

Abstract
Rather than just another “review,” this is intended to be an “overview” of the entire subject of the medial sural artery perforator (MSAP) flap as has been presented in the reconstructive literature from its inception in 2001 until the present, with any exceptions not purposefully overlooked. Unfortunately, the pertinent anatomy of the MSAP flap is always anomalous like most other perforator flaps, and perhaps even more variable. No schematic exists to facilitate the identification of a dominant musculocutaneous perforator about which to design the flap, so some adjunctive technology may be highly valuable for this task. However, if a relatively thin free flap is desirable for a small or moderate sized defect that requires a long pedicle with larger caliber vessels, the MSAP flap deserves consideration. Indeed, for many, this has replaced the radial forearm flap such as for partial tongue reconstruction. Most consider the donor site deformity, even if only a conspicuous scar on the calf, to be a contraindication. Yet certainly if used as a local flap for the knee, popliteal fossa, or proximal leg, or as a free flap for the ipsilateral lower extremity where a significant recipient site deformity already exists, can anyone really object that this is not a legitimate indication? As with any perforator flap, advantages and disadvantages exist, which must be carefully perused before a decision to use the MSAP flap is made. Perhaps not a “workhorse” flap for general use throughout the body, the MSAP flap in general may often be a valuable alternative.
Keywords: medial sural artery perforator flap, MSAP flap, calf flap, lower extremity
The History
This odyssey began at the 5th International Course on Perforator Flaps, in Gent, Belgium, in 2001. There in the free paper session, Hallock presented an anatomical study of above-knee amputation specimens that traced the origin of the dominant musculocutaneous perforators of the heads of the gastrocnemius muscle that showed potential for design of “gastrocnemius perforator-based” flaps. 1 This was immediately followed by a similar anatomical study by Cavadas et al, but in addition summarized the first clinical series of what with prescience was termed the “medial sural artery perforator flap” (MSAP) flap. 2 One must remember that the “Gent Consensus” for proper perforator flap nomenclature was still being debated at that very meeting. 3 In any event, both these presenters in November of the same year published their presentations in respectable plastic surgery journals. 1 2 4 Subsequently, most manuscripts scrutinizing in more detail the “medial sural artery perforator flap” or more concisely the “MSAP flap” inevitably and for the most part correctly have always referred to Cavadas as the MSAP flap originator.
Alas, as is often the case, a more careful perusal of the literature will reveal that the MSAP “innovator” has had many legitimate predecessors. Early on, many MSAP authors recognized that Taylor and Daniel after their first successful composite tissue transfer 5 had then explored the anatomy of several other potential free flap donor sites that would be suitable if their vascular supply could be predictable. 6 With Taylor's personal persistence (1975), one “possible island flap supplied by musculocutaneous branches of the medial and lateral sural vessels” was called the “popliteal flap.” 6 By serendipity, Montegut and Allen, after struggling with gastrocnemius musculocutaneous local flaps that sometimes had restricted reach requiring microvascular extension of their vascular pedicle, 7 instead found the “sural artery perforator flap” without the muscle to be a simpler and so a better alternative in clinical cases. 8
Yet a true chronicle of the MSAP flap should at the least begin by recognizing the anatomical observations of the German medical student Manchot (1889) 9 who noted “two sural arteries … the largest branches of the popliteal artery. They emerge … at the level of the knee joint, often from a common stem.” Manchot on occasion in his cadavers discovered the presence of “cutaneous branches from the deep muscle branches of the gastrocnemius muscles, which appeared in various positions.” 10 Easily also forgotten was Mathes and Vasconez's 11 description of a “medial skin-fascial gastrocnemius flap” that was a so-called random cutaneous extension allowing reach to the proximal and middle third of the leg, yet relied on the retention of medial gastrocnemius musculocutaneous perforators. Later, the sural artery flap of Mathes and Nahai 12 was a fasciocutaneous flap that encompassed the cutaneous territory from the popliteal fossa to the midpoint of the leg, and occasionally the vascular basis relied on its minor pedicle, those same gastrocnemius musculocutaneous perforators. Venkataramakrishnan et al 13 used “free style” V-Y advancement flaps based on a calf perforator to close adjacent wounds, but never performed any intramuscular dissection of that perforator. Taylor and Pan 14 once again depicted these MSAPs as germane to their respective calf angiosome. The island posterior calf fasciocutaneous flap of Shaw et al 15 was used as a local pedicled flap for coverage of knee and tibial defects as an alternative to the gastrocnemius muscle, and occasionally required an intramuscular dissection of retained gastrocnemius musculocutaneous perforators for salvage, indeed then being transformed into a “true” perforator flap. 16
Numerous other recent reviews of the MSAP flap due it the justice it deserves, 17 18 19 20 21 22 but comparatively little effort has been spent in the utilization of calf fasciocutaneous flaps based on the lateral sural artery perforators, 23 24 25 26 primarily due to the common absence of those perforators altogether as found in most anatomical studies of this region. 1 2 27 28 Thus, to follow Taylor's admonition that a preferred free flap donor site has a reasonably predictable vascular supply, 6 this should explain why the emphasis presently only on the MSAP flap has caught everyone's attention, and is the rationale for this comprehensive overview also.
The Anatomy
The first efforts to determine the vascular anatomy of the MSAP flap specifically as a “perforator flap” initially by Cavadas et al 2 and Hallock 1 have been repeated by many others in an attempt to find any consistency that would better assure reliability. 27 28 29 30 31 32 33 34 35 Unfortunately, as is usually the outcome with investigations of perforator flaps, the pattern in an individual's contralateral side is rarely identical to that of the ipsilateral, 36 and often even less so when seeking comparisons with others—the MSAP flap is no exception to this rule! 28
Arterial
Most would agree with Manchot 9 that the medial sural artery (MSA) originates from the middle third of the popliteal artery at the level of the femoral condyles, although sometimes from a common stem with the lateral sural artery. 1 37 The MSA descends in the popliteal fossa for a few centimeters, 37 where on occasion is itself the origin of the median sural artery that is eventually found in the furrow between the two heads of the gastrocnemius muscle to accompany the medial sural cutaneous nerve. 9 Then proceeding posteriorly, the MSA enters the undersurface of the medial head of the gastrocnemius muscle at the level of the fibular head, which corresponds to the articulation of the knee joint. Before or after entering this muscle hilum, Manchot long ago knew that, sometimes the MSA will “divide into one or more deep muscular branches.” 9 More recently, Thione et al 31 described two such major branches, but others have rarely discovered the presence of three or more branches. 28 33 37 Dusseldorp et al 28 devised a classification schema for these various branching patterns ( Fig. 1 ).
Fig. 1.
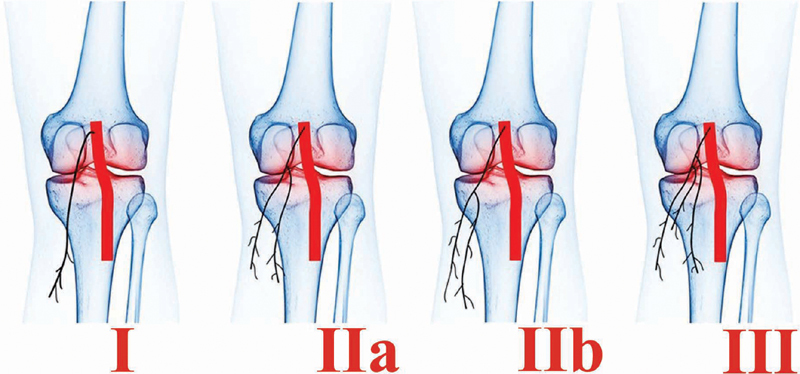
Classification and frequency (%) of branching patterns of the medial sural artery according to Dusseldorp et al. 28 Type I: single branch (31%). Type IIa: dual branches with takeoff superior to tibial plateau (35%). Type IIb: dual branches with takeoff inferior to tibial plateau (24%). Type III: three or more branches, all with takeoff superior to the tibial plateau (10%).
The importance of the MSA branching patterns should not be overlooked, as these ultimately give rise to the musculocutaneous perforators that must be included in the MSAP flap. Thione et al 31 stated that two-thirds of such perforators arose from the lateral branch, but 87% overall were within 1 cm of the midline of the medial gastrocnemius muscle (MGM) itself. When only two branches were present, according to Wong et al, 33 the lateral branch would be the larger with a typically straight and relatively superficial intramuscular course away from the muscle hilum. This opinion is in contradistinction to that of Dusseldorp et al, 28 who found their type IIa ( Fig. 1 ) medial branch to be more superficial (0.5 ± 0.2 cm) than the lateral (1.3 ± 0.4 cm), and in type III, all branches were superficial, whereas in type I or type IIb all were deeper.
To further complicate matters, sometimes MSAPs may not even exist, yet the number of dominant perforators (i.e., subfascial caliber ∼0.5 cm 28 31 ) could range even up to half a dozen! 25 28 29 32 34 In the absence of an MSAP, Dusseldorp et al 28 in 9% and Wang et al 38 in 10% of the time found instead a suitable median sural artery perforator as an alternative, so that although a “true” MSAP perforator flap would only be possible ∼90% of the time, almost always a satisfactory calf perforator flap was still possible. Caution here must be heeded with more distal perforators, as these could arise directly from the posterior tibial artery, be a musculocutaneous perforator of the soleus muscle, or even cross the midline to reach the lateral sural artery. 35
In most of these anatomical studies, a Cartesian coordinate system was set up to plot the location of each perforator on the basis of its distance from the popliteal crease (PC) as the “y” axis and from the midline of the calf as the “x” axis. The vertical distance was highly variable, but in general no perforators were found <6.0 cm from the PC, nor any including a second perforator if present >18.0 cm, 17 albeit with many exceptions. 2 33 The distance from the midline varied from 0.5 to 5 cm, 29 34 whereas the mean muscle width itself was only 6.8 cm. 1 Understandably, these measurements would be highly variable, as they are dependent on the intramuscular branching pattern of the individual. In addition, Pease et al 39 argue that the location of the PC and midline of the calf should not be valid topographic locations, although by default they are so commonly used during physical examination to estimate the perforator location. Instead, they point out that the head of the fibula would be a constant point rather than a crease that would vary according to body habitus, and the medial head is typically larger than the lateral head, so the former always would extend not to but more lateral to the midline.
The caliber of the MSA ranges from 1 to 4 mm at its origin. 29 40 After entering the muscle, this dimension logically diminishes, as Fu et al 37 found that its dimension decreased 25% after traversing only 2 cm. The length of the pedicle as measured from the popliteal artery to where the perforator entered the flap could be as short as 5 cm 32 or as long as 21 cm. 34 Again, this would depend on the number of perforators retained, their location entering any flap, and the choice of intramuscular branch, if multiple.
Of course, preservation of muscle function is the sine qua non of perforator flaps, so viability of the MGM must be assured after any devascularization caused by harvest of the MSA source vessel. Tsetsonis et al 41 have shown in cadaver studies that communicating bundles or arterioles exist crossing the raphe from the lateral head that would serve as a collateral. Secondary venous outflow could be via direct anastomotic veins in a similar manner, or via the median sural vein accompanying the medial sural cutaneous nerve. 42 In addition, overall circulation could be maintained by reverse flow via retained musculocutaneous perforators or branches entering from the underlying soleus muscle. 43
Venous
Any islanded perforator flap must by definition have disconnected the superficial venous system so that outflow will depend on the perforator venae comitantes that will then drain into the intramuscular venae comitantes of the deep system, ultimately for the MSAP flap reaching the popliteal fossa along with the MSA. Typically, at least one of these paired veins will have a caliber larger than the corresponding artery, even up to 5 mm, and it is not unusual that the other can be quite diminutive or almost nonexistent. However, whereas the perforasome of an artery readily interconnects with its neighbor, 44 the same may not be true with the venous perforasome. 45 Taylor et al 45 suggest that the line of necrosis on the venous side can be due to intrinsic or unpredictable anatomical obstructions such as physiologic strictures or even the subordinate role of the deep system, so that outflow does not proceed as expected from the superficial to the deep system or from one venous perforasome to its neighbor, as has already been shown to occur with the MSAP flap as a model. 46 Perforators near the midline may have the course of their venous branches diverted toward the median sural vein and/or lesser saphenous vein, which for the sake of security should be included with a flap harvested nearby to ensure drainage of the superficial system. 47 48 49 50 Branches of the greater saphenous vein are also always present within the more anteromedial calf, and can always be kept for the same reason. 38 51
Innervation
No significant clinical series has yet described a sensate MSAP flap. Although Kao et al 40 suggested that the sural nerve can provide this capability, details of how this would be possible were not given. In their cadaver dissections seeking sensate free flap donor sites, Taylor and Daniel in the diagram of their so-called “popliteal flap” pictured the posterior cutaneous nerve of the thigh terminating in the pertinent calf skin territory. 6 However, the nerve identified below that in the figure of the actual cadaver dissection was identified as the lateral cutaneous nerve of the calf, which they admitted occasionally replaced the former nerve. 6 More medially, sometimes the saphenous nerve can also contribute to the innervation of this region. 6
The Technique
Every surgeon will have their preferential approach to the actual harvest of the MSAP flap, but many pragmatic maneuvers are found to be common, which is the basis for this summary of reasonable steps to follow.
Step 1: Perforator Identification
Since the viability of any flap depends on capturing the requisite source of circulation, for a perforator flap it is imperative to preoperatively find a reasonable perforator that will serve that purpose in the optimal donor territory. Only then can the desired flap boundaries be designed with some assurance of its survival. Schematics to guide surveillance of the most common location of perforators in the “workhorse” flaps like the anterolateral thigh (ALT) flap are well known, 52 but are not yet universally accepted for the MSAP flap ( Fig. 2 ). Most frequently used has been the suggestion of Kim et al 32 to draw a line from the midpoint of the PC to the prominence of the medial malleolus. A perforator may be found within a distal hemi-circle with a radius of 2 cm centered on the former line 8 cm below the PC 32 ; and a second perforator, if present, may be in a circle 6 cm in diameter 15 cm below the PC. 52 Song et al 53 simply expanded their search at a point “A” located at the midpoint of the line of Kim et al. 32 Thione et al 31 even more simply dropped a vertical line along the midline of the MGM, as in their cadaver dissections 87% of all desirable perforators were within ± 1.0 cm of that line. Choi et al 54 determined that most sizable perforators were near the midline of the lower leg inside a triangle outlined by the extent of the MGM between two lines originating from the midpoint of the PC, with one extending to the medial calcaneus and the other to the Achilles tendon. To take into account variability in height, Wang et al 38 dropped a second line from the medial epicondyle of the femur to the prominence of the lateral malleolus that intersected the line of Kim et al, 32 where a circle with a radius of 4.0 cm centered at that point would encompass the necessary perforators. Remember that the mean width of the MGM may be 6.8 cm, 1 and as Pease et al 39 have reflected, the location of the PC depends on the individual's body contour and the larger MGM head most often extends lateral to the midline. Also, one cannot forget that the intramuscular branching pattern leading to these perforators can be highly variable, 28 so a single schematic intuitively for these reasons from the outset would not seem logically to be a universal possibility. To overcome all this inconsistency, Kao et al 30 55 rely on four lines marked with the patient standing:(1) the PC, (2) from the midpoint of the PC to the Achilles tendon, (3) along the distal border of the MGM, and (4) from the medial tibial condyle to the prominence of the medial malleolus. Note these intersect to essentially outline the entirety of the MGM ( Fig. 2 ), through which, of course, any available musculocutaneous perforator must indeed pass.
Fig. 2.
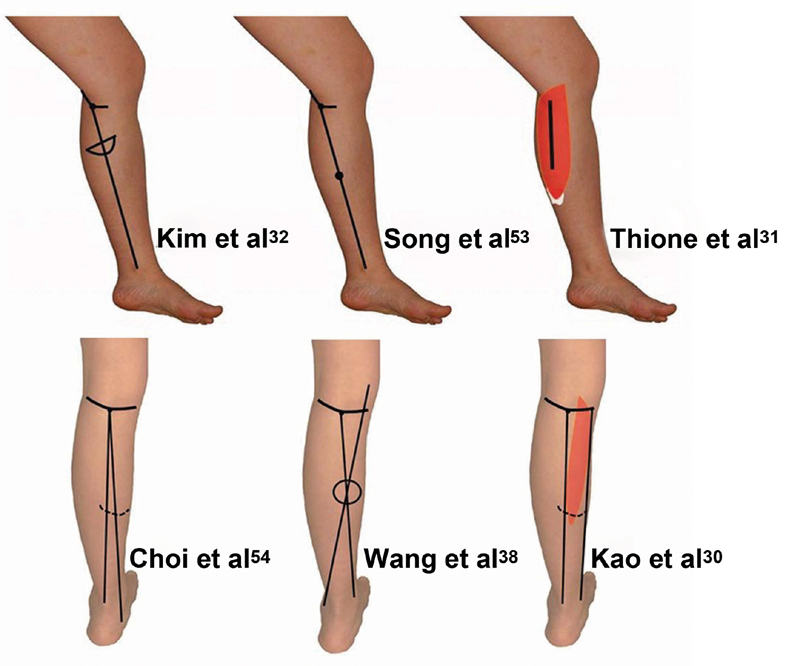
Existing schematics intended to facilitate the preoperative identification of the location of a medial sural artery perforator (see text for details): Kim et al 32 : within hemi-circle 8 cm below the popliteal crease (PC) on line drawn from midpoint of PC to prominence of the medial malleolus (MM). Song et al 53 : search begins at midpoint of line of Kim; Thione et al 31 : found ± 1.0 cm from the vertical midline of the medial gastrocnemius muscle (MGM); Choi et al 54 : inside the triangle formed by the extent of the MGM between lines from the midpoint of the PC to the Achilles tendon and the medial calcaneus; Wang et al 38 : within the circle centered at the intersection of line from the medial epicondyle of the femur to the prominence of the lateral malleolus with the line of Kim; Kao et al 30 : region encompassed superiorly by the PC, line from the midpoint of the PC to the Achilles tendon, the distal border of the MGM, and the fourth line from the medial tibial condyle to the prominence of the MM.
The take-home message from the aforementioned schematic choices should be that some technological support would inevitably be more helpful. The ubiquitous audible Doppler can be tediously dragged over the entire MGM, 17 55 56 57 58 but care must be taken as the audio heard from the usually very superficial course of the intramuscular branches may be enhanced, thereby obscuring differentiation from the perforators themselves. 59 Computed tomography (CT) angiography 32 60 61 62 63 and color duplex ultrasound 27 32 64 may be beneficial means to show the course and origin of potential perforators—if available. A cheaper alternative may be just smartphone thermography to find “hot spots” after a “cold challenge” ( Fig. 3 ), allowing their follow-up with an audible Doppler to be thereby used in a more efficient mode. 65
Fig. 3.
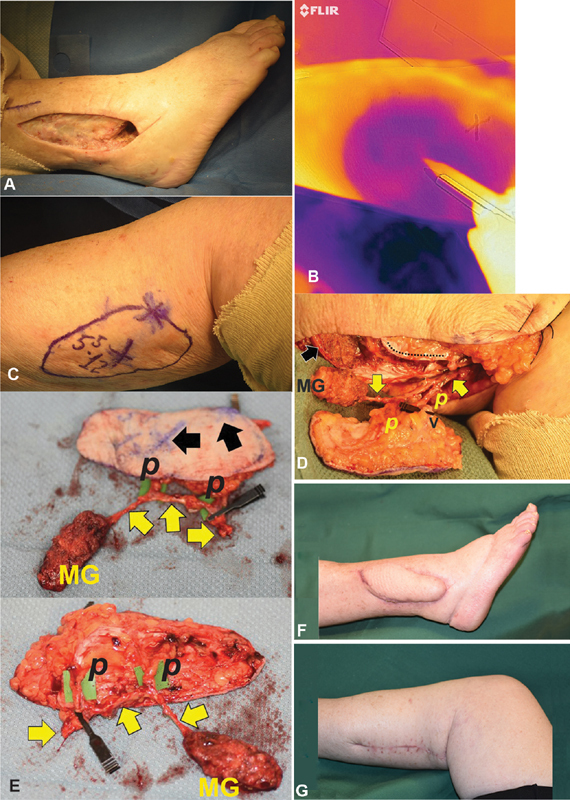
( A ) Failed right ankle pilon fracture reduction, with open lateral malleolus wound extending into ankle joint. ( B ) Using a thermography camera, the second “hotspot” seen marked on the medial calf as was the spot “X” above. ( C ) Medial sural artery perforator (MSAP) flap designed on the medial calf to potentially include both perforator sites “X” as determined by thermography. ( D ) Chimeric MSAP flap in situ, with perforators ( P ) found exactly at predicted points “X,” vascular clamp on the greater saphenous vein branch (V) available for supercharging, course of the medial sural artery superficial intramuscular source branch (proximal yellow arrow), continuation of this branch ( distal yellow arrow ) past the second perforator origin to independently supply a small portion of the medial gastrocnemius muscle (MG) that will be inset into the cavity entering the ankle joint, harvest site of the MG ( black arrow ), rent through the MG for pedicle harvest (inferior to dotted line ). ( E ) Free chimeric MSAP flap, predicted perforator sites “X” ( black arrows ) corresponded to their actual location ( P [yellow arrows follow course of medial sural pedicle]). ( F ) Right lateral ankle status 5 weeks posttransfer prior to fusion. ( G ) Typical final calf donor site scar.
Step 2: Flap Design
The dimensions of any chosen flap must be satisfactory to accomplish the desired coverage. Injection studies by Walton and Bunkis 66 of the vascular plexus of their posterior calf fasciocutaneous flap indicated that “perfusion beyond the medial and lateral mid-axial line of the leg is unpredictable,” and vertically this extended from about the PC to the middle or lower one-third of the leg. This is consistent with the extensive microanastomoses interconnecting the angiosomes surrounding that of the MSA, 38 allowing an MSAP flap 15 × 20 cm in size reported by Kim et al 67 and, the longest of all, 10 × 25 cm by Teven et al. 68 A flap wider than 5 cm 2 40 or at most 8 cm 32 might not allow primary donor site closure. A “pinch test” may be a more accurate means to determine an acceptable flap width, 69 if primary donor site closure is essential.
Pedicle length will mostly be determined by the location of the chosen perforator. Eccentric placement of that perforator at the proximal end of the flap design will maximize the potential length. Eccentric placement at the distal end of the flap will allow proximal tissues to be rotated in a propeller fashion to also obtain maximum pedicle length, albeit requiring some twist about the perforator. 69 Theoretically, centralizing the perforator will best assure total flap perfusion especially for a narrow flap, but for a very long flap, retention of a second perforator in the more distal flap design would be highly desirable to ensure adequate circulation. 64 In addition, the axis of the flap should have a longitudinal and not curved or oblique orientation, so that “choke vessels” or true anastomoses will best capture adjacent perforator angiosomes sufficiently. 36 44 70
Step 3: Perforator Confirmation
With the patient typically supine after induction of anesthesia, the thigh is abducted and externally rotated at the hip, and the knee is flexed. A bloodless field simplifies perforator dissection, so use of a tourniquet, but without limb exsanguination so as to maintain venous fill, is preferable. Two small subfascial incisions at the anterior border of the MGM will allow passage of retractors and a 4-mm endoscope with a 30-degree angle for actual visualization of the perforator. 48 59 62 71 As an alternative, a small subfascial exploratory incision along the proposed anterior border of the flap with upward traction on the flap might be sufficient to lead to accurate citing of the perforator where it enters the deep fascia. 55 Once confirmed, the flap design should be revised as necessary. Completion of the anterior flap border incision can then safely be done, usually retaining proximally a few centimeters of a subcutaneous vein for later potential supercharging. Because of the relatively notoriously small perforators usually encountered in this donor site, a suprafascial dissection is rarely chosen. 64 A subfascial dissection allows a rapid posterior retraction of the flap above a bloodless subfascial plane, except where the perforator is located. Be careful of the corkscrew path of the perforator, as it may exit the MGM at a point even a few centimeters away from where it perforates the deep fascia. Towels placed on the operating room table under the flap as it falls backward will serve as a cushion that will prevent excessive tension on the perforator during the next steps. 72
Step 4: Pedicle Dissection
Muscle fibers should first be gently spread apart above and below the chosen perforator. Often, its origin from a superficial intramuscular branch will then rapidly be seen. De-roofing of that branch proximally should proceed by spreading apart the usually longitudinally oriented muscle fibers. This stops once the desired pedicle length or vessel caliber has been reached, which can extend through the hilum as far back to the vascular origin from the popliteal vessels. Circumferential freeing of the pedicle from other muscular branches is next done, being careful using available means for hemostasis. Any motor nerve encountered should be meticulously separated away from the MSA. Once all has been completed, the muscle branch distal to the perforator origin can be ligated if the usual orthograde flow to the perforator is to be maintained.
Step 5: Flap Harvest
Only after completion of the skeletonization of the vascular pedicle should the posterior border of the flap be incised also through the deep fascia, being careful to ensure that the perforator has been retained. If that border is near or crosses the midline, inclusion of the lesser saphenous vein or its branches may be advisable also for potential supercharging. 48 From distal to proximal, the deep fascia of the flap is teased away from the intrinsic MGM fascia to make this a true island flap. At this point, the tourniquet may be deflated, and vascular perfusion to the flap assessed and managed, as well as control of any hemorrhage. The flap is then ready for transfer as per the original overall surgical plans.
Technical Variations
Patient Position
The location of the recipient site will determine what should be the most efficient intraoperative position that will still allow unimpeded MSAP flap harvest. Not only can a supine or lateral decubitus position be acceptable, but also the MSAP flap is actually an “ideal” donor site when the prone position is used, 67 because as such few other perforator flaps with a long vascular pedicle are available. 50
Propeller
Any MSAP can serve as the hub for a propeller flap. If the hub is located proximally, following rotation about that hub, distal calf tissues can be transferred to a more proximal defect. Similarly, if the hub is located distally, more proximal calf tissues can be transferred even more distally. Using the latter design, if the MSAP intramuscular pedicle itself is dissected somewhat more proximally, Tee et al 69 have shown that this as a “pedicled propeller flap” will reach the anterior middle third of the leg. If the same pedicle were divided and then based on a distal pedicle with retrograde flow, reach to the distal leg is possible, but caution is advised as Tee et al 69 had complications in every case so reported. If a second MSAP perforator exists, that can similarly be used separately as a retrograde perfused propeller flap to facilitate direct closure of the donor site. 63
Perforator Plus
Any flap maintaining a dual blood supply that includes a dissected perforator would be a “perforator plus” flap. 73 A peninsular flap with an intact base (either proximal or distal based) where an encountered MSAP is dissected as far as necessary so as not to impede rotation of the flap may provide some security in assuring superior circulation to the entire flap. An MSAP “perforator plus” flap could also be completely islanded on its medial sural vascular pedicle, with a second source of circulation included such as the retention of the lesser saphenous vein and/or the medial sural cutaneous nerve with the accompanying median sural vessels, as Kim et al 67 deemed necessary when the donor site consisted of burned skin to better ensure both inflow and outflow.
Adipofascial
If primary closure of the MSAP flap donor site is essential, or bulk need be minimized, the subcutaneous layer along with the usually retained deep fascia only need be transferred without the overlying integument as an adipofascial flap. 74 75
Chimeric
A chimeric flap is a combination of flaps that each have an independent vascular supply, and are independent of any physical interconnection except where linked to a common source vessel. 76 77 If two or more dominant MSAPs are present, two narrow MSAP flaps can be harvested only with a common medial sural vascular pedicle, which Sano et al 78 have shown allows greater surface area coverage at the recipient site while obeying the “kiss” principle of Zhang et al 79 with the specific advantage of allowing primary donor site closure that would not have been possible if a single wide flap had been used. In addition, if one flap were buried, monitoring would be possible by externalizing the second. 71
Of course, since the MSAP flap is a “true” perforator flap, 16 the requisite musculocutaneous perforator is intimately attached to MGM branches so that a portion if not all of that muscle could be combined as a chimeric flap. If the intramuscular branching pattern were type II or III ( Fig. 1 ), Lee et al 62 have shown that the MSAP flap could arise from the lateral branch while the medial branch independently supplies the muscle, or vice versa. Another option is to keep the continuation of the intramuscular branch distal to the perforator origin (or any other reasonably large muscle branch) to serve the muscle portion separately ( Fig. 3 ). Whether utilized as a pedicled local flap 24 62 75 80 or free flap, 53 62 78 81 the more malleable muscle component can readily fill deep spaces or provide additional bulk, while the perforator flap simultaneously provides cutaneous or mucosal coverage.
An even simpler chimeric flap alternative would be the traditional transfer of a medial gastrocnemius musculocutaneous flap, where the skin paddle were isolated on its perforator enough only to allow its rotation in any direction so as to better fit a given skin defect, as Innocenti et al 82 have done for knee defects. Some would call this variation a “chimeric propeller flap.” 83
Composite Tissues
The subfascial elevation of the MSAP flap readily allows access to other tissue donor sites. Vascularized muscle, as just described, could be a part of a chimeric flap. The medial sural cutaneous nerve that runs in the furrow between the heads of the gastrocnemius muscle could even be a vascularized nerve transfer if a mesentery of the muscle is kept wrapped about it as Kashiwa et al 26 have shown, corroborating Al Qaatan 84 85 who found that this maneuver also maintains circulation to extend the more proximal skin territory of a distal-based sural flap. This region is also a source of nearby nonvascularized grafts such as the saphenous nerve, plantaris tendon, and the lesser saphenous vein. 17 20 21
The Versatility
As with any flap, enthusiastic use of the MSAP flap anywhere in the body will be eventually tempered by recognition of its true advantages ( Table 1 ) and disadvantages ( Table 2 ). Appropriate selection must consider all inherent qualities and also known risks. For example, in contrast to the rest of the body, in general the MSAP flap is markedly thinner ( Fig. 4 ), ranging from 4 to 8 mm in Asian series. 17 30 Many have therefore chosen this over the radial forearm flap so as to preserve the radial artery and minimize risk of hand function morbidity while allowing immediate donor site rehabilitation. 40 48 53 56 86 Doğan et al 87 compared this attribute with the ALT flap, which on average was much thicker, and concluded that in general the actual MSAP flap thickness is directly proportional to gender and body mass index (BMI), the latter perhaps explaining why in the Western cultures this may not be so thin as would be desirable ( Fig. 5 ). Color and texture should also be concerns, as the match is poor when used to resurface exposed defects ( Fig. 6 ).
Table 1. Attributes of the medial sural artery perforator flap.
| 1. Function preservation |
| 2. Donor territory rarely unavailable |
| 3. Accessible with the patient supine, ipsilateral decubitus, or prone |
| 4. Lengthy vascular pedicle |
| 5. Pedicle caliber does not require super-microsurgery |
| 6. Usually facile pedicle harvest, with superficial intramuscular location |
| 7. Spinal anesthesia sometimes possible |
| 8. Concurrent approach by multiple teams for head and neck, upper extremity, or trunk reconstruction |
| 9. Relatively thin, regardless of body mass index |
| 10. Contour often permits as substitute for radial forearm flap |
| 11. Local flap alternative for the gastrocnemius muscle |
| 12. Legitimate free flap option for oral cavity and ipsilateral lower extremity |
| 13. Numerous chimeric flap options |
| 14. Synchronous harvest of multiple composite tissues, e.g., muscle, tendon, nerve, vein |
Table 2. Detriments of the medial sural artery perforator flap.
| 1. Nonaesthetic appearance of donor site skin graft or scar |
| 2. Medial sural artery perforator may be absent |
| 3. Nonexistence of schematic for reliable preoperative perforator site identification |
| 4. Even dominant perforator caliber relatively small |
| 5. Corkscrew subfascial perforator path could skew flap design |
| 6. Potential for coverage of only small to moderate surface area |
Fig. 4.
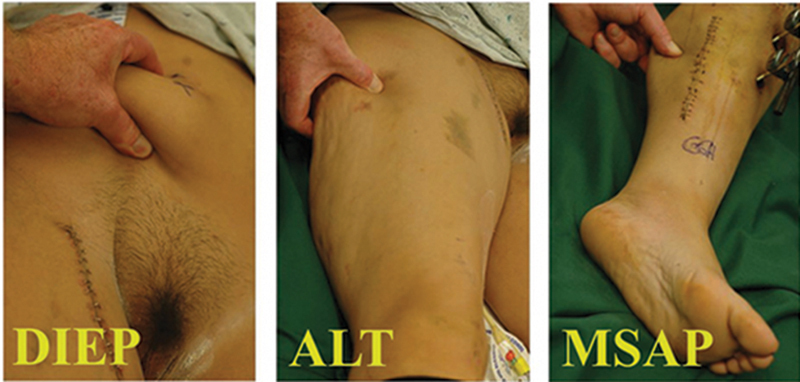
“Pinch test” donor site comparison in another individual with deep inferior epigastric perforator (DIEP), anterolateral thigh (ALT), and medial sural artery perforator (MSAP)—proving typically to be the thinnest.
Fig. 5.

This medial sural artery perforator (MSAP) flap thickness as measured in situ was 2.0 cm. The same flap used for Fig. 3 was used here.
Fig. 6.

The medial sural artery perforator (MSAP) free flap for resurfacing the lower lip provided coverage, but obliterated subunit contour with a color differential from the rest of the face that would be aesthetically unacceptable.
The absence of a MSAP clearly does not allow harvest of this flap, 30 but so too in the dysvascular patient should this donor site be avoided as that perforator may be important for contributing to more distal lower limb collateral circulation. 88 Many have in addition arbitrarily condemned this flap choice solely on the basis of the donor site sequela ( Fig. 3 ). A flap wider than 5 to 9 mm 2 32 40 50 may require a skin graft on the calf that will be obvious, and just not acceptable to most women. 4 Tissue stretching 64 or tissue expansion 89 techniques to allow primary closure will still leave a conspicuous scar that might be just as unacceptable. Understanding all these detriments by the surgeon is essential, so that selection of the MSAP flap will provide an unequaled benefit, as has been suggested by the following references from head to toe.
External Head and Neck
The MSAP flap may be a thin flap to resurface the cheek, neck, or even scalp with a long vascular pedicle of reasonable caliber needed to reach available recipient sites. 20 21 30 54 59 90 Contour and appearance here will be obvious, so this will always be an unavoidable concern Fig. 6 .
Internal Head and Neck
A meta-analysis of the literature stated that to date the oropharynx was one of the commonest sites where use of the MSAP flap had been reported. 18 The thin, relatively pliable small-volume MSAP flap is often ideally suited as a solution for reconstruction of the oral cavity. 56 91 92 This is most appropriate for the two-dimensional surfaces of the floor of mouth 30 48 56 59 93 and buccal mucosa, 30 48 56 and also rarely for the hard 56 and soft palate 30 and retromolar trigone. 48 Many consider this the best solution for partial tongue defects where the anterolateral flap would just be too bulky, thereby better allowing maximal tongue movement for the purposes of speech and swallowing, and, sometimes if a small portion of the MGM is included as a chimeric flap, providing sufficient bulk for deglutition. 30 48 56 59 60 81 86 93 94 Since this donor site is well away from the intended recipient site of the head and neck, a simultaneous two-team approach will be another advantage. 92
Upper Extremity and Hand
The thinness of the MSAP flap that has a gliding fascial undersurface may be sufficient reason for resurfacing the hand or elsewhere in the upper extremity where there is exposed bone or tendon. 20 21 38 58 90 95 96 97 98 99 This donor site simultaneously allows access to tendon and nerve grafts, which often are secondary requirements. 20 58 99
Genitalia
Although this is a popular topic today in reconstructive surgery, only a single manuscript regarding use of the MSAP flap in this region was found. That was a free flap by Teven et al, 68 where in the absence of local thigh-based flaps, this was used to resurface the groin and pubis while creating a neo-scrotum for a buried testicle.
Leg
The oft-quoted original paper by Cavadas et al 2 included six cases where five were a free flap and the other a local pedicled flap, all for varied lower extremity reconstructions. Typical problems of exposed bone that required a small to moderate-sized free flap were reasonable candidates for an MSAP flap, 20 90 100 but this has also been used in the presence of chronic osteomyelitis. 61 Many who would not select this flap since they are intimidated by the donor site morbidity may find this to be one of the few body regions where there would be a legitimate indication for its selection, as deformities secondary to the recipient site already exist. 101
Montegut and Allen were the first to report a pedicled version of the MSAP flap as “an alternative for the gastrocnemius myocutaneous flap.” 8 The more extended reach of the island MSAP flap compared with the MGM better permits knee coverage of small to moderate-sized traumatic wounds, oncologic resections, or prosthesis exposures. 47 57 64 80 102 103 A chimeric version that includes a portion of the more malleable muscle will allow the latter to concomitantly fill deeper recesses. 24 75 82 Prophylactic para-patellar soft-tissue augmentation especially for secondary knee surgery such as a repeat total knee prosthesis can prevent later untoward wound healing issues leading to loss of the prosthesis. 104 105
The popliteal space such as following a knee scar flexion contracture can also be resurfaced with a pedicled MSAP flap to avoid a skin graft that might recontract. 67 V-Y advancement island flaps requiring minimal perforator intramuscular dissection can reach other adjacent calf defects. 13 106 The same perforators can be the hub of a propeller flap that can cover the anterior middle third of the leg. 69 If the pedicle of an island flap is ligated proximally with then reverse flow to the perforator, even the more distal leg can be reached, albeit with an increased risk of complications due to insufficient perfusion. 69 107
Foot
Any flap chosen to cover any of the zones of the foot and ankle while adhering to the subunit principle 108 must be thin and pliable enough to permit normal fitting of shoewear. 74 The MSAP free flap, depending on the proper patient body habitus and when only a small to moderate sized flap is required, can be used successfully for all zones. 49 101 109 Much like use of the archival cross-leg flap to cover the foot, a contralateral MSAP free flap could be used in a single stage as an immediate cross-leg flap without the need for a microanastomosis—but beware of that technical exercise, as it is far better today to use the ipsilateral version to restrict morbidity to only a single lower extremity! 110 Plantar reconstruction remains our nemesis, as any flap choice must withstand constant weight-bearing pressures and shear forces, which some say must include protective sensation. Kim et al 111 found that plantar resurfaced MSAP flaps proved adequate and regained relatively good protective sensation within 12 months.
Recipient Site
Just as important as knowledge of the MSAP flap as a donor flap is an understanding of its vascular supply that could also serve as a recipient site for another free flap. For large para-patellar defects, this could avoid use of lower limb source vessels that may be difficult to access or may be compromised in some other way. The medial sural vessels can be dissected in orthograde fashion from their popliteal vessel origin to their muscle hilum to provide a more accessible vascular leash for microanastomosis with the patient in almost any position 112 —prone, 113 lateral decubitus, 37 114 or supine. 43 115 Another option would be a retrograde intramuscular dissection of the medial sural vessels as done by Trapero et al 116 after a prior medial gastrocnemius flap, but even safer if an MSAP could be followed until the caliber and length of its source branch were sufficient to match that needed. 117
The Workhorse
If anything can be gleaned from this overview and from previous studies by many others, 17 18 19 20 21 22 the anatomy of the MSAP flap can be obstinate, as there is no consistency that permits use of a schematic based on anatomical landmarks that would quickly lead to finding the perforator around which the necessary flap can be accurately designed. Instead, as is the case with most perforator flaps, this may be an adventure even using available technology—but worth the effort as long as an adequate perforator can be found. If not available or if the first MSAP flap is unsalvageable, 21 perhaps the contralateral calf would be more receptive; or one must remember that the medial gastrocnemius muscle usually remains virtually unharmed and can always be an alternative local flap. 118
If a thin and pliable flap of small or moderate size with a pedicle of moderate length is needed anywhere in the body, the MSAP flap could be the ideal choice as there are many legitimate attributes ( Table 1 ), such as allowing exquisite partial tongue repair with minimal donor site morbidity. 56 86 94 However, many object to any MSAP indication—finding the donor site appearance of even a longitudinal scar to be unacceptable. 4 Yet its use as a pedicle flap for the knee, 64 75 80 103 105 popliteal space, 67 or even proximal third of the leg, 69 or even as a free flap for an ipsilateral lower extremity challenge 101 should all be legitimate reasons for acceptance of this as the best cutaneous flap option, since donor site sequela probably would be less than that already existing at the recipient site. It behooves the reconstructive microsurgeon to be knowledgeable of the versatile possibilities and alternatives for this MSAP flap, so that the benefits when selected will always supersede the detriments.
Acknowledgments
David C. Rice, B.S., Physician Assistant, St. Luke's Hospital, Sacred Heart Division, Allentown, Pennsylvania, assisted with all microsurgeries.
Conflict of Interest None declared.
Author Contribution
All conceptualization and writing including original draft, review, and editing were done by the corresponding author.
References
- 1.Hallock G G. Anatomic basis of the gastrocnemius perforator-based flap. Ann Plast Surg. 2001;47(05):517–522. doi: 10.1097/00000637-200111000-00008. [DOI] [PubMed] [Google Scholar]
- 2.Cavadas P C, Sanz-Giménez-Rico J R, Gutierrez-de la Cámara A, Navarro-Monzonís A, Soler-Nomdedeu S, Martínez-Soriano F. The medial sural artery perforator free flap. Plast Reconstr Surg. 2001;108(06):1609–1615. doi: 10.1097/00006534-200111000-00027. [DOI] [PubMed] [Google Scholar]
- 3.Blondeel P N, Van Landuyt K H, Monstrey S J. The “Gent” consensus on perforator flap terminology: preliminary definitions. Plast Reconstr Surg. 2003;112(05):1378–1383. doi: 10.1097/01.PRS.0000081071.83805.B6. [DOI] [PubMed] [Google Scholar]
- 4.Koshima I. The medial sural artery perforator free flap. Plast Reconstr Surg. 2001;108:1616–1617. doi: 10.1097/00006534-200111000-00027. [DOI] [PubMed] [Google Scholar]
- 5.Taylor G I, Daniel R K. The free flap: composite tissue transfer by vascular anastomosis. Aust N Z J Surg. 1973;43(01):1–3. doi: 10.1111/j.1445-2197.1973.tb05659.x. [DOI] [PubMed] [Google Scholar]
- 6.Taylor G I, Daniel R K. The anatomy of several free flap donor sites. Plast Reconstr Surg. 1975;56(03):243–253. doi: 10.1097/00006534-197509000-00001. [DOI] [PubMed] [Google Scholar]
- 7.Keller A, Allen R, Shaw W. The medial gastrocnemius muscle flap: a local free flap. Plast Reconstr Surg. 1984;73(06):974–976. doi: 10.1097/00006534-198406000-00025. [DOI] [PubMed] [Google Scholar]
- 8.Montegut W J, Allen R J.Sural artery perforator flap as an alternative for the gastrocnemius myocutaneous flapThe 90th Annual Scientific Assembly of the Southern Medical Association; Baltimore, MD; November 20–24,1996
- 9.Morain W D. New York, NY: Springer-Verlag; 1983. [Translator], Carl Manchot: The Cutaneous Arteries of the Human Body [Introduction] p. 112. [Google Scholar]
- 10.Morain W D. New York, NY: Springer-Verlag; 1983. [Translator], Carl Manchot: The Cutaneous Arteries of the Human Body [Introduction] p. 113. [Google Scholar]
- 11.Mathes S J, Vasconez L O. St. Louis, MO: CV Mosby Co; 1982. Lower extremity reconstruction; pp. 552–553. [Google Scholar]
- 12.Mathes S J, Nahai F. New York, NY: Churchill Livingstone; 1997. Leg: sural artery flap; pp. 1489–1499. [Google Scholar]
- 13.Venkataramakrishnan V, Mohan D, Villafane O. Perforator based V-Y advancement flaps in the leg. Br J Plast Surg. 1998;51(06):431–435. doi: 10.1054/bjps.1997.0229. [DOI] [PubMed] [Google Scholar]
- 14.Taylor G I, Pan W R. Angiosomes of the leg: anatomic study and clinical implications. Plast Reconstr Surg. 1998;102(03):599–616. [PubMed] [Google Scholar]
- 15.Shaw A D, Ghosh S J, Quaba A A. The island posterior calf fasciocutaneous flap: an alternative to the gastrocnemius muscle for cover of knee and tibial defects. Plast Reconstr Surg. 1998;101(06):1529–1536. doi: 10.1097/00006534-199805000-00016. [DOI] [PubMed] [Google Scholar]
- 16.Wei F C, Jain V, Suominen S, Chen H C. Confusion among perforator flaps: what is a true perforator flap? Plast Reconstr Surg. 2001;107(03):874–876. doi: 10.1097/00006534-200103000-00037. [DOI] [PubMed] [Google Scholar]
- 17.Xie X T, Chai Y M. Medial sural artery perforator flap. Ann Plast Surg. 2012;68(01):105–110. doi: 10.1097/SAP.0b013e31821190e6. [DOI] [PubMed] [Google Scholar]
- 18.Daar D A, Abdou S A, Cohen J M, Wilson S C, Levine J P. Is the medial sural artery perforator flap a new workhorse flap? a systematic review and meta-analysis. Plast Reconstr Surg. 2019;143(02):393e–403e. doi: 10.1097/PRS.0000000000005204. [DOI] [PubMed] [Google Scholar]
- 19.Hallock G G. A pragmatic evaluation of the role of the medial sural artery perforator flap. J Xiangya Med. 2018;3:19. [Google Scholar]
- 20.Sue G R, Kao H K, Borrelli M R, Cheng M H. The versatile free medial sural artery perforator flap: an institutional experience for reconstruction of the head and neck, upper and lower extremities. Microsurgery. 2020;40(04):427–433. doi: 10.1002/micr.30543. [DOI] [PubMed] [Google Scholar]
- 21.Deek N FA, Hsiao J C, Do N T. The medial sural artery perforator flap: lessons learned from 200 consecutive cases. Plast Reconstr Surg. 2020;146(05):630e–641e. doi: 10.1097/PRS.0000000000007282. [DOI] [PubMed] [Google Scholar]
- 22.Hsiao J C, Deek N, Lin C H.Versatility of the medial sural artery perforator flap: experience with 200 consecutive cases Plast Reconstr Surg 2015136(4S):17. [DOI] [PubMed] [Google Scholar]
- 23.Hallock G G. Colgajo Sensible Basado en Perforantes de la Arteria Sural Lateral [A sensate lateral sural artery muscle perforator flap] Cir Plas Iberolatinoam. 2006;32:293–297. [Google Scholar]
- 24.Hallock G G. Chimeric gastrocnemius muscle and sural artery perforator local flap. Ann Plast Surg. 2008;61(03):306–309. doi: 10.1097/SAP.0b013e31815b2792. [DOI] [PubMed] [Google Scholar]
- 25.Shimizu F, Kato A, Sato H, Taneda H. Sural perforator flap: assessment of the posterior calf region as donor site for a free fasciocutaneous flap. Microsurgery. 2009;29(04):253–258. doi: 10.1002/micr.20626. [DOI] [PubMed] [Google Scholar]
- 26.Kashiwa K, Kobayashi S, Hayashi M, Honda T, Nasu W. Gastrocnemius perforating artery flap including vascularized sural nerve. J Reconstr Microsurg. 2003;19(07):443–450. doi: 10.1055/s-2003-44631. [DOI] [PubMed] [Google Scholar]
- 27.Kosutic D, Pejkovic B, Anderhuber F. Complete mapping of lateral and medial sural artery perforators: anatomical study with Duplex-Doppler ultrasound correlation. J Plast Reconstr Aesthet Surg. 2012;65(11):1530–1536. doi: 10.1016/j.bjps.2012.04.045. [DOI] [PubMed] [Google Scholar]
- 28.Dusseldorp J R, Pham Q J, Ngo Q, Gianoutsos M, Moradi P. Vascular anatomy of the medial sural artery perforator flap: a new classification system of intra-muscular branching patterns. J Plast Reconstr Aesthet Surg. 2014;67(09):1267–1275. doi: 10.1016/j.bjps.2014.05.016. [DOI] [PubMed] [Google Scholar]
- 29.Altaf F M. The anatomical basis of the medial sural artery perforator flaps. West Indian Med J. 2011;60(06):622–627. [PubMed] [Google Scholar]
- 30.Kao H K, Chang K P, Chen Y A, Wei F C, Cheng M H. Anatomical basis and versatile application of the free medial sural artery perforator flap for head and neck reconstruction. Plast Reconstr Surg. 2010;125(04):1135–1145. doi: 10.1097/PRS.0b013e3181d180ac. [DOI] [PubMed] [Google Scholar]
- 31.Thione A, Valdatta L, Buoro M, Tuinder S, Mortarino C, Putz R. The medial sural artery perforators: anatomic basis for a surgical plan. Ann Plast Surg. 2004;53(03):250–255. doi: 10.1097/01.sap.0000116242.26334.b5. [DOI] [PubMed] [Google Scholar]
- 32.Kim H H, Jeong J H, Seul J H, Cho B C. New design and identification of the medial sural perforator flap: an anatomical study and its clinical applications. Plast Reconstr Surg. 2006;117(05):1609–1618. doi: 10.1097/01.prs.0000207077.19601.86. [DOI] [PubMed] [Google Scholar]
- 33.Wong M Z, Wong C H, Tan B K, Chew K Y, Tay S C. Surgical anatomy of the medial sural artery perforator flap. J Reconstr Microsurg. 2012;28(08):555–560. doi: 10.1055/s-0032-1315778. [DOI] [PubMed] [Google Scholar]
- 34.Okamoto H, Sekiya I, Mizutani J, Otsuka T. Anatomical basis of the medial sural artery perforator flap in Asians. Scand J Plast Reconstr Surg Hand Surg. 2007;41(03):125–129. doi: 10.1080/02844310601159972. [DOI] [PubMed] [Google Scholar]
- 35.Hupkens P, Westland P B, Schijns W, van Abeelen M HA, Kloeters O, Ulrich D JO. Medial lower leg perforators: an anatomical study of their distribution and characteristics. Microsurgery. 2017;37(04):319–326. doi: 10.1002/micr.30076. [DOI] [PubMed] [Google Scholar]
- 36.The Vascular Territories . Taylor G I, Palmer J H. The vascular territories (angiosomes) of the body: experimental study and clinical applications. Br J Plast Surg. 1987;40(02):113–141. doi: 10.1016/0007-1226(87)90185-8. [DOI] [PubMed] [Google Scholar]
- 37.Fu J, Gao J, Yi Y. The clinical application of medial sural vessels as recipient vessels in repairing traumatic tissue defects in the lower limbs. Ann Plast Surg. 2020;84(04):418–424. doi: 10.1097/SAP.0000000000002156. [DOI] [PubMed] [Google Scholar]
- 38.Wang X, Mei J, Pan J, Chen H, Zhang W, Tang M. Reconstruction of distal limb defects with the free medial sural artery perforator flap. Plast Reconstr Surg. 2013;131(01):95–105. doi: 10.1097/PRS.0b013e3182729e3c. [DOI] [PubMed] [Google Scholar]
- 39.Pease N L, Ong J, Townley W A. Fixed reference points in mapping medial sural artery perforator location. J Plast Reconstr Aesthet Surg. 2015;68(04):589–590. doi: 10.1016/j.bjps.2014.10.048. [DOI] [PubMed] [Google Scholar]
- 40.Kao H K, Chang K P, Wei F C, Cheng M H. Comparison of the medial sural artery perforator flap with the radial forearm flap for head and neck reconstructions. Plast Reconstr Surg. 2009;124(04):1125–1132. doi: 10.1097/PRS.0b013e3181b457cf. [DOI] [PubMed] [Google Scholar]
- 41.Tsetsonis C H, Kaxira O S, Laoulakos D H, Spiliopoulou C A, Koutselinis A S. The arterial communication between the gastrocnemius muscle heads: a fresh cadaveric study and clinical implications. Plast Reconstr Surg. 2000;105(01):94–98. doi: 10.1097/00006534-200001000-00016. [DOI] [PubMed] [Google Scholar]
- 42.Tsetsonis C H, Kaxira O S, Laoulakos D H, Spiliopoulou C A, Koutselinis A S. The venous communication between the gastrocnemius muscle heads. Plast Reconstr Surg. 2000;105(04):1357–1360. doi: 10.1097/00006534-200004040-00014. [DOI] [PubMed] [Google Scholar]
- 43.Hallock G G. The medial approach to the sural vessels to facilitate microanastomosis about the knee. Ann Plast Surg. 1994;32(04):388–393. doi: 10.1097/00000637-199404000-00012. [DOI] [PubMed] [Google Scholar]
- 44.Saint-Cyr M, Wong C, Schaverien M, Mojallal A, Rohrich R J. The perforasome theory: vascular anatomy and clinical implications. Plast Reconstr Surg. 2009;124(05):1529–1544. doi: 10.1097/PRS.0b013e3181b98a6c. [DOI] [PubMed] [Google Scholar]
- 45.Taylor G I, Caddy C M, Watterson P A, Crock J G. The venous territories (venosomes) of the human body: experimental study and clinical implications. Plast Reconstr Surg. 1990;86(02):185–213. doi: 10.1097/00006534-199008000-00001. [DOI] [PubMed] [Google Scholar]
- 46.Hallock G G. The venous perforasome? Plast Reconstr Surg. 2020;146(06):840e–841e. doi: 10.1097/PRS.0000000000007382. [DOI] [PubMed] [Google Scholar]
- 47.Hallock G G. The medial sural(medial gastrocnemius) perforator local flap. Ann Plast Surg. 2004;53(05):501–505. doi: 10.1097/01.sap.0000116338.59679.12. [DOI] [PubMed] [Google Scholar]
- 48.Chen S L, Yu C C, Chang M C, Deng S C, Wu Y S, Chen T M. Medial sural artery perforator flap for intraoral reconstruction following cancer ablation. Ann Plast Surg. 2008;61(03):274–279. doi: 10.1097/SAP.0b013e318157a1a0. [DOI] [PubMed] [Google Scholar]
- 49.Jandali Z, Lam M C, Aganloo K. The free medial sural artery perforator flap: versatile option for soft tissue reconstruction in small-to-moderate size defects of the foot and ankle. Microsurgery. 2018;38(01):34–45. doi: 10.1002/micr.30100. [DOI] [PubMed] [Google Scholar]
- 50.Hallock G G, Sano K. The medial sural medial gastrocnemius perforator free flap: an “ideal” prone position skin flap. Ann Plast Surg. 2004;52(02):184–187. doi: 10.1097/01.sap.0000095438.33962.31. [DOI] [PubMed] [Google Scholar]
- 51.Ranson J, Rosich-Medina A, Amin K, Kosutic D. Medial sural artery perforator flap: using the superficial venous system to minimize flap congestion. Arch Plast Surg. 2015;42(06):813–815. doi: 10.5999/aps.2015.42.6.813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Hallock G G. A primer of schematics to facilitate the design of the preferred muscle perforator flaps. Plast Reconstr Surg. 2009;123(03):1107–1115. doi: 10.1097/PRS.0b013e318199f7d2. [DOI] [PubMed] [Google Scholar]
- 53.Song X, Wu H, Zhang W. Medial sural artery perforator flap for postsurgical reconstruction of head and neck cancer. J Reconstr Microsurg. 2015;31(04):319–326. doi: 10.1055/s-0035-1544180. [DOI] [PubMed] [Google Scholar]
- 54.Choi J W, Nam S Y, Choi S H, Roh J L, Kim S Y, Hong J P. Applications of medial sural perforator free flap for head and neck reconstructions. J Reconstr Microsurg. 2013;29(07):437–442. doi: 10.1055/s-0033-1343959. [DOI] [PubMed] [Google Scholar]
- 55.Chalmers R L, Rahman K MA, Young S. The medial sural artery perforator flap in intra-oral reconstruction: a northeast experience. J Plast Reconstr Aesthet Surg. 2016;69(05):687–693. doi: 10.1016/j.bjps.2016.01.005. [DOI] [PubMed] [Google Scholar]
- 56.Molina A R, Citron I, Chinaka F, Cascarini L, Townley W A. Calf perforator flaps: a freestyle solution for oral cavity reconstruction. Plast Reconstr Surg. 2017;139(02):459–465. doi: 10.1097/PRS.0000000000002953. [DOI] [PubMed] [Google Scholar]
- 57.Shim J S, Kim H H.A novel reconstruction technique for the knee and upper one third of lower leg J Plast Reconstr Aesthet Surg 20065909919–926., discussion 927 [DOI] [PubMed] [Google Scholar]
- 58.Zheng H, Liu J, Dai X, Schilling A F. Free conjoined or chimeric medial sural artery perforator flap for the reconstruction of multiple defects in hand. J Plast Reconstr Aesthet Surg. 2015;68(04):565–570. doi: 10.1016/j.bjps.2014.12.031. [DOI] [PubMed] [Google Scholar]
- 59.Shen X Q, Lv Y, Shen H, Lu H, Wu S C, Lin X J. Endoscope-assisted medial sural artery perforator flap for head and neck reconstruction. J Plast Reconstr Aesthet Surg. 2016;69(08):1059–1065. doi: 10.1016/j.bjps.2016.01.029. [DOI] [PubMed] [Google Scholar]
- 60.He Y, Jin S F, Zhang Z Y, Feng S Q, Zhang C P, Zhang Y X. A prospective study of medial sural artery perforator flap with computed tomographic angiography-aided design in tongue reconstruction. J Oral Maxillofac Surg. 2014;72(11):2351–2365. doi: 10.1016/j.joms.2014.05.019. [DOI] [PubMed] [Google Scholar]
- 61.Park G, Kim H. Treatment of chronic osteomyelitis using the medial sural perforator flap. J Plast Reconstr Aesthet Surg. 2010;63(01):153–159. doi: 10.1016/j.bjps.2008.07.018. [DOI] [PubMed] [Google Scholar]
- 62.Lee C H, Chang N T, Hsiao J C.Extended use of chimeric medial sural artery perforator flap for 3-dimensional defect reconstruction Ann Plast Surg 201982(1S, Suppl 1):S86–S94. [DOI] [PubMed] [Google Scholar]
- 63.Scaglioni M F, Rodi T, Fritsche E. The versatility of the pedicled medial sural artery perforator flap: from simple to its chimeric pattern and clinical experience with 37 cases. Plast Reconstr Surg. 2021;147(04):960–969. doi: 10.1097/PRS.0000000000007795. [DOI] [PubMed] [Google Scholar]
- 64.Luca-Pozner V, Delgove A, Kerfant N, Karra A, Herlin C, Chaput B. Medial sural artery perforator flap for leg and knee coverage: extended skin paddle with 2 perforators. Ann Plast Surg. 2020;85(06):650–655. doi: 10.1097/SAP.0000000000002356. [DOI] [PubMed] [Google Scholar]
- 65.Pereira N, Hallock G G. Smartphone thermography for lower extremity local flap perforator mapping. J Reconstr Microsurg. 2021;37(01):59–66. doi: 10.1055/s-0039-3402032. [DOI] [PubMed] [Google Scholar]
- 66.Walton R L, Bunkis J. The posterior calf fasciocutaneous free flap. Plast Reconstr Surg. 1984;74(01):76–85. doi: 10.1097/00006534-198407000-00011. [DOI] [PubMed] [Google Scholar]
- 67.Kim K S, Kim E S, Hwang J H, Lee S Y. Medial sural perforator plus island flap: a modification of the medial sural perforator island flap for the reconstruction of postburn knee flexion contractures using burned calf skin. J Plast Reconstr Aesthet Surg. 2012;65(06):804–809. doi: 10.1016/j.bjps.2011.12.018. [DOI] [PubMed] [Google Scholar]
- 68.Teven C M, Yu J W, Zhao L C, Levine J P. Extended medial sural artery perforator free flap for groin and scrotal reconstruction. Arch Plast Surg. 2020;47(04):354–359. doi: 10.5999/aps.2019.01921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Tee R, Jeng S F, Chen C C, Shih H S. The medial sural artery perforator pedicled propeller flap for coverage of middle-third leg defects. J Plast Reconstr Aesthet Surg. 2019;72(12):1971–1978. doi: 10.1016/j.bjps.2019.08.006. [DOI] [PubMed] [Google Scholar]
- 70.Taylor G I, Chubb D P, Ashton M W. True and “choke” anastomoses between perforator angiosomes: part I. anatomical location. Plast Reconstr Surg. 2013;132(06):1447–1456. doi: 10.1097/PRS.0b013e3182a80638. [DOI] [PubMed] [Google Scholar]
- 71.Shen H, Shen X Q, Lv Y, Xu J H, Lu H. Pharyngoesophageal reconstruction with the medial sural artery perforator flap after total laryngopharyngectomy: a new method. Ann Plast Surg. 2017;78(02):191–194. doi: 10.1097/SAP.0000000000000794. [DOI] [PubMed] [Google Scholar]
- 72.Hsiang-Shun S, Kokkoli E, Jeng S F.Medial sural artery perforator flap a practical way of optimizing the harvesting procedure Plast Reconstr Surg 2015136(4S):16725829155 [Google Scholar]
- 73.Mehrotra S. Perforator-plus flaps: a new concept in traditional flap design. Plast Reconstr Surg. 2007;119(02):590–598. doi: 10.1097/01.prs.0000239570.18647.83. [DOI] [PubMed] [Google Scholar]
- 74.Chen S L, Chuang C J, Chou T D, Chen T M, Wang H J. Free medial sural artery perforator flap for ankle and foot reconstruction. Ann Plast Surg. 2005;54(01):39–43. doi: 10.1097/01.sap.0000141376.15470.9b. [DOI] [PubMed] [Google Scholar]
- 75.Cho Y J, Lee J H, Chung D W. Pedicled chimeric gastrocnemius-medial sural artery adipofascial flap for reconstruction of anterolateral defects of the knee. Microsurgery. 2017;37(03):206–211. doi: 10.1002/micr.22436. [DOI] [PubMed] [Google Scholar]
- 76.Hallock G G. The complete nomenclature for combined perforator flaps. Plast Reconstr Surg. 2011;127(04):1720–1729. doi: 10.1097/PRS.0b013e31820a662b. [DOI] [PubMed] [Google Scholar]
- 77.Huang W C, Chen H C, Wei F C, Cheng M H, Schnur D P. Chimeric flap in clinical use. Clin Plast Surg. 2003;30(03):457–467. doi: 10.1016/s0094-1298(03)00046-4. [DOI] [PubMed] [Google Scholar]
- 78.Sano K, Hallock G G, Hamazaki M, Daicyo Y. The perforator-based conjoint (chimeric) medial sural(medial gastrocnemius) free flap. Ann Plast Surg. 2004;53(06):588–592. doi: 10.1097/01.sap.0000136971.16368.80. [DOI] [PubMed] [Google Scholar]
- 79.Zhang Y X, Hayakawa T J, Levin L S, Hallock G G, Lazzeri D. The economy in autologous tissue transfer: part 1. The kiss flap technique. Plast Reconstr Surg. 2016;137(03):1018–1030. doi: 10.1097/01.prs.0000479971.99309.21. [DOI] [PubMed] [Google Scholar]
- 80.Han S E, Lee K T, Mun G H. Muscle-chimaeric medial sural artery perforator flap: a new design for complex three-dimensional knee defect. J Plast Reconstr Aesthet Surg. 2014;67(04):571–574. doi: 10.1016/j.bjps.2013.09.023. [DOI] [PubMed] [Google Scholar]
- 81.Ooi A SH, Ng M JM, Sudirman S RB, Chang D. The chimeric medial sural artery perforator flap as the ideal for partial tongue reconstruction: a case series and technical refinements. J Plast Reconstr Aesthet Surg. 2021;74(10):2613–2621. doi: 10.1016/j.bjps.2021.03.024. [DOI] [PubMed] [Google Scholar]
- 82.Innocenti M, Cardin-Langlois E, Menichini G, Baldrighi C. Gastrocnaemius-propeller extended miocutanous flap: a new chimaeric flap for soft tissue reconstruction of the knee. J Plast Reconstr Aesthet Surg. 2014;67(02):244–251. doi: 10.1016/j.bjps.2013.10.011. [DOI] [PubMed] [Google Scholar]
- 83.Hallock G G. The chimeric propeller flap. Semin Plast Surg. 2020;34(03):207–209. doi: 10.1055/s-0040-1714290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Al-Qattan M M. A modified technique for harvesting the reverse sural artery flap from the upper part of the leg: inclusion of a gastrocnemius muscle “cuff” around the sural pedicle. Ann Plast Surg. 2001;47(03):269–274. doi: 10.1097/00000637-200109000-00009. [DOI] [PubMed] [Google Scholar]
- 85.Hallock G G. A modified technique for harvesting the reverse sural artery flap from the upper part of the leg: Inclusion of a Gastrocnemius Muscle “Cuff” Around the Sural Pedicle (Discussion) Annal Plast Surg. 2001;47:274–278. doi: 10.1097/00000637-200109000-00009. [DOI] [PubMed] [Google Scholar]
- 86.Ng M JM, Goh C SL, Tan N C, Song D H, Ooi A SH. A head-to-head comparison of the medial sural artery perforator versus radial forearm flap for tongue reconstruction. J Reconstr Microsurg. 2021;37(05):445–452. doi: 10.1055/s-0040-1718551. [DOI] [PubMed] [Google Scholar]
- 87.Akdeniz Doğan Z D, Çavuş Özkan M, Tuncer F B, Saçak B, Çelebiler Ö. A comparative clinical study of flap thickness: medial sural artery perforator flap versus anterolateral thigh flap. Ann Plast Surg. 2018;81(04):472–474. doi: 10.1097/SAP.0000000000001488. [DOI] [PubMed] [Google Scholar]
- 88.Edmondson S J, Townley W A, Orfaniotis G. Elevation of medial sural artery perforator free flap in a chronically ischaemic donor leg: findings and outcome in a case of salvage laryngopharyngectomy. Microsurgery. 2020;40(07):827–828. doi: 10.1002/micr.30630. [DOI] [PubMed] [Google Scholar]
- 89.Hallock G G. Free flap donor site refinement using tissue expansion. Ann Plast Surg. 1988;20(06):566–572. doi: 10.1097/00000637-198806000-00013. [DOI] [PubMed] [Google Scholar]
- 90.Ives M, Mathur B. Varied uses of the medial sural artery perforator flap. J Plast Reconstr Aesthet Surg. 2015;68(06):853–858. doi: 10.1016/j.bjps.2015.02.001. [DOI] [PubMed] [Google Scholar]
- 91.Chang E I. Discussion: calf perforator flaps: a freestyle solution for oral cavity reconstruction. Plast Reconstr Surg. 2017;139(02):466–467. doi: 10.1097/PRS.0000000000002985. [DOI] [PubMed] [Google Scholar]
- 92.Mughal M, Gabuniya N, Zoccali G, Roblin P, Townley W. Functional outcomes of the medial sural artery perforator flap in oral cavity reconstruction. Ann Plast Surg. 2020;85(03):256–259. doi: 10.1097/SAP.0000000000002352. [DOI] [PubMed] [Google Scholar]
- 93.Chen S L, Chen T M, Dai N T, Hsia Y J, Lin Y S. Medial sural artery perforator flap for tongue and floor of mouth reconstruction. Head Neck. 2008;30(03):351–357. doi: 10.1002/hed.20712. [DOI] [PubMed] [Google Scholar]
- 94.He Y, Jin S F, Zhang C P, Zhang Z Y. Medial sural artery perforator flap aided by preoperative computed tomography angiography mapping for tongue reconstruction. Int J Oral Maxillofac Surg. 2014;43(09):1064–1068. doi: 10.1016/j.ijom.2014.05.016. [DOI] [PubMed] [Google Scholar]
- 95.Lin C H, Lin C H, Lin Y T, Hsu C C, Ng T W, Wei F C. The medial sural artery perforator flap: a versatile donor site for hand reconstruction. J Trauma. 2011;70(03):736–743. doi: 10.1097/TA.0b013e318203179e. [DOI] [PubMed] [Google Scholar]
- 96.Hallock G G. The medial sural artery perforator flap: a versatile donor site for hand reconstruction. J Trauma. 2011;70:742–743. doi: 10.1097/TA.0b013e318203179e. [DOI] [PubMed] [Google Scholar]
- 97.Ryu M H, Kim H H. Hand reconstruction with medial sural perforator free flap. J Korean Soc Plast Reconstr Surg. 2006;33:715–722. [Google Scholar]
- 98.Jeevaratnam J A, Nikkhah D, Nugent N F, Blackburn A V. The medial sural artery perforator flap and its application in electrical injury to the hand. J Plast Reconstr Aesthet Surg. 2014;67(11):1591–1594. doi: 10.1016/j.bjps.2014.07.023. [DOI] [PubMed] [Google Scholar]
- 99.Xie R G, Gu J H, Gong Y P, Tang J B. Medial sural artery perforator flap for repair of the hand. J Hand Surg Eur Vol. 2007;32(05):512–517. doi: 10.1016/J.JHSE.2007.05.010. [DOI] [PubMed] [Google Scholar]
- 100.Sano K, Hallock G G, Hyakusoku H. Free medial gastrocnemius perforator flap for reconstruction of soft tissue defect in extremities. J Jpn SRM. 2005;18:359–363. [Google Scholar]
- 101.Hallock G G. Medial sural artery perforator free flap: legitimate use as a solution for the ipsilateral distal lower extremity defect. J Reconstr Microsurg. 2014;30(03):187–192. doi: 10.1055/s-0033-1357276. [DOI] [PubMed] [Google Scholar]
- 102.Umemoto Y, Adachi Y, Ebisawa K. The sural artery perforator flap for coverage of defects of the knee and tibia. Scand J Plast Reconstr Surg Hand Surg. 2005;39(04):209–212. doi: 10.1080/02844310410004964. [DOI] [PubMed] [Google Scholar]
- 103.Chiang I H, Wu C C, Chen S G, Wang C H. Pedicled medial sural perforator flap for the reconstruction of knee defects. Int Wound J. 2017;14(04):673–677. doi: 10.1111/iwj.12668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Hallock G G. The medial sural artery perforator island flap as a simpler alternative for prophylactic skin augmentation prior to total knee arthroplasty. Internat J Orthoplast Surg. 2019;1:1–4. [Google Scholar]
- 105.Azoury S C, Stranix J T, Piper M, Kovach S J, Hallock G G. Attributes of perforator flaps for prophylatic soft tissue augmentation prior to definitive total knee arthroplasty. J Reconstr Microsurg. 2021;37(01):51–58. doi: 10.1055/s-0039-3401847. [DOI] [PubMed] [Google Scholar]
- 106.John J R. Medial sural artery V-Y advancement flap: bridging a learning curve. J Reconstr Microsurg. 2013;29(07):491–492. doi: 10.1055/s-0033-1343954. [DOI] [PubMed] [Google Scholar]
- 107.Persichetti P, Brunetti B, Aveta A, Segreto F. Reverse-flow medial sural artery perforator flap: pedicle extension for distal lower limb defects. Ann Plast Surg. 2013;70(02):246–247. doi: 10.1097/SAP.0b013e3182480354. [DOI] [PubMed] [Google Scholar]
- 108.Hollenbeck S T, Woo S, Komatsu I, Erdmann D, Zenn M R, Levin L S. Longitudinal outcomes and application of the subunit principle to 165 foot and ankle free tissue transfers. Plast Reconstr Surg. 2010;125(03):924–934. doi: 10.1097/PRS.0b013e3181cc9630. [DOI] [PubMed] [Google Scholar]
- 109.Lee G, Jeong E. Coverage of defect over toes after failure of microsurgical replantation with medial sural artery perforator flap: a case report. Microsurgery. 2016;36(02):161–164. doi: 10.1002/micr.22415. [DOI] [PubMed] [Google Scholar]
- 110.Hallock G G. Medial sural gastrocnemius muscle perforator free flap: an immediate cross-leg flap? J Reconstr Microsurg. 2005;21(04):217–223. doi: 10.1055/s-2005-871746. [DOI] [PubMed] [Google Scholar]
- 111.Kim E S, Hwang J H, Kim K S, Lee S Y. Plantar reconstruction using the medial sural artery perforator free flap. Ann Plast Surg. 2009;62(06):679–684. doi: 10.1097/SAP.0b013e3181835abf. [DOI] [PubMed] [Google Scholar]
- 112.Pyon J K, Ha B J, Hyun W S. Sural vessels as recipient vessels for free flap transfer to the single vessel leg. J Korean Soc Plast Reconstr Surg. 1999;26:366–371. [Google Scholar]
- 113.Beumer J D, Karoo R, Caplash Y, Semmler J G, Taylor J. The medial sural artery as recipient vessel and the impact on the medial gastrocnemius. Ann Plast Surg. 2011;67(04):382–386. doi: 10.1097/SAP.0b013e318209a761. [DOI] [PubMed] [Google Scholar]
- 114.Morelli Coppola M, Brunetti B, Ciarrocchi S, Tenna S, Persichetti P. Reconstruction of the posterior compartment of the leg with functional free latissimus dorsi flap to the medial sural neurovascular pedicle. Ann Plast Surg. 2021;86(06):731–733. doi: 10.1097/SAP.0000000000002531. [DOI] [PubMed] [Google Scholar]
- 115.Baliarsing A, Date S, Ciudad P. Medial sural artery as a salvage recipient vessel for complex post traumatic microvascular lower limb reconstruction. Microsurgery. 2018;38(02):157–163. doi: 10.1002/micr.30158. [DOI] [PubMed] [Google Scholar]
- 116.Trapero A, Pérez-García A, Thione A, Sánchez-García A, Ruiz-Valls A. Use of medial sural vessels as recipient vessels in a previous gastrocnemius flap. Ann Plast Surg. 2020;85(03):333–334. doi: 10.1097/SAP.0000000000002438. [DOI] [PubMed] [Google Scholar]
- 117.Smith M L, Molina B J, Dayan E, Kim J N, Kagen A, Dayan J H. Use of distal medial sural vessels as recipient vessels in free tissue transfer. J Reconstr Microsurg. 2017;33(01):59–62. doi: 10.1055/s-0036-1588016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Hallock G G. Sequential use of a true perforator flap and its corresponding muscle flap. Ann Plast Surg. 2003;51(06):617–620. doi: 10.1097/01.SAP.0000067960.70364.83. [DOI] [PubMed] [Google Scholar]