

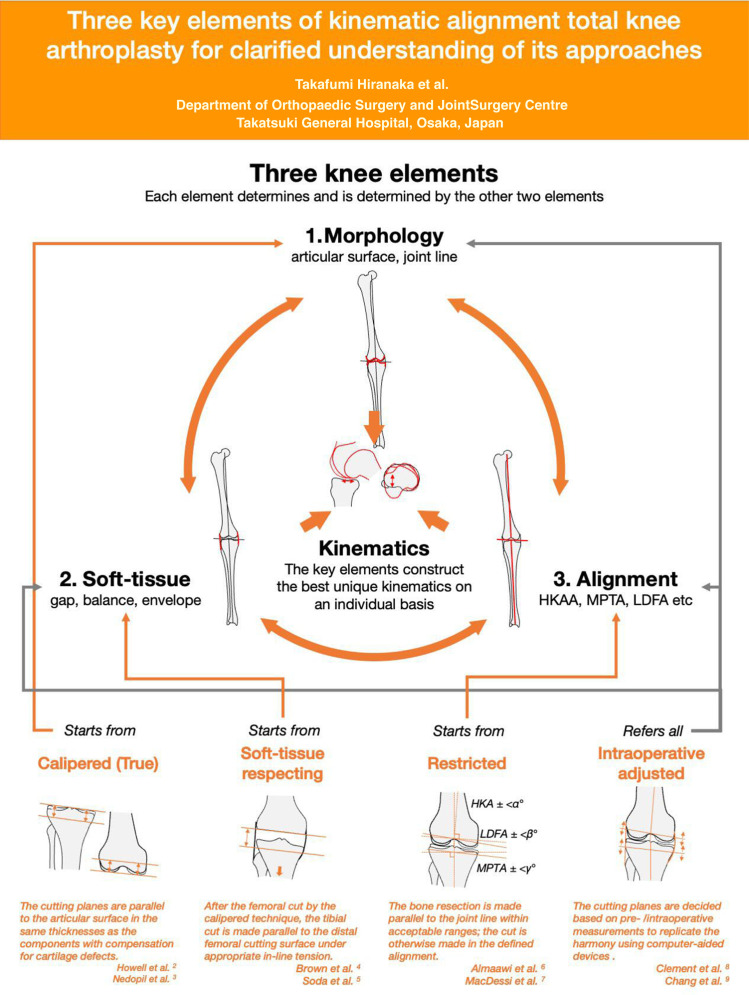
Kinematic alignment total knee arthroplasty (KA-TKA) was advocated by Howell et al, 1 and with growing interest there have been increasing reports on various approaches to it. Such enthusiasm, however, has also led to confusion. In order to better understand KA-TKA and its derivatives, clarification may be provided by consideration of three key knee elements: morphology, soft-tissue, and alignment. Each element determines and is determined by the others, maintaining the best harmony of the elements to construct the best unique kinematics on an individual basis. Differing from the original concept of kinematic alignment, which is alignment that follows the three kinematic axes (cylindrical, patellar, and tibial rotation), 2 recent KA-TKA instead aims to recreate the patient’s original kinematics by setting the harmony of these components in a bespoke alignment.
The three elements of harmony can be the starting points of a KA-TKA approach. Calipered or true KA-TKA starts from the morphology, aiming to mimic the original articular surface (or joint line) by bone resections with compensation for cartilage defects. 2,3 The soft-tissue-based KA-TKA originates from the idea of balancing the soft-tissue, and the tibial cutting surface is made parallel to the femoral resection surface under appropriate in-line tension based on this balance. 4,5 These two approaches are categorized as unrestricted KA-TKA. Restricted KA-TKA, meanwhile, commences with alignment evaluation and control. The bone is cut parallel to the joint line within a safe range; the cut is otherwise made in the defined alignment. 6,7 Intraoperative adjustment of KA-TKA, such as functional alignment and robot-assisted KA-TKA, decides the bone cut plane based on pre- and intraoperative measurements of the three elements to replicate the harmony using computer-aided devices, 8,9 although intraoperative adjustment protocols are provided in other approaches. 3 The question of how to adjust the component alignment and soft-tissue balance is crucial; therefore, they should be clearly defined in each approach. 10 The starting points and adjustment protocols concerning the other elements may differ, but all approaches aim to achieve the same goal: patient-specific kinematics with individual harmony of alignment, soft-tissue, and morphology. The term ‘kinematic’ suggests that kinematics are the goal of KA, irrespective of the approach used, while ‘alignment’ suggests involvement of component alignment to fulfil the harmony.
Author contributions
T. Hiranaka: Writing – original draft, Conceptualization, Visualization.
Y. Suda: Writing – review & editing.
A. Saitoh: Writing – review & editing.
M. Koide: Writing – review & editing.
A. Tanaka: Writing – review & editing.
A. Arimoto: Writing – review & editing.
T. Fujishiro: Writing – review & editing.
K. Okamoto: Writing – review & editing.
Funding statement
The authors received no financial or material support for the research, authorship, and/or publication of this article.
ICMJE COI statement
T. Hiranka reports honoraria for presentations and instructions from Zimmer Biomet, unrelated to the present work.
Acknowledgements
The authors thank Benjamin Phillis at the Clinical Study Support Center, Wakayama Medical University for proofreading and editing.
© 2022 Author(s) et al. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial No Derivatives (CC BY-NC-ND 4.0) licence, which permits the copying and redistribution of the work only, and provided the original author and source are credited. See https://creativecommons.org/licenses/by-nc-nd/4.0/.
Contributor Information
Takafumi Hiranaka, Email: takafumi.hiranaka@gmail.com.
Yoshihito Suda, Email: y.suda834@gmail.com.
Akira Saitoh, Email: akira.saitoh0315@gmail.com.
Motoki Koide, Email: kokokoide4712@yahoo.co.jp.
Atsuki Tanaka, Email: atsuki.tanaka1991@gmail.com.
Akihiko Arimoto, Email: ariponanb@yahoo.co.jp.
Takaaki Fujishiro, Email: taka2446@yg8.so-net.ne.jp.
Koji Okamoto, Email: okamoto.kouji@aijinkai-group.com.
References
- 1. Howell SM, Howell SJ, Kuznik KT, Cohen J, Hull ML. Does a kinematically aligned total knee arthroplasty restore function without failure regardless of alignment category? Clin Orthop Relat Res. 2013;471(3):1000–1007. 10.1007/s11999-012-2613-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Howell SM. Calipered kinematically aligned total knee arthroplasty: an accurate technique that improves patient outcomes and implant survival. Orthopedics. 2019;42(3):126–135. 10.3928/01477447-20190424-02 [DOI] [PubMed] [Google Scholar]
- 3. Nedopil AJ, Howell SM, Hull ML. Kinematically Aligned Total Knee Arthroplasty Using Calipered Measurements, Manual Instruments, and Verification Checks. In: Rivière C, Vendittoli PA. Personalized Hip and Knee Joint Replacement. Cham: Springer, 2020: 279–300. [PubMed] [Google Scholar]
- 4. Brown JHM. Traction during total knee arthroplasty leads to a bone-conserving tibial resection: a retrospective comparative study. International Journal of Orthopaedics. 2020;7(3):1283–1288. 10.17554/j.issn.2311-5106.2020.07.345 [DOI] [Google Scholar]
- 5. Soda Y, Nakamura M, Adachi N. Coronal alignment of three different types of implants in kinematically aligned total knee arthroplasty: a comparative study. Open Journal of Orthopedics. 2021;11(6):183–198. 10.4236/ojo.2021.116018 [DOI] [Google Scholar]
- 6. Almaawi AM, Hutt JRB, Masse V, Lavigne M, Vendittoli PA. The impact of mechanical and restricted kinematic alignment on knee anatomy in total knee arthroplasty. J Arthroplasty. 2017;32(7):2133–2140. 10.1016/j.arth.2017.02.028 [DOI] [PubMed] [Google Scholar]
- 7. MacDessi SJ, Griffiths-Jones W, Chen DB, et al. . Restoring the constitutional alignment with a restrictive kinematic protocol improves quantitative soft-tissue balance in total knee arthroplasty: a randomized controlled trial. Bone Joint J. 2020;102-B(1):117–124. 10.1302/0301-620X.102B1.BJJ-2019-0674.R2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Clement ND, Calliess T, Christen B, Deehan DJ. An alternative technique of restricted kinematic alignment of the femur and gap balanced alignment of the tibia using computer aided navigation. Bone Joint Res. 2020;9(6):282–284. 10.1302/2046-3758.96.BJR-2020-0119.R1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Chang JS, Kayani B, Wallace C, Haddad FS. Functional alignment achieves soft-tissue balance in total knee arthroplasty as measured with quantitative sensor-guided technology. Bone Joint J. 2021;103-B(3):507–514. 10.1302/0301-620X.103B.BJJ-2020-0940.R1 [DOI] [PubMed] [Google Scholar]
- 10. Clement ND, Deehan DJ. Minimum reporting criteria for robotic assisted total knee arthroplasty studies: alignment and balancing techniques should both be defined. Bone Joint Res. 2020;9(6):279–281. 10.1302/2046-3758.96.BJR-2020-0033.R2 [DOI] [PMC free article] [PubMed] [Google Scholar]