

Abstract
This study uses data from the Vaccine Safety Datalink on receipt of booster doses of COVID-19 vaccines among pregnant individuals aged 18 to 49 years.
Booster doses of COVID-19 vaccines were recommended for people aged 18 years or older in November 2021 following the recommendation of an additional primary dose of COVID-19 vaccine for select immunocompromised populations on August 13, 2021.1 As of February 26, 2022, more than 93 million booster doses of COVID-19 vaccines had been administered in the US2; however, data on receipt of booster doses among pregnant individuals are lacking. We present findings on receipt of booster doses among pregnant individuals in the Vaccine Safety Datalink (VSD).
Methods
The VSD is a collaboration between the Immunization Safety Office at the US Centers for Disease Control and Prevention and 9 integrated health care organizations, 8 of which provide data and 1 provides subject matter expertise. This analysis used VSD’s validated dynamic pregnancy algorithm to identify and estimate pregnancies weekly3 and included individuals who were pregnant during the week ending February 26, 2022. This research was reviewed and approved by the US Centers for Disease Control and Prevention and all participating VSD sites with a waiver of informed consent.
In addition, we assessed trends over time among individuals who were pregnant during each specified week since August 13, 2021 (when additional doses were first authorized). Vaccination data came from electronic health records, medical and pharmacy claims, and regional or state immunization information systems, which would capture vaccinations regardless of source. We included pregnant individuals who received either a booster dose or an additional primary dose, which could not be analyzed individually.
We assessed receipt of booster doses among fully vaccinated (defined as receipt of 2 doses of the Pfizer-BioNTech [BNT162b2] or Moderna [mRNA-1273] vaccines or 1 dose of the Johnson & Johnson [JNJ-78436735] vaccine) pregnant individuals aged 18 to 49 years overall, by race and ethnicity, and by whether the dose was received before or during pregnancy. Race and ethnicity was self-reported using open-ended questions and was included to highlight any inequities in vaccine uptake. The analyses were performed using SAS software version 9.4 (SAS Institute Inc).
Results
Among 71 745 individuals in the VSD who were pregnant during the week ending on February 26, 2022, 49 072 (68.4%) were fully vaccinated. Among those who were fully vaccinated, 24 321 (49.6%) had received a booster dose. Receipt of a booster dose was highest among pregnant individuals aged 35 to 49 years (60.4%), Asian individuals (63.7%), and non-Hispanic White individuals (57.9%).
Receipt of a booster dose was lowest among pregnant individuals aged 18 to 24 years (22.3%), non-Hispanic Black individuals (30.8%), and Hispanic individuals (37.6%). Among pregnant individuals who received a booster dose, 10.9% received it before pregnancy and 89.1% during pregnancy (Table). Furthermore, uptake of booster dose remained lowest among non-Hispanic Black and Hispanic pregnant individuals since August 2021 (Figure).
Table. Receipt of COVID-19 Booster Dose Among Fully Vaccinated Pregnant Individuals Aged 18 to 49 Years by Select Characteristics and Timing of Receipt of Booster Dose With Respect to Pregnancya.
| Characteristic | Total No. of pregnant individuals | No. (%) | ||
|---|---|---|---|---|
| Fully vaccinated pregnant individualsb | Receipt of booster dose among fully vaccinatedc | Receipt of booster dose during pregnancyd | ||
| Total | 71 745 | 49 072 (68.4) | 24 321 (49.6) | 21 662 (89.1) |
| Age group, y | ||||
| 18-24 | 9571 | 4489 (46.9) | 999 (22.3) | 923 (92.4) |
| 25-34 | 45 096 | 31 211 (69.2) | 15 242 (48.8) | 13 729 (90.1) |
| 35-49 | 17 078 | 13 372 (78.2) | 8080 (60.4) | 7010 (86.8) |
| Race and ethnicitye | ||||
| Asian | 10 548 | 9230 (87.5) | 5880 (63.7) | 5157 (87.7) |
| Hispanic | 24 170 | 16 003 (66.9) | 6020 (37.6) | 5435 (90.3) |
| Non-Hispanic Black | 5064 | 2765 (54.4) | 850 (30.8) | 772 (90.8) |
| Non-Hispanic White | 23 534 | 15 490 (65.8) | 8970 (57.9) | 7948 (88.6) |
| Otherf | 3270 | 2219 (67.9) | 1065 (48.0) | 958 (90.0) |
Data are from the US Vaccine Safety Datalink (end date: February 26, 2022). The time interval between the primary series and booster dose was not considered.
Defined as receipt of 2 doses of the Pfizer-BioNTech (BNT162b2) or Moderna (mRNA-1273) vaccines or 1 dose of the Johnson & Johnson (JNJ-78436735) vaccine.
Includes anyone who was fully vaccinated and had received another dose of COVID-19 vaccine as of February 26, 2022 (received booster doses and those who received additional doses as part of the primary series).
Includes individuals who were pregnant during week ending February 26, 2022. If the pregnancy ended prior to this date, the individual was excluded from the numerator and the denominator.
Self-reported using open-ended questions and category was included to highlight any inequities in vaccine uptake. The numbers do not add up to the total due to missing race and ethnicity for 5284 pregnant individuals.
Includes American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, and multiple or other races.
Figure. Receipt of COVID-19 Booster Dose Overall, by Race and Ethnicity, and by Week Ending Date Among Fully Vaccinated Pregnant Individuals Aged 18 to 49 Years.
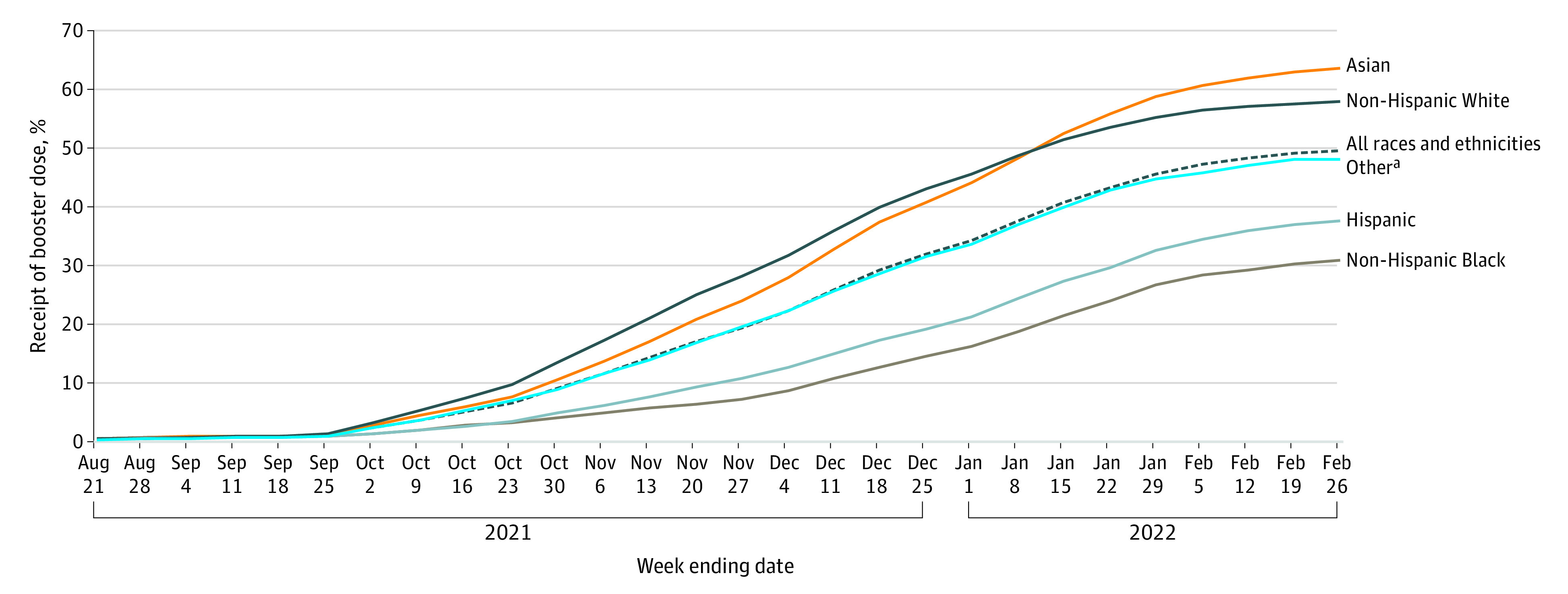
Data are from the US Vaccine Safety Datalink. The percentage of pregnant individuals who received a booster dose includes anyone fully vaccinated and who has received another dose of COVID-19 vaccine as of February 26, 2022. This includes people who received booster doses and people who received additional doses. The time interval between the primary series and the booster dose was not considered. Fully vaccinated was defined as receipt of 2 doses of the Pfizer-BioNTech (BNT162b2) or Moderna (mRNA-1273) vaccines or 1 dose of the Johnson & Johnson (JNJ-78436735) vaccine. Race and ethnicity was self-reported using open-ended questions and was included to highlight any inequities in vaccine uptake. The denominator includes individuals who were pregnant during each specified week since August 13, 2021. Additional doses of the COVID-19 vaccine were recommended for individuals who are immunocompromised beginning on August 13, 2021; therefore, weekly reporting for these doses started the week ending on August 21, 2021.
aIncludes American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, and multiple or other races.
Discussion
Using data from the VSD, it is estimated that less than half of fully vaccinated pregnant individuals had received a COVID-19 booster dose by February 2022 with differences observed by age and race and ethnicity. Several limitations should be noted. First, although vaccination status was identified using multiple data sources, some vaccinations among pregnant individuals may have been missed. Second, this analysis did not differentiate between an additional primary and a booster dose. Third, this analysis did not account for the time interval between receipt of primary dose or series of doses and the booster dose; therefore, pregnant individuals who were not yet eligible to receive a booster dose may have been included, leading to underestimation of booster dose coverage. Fourth, pregnancies in the VSD are generally identified at approximately 8 to 10 weeks’ gestational age; therefore, pregnancies since November 2021 may be underrepresented. Fifth, the findings may not be generalizable to the population of pregnant individuals in the US.4
Despite these limitations, the findings can inform strategies to increase booster dose vaccinations and effective messaging. COVID-19 vaccinations significantly lower the risk of serious illness from COVID-19 in pregnant individuals, and data indicate potential benefits to the developing fetus.5,6 Thus, continued focus to improve vaccinations with booster doses in this population, especially among those with lower vaccination coverage, such as individuals of Black or Hispanic race and ethnicity, is critical.
Section Editors: Jody W. Zylke, MD, Deputy Editor; Kristin Walter, MD, Associate Editor.
References
- 1.US Centers for Disease Control and Prevention . CDC expands eligibility for COVID-19 booster shots to all adults. Accessed January 22, 2022. https://www.cdc.gov/media/releases/2021/s1119-booster-shots.html
- 2.US Centers for Disease Control and Prevention . COVID-19 vaccinations in the United States. Accessed December 9, 2021. https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-people-onedose-pop-5yr
- 3.Naleway AL, Crane B, Irving SA, et al. Vaccine Safety Datalink infrastructure enhancements for evaluating the safety of maternal vaccination. Ther Adv Drug Saf. 2021;12:20420986211021233. doi: 10.1177/20420986211021233 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sukumaran L, McCarthy NL, Li R, et al. Demographic characteristics of members of the Vaccine Safety Datalink (VSD): a comparison with the United States population. Vaccine. 2015;33(36):4446-4450. doi: 10.1016/j.vaccine.2015.07.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fell DB, Dhinsa T, Alton GD, et al. Association of COVID-19 vaccination in pregnancy with adverse peripartum outcomes. JAMA. Published online March 24, 2022. doi: 10.1001/jama.2022.4255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Magnus MC, Örtqvist AK, Dahlqwist E, et al. Association of SARS-CoV-2 vaccination during pregnancy with pregnancy outcomes. JAMA. Published online March 24, 2022. doi: 10.1001/jama.2022.3271 [DOI] [PMC free article] [PubMed] [Google Scholar]