

Abstract
Although a substantial body of work has investigated drivers of tie formation, there is growing interest in understanding why relationships decay or dissolve altogether. The networks literature has tended to conceptualize tie decay as driven by processes similar to those underlying tie formation. Yet information that is revealed through ongoing interactions can exert different effects on tie formation and tie decay. This paper investigates how tie decay and tie formation processes differ by focusing on contentious practices. To the extent that information about dissimilarities in contentious practices is learned through ongoing interactions, it can exert diverging effects on tie formation and tie decay. Using a longitudinal data set of 141,543 physician dyads, we find that differences in contentious prescribing led ties to weaken or dissolve altogether but did not affect tie formation. The more contentious the practice and the more information available about the practice, the stronger the effect on tie decay and dissolution. Collectively, these findings contribute to a more nuanced understanding of relationship evolution as an unfolding process through which deeper-level differences are revealed and shape the outcome of the tie.
Keywords: tie decay, tie dissolution, network evolution, contentious practices, physicians, prescription drug epidemic
How do networks evolve? An extensive line of sociological inquiry has focused on tie formation. This work has found a strong tendency for people to form relationships based on shared attributes such as socioeconomic status, gender, race, age, geographic propinquity, and shared social foci (Keller 1952, Lazarsfeld and Merton 1954, Festinger et al. 1963, McPherson et al. 2001, Ibarra 2006, Kossinets and Watts 2009, Kleinbaum et al. 2013). However, focusing solely on tie formation provides an incomplete picture of how networks evolve. As Ahuja et al. (2012) summarized, network evolution is fundamentally driven by microinteractions between actors “to form, maintain, or dissolve ties” (p. 446). An emerging area of research has begun to look beyond tie formation by examining tie dormancy and revival (Levin et al. 2011), network churn (Sasovova et al. 2010), and tie decay and dissolution (Dahlander and McFarland 2013, Kleinbaum 2018).
Although the field has gradually shifted to exploring tie decay and dissolution, it has tended to focus on many of the same drivers that have been found to shape tie formation—most notably homophily on readily observable characteristics. Homophily in race, age, and other sociodemographic traits that are key to tie formation has also been found to impede tie decay (Tuma and Hallinan 1979, Hallinan and Williams 1989, Popielarz and McPherson 1995, Burt 2000). These parallel findings have frequently prompted scholars to conceptualize decay as following a similar process as tie formation. As summarized by McPherson et al. (2001, p. 436), “The patterns of tie dissolution mimic those of tie formation, but perhaps in a somewhat weaker manner.” Yet how tie decay processes differ from tie formation remains a key issue in networks research (Lewis 2015).
We argue that recognizing relationships as an unfolding process—in which different types of information become revealed at different stages of the relationship—can help us better appreciate how tie formation and tie decay processes might differ. In tie formation, individuals are drawn together by a confluence of shared social foci as well as similarity on readily observable social traits. It reflects a process of two unfamiliar individuals seeking similarity based on the available information they have, often limited to visible traits such as race, gender, and age or easily accessible information such as profession. This may partially explain why homophily on ascribed and readily observable social characteristics is one of the most extensively documented drivers of tie formation. Once a relationship is formed, however, whether individuals will subsequently strengthen, weaken, or end their relationships likely depends on whether they reach agreement on norms and practices. Similarity in attitudes, beliefs, and practices, which Lazarsfeld and Merton (1954) refer to as value homophily, often only becomes available through social interactions as relationships gradually move into deeper levels of exchange (Altman and Taylor 1973).
Drawing on insights from a long tradition of work on the importance of shared norms and practices in interpersonal relationships (Argyle and Henderson 1984, Duck 2007), we argue that differences in norms and practices can have the potential to guide our choice of relationship partners. Divergences in practices may be particularly salient when the practice is contentious, in which case stark differences may be harder to reconcile because they reveal deeper moral divergences. We investigate the impact of dissimilarities in contentious practices on tie decay and dissolution, as well as tie formation. Divergence on contentious practices is likely not readily known before a relationship exists but is revealed and learned as the relationship unfolds. The asymmetry in information is put succinctly in work speculating about interpersonal relationships: “Two strangers cannot be incompatible. Before there is friction, there must be interconnections between two people’s behaviors” (Blumstein and Kollock 1988, p. 483). In support of this expectation, we find that divergence in contentious behaviors prompts individuals to weaken their relationships (tie decay) or even drop their ties altogether (tie dissolution). The more contentious the practice, the stronger the effect dissimilarities have on tie decay and dissolution. By contrast, dyadic differences in contentious practices do not impede tie formation.
We also distinguish between whether preexisting ties strengthen or weaken (tie decay) as well as whether they exist or are dropped altogether (tie dissolution). The literature has tended to treat ties as a binary construct by focusing on their presence and absence. However, meaningful differences may undergird tie formation and decay processes. Whereas tie dissolution—when relationships come to a complete end—can be prompted when individuals discover stark, irreconcilable differences, tie decay—a weakening in the relationship—can occur when the discovered differences outweigh the strong social inertia holding the relationship in place. We examine both the persistence of relationships and their strength. Comparing norm-violating practices that differ in how morally contentious they are, we find that the more contentious the practice, the higher the odds the tie will disappear entirely. This finding highlights the need to make the distinction between decay and dissolution.
Our paper contributes to the network evolution literature by showing important ways in which tie formation, decay, and dissolution differ. Our findings suggest that shared norms and practices often require prior interactions to be discovered and can thus affect tie decay and tie formation differently. Furthermore, our findings shed light on the importance of recognizing relationships as an ongoing process, in which different sources of knowledge and information are exchanged as relationships develop. We also move beyond the binary conceptualization of relationships by examining both tie decay (weakened tie strength) and tie dissolution (loss of the relationship). The finding that tie decay and dissolution differ along the contention of the practice highlights that different social processes are at play. Finally, this paper offers a unique contribution to the networks and professional wrongdoing literature, which frequently examines the emergence of wrongdoing as a consequence of being connected to norm-violating peers, by turning this around and asking how differences in norm-violating practices affect the ties themselves.
Theory
Understanding network evolution requires investigating how relationships form, as well as how they decay and dissolve. The networks literature has directed extensive attention to the antecedents of tie formation. Summarizing this literature, Lewis (2015, p. 1) notes that there are “three mechanisms of network generation that have received particular attention in the literature: homophily, opportunity constraints, and structural balance.” In particular, the principle of homophily—the “tendency for friendships to form between those who are alike in some designated respect” (Lazarsfeld and Merton 1954, p. 23)—has been documented as an omnipresent social force underlying tie formation. Voluminous studies have shown the effect of similarity in ascribed social characteristics such as gender, race, ethnicity, age, education, and occupation on tie formation (Lazarsfeld and Merton 1954, Blau 1977, Verbrugge 1977, McPherson et al. 2001, Ibarra 2006).
Recent years have seen growing attention to another facet of network evolution: tie decay and dissolution. This stream of work has followed in the footsteps of scholarship on tie formation by focusing on homophily on ascribed characteristics. Accumulating studies find that shared sociodemographic traits act as social glue holding preexisting ties in place. For instance, same-race and same-gender friendships among school children are more likely to be sustained than cross-race or cross-gender friendships (Tuma and Hallinan 1979, Hallinan and Williams 1989). Age homophily decreases the probability of tie dissolution between bankers (Burt 2000), and being of similar sociodemographic traits with other team members lowered the group exit rate among professionals (Popielarz and McPherson 1995).
The parallel findings have prompted scholars to draw the preliminary conclusion that tie decay follows a similar pattern as tie formation (McPherson et al. 2001). However, this assumption is worth revisiting. Taking the logic that the same set of factors drive both tie formation and tie decay to the extreme, why would ties that formed dissolve at all? A deeper understanding of the distinction between tie decay and tie formation—the two basic generative process driving network evolution—will help advance the field of network evolution. As reflected in Lewis’ review, one of the fundamental questions that remains in the networks literature is, “how is the process of tie formation different from that of tie maintenance—not to mention tie dissolution?” (Lewis 2015, p. 8).
Recent advances in the literature have shed light on one distinction between tie decay and tie formation. Noting that “some cues are only available after a tie has formed” (Dahlander and McFarland 2013, p. 71), scholars argue that information obtained through the course of the relationship—which is not available to strangers—allows individuals to better assess the benefits they derive from the relationship. The new information induces individuals to drop less valuable ties (Dahlander and McFarland 2013, Kleinbaum 2018). In short, having a history of interaction gives individuals more first-hand information about the returns of their relationship, thereby helping them make more informed tie decay choices.
Dissimilarity in Contentious Practices and Tie Formation, Tie Decay, and Tie Dissolution
Learning is certainly not limited to gains from the relationship. At a fundamental level, the development of a relationship allows individuals to acquire deeper knowledge about how one thinks and behaves. Homophily based on as similarity in attitudes, values, and beliefs—referred to as value homophily by Lazarsfeld and Merton (1954)—is pivotal to relationships: alignment in value homophily increases relationship satisfaction (Coombs 1966), whereas disagreements lead to repulsion (Rosenbaum 1986). Conceptually, value homophily is often thought of as “derivative of social positions themselves” (McPherson et al. 2001, p. 419), reflecting homophily on observable characteristics. Yet the effect of value homophily on relationship evolution likely varies depending on the stage of the relationship. Prior to the existence of a relationship, information about one another is mostly limited to appearances and other readily accessible social characteristics. As described in Dahlander and McFarland (2013, p. 71), the initiation of relationships reflects “two unfamiliar individuals meeting and seeking points of similarity, mostly in appearances and credentials.” The predominant focus on readily observable characteristics in the tie formation literature may partially reflect the lack of deeper knowledge about values and behaviors between strangers. As the relationship unfolds, ongoing interactions allow people to observe and learn about each other’s behaviors and practices, and the degree of alignment in value homophily becomes more evident. Interactions also tend to increase individuals’ trust and willingness to share about their beliefs and practices that are otherwise difficult to observe—as theories of interpersonal relationships predict, as relationships deepen, people gradually move from shallow into deeper levels of exchange (Altman and Taylor 1973). Whereas surface-level variables are overtly identifiable (e.g., age, race, training discipline), deep-level variables underlying psychological states (e.g., personality, attitudes) are discoverable only after interacting with someone (Bell 2007).
The asymmetry in information about one another’s opinions and practices can have quite profound implications for tie decay and tie formation. A long tradition within psychology has theorized that shared norms and practices are fundamental to the development and maintenance of interpersonal relationships (Morton and Douglas 1981, Argyle and Henderson 1984, Blumstein and Kollock 1988, Duck 2007). A breaking of some type of norm “may lead to some kind of disruption, such as the dissolution of a relationship” (Argyle and Henderson 1984, p. 212). The idea that incompatibility in norms and practices has the potential to lead to relationship dissolution is similarly present in Burt’s early work on tie decay, in which he postulated that “people who discover that they do not enjoy one another or cannot work together … disengage in favor of more compatible contacts” (Burt 2000, p. 2).
Nonetheless, once recognized, not all differences in behaviors necessarily lead to tie decay. Relationship evolution is theorized to be accompanied by constant negotiation to reach minimal agreement on norms and practices, the result of which drives the ebb and flow of relationships (Blumstein and Kollock 1988). Drawing from this insight in psychology, we argue that the moral contention of the practice in question likely affects whether differences will be tolerated or result in tie decay. When differences surface, they may be negotiated and reconciled through interactions. However, when stark differences on a highly contentious or norm-violating practice are discovered, it may be harder to reach a common ground and maintain the relationship. Contentious issues often evoke strong emotional or moral responses, as they can reflect deeper ideological divergences. For instance, differences in abiding by professional guidelines may reflect divergence in upholding one’s professional ethics and moral integrity, differences in political support may reflect ideologies toward wealth distribution or environmental issues, and differences in attitudes toward abortion may reflect divergence on ideologies of “pro-choice” or “pro-life.” We would expect that the more contentious (and hence, emotionally charged) the practice in question, the harder it is to come to terms with these differences, leading relationships to decay or dissolve.
Contentious practices offer a particularly fruitful domain to investigate the nature of tie decay and tie formation processes. Importantly, differences in contentious or norm-violating practices may not be revealed or easily observed by others unless a tie is present. Several factors drive this pattern. First, the discomfort and avoidance of discussing divisive and controversial topics (Chen and Berger 2013) and expected feelings of social threat may be strongest between strangers. However, the discomfort may be reduced as people develop a feeling of closeness through social interactions, making it more likely that controversial topics and practices will be broached. Moreover, to the extent that people perceive their own practices to depart from norms, they may have incentives to avoid publicizing their practices until they have established a relationship with others and built trust over the exchange. Finally, many practices may only be learned through close collaborations. For instance, academic fraud is most likely to be uncovered by coauthors, students, or others who have the opportunity to repeatedly observe the scientists’ work (Stroebe et al. 2012).
Although there is a body of work examining the consequence of experiencing divergences of norm-violating practices, it primarily focuses on social influence as the mechanism to reach a psychological resolution. Social influence can lead the “innocent” to become co-opted (Ashforth and Anand 2003, Nash et al. 2013, Palmer and Moore 2016). Rather than ending a relationship, for example, an employee may convince their coworker that theft is justified and acceptable, eventually convincing the coworker to join (Chan et al. 2019). At the extreme, what was once perceived as a norm violation can permeate through social interactions and become entrenched within the entire organization, a phenomenon termed as “the normalization of deviance” (Vaughan 1996, p. 77).
Disengaging and searching for more compatible contacts instead is another viable option. Distancing oneself from the perceived offender may be an easier route than reporting the practice, having an overt confrontation, or succumbing to peer influence and becoming co-opted. To the extent that differences in contentious practices are revealed and learned over the course of the relationship, such dissimilarities can push preexisting relationships to weaken or completely dissolve. However, they do not necessarily impede tie formation, given that the differences have yet to be revealed. Similarities on surface-level, observable dimensions may create (sometimes inaccurate) expectations of deeper-level similarities on beliefs and actual practices. When these expectations are revealed to be erroneous, ties decay. We summarize the asymmetrical effect of differences in contentious practice on tie formation and decay in the first hypothesis.
Hypothesis 1. Dyadic dissimilarity in contentious practices will have positive effects on tie decay but will have no effect on tie formation.
Once a relationship is formed, how readily each party learns of the other’s norm-violating practice also depends on how salient the practice is within that relationship. Differences are likely to be revealed if the nature of the relationship makes the practice more relevant and provides more opportunities to learn about it. For instance, one is more likely to discover violations of company policies of their coworker than of their neighbor (even if they have a close relationship with their neighbor), because the nature of their tie allows close interactions to observe the practice in question. To give another example, academics who collaborate on quantitative projects are more likely to learn about differences in opinions about p-hacking. Although the collaboration will likely help reveal differences in standards of quantitative analyses, collaborators do not necessarily learn the others’ standards of good qualitative analyses. Therefore, if the mechanism driving tie decay is the revelation of information, then dyads with more relevant and salient information specific to that practice should experience stronger effects. We thus predict that in a dyadic exchange, information salience of the practice moderates whether dissimilarity on that dimension leads to tie decay.
Hypothesis 2. The positive effect of practice dissimilarity on tie decay is moderated by the salience of information between a dyad.
We also seek to understand the effects of dissimilarity in contentious practices on tie decay (weakening of the tie) as well as tie dissolution (complete tie loss). Empirical work has largely been focused on the latter process, as illustrated in studies of the persistence of relationships between academics (Dahlander and McFarland 2013), professionals (Burt 2002, Jonczyk et al. 2016), adolescents (DeLay et al. 2013), and MBA students (Kleinbaum 2018). This binary conceptualization of relationships, which may be partly driven by data constraints, reflects the predominant framework in the networks literature that operationalizes relationships as having only two states: existent and nonexistent. In effect, it simplifies the study of tie decay to the persistence of relationships.
Examining both tie decay and tie dissolution processes is fruitful because more complex dynamics drive the ebb and flow of relationships. The conceptualization of tie strength as varying on a continuous spectrum recognizes that differences may lead relationships to decay in strength rather than end abruptly. The distinction between tie decay and dissolution may be particularly helpful when we consider the impact of practices that vary in their moral contention. When a practice deviates from formal guidelines or intended outcomes but is ambiguous in their moral implications, there may be more ambiguity and tolerance surrounding that behavior. To give a few examples, practices such as financial reporting errors, academic retractions as a result of analysis mistakes, and inadvertent overprescribing may all be perceived to arise inadvertently (from inattention or a lack of expertise) rather than by intention. The moral ambiguity and perceived lack of intentionality might make people more forgiving of differences. In some cases, the practice may not be considered problematic at all by peers (Mohliver 2019). It follows that differences in arguably less contentious practices may not be strong enough to counteract social factors holding the relationship in place. The literature has established that relationships can have strong inertia arising from multiple factors: the avoidance of distress and hurt that can arise when relationships terminate (Blumstein and Kollock 1988), task dependence, being in the same social circle, geographic constraints, and path dependence where relationships are repeated even when better partners are available (Sorenson and Waguespack 2006). Thus, differences on less morally contentious practices may push a tie to simply weaken rather than end.
On the other hand, we might expect that when individuals differed on a highly contentious practice, they are more likely to end the relationship. This would then be captured in the binary conceptualization of tie dissolution. Highly contentious practices can consist of wrongdoing that is carried out to advance self- or group interests (financial fraud, academic p-hacking, drug trafficking, and terrorist activities, to name a few). To the extent that differences in decidedly deviant practices—typically illegal—are a stronger signal of sharp divergence in moral and professional standards, they will provoke stronger responses than more ambiguous forms of norm violations. For instance, the study of academic retractions by Azoulay et al. (2017) finds that scholars suffer a sharper reputation decline when the retraction is due to clear-cut misconduct as opposed to “honest mistakes” (i.e., contaminated samples or statistical errors). If one discovers the other to be engaging in deviant practice, they might cease all interactions with the other party to uphold their moral integrity and to avoid “contamination,” moral degrading, and inferred guilt by association (Hussinger and Pellens 2019), thus completely severing the relationship. The party engaged in the deviant practice also has incentives to sever the relationship to maintain secrecy and avoid being reported and penalized (Simmel 1906, Lindelauf et al. 2009). Therefore, we would expect that divergences on more contentious practices to have greater effects on tie dissolution.
Hypothesis 3. Dyadic dissimilarity in highly contentious practices is more likely to lead to complete tie dissolution than less contentious practices.
These hypotheses underscore the importance of appreciating relationships as a process unfolding over time, during which revealed information can affect its subsequent trajectory. Collectively, they begin to shift our framework toward a more nuanced understanding of the complex processes underlying tie decay and network evolution more generally.
Empirical Context
Physician Networks
We study the effect of practice dissimilarity on tie formation, decay, and dissolution in the context of physicians’ professional networks. A key empirical challenge in studying tie decay and dissolution is the difficulty of collecting longitudinal data on relationship persistence as well as strength over time. This setting helps address this challenge by using patient-sharing relationships. A large body of literature (primarily within medicine) has documented how sharing patients creates relationships between physicians. Physicians rely heavily on colleagues for information and advice about the care of their patients (Keating et al. 2007), and patient referrals are one way for them to get advice from their colleagues for a second opinion. Shared patients also act as conduits for information, learning, and advice to flow between physicians (Pollack et al. 2017). Moreover, in the process of providing care to shared patients, physicians gain deeper knowledge about colleagues’ practices and develop their professional connections through informal discussions and by sharing medical records.
The medical literature has also shown that informal interactions embodied by patient-sharing are powerful conduits of information and influence. For instance, Donohue et al. (2018) found that patient-sharing networks had the largest effect on the adoption of new drugs compared with networks constructed from medical group affiliations, hospital affiliations, and medical school/residency training groups. They concluded that “the patient-sharing network may exert the most influence on physician adoption because it captures more active connections over which physicians exercise the most control. A physician likely has more discretion, for example, over whom he refers his patients to than he does over the physicians with admitting privileges to the same hospital. In essence, there is “an element of choice” (Donohue et al. 2018, p. 11). Other work in this domain also finds that patient sharing is associated with whether physicians avoid coprescribing interacting drugs (Ong et al. 2017), their patients’ rates of complications after surgery (Pollack et al. 2014), and the diffusion of medical innovations from physician to physician (Pollack et al. 2017), among many other healthcare outcomes. For a review, see DuGoff et al. (2018b).
Building on this large body of research validating professional networks between physicians based on patient sharing (Barnett et al. 2011, Donohue et al. 2018, Onnela et al. 2018), we can observe the existence (and hence, the persistence) of a tie. Patient sharing (beyond a threshold) obtained through administrative records corresponded to meaningful relationships, as self-reported by surveyed physicians (Barnett et al. 2011). At a threshold of six or more shared patients, physicians reported having professional relationships with approximately 80% of colleagues with whom they shared patients. Moreover, physicians acknowledging referral ties are cognizant of each other’s practice styles, and they cited clinical expertise and communication as top reasons for patient referral (Barnett et al. 2012). This approach has been compared with networks constructed from shared clinical episodes and validated using the entire Medicare database (Onnela et al. 2018).
This context also provides us with a measure of tie strength. As studies have shown, the more physicians have shared patients, the stronger their collaborative relationship was, as indicated by better care outcomes for patients (Pollack et al. 2013). Just as scholars who have more joint publications are presumed to have a stronger collaborative tie (Dahlander and McFarland 2013), and employees exchanging more emails have stronger relationships (Kossinets and Watts 2006), physicians sharing more patients would have increased channels of information flow and stronger professional relationships. The continuous measure of tie strength helps us distinguish between truly dissolved ties with dormant ties.
Contentious Prescribing of Benzodiazepines
To understand how differences in contentious professional practices affect network evolution, we focus on prescribing of benzodiazepines. Benzodiazepines, commonly known in the forms of Valium and Xanax, are a class of psychoactive drugs. They are a major contributor to the prescription drug epidemic. In 2013, one in three overdose deaths involved the use of benzodiazepines (Bachhuber et al. 2016). Widely prescribed in the 1970s to treat anxiety and sleep problems (Wick 2013), the adverse effects of long-term benzodiazepine use include higher risks of impaired cognitive functioning (Billioti de Gage et al. 2012), falls (Wagner et al. 2004), Alzheimer’s (Billioti de Gage et al. 2014), and drug abuse and dependence (Fenton et al. 2010).
Well-established benzodiazepine prescribing guidelines are widely available. Using benzodiazepines for more than 120 days in a year is generally considered medically problematic and has been adopted as a standard cutoff for overprescribing in expert consensus statements and in the literature (Ross-Degnan et al. 2004, Olfson et al. 2015). The prescribing guidelines are also readily accessible. For instance, New York City posted the guideline on their website, stating that with the exception of end-of-life care, “If benzodiazepines are indicated, prescribe the lowest effective dose for the shortest duration—no more than two to four weeks” (New York City Department of Health and Mental Hygiene 2016). Such recommendations are echoed by numerous safety guidelines widely circulated online and by healthcare organizations (Maine Benzodiazepines Study Group 2008). For example, the safety guideline from the Kaiser Foundation (2014) states that “benzodiazepines are not recommended for long-term use (longer than 6 weeks), apart from in exceptional circumstances (i.e., terminally ill patients).”
Despite the availability and clarity of guidelines, a wide divergence exists between clinical practice and expert opinion. High variability in practice styles exists and cannot be explained by differences in patient health status (Paulozzi et al. 2016). Qualitative evidence highlights significant differences in physicians’ opinions of appropriate standards of care (Sirdifield et al. 2013). Although many physicians are aware of the guidelines, some do not regard long-term use as problematic (Cook et al. 2007). Consensus statements and guidelines advise physicians to taper patients off from long-term benzodiazepine use, yet there is variance in the degree that physicians feel responsible to do so (Sirdifield et al. 2013). Among elderly patients receiving any benzodiazepine prescription, one in three received a yearly days’ supply that significantly exceeds prescribing guidelines (Olfson et al. 2015).
In contrast to overlength prescribing, a distinct form of contentious prescribing occurs when physicians prescribe to individuals who misuse prescription drugs (doctor shoppers). Doctor shoppers obtain a large number of prescription pills by visiting multiple doctors or pharmacies within a short period. Doctor shopping is illegal (Centers for Disease Control and Prevention 2011). To combat it, states have initiated doctor-shopping laws and prescription drug monitoring programs (PDMPs), which enable physicians to access patients’ past medical records to screen out doctor shoppers (Paulozzi et al. 2011, Brady et al. 2014; for a review, see Haegerich et al. (2014)). Unlike overlength prescribing, which is more morally ambiguous, routinely prescribing to nonmedical users violates professional ethics and is more contentious.
Our context thus offers a unique opportunity to test two types of professional practices that vary in their moral contention: Overlength prescribing is more ambiguous, whereas prescribing to nonmedical users evokes greater moral contention. This allows us to assess how moral contention of the practice affects relationship evolution.
Industry reports have suggested that incongruence in prescribing can lead to the withdrawal of professional relationships and even result in physicians exiting practice groups. The national report “Silence Kills” (Maxfield et al. 2005) documents a striking 84% of physicians reported seeing colleagues with poor clinical judgment, but fewer than 1 in 10 confronted their colleagues. Instead, they withdrew from these relationships, as was concluded that “people don’t want to make others angry or disrupt their working relationships, so they leave difficult discussions to others or to another time, and never go back to the person” (Maxfield et al. 2005, p. 10). Imagine that a pair of physicians, after forming a professional relationship, learn that they differed in the extent to which they prescribe inappropriately. To address this dissonance, physicians can confront one another or try to educate the less compliant physician. Yet one in three physicians do not take any action to confront deviant or incompetent colleagues (DesRoches et al. 2010), and few physicians communicated their concerns with colleagues over broken rules, mistakes, and incompetence (Maxfield et al. 2005). Another option is to change their behavior to become more similar (social influence). However, for judicious prescribers, if inappropriate prescribing violates their beliefs, the easier route may be to disassociate with the other physician by limiting or severing their professional interactions. Given that physicians refer patients to colleagues who they believe have clinical expertise (Barnett et al. 2012), they would also stop sending patients to doctors they consider incompetent. Physicians who routinely engage in deviant prescribing to doctor shoppers may also distance themselves from dissimilar others to stay covert. Either way, this would lead to a weakening of professional ties between dissimilar physicians.
Data and Methods
We use IQVIA’s LRx Longitudinal Prescription Database from January 1, 2005, to December 31, 2008. IQVIA LRx is a commercial database that covered about 65% of all retail prescriptions in the United States at the time of our study. It is representative by age, sex, and insurance coverage, and it includes prescriptions dispensed for all methods of payment, including private insurance, Medicare, and cash payments. This allows us to better identify doctor shoppers, who often fill prescriptions out of pocket to avoid paper trails (Cepeda et al. 2013b). Our data are restricted to mental health prescriptions. The 2008 data cover approximately 39 million patients and 213 million mental health prescriptions. It provides physician attributes (age, gender, practice, medical school, graduation year, and three-digit zip code), patient characteristics (age, gender, and payment type), and information about the prescription. Each physician has a unique deidentified number that allows us to track him or her over time. We exclude physicians specializing in addiction medicine and addiction psychiatry (0.03%) because these physicians may be tapering patients who were dependent on benzodiazepines.
Ties Between Physicians
Following the standard approach of Barnett et al. (2011), we constructed physician networks for each calendar year based on all mental health patients, excluding benzodiazepines patients. We began with a two-mode network in which each tie represents a connection between a patient and a physician and transformed it into a one-mode network in which each tie represents patient sharing between a pair of physicians. A tie is created between physicians A and B if they prescribed mental health prescriptions to six or more patients in common in the calendar year. We assigned a tie weight based on the number of mental health patients shared by two physicians in the calendar year. For instance, if A and B both saw eight patients, each of whom received mental health prescriptions from them, the tie weight between A and B would be eight. Patient-sharing ties are constructed for each calendar year, so we have repeated measures for the same dyads over time.
We took care to minimize spurious ties—cases in which physicians shared patients but do not recognize the relationship—by opting for conservative ways to measure relationships. Because our sample includes only mental health prescriptions, patient sharing within the same category of medications should be much more likely to correspond to a true relationship (recall that the validation study conducted by Barnett and colleagues was for all office-based specialties). Imagine, to the contrary, that the mapping from patient sharing to professional tie occurs regardless of medication category. Then, if a patient goes to two doctors for separate conditions (i.e., the patient goes to physician A for an arthritis medication and to B for a mental health medication), then a tie may be generated even though the two physicians do not know each other. To further reduce potential spurious relationships, we tested our findings to higher patient-sharing thresholds.
Importantly, we excluded benzodiazepine patients from the network construction, so that any tie decay can only arise from a decline in shared nonbenzodiazepine patients.1 This removes the concern that tie decay is driven by doctor shoppers or patients moving from physician to physician (i.e., if the individual shopped benzodiazepines from both physicians A and B, this may generate a tie between A and B although they do not know each other). It is also unlikely for nonbenzodiazepine patients to shop for other drugs, given that most other drug classes in our sample do not have the same abuse potential. An exception is stimulants, yet they only account for 5% of mental health prescriptions.
Measures
Tie Decay and Tie Dissolution.
We constructed two dependent variables at the dyad level to measure how relationships change over time. We model the change in the strength of a tie—measured by the number of nonbenzodiazepine patients shared in a calendar year (beyond the recognition threshold)—to understand tie decay dynamics. Tie decay is captured by a weakening of tie strength. The idea is that controlling for other factors, if two physicians shared 20 patients at time 1 but 8 patients at time 2, their relationship became weaker. Tie dissolution is a binary measure that is set to 1 if a preexisting tie dissolved and 0 otherwise. On the basis of previous work by Barnett et al. (2011), when physicians share a minimum of six patients, we consider that a relationship exists. We also measured tie dissolution using different thresholds.
Dissimilarity in Prescribing Practice.
We construct a general prescribing measure across all patients to capture a physician’s overall tendency of overprescribing or prescribing to doctor shoppers. The dissimilarity measures are thus based on the differences in the overall prescribing practices of two physicians. This helps capture a general pattern and attitude of prescribing rather than reflecting idiosyncratic differences of particular patients. The idea is that general attitudes of benzodiazepine prescribing are learned in the course of providing care to shared patients.2
We created two individual-level measures to capture physician practice styles: (1) percent overprescribed and (2) the percentage of a physician’s patients who are doctor shoppers. The latter is a measure of receptivity to nonmedical users. Following the medical literature, we measure percent overprescribed as the percentage of patients who the physician prescribed a 120-day supply or greater in a given calendar year. The receptivity measure—the percentage of doctor shoppers—is operationalized using the percentage of a physician’s patients who likely obtained benzodiazepine prescriptions for nonmedical use in the given calendar year. We began with individuals filling medically problematic days’ supply (≥ 120-days supply in a calendar year) from three or more prescribers. This definition was developed and validated by Cepeda et al. (2012) using the same database employed in this study. Cepeda et al. (2012) compared fill patterns for commonly misused medications (benzodiazepines and opioids) and medications that are not misused (such as diuretics). The doctor shopping measure is correlated with known risk factors for shopping including distance traveled and cash payments (Cepeda et al. 2013a, b). Consistent early refills, defined as those that overlapped by at least 25% of the days prescribed, are also a sign of misuse (Yang et al. 2015). A nonmedical user may repeatedly visit the same doctor who meets his or her needs. To incorporate this case, individuals who had three or more early refills and no fewer than a 120-day supply in a year are also identified as doctor shoppers.
We then construct practice dissimilarity for any physician dyad A-B. Dissimilarity in overprescribing takes the absolute value of the difference between the percentage of patients overprescribed by A and the percentage of patients overprescribed by B. Dissimilarity in doctor shopping is the absolute value of the difference between the percentage of doctor shoppers A sees and the percentage of doctor shoppers B sees. Both measures range from 0 to 1.
Information Salience on Benzodiazepine Prescribing.
The ideal test of our theory would be to directly measure the extent of information revelation regarding benzodiazepine prescribing within a physician dyad. However, such qualitative information is not available to us. Nonetheless, the type of patients a pair of physicians share can serve as a potentially useful pointer for the salience of benzodiazepine prescribing. The idea is that each patient provides an opportunity for involved physicians to discuss that patient’s care. Using this logic, we would expect that differences in benzodiazepine prescribing would be much more readily revealed within physician dyads that had shared many benzodiazepine patients than a dyad that did not share any benzodiazepine patient (and hence, no discussion or observation of benzodiazepine prescribing) at all. In other words, the higher the proportion of shared benzodiazepine patients, the more information channels of learning and information revelation, and the stronger the link between benzodiazepine prescribing discrepancies and tie decay and dissolution. More specifically, we calculate the percentage of benzodiazepine patients shared as the proportion of benzodiazepine patients shared among all shared patients to test the mechanism of information revelation. This is by no means a perfect measure of information revelation, but given the constraints of the data, it is a reasonable proxy of information salience that can be leveraged to get at the content of information exchange within a physician dyad.
Control Variables.
Tie Inertia.
Past work has found that ties have strong inertia—that ties already in place are likely to remain so (Burt 2000, Dahlander and McFarland 2013). Although we do not have the tenure of the relationship, some of this carries over to the strength of the relationship. To account for the fact that stronger ties tend to be stickier, we control for tie strength at (T – 1) when analyzing tie strength at T. We take the logarithm of tie strength at (T – 1) to account for the exponential scaling in all the quasi-maximum likelihood Poisson models.
Trait Homophily.
We include several control variables to account for the effects of social similarity. Because physicians with similar characteristics have more persistent relationships (DuGoff et al. 2018a), we control for age, gender, and specialty similarity. Same Cohort is a binary indicator set to 1 for physicians who graduated within the same graduation decades from 1960 to 2008 and to 0 otherwise. Same Gender is a binary indicator set to 1 if the physician dyads are male-male or female-female and 0 for mixed-gender dyads.
Geographic Proximity.
Social relationships also tend to decay with greater geographic distance. Physicians are more likely to share information with peers who are geographically proximate (Paul et al. 2014), and connected physician pairs are in closer geographic proximity than unconnected physicians (Landon et al. 2012). Physician ties in the same hospital referral region have a substantially higher probability of persistence compared with ties in different regions (DuGoff et al. 2018a). To account for the effects of geographic proximity, we control for the Same 3-Digit Zip Code, a binary variable set to 1 if both physicians in the dyad practice within the same three-digit zip code. This is the smallest geographic locality data available.
Homophily in Specialization.
Although Barnett et al. (2011) established the correspondence between patient sharing and professional relationships for any office-based specialties, one may worry that a dyad consisting of both primary care physicians (PCPs) would have different decay patterns from a dyad where both physicians are specialists. We address the concern that referral structures may affect patient-sharing dynamics by including dummy variables for the dyadic composition of physicians’ specializations. Both PCP is a binary measure that takes the value of 1 for physician dyads that are PCP-PCP and 0 otherwise. Both Psychiatrist is a binary measure that takes the value of 1 for physician dyads that are both psychiatrists and 0 otherwise.
Structural Embeddedness.
A common finding within the tie decay literature is that structural embeddedness makes ties more resistant to decay. The social environment in which a dyad is embedded can play a key role in the durability of that relationship. Socially “isolated” and socially “integrated” relationships follow different decay patterns. Following Granovetter’s (1973, p. 1363) influential logic of the “forbidden triad,” just as it is difficult to have two strong ties but no third tie in the triad, it is much harder for a tie to decay when embedded with two other strong ties (Krackhardt 1999). Studies have consistently found that in a number of contexts—including friendships, phone communications, professional ties, interorganizational partnership, and academic collaborations—relationships embedded in closed triads and sharing more contacts in common are more likely to last (Burt 2000, Shipilov et al. 2006, Raeder et al. 2011, Jonczyk et al. 2016, Kleinbaum 2018). This is often operationalized through triadic closure or the number of shared contacts (Krackhardt 1999, Dahlander and McFarland 2013, Kleinbaum 2018). To account for the effect of triadic closure on the propensity of tie decay, we control for the number of contacts shared by each dyad. We scale it by log(1 + mutual neighbors) at (T – 1) to account for the decreasing marginal effect of having more mutual neighbors. Original measures of the number of common neighbors are used in robustness checks.
Patient Characteristics.
Certain demographic groups have higher rates of benzodiazepine dependence (Olfson et al. 2015), and one may be worried that physicians may prescribe differently given that their patient pool was different. To account for this effect, we control for similarity in patient panels at (T – 1) by creating three dyad-level variables: similarity in the percentage of elderly patients (over 65 years old), similarity in the percentage of female patients, and similarity in the socioeconomic status of the patients (proxied by the percentage of patients on private health insurance). These measures are constructed as one minus the absolute difference in percent patients between physicians A and B. These controls help us evaluate the effect of prescribing differences for physicians who had similar patient demographics.
Analytic Strategy
Practice Dissimilarity and Tie Formation
We begin by testing whether having different benzodiazepine prescribing patterns reduce the likelihood of tie formation between two physicians. If we do not find an effect here, it will support our hypothesis that the revelation of differences requires the experience of working together. To do this, we treat physicians practicing in the same three-digit zip code but who do not have any patient-sharing tie to be at risk for forming a tie. For the median three-digit zip code, there are 376 prescribers, and the cell size for tie formation in the risk set would quickly accelerate when enumerating every possible pairwise combination. To make computations feasible, we ranked all three-digit zip codes and sampled every 10th zip code region to construct a “case-cohort” data set (King and Zeng 2001). This is done by including all realized ties and a random sample of unrealized ties drawn to generate a 1:2 ratio of realized to unrealized dyads (results are robust to alternative samples). Because realized ties provide the most information, we adjusted the sampling weights for unrealized ties to account for the probability of being drawn into the sample (Russell et al. 2001, Kleinbaum et al. 2013). Our final tie formation sample thus includes 9,079 realized ties and 18,158 unrealized ties. Similar sampling and weighting approaches have been adopted by prior study on tie formation with a large sample size (Kleinbaum et al. 2013).
We created a dummy variable for tie formation. It is set to 1 when a tie is formed at T2 from the risk set and 0 otherwise. On the basis of the finding of Barnett et al. (2011) that a threshold of six or more patients highly corresponds to tie recognition between physicians, we used a threshold of six patients for a tie to be in place (results are robust to other thresholds and available upon request). We then run logistic regressions with tie formation as the dependent variable and dissimilarity in overprescribing and in doctor shopping as the independent variables, and we include all other controls.
Practice Dissimilarity and Tie Decay and Dissolution
To investigate how practice dissimilarity affects tie decay and dissolution, we sample all connected dyads at T1 (2005) and examine how these relationships change over time in light of their prescribing differences. We first focus on changes in tie strength and tie dissolution from T1 to T2 as a baseline model. Then, we use the full period from T1 to T4 and include dyad fixed effects models. These models examine whether ties weaken or dissolve when practices become more dissimilar, restricted to the same dyad over time. Finally, we test whether information salience—proxied by the proportion of shared benzodiazepine patients—moderates the effect of practice dissimilarity on tie decay and dissolution.
For the tie decay analysis, we employ quasi-maximum likelihood (QML) Poisson models. The dependent variable is tie strength at T2, and the independent variables are dissimilarity in overprescribing at T1 and dissimilarity in doctor shopping at T1, as well as our control variables. Tie strength is a count variable that follows a skewed distribution. QML Poisson models are well suited here because they are only characterized by their mean and variance and require no assumptions about the distribution of the data. Hence, they are more robust to distributional misspecification compared with negative binomial models (Wooldridge 2002, Cameron and Trivedi 2013).
We also tested whether dyadic ties weaken within the same pair of physicians if their prescribing practices became more divergent over time. To do so, we use data from T1 to T4 and include dyad fixed effects. Fixed effects require few assumptions and are a conservative approach to our problem. We do not have information on physician practice groups or hospital affiliations. However, any time-invariant variable is absorbed within physician dyads over time. In effect, we are comparing the number of patients shared by physicians A and B at each time point as a function of their practice dissimilarity. Dyad fixed effects also absorb effects of time-invariant confounders, such as formal institutional constraints that may confound the effect of similar prescribing and tie persistence, and the specialty composition of the dyad. We also include year fixed effects to absorb any time trend effects or year heterogeneity. The dyad fixed effects models include the same covariates as the baseline models, except that time-invariant dyad-level variables are dropped. The models also exclude observations with no variation in the dependent variable.
For the tie dissolution analysis, we follow a similar analysis strategy. We first employ logistic regressions to examine the effects of practice dissimilarity on our dichotomous measure of tie dissolution using dyads from T1 to T2. We then employ conditional logistic regression with dyad fixed effects to investigate tie dissolution within physician dyads.
Effects of Information Salience on Tie Decay and Dissolution
Finally, we investigate whether a dyad with more salient information (through sharing more benzodiazepine patients) experiences stronger tie decay and dissolution effects when engaged in dissimilar benzodiazepine prescribing. This is tested in models that included the proportion of benzodiazepine patients among all shared patients, practice dissimilarity, and the interaction between these two variables. The interaction tests whether having more sharing of benzodiazepine patients strengthens the expected effects on tie decay and dissolution. As already detailed, we use QML Poisson to estimate tie decay and logistic regressions to estimate tie dissolution.
Standard Errors
A common problem facing regression analyses with dyadic network data are the violation of the independence assumption. A well-known concern of dependence in dyadic network data is generated if the same person appears in multiple dyads (i.e., common person effects). For instance, A and B having a tie may correlate with A and C having a tie as a result of unobserved attributes of A. In this case, conventional approaches would underestimate the standard errors. To address this concern, we adopt the multiway clustering method theoretically developed by Cameron et al. (2011) and implemented by Kleinbaum et al. (2013). This approach allows estimation of robust standard errors clustered on both A and B of a dyad A-B and has been applied by a number of studies that analyze dyadic network data (Martin and Yeung 2006, Dahlander and McFarland 2013, Jonczyk et al. 2016, Kleinbaum 2018). It is functionally similar to the quadratic assignment bootstrap approach in multiple regression (MR-QAP), with the advantage of enhanced speed in processing large data sets (Cameron et al. 2011). It has also been independently validated to perform very well in large samples and produce comparable results to nonparametric permutation models, including QAP and randomization tests (Kennedy 1995, Lindgren 2010, Feiler and Kleinbaum 2015). Moreover, this approach is feasible in our scenario because it applies to networks with nondichotomous ties as well as models outside of the ordinary least squares family such as quasi-maximum likelihood Poisson models (Kleinbaum et al. 2013).
In the tie formation analysis, standard errors are clustered by both physicians of the dyad as well as the three-digit zip code of both physicians. We apply two-way clustering of robust standard errors by both physician A and physician B within a dyad A-B in all baseline models. We also apply robust standard errors in all dyad fixed effects models.3 In robustness checks, we test these models under a linear specification with a three-way clustering of robust standard errors by physician A, physician B, and year. Finally, we also included individual fixed effects for both physicians of a dyad to account for any potential individual-level heterogeneity.
Results
As shown in Figure 1, there is significant variability in the rates of norm-violating prescribing: 59.7% of physicians have no overlength prescribing, and 50.1% of physicians do not prescribe to any doctor shoppers. However, there is a long right tail with high rates of contentious prescribing.
Figure 1.
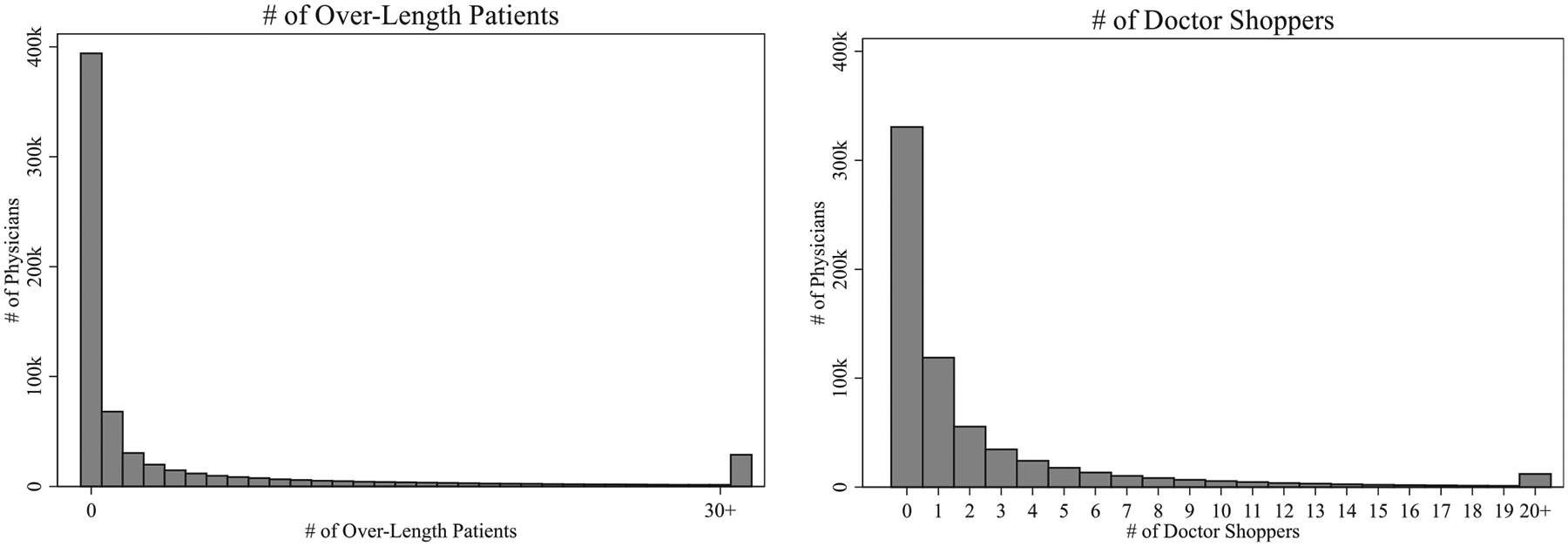
Distribution of Overlength Patients and Doctor-Shopping Patients
Note. The figures show the distribution for all physicians who prescribed any benzodiazepine in 2005 based on the IQVIA data set.
We report both individual-level descriptive statistics (Table 1, panel A) in addition to dyad-level statistics (Table 1, panel B) to give a better sense of the data. Our sample consists of all ties that existed at T1, and we followed them from T1 to T4. This sample consists of 104,172 unique physicians in 141,543 undirected dyads. As shown in Table 1, panel A, overlength prescribing and prescribing to doctor shoppers have a low correlation (r = 0.10). The correlation between dyadic dissimilarity in overprescribing and dyadic dissimilarity in doctor shopping is also relatively low (r = 0.20). This indicates that overlength prescribing and nonmedical prescribing capture relatively distinct prescribing practices.
Table 1.
Descriptive Statistics and Correlation Matrices
| Panel A: Individual-level descriptive statistics and correlation matrices at T1 (N individuals = 104,172) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Variable | Mean | SD | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) |
| (1) | % Overprescribing | 0.19 | 0.16 | 1.00 | ||||||||
| (2) | % Doctor Shopping | 0.11 | 0.13 | 0.10 | 1.00 | |||||||
| (3) | Male | 0.70 | 0.46 | 0.13 | −0.01 | 1.00 | ||||||
| (4) | Graduation Year | 1,984.61 | 10.77 | −0.19 | 0.00 | −0.27 | 1.00 | |||||
| (5) | Psychiatrist | 0.17 | 0.38 | 0.22 | 0.18 | −0.01 | −0.16 | 1.00 | ||||
| (6) | PCP | 0.57 | 0.49 | 0.02 | −0.13 | −0.02 | 0.17 | −0.53 | 1.00 | |||
| (7) | % Female Patients | 0.68 | 0.19 | 0.01 | −0.02 | −0.22 | 0.06 | −0.01 | 0.15 | 1.00 | ||
| (8) | % Elderly Patients | 0.18 | 0.16 | 0.19 | −0.04 | 0.09 | −0.06 | −0.26 | 0.30 | 0.10 | 1.00 | |
| (9) | % Private Insurance | 0.69 | 0.24 | −0.07 | −0.18 | −0.03 | 0.03 | −0.14 | 0.14 | 0.09 | 0.12 | 1.00 |
| Panel B: Dyad-level descriptive statistics and correlation matrices at T1 (N dyads = 141,543) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Variable | Mean | SD | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | (13) |
| (1) | Tie Strength | 17.07 | 22.24 | 1.00 | ||||||||||||
| (2) | Dissimilarity in Overprescribing | 0.14 | 0.13 | −0.06 | 1.00 | |||||||||||
| (3) | Dissimilarity in Doctor Shoppers | 0.09 | 0.12 | −0.03 | 0.20 | 1.00 | ||||||||||
| (4) | % Shared Benzo Patients | 0.11 | 0.11 | 0.10 | −0.11 | −0.15 | 1.00 | |||||||||
| (5) | Same Gender | 0.63 | 0.48 | 0.00 | 0.00 | −0.03 | 0.03 | 1.00 | ||||||||
| (6) | Same Cohort | 0.31 | 0.46 | 0.01 | −0.04 | −0.02 | 0.00 | 0.00 | 1.00 | |||||||
| (7) | Both Psychiatrist | 0.21 | 0.41 | 0.04 | 0.13 | 0.14 | −0.18 | −0.03 | −0.01 | 1.00 | ||||||
| (8) | Both PCP | 0.39 | 0.49 | 0.06 | −0.17 | −0.19 | 0.39 | −0.02 | 0.03 | −0.41 | 1.00 | |||||
| (9) | Same 3-Digit Zip Code | 0.61 | 0.49 | 0.03 | −0.07 | −0.12 | 0.06 | 0.02 | 0.02 | −0.17 | 0.14 | 1.00 | ||||
| (10) | No. Common Neighbors | 1.57 | 1.98 | 0.27 | −0.01 | 0.07 | −0.06 | −0.03 | −0.02 | 0.24 | −0.08 | −0.02 | 1.00 | |||
| (11) | Similarity in % Female Patients | 0.85 | 0.17 | 0.03 | −0.07 | −0.17 | 0.26 | 0.14 | 0.00 | 0.00 | 0.15 | 0.01 | 0.03 | 1.00 | ||
| (12) | Similarity in % Elderly Patients | 0.90 | 0.11 | 0.12 | −0.07 | −0.05 | 0.06 | −0.02 | 0.01 | 0.13 | −0.01 | 0.01 | 0.12 | 0.02 | 1.00 | |
| (13) | Similarity in % Private Insurance | 0.85 | 0.17 | 0.06 | −0.12 | −0.21 | 0.26 | 0.03 | 0.02 | −0.12 | 0.25 | 0.08 | 0.01 | 0.27 | 0.07 | 1.00 |
| Panel C: Dyad-level descriptive statistics from T1 to T4 (N dyads = 141,543, followed from T1 to T4) | ||||
|---|---|---|---|---|
| 2005 (T1) | 2006 (T2) | 2007 (T3) | 2008 (T4) | |
| Tie Strength (Mean, SD) | 17.07 (22.24) | 14.40 (26.92) | 9.32 (23.43) | 10.10 (24.80) |
| Tie Dissolution (Mean) | 0.00 (0.00) | 0.40 (0.49) | 0.63 (0.48) | 0.61 (0.49) |
| Dissimilarity in Overprescribing (Mean, SD) | 0.142 (0.094) | 0.153 (0.103) | 0.161 (0.109) | 0.163 (0.108) |
| Dissimilarity in Doctor Shoppers (Mean, SD) | 0.133 (0.124) | 0.136 (0.126) | 0.144 (0.133) | 0.145 (0.134) |
Table 1, panel B shows that the average tie strength is 17.07, indicating that, on average, physicians in the network share close to 17 nonbenzodiazepine patients. This is well above the threshold for relationship recognition (Barnett et al. 2011) and increases our confidence that ties within our sample likely reflect meaningful relationships. We also note that physician dyads varied in the proportion of benzodiazepine patients. On average, shared benzodiazepine patients account for 11% of all shared patients, with a standard deviation of 0.11. The variation allows us to test how the salience of benzodiazepine prescribing affects tie decay. All else equal, we would expect dyads that had shared a large proportion of benzodiazepine patients to more likely weaken or dissolve their relationships over prescribing differences.
Table 1, panel C reports trends in the mean and the standard deviation of dyad-level statistics from T1 to T4. Within this period, the average tie weakens and then gradually levels off from T3 to T4. This trend is similarly reflected in tie dissolution: 40% of the dyads experienced complete dissolution in T2 (i.e., 60% of ties connected at T1 remained intact). This number is comparable to recent findings by DuGoff et al. (2018a) using Medicare data, where the authors find that 70.7% of physician ties that were present in 2012 persisted in 2013.
Effects of Practice Dissimilarity on Tie Formation
The first set of findings on tie formation, reported in Table 2, shows that prescribing dissimilarity at T1 played little role in tie formation at T2. Consistent with the voluminous body of work, we find that tie formation is heavily driven by similarity in observable traits and structural embeddedness (i.e., having mutual contacts). Estimates in model (1) show that mutual contacts exert a particularly strong effect on tie formation. Ceteris paribus, the probability of tie formation between dyads that shared one mutual contact is 16.9 times the probability of an otherwise similar dyad that had no mutual contact. Though large, the effect is highly consistent with prior research that tie formation is strikingly biased by triadic closure. For instance, research has found that the likelihood of tie formation between individuals with mutual acquaintances was 30 times greater than those one step further away (Kossinets and Watts 2009). The effects for homophily in specialty are also strong: the probability of tie formation between physicians who are both psychiatrists are 5.9 times than physicians who are of other specialty compositions, and the probability of tie formation for both primary care physician dyads are 4.6 times higher than other specialty combinations. There is also evidence of gender and age homophily, with same-gender dyads 79% more likely to form a professional tie than mixed-gender dyads, and physicians from the same graduation cohort are 86% more likely to form a tie than mixed cohort dyads. Homophily in patient composition also played a significant role in tie formation. The probability of tie formation between dyads that is one standard deviation above the mean score on patient homophily in private insurance, in percentage of elderly patients, and in percentage of female patients, is 6.5, 4.9, and 2.9 times the probability of tie formation between dyads at their respective mean scores. These effects remain substantively similar across models (1)–(3). All effects are statistically significant with p < 0.001.
Table 2.
The Effect of Practice Dissimilarity at (T – 1) on Tie Formation at T
| Tie Formation | |||
|---|---|---|---|
| Variable | (1) | (2) | (3) |
| Dissimilarity in Overprescribing | −0.235 (0.374) |
−0.185 (0.386) |
|
| Dissimilarity in Doctor Shoppers | −0.767 (0.404) |
−0.751 (0.410) |
|
| Both Psychiatrist | 1.845*** (0.461) |
1.847*** (0.454) |
1.848*** (0.456) |
| Both PCP | 1.578*** (0.252) |
1.551*** (0.259) |
1.552*** (0.257) |
| Same Cohort | 0.647*** (0.069) |
0.645*** (0.070) |
0.644*** (0.070) |
| Same Gender | 0.608*** (0.162) |
0.612*** (0.168) |
0.608*** (0.163) |
| Similarity in % Female Patients | 3.055*** (0.369) |
3.062*** (0.387) |
3.054*** (0.374) |
| Similarity in % Elderly Patients | 2.547*** (0.390) |
2.557*** (0.381) |
2.549*** (0.394) |
| Similarity in % Private Insurance | 3.679*** (0.644) |
3.593*** (0.625) |
3.606*** (0.615) |
| ln(No. Common Neighbors + 1) | 9.449*** (0.659) |
9.429*** (0.671) |
9.436*** (0.661) |
| Observations | 27,237 | 27,237 | 27,237 |
| Same 3-Digit Zip Code | Yes | Yes | Yes |
Notes. The dependent variable is tie formation at T. All time-varying variables are lagged by one year. Logistic regressions, with three-way clustered standard errors (in parentheses) by physician A and physician B, and three-digit zip codes are shown.
p < 0.001.
By contrast, the estimates for dissimilarity in overprescribing and dissimilarity in doctor shoppers are not statistically significant. This provides preliminary support for Hypothesis 1 by showing that dissimilarity in contentious professional practices does not deter tie formation between two individuals.
Effects of Practice Dissimilarity on Tie Decay
The second set of results on tie decay, reported in Table 3, panel A, shows that conditioning on having established a relationship being dissimilar in prescribing practice pushed preexisting ties to subsequently decay in strength. Although our theoretical focus is on practice dissimilarity, we first briefly discuss effects from other control variables, which are in line with the theoretical expectations from the literature. Consistent with prior work (Burt 2000, Dahlander and McFarland 2013), tie decay is characterized by strong inertia. Tie strength at (T – 1) positively and significantly predicts tie strength at T. Geographic proximity exerted strong effects making ties more resistant to decay. According to model (6), physician dyads practicing in the same three-digit zip codes have an approximate tie strength of 16 (i.e., 16 shared patients), whereas an otherwise similar dyad that practices in different three-digit zip codes has a tie strength of 12 (i.e., 12 shared patients). Moreover, same-cohort and same-gender dyads are more resistant to a decay in tie strength. All else equal, tie relationship strength between physicians graduating from different decades is 4.2% weaker than those graduating from the same decade at T2. There is also evidence of some gender effect, although the effect size is smaller: tie strength weakened by 2.2% when an otherwise similar dyad is cross gender than same gender. Compared with same-psychiatrist dyads and same-PCP dyads, dyads of other specialty compositions also suffered 6.3% and a 5.8% decays in tie strength, respectively. Similarity in patient compositions also sustained tie strength among physician dyads. Finally, dyads that shared more mutual contacts in common decayed less. Dyads that had no common neighbors suffered a 0.7% decline in tie strength compared with dyads that had one common neighbor. The direction and magnitude of these effects are substantively similar across models (6)–(8).
Table 3.
Baseline Models of Practice Dissimilarity at (T – 1)
| Panel A: Baseline models of practice dissimilarity at (T − 1) on tie decay at T | ||||||||
|---|---|---|---|---|---|---|---|---|
| Tie Strength (Baseline Model) | Tie Strength (Fixed Effects) | |||||||
| Variable | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) |
| Dissimilarity in Overprescribing | −0.267*** (0.041) |
−0.084* (0.041) |
0.009 (0.042) |
−0.218*** (0.033) |
−0.181*** (0.034) |
|||
| Dissimilarity in Doctor Shoppers | −0.817*** (0.067) |
−0.558*** (0.065) |
−0.560*** (0.065) |
−0.336*** (0.034) |
−0.315*** (0.035) |
|||
| Both Psychiatrist | 0.059*** (0.016) |
0.065*** (0.016) |
0.065*** (0.016) |
|||||
| Both PCP | 0.123*** (0.010) |
0.111*** (0.010) |
0.111*** (0.010) |
|||||
| Same Cohort | 0.037*** (0.008) |
0.037*** (0.008) |
0.037*** (0.008) |
|||||
| Same 3-Digit Zip Code | 0.260*** (0.011) |
0.251*** (0.011) |
0.251*** (0.011) |
|||||
| Same Gender | 0.019* (0.008) |
0.018* (0.008) |
0.018* (0.008) |
|||||
| Similarity in %Female Patients | 0.132*** (0.028) |
0.099*** (0.028) |
0.099*** (0.028) |
0.213*** (0.026) |
0.205*** (0.026) |
0.199*** (0.026) |
||
| Similarity in %Elderly Patients | 0.440*** (0.043) |
0.412*** (0.043) |
0.412*** (0.043) |
0.451*** (0.037) |
0.443*** (0.037) |
0.435*** (0.037) |
||
| Similarity in %Private Insurance | 0.243*** (0.031) |
0.195*** (0.031) |
0.195*** (0.031) |
0.343*** (0.025) |
0.339*** (0.025) |
0.333*** (0.025) |
||
| ln(No. Common Neighbor + 1) | 0.034*** (0.008) |
0.041*** (0.008) |
0.041*** (0.008) |
0.093*** (0.006) |
0.093*** (0.006) |
0.092*** (0.006) |
||
| Tie Strength at (T − 1) | 1.062*** (0.007) |
1.061*** (0.007) |
1.029*** (0.007) |
1.028*** (0.007) |
1.028*** (0.007) |
0.000* (0.000) |
0.000* (0.000) |
0.000* (0.000) |
| Observations | 141,543 | 141,543 | 141,543 | 141,543 | 141,543 | 277,432 | 277,432 | 277,432 |
| Panel B: Baseline models of practice dissimilarity at (T − 1) on tie dissolution at T | ||||||||
|---|---|---|---|---|---|---|---|---|
| Tie Dissolution (Baseline Model) | Tie Dissolution (Fixed Effects) | |||||||
| Variable | (12) | (13) | (14) | (15) | (16) | (17) | (18) | (19) |
| Dissimilarity in Overprescribing | 0.773*** (0.051) |
0.278*** (0.052) |
0.066 (0.053) |
0.574*** (0.070) |
0.492*** (0.071) |
|||
| Dissimilarity in DoctorShoppers | 2.249*** (0.069) |
1.621*** (0.069) |
1.610*** (0.069) |
0.899*** (0.070) |
0.852*** (0.071) |
|||
| Both Psychiatrist | 0.086*** (0.022) |
0.061** (0.022) |
0.060** (0.022) |
|||||
| Both PCP | −0.250*** (0.017) |
−0.221*** (0.017) |
−0.219*** (0.017) |
|||||
| Same Cohort | −0.088*** (0.013) |
−0.087*** (0.013) |
−0.087*** (0.013) |
|||||
| Same 3-Digit Zip Code | −0.616*** (0.015) |
−0.590*** (0.015) |
−0.590*** (0.015) |
|||||
| Same Gender | −0.064*** (0.013) |
−0.061*** (0.013) |
−0.061*** (0.013) |
|||||
| Similarity in % Female Patients | −0.722*** (0.045) |
0.607*** (0.046) |
−0.605*** (0.046) |
−0.621*** (0.060) |
−0.606*** (0.060) |
−0.581*** (0.061) |
||
| Similarity in % Elderly Patients | −0.437*** (0.061) |
−0.363*** (0.061) |
−0.358*** (0.061) |
−1.150*** (0.085) |
−1.136*** (0.085) |
−1.112*** (0.085) |
||
| Similarity in % Private Insurance | −0.836*** (0.043) |
−0.707*** (0.043) |
−0.705*** (0.043) |
−0.975*** (0.057) |
−0.951*** (0.058) |
−0.933*** (0.058) |
||
| ln(No. Common Neighbor + 1) | −0.281*** (0.014) |
−0.303*** (0.014) |
−0.302*** (0.014) |
−0.548*** (0.017) |
−0.550*** (0.017) |
−0.548*** (0.017) |
||
| Observations | 141,543 | 141,543 | 141,543 | 141,543 | 141,543 | 172,015 | 172,015 | 172,015 |
Notes. In Panel A, the dependent variable is the number of patients shared at T. All time-varying variables are lagged by one year. In columns (4)–(8), we show QML Poisson models from T1 to T2. Robust standard errors (in parentheses) are clustered by physician A and physician B. In columns (9)–(11), conditional dyad and year fixed effects Poisson models from T1 to T4 are shown, with robust standard errors in parentheses. In panel B, the dependent variable is tie dissolution T. All time-varying variables are lagged by one year. In columns (12)–(16), we show logistic regressions from T1 to T2; robust standard errors (in parentheses) are clustered by physician A and physician B. In columns (17)–(19), we show conditional dyad and year fixed effects logistic regressions from T1 to T4, with robust standard errors in parentheses.
p < 0.05;
p < 0.01;
p < 0.001.
Across all the baseline models from models (4)–(8), there is a strong tendency for dyads with incongruent prescribing practices to decay in the next period. Models (4) and (5) report the unadjusted estimates for prescribing dissimilarity at (T – 1), controlling for tie strength at (T – 1). Both types of practice dissimilarity have negative effects on tie strength. When other dyadic-level controls of social similarity and geographic proximity, as well as the logarithm of the number of common neighbors, are included, the practice dissimilarity effects remain negative and statistically significant in models (6) and (7). We also include both prescribing measures and all the control variables in model (8) to test whether the effect of two prescribing dissimilarity measures overlap. Here, the significance on overprescribing disappears, but the effect size and significance for dissimilarity in doctor shopping remain substantively similar. This suggests that when comparing across dyads, the effect of differences in overprescribing is partially absorbed by differences in receptivity to doctor shoppers. This could partly be driven by the fact that dyads that are dissimilar on overprescribing also tend to be dissimilar in receptivity to doctor shoppers.
We next turn to the dyad fixed effects models to gain more insight into this finding. Whereas the baseline models compare the association between practice dissimilarity and tie strength across dyads, the dyad fixed effects models restrict the comparison within the same physician dyad over time, thereby allowing us to test whether changes in the two types of prescribing differences exert distinguishable effects on tie strength within a given physician dyad. Dyad fixed effects models are reported in models (9)–(11). These models hold constant time-invariant factors and exploit variation in tie strength among the same physician dyads over time. Collectively, they show that for the same physician dyad, when practices become more divergent, relationships decay in strength. The effects of dissimilarity in overlength prescribing and dissimilarity in prescribing to doctor shoppers are both negative and statistically significant in model (11). This indicates that within the same physician dyad, changes in these two types of prescribing differences have distinct effects on weakening tie strength. The consistent findings in the fixed effects models provide strong support for our hypothesis by removing any time-invariant unobserved heterogeneities, providing a cleaner and more conservative test. These findings support Hypothesis 1 that dissimilarity in overlength prescribing induces tie decay. Moreover, the effect size for practice dissimilarity in prescribing to doctor shoppers is greater than overlength prescribing in model (11), providing preliminary support for our expectation that the more contentious the practice, the stronger the effect of practice dissimilarity on tie decay.
Effects of Practice Dissimilarity on Tie Dissolution
To further investigate whether the effects of doctor shopping are stronger than the effects of overprescribing (Hypothesis 3), we report tie dissolution results in Table 3, panel B. Our hypothesis would be supported if dissimilarity in doctor shopping has a larger effect size on tie dissolution than dissimilarity in overprescribing. We present the tie dissolution results in a parallel way as the tie decay results. Models (12)–(16) present the baseline logistic results, and models (17)–(19) present results with dyad fixed effects. Although we find same gender, similarity in patient composition, similar graduation year, and geographic proximity deter tie dissolution, we choose to focus the discussion on the effect of practice dissimilarities to provide support for our hypotheses.
Models (12) and (13) report the estimates on practice dissimilarities controlling for tie strength at (T – 1). They show that practice dissimilarity at (T – 1) positively predicts tie dissolution at T. These predictions remain statistically significant when other dyadic-level controls are added in models (14)–(16). Similar to our prior results on tie decay, physician dyads that are dissimilar in overlength prescribing and prescribing to doctor shoppers are more likely to subsequently experience tie dissolution, as shown in models (14) and (15). Although model (16) shows that the effect of overprescribing dissimilarity on tie dissolution becomes insignificant when both measures are included, the dyad fixed effects in model (19) recover the positive effect of dissimilarity in overlength prescribing on tie dissolution, suggesting that they each exert distinct effects within a given physician dyad. Moreover, when both dissimilarity measures are included in model (19), the models reveal a stronger effect of dissimilarity in doctor shopping on tie dissolution. The difference in the coefficient estimate for dissimilarity in overlength prescribing and dissimilarity in doctor shopping is statistically significant, supporting Hypothesis 3 that the moral contention of the practice increases the effect of tie dissolution.
Information Salience, Practice Dissimilarity, and Tie Decay and Dissolution
Table 4 shows that physician dyads sharing a higher proportion of benzodiazepine patients experience a stronger effect of practice dissimilarity on tie decay and dissolution. This set of results provides strong support for our argument that shared benzodiazepine patients make benzodiazepine prescribing more salient in the dyadic exchange. All models follow a similar estimation strategy and include the same controls as the baseline models. The estimated effects from control covariates are substantively similar to our prior findings and are available upon request. We focus on the key variable to our argument—the interaction effects between practice dissimilarity and percent shared benzodiazepine patients. Given that interaction effects can be misleading in logistic models (Ai and Norton 2003), we plot the predicted outcomes for tie decay (models (20) and (21)) in Figure 2 to facilitate the interpretation of tie decay effects. The left panel visualizes the effect for dissimilarity in overprescribing, and the right panel visualizes the effect for receptivity to doctor shoppers. The x axis for both plots ranges from 0% to 60% to reflect values from the 0th to 99th percentiles for both dissimilarity measures, respectively. The high percent shared and no percent shared legends represent dyads at one standard deviation above the mean on percentage shared benzodiazepine patients (21.3%) and no shared benzodiazepine patients (which also happens to be approximately one standard deviation below the mean).
Table 4.
Effects of Shared Benzodiazepine Patients and Practice Dissimilarity at (T – 1) on Tie Decay and Dissolution at T
| Tie Strength | Tie Dissolution | |||||
|---|---|---|---|---|---|---|
| Variable | (20) | (21) | (22) | (23) | (24) | (25) |
| Dissimilarity in Overprescribing | −0.025 (0.051) |
0.033 (0.052) |
0.008 (0.063) |
−0.137* (0.064) |
||
| Dissimilarity in Overprescribing ×% Shared Benzo Patients | −0.844* (0.342) |
−0.345 (0.337) |
4.273*** (0.512) |
3.305*** (0.524) |
||
| Dissimilarity in Doctor Shoppers | −0.333*** (0.068) |
−0.342*** (0.069) |
1.048*** (0.074) |
1.077*** (0.075) |
||
| Dissimilarity in Doctor Shoppers × % Shared Benzo Patients | −4.793*** (0.638) |
−4.695*** (0.647) |
11.729*** (0.740) |
11.089*** (0.745) |
||
| % Shared Benzo Patients | 0.044 (0.057) |
0.243*** (0.055) |
0.279*** (0.062) |
−0.506*** (0.100) |
−0.819*** (0.091) |
−1.214*** (0.111) |
| Observations | 141,543 | 141,543 | 141,543 | 141,543 | 141,543 | 141,543 |
| Controls | All | All | All | All | All | All |
Notes. In columns (20)–(22), the dependent variable is the number of patients shared at T, with QML Poisson models. In columns (23)—(25), the dependent variable is tie dissolution at T, with logistic regressions.
All time-variant variables are lagged by one year. Robust standard errors (in parentheses) are clustered by physician A and physician B. Models include all controls as in the baseline model.
p < 0.05;
p < 0.001.
Figure 2.
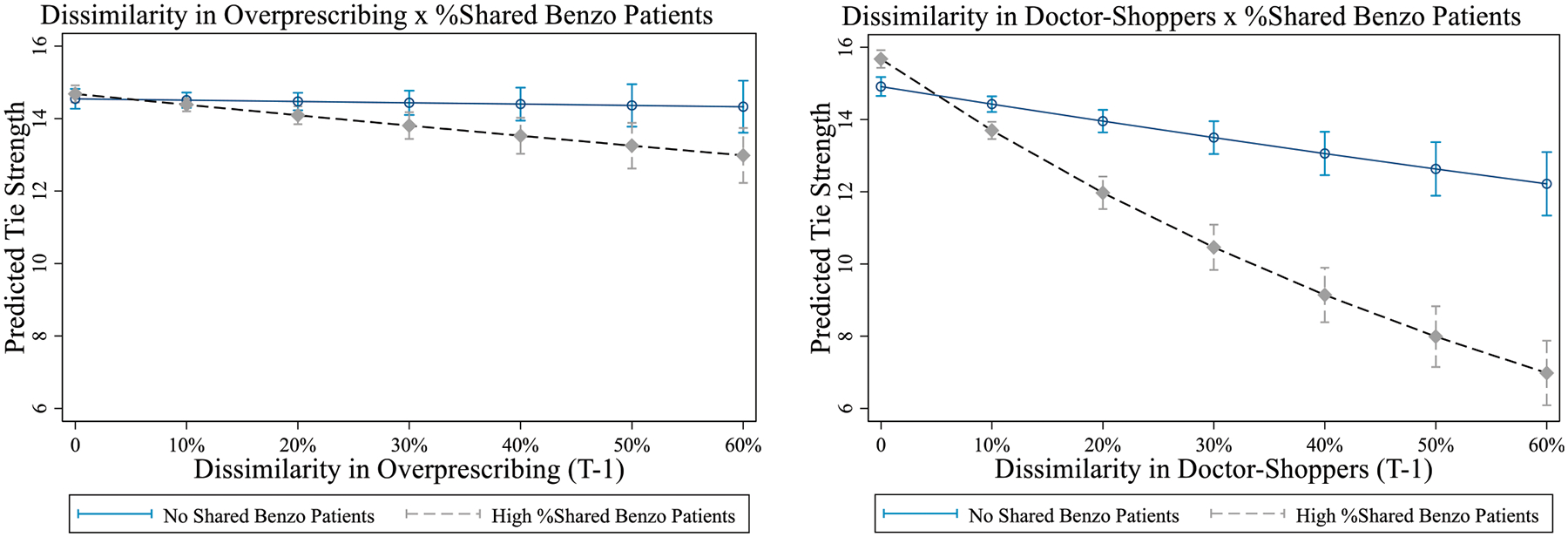
Effects of Prescribing Dissimilarity and Proportion of Shared Benzodiazepine Patients at (T – 1) on Tie Decay at T
Notes. “High %Shared Benzo Patients” indicates dyads whose proportion of benzodiazepine patients among all shared patients is one standard deviation above the mean, at 21.3%. “No Shared Benzo Patients” indicates dyads without any benzodiazepine patients among all shared patients.
As depicted in Figure 2, dissimilarity in overprescribing did not diminish strength when physicians shared zero benzodiazepine patients. In fact, the effect of prescribing dissimilarity on tie decay is almost entirely driven by prior sharing of benzodiazepine patients. This suggests that through the process of caring for shared benzodiazepine patients, differences in contentious practices become revealed, prompting the tie to decay. The effect of prescribing difference in prescribing to doctor shoppers is stronger, consistent with our expectation that more contentious practices evoke stronger responses. Interestingly, for prescribing to doctor shoppers, there is a small main effect of dissimilarity on tie decay and dissolution even when the dyad did not share any benzodiazepine patients. One reason this may occur is through the behavior “spilling over” to other types of practices. Nonetheless, the finding that tie decay and dissolution over differences grows substantially stronger with more benzodiazepine patients represents a “dose-response” test for our hypothesis. It provides strong evidence of information revelation through shared benzodiazepine patients.
We plot the predicted probability of tie dissolution based on models (23) and (24) in Figure 3. These reveal a similar pattern as the tie decay results. When a dyad did not share any benzodiazepine patients, practice dissimilarities did not exert a discernable effect on the probability of tie dissolution. Yet the effects on tie dissolution are much more pronounced when the physician dyad had shared benzodiazepine patients. In fact, the left panel in Figure 3 shows that tie dissolution over differences in overlength prescribing is almost entirely driven by whether physician dyads had previously shared benzodiazepine patients. The right panel in Figure 3 shows that the channel of shared patients also substantially impacted whether physician dyads dropped their ties over differences in prescribing to doctor shoppers, providing support for Hypothesis 2. The dissolution effects for the difference in doctor shoppers is stronger than the difference in overlength prescribing, again supporting Hypothesis 3 that the more contentious the practice, the stronger differences would affect tie dissolution.
Figure 3.
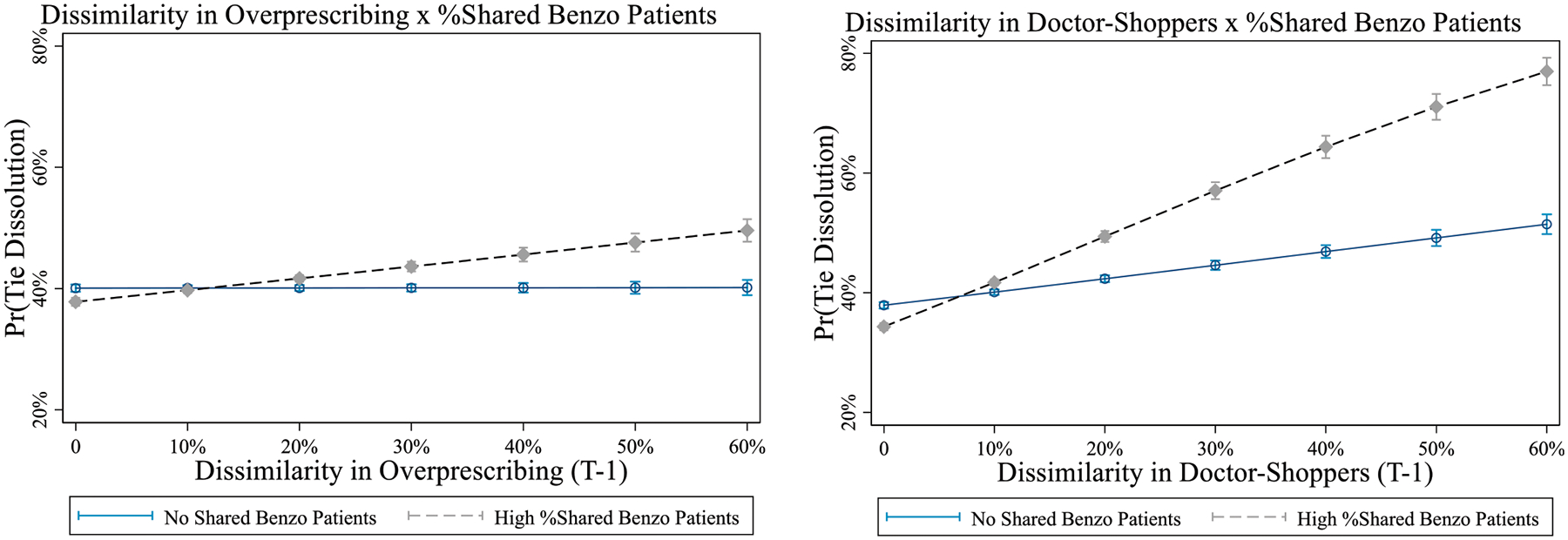
Effects of Prescribing Dissimilarity and Proportion of Shared Benzodiazepine Patients at (T – 1) on Tie Dissolution at T
Notes. “High %Shared Benzo Patients” indicates dyads whose proportion of benzodiazepine patients among all shared patients is one standard deviation above the mean, at 21.3%. “No Shared Benzo Patients” indicates dyads without any benzodiazepine patients among all shared patients.
Robustness Tests.
We conducted additional checks to test the robustness of our results. First, we used an alternative measure for “local” prescribing dissimilarity—the extent to which physicians prescribed differently to shared patients. However, focusing on shared patients can be problematic for both overlength prescribing and prescribing to doctor shoppers: (1) The difference in overlength prescribing to the shared patients may simply reflect idiosyncratic differences (because of differences in specialty, in the length of interactions with the patient, etc.) rather than a general difference in the prescribing attitudes. Moreover, our data show that physicians also tapered the amount they prescribed when another physician was also prescribing (or had prescribed) benzodiazepines to the same patient, making it difficult to treat prescribing to shared patients as reflecting their general tendencies to overprescribe. Nonetheless, when we constructed the differences in overlength prescribing to the shared patient, we find that these local practice differences had substantively similar effects on tie decay and dissolution as their global counterparts (Table A.4 in the appendix). (2) For prescribing to doctor shoppers, there would be a complete dependence on this measure if we were to focus on the prescribing difference in shared patients. This is because two physicians in a dyad share the same number of doctor shoppers, rendering their local prescribing measure to be equivalent. Alternatively, we exploited differences in the days’ supply physicians prescribed to shared doctor-shopping patients, but these measures did not meaningfully correspond to differences their general prescribing tendency. In fact, the correlation between the global prescribing difference and local prescribing difference is negative (−0.17) and is likely highly sensitive because of the noise generated by the doctor shoppers. For these reasons, we opted to use the general differences in prescribing in our main analyses.
We tested our models under higher tie thresholds (4, 8, and 10) (Table A.1 in the appendix), which ensures that our results are robust to threshold specifications. Our findings also remained qualitatively similar to the number of common neighbors (instead of their logarithms) as controls (the baseline models are reported in Table A.2, and the fixed effects models are reported in Table A.3). We also included models with individual fixed effects in addition to dyad fixed effects. This is a strong test of our hypothesis because it absorbs any potential heterogeneity that may remain at the individual level, such as differential rates for physicians to churn their personal network. This is done by analyzing the probability of tie dissolution within the same dyads over time in a linear probability model using the reghdfe package in Stata (Correia 2017), which allows us to include multiple fixed effects as well as clustering on both physician A and physician B. Our results are robust under this specification.
We tested whether the dyadic results are robust to the inclusion of degree centrality. Accounting for degree centrality also accounts for the possibility that dyads may more readily maintain ties when both physicians have similar degree centrality. We also tested this using alternative control variables, including the absolute difference in degree at (T – 1), as well as a categorical specification to distinguish between three types of dyads: when both are of high degree, when only one has a high degree, and when both are low in degree centrality. Our results are robust to all these specifications. All analyses are available from the authors.
Discussion
The formation and dissolution of dyadic ties are two key processes underlying network evolution. Extensive work has focused on tie formation and has found homophily to be a key driver in tie formation. Guided by the voluminous body of literature documenting the importance of homophily for tie formation, much of the scholarship on tie decay has tended to focus on the same factors (i.e., observable or readily accessible traits and characteristics). However, unique features of tie decay make it distinct from tie formation. Although tie formation occurs between strangers—largely driven by opportunities and attraction based on readily obtainable information (gender, race, age, etc.)—tie decay occurs between two people who are already acquainted. Revealed information about differences related to core beliefs, values, or practices (i.e., value homophily) may shape the trajectory of existing relationships, determining whether they weaken or end altogether.
This paper examines how differences in highly contentious professional practices lead to tie decay and dissolution. Divergences on norm-violating practices, which are often only revealed through ongoing interactions, are a critical determinant of whether ties persist. By contrast, differences in contentious practices have no effect on tie formation because they are difficult to observe before a relationship forms. Our paper demonstrates that tie formation, decay, and dissolution are guided by distinct processes. By highlighting the unfolding and revelatory nature of professional relationships, we identify one key dimension that distinguishes the processes through which relationships form and dissolve.
We test our hypotheses in the context of benzodiazepine prescribing. Inappropriate prescribing of benzodiazepines is a key contributor to the prescription drug epidemic. Despite widely established guidelines, the prescribing of benzodiazepines is highly contentious. There is a wide variation in what physicians consider to be appropriate care. Following a large sample of 141,543 physician dyads over time, we find that physicians weakened or dissolved their ties when they differed in contentious prescribing of benzodiazepines. Over time, as practices between two physicians grew more divergent, their relationship grew weaker. The more contentious the practice, the less likely the relationship would survive. Moreover, dissimilarities in prescribing played a critical role in the decay and dissolution of professional ties, but it did not affect the formation of professional ties. In addition, when benzodiazepine prescribing is more salient in the professional relationship, making it more likely that two physicians will observe or exchange attitudes about the practice, the stronger this effect. Our findings provide strong evidence that dissimilarities in prescribing practices are learned by sharing patients and that physicians actively shaped their professional networks as differences in practices are discovered.
We make three contributions to the network evolution literature by testing the effect of differences in contentious practices on the formation, decay, and dissolution of professional relationships. First, our work shows that separate processes make govern tie formation and dissolution. Second, we demonstrate that at later stages of relationship development, revealed information can shape the trajectories of relationships. By considering relationships as an unfolding process through which deeper information becomes gradually discovered, we gain a deeper understanding of the generative processes of network evolution. Finally, by investigating both changes in tie strength as well as complete tie loss, we highlight what can be gained by conceptually distinguishing between decay and dissolution. Here, the level of contention is key.
Investigating how practice dissimilarity affects tie decay and formation differently requires a rich longitudinal data set recording changes in dyadic relationships as well as individuals’ norm-violating practices over time. These data are difficult to come by. Our setting provides a unique opportunity to investigate this question. Although many potentially inappropriate practices may be ignored, unreported, or concealed, our data contain rich information on all prescriptions written by each sampled physician, thereby recording all types of practices and tracing their changes over time. It also allows us to compare practices that differ on the gradient of contention. In addition, the approach of using patient-sharing networks also offers tremendous value to studying relationship evolution, allowing us to examine a population of longitudinal professional relationships at an unprecedented scale. Although a large body of work has established the validity of using patient-sharing ties to measure professional relationships, this approach is not without limitations. Because the network is undirected, our analysis does not disentangle the extent to which this effect was driven by distancing from offenders (to avoid blame or sanction) or from nonoffenders (out of disgust or to avoid staining one’s reputation). Moreover, the administrative nature of our data prevents us from gaining more qualitative information regarding when and what information is learned and revealed between a dyad of physicians. Here, leveraging the type of patients shared enabled us to gain some insights into this process.
Finally, we also contribute to networks and misconduct literature, where a large body of work has examined the diffusion of norm-violating practices by examining whether ties to deviant others increase the likelihood of wrongdoing (Ashforth and Anand 2003, Nash et al. 2013, Palmer and Moore 2016). The predominant lens is social influence (i.e., how the presence of a tie to a deviant other affects the practice of wrongdoing). This paper turns the dependent variable on its head to explore how differences in wrongdoing affect the survival of the preexisting relationship. Distancing from “noncompatible” actors may be an important mechanism for deviant activities to stay covert.
An interesting future direction is investigating the conditions under which co-optation, normalization, and social influence take place as opposed to tie decay and dissolution over incongruent behaviors. Recent scholarship suggests several factors that might shape actors’ reaction over discovery of contentious practices. Studying peer influence effects on employee theft from restaurants, Chan et al. (2020) find that new employees working with high-theft peers were most receptive to peer influence, suggesting that imprinting plays a role in behavioral normalization. This finding might suggest that for professionals holding longer organizational or professional tenure, discovered differences may be more likely to result in tie decay and dissolution as opposed to co-optation. Trust, relationship strength, and relationship history likely also drive whether normalization or disengagement over contentious practices occurs: stronger relationships may increase lenience (Aven et al. 2019), whereas early-stage relationships are likely more fragile and decay and dissolve following the discovery of norm-violating practices.
Our findings also offer some practical implications for organizations. There are downstream consequences of social disengagement in the form of tie decay and dissolution when people recognize differences in how guidelines and norms are interpreted and enacted. Yet the consequences of these ignored differences in norm violations can be striking. Surveying the healthcare industry alone reveals that a depressing 9 out of 10 healthcare workers did not confront their colleagues over broken rules or poor clinical judgment but instead remained silent or chose to withdraw from these relationships (Maxfield et al. 2005). But the failures in judgment or abiding by rules can result in suboptimal patient outcomes and even deaths. When dyadic patterns of tie decay over dissimilarity aggregate into macropatterns, it can generate a pernicious culture of silence and disengagement, letting norm-violating acts persist without correction or confrontation and pushing capable individuals out of the organization. The fact that we have observed norm violations and massive fraud occurring on the scale of entire teams, and even organizations (such as NASA, Enron, and Theranos) could partially be driven by the same mechanism whereby those who disagree with the company’s practices leave the organization. Effective organizations should be wary of these dynamics and promote a culture of transparency and open discussions of what the norm should be.
Dyadic interactions also have far-reaching implications for understanding more macrolevel patterns of segregation. Our world is speeding toward increased polarization on a wide array of issues, opinions, and practices. On issues such as climate change, abortion, and political party affiliation, opinions and practices are growing increasingly distant across different camps. Our findings help to uncover one mechanism that may be contributing to the rise and aggravation of these phenomena. In the face of disagreements and potential conflict, it may be easier to cease interactions with the dissenting party than to engage in a debate and try to convince the other to change his or her mind. This paper unveils the microlevel network conditions that contribute to these divisions, in the hope of informing interventions to help address them.
Acknowledgements
The authors thank IQVIA and Allen Campbell for help with data acquisition and Jim Baron, Anne Bowers, Ivana Katic, Daniel Levin, Olav Sorenson, Ezra Zuckerman, two anonymous reviewers, and participants of seminars at Yale and the INSEAD Network Evolution conference for comments on earlier versions of this paper. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding:
This work was fully supported by the National Institute on Drug Abuse of the National Institutes of Health [Grant R01DA044981].
Biography
Victoria (Shu) Zhang is a postdoctoral associate at Yale School of Management. She received her PhD in organizations and management from Yale University. Her research focuses on social networks, norm violations, and behavioral change. Her current research examines the social network dynamics underlying norm-violating professional practices.
Marissa D. King is a professor of organizational behavior at Yale School of Management. Her research examines factors associated with network-based learning. To understand how large-scale social transformations arise from local networks, she has studied cases ranging from the rise in autism prevalence during the past decade to the opioid epidemic.
Appendix
Table A.1.
Effects of Prescribing Dissimilarity at (T – 1) on Tie Decay and Dissolution at T, with Alternative Tie Thresholds (4, 8, and 10)
| Tie Strength | Tie Dissolution | |||||
|---|---|---|---|---|---|---|
| Variable | (1) | (2) | (3) | (4) | (5) | (6) |
| Tie Strength at (T − 1) | 1.048*** (0.006) |
0.988*** (0.008) |
0.981*** (0.008) |
−1.026*** (0.013) |
−0.969*** (0.017) |
−0.977*** (0.020) |
| Dissimilarity in Overprescribing (T − 1) | −0.016 (0.038) |
0.033 (0.045) |
0.034 (0.048) |
0.046 (0.045) |
0.113 (0.063) |
0.137 (0.073) |
| Dissimilarity in Doctor Shoppers (T − 1) | −0.555*** (0.059) |
−0.548*** (0.068) |
−0.524*** (0.071) |
1.582*** (0.060) |
1.628*** (0.079) |
1.530*** (0.088) |
| Both Psychiatrist | 0.110*** (0.014) |
0.034* (0.016) |
0.014 (0.017) |
−0.004 (0.019) |
0.047 (0.026) |
0.066* (0.029) |
| Both Generalist | 0.148*** (0.009) |
0.055*** (0.011) |
0.037** (0.012) |
−0.126*** (0.015) |
−0.242*** (0.020) |
−0.250*** (0.023) |
| Same Cohort | 0.034*** (0.007) |
0.038*** (0.008) |
0.040*** (0.009) |
−0.071*** (0.011) |
−0.103*** (0.015) |
−0.121*** (0.018) |
| Same 3-Digit Zip Code | 0.240*** (0.010) |
0.251*** (0.011) |
0.263*** (0.012) |
−0.532*** (0.013) |
−0.636*** (0.017) |
−0.680*** (0.019) |
| Same Gender | 0.013 (0.008) |
0.020* (0.009) |
0.022* (0.009) |
−0.041*** (0.011) |
−0.047** (0.015) |
−0.043* (0.018) |
| Difference in % Female Patients (T − 1) | −0.075** (0.027) |
−0.157*** (0.030) |
−0.177*** (0.032) |
0.730*** (0.041) |
0.596*** (0.052) |
0.593*** (0.058) |
| Difference in % Elderly Patients (T − 1) | −0.410*** (0.039) |
−0.372*** (0.046) |
−0.358*** (0.051) |
0.387*** (0.054) |
0.468*** (0.074) |
0.500*** (0.088) |
| Difference in % Private Insurance (T − 1) | −0.178*** (0.028) |
−0.193*** (0.032) |
−0.186*** (0.035) |
0.640*** (0.037) |
0.674*** (0.051) |
0.670*** (0.058) |
| ln(No. Common Neighbors + 1) at (T − 1) | 0.040*** (0.007) |
0.014 (0.010) |
−0.001 (0.010) |
−0.375*** (0.011) |
−0.156*** (0.019) |
−0.063*** (0.018) |
| Constant | −0.578*** (0.021) |
−0.253*** (0.028) |
−0.212*** (0.032) |
2.237*** (0.032) |
2.469*** (0.054) |
2.673*** (0.066) |
| Observations | 219,134 | 101,069 | 76,894 | 219,134 | 101,069 | 76,894 |
| Tie threshold | 4 | 8 | 10 | 4 | 8 | 10 |
Notes. For models (1)–(3), the Dependent variable is the number of patients shared at T. QML Poisson models are shown. For models (4)–(6), the dependent variable is tie dissolution T. Logistic regressions are shown. Robust standard errors (in parentheses) are clustered by physician A and physician B.
p < 0.05;
p < 0.01;
p < 0.001.
Table A.2.
Tie Decay and Tie Dissolution, with Number of Common Neighbors as Control
| Tie Strength | Tie Dissolution | |||||
|---|---|---|---|---|---|---|
| Variable | (1) | (2) | (3) | (4) | (5) | (6) |
| Tie Strength at (T − 1) | 1.035*** (0.007) |
1.033*** (0.007) |
1.033*** (0.007) |
−0.951*** (0.015) |
−0.954*** (0.015) |
−0.953*** (0.015) |
| Dissimilarity in Overprescribing (T − 1) | −0.086* (0.041) |
0.004 (0.042) |
0.284*** (0.052) |
0.074 (0.053) |
||
| Dissimilarity in Doctor-Shoppers (T − 1) | −0.546*** (0.064) |
−0.547*** (0.065) |
1.606*** (0.069) |
1.594*** (0.069) |
||
| Both Psychiatrist | 0.068*** (0.016) |
0.073*** (0.016) |
0.073*** (0.016) |
0.076*** (0.022) |
0.052* (0.022) |
0.050* (0.022) |
| Both Generalist | 0.121*** (0.010) |
0.110*** (0.010) |
0.110*** (0.010) |
−0.253*** (0.017) |
−0.224*** (0.017) |
−0.223*** (0.017) |
| Same Cohort | 0.036*** (0.008) |
0.036*** (0.008) |
0.036*** (0.008) |
−0.086*** (0.013) |
−0.085*** (0.013) |
−0.084*** (0.013) |
| Same 3-Digit Zip Code | 0.260*** (0.011) |
0.251*** (0.011) |
0.251*** (0.011) |
−0.616*** (0.015) |
−0.590*** (0.015) |
−0.590*** (0.015) |
| Same Gender | 0.018* (0.008) |
0.017* (0.008) |
0.017* (0.008) |
−0.060*** (0.013) |
−0.057*** (0.013) |
−0.057*** (0.013) |
| Difference in % Female Patients (T − 1) | −0.132*** (0.028) |
−0.100*** (0.028) |
−0.100*** (0.028) |
0.721*** (0.045) |
0.606*** (0.046) |
0.605*** (0.046) |
| Difference in % Elderly Patients (T − 1) | −0.451*** (0.043) |
−0.424*** (0.043) |
−0.425*** (0.043) |
0.462*** (0.060) |
0.390*** (0.061) |
0.385*** (0.061) |
| Difference in % Private Insurance (T − 1) | −0.243*** (0.031) |
−0.195*** (0.031) |
−0.195*** (0.031) |
0.831*** (0.043) |
0.703*** (0.043) |
0.701*** (0.043) |
| No. of Common Neighbors (T − 1) | 0.003 (0.003) |
0.005 (0.003) |
0.005 (0.003) |
−0.085*** (0.007) |
−0.093*** (0.007) |
−0.093*** (0.007) |
| Constant | −0.511*** (0.023) |
−0.478*** (0.023) |
−0.479*** (0.024) |
2.330*** (0.042) |
2.257*** (0.042) |
2.246*** (0.043) |
| Observations | 141,543 | 141,543 | 141,543 | 141,543 | 141,543 | 141,543 |
Notes. For models (1)–(3), the dependent variable is the number of patients shared at T. QML Poisson models from T1 to T2 are shown. For models (4)–(6), the dependent variable is tie dissolution T. Logistic regressions from T1 to T2 are shown. Robust standard errors (in parentheses) are clustered by physician A and physician B.
p < 0.05;
p < 0.01;
p < 0.001.
Table A.3.
Fixed Effects Estimates of Dissimilarity on Tie Decay and Tie Dissolution, with the Number of Common Neighbors as a Control
| Tie Strength (Fixed Effects) | Tie Dissolution (Fixed Effects) | |||||
|---|---|---|---|---|---|---|
| Variable | (1) | (2) | (3) | (4) | (5) | (6) |
| Tie Strength at (T − 1) | −0.073*** −0.003 |
−0.073*** −0.003 |
−0.074*** −0.003 |
0.927*** −0.008 |
0.927*** −0.008 |
0.928*** −0.008 |
| Dissimilarity in Doctor Shoppers | −0.365*** (0.034) |
−0.341*** (0.035) |
0.891*** (0.070) |
0.843*** (0.071) |
||
| Difference in % Female Patients | −0.239*** (0.026) |
−0.230*** (0.026) |
−0.223*** (0.026) |
0.627*** (0.060) |
0.614*** (0.060) |
0.588*** (0.060) |
| Difference in % Elderly Patients | −0.517*** (0.037) |
−0.508*** (0.037) |
−0.499*** (0.037) |
1.179*** (0.084) |
1.166*** (0.085) |
1.141*** (0.085) |
| Difference in % Private Insurance | −0.378*** (0.025) |
−0.374*** (0.025) |
−0.367*** (0.025) |
0.983*** (0.057) |
0.961*** (0.058) |
0.942*** (0.058) |
| No. of Common Neighbors | 0.021*** (0.002) |
0.021*** (0.002) |
0.021*** (0.002) |
−0.164*** (0.005) |
−0.164*** (0.005) |
−0.164*** (0.005) |
| Observations | 277,432 | 277,432 | 277,432 | 172,015 | 172,015 | 172,015 |
Notes. For models (1)–(3), the dependent variable is the number of patients shared at T. Conditional dyad and year fixed effects Poisson models from T1 to T4 are shown. For models (4)–(6), the dependent variable is tie dissolution T. Conditional dyad and year fixed effects logistic regressions from T1 to T4 are shown. Robust standard errors are shown in parentheses.
p < 0.001.
Table A.4.
Effects of Local Prescribing Dissimilarity at (T – 1) on Tie Decay and Dissolution at T
| Variable | Tie Strength | Tie Dissolution |
|---|---|---|
| Local Dissimilarity in Overprescribing (T − 1) | −0.157*** (0.015) |
0.114*** (0.022) |
| Both Psychiatrist | 0.029 (0.019) |
0.204*** (0.030) |
| Both Generalist | 0.082*** (0.012) |
−0.215*** (0.021) |
| Same Cohort | 0.041*** (0.009) |
−0.122*** (0.017) |
| Same 3-Digit Zip Code | 0.268*** (0.013) |
−0.706*** (0.019) |
| Same Gender | 0.029** (0.010) |
−0.061*** (0.018) |
| Difference in % Female Patients (T − 1) | −0.101* (0.048) |
0.437*** (0.085) |
| Difference in % Elderly Patients (T − 1) | −0.556*** (0.053) |
0.683*** (0.093) |
| Difference in % Private Insurance (T − 1) | −0.453*** (0.050) |
1.055*** (0.075) |
| ln(No. Common Neighbor + 1) at (T − 1) | 0.010 (0.009) |
−0.277*** (0.018) |
| Tie Strength at (T − 1) | 1.002*** (0.008) |
−0.974*** (0.018) |
| Observations | 87,128 | 87,128 |
Notes. Local dissimilarity in overprescribing is a dyad-level measure of the absolute difference in the rate of overprescribing to shared patients for a given physician dyad A-B. For tie strength, the dependent variable is the number of patients shared at T. QML Poisson models from T1 to T2 are shown. For tie dissolution, the dependent variable is tie dissolution T. Logistic regressions from T1 to T2 are shown. Robust standard errors (in parentheses) are clustered by physician A and physician B.
p < 0.05;
p < 0.01;
p < 0.001.
Footnotes
Eliminating benzodiazepine patients from inferring relationships would be problematic if physicians mostly share benzodiazepine patients and have few non-benzodiazepine patients. If so, not factoring in shared benzodiazepine patients would remove many real relationships. However, this is unlikely given that physicians who saw benzodiazepine patients typically also saw many more nonbenzodiazepine patients. In our data set, on average, benzodiazepine patients only account for fewer than 14% of shared patients among physician dyads.
In robustness tests, we discuss the concerns of using alternative measure of “local” prescribing differences constructed based on prescribing to “locally” shared patients.
Multiway clustering under nonlinear models with dyad fixed effects is computationally infeasible given our sample size. However, obtaining consistent results across multiple model specifications, including LPM with multiway clustering and individual fixed effects, increases our confidence in the inference.
References
- Ahuja G, Soda G, Zaheer A (2012) The genesis and dynamics of organizational networks. Organ. Sci 23(2):434–448. [Google Scholar]
- Ai C, Norton EC (2003) Interaction terms in logit and probit models. Econom. Lett 80(1):123–129. [Google Scholar]
- Altman I, Taylor DA (1973) Social penetration: The development of interpersonal relationships. Social Penetration: The Development of Interpersonal Relationships (Holt, Rinehart & Winston, New York: ), viii. [Google Scholar]
- Argyle M, Henderson M (1984) The rules of friendship. J. Soc. Personal Relationships 1(2):211–237. [Google Scholar]
- Ashforth BE, Anand V (2003) The normalization of corruption in organizations. Res. Organ. Behav 25:1–52. [Google Scholar]
- Aven B, Morse L, Iorio A (2019) The valley of trust: The effect of relational strength on monitoring quality. Organ. Behav. Human Decision Processes, ePub ahead of print October 26, 10.1016/j.obhdp.2019.07.004. [DOI] [Google Scholar]
- Azoulay P, Bonatti A, Krieger JL (2017) The career effects of scandal: Evidence from scientific retractions. Res. Policy 46(9):1552–1569. [Google Scholar]
- Bachhuber MA, Hennessy S, Cunningham CO, Starrels JL (2016) Increasing benzodiazepine prescriptions and overdose mortality in the United States, 1996–2013. Amer. J. Public Health 106(4): 686–688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnett ML, Keating NL, Christakis NA, O’Malley AJ, Landon BE (2012) Reasons for choice of referral physician among primary care and specialist physicians. J. General Internal Medicine 27(5): 506–512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnett ML, Landon BE, O’Malley AJ, Keating NL, Christakis NA (2011) Mapping physician networks with self-reported and administrative data: Mapping physician networks. Health Services Res 46(5):1592–1609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bell ST (2007) Deep-level composition variables as predictors of team performance: A meta-analysis. J. Appl. Psych 92(3):595–615. [DOI] [PubMed] [Google Scholar]
- Billioti de Gage S, Bégaud B, Bazin F, Verdoux H, Dartigues J-F, Pérès K, Kurth T, Pariente A (2012) Benzodiazepine use and risk of dementia: Prospective population based study. BMJ 345:e6231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Billioti de Gage S, Moride Y, Ducruet T, Kurth T, Verdoux H, Tournier M, Pariente A, Bégaud B (2014) Benzodiazepine use and risk of Alzheimer’s disease: Case-control study. BMJ 349:g5205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blau PM (1977) A macrosociological theory of social structure. Amer. J. Sociol 83(1):26–54. [Google Scholar]
- Blumstein P, Kollock P (1988) Personal relationships. Annual Rev. Sociol 14(1):467–490. [Google Scholar]
- Brady JE, Wunsch H, DiMaggio C, Lang BH, Giglio J, Li G (2014) Prescription drug monitoring and dispensing of prescription opioids. Public Health Rep 129(2):139–147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burt RS (2000) Decay functions. Soc. Networks 22(1):1–28. [Google Scholar]
- Burt RS (2002) Bridge decay. Soc. Networks 24(4):333–363. [Google Scholar]
- Cameron AC, Trivedi PK (2013) Regression Analysis of Count Data (Cambridge University Press, Cambridge, UK: ). [Google Scholar]
- Cameron AC, Gelbach JB, Miller DL (2011) Robust inference with multiway clustering. J. Bus. Econom. Statist 29(2):238–249. [Google Scholar]
- Centers for Disease Control and Prevention (2011) Doctor shopping laws. Report, Public Health Law Program, Centers for Disease Control and Prevention, Atlanta. [Google Scholar]
- Cepeda MS, Fife D, Yuan Y, Mastrogiovanni G (2013a) Distance traveled and frequency of interstate opioid dispensing in opioid shoppers and nonshoppers. J. Pain 14(10):1158–1161. [DOI] [PubMed] [Google Scholar]
- Cepeda MS, Fife D, Chow W, Mastrogiovanni G, Henderson SC (2012) Assessing opioid shopping behaviour: A large cohort study from a medication dispensing database in the US. Drug Safety 35(4):325–334. [DOI] [PubMed] [Google Scholar]
- Cepeda MS, Fife D, Chow W, Mastrogiovanni G, Henerson SC (2013b) Opioid shopping behavior: How often, how soon, which drugs, and what payment method. J. Clinical Pharmacol 53(1): 112–117. [DOI] [PubMed] [Google Scholar]
- Chan TY, Chen Y, Pierce L, Snow D (2019) Peer effects in worker misconduct: Evidence from theft in a thousand restaurants Working paper, Washington University in St. Louis, St. Louis. [Google Scholar]
- Chan TY, Chen Y, Pierce L, Snow D (2020) The influence of peers in worker misconduct: Evidence from restaurant theft. Manufacturing Service Oper. Management, ePub ahead of print April 7, 10.1287/msom.2019.0848. [DOI] [Google Scholar]
- Chen Z, Berger J (2013) When, why, and how controversy causes conversation. J. Consumer Res 40(3):580–593. [Google Scholar]
- Cook JM, Biyanova T, Thompson R, Coyne JC (2007) Older primary care patients’ willingness to consider discontinuation of chronic benzodiazepines. General Hospital Psychiatry 29(5):396–401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coombs RH (1966) Value consensus and partner satisfaction among dating couples. J. Marriage Family 28(2):166–173. [Google Scholar]
- Correia S (2017) Linear models with high-dimensional fixed effects: An efficient and feasible estimator Working paper, Duke University, Durham, NC. [Google Scholar]
- Dahlander L, McFarland DA (2013) Ties that last. Admin. Sci. Quart 58(1):69–110. [Google Scholar]
- DeLay D, Laursen B, Kiuru N, Salmela-Aro K, Nurmi J-E (2013) Selecting and retaining friends on the basis of cigarette smoking similarity. J. Res. Adolescence 23(3):464–473. [Google Scholar]
- DesRoches CM, Rao SR, Fromson JA, Birnbaum RJ, Iezzoni L, Vogeli C, Campbell EG (2010) Physicians’ perceptions, preparedness for reporting, and experiences related to impaired and incompetent colleagues. J. Amer. Medical Assoc 304(2):187–193. [DOI] [PubMed] [Google Scholar]
- Donohue JM, Guclu H, Gellad WF, Chang C-CH, Huskamp HA, Choudhry NK, Zhang R, et al. (2018) Influence of peer networks on physician adoption of new drugs. PLOS One 13(10):e0204826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duck S (2007) Human Relationships, 4th ed. (Sage, London: ). [Google Scholar]
- DuGoff EH, Cho J, Si Y, Pollack CE (2018a) Geographic variations in physician relationships over time: Implications for care coordination. Medical Care Res. Rev 75(5):586–611. [DOI] [PubMed] [Google Scholar]
- DuGoff EH, Fernandes-Taylor S, Weissman GE, Huntley JH, Pollack CE (2018b) A scoping review of patient-sharing network studies using administrative data. Translational Behav. Medicine 8(4):598–625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feiler DC, Kleinbaum AM (2015) Popularity, similarity, and the network extraversion bias. Psych. Sci 26(5):593–603. [DOI] [PubMed] [Google Scholar]
- Fenton MC, Keyes KM, Martins SS, Hasin DS (2010) The role of a prescription in anxiety medication use, abuse, and dependence. Amer. J. Psychiatry 167(10):1247–1253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Festinger L, Back KW, Schachter S (1963) Social Pressures in Informal Groups: A Study of Human Factors in Housing (Tavistock, London: ). [Google Scholar]
- Granovetter MS (1973) The strength of weak ties. Amer. J. Sociol 78(6):1360–1380. [Google Scholar]
- Haegerich TM, Paulozzi LJ, Manns BJ, Jones CM (2014) What we know, and don’t know, about the impact of state policy and systems-level interventions on prescription drug overdose. Drug Alcohol Dependence 145:34–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hallinan MT, Williams RA (1989) Interracial friendship choices in secondary schools. Amer. Sociol. Rev 54(1):67–78. [Google Scholar]
- Hussinger K, Pellens M (2019) Guilt by association: How scientific misconduct harms prior collaborators. Res. Policy 48(2):516–530. [Google Scholar]
- Ibarra H (2006) Homophily and differential returns: Sex differences in network structure and access in an advertising firm. Admin. Sci. Quart 37(3):422–447. [Google Scholar]
- Jonczyk CD, Lee YG, Galunic CD, Bensaou BM (2016) Relational changes during role transitions: The interplay of efficiency and cohesion. Acad. Management J 59(3):956–982. [Google Scholar]
- Kaiser Foundation (2014) Benzodiazepine and Z-drug safety guideline Report, Kaiser Foundation Health Plan of Washington, Oakland, CA. [Google Scholar]
- Keating NL, Ayanian JZ, Cleary PD, Marsden PV (2007) Factors affecting influential discussions among physicians: A social network analysis of a primary care practice. J. General Internal Medicine 22(6):794–798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keller M (1952) Social pressures in informal groups: A study of human factors in housing. Milbank Memorial Fund Quart 30(4): 384–387. [Google Scholar]
- Kennedy PE (1995) Randomization tests in econometrics. J. Bus. Econom. Statist 13(1):85–94. [Google Scholar]
- King G, Zeng L (2001) Logistic regression in rare events data. Political Anal 9(2):137–163. [Google Scholar]
- Kleinbaum AM (2018) Reorganization and tie decay choices. Management Sci 64(5):2219–2237. [Google Scholar]
- Kleinbaum AM, Stuart TE, Tushman ML (2013) Discretion within constraint: Homophily and structure in a formal organization. Organ. Sci 24(5):1316–1336. [Google Scholar]
- Kossinets G, Watts DJ (2006) Empirical analysis of an evolving social network. Science 311(5757):88–90. [DOI] [PubMed] [Google Scholar]
- Kossinets G, Watts DJ (2009) Origins of homophily in an evolving social network. Amer. J. Sociol 115(2):405–450. [Google Scholar]
- Krackhardt D (1999) The ties that torture: Simmelian tie analysis in organizations. Research in the Sociology of Organizations, vol. 16 (JAI Press, Greenwich, CT: ), 183–210. [Google Scholar]
- Landon BE, Keating NL, Barnett ML, Onnela J-P, Paul S, O’Malley AJ, Keegan T, Christakis NA (2012) Variation in patient-sharing networks of physicians across the United States. J. Amer. Medical Assoc 308(3):265–273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lazarsfeld PF, Merton RK (1954) Friendship as a social process: A substantive and methodological analysis. Berger M, Abel T, Page CH, eds. Freedom and Control in Modern Society (Van Nostrand, New York: ), 18–66. [Google Scholar]
- Levin DZ, Walter J, Murnighan JK (2011) Dormant ties: The value of reconnecting. Organ. Sci 22(4):923–939. [Google Scholar]
- Lewis K (2015) How networks form: Homophily, opportunity, and balance. Scott RA, Kosslyn SM, Buchmann M, eds. Emerging Trends in the Social and Behavioral Sciences (John Wiley & Sons, Hoboken, NJ: ), 1–14. [Google Scholar]
- Lindelauf R, Borm P, Hamers H (2009) The influence of secrecy on the communication structure of covert networks. Soc. Networks 31(2):126–137. [Google Scholar]
- Lindgren K-O (2010) Dyadic regression in the presence of heteroscedasticity—An assessment of alternative approaches. Soc. Networks 32(4):279–289. [Google Scholar]
- Maine Benzodiazepines Study Group (2008) Guidelines For the Use of Benzodiazepines in Office Practice in the State of Maine Report, Maine Benzodiazepine Study Group, University of Maine Center on Aging, Bangor, ME. [Google Scholar]
- Martin JL, Yeung KT (2006) Persistence of close personal ties over a 12-year period. Soc. Networks 28(4):331–362. [Google Scholar]
- Maxfield D, Grenny J, Mcmillan R, Patterson K, Switzler A (2005) Silence kills: The seven crucial conversations in healthcare Report, American Association of Critical-Care Nurses, Aliso Viejo, CA. [Google Scholar]
- McPherson M, Smith-Lovin L, Cook JM (2001) Birds of a feather: Homophily in social networks. Annual Rev. Sociol 27:415–444. [Google Scholar]
- Mohliver A (2019) How misconduct spreads: Auditors’ role in the diffusion of stock-option backdating. Admin. Sci. Quart 64(2): 310–336. [Google Scholar]
- Morton TL, Douglas MA (1981) Growth of relationships. Duck S, Gilmour R, eds. Personal Relationships 2: Developing Personal Relationships (Academic Press, New York: ), 3–26. [Google Scholar]
- Nash R, Bouchard M, Malm A (2013) Investing in people: The role of social networks in the diffusion of a large-scale fraud. Soc. Networks 35(4):686–698. [Google Scholar]
- New York City Department of Health and Mental Hygiene (2016) Judicious prescribing of benzodiazepines. City Health Inform 35(2):13–20. [Google Scholar]
- Olfson M, King M, Schoenbaum M (2015) Benzodiazepine use in the United States. J. Amer. Medical Assoc. Psychiatry 72(2):136–142. [DOI] [PubMed] [Google Scholar]
- Ong M-S, Olson KL, Chadwick L, Liu C, Mandl KD (2017) The impact of provider networks on the co-prescriptions of interacting drugs: A claims-based analysis. Drug Safety 40(3):263–272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Onnela J-P, O’Malley AJ, Keating NL, Landon BE (2018) Comparison of physician networks constructed from thresholded ties versus shared clinical episodes. Appl. Network Sci 3(1):Article 28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palmer D, Moore C (2016) Social networks and organizational wrongdoing in context. Palmer D, Smith-Crowe K, Greenwood R, eds. Organizational Wrongdoing: Key Perspectives and New Directions (Cambridge University Press, Cambridge, UK: ), 203–234. [Google Scholar]
- Paul S, Keating NL, Landon BE, James O’Malley AJ (2014) Results from using a new dyadic-dependence model to analyze socio-centric physician networks. Soc. Sci. Medicine 117(September): 67–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paulozzi LJ, Kilbourne EM, Desai HA (2011) Prescription drug monitoring programs and death rates from drug overdose. Pain Medicine 12(5):747–754. [DOI] [PubMed] [Google Scholar]
- Paulozzi LJ, Mack KA, Hockenberry JM (2016) Vital signs: Variation among states in prescribing of opioid pain relievers and benzodiazepines—United States, 2012. Morbidity Mortality Weekly Rep 63(26):563–568. [PMC free article] [PubMed] [Google Scholar]
- Pollack CE, Weissman GE, Lemke KW, Hussey PS, Weiner JP (2013) Patient sharing among physicians and costs of care: A network analytic approach to care coordination using claims data. J. General Internal Medicine 28(3):459–465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollack E, Craig HW, Bekelman JE, Weissman G, Epstein AJ, Liao K, DuGoff EH, Armstrong K (2014) Physician social networks and variation in rates of complications after radical prostatectomy. Value Health 17(5):611–618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollack CE, Soulos PR, Herrin J, Xu X, Christakis NA, Forman HP, Yu JB, Killelea BK, Shi YW, Gross CP (2017) The impact of social contagion on physician adoption of advanced imaging tests in breast cancer. J. Natl. Cancer Inst 109(8):djw330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Popielarz PA, McPherson JM (1995) On the edge or in between: Niche position, niche overlap, and the duration of voluntary association memberships. Amer. J. Sociol 101(3):698–720. [Google Scholar]
- Raeder T, Lizardo O, Hachen D, Chawla NV (2011) Predictors of short-term decay of cell phone contacts in a large scale communication network. Soc. Networks 33(4):245–257. [Google Scholar]
- Rosenbaum ME (1986) The repulsion hypothesis: On the nondevelopment of relationships. J. Personality Soc. Psych 51(6):1156–1166. [Google Scholar]
- Ross-Degnan Dennis, Simoni-Wastila Linda, Brown Jeffrey S., Gao Xiaoming, Mah Connie, Cosler Leon E., Fanning Thomas, et al. (2004) A controlled study of the effects of state surveillance on indicators of problematic and non-problematic benzodiazepine use in a Medicaid population. Internat. J. Psychiatry Med 34(2):103–123. [DOI] [PubMed] [Google Scholar]
- Russell LB, Teutsch SM, Kumar R, Dey A, Milan E (2001) preventable smoking and exercise-related hospital admissions: A model based on the NHEFS. Amer. J. Preventive Medicine 20(1):26–34. [DOI] [PubMed] [Google Scholar]
- Sasovova Z, Mehra A, Borgatti SP, Schippers MC (2010) Network churn: The effects of self-monitoring personality on brokerage dynamics. Admin. Sci. Quart 55(4):639–670. [Google Scholar]
- Shipilov AV, Rowley TJ, Aharonson BS (2006) When do networks matter? A study of tie formation and decay. Baum JAC, Dobrev SD, Van Witteloostuijn A, eds. Ecology and Strategy, Advances in Strategic Management, vol. 23 (Emerald Group Publishing, Bingley, UK: ), 481–519. [Google Scholar]
- Simmel G (1906) The sociology of secrecy and of secret societies. Amer. J. Sociol 11(4):441–498. [Google Scholar]
- Sirdifield C, Anthierens S, Creupelandt H, Chipchase SY, Christiaens T, Siriwardena AN (2013) General practitioners’ experiences and perceptions of benzodiazepine prescribing: Systematic review and meta-synthesis. BMC Family Practice 14(1):Article 191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sorenson O, Waguespack DM (2006) Social structure and exchange: Self-confirming dynamics in Hollywood. Admin. Sci. Quart 51(4):560–589. [Google Scholar]
- Stroebe W, Postmes T, Spears R (2012) Scientific misconduct and the myth of self-correction in science. Perspect. Psych. Sci 7(6):670–688. [DOI] [PubMed] [Google Scholar]
- Tuma NB, Hallinan MT (1979) The effects of sex, race, and achievement on schoolchildren’s friendships. Soc. Forces 57(4):1265–1285. [Google Scholar]
- Vaughan D (1996) The Challenger Launch Decision: Risky Technology, Culture, and Deviance at NASA (University of Chicago Press, Chicago: ). [Google Scholar]
- Verbrugge LM (1977) The structure of adult friendship choices. Soc. Forces 56(2):576–597. [Google Scholar]
- Wagner AK, Zhang F, Soumerai SB, Walker AM, Gurwitz JH, Glynn RJ, Ross-Degnan D (2004) Benzodiazepine use and hip fractures in the elderly. Arch. Internal Medicine 164(14):1567–1572. [DOI] [PubMed] [Google Scholar]
- Wick JY (2013) The history of benzodiazepines. Consultant Pharmacist 28(9):538–548. [DOI] [PubMed] [Google Scholar]
- Wooldridge JM (2002) Econometric Analysis of Cross Section and Panel Data, 1st ed. (MIT Press, Cambridge, MA: ). [Google Scholar]
- Yang Z, Wilsey B, Bohm M, Weyrich M, Roy K, Ritley D, Jones C, Melnikow J (2015) Defining risk of prescription opioid overdose: Pharmacy shopping and overlapping prescriptions among long-term opioid users in Medicaid. J. Pain 16(5):445–453. [DOI] [PubMed] [Google Scholar]