

Abstract
Background:
Macroeconomic changes are associated with population health outcomes, such as mortality, accidents, and alcohol use. Diet quality is a risk or protective factor that could be influenced by economic conditions.
Objective:
This study examined the trajectory of diet quality measured by the Healthy Eating Index 2015 before, during, and after the 2008/2009 Great Recession.
Design:
Repeated cross-sectional survey data from the National Health and Nutrition Examination Survey (NHANES) were analyzed.
Participants/setting:
The analytic sample included 48,679 adults who completed at least one dietary recall from NHANES 1999–2018.
Main Outcome Measures:
Diet quality was assessed with a 24-hour dietary recall to calculate the Healthy Eating Index (HEI)-2015 total scores, a measure of the conformance with the 2015–2020 Dietary Guidelines for Americans.
Statistical Analyses Performed:
Least squares regression was used to adjust for demographic changes across waves.
Results:
Diet quality improved noticeably during the Great Recession and deteriorated as economic conditions improved.
Conclusions:
Deteriorating economic circumstances may constrain choices, but that does not necessarily imply a worsening of dietary quality. During the Great Recession, American diets became more consistent with Dietary Guidelines for Americans recommendations, possibly because of a shift towards food prepared at home instead of prepared food bought away from home.
Keywords: Healthy Eating Index, Economic conditions, Recession, NHANES
Introduction
Dietary guidelines aim to reduce the societal burden of diet-related diseases, as poor diet quality is a risk factor for chronic conditions, premature mortality and lower disability-adjusted life years.1,2 The Great Recession, which had a major economic impact worldwide, is now well in the past3 and consistent data that cover the period before, during, and after it are now available. In the US, the recession technically lasted from December 2007 – June 2009 as measured by the nominal GDP trough,3 but unemployment rates reacted with a lag and peaked at 10% in October 2009, a level that had not been reached in the previous 25 years.4 Recovery was slower— unemployment rates dropped to 2005 levels by 2015.4 But economic conditions kept improving and by 2018, the seasonally adjusted unemployment rate had dropped under 4%, far below the historical average since 1948 and reached the lowest levels since 1969.4
The analysis of diet quality falls under the broader topic of economic conditions and health, including the seemingly counterintuitive association that economic downturns are often accompanied by lower overall mortality rates and improvements in some measures of physical health.5–9 The relationship between economic downturns and reduced mortality appears to have weakened in more recent periods,5 possibly because some causal pathways may have become less important, such as reduced air pollution and occupational or traffic accidents during downturns.10,11 Other relationships have always been in the opposite direction, such as increased suicide rates during economic downturns,12 which may have become more important recently.
Evidence on causal pathways remains far from being settled. One proposed pathway is through improved health behaviors, for example reduced smoking, loss of excess body weight and increased leisure-time physical activity during economic downturns.13 In contrast, another study concluded that 2008/2009 Great Recession negatively impacted blood pressure and blood glucose levels, casting doubt on the idea of improved cardiovascular health.14
Previous studies have reported improvements in diet quality over time.15–17 Wilson and colleagues fitted a linear trend line to the National Health and Nutrition Examination Survey (NHANES) data from 1999/2000 to 2011/2012 and concluded that the average Healthy Eating Index-2010 (HEI-2010) scores increased about 1.6 points every two years.15 Based on this time trend, they predicted that the US population could reach a total HEI-2010 score of 65 by the year 2020, a large improvement since the beginning of the current NHANES data collection (1999/2000), but still 9 points short of the Healthy People 2020 targets.15
This paper focuses on the relationship between macroeconomic conditions and diet quality, separating out demographic trends such as increasing levels of education and aging population. It uses several cycles of NHANES data, including recent waves that span the largest macroeconomic swings in the last 80 years with both a downturn and a recovery.
Materials and Methods
Data source
This analysis uses one-day 24-recall dietary data from NHANES 1999–2018, a nationally representative survey conducted every two years on health and nutritional status of the noninstitutionalized civilian population in the United States.18 The Research Ethics Review Board of the National Center for Health Statistics has approved NHANES protocols and written informed consents are obtained for all participants. Since NHANES is publicly available and contains no information that can identify subjects, this study is deemed exempt from the Institutional Review Board (IRB) under federal regulation 45 46.101 (b) CFR.
Analytic Sample
The study population consists of 48,679 respondents aged 18 years or older who completed an in-person dietary recall interview by a trained interviewer and with complete data on sex, age, race/ethnicity, and educational level.19 Beginning in 2003, a second 24-hour recall was added, but administered by telephone 3 to 10 days after the first interview.19 For consistency over time, we only use the first 24-hour dietary recall across all waves; early and later waves would not be comparable otherwise due to the changes in survey administration. As a sensitivity analysis, we use both recalls in later waves– that is, we sum across the dietary constituents consumed in both recalls per person then take the ratio before applying the scoring standards.20
Assessment of Diet Quality
Diet quality is assessed by the Healthy Eating Index-2015 (HEI-2015),21,22 which measures conformance with the 2015–2020 Dietary Guidelines for Americans.2 The HEI-2015 has 13 components, including nine components assessing adequacy (dietary components recommended for inclusion in a healthy diet) and four components assessing moderation (dietary components that should be consumed sparingly). Each of the components is scored on a density basis out of 1,000 calories and then scored according to standards, except for fatty acids, which is scored on a ratio of unsaturated to saturated fatty acid.23 The complete list of components is: (1) Total Fruits, (2) Whole Fruits, (3) Total Vegetables, (4) Greens and Beans, (5) Whole Grains, (6) Dairy, (7) Total Protein Foods, (8) Seafood and Plant Proteins, (9) Fatty Acids (the ratio of unsaturated fatty acids to saturated fatty acids), (10) Refined Grains, (11) Sodium, (12) Added Sugars, and (13) Saturated Fats.22 The first nine are adequacy components and the remaining four are moderation components. Total HEI-2015 score ranges from 0 (nonadherence) to 100 (perfect adherence).24
There are several methods to calculate the HEI for a data set, with different limitations.25 The resulting numbers can differ depending on assumptions about measurement error, episodic intake, skewness, or correlation between components energy.25 We use the Simple HEI Scoring Algorithm Method, which creates individual scores and can be used in regression models.20 Its disadvantage is that it has a higher variance due to episodic intake and can be more affected by measurement error than the population ratio method, which calculates a single number for a population and cannot be used in regression models.25 The calculation of HEI-2015 scores is performed using SAS and the macros provided by National Cancer Institute.20,26
Statistical Analysis
All analyses incorporate the dietary sample weights to ensure nationally representative estimates and standard errors are adjusted for stratification/clustering in the survey design. Ordinary least squares (OLS) regression is applied with the HEI-2015 scores as the dependent variable and the cycle indicator as the key independent variable to investigate the general trend. Wald F statistics are used to examine whether the coefficients of different cycles are statistically different.
Sociodemographic characteristics were controlled in the regression model for changes in the demographic composition over time. These demographic changes can affect diet quality,17,27 and we want to separate them from changes in diet quality over the economic cycle. Sex, age group in years, race/ethnicity, and educational level were collected by trained NHANES interviewers according to fixed categories provided by the National Center for Health Statistics using the Computer-Assisted Personal Interview system.28 Age is categorized into three groups (18–39, 40–59, 60 or above); race/ethnicity into non-Hispanic White participants, Hispanic participants, non-Hispanic Black participants, and participants of other race; educational levels into less than high school, high school, and some college or more. As a sensitivity check, a model that includes family income expressed as percentage of the federal poverty guideline (<130%, 130%−349%, 350% or above) is also estimated. All data are analyzed using Stata 16 and statistical significance was set at a 2-tailed P < 0.05 for all primary analyses.29
Results
Between 1999 and 2018, the demographic characteristics of the US population changed, with fewer non-Hispanic White respondents, an increase in age, and an increase in education. (Table 1)
Table 1:
Sociodemographic Characteristics of US Adults in the National Health and Nutrition Examination Survey, 1999 to 2018
| 1999–2000 | 2001–2002 | 2003–2004 | 2005–2006 | 2007–2008 | 2009–2010 | 2011–2012 | 2013–2014 | 2015–2016 | 2017–2018 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | ||||||||||
| Number of unique participants | 4225 | 4738 | 4442 | 4518 | 5416 | 5749 | 4798 | 5044 | 5015 | 4734 |
| Socio-demographics, n (weighted %) | ||||||||||
| Sex | ||||||||||
| Male | 1,972 (47.78) | 2,247 (48.22) | 2,131 (48.06) | 2,163 (48.04) | 2,661 (47.09) | 2,785 (48.18) | 2,392 (48.72) | 2,413 (48.51) | 2,414 (48.13) | 2,302 (48.01) |
| Female | 2,253 (52.22) | 2,491 (51.78) | 2,311 (51.94) | 2,355 (51.96) | 2,755 (52.91) | 2,964 (51.82) | 2,406 (51.28) | 2,631 (51.49) | 2,601 (51.87) | 2,432 (51.99) |
| Age group in years | ||||||||||
| 18–39 | 1,480 (43.95) | 1,731 (41.00) | 1,536 (38.86) | 1,747 (38.02) | 1,750 (37.54) | 1,925 (37.00) | 1,714 (36.27) | 1,744 (36.20) | 1,687 (36.19) | 1,430 (36.16) |
| 40–59 | 1,217 (33.30) | 1,486 (37.37) | 1,251 (37.09) | 1,375 (37.61) | 1,722 (38.81) | 1,931 (38.33) | 1,586 (37.93) | 1,734 (36.96) | 1,646 (35.86) | 1,500 (34.72) |
| 60+ | 1,528 (22.75) | 1,521 (21.63) | 1,655 (24.05) | 1,396 (24.37) | 1,944 (23.65) | 1,893 (24.67) | 1,498 (25.81) | 1,566 (26.84) | 1,682 (27.95) | 1,804 (29.12) |
| Race/ethnicity | ||||||||||
| Non-Hispanic White | 1,888 (70.57) | 2,491 (72.16) | 2,388 (72.98) | 2,274 (72.66) | 2,547 (70.19) | 2,781 (68.71) | 1,842 (66.57) | 2,233 (65.69) | 1,711 (64.44) | 1,694 (62.04) |
| Hispanic | 1,417 (13.95) | 1,197 (12.70) | 1,016 (10.84) | 1,049 (10.64) | 1,522 (13.24) | 1,642 (13.62) | 931 (14.28) | 1,125 (14.72) | 1,541 (15.03) | 1,055 (15.83) |
| Non-Hispanic Black | 787 (10.79) | 890 (10.95) | 864 (11.21) | 1,012 (11.49) | 1,136 (11.29) | 1,024 (11.40) | 1,272 (11.48) | 1,006 (11.36) | 1,060 (10.96) | 1,125 (11.58) |
| Othera | 133 (4.69) | 160 (4.19) | 174 (4.97) | 183 (5.22) | 211 (5.29) | 302 (6.28) | 753 (7.66) | 680 (8.22) | 703 (9.57) | 860 (10.55) |
| Educational Level | ||||||||||
| Less than high school graduate | 1,635 (23.97) | 1,421 (19.21) | 1,288 (18.14) | 1,234 (17.09) | 1,665 (20.10) | 1,634 (18.80) | 1,102 (16.32) | 1,028 (14.74) | 1,150 (13.77) | 891 (10.73) |
| High school graduate/GED | 957 (26.25) | 1,110 (24.73) | 1,111 (26.42) | 1,093 (25.39) | 1,341 (25.82) | 1,316 (22.46) | 1,008 (19.92) | 1,141 (22.30) | 1,108 (20.98) | 1,146 (28.13) |
| Some college or more | 1,633 (49.78) | 2,207 (56.06) | 2,043 (55.44) | 2,191 (57.52) | 2,410 (54.08) | 2,799 (58.75) | 2,688 (63.77) | 2,875 (62.97) | 2,757 (65.25) | 2,697 (61.14) |
Other race includes non-Hispanic Asian persons and non-Hispanic persons reported races other than Black, Asian, or White.
Figure 1 shows the adjusted predicted HEI-2015 scores using weighted OLS regression to control for demographic changes, with arrows indicating economic conditions and unemployment rates from the Bureau of Labor Statistics.4 Holding population characteristics constant, diet quality improved from 1999/2000 up to 2011/2012 and then deteriorated. Except for 2003/2004, the diet quality was significantly higher in every cycle until 2011/2012 than in 1999/2000. The highest adjusted predicted HEI-2015 score using weighted OLS regression occurred in the 2011/2012 cycle, a 2.22-point improvement from cycle 1999/2000 (p-value<0.001) and a 1.40-point increase over cycle 2005/2006 before the Great Recession (p-value<0.001).
Figure 1:
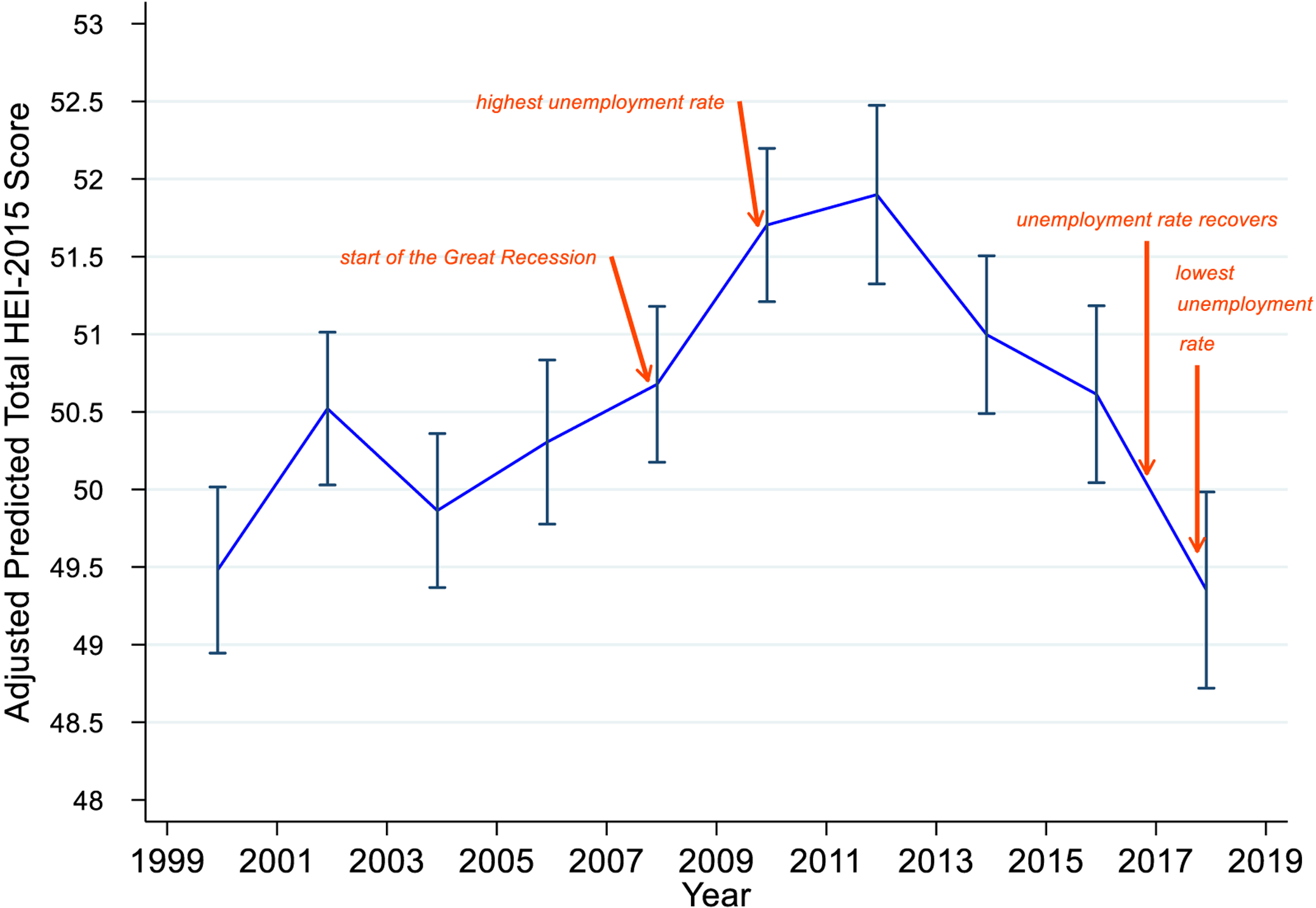
The Adjusted Predicted Total HEIa-2015 Score Trend and 95% Confidence Intervalb using the National Health and Nutrition Examination Survey, 1999–2018
a HEI = Healthy Eating Index
b predicted values and their 95% confidence intervals are from weighted ordinary least squares regression using margins command in Stata, controlling for sex, age group in years (18–39,40–59,60 or above), race/ethnicity (Non-Hispanic White, Hispanic, Non-Hispanic Black, and other race), and educational level (less than high school, high school graduate/ General Equivalency Diploma, some college/associates (AA) degree or higher)
Diet quality declined consistently in later waves from the peak in 2011/2012 just as unemployment rates decreased. By 2015/2016, adjusted average HEI-2015 scores deteriorated to the level of cycle 2005/2006, the latest wave before the Great Recession. National unemployment rates started to decline in 2010 and were lowest in the most recent cycle (2017/2018),4 in which diet quality is significantly lower than cycle 2005/2006 (p-value= 0.02) and no different than the adjusted predicted HEI-2015 score in 1999/2000 (p-value= 0.76). The sensitivity analysis using both recalls in waves later than 2003 and including the ratio of family income to poverty as a covariate demonstrate similar results.
In general, females had 1.53-point higher HEI-2015 score than males (p-value<0.001). (Table 2) Respondents ages 40 to 59 had on average 3.08-point higher HEI-2015 score than their younger counterparts (p-value<0.001), while those ages 60 or above are predicted to have 6.66-point higher HEI-2015 score than respondents ages 18 to 39 (p-value<0.001). (Table 2) Compared with non-Hispanic White respondents, Hispanic respondents possessed better diet quality (p-value<0.001), whilst non-Hispanic Black respondents had worse diet quality (p-value<0.001). Respondents with some college education had higher HEI-2015 scores than those who did not graduate from high school (p-value<0.001).
Table 2:
Result of multivariable-adjusteda OLSb regression, investigating factors associated with total HEIc-2015 score among American adults aged 18 and older who participated in the National Health and Nutrition Examination Survey, 1999–2018 (n =48,679)
| Coefficient | Standard Error | p-value | [95% Confidence | Interval] | |
|---|---|---|---|---|---|
| Year (reference: 1999/2000) | |||||
| 2001/2002 | 1.04 | 0.37 | 0.01 | 0.31 | 1.77 |
| 2003/2004 | 0.38 | 0.37 | 0.30 | −0.35 | 1.11 |
| 2005/2006 | 0.82 | 0.38 | 0.03 | 0.07 | 1.58 |
| 2007/2008 | 1.20 | 0.37 | 0.001 | 0.46 | 1.93 |
| 2009/2010 | 2.22 | 0.37 | <0.001 | 1.50 | 2.95 |
| 2011/2012 | 2.42 | 0.40 | <0.001 | 1.63 | 3.21 |
| 2013/2014 | 1.52 | 0.38 | <0.001 | 0.78 | 2.26 |
| 2015/2016 | 1.13 | 0.40 | 0.01 | 0.35 | 1.92 |
| 2017/2018 | −0.13 | 0.42 | 0.76 | −0.96 | 0.70 |
| Sex (reference: male) | |||||
| Female | 1.53 | 0.17 | <0.001 | 1.19 | 1.87 |
| Age group in years (reference: 18–39) | |||||
| 40–59 | 3.08 | 0.21 | <0.001 | 2.67 | 3.49 |
| 60 or above | 6.66 | 0.21 | <0.001 | 6.24 | 7.08 |
| Race/ethnicity (reference: non-Hispanic White) | |||||
| Hispanic | 2.26 | 0.22 | <0.001 | 1.82 | 2.70 |
| Non-Hispanic Black | −1.12 | 0.20 | <0.001 | −1.50 | −0.73 |
| Othersd | 3.17 | 0.33 | <0.001 | 2.53 | 3.82 |
| Educational level (reference: less than high school graduate) | |||||
| High school graduate/GEDe | 0.31 | 0.24 | 0.20 | −0.16 | 0.78 |
| Some college or more | 4.76 | 0.21 | <0.001 | 4.35 | 5.18 |
| Constant | 42.61 | 0.35 | <0.001 | 41.92 | 43.30 |
Adjusted for year, sex, age group in years, race/ethnicity, educational level.
OLS =Ordinary Least Squares
HEI = Healthy Eating Index.
Other race includes non-Hispanic Asian persons and non-Hispanic persons reported races other than Black, Asian, or White.
GED = General Equivalency Diploma
Discussion
Previous NHANES studies reported that overall diet quality among US adults improved over time, which we confirmed over the same periods.15–17 Instead of modeling a linear time trend, as in Wilson et al.15, we focus on cyclical changes related to macroeconomic conditions. Tracking the time path of diet quality over 20 years that includes one of the strongest economic cycle shows that improving macroeconomic conditions are associated with deteriorating diet quality. Diet quality using the HEI-2015 peaked in 2011/2012, when unemployment rates were at high levels, and declined afterwards. The deterioration in diet quality continued as the macroeconomic conditions improved and unemployment rates fell. By 2017/2018, the HEI-2015 scores have deteriorated to the levels in 1999/2000. The association of poorer diet quality with better economic conditions may seem counter-intuitive, but is consistent with economic research on health behaviors and outcomes over the economic cycle.5–9,13
Income/poverty itself is a result of macroeconomic conditions,30 so our main analysis does not control for family income. Instead, only factors that are not changed in the economic cycle, such as sex, age, race/ethnicity, and educational level are controlled. Including income may control away the effect of macroeconomic cycles, but the result from sensitivity analysis shows little difference between adding or not adding the ratio of family income to poverty to the regression model, implying that income changes alone may not be responsible for the change in diet quality.
One plausible explanation is that food prepared at home becomes relatively more attractive and economical during worse economic times. Research from the US Department of Agriculture has shown that working-age adults reported a decline in the share of energy from food-away-from-home during deteriorating economic conditions31 and that the nutritional quality of food-away-from-home was lower compared to food prepared at home.32 Other work reported that food away from home provided fewer servings of whole grains, dairy and vegetables, and increased the percent of calories from added sugar and saturated and solid fat.33 The quantified impact of food away from home on diet quality is equal to lowering total HEI-2005 scores by two points.34 More frequent cooking at home is associated with better diet quality among both lower- and higher-income adults.35 Thus, economizing may result in giving up convenience, but does not necessarily imply deteriorating diet quality.
We find the same qualitative result as Wilson et al.15 up to 2011/2012 when their data ended, namely that diet quality consistently improved until 2011/2012. The key distinction of this study and Wilson et al. is in the dynamics – we focus on cyclical behavior in diet and the data show as strong a decline in diet quality in recent years as they show an improvement in early NHANES waves. However, our absolute scores and the increase in magnitude is lower than what Wilson et al. reported. The two main reasons are that we adjust for population characteristics and that we use the simple HEI method rather than the population ratio method. First, an aging and more educated population increases measured diet quality on its own.17,27 While Wilson et al.’s results include this demographic effect, our approach removes this population trend, as the adjusted predicted scores represent the average population characteristics over the study period. Second, different methods to calculate HEI scores result in different means. The simple scoring algorithm is most appropriate for our purposes because we want to use individual scores in the regression models and only a single 24-hour recall was available in early NHANES waves, but it does not capture usual intake and is more vulnerable to measurement error.25 Other potential reasons for numerical differences are the inclusion of children in Wilson et al. compared with our focus on adults, and the shift from HEI-2010 in Wilson et al. to HEI-2015 in this study. Compared to HEI-2010, HEI-2015 replaced the empty calories category with two separate components (saturated fats and added sugars), and included legumes in the scoring of 4 components (total vegetables, greens and beans, total protein foods, and seafood and plant protein) instead of just two.22 Such changes can have limited impact on HEI scores.
This study is a descriptive research of population statistics over time, which are suggestive but provide no evidence of causality. However, this study is the first to indicate associations between the total HEI-2015 scores and economic cycles, and thus shedding light to the need for future research into possible mechanisms. The changes in the total HEI-2015 scores over time are statistically significant, and the observed magnitude could have an impact on population health, as past research concluded that each additional increase in the standard deviation of HEI-2015 reduced the risk of cardiovascular disease by 3–7%.36 Dietary data from NHANES are subject to the limitations of 24-hour recalls, including measurement error from respondents’ short-term memory and underreporting of energy intake and some macronutrients (e.g., fat and sugar).37–41 Moreover, the reporting bias is related to weight status and social approval.42,43 It is unknown how varying degrees of under- and over-reporting can influence the differences we observed in diet quality over the years.
Conclusions
This paper highlights the importance of economic cycles to diet quality. Population diet quality in the US improved substantially during the Great Recession but deteriorated when the macroeconomic conditions recovered. A possible mechanism is substitution of food prepared at home with nutritionally less desirable food away from home during economic recovery. If that were true, the COVID-19 pandemic may result in even larger changes in diet quality.
Research Snapshot.
Research Question:
How does population diet quality change during economic downturns or economic recoveries?
Key Findings:
Diet quality among US adults improved during the Great Recession but deteriorated as the economy recovered.
Financial Support:
This paper was supported through NIH grant R01HD087257.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of Interest: The authors report no conflict of interest.
References
- 1.U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2020 – 2025 Dietary Guidelines for Americans. December 2020.
- 2.U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015 – 2020 Dietary Guidelines for Americans. December 2015.
- 3.The National Bureau of Economic Research. US Business Cycle Expansions and Contractions. https://www.nber.org/research/data/us-business-cycle-expansions-and-contractions. Updated June 8, 2020. Accessed May 1, 2021.
- 4.Bureau of Labor Statistics. Labor Force Statistics from the Current Population Survey, 1948–2020,. Data series LNS14000000 Web site. https://data.bls.gov/cgi-bin/surveymost?bls. Published 2020. Accessed December 28, 2020 (2:27:27 PM), 2020.
- 5.Ruhm CJ. Health Effects of Economic Crises. Health Econ. 2016;25 Suppl 2:6–24. [DOI] [PubMed] [Google Scholar]
- 6.Moreno-Lostao A, Barrio G, Sordo L, Cea-Soriano L, Martinez D, Regidor E. Mortality in working-age population during the Great Recession and austerity in Spain. PLoS One. 2019;14(6):e0218410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Toffolutti V, Suhrcke M. Assessing the short term health impact of the Great Recession in the European Union: a cross-country panel analysis. Prev Med. 2014;64:54–62. [DOI] [PubMed] [Google Scholar]
- 8.Miller DL, Page ME, Stevens AH, Filipski M. Why Are Recessions Good for Your Health? Am Econ Rev. 2009;99(2):122–127. [Google Scholar]
- 9.Tapia Granados JA. Increasing mortality during the expansions of the US economy, 1900–1996. Int J Epidemiol. 2005;34(6):1194–1202. [DOI] [PubMed] [Google Scholar]
- 10.Heutel G, Ruhm CJ. Air Pollution and Procyclical Mortality. J Assoc Environ Reso. 2016;3(3):667–706. [Google Scholar]
- 11.Stevens AH, Miller DL, Page ME, Filipski M. The Best of Times, the Worst of Times: Understanding Pro-cyclical Mortality. Am Econ J-Econ Polic. 2015;7(4):279–311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Frasquilho D, Matos MG, Salonna F, et al. Mental health outcomes in times of economic recession: a systematic literature review. BMC Public Health. 2016;16:115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ruhm CJ. Healthy living in hard times. J Health Econ. 2005;24(2):341–363. [DOI] [PubMed] [Google Scholar]
- 14.Seeman T, Thomas D, Merkin SS, Moore K, Watson K, Karlamangla A. The Great Recession worsened blood pressure and blood glucose levels in American adults. Proc Natl Acad Sci U S A. 2018;115(13):3296–3301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wilson MM, Reedy J, Krebs-Smith SM. American Diet Quality: Where It Is, Where It Is Heading, and What It Could Be. Journal of the Academy of Nutrition and Dietetics. 2016;116(2):302–+. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Shan Z, Rehm CD, Rogers G, et al. Trends in Dietary Carbohydrate, Protein, and Fat Intake and Diet Quality Among US Adults, 1999–2016. JAMA. 2019;322(12):1178–1187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Liu JX, Micha R, Li Y, Mozaffarian D. Trends in Food Sources and Diet Quality Among US Children and Adults, 2003–2018. Jama Network Open. 2021;4(4). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ahluwalia N, Dwyer J, Terry A, Moshfegh A, Johnson C. Update on NHANES Dietary Data: Focus on Collection, Release, Analytical Considerations, and Uses to Inform Public Policy. Adv Nutr. 2016;7(1):121–134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.National Center for Health Statistics. NHANES Survey Methods and Analytic Guidelines. https://wwwn.cdc.gov/nchs/nhanes/AnalyticGuidelines.aspx. Accessed August 14, 2021.
- 20.National Cancer Institute. The Healthy Eating Index – Simple HEI Scoring Algorithm Method. https://epi.grants.cancer.gov/hei/hei-scoring-method.html. Updated August 29, 2017. Accessed Feb 15, 2021.
- 21.Reedy J, Lerman JL, Krebs-Smith SM, et al. Evaluation of the Healthy Eating Index-2015. J Acad Nutr Diet. 2018;118(9):1622–1633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Krebs-Smith SM, Pannucci TE, Subar AF, et al. Update of the Healthy Eating Index: HEI-2015. J Acad Nutr Diet. 2018;118(9):1591–1602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kirkpatrick SI, Reedy J, Krebs-Smith SM, et al. Applications of the Healthy Eating Index for Surveillance, Epidemiology, and Intervention Research: Considerations and Caveats. J Acad Nutr Diet. 2018;118(9):1603–1621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.National Cancer Institute. Developing the Healthy Eating Index. https://epi.grants.cancer.gov/hei/developing.html. Accessed May 9, 2021.
- 25.National Cancer Institute. Overview of the Methods & Calculations. https://epi.grants.cancer.gov/hei/hei-methods-and-calculations.html. Accessed May 9, 2021.
- 26.SAS Version 9.4 [computer program]. Cary, NC: SAS Institute Inc; 2018. [Google Scholar]
- 27.Hiza HA, Casavale KO, Guenther PM, Davis CA. Diet quality of Americans differs by age, sex, race/ethnicity, income, and education level. J Acad Nutr Diet. 2013;113(2):297–306. [DOI] [PubMed] [Google Scholar]
- 28.Zipf GCM, Porter KS. National Health and Nutrition Examination Survey: Plan and operations, 1999–2010. Vital Health Stat 1(56). 2013. [PubMed] [Google Scholar]
- 29.Stata Statistical Software: Release 16 [computer program]. College Station, TX: StataCorp LLC; 2019. [Google Scholar]
- 30.Smeeding T. Income Wealth and Debt and the Great Recession Stanford, CA: Stanford Center on Poverty and Inequality;2012. [Google Scholar]
- 31.Todd JE. Changes in consumption of food away from home and intakes of energy and other nutrients among US working-age adults, 2005–2014. Public health nutrition. 2017;20(18):3238–3246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lin B, Guthrie J. Nutritional Quality of Food Prepared at Home and Away From Home, 1977–2008. In: Service ER, ed: U.S. Department of Agriculture; 2012. [Google Scholar]
- 33.McGuire S Todd JE, Mancino L, Lin B-H. The Impact of Food Away from Home on Adult Diet Quality. ERR-90, US Department of Agriculture, Econ. Res. Serv., February 2010. Advances in Nutrition. 2011;2(5):442–443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Mancino L, Todd J, Lin BH. Separating what we eat from where: Measuring the effect of food away from home on diet quality. Food Policy. 2009;34(6):557–562. [Google Scholar]
- 35.Wolfson JA, Leung CW, Richardson CR. More frequent cooking at home is associated with higher Healthy Eating Index-2015 score. Public Health Nutr. 2020;23(13):2384–2394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hu EA, Steffen LM, Coresh J, Appel LJ, Rebholz CM. Adherence to the Healthy Eating Index-2015 and Other Dietary Patterns May Reduce Risk of Cardiovascular Disease, Cardiovascular Mortality, and All-Cause Mortality. J Nutr. 2020;150(2):312–321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ferrari P, Slimani N, Ciampi A, et al. Evaluation of under- and overreporting of energy intake in the 24-hour diet recalls in the European Prospective Investigation into Cancer and Nutrition (EPIC). Public Health Nutr. 2002;5(6b):1329–1345. [DOI] [PubMed] [Google Scholar]
- 38.Subar AF, Kipnis V, Troiano RP, et al. Using intake biomarkers to evaluate the extent of dietary misreporting in a large sample of adults: The OPEN Study. Am J Epidemiol. 2003;158(1):1–13. [DOI] [PubMed] [Google Scholar]
- 39.Briefel RR, Sempos CT, McDowell MA, Chien SCY, Alaimo K. Dietary methods research in the third national health and nutrition examination survey: Underreporting of energy intake. Am J Clin Nutr. 1997;65(4):1203–1209. [DOI] [PubMed] [Google Scholar]
- 40.Archer E, Hand GA, Blair SN. Validity of U.S. nutritional surveillance:National Health and Nutrition Examination Survey caloric energy intake data, 1971–2010. PLoS One. 2013;8(10):e76632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Grandjean AC. Dietary intake data collection: challenges and limitations. Nutr Rev. 2012;70:S101–S104. [DOI] [PubMed] [Google Scholar]
- 42.Moshfegh AJ, Rhodes DG, Baer DJ, et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am J Clin Nutr. 2008;88(2):324–332. [DOI] [PubMed] [Google Scholar]
- 43.Miller TM, Abdel-Maksoud MF, Crane LA, Marcus AC, Byers TE. Effects of social approval bias on self-reported fruit and vegetable consumption: a randomized controlled trial. Nutr J. 2008;7. [DOI] [PMC free article] [PubMed] [Google Scholar]