

Abstract
Objective
To create reference charts for sitting height to standing height ratio (SitHt/Ht) for children in the US, and to describe the trajectory of SitHt/Ht during puberty.
Study design
This was a cross-sectional study using data from the 1988-1994 National Health and Nutrition Examination Survey III, a strategic random sample of the US population. Comparison between non-Hispanic White (NHW), non-Hispanic Black (NHB) and Mexican American groups was performed by ANOVA to determine if a single population reference chart could be used. ANOVA was used to compare SitHt/Ht in pre-, early, and late puberty.
Results
NHANES III recorded sitting height and standing height measurements in 9569 children aged 2-18 years of NHW (n = 2715), NHB (n = 3336), and Mexican American (n = 3518) ancestry. NHB children had lower SitHt/Ht than NHW and Mexican American children throughout childhood (P < .001). In both sexes, the SitHt/Ht decreased from prepuberty to early puberty and increased in late puberty. Sex-specific percentile charts of SitHt/Ht vs age were generated for NHB and for NHW and Mexican American youth combined.
Conclusions
SitHt/Ht assessment can detect disproportionate short stature in children with skeletal dysplasia, but age-, sex-, and population-specific reference charts are required to interpret this measurement. NHB children in the US have significantly lower SitHt/Ht than other children, which adds complexity to interpretation. We recommend the use of standardized ancestry-specific reference charts in screening for skeletal dysplasias and have developed such charts in this study.
Faltering growth or short stature can be an early sign of genetic, systemic, or endocrine disease in children.1 Growth concerns are one of the most common reasons for referral to a pediatric endocrinologist, although only a small proportion of referred children are found to have an endocrine disease.2,3 However, new genetic causes of isolated short stature are being identified as our understanding of the genetic factors that regulate growth expands.4,5 Many of these genetic variants predominantly affect the growth plate.6,7
Skeletal dysplasias can be associated with disproportionate short stature through growth attenuating effects on the long bones or on the vertebral bones. A child’s sitting height to standing height ratio (SitHt/Ht) can be used to screen for these disorders by identifying disproportionate short stature.8 More than 460 skeletal dysplasias have been described, and examples of those that can present with disproportionate short stature include short stature homeobox-containing gene defects, aggrecan mutations, hypochondroplasia, and achondroplasia.8-12 Skeletal disproportion in these conditions can be subtle, leading to misdiagnosis of idiopathic short stature.13 Some skeletal dysplasias can be associated with neurosurgical complications, including atlantoaxial instability and spinal stenosis.14
Numerous approaches to assess proportionality have been described, including SitHt/Ht, arm span to height ratio and upper to lower segment ratio. Arm span to height ratio assessment involves measuring arm span against a wall and calculating the ratio to standing height. Upper to lower segment ratio measurement involves measuring the distance between the pubic symphysis and the ground (lower segment) and subtracting this from the standing height to calculate the upper segment measurement.15 Measurements of sitting height and height involve the use of a calibrated stadiometer, increasing the likelihood that this approach to assessing proportionality is more accurate.
There are age-related, pubertal, and population ancestry effects on SitHt/Ht that need to be considered in interpreting these measurements. In infancy, sitting height represents approximately two-thirds of an infant’s length. In the prepubertal years, limb growth exceeds spinal growth leading to a sitting height closer to 50% of standing height in adolescents.8,16,17 Differences in proportionality are seen across European, African, and East Asian populations.18,19 African American children tend to have proportionally longer legs and arms than European children, and European children have relatively longer legs than Japanese children.19-21 There are also environmental effects on SitHt/Ht. Children who have been exposed to neglect or physical abuse have relatively shorter legs, and this metric improves with social intervention.22 Secular trends seem to affect proportionality; as height increases in populations, there are greater increases in leg length compared with sitting height.8,23,24
Population-specific reference data are required to determine if a child’s SitHt/Ht is outside of the typical range. A study of Dutch children has demonstrated that such reference data can be used to identify mild skeletal dysplasia.8 Although sitting height measurement has been included in surveys from the National Health and Nutrition Examination Survey (NHANES), smoothed reference percentiles and visual growth charts for SitHt/Ht have not been developed for clinical use for children in the US.25
The aim of this study was therefore to develop SitHt/Ht charts for healthy children in the US, and to prepare these as a tool that can be integrated easily into the clinical evaluation of children with short stature. As a secondary aim, we sought to assess the effect of self-reported population ancestry and pubertal stage on SitHt/Ht in this population.
Methods
The NHANES are conducted periodically by the Centers for Disease Control and Prevention’s National Center for Health Statistics (Hyattsville, MD). The most recent survey with available sitting height measurements was performed from 1988 to 1994 (NHANES III). In this study, we used data collected in the NHANES III survey to generate population-specific reference charts for children in the US. For participation in the NHANES III survey, parental consent was provided for all children <18 years of age and the protocol was approved by the National Center for Health Statistics Research Ethics Review Board.
Population
The NHANES III survey randomly selected participants from households in 81 counties in the US, with a goal of enrolling a representative sample of the US population.26,27 The study design included an oversampling of young, non-Hispanic black (NHB) and Mexican American children and these are corrected for using weighted analysis, summarized below.28 All children aged 2-18 years included in this NHANES III survey that had standing and sitting height measurements performed were included in this analysis.
Anthropometry
Anthropometric measurements were performed in the NHANES mobile examination center (MEC) that was equipped with a digital floor scale and a wall-mounted stadiometer. The stadiometer was calibrated using calibration rods at each new MEC stand, every 2 weeks, and at the end of each MEC stand. For height measurements, the participant stood on the floor-board of the stadiometer with both heels together. Heels, buttocks, and scapulae were touching the vertical backboard. The participant’s arms were allowed to hang freely by their side, with palms facing thighs. The head was in the Frankfurt horizontal plane.
To measure sitting height, the participant sat on a measurement box with their back and buttocks touching the backboard of the stadiometer, knees directed straight ahead, arms and hands resting at their side, and head in the Frankfort horizontal plane.29 Leg length was calculated by subtracting sitting height from standing height.
If permission was given, a board-eligible physician assessed pubertal stage in participants aged 8-18 years. Pubertal stage was assigned according to male genitalia or female breast.30 Ancestry was self-reported.
SitHt/Ht Chart Development
The SitHt/Ht was calculated for all participants. Children with physiologically improbable measurements were excluded from the sample as follows. A third-degree polynomial regression of SitHt/Ht against age, with an age/sex interaction was performed. Polynomial age terms were included to adjust for the non-linear relationship with age. Standardized residuals were calculated and participants with residuals ≥3.5 or <−3.5 SD from the mean were removed.
The NHANES used a strategic random sampling strategy and assigned sample weights to data from each participant. The weighting assigned to all participants who underwent MEC assessment (designated WTPFEX6 in the NHANES dataset) was used in generating population-specific reference charts representative of the entire US population, as described elsewhere.28,31 All analyses included these sample weights and were performed separately for each imputation.26 Sex-specific reference curves for SitHt/Ht were generated using LMS Chartmaker Pro (Harlow Printing Ltd., Tyne and Wear, UK). The LMS method uses a Box-Cox transformation to obtain normality, and separate smooth curves are generated for skewness, median, and variability.32 These are constrained to smooth changes over time and combined in one graph. As per software recommendations, these were adjusted until the fit of the curve was visually optimized.
Statistical Analyses
Using the weighted NHANES data, a population-specific growth chart was generated and SitHt/Ht Z-scores were calculated for each participant. Comparisons of SitHt/Ht Z-scores across ancestries on a single-population centile chart and of absolute values for SitHt/Ht between ancestries and pubertal stages were performed using ANOVA. The Scheffe test was used for post-hoc comparisons between groups. Statistical analyses were performed using Stata SE 14.0 (StataCorp LLC, College Station, Texas) and SPSS 25.0 (IBM, New York, New York).
Results
Of the 31 311 participants included in NHANES III, 10,305 were between 2 and 18 years of age. There were 205 excluded for missing a sitting or standing height measurement, and 42 were excluded as outliers. An additional were 489 excluded from ancestry analyses due to having ancestries other than non-Hispanic white (NHW), NHB and Mexican American. Of the remaining 9569 children, 2715 were of NHW, 3336 of NHB, and 3518 of Mexican American ancestry (Figure 1).
Figure 1.

Consort diagram demonstrating participants aged 2-18 years included in centile chart production and analyses.
Among the 4090 participants with assessed pubertal status, 928 were prepubertal, 1444 were Tanner stage 2-3, and 1718 were Tanner stage 4-5. For all ages, puberty stage and sex groups, SitHt/Ht were lower in male and female NHB children compared with NHW or Mexican American children (Table I; available at www.jpeds.com). Across the entire population in both sexes, SitHt/Ht was higher among prepubertal (Tanner stage 1) participants compared with those in early puberty (Tanner stage 2-3) (P < .001), indicating that there is more long bone than spinal growth in early puberty. The opposite is true in later puberty, as SitHt/Ht were greater among later pubertal (Tanner stage 4-5) participants were compared with those in early puberty (Tanner stages 2-3) (P < .001). This same pattern was seen when NHW, NHB, and Mexican American children were analyzed separately (Table I and Figure 2).
Figure 2.
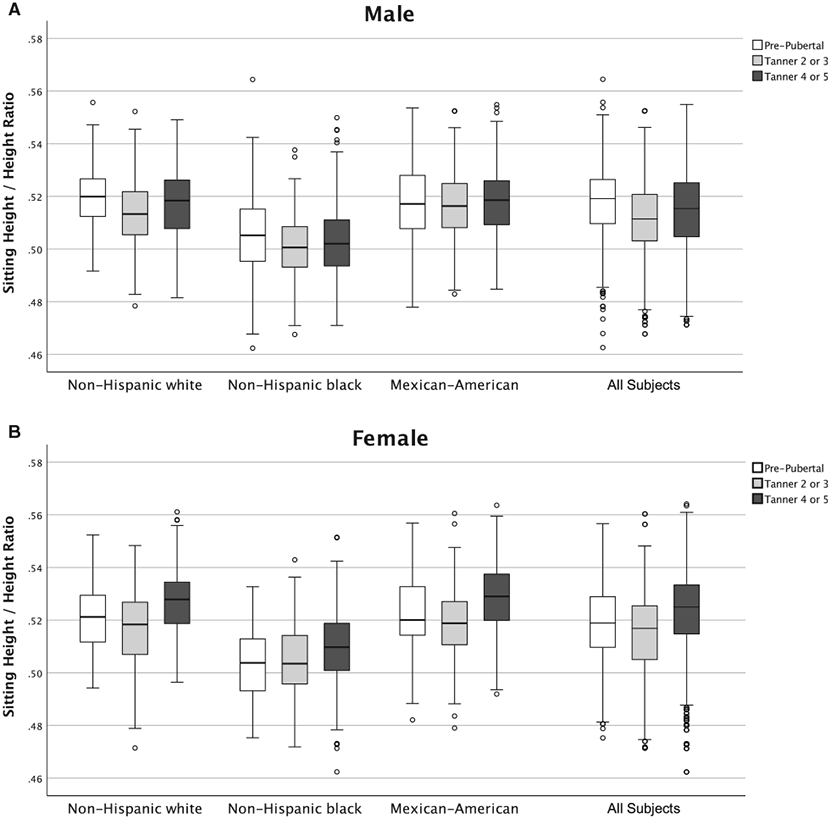
SitHt/Ht in prepuberty, early puberty (Tanner 2 or 3) or late puberty (Tanner 4 or 5) in male and female children aged ≥8 years. There is relative increase in lower limb growth in early puberty followed by a relative increase in spinal growth in later puberty. This pattern is seen in both males and females and is statistically significant (P < .001).
The distribution of SitHt/Ht in NHB children was lower than that of NHW and Mexican American children throughout childhood (Figure 3, A and B). Sex-specific references ranges and corresponding growth charts for SitHt/Ht relative to age were created using the entire cohort with weighted representation of ancestries to reflect the US Population (Figure 5; available at www.jpeds.com). Z-scores calculated from these sex-specific reference charts showed that the mean ± SD Z-score was lowest in NHB (−0.6 ± 0.9 males, −0.64 ± 0.9 females) when compared with NHW (0.29 ± 0.9 males, 0.34 ± 0.9 females) (P < .001) and with Mexican American (0.32 ± 0.9 males, 0.31 ± 0.9 females) children (P < .001) (Figure 3, C). When Z-scores were compared between NHW and Mexican American children, the difference between these groups was not statistically significant using this approach (P = .1).
Figure 3.
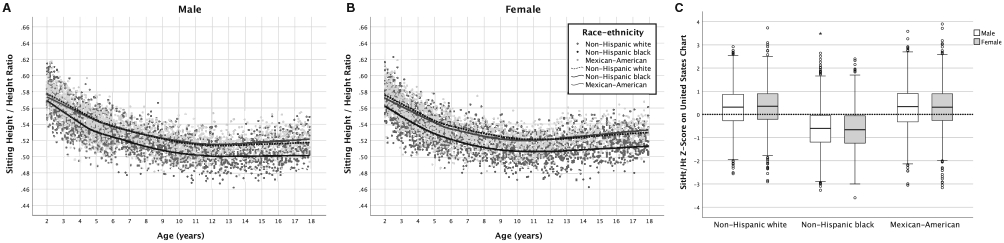
A and B, Scatterplot demonstrating lower SitHt/Ht in NHB children throughout childhood when compared with NHW and Mexican American children. C, Distribution of Z-scores in each ancestry when a single centile chart for the entire US population is used to calculate SitHt/Ht Z-scores. C, NHB children will have SitHt/Ht z-scores of approximately −0.6, whereas NHW and Mexican American children will have an average z-score of +0.3.
Figure 5.

Ancestry-agnostic SitHt/Ht centile charts for all male and female children in the US. This was generated using weighted representations of ethnicities, to reflect the distribution of the US population. Note that NHB children with have an average z-score of −0.6, and NHW and Mexican American children will have an average z-score of +0.3 using this chart.
Given this marked difference in body proportion in children of NHB ancestry, separate sex-specific SitHt/Ht smoothed centile charts were created for NHB and for the combined sample of NHW and Mexican American children (Figure 4). Detailed LMS data are presented for these charts in Tables II-VI (available at www.jpeds.com).
Figure 4.

Ancestry and sex-specific SitHt/Ht charts for NHW, NHB, and Mexican American youth in the US.
Discussion
We have generated sex-specific sitting height reference charts for children in the US, and described significant differences in SitHt/Ht between NHB and NHW or Mexican American children in the US. These differences present challenges in developing an ancestry-agnostic SitHt/Ht chart to identify children with disproportionate growth across the predominant ancestry groups in the US. We have created separate SitHt/Ht charts for NHB and for NHW and Mexican American children. In addition, we have described the pattern of early and late pubertal long bone and spinal growth in male and female children.
Although sex-specific reference charts for all ancestry groups in the US would be more convenient for clinical use, we have demonstrated that this approach would lead to a substantial difference of approximately 0.9 Z-scores between mean SitHt/Ht measurements of NHB children when compared with NHW or Mexican American children. This difference could result in the misdiagnosis of disproportion, especially in NHB children. Therefore, we developed ancestry-specific reference charts for this measure, an approach used by other studies describing reference data for characteristics that differ across ancestries.33 Our observation of lower SitHt/Ht in NHB children is consistent with prior studies of NHB and NHW children in Philadelphia by Krog-man et al and in Washington, DC, by Verghese et al in the early 1970s.34,35 In fact, NHB children living in the US have relatively longer legs even when compared with NHB children in Nigeria and in Tanzania.19,34,35 NHB children have a faster tempo of linear growth in childhood, which may also contribute to ethnic differences in proportion.36 Thus, it is not surprising that a separate SitHt/Ht chart is required for clinical use. Furthermore, the data in this study differ from previously reported reference data in other populations. Turkish children generally have higher mean SitHt/Ht than the NHW, Mexican American, and NHB children in the US, and Sit/Ht ratios in Dutch children are closer to those of the NHW and Mexican American children in this study.8,37 These population differences reinforce the need to generate population-specific reference charts for this measure.
Currently, children identified as having short stature are assessed for medical etiologies, including celiac disease and thyroid dysfunction, and these tests have an extremely low diagnostic yield in asymptomatic children.2 Although skeletal dysplasias can result in marked disproportion detected on routine clinical examination, skeletal dysplasias may be more subtle in some children. These children may be misdiagnosed as having idiopathic short stature or small for gestational age, and may even be treated with growth hormone under these indications.13 In some cases, children with mild skeletal dysplasia could have avoided unnecessary testing and been diagnosed more efficiently if disproportionate short stature was identified early through SitHt/Ht measurement.2,5,8 The American College of Medical Genetics recommends performing a skeletal survey in children with disproportionate short stature, and accurate determination of disproportion will ensure that the radiation exposure associated with this study is limited to those where it is clinically indicated.38 Current pediatric practice does not routinely include SitHt/Ht measurement, but the reference charts developed in this study make such practice both feasible and clinically relevant. In addition, these charts may have a role in characterizing the effects of adverse environmental and nutritional conditions on childhood growth.
Early and late puberty can also affect SitHt/Ht, and this factor should be considered when interpreting the ratio in adolescents. Children with delayed puberty can have a lower SitHt/Ht than would be expected for age on these growth charts.39,40 In this study, we have further characterized the difference in proportionate growth in early and late puberty. In both males and females, lower limb growth exceeds trunk growth in early puberty and the opposite pattern is seen in later puberty.
The strengths of this study include the large sample size and the use of sample weights to provide data that represent the US pediatric population. However, it should be noted that these data are from measurements of children between 1988 and 1994. Unfortunately, more recent data are not available, because NHANES did not measure sitting height in subsequent surveys. Although we have not validated these charts as a screening tool for skeletal dysplasia, a similar approach in the Netherlands has demonstrated that children with mild hypochondroplasia can be identified with population-specific reference charts.8 SitHt/Ht assessment has also been described previously as a screening tool to identify children for short stature homeobox-containing haploinsufficiency testing.10,41 Further study will be required to determine the diagnostic accuracy of this screening tool and describe how the predictive value of this test changes as the magnitude of a child’s SitHt/Ht difference from the population mean increases.
The SitHt/Ht can be useful in screening for disproportionate growth and may play a role in guiding the diagnosis and management of children with short stature. In the US, male and female NHB children have significantly lower SitHt/Ht at all ages and this must be considered in interpreting measurements in children of different ancestries. We suggest the use of these standardized reference charts in screening for disproportionate growth and in considering whether a diagnosis of skeletal dysplasia should be considered in children with short stature or faltering growth.
Supplementary Material
Glossary
- MEC
Mobile examination center
- NHANES
National Health and Nutrition Examination Surveys
- NHB
Non-Hispanic black
- NHW
Non-Hispanic white
- SitHt/Ht
Sitting height to standing height ratio
Footnotes
A.G. served as consultant for the Pediatric Endocrine Society Growth Hormone Deficiency Knowledge Center, sponsored by Sandoz. The other authors declare no conflicts of interest.
Data Statement
Data sharing statement available at www.jpeds.com.
References
- 1.Hagan JF, Shaw JS, Duncan PM. Bright Futures: guidelines for health supervision of infants, children, and adolescents. Itasca (IL): American Academy of Pediatrics; 2008. [Google Scholar]
- 2.Sisley S, Trujillo MV, Khoury J, Backeljauw P. Low incidence of pathology detection and high cost of screening in the evaluation of asymptomatic short children. J Pediatr 2013;163:1045–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Grote FK, Oostdijk W, De Muinck Keizer-Schrama SM, van Dommelen P, van Buuren S, Dekker FW, et al. The diagnostic work up of growth failure in secondary health care; an evaluation of consensus guidelines. BMC Pediatr 2008;8:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Baron J, Savendahl L, De Luca F, Dauber A, Phillip M, Wit JM, et al. Short and tall stature: a new paradigm emerges. Nat Rev Endocrinol 2015;11:735–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dauber A, Rosenfeld RG, Hirschhorn JN. Genetic evaluation of short stature. J Clin Endocrinol Metab 2014. jc20141506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Freire BL, Homma TK, Funari MFA, Lerario AM, Vasques GA, Malaquias AC, et al. Multigene sequencing analysis of children born small for gestational age with isolated short stature. J Clin Endocrinol Metab 2019;104:2023–30. [DOI] [PubMed] [Google Scholar]
- 7.Hauer NN, Popp B, Schoeller E, Schuhmann S, Heath KE, Hisado-Oliva A, et al. Clinical relevance of systematic phenotyping and exome sequencing in patients with short stature. Genet Med 2018;20:630–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fredriks AM, van Buuren S, van Heel WJ, Dijkman-Neerincx RH, Ver- loove-Vanhorick SP, Wit JM. Nationwide age references for sitting height, leg length, and sitting height/height ratio, and their diagnostic value for disproportionate growth disorders. Arch Dis Child 2005;90:807–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mortier GR, Cohn DH, Cormier-Daire V, Hall C, Krakow D, Mundlos S, et al. Nosology and classification of genetic skeletal disorders: 2019 revision. Am J Med Genet A 2019;179:2393–419. [DOI] [PubMed] [Google Scholar]
- 10.Malaquias AC, Scalco RC, Fontenele EG, Costalonga EF, Baldin AD, Braz AF, et al. The sitting height/height ratio for age in healthy and short individuals and its potential role in selecting short children for SHOX analysis. Horm Res Paediatr 2013;80:449–56. [DOI] [PubMed] [Google Scholar]
- 11.Gkourogianni A, Andrew M, Tyzinski L, Crocker M, Douglas J, Dunbar N, et al. Clinical characterization of patients with autosomal dominant short stature due to aggrecan mutations. J Clin Endocrinol Metab 2017;102:460–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Merker A, Neumeyer L, Hertel NT, Grigelioniene G, Mohnike K, Hagenas L. Development of body proportions in achondroplasia: sitting height, leg length, arm span, and foot length. Am J Med Genet A 2018;176:1819–29. [DOI] [PubMed] [Google Scholar]
- 13.Flechtner I, Lambot-Juhan K, Teissier R, Colmenares A, Baujat G, Beltrand J, et al. Unexpected high frequency of skeletal dysplasia in idiopathic short stature and small for gestational age patients. Eur J Endocrinol 2014;170:677–84. [DOI] [PubMed] [Google Scholar]
- 14.Song D, Maher CO. Spinal disorders associated with skeletal dysplasias and syndromes. Neurosurg Clin N Am 2007;18:499–514. [DOI] [PubMed] [Google Scholar]
- 15.Hall J, Allanson J, Gripp K, Slavotinek A. Handbook of physical measurements. Oxford (UK): Oxford University Press; 2006. [Google Scholar]
- 16.Dimeglio A. Growth in pediatric orthopaedics. J Pediatr Orthop 2001;21:549–55. [PubMed] [Google Scholar]
- 17.Hall J, Allanson J, Gripp K, Slavotinek A. Proportional growth and normal variants. Handbook of Physical Measurements. Oxford (UK): Oxford University Press; 2006. [Google Scholar]
- 18.Eveleth PB, Tanner JM, Tanner JM. Worldwide variation in human growth. Cambridge (UK): Cambridge University Press; 1990. [Google Scholar]
- 19.Eveleth PB. Differences between populations in body shape of children and adolescents. Am J Phys Anthropol 1978;49:373–81. [DOI] [PubMed] [Google Scholar]
- 20.Quanjer PH, Capderou A, Mazicioglu MM, Aggarwal AN, Banik SD, Popovic S, et al. All-age relationship between arm span and height in different ethnic groups. Eur Respir J 2014;44:905–12. [DOI] [PubMed] [Google Scholar]
- 21.Tanner JM, Hayashi T, Preece MA, Cameron N. Increase in length of leg relative to trunk in Japanese children and adults from 1957 to 1977: comparison with British and with Japanese Americans. Ann Hum Biol 1982;9:411–23. [DOI] [PubMed] [Google Scholar]
- 22.Wales JK, Herber SM, Taitz LS. Height and body proportions in child abuse. Arch Dis Child 1992;67:632–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dangour AD, Schilg S, Hulse JA, Cole TJ. Sitting height and subischial leg length centile curves for boys and girls from Southeast England. Ann Hum Biol 2002;29:290–305. [DOI] [PubMed] [Google Scholar]
- 24.Cox SL, Ruff CB, Maier RM, Mathieson I. Genetic contributions to variation in human stature in prehistoric Europe. Proc Natl Acad Sci U S A 2019;116:21484–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.US Department of Health and Human Services Centers for Disease Control and Prevention. Anthropometric reference data for children and adults: United States 1988-1994. Washington (DC): Author; 2009. [Google Scholar]
- 26.Johnson CL, Paulose-Ram R, Ogden CL, Carroll MD, Kruszon-Moran D, Dohrmann SM, et al. National Health and Nutrition Examination Survey: analytic guidelines, 1999-2010. Vital Health Stat 2013;2:1–24. [PubMed] [Google Scholar]
- 27.Plan and operation of the Third National Health and Nutrition Examination Survey, 1988-94. Series 1: programs and collection procedures. Vital Health Stat 1994;1:1–407. [PubMed] [Google Scholar]
- 28.Mohadjer L, Montaquila JM, Waksberg J, Bell B, James P, Flores-Cervantes I, et al. National Health and Nutrition Examination Survey III: weighting and estimation methodology. Washington (DC): US Department of Health and Human Services; 1996. [Google Scholar]
- 29.National Health and Nutrition Examination Survey III. Body measurements (Anthropometry) manual. Washington (DC): US Department of Health and Human Services; 1988. [Google Scholar]
- 30.Tanner JM. Normal growth and techniques of growth assessment. Clin Endocrinol Metab 1986;15:411–51. [DOI] [PubMed] [Google Scholar]
- 31.National Center for Health Statistics Centers for Disease Control and Prevention. Analytic and Reporting Guidelines: The Third National Health and Nutrition Examination Survey, NHANES III (1988-94). Washington (DC): US Department of Health and Human Services; 1996. [Google Scholar]
- 32.Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med 1992;11:1305–19. [DOI] [PubMed] [Google Scholar]
- 33.Kindler JM, Lappe JM, Gilsanz V, Oberfield S, Shepherd JA, Kelly A, et al. Lumbar spine bone mineral apparent density in children: results from the Bone Mineral Density in Childhood Study. J Clin Endocrinol Metab 2019;104:1283–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Krogman WM. Growth of head, face, trunk, and limbs in Philadelphia white and Negro children of elementary and high school age. Monogr Soc Res Child Dev 1970;35:1–80. [PubMed] [Google Scholar]
- 35.Verghese KP, Scott RB, Teixeira G, Ferguson AD. Studies on growth and development. XII. Physical growth of North American Negro Children. Pediatrics 1969;44:243–7. [PubMed] [Google Scholar]
- 36.Komlos J, Breitfelder A. Differences in the physical growth of US-born black and white children and adolescents ages 2-19, born 1942-2002. Ann Hum Biol 2008;35:11–21. [DOI] [PubMed] [Google Scholar]
- 37.Bundak R, Bas F, Furman A, Gunoz H, Darendeliler F, Saka N, et al. Sitting height and sitting height/height ratio references for Turkish children. Eur J Pediatr 2014;173:861–9. [DOI] [PubMed] [Google Scholar]
- 38.Seaver LH, Irons M. American College of Medical Genetics Professional Practice and Guidelines Committee. ACMG practice guideline: genetic evaluation of short stature. Genet Med 2009;11:465–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Albanese A, Stanhope R. Does constitutional delayed puberty cause segmental disproportion and short stature? Eur J Pediatr 1993;152:293–6. [DOI] [PubMed] [Google Scholar]
- 40.Poyrazoglu S, Gunoz H, Darendeliler F, Saka N, Bundak R, Bas F. Constitutional delay of growth and puberty: from presentation to final height. J Pediatr Endocrinol Metab 2005;18:171–9. [DOI] [PubMed] [Google Scholar]
- 41.Binder G, Ranke MB, Martin DD. Auxologyis a valuable instrument for the clinical diagnosis of SHOX haploinsufficiency in school-age children with unexplained short stature. J Clin Endocrinol Metab 2003;88:4891–6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data sharing statement available at www.jpeds.com.