

Abstract
Anal squamous cell carcinoma (SCC) is rare, but it has been commonly detected as an invasive cancer. The standard treatment for anal SCC was surgical resection. However, recent medical advances have enabled the standard treatment to be chemoradiotherapy. Anal intraepithelial neoplasia (AIN) is a premalignant lesion of SCC. The screening test for AIN and human papilloma virus vaccine are important for the following high-risk patients: patients positive for human immunodeficiency virus and men who have sexual intercourse with men. Although cytology can be easily applied for a screening test, the false-negative rate for AIN is high. Instead, high-resolution anoscopy (HRA) has been gaining attention as a promising screening method for high-risk patients. Investigations comparing characteristic findings of HRA with the histology of AIN have demonstrated that HRA is a highly specific test for AIN.
Magnifying or image-enhanced endoscopies are also routinely used for colonoscopy, as they allow detailed observations at higher magnifications than those of HRA. Hence, these endoscopic modalities can be applied for assessing AIN. Ablation therapies or topical medications are available as the local treatment for AIN. Although endoscopic submucosal dissection is considered to be feasible to remove AIN, it has a technical difficulty to approach endoscopically invisible areas. Hence, this technique may be useful to resect AIN localized in the endoscopically visible areas, when the localization is confirmed via targeted biopsy.
Keywords: anal intraepithelial neoplasia, squamous cell carcinoma, clinical management
Introduction
In the anal canal, the interanal space has been considered as a tubular area from the puborectal muscle attachment to the anal verge. Therefore, anal canal carcinoma includes the following pathological types: (a) rectal adenocarcinoma arising from the mucosa of the rectal part of the anal canal, (b) squamous cell carcinoma (SCC) from the epithelium of the anal canal, (c) anal adenocarcinoma from the anal glands, and (d) hemorrhoidal carcinoma from their conduits. Malignant tumors originating from the anal canal account for only 1%-2% of all colorectal cancers[1]. The most common pathological type of anal canal malignant tumors is adenocarcinoma (78.3%), followed by SCC (18%) according to the report on the registration system of the Japanese Society for the Cancer of the Colon and Rectum. Conversely, SCC has been determined as the most common type of anal canal cancer, accounting for 80%-85% of all anal canal cancers in Western countries[1-3]. For squamous cell carcinoma (SCC), the risk factors for its precursor lesions have been clarified, and clinical management has already been reported mainly in Western countries. Thus, in this article, we will focus on intraepithelial neoplasia, which are considered to be precursor lesions of SCC.
Currently, the standard treatment for SCC of the anal canal is radiation chemotherapy[4,5], as few lesions may be detected at the stage of intraepithelial carcinoma or anal intraepithelial neoplasia (AIN). Recent endoscopic advances have been enabling endoscopic therapeutic approaches for intraepithelial carcinoma and AIN, which are considered to have a very low risk of metastasis. Several case reports of its endoscopic resection have been published[6-8]. However, data as regards the feasibility of its endoscopic resection has remained to be lacking. Therefore, endoscopic resection can be considered if the lesions have no or very low metastatic risk. This work discusses the clinical features of AIN and the future possibilities for its diagnosis and treatment.
Risk Factors and Prevention of AIN
The crucial risk factors for AIN include human papilloma virus (HPV), certain sexual behaviors, and human immunodeficiency virus (HIV)[9-12]. Its association with HPV is of particularly high importance. Approximately 80%-90% of SCCs in the anal canal have been associated with HPV[13-15]. SCC can develop via persistent infection and precursor lesions of HPV. More than 100 different types of HPV have been discovered in humans, and several types can infect the skin and the mucous membranes. While anal SCC is caused by HPV-16 or HPV-18[13,15], anal condyloma, which is a variant of LSILs, has been associated with HPV-6 and HPV-11[9].
In Japan, a recombinant adsorbed quadrivalent HPV-like particle vaccine (yeast origin) was approved for preventing HPV-associated diseases in August 2011. It is indicated for the prevention of cervical cancer and its precursor lesions, vulvar intraepithelial tumors, vaginal intraepithelial tumors, and condyloma acuminatum in women aged 9 years and older. In light of the significance of prophylaxis in males, vaccination in males was later approved in December 2020. The new indication also includes anal squamous cell carcinoma and its precursor lesions. A large, randomized, double-blinded study assessed the efficacy of the quadrivalent HPV vaccine for male patients with AIN who have sexual intercourse with men and revealed that the vaccine was able to reduce the incidence of genital warts in young men[16]. This study also demonstrated that the efficacy of the vaccine for preventing AIN was 50.3% (95% confidence interval [CI], 25.7-67.2) in the intention-to-treat population; furthermore, in the per-protocol efficacy population, its efficacy for preventing AIN was 77.5% (95% CI, 39.6-93.3).
Statements regarding safety for HPV vaccines have been issued by the World Health Organization, Centers for Disease Control and Prevention, European Medicines Agency, and French National Agency for Medicines and Health Products Safety[17-19]. The European Medicines Agency statement addresses that the current evidence does not support the association between HPV vaccines and causes complex regional pain syndrome or postural orthostatic tachycardia syndrome. The Agence Nationale de Sécurité du Médicament (ANSM) statement has cited a study (which examined approximately 2.2 million individuals) that showed the risk of Guillain-Barré syndrome attributable to the vaccination was 1-2 cases per 100,000 vaccinations[20].
HPV vaccination efforts can vary among countries. In some countries, vaccination completion rates exceed 80% because of a high awareness of cervical cancer prevention. However, Japanese data in 2018 reported that the vaccination rate is only 0.8%, which is extremely lower than the rate in Western countries. HPV vaccination plays an important role in preventing cervical cancer. Given that an age-adjusted incidence of anal cancer in Japan has been increasing since 1990[21], the implementation of HPV vaccines is an issue that needs to be addressed from the perspective of anal SCC prevention. In October 2020, the Ministry of Health, Labour and Welfare asked local governments to ensure that those eligible for routine HPV vaccination are informed through individual notifications about cervical cancer and the vaccine. Furthermore, the “active recommendation for vaccination,” which had been suspended since June 2013, was practically resumed. Along with monitoring of the safety of the HPV vaccine, its widespread use is expected.
Screening and Diagnosis for AIN
Screening has been recommended for early detection of AIN and prevention of anal SCC. An anal Pap smear should be performed for patients identified to be at high-risk for AIN such as immunocompromised individuals or men having sex with men (MSM)[22-24]. If atypical cells are detected in the Pap smear, high-resolution anoscopy (HRA) with magnifying observation of the anal canal and tissue biopsy are recommended. HRA uses a colposcope or operating microscope with acetic acid and Lugol's solution and is known to provide a high-power view of the squamocolumnar junction of the lower rectum and anus[25-27]. Using the vital stain method, abnormal epithelial or vascular findings can be distinct from normal tissues during examination.
Characteristics of LSILs and HSILs are listed in Table 1[28]. Considering these findings, vessel findings seem to be crucial for the detection and characterization of AIN. Magnifying endoscopy is a novel method of observing vessel findings because of its optical properties. Magnification power of endoscopy is higher than that of HRA, and its focus is adjustable according to the observation conditions. When endoscopy identifies abnormal findings, target biopsy can be performed as well. Image-enhanced endoscopy, such as narrowband imaging (NBI) and blue laser/light imaging, can visualize not only microvessels of the tumor surface by using wavelengths strongly absorbed by hemoglobin but also its surface patterns using a structure enhancement function[29,30]. Given that endoscopy has such advantages to evaluate vessel and surface patterns of the tumor in detail, it may have a better diagnostic performance compared with HRA and can be used to assess AIN as well. Although endoscopy may have some limitations to observe narrow areas such as the anal canal, the squamocolumnar junction can be sufficiently observed via insufflation and retroflexion technique. Furthermore, tip attachment makes an observation of the anal canal possible.
Table 1.
Morphological Features of LSIL, HSIL, and Squamous Cell Carcinoma as Observed Using High-resolution Anoscopy.
| LSIL | HSIL | Cancer | |
|---|---|---|---|
| Color | Acetowhite, shiny, barely visible, or distinct | Flat acetowhite, matted tone, gray | Thick acetowhite, red, or cannot be assessed because of friability |
| Contour | Flat, thin, raised or thickened, warty papillae, micropapillae | Flat, thickened, eroded, atypical papillae, ulcerations | Thickened, raised, eroded, friable ulcerations, growths |
| Vessels | Warty, looped capillary, punctation, striated, fine increased vascularity, fine mosaic pattern (rare) | Coarse mosaic, coarse punctuation, atypical vessels, variable dilations, friable | Very coarse, atypical or abnormal vessels with bizarre shapes, wide variability in dilations, friable |
| Epithelial changes | Lacy metaplasia, atypical clustered glands, honeycombing |
HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion.
Image-enhanced endoscopy can be used to evaluate vascular patterns more precisely in comparison to HRA. The NBI findings of AIN are similar to magnified endoscopic patterns of superficial esophageal cancer (Figure 1)[31]. Indeed, several case reports revealed that AIN can share the following findings, which are observed in esophageal carcinoma: microvessels with dilatation, tortuosity, caliber changes, and uneven shapes. Hence, it may be feasible to apply the endoscopic classification of the Japan Esophageal Society in order to determine the extent and depth of AIN[32,33]. Future studies with larger sample size are warranted to understand its diagnostic accuracy for AIN.
Figure 1.

Anal intraepithelial neoplasia in the anal transition zone. Recognized as a flat elevated lesion with nodular elevation with mild reddish color with white-light observation (a). Irregular microvessel patterns similar to superficial esophageal carcinoma are recognized using narrowband imaging (b-d).
Pathological Definition of AIN
AIN is a premalignant lesion of SCC. The lesion commonly appears at the anal transition zone (ATZ), where the rectal columnar epithelium meets the anal squamous epithelium. This lesion has been considered to be associated with HPV. The Lower Anogenital Squamous Terminology Standardization (LAST) project for HPV-associated lesions has provided guidelines for unified nomenclature[34]. The latest guidelines have accurately reflected the biology of HPV-related lesions and provided a two-tiered approach to low-grade intraepithelial lesions (LSILs) and high-grade intraepithelial lesions (HSILs). For many years, HPV-associated dysplasia of the anogenital tract, including the anus, was classified by three-tiered nomenclature (i.e., AIN1-3). However, the LAST published in 2012 recommended a two-tiered nomenclature, designated as LSIL or HSIL. In the anal canal, LSIL corresponds to anal intraepithelial neoplasia (AIN-1) or anal condyloma, while HSIL corresponds to AIN-2 and AIN-3 (Table 2).
Table 2.
The Two-tiered Nomenclature for Anal Intraepithelial Lesions.
| LSIL | HSIL | ||
|---|---|---|---|
| Condyloma | AIN grade I | AIN grade II | AIN grade III |
| Very mild to mild dysplasia | Moderate
dysplasia |
Severe
dysplasia/ carcinoma in situ |
|
AIN, anal intraepithelial neoplasia; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion.
Histologically, LSIL shows cytological atypia limited to the lower third of the epithelium and associated with koilocytosis, which is characterized by nuclear atypia and perinuclear halos. HSIL often exhibits involvement of at least two-thirds or more of the epithelial layer by markedly atypical cells. HSILs involve the entire epithelium or the lower two-thirds and are typified by a loss of maturation, nuclear hyperchromasia, and membrane irregularity, as well as an increase in the nucleus-to-cytoplasm ratio. HSILs typically show strong and diffuse nuclear and cytoplasmic p16 expression by immunohistochemical staining (Figure 2)[35,36].
Figure 2.

Microscopic images of low- (a, b) and high- (c, d) grade squamous intraepithelial lesions. Low-grade dysplasia shows atypical squamous cells with enlarged nuclei confined to the lower layer (a). The p16 staining shows scattered positive cells with weak to moderate staining (b). Atypical squamous cells occupy the entire epithelial layers (c). Diffuse, strong positive expression of p16 (d).
Local Treatments of AIN
In terms of local treatment for AIN, fulguration with electrocautery during HRA or anoscopy has been reported as a treatment option. Chang et al. reported that 8 HIV-negative patients did not develop recurrent lesions, whereas 23 of 29 HIV-positive patients had persistent or recurrent high-grade squamous intraepithelial lesions after the procedure[37]. Goldstone et al. assessed clinical outcomes of infrared coagulation for AIN, an outpatient procedure, and showed that 40 patients (53%) developed postoperative recurrence[37]. In this study, local recurrence was retreated with coagulation therapy. The probability of successfully treating an individual lesion after the first infrared coagulation procedure was 81% and 93% when local recurrence was retreated. HIV-positive patients were found to be twice as likely to have persistent lesions and 1.7-times more likely to develop local recurrence[38]. These studies reported no serious adverse events such as anal stenosis requiring surgical anastomosis.
Topical therapy is an alternative treatment option. The known topical agents include trichloroacetic acid (TCA), imiquimod, and 5-fluorouracil (5FU)[39-41]. TCA demonstrated the most favorable outcomes to resolve AINs to normal or LSIL pathology. Cranston et al. reported that 77 (78.6%) of 98 HSILs treated with TCA resolved to normal epithelium or LSIL during follow-up[39]. Once HRA identifies lesions, TCA can be applied during the examination, and specific serious adverse events have not been reported. Imiquimod and 5FU have also been reported as effective topical agents with clearance rates ranging from 40% to 60%; however, pain and anal burning were occasionally reported in patients using imiquimod and perianal irritation in patients using 5FU.
Given the effectiveness and safety of ablation therapies or topical medications for AIN, it is understandable that these are selected for the local treatment of AIN. However, from the standpoint of gastrointestinal endoscopists, especially considering the basic concept of endoscopic submucosal dissection for gastrointestinal tumors, the incidence of postoperative local recurrence of AIN is deemed to be relatively high. In case of gastrointestinal tumors, it is important to achieve a reliable cure using en bloc resection of the lesion and accurately determine the negative margins of resected lesions. With regard to AIN, case reports have shown that endoscopic findings of every single lesion may be heterogeneous, suggesting the need for en bloc resection and accurate histopathological evaluation of the lesion, as the endoscopic intervention of gastrointestinal tumors[8]. Several Japanese studies have demonstrated the effectiveness of endoscopic submucosal dissection as a local excision for AIN and noninvasive SCC, which are considered to have a very low risk of metastasis[6-8]. In our own experience, the tumors can spread to endoscopically invisible areas[8]. Therefore, it may be difficult to accurately determine the extent of lesions and achieve R0 resection despite wide resection, which can often cause adverse events such as post-treatment pain and stenosis. From our perspectives, endoscopic submucosal dissection may be useful to resect AIN localized in endoscopically visible areas including the anal transitional zone or lower rectum (Figure 3).
Figure 3.
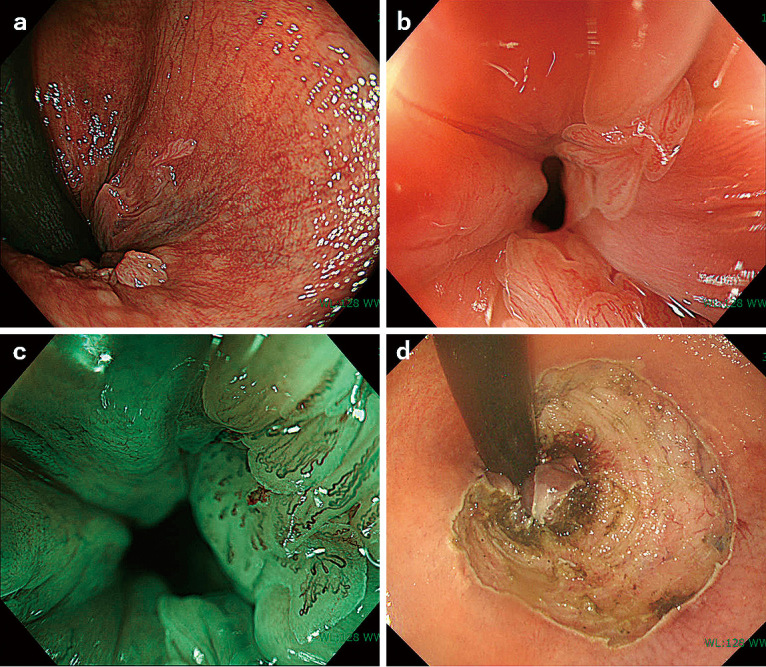
Intraepithelial neoplasia located between the anal canal and anal transition zone (ATZ) resected using the endoscopic submucosal dissection technique. Small or tiny lesions are scattered discontinuously in the anal canal and ATZ (a). Magnifying narrowband observations showed irregular vessel pattern similar to superficial esophageal carcinoma (b, c). Considering the localization of the lesion in the anal canal, a certain area visible as definite lesion was continuously resected by endoscopic submucosal dissection (d).
In terms of treatment for SCC, chemoradiation therapy is recommended as the first-line treatment. However, some early and late adverse events (e.g., skin dermatitis, proctitis, hematologic toxic effects, incontinence, fecal urgency, etc.) are adverse events that cannot be ignored. As for endoscopic or surgical local excision, complications were noted, such as pain and bleeding in the short term and stenosis in the long term. However, the long-term and systemic complications are relatively less severe than those of chemoradiotherapy. Therefore, endoscopic local resection may be applicable for intraepithelial cancers that are considered to have no metastatic risk, and a clinical research plan to expand treatment options is thus expected.
Conclusions
AIN is a precursor lesion of anal SCC. Although it is considered a rare lesion, it can be detected during colonoscopy screening because of the improved capabilities of endoscopic equipment. Magnifying or image-enhanced endoscopies such as NBI and blue laser/light imaging may be useful for AIN detection and diagnosis. However, there is no evidence to determine the optimal diagnostic and therapeutic strategy. Therefore, appropriate guidelines for AIN must be needed to understand which local treatments can be applied or which examination is the best to determine the extent of the lesion, when the localization is confirmed via target biopsy.
Conflicts of Interest
There are no conflicts of interest.
Author Contributions
Taku Sakamoto: Conceptualization, methodology, data curation, investigation, and writing of the original draft.
Shintaro Akiyama: Assistance in preparing the original draft, critical revision, and editing of the manuscript.
Shigeki Sekine and Yutaka Saito: Resources (images), critical revision, and editing of the manuscript.
Toshiaki Narasaka and Hideo Suzuki: Critical revision and editing of the manuscript.
Kiichiro Tsuchiya: Critical revision, editing of the manuscript, and project administration.
Approval by Institutional Review Board (IRB)
No approval from any IRB was required because this review article was based on previously published papers.
Disclaimer
Yutaka Saito is one of the Associate Editors of Journal of the Anus, Rectum and Colon and on the journal's Editorial Board. He was not involved in the editorial evaluation or decision to accept this article for publication at all.
References
- 1.Inatsugi N. The recent trend of malignant tumors of the anal canal in Japan. J Anus Rectum Colon. 2008 Oct; 61(10): 967-70. [Google Scholar]
- 2.Scholefield JH, Castle MT, Watson NF. Malignant transformation of high-grade anal intraepithelial neoplasia. Br J Surg. 2005 Sept; 92(9): 1133-6. [DOI] [PubMed] [Google Scholar]
- 3.Watson AJ, Smith BB, Whitehead MR, et al. Malignant progression of anal intra-epithelial neoplasia. ANZ J Surg. 2006 Aug; 76(8): 715-7. [DOI] [PubMed] [Google Scholar]
- 4.Epidermoid anal cancer: results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. UKCCCR Anal Cancer Trial Working Party. UK Co-ordinating Committee on Cancer Research. Lancet. 1996 Oct; 348(9034): 1049-54. [PubMed] [Google Scholar]
- 5.Bartelink H, Roelofsen F, Eschwege F, et al. Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J Clin Oncol. 1997 May; 15(5): 2040-9. [DOI] [PubMed] [Google Scholar]
- 6.Chou YP, Saito Y, Matsuda T, et al. Novel diagnostic methods for early-stage squamous cell carcinoma of the anal canal successfully resected by endoscopic submucosal dissection. Endoscopy. 2009 Oct; 41(Suppl 2): E283-5. [DOI] [PubMed] [Google Scholar]
- 7.Oono Y, Fu K, Nakamura H, et al. Narrowband imaging colonoscopy with a transparent hood for diagnosis of a squamous cell carcinoma in situ in the anal canal. Endoscopy. 2010 Dec; 42(Suppl 2): E183-4. [DOI] [PubMed] [Google Scholar]
- 8.Kasuga K, Saito Y, Wu SYS, et al. Impact of endoscopic submucosal dissection of an anal squamous intraepithelial lesion with indistinct border. Endoscopy. 2020 Feb; 52(2): E75-7. [DOI] [PubMed] [Google Scholar]
- 9.Dempsey AF. Human papillomavirus: the usefulness of risk factors in determining who should get vaccinated. Rev Obstet Gynecol. 2008; 1(3): 122-8. [PMC free article] [PubMed] [Google Scholar]
- 10.Dindo D, Nocito A, Schettle M, et al. What should we do about anal condyloma and anal intraepithelial neoplasia? Results of a survey. Colorectal Dis. 2011 Jul; 13(7): 796-801. [DOI] [PubMed] [Google Scholar]
- 11.Long KC, Menon R, Bastawrous A, et al. Screening, surveillance, and treatment of anal intraepithelial neoplasia. Clin Colon Rectal Surg. 2016 Mar; 29(1): 57-64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Crawshaw BP, Russ AJ, Stein SL, et al. High-resolution anoscopy or expectant management for anal intraepithelial neoplasia for the prevention of anal cancer: is there really a difference? Dis Colon Rectum. 2015 Jan; 58(1): 53-9. [DOI] [PubMed] [Google Scholar]
- 13.De Vuyst H, Clifford GM, Nascimento MC, et al. Prevalence and type distribution of human papillomavirus in carcinoma and intraepithelial neoplasia of the vulva, vagina and anus: a meta-analysis. Int J Cancer. 2009 Apr; 124(7): 1626-36. [DOI] [PubMed] [Google Scholar]
- 14.Parkin DM. The global health burden of infection-associated cancers in the year 2002. Int J Cancer. 2006 Jun; 118(12): 3030-44. [DOI] [PubMed] [Google Scholar]
- 15.Medford RJ, Salit IE. Anal cancer and intraepithelial neoplasia: epidemiology, screening and prevention of a sexually transmitted disease. CMAJ. 2015 Feb; 187(2): 111-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Palefsky JM, Giuliano AR, Goldstone S, et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N Engl J Med. 2011 Oct; 365(17): 1576-85. [DOI] [PubMed] [Google Scholar]
- 17.World Health Organization. Human papillomavirus vaccines: WHO position paper. Weekly Epidemiological Record. 2017 May; 92(19): 241-68. [Google Scholar]
- 18.Meites E, Szilagyi PG, Chesson HW, et al. Human papillomavirus vaccination for adults: updated recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep. 2019 Aug; 68(32): 698-702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zureik M, Dray-Spira R, Miranda S, et al. Vaccins anti-HPV et risque de maladies autoimmunes: étude pharmacoépidémiologique. Rapport CNAM/ANSM. 2015 Sep. [Google Scholar]
- 20.Miranda S, Chaignot C, Collin C, et al. Human papillomavirus vaccination and risk of autoimmune diseases: a large cohort study of over 2 million young girls in France. Vaccine. 2017 Aug; 35(36): 4761-8. [DOI] [PubMed] [Google Scholar]
- 21.Forman D, de Martel C, Lacey CJ, et al. Global burden of human papillomavirus and related diseases. Vaccine. 2012 Nov; 30(Suppl 5): F12-23. [DOI] [PubMed] [Google Scholar]
- 22.Chin-Hong PV, Palefsky JM. Natural history and clinical management of anal human papillomavirus disease in men and women infected with human immunodeficiency virus. Clin Infect Dis. 2002 Nov; 35(9): 1127-34. [DOI] [PubMed] [Google Scholar]
- 23.Cranston RD, Darragh TM, Holly EA, et al. Self-collected versus clinician-collected anal cytology specimens to diagnose anal intraepithelial neoplasia in HIV-positive men. J Acquir Immune Defic Syndr. 2004 Aug; 36(4): 915-20. [DOI] [PubMed] [Google Scholar]
- 24.Chin-Hong PV, Berry JM, Cheng SC, et al. Comparison of patient- and clinician-collected anal cytology samples to screen for human papillomavirus-associated anal intraepithelial neoplasia in men who have sex with men. Ann Intern Med. 2008 Sep; 149(5): 300-6. [DOI] [PubMed] [Google Scholar]
- 25.Berry JM, Palefsky JM, Jay N, et al. Performance characteristics of anal cytology and human papillomavirus testing in patients with high-resolution anoscopy-guided biopsy of high-grade anal intraepithelial neoplasia. Dis Colon Rectum. 2009 Feb; 52(2): 239-47. [DOI] [PubMed] [Google Scholar]
- 26.Dalla Pria A, Alfa-Wali M, Fox P, et al. High-resolution anoscopy screening of HIV-positive MSM: longitudinal results from a pilot study. AIDS. 2014 Mar; 28(6): 861-7. [DOI] [PubMed] [Google Scholar]
- 27.Botes LP, Pett S, Carr A, et al. Anal cytological abnormalities are poor predictors of high-grade intraepithelial neoplasia amongst HIV-positive men who have sex with men. Sex Health. 2013 Mar; 10(1): 9-17. [DOI] [PubMed] [Google Scholar]
- 28.Jay N. High-resolution anoscopy: procedure and findings. Semin Colon Rectal Surg. 2017 Jun; 28(2): 75-80. [Google Scholar]
- 29.Gono K, Obi T, Yamaguchi M, et al. Appearance of enhanced tissue feature in narrow-band endoscopic imaging. J Biomed Opt. 2004 May; 9(3): 568-77. [DOI] [PubMed] [Google Scholar]
- 30.Muto M, Katada C, Sano Y, et al. Narrow band imaging: a new diagnostic approach to visualize angiogenesis in superficial neoplasia. Clin Gastroenterol Hepatol. 2005 Jul; 3(7 Suppl 1): S16-20. [DOI] [PubMed] [Google Scholar]
- 31.Oyama T, Inoue H, Arima M, et al. Prediction of the invasion depth of superficial squamous cell carcinoma based on microvessel morphology: magnifying endoscopic classification of the Japan Esophageal Society. Esophagus. 2017 Apr; 14(2): 105-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kuwano H, Nishimura Y, Oyama T, et al. Guidelines for diagnosis and treatment of carcinoma of the esophagus April 2012 edited by the Japan Esophageal Society. Esophagus. 2015 Jan; 12(1): 1-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ishihara R, Mizusawa J, Kushima R, et al. Assessment of the diagnostic performance of endoscopic ultrasonography after conventional endoscopy for the evaluation of esophageal squamous cell carcinoma invasion depth. JAMA Netw Open. 2021 Sep; 4(9): e2125317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Darragh TM, Colgan TJ, Cox JT, et al. The Lower Anogenital Squamous Terminology Standardization Project for HPV-Associated Lesions: background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Arch Pathol Lab Med. 2012 Oct; 136(10): 1266-97. [DOI] [PubMed] [Google Scholar]
- 35.Abbasakoor F, Boulos PB. Anal intraepithelial neoplasia. Br J Surg. 2005 Mar; 92(3): 277-90. [DOI] [PubMed] [Google Scholar]
- 36.Zhang G, Yang B, Abdul-Karim FW. p16 immunohistochemistry is useful in confirming high-grade squamous intraepithelial lesions (HSIL) in women with negative HPV testing. Int J Gynecol Pathol. 2015 Mar; 34(2): 180-6. [DOI] [PubMed] [Google Scholar]
- 37.Chang GJ, Berry JM, Jay N, et al. Surgical treatment of high-grade anal squamous intraepithelial lesions: a prospective study. Dis Colon Rectum. 2002 Apr; 45(4): 453-8. [DOI] [PubMed] [Google Scholar]
- 38.Goldstone SE, Hundert JS, Huyett JW. Infrared coagulator ablation of high-grade anal squamous intraepithelial lesions in HIV-negative males who have sex with males. Dis Colon Rectum. 2007 May; 50(5): 565-75. [DOI] [PubMed] [Google Scholar]
- 39.Cranston RD, Baker JR, Liu Y, et al. Topical application of trichloroacetic acid is efficacious for the treatment of internal anal high-grade squamous intraepithelial lesions in HIV-positive men. Sex Transm Dis. 2014 Jul; 41(7): 420-6. [DOI] [PubMed] [Google Scholar]
- 40.van der Snoek EM, den Hollander JC, van der Ende ME. Imiquimod 5% cream for five consecutive days a week in an HIV-infected observational cohort up to 32 weeks in the treatment of high-grade squamous intraepithelial lesions. Sex Transm Infect. 2015 Jun; 91(4): 245-7. [DOI] [PubMed] [Google Scholar]
- 41.Stier EA, Goldstone SE, Einstein MH, et al. Safety and efficacy of topical cidofovir to treat high-grade perianal and vulvar intraepithelial neoplasia in HIV-positive men and women. AIDS. 2013 Feb; 27(4): 545-51. [DOI] [PMC free article] [PubMed] [Google Scholar]