018;105:137-146. doi: 10.1016/j.jpsychires.2018.08.028 [DOI] [PubMed] [Google Scholar]
- 75.Romeo B, Choucha W, Fossati P, Rotge J-Y. Meta-analysis of central and peripheral γ-aminobutyric acid levels in patients with unipolar and bipolar depression. J Psychiatry Neurosci. 2018;43(1):58-66. doi: 10.1503/jpn.160228 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Gião T, Saavedra J, Cotrina E, et al. Undiscovered roles for transthyretin: from a transporter protein to a new therapeutic target for Alzheimer’s disease. Int J Mol Sci. 2020;21(6):2075. doi: 10.3390/ijms21062075 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Polyakova M, Stuke K, Schuemberg K, Mueller K, Schoenknecht P, Schroeter ML. BDNF as a biomarker for successful treatment of mood disorders: a systematic & quantitative meta-analysis. J Affect Disord. 2015;174:432-440. doi: 10.1016/j.jad.2014.11.044 [DOI] [PubMed] [Google Scholar]
- 78.Wang AK, Miller BJ. Meta-analysis of cerebrospinal fluid cytokine and tryptophan catabolite alterations in psychiatric patients: comparisons between schizophrenia, bipolar disorder, and depression. Schizophr Bull. 2018;44(1):75-83. doi: 10.1093/schbul/sbx035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Enache D, Pariante CM, Mondelli V. Markers of central inflammation in major depressive disorder: a systematic review and meta-analysis of studies examining cerebrospinal fluid, positron emission tomography and post-mortem brain tissue. Brain Behav Immun. 2019;81:24-40. doi: 10.1016/j.bbi.2019.06.015 [DOI] [PubMed] [Google Scholar]
- 80.Bechter K, Reiber H, Herzog S, Fuchs D, Tumani H, Maxeiner HG. Cerebrospinal fluid analysis in affective and schizophrenic spectrum disorders: identification of subgroups with immune responses and blood-CSF barrier dysfunction. J Psychiatr Res. 2010;44(5):321-330. doi: 10.1016/j.jpsychires.2009.08.008 [DOI] [PubMed] [Google Scholar]
- 81.Milak MS, Parsey RV, Keilp J, Oquendo MA, Malone KM, Mann JJ. Neuroanatomic correlates of psychopathologic components of major depressive disorder. Arch Gen Psychiatry. 2005;62(4):397-408. doi: 10.1001/archpsyc.62.4.397 [DOI] [PubMed] [Google Scholar]
- 82.Gaynes BN, Rush AJ, Trivedi MH, Wisniewski SR, Spencer D, Fava M. The STAR*D study: treating depression in the real world. Cleve Clin J Med. 2008;75(1):57-66. doi: 10.3949/ccjm.75.1.57 [DOI] [PubMed] [Google Scholar]
- 83.Abbasi S-H, Hosseini F, Modabbernia A, Ashrafi M, Akhondzadeh S. Effect of celecoxib add-on treatment on symptoms and serum IL-6 concentrations in patients with major depressive disorder: randomized double-blind placebo-controlled study. J Affect Disord. 2012;141(2-3):308-314. doi: 10.1016/j.jad.2012.03.033 [DOI] [PubMed] [Google Scholar]
- 84.Raison CL, Rutherford RE, Woolwine BJ, et al. A randomized controlled trial of the tumor necrosis factor antagonist infliximab for treatment-resistant depression: the role of baseline inflammatory biomarkers. JAMA Psychiatry. 2013;70(1):31-41. doi: 10.1001/2013.jamapsychiatry.4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Zhan Y, Zhou Y, Zheng W, et al. Alterations of multiple peripheral inflammatory cytokine levels after repeated ketamine infusions in major depressive disorder. Transl Psychiatry. 2020;10(1):246. doi: 10.1038/s41398-020-00933-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Casarotto PC, Girych M, Fred SM, et al. Antidepressant drugs act by directly binding to TRKB neurotrophin receptors. Cell. 2021;184(5):1299-1313.e19. doi: 10.1016/j.cell.2021.01.034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Kim YK, Won E. The influence of stress on neuroinflammation and alterations in brain structure and function in major depressive disorder. Behav Brain Res. 2017;329:6-11. doi: 10.1016/j.bbr.2017.04.020 [DOI] [PubMed] [Google Scholar]
- 88.Burlina AB, Celato A, Polo G, Edini C, Burlina AP. The utility of CSF for the diagnosis of primary and secondary monoamine neurotransmitter deficiencies. EJIFCC. 2017;28(1):64-76. [PMC free article] [PubMed] [Google Scholar]
- 89.Gerner RH, Fairbanks L, Anderson GM, et al. CSF neurochemistry in depressed, manic, and schizophrenic patients compared with that of normal control individuals. Am J Psychiatry. 1984;141(12):1533-1540. doi: 10.1176/ajp.141.12.1533 [DOI] [PubMed] [Google Scholar]
- 90.Powell TR, Gaspar H, Chung R, et al. Assessing 42 inflammatory markers in 321 control subjects and 887 major depressive disorder cases: BMI and other confounders and overall predictive ability for current depression. bioRxiv. Preprint posted May 21, 2018. doi: 10.1101/327239 [DOI]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. PRISMA 2020 Checklist
eTable 2. MOOSE Checklist for Meta-analyses of Observational Studies
eTable 3. Search string
eFigure 1. PRISMA 2020 flow diagram
eTable 4. Baseline characteristics from CSF studies
eFigure 2. Neurotransmitters and their metabolites
eFigure 3. Hormones, neuropeptides and metabolites
eFigure 4. Inflammation and BBB permeability
eFigure 5. Neurodegeneration and synaptic plasticity
eFigure 6. Forest plots of biomarkers quantified in only one study
eTable 5. Presentation of all biomarkers identified for the meta-analysis and a brief description of their function
eFigure 7. Meta-regression analyses of mean biomarker levels in relation to mean HAM-D scores for patients. Performed on biomarkers with data for ≧10 studies
eFigure 8. Hospitalized patients compared to not hospitalized patients for biomarkers with data on ≧5 studies
eFigure 9. Patients off antidepressant treatment for ≦14 days compared to >14 days for biomarkers with data on ≧5 studies
eFigure 10. Studies with a total score of ≧4 compared to <4 on the Newcastle Ottawa Scale (NOS) for biomarkers quantified in ≧5 studies
eFigure 11. Studies published before year 2000 compared to studies published in or after 2000 for biomarkers quantified in ≧5 studies
eFigure 12. Funnel plots of biomarkers examined in ≧10 studies
eFigure 13. Meta-regression analyses of mean group size in relation to standard mean difference (SMD) on biomarkers examined in ≧10 studies
eFigure 14. Meta-regression analyses of publication year in relation to standard mean difference (SMD) on biomarkers examined in ≧10 studies
eTable 6. Definition of terms for bias assessment according to the Newcastle-Ottawa criteria for case-control studies
eTable 7. Bias assessment according to the Newcastle-Ottawa criteria for case-control studies
eTable 8. Studies contacted for data request
eTable 9. Studies that had been included in previous meta-analyses but were excluded due to neurological or surgical controls
eTable 10. GRADE evidence profile for biomarkers quantified in ≧2 studies