

Abstract
Physical activity improves quality of life and extends independence in older adults. Yet, how to motivate older adults to engage in physical activity is unclear. In the present study, 4108 older women, aged 70–99, reported how they motivated themselves to move when they did not feel like it, and their hours of physical activity and walking each week. Findings indicated that participants who endorsed more strategies had more hours of physical activity and walking. Strategic categories that correlated with more physical activity include focusing on the benefits and utilizing the surrounding environment to help motivate movement.
Keywords: exercise, motivation, older adults, strategies, walking
Physical activity is an effective way to improve quality of life and extend independence in older adults (Fries, 2012; Kohl et al., 2012; Paúl et al., 2012; Powell et al., 2011). Less than 8% of women aged 75 and over met the national physical activity guidelines for both aerobic and muscle-strengthening activities from January to March 2016 based on the National Health Interview Survey (Katzmarzyk et al., 2017). Motivating physical activity does not have a static, single solution. A participant-based approach to identifying multiple successful strategies is to ask women what has worked to get them moving.
Increasing activity levels
Creating effective interventions to increase physical activity in older adults requires addressing age-related barriers. Aging is associated with chronic diseases, physical pain, and lower levels of physical functioning (Brawley et al., 2003; Fleg Jerome et al., 2005; Schrack et al., 2010, 2014; Studenski et al., 2011), which make movement challenging. Furthermore, older adults report fear of falling, fear of pain, and concern for neighborhood safety as barriers (Brawley et al., 2003; Grossman and Stewart, 2003; Lees et al., 2005).
In addition to addressing barriers, it is also necessary to understand what motivates older adults to move (Bennett and Winters-Stone, 2011; Campbell et al., 2001; Chase, 2015; Cousins, 2000; French et al., 2014; Freund et al., 2010). For instance, Freund et al. (2010) found older adults preferred messages that focus on the process of exercise, rather than the health-related outcomes. Campbell et al. (2001) found older adults ranked “to feel mentally alert” higher than “to improve or maintain health” compared to younger adults. Yardley et al. (2006) found the benefits of enjoyment and improved independence were strong motivators for adults 67–99.
The present study
In the present study, we focused on motivation. In particular, we investigated the strategies that older women report using when they do not feel like moving using a subgroup of women from the Women’s Health Initiative (WHI) Strong and Healthy trial (WHISH) (The Women’s Health Initiative Study Group, 1998). In coding our participants’ free-response strategies, we distinguished two major types: Those that occur inside the head, or “Internal” strategies, and those that use the world as a prop, or “External” strategies (Duckworth et al., 2016; Oppezzo and Schwartz, 2013). An Internal strategy targets one’s thoughts about the active behavior, for example reminding oneself how good it is for bodies to move, or reminding oneself “you’ve done this before, and you can do it again.” An External strategy utilizes the world to help motivate the behavior, for example leaving tennis shoes by the door, or setting an hourly alarm to remind oneself to stretch. Oppezzo and Schwartz (2013) proposed that External strategies are particularly valuable when willpower is at its weakest. Duckworth et al. (2014, 2016) posited that External strategies can be especially effective because they operate early in the behavioral timeline, before psychological impulses to avoid the activity have grown too strong, or before willpower may be weakened.
Our first aim was to identify strategies older women used to increase physical activity and categorize them according to Internal or External. Inductive coding methods were also used to reveal distinctive subcategories as they emerged. Our second aim was to test the link between strategies and physical activity levels. Aim 2a was to identify the relation between the overall number of strategies and physical activity. We hypothesized that the overall number of strategies women reported would be associated with higher average hours of self-reported amount (hours of physical activity per week) and intensity (MET-hours of walking) per week. Aim 2b was to identify how the number of Internal strategies and External strategies relate to physical activity. We hypothesized that External, but not Internal, strategies would correlate with greater amount and intensity of activity.
We also explored relations among subcategories of the Internal and External strategies and physical activity. Eight subcategories of responses emerged with the coding: Three for Internal, two for External, and three for non-actionable strategies (Other). We examined which subcategories were associated with the highest levels of physical activity, and whether that differed for amount and intensity. We also coded whether strategies had a social component, as social strategies predict higher levels of activity (Cutt et al., 2007; Moudon et al., 2007).
Method
Participants
Participants came from a parent physical activity intervention, the WHISH trial (ClinicalTrials.gov: NCT02425345), a pragmatic randomized controlled trial testing whether an intervention designed to deliver the National Institute of Health’s Department of Health and Human Services Physical Activity Guidelines (U.S. Department of Health and Human Services, 2008, 2018) reduces major cardiovascular events in older women. WHISH is embedded in the Women’s Health Initiative-Extension Study (see Supplemental Materials). A postcard was sent to the 19,598 WHISH intervention participants ages 70–99 years. The subgroup of women who returned return the postcard had higher average education level, greater amount and intensity of physical activity per week, and were younger than those who did not return the postcard, with no significant differences in race and ethnicity (see Supplemental Materials). We present data from the 4108 respondents (20.9%).
Procedure
In January 2018 WHISH intervention participants were mailed their quarterly physical activity newsletter, a pedometer with a belt clip, a notepad for goal setting, and the postcard. One side of the postcard had a checkbox to order a free pedometer belt. The flip-side had an optional, single, open-ended prompt (see below) with space for a written response. Participants could receive the free belt without answering this question. In addition, physical activity data were collected over the course of a year, May 2017 to May 2018 as subsets of already occurring annual WHISH questionnaires sent to participants as scheduled.
Measures
Demographic measures.
Baseline demographic data (age, ethnicity, race, education, region) were collected as part of the WHISH database.
Strategies for movement.
The postcard prompt was: “Think about the last time you didn’t feel like being active. How did you get yourself to move or get up?”
Self-reported physical activity.
The WHISH women receive annual surveys asking questions on physical activity and health. Amount of physical activity per week was calculated summing self-reported hours of physical activity on a subset of the Community Healthy Activities Model Program for Seniors (CHAMPS) physical activity questionnaire for older adults (Stewart et al., 2001), including 16 activities of various intensities (from light to vigorous walking, swimming, biking, housework/errands, flexibility exercises etc.); responses totaling more than 5 hours per day were removed per guidelines (Stewart et al., 2001). To assess intensity of physical activity, we used MET-hours of walking per week based on a standardized classification of the energy costs of different physical activities in Ainsworth et al.’s (1993) Compendium of Physical Activities. MET-hours of walking were calculated using three questions asking about intensities of >10 minute walking bouts (see Supplemental Materials).
Physical activity amount and intensity were analyzed as separate dependent measures.
Data reduction
Primary analyses.
Aim 1 was to identify motivational strategies older women use to increase physical activity. The development of the coding scheme and resulting coding process was iterative (see Supplemental Materials). In line with Oppezzo and Schwartz (2013) and Duckworth et al. (2016), the two broad categories were: Internal and External. Additional mutually exclusive subcategories emerged that provided more refined distinctions within the Internal and External broader categories. All Kappas on initial ratings were above 0.8 for 400 random responses (~10% of the dataset) except for three subcategories of responses: “Unclear,” “Nothing Worked,” and “Passive,” which were then jointly discussed given low base rates.
For our second aim, we tallied strategies endorsed by Internal and External strategies together (aim 2a), or all Internal and all External subcategories (aim 2b).
Secondary analyses.
For exploratory aim 1, each subcategory was collapsed into a binary score of present or absent. For exploratory aim 2, we added a “Social” qualifying code to each Internal and External strategy that referenced a motivator that involves another being (person or pet). Kappa for this binary code was 0.91.
Data analyses
Preliminary analyses.
Correlations and an ANCOVA tested the effect of age, education, and region on the two physical activity measures.
Primary analyses.
For aim 1, frequencies describe the relative percentages within subcategories, either of number of responses (4842) or number of women (4108) (some women reported more than one strategy). For aim 2a, we used a linear regression to identify associations between total number of strategies against amount and intensity of physical activity. To test aim 2b, we used a linear regression with number of Internal strategies, number of External strategies, and their interaction term.
Secondary analyses.
For exploratory aim 1, a linear regression analyzed the relationships between subcategory of strategy and amount and intensity of physical activity. For exploratory aim 2, we used ANOVAs with social coding as a factor on the dependent measures of amount and intensity of activity.
For a given analysis, the sample size deviated from the 4108 postcard responders in three ways: exclusion for incomplete survey data; exclusion for analyses of walking due to wheelchair ambulation (n = 4); and exclusion for analyses on strategies of responses without actual strategies listed (Motivation Not an Issue, Described Condition, and Unclear). For aim 2b, we also excluded those who reported that nothing they tried got them moving, “Nothing Worked,” where social components could not be determined.
Data sharing statement
The current article includes the complete raw dataset collected in the study including the participant responses, data analyses syntax file, data analysis log files for analysis, and coding scheme. Pending acceptance for publication, all of the data files will be automatically uploaded to the Figshare repository.
Results
Preliminary analyses
Table 1 provides the demographics of the 4108 women. They averaged 7.9 (SE = 0.1) hours of physical activity per week and 5.2 (SE = 0.1) MET-hours of walking per week. They were modestly correlated; r = 0.44, p < 0.001. An ANCOVA tested differences in physical activity for those with complete data for age, education, and region, F(6, 3802) = 27.4, p < 0.001, with significant main effects of age, F(1, 3802) = 66.0, p < 0.001, and education, F(2, 3802) = 42.3, p < 0.001, but no significant effects of region, F(3, 3802) = 0.500, p = 0.682. Age had a small, negative correlation, r = −0.136, p < 0.001, with amount of activity. The same model, on MET-hours of walking per week was significant, F(6, 3835) = 31.2, p < 0.001, with significant main effects of age, F(1, 3835) = 140.2, p < 0.001, education, F(2, 3835) = 15.04, p < 0.001, and region F(3, 3835) = 2.61, p = 0.050. Age had a small, negative correlation, r = −0.191, p < 0.001, with MET-hours of walking per week (see Supplemental Materials).
Table 1.
Sample demographics and characteristics.
| Characteristic | Total sample n, within characteristic (%) | M (SE), range |
|---|---|---|
|
| ||
| Age | 4108 | 81.2 (0.1), 70–99 |
| Education | 4069 | |
| High school or less | 538, 13 | |
| School after high school | 1408, 35 | |
| College degree or higher | 2123, 52 | |
| Race/ethnicity | 4092 | |
| White | 3359, 82 | |
| African American | 426, 10 | |
| Hispanic | 145, 4 | |
| Asian/Pacific Islander | 97, 2 | |
| Native American/Native Alaskan | 20, 4 | |
| Other/unknown | 45, 1 | |
| Region | 4092 | |
| Northeast | 1165, 28 | |
| Southeast | 862, 21 | |
| Midwest | 1034, 25 | |
| West | 1031, 25 | |
Due to effects of age, education, and region on the measures of activity, we controlled for them to identify the unique effects of number and type of strategies on activity levels.
Primary analyses
Aim 1.
Across respondents, 604 listed more than one strategy in their response, yielding 4842 total codable strategies. The coding categories are in Table 2, with more detail in the Supplemental Materials. Each Internal strategy was coded into the following subcategories: Intrapsychic (self-encouraging talk and cognitive reframing, among others); Avoid Bad (cons of non-movement); Approach Good (pros of movement). External strategies were either: Manipulate (change the environment to encourage motivation or facilitate the movement); or Capitalize (use something already in place in the environment, like a role as a pet-owner).
Table 2.
Category descriptions and examples.
| Category | Subcategory | Description | Example |
|---|---|---|---|
|
| |||
| Internal | Intrapsychic | Self-talk; reframing; mindset; prayer; general goals. | • “I gave myself a good talking’ to” • “I remembered how important it is to be physically active” • “He never gave up till cancer hit him! Thought of my husband, now deceased. He LOVED going to the gym 3× per week, health allowing” |
| Avoid bad | Try to avoid a future negative outcome; focus on the cons of not moving. | • “I thought about my sister who is much younger than me and in a wheelchair because she never moved” • “My doctor told me I could either move or start taking blood pressure medication. . .” • “I don’t want to gain weight and have to buy new clothes!” |
|
| Approach good | Look forward to an outcome; focus on a future benefit. | • “I remember how much better I feel when I take a walk” • “I want to be able to keep up with my grandchildren!” • “Exercise is good for me- for my blood sugar, my mental health” |
|
| External | Manipulate | Active manipulation of world with putting things place to help activity. For example: rewards, reminders, visible tracking (e.g. pedometer step count), specific visibly achieved goals, partner reinforcement, time-triggered routine, gym membership. | • “I set a timer for 30 minutes and get up each time it goes off” • “I am a part of SilverSneakers and take a class at the YMCA 3 times a week” • “I promise myself a small treat if I go for my walk” |
| Capitalize | Making use of something in the world one did not place ahead of time for exercise motivation. For example: chores to do, role as caretaker or pet owner. | • “I am my husband’s caretaker, so I’m always on the move” • “I take my dogs for their daily walk” • “I look at the mess around me and decide to get up and do some cleaning” |
|
| Other | Just do it | Reference to willpower, forcing oneself, “just did it.” | • “I just did it” • “I forced myself” • “Willpower” |
| Passive | Participant ended up moving, but not of own accord, strategy, or intervention. | • “The doorbell rang” • “The sun was out – blue skies and appropriate temperature. I love spring.” “What got me up was the need to empty my bladder.” |
|
| Nothing worked | Nothing worked for the recalled time to get them up and moving. | • “Unfortunately, I didn’t because of the pain. I’ll try again” • “I didn’t.” • “Still working on it. . .” |
|
| Non strategy codes | Motivation not an issue | Respond that motivation is not a problem, no strategy given. | • “I never have had any problem exercising. I’m always physically active!” • “No problem with motivation” • “I’m always active. I love it” |
| Described condition | A description of one’s health situation. | • “I had back surgery last month. The pain was bad but it is getting better” • “It’s hard for me to get up when I sit low. I take a hot bath to help my knee” • “Had a few falls, which has affected my balance. I’m not nearly as active as I used to be.” |
|
| Unclear | Unclear response, appeared to misunderstand prompt | ||
Responses that were either non-actionable strategies or not under women’s control received a code of “Other.” These were “Just Do It” (referenced willpower or forcing oneself, which bypasses the motivational part of the strategy); “Passive” (something happening in the world that resulted in behavior change); “Nothing Worked” (no strategy listed). Finally, responses that were irrelevant were called Non-Strategy Codes, and included: Motivation not an Issue, Described Condition, and Unclear.
Table 3 shows the frequencies of subcategories by both number of people who reported them and number of responses that used them. Most of the strategies could be coded as Internal or External, with only ~4% of strategies as Other. The most frequently reported strategy was Manipulate, making External strategies the most common category. Of the Internal strategies, Approach Good and Avoid Bad were similar in their frequency. The average number of strategies was 1.08(SE = 0.01). Most women reported one strategy, with ~15% of the participants reporting two or more strategies.
Table 3.
Frequencies of subcategories.
| Category | Subcategory | % of 4108 participants* | % of 4842 responses |
|---|---|---|---|
|
| |||
| Internal | Intrapsychic | 12.6 | 10.9 |
| Avoid bad | 14.4 | 12.4 | |
| Approach good | 14.9 | 13.4 | |
| External | Manipulate | 46.7 | 45.0 |
| Capitalize | 7.3 | 7.1 | |
| Other | Just do it | 3.4 | 2.9 |
| Passive | 0.9 | 0.7 | |
| Nothing worked | 0.9 | 0.7 | |
| Non-strategy codes | Motivation not an issue | 2.5 | 2.1 |
| Described condition | 2.3 | 1.9 | |
| Unclear | 3.2 | 2.7 | |
Percentages of participants total to more than 100% because a participant could be counted twice if they had more than one category of response.
Aim 2a.
We hypothesized that total number of strategies women reported would be associated with higher levels of self-reported physical activity (see Figure 1a and b). For both amount and intensity, there is a steady increase by number of strategies until four or more strategies, where there are diminishing returns. A linear regression with total number of strategies, age, and education as an independent factor on amount had a significant overall model fit of R2 = 0.044, F(3, 3339) = 50.87, p < 0.001. Number of strategies (Beta = 0.091, p < 0.001), age (Beta = −0.117, p < 0.001), and education (Beta = 0.133, p < 0.001) correlated with amount. The same model, additionally controlling for region, on intensity had a significant overall model fit of R2 = 0.045, F(4, 3363) = 39.86, p < 0.001. Number of strategies (Beta = 0.050, p = 0.003), age (Beta = −0.18, p < 0.001), and education (Beta = 0.076, p < 0.001) significantly correlated with intensity per week; region (Beta = 0.027, p = 0.108) did not.
Figure 1.
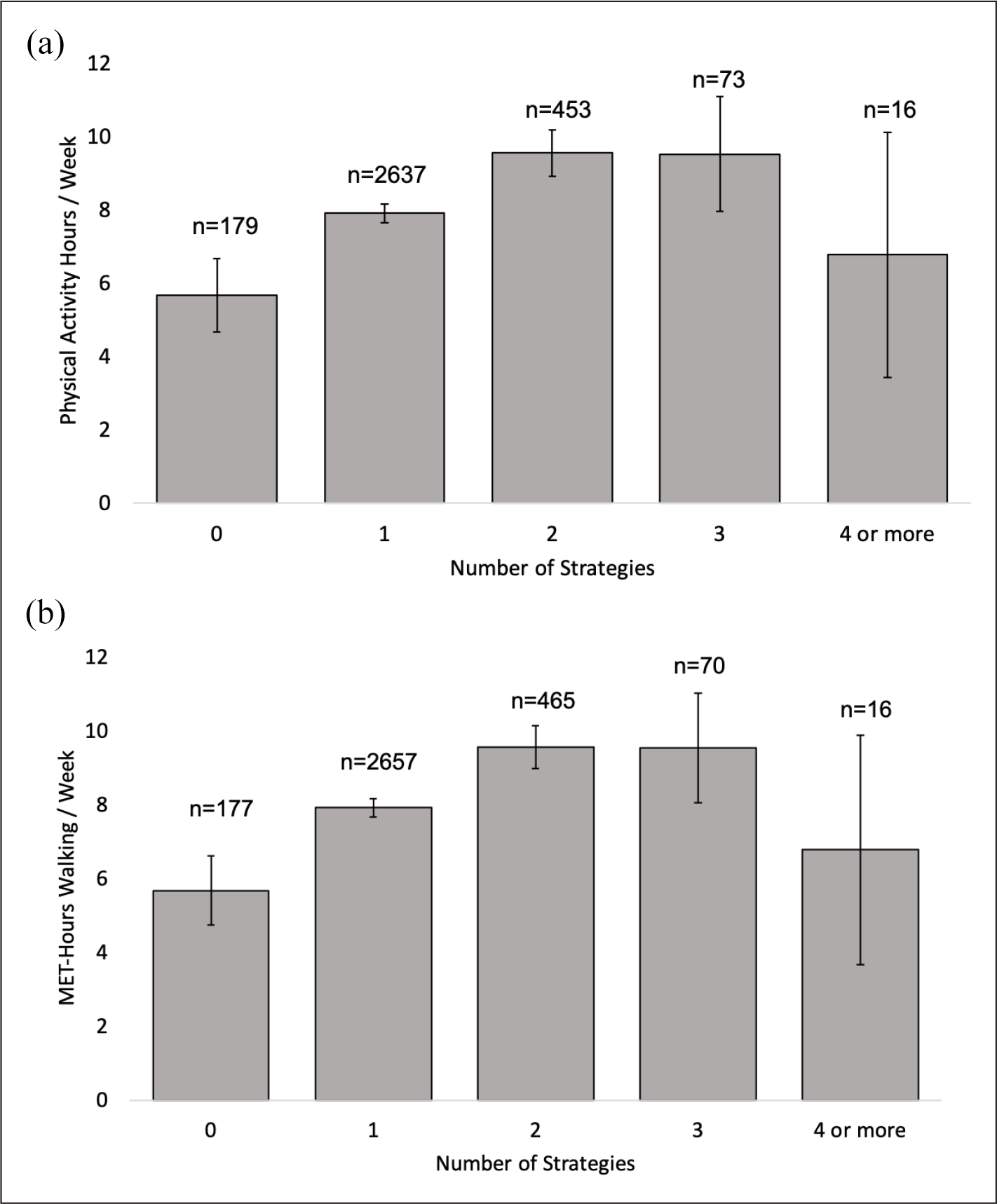
(a) Physical activity hours per week × number of strategies. (b) MET-hours of walking per week × number of strategies.
Error bars represent 95% confidence intervals. Sample size n’s refer to number of women who reported that number of strategies.
Aim 2b.
We hypothesized that the number of External strategies endorsed would correlate with higher levels of self-reported physical activity. A linear regression with Internal strategies (tallied participant’s Internal strategies), External (tallied participant’s External strategies), an interaction term of Internal × External, controlling for age and education on amount had a significant overall model fit of R2 = 0.042, F(5, 3337) = 30.58, p < 0.001. Internal (Beta = 0.10, p < 0.001), External (Beta = 0.121, p < 0.001), age (Beta = −0.117, p < 0.001), and education (Beta = 0.133, p < 0.001) significantly correlated with amount. The interaction term was not significant (Beta = −0.016, p = 0.445). Both the number of Internal and number of External strategies are associated with more activity hours, but that there were no interactive effects, meaning that the impact of one did not depend on the impact of the other. Also, the effect of the number of Internal strategies is not appreciably different from number of External strategies.
The same model, additionally controlling for region, on intensity had a significant the overall model fit of R2 = 0.047, F(6, 3361) = 27.48, p < 0.001. Only External strategies (Beta = 0.084, p = 0.001), age (Beta = −0.183, p < 0.001), and education (Beta = 0.076, p < 0.001) showed a significant relationship. Internal (Beta = 0.040, p = 0.117), the interaction term (Beta = −0.012, p = 0.551), and region (Beta = 0.026, p = 0.117) were not significant. External consistently correlated with physical activity for both amount and intensity. Again, the total number of strategies matters more than the number of a particular category.
Secondary analyses
To address our exploratory aims, we sought to identify which of the subcategories correlated with the highest levels of self-reported physical activity (see Figure 2a and b).
Figure 2.
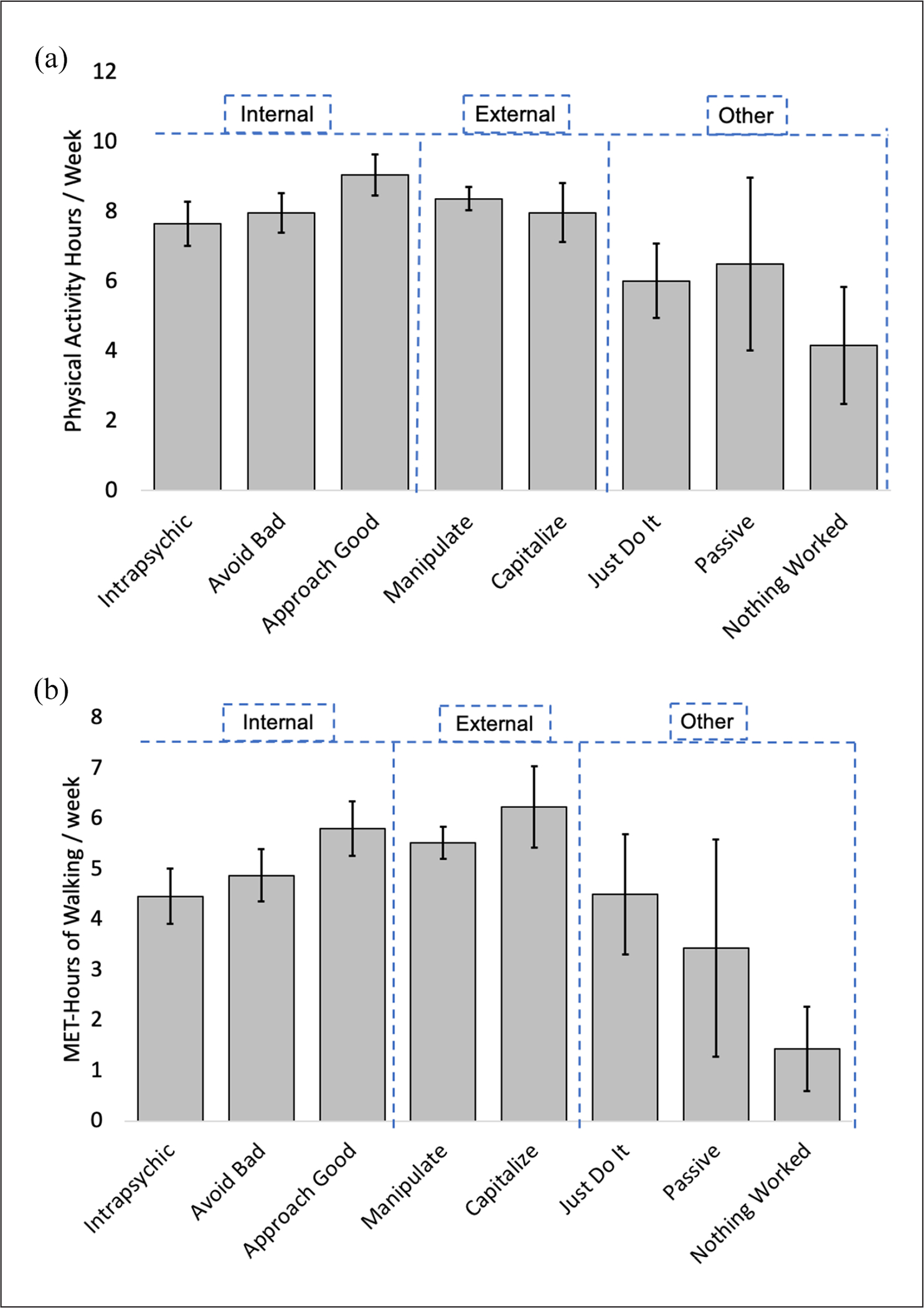
(a) Average physical activity hours per week × strategy category. (b) Average MET-hours of walking per week × strategy category.
Error bars represent 95% confidence intervals. If a participant reported both an avoid bad and approach good, her physical activity score would contribute to each subcategory’s average.
Internal and External subcategories largely fall within the 95% confidence intervals of each other. The exception is those who report Approach Good strategies appear to have more activity hours per week than those using Avoid Bad or other Intrapsychic strategies. The smaller sized groups who reported Just Do It, Passive, or Nothing Worked, also show fewer activity hours compared to those using the more active Internal or External strategies.
Figure 2b indicates for MET-hours of walking per week, Approach Good remains the highest of the Internal strategies, with no overlap in their 95% CI. The women reporting External strategies report similar MET-hours of walking both within subcategories of Capitalize and Manipulate, as well as those reporting Approach Good.
A linear regression with each subcategory as independent variables, controlling for age and education on amount had an overall model fit of R2 = 0.046, F(10, 3332) = 16.00, p < 0001. Approach Good (Beta = 0.089, p < 0.001), Manipulate (Beta = 0.081, p = 0.008), and education (Beta = 0.130, p < 0.001) were significantly positively correlated, and Nothing Worked (Beta = −0.035, p = 0.047) and age (Beta = −0.114, p < 0.001) were significantly negatively correlated with activity hours. Intrapsychic (Beta = 0.018, p = 0.436), Avoid Bad (Beta = 0.035, p = 0.153), Capitalize (Beta = 0.029, p = 0.164), Just Do It (Beta = −0.021, p = 0.315), and Passive (Beta = −0.007, p = 0.700) were not significantly correlated.
The same model, additionally controlling for region, on intensity had an overall model fit of R2 = 0.051, F(11, 3356) = 17.26, p < 0.001. Approach Good (Beta = 0.069, p = 0.004), Manipulate (Beta = 0.078, p = 0.010), Capitalize (Beta = 0.072, p = 0.001), and education (Beta = 0.074, p < 0.001) significantly positively correlated, and Nothing Worked (Beta = −0.040, p = 0.022) and age (Beta = −0.181, p < 0.001) significantly negatively correlated with intensity. Intrapsychic (Beta = −0.003, p = 0.890), Avoid Bad (Beta = −0.017, p = 0.483), Just Do It (Beta = 0.016, p = 0.430), Passive (Beta = −0.010, p = 0.585), and region (Beta = 0.025, p = 0.142) were not significantly correlated.
Exploratory aim 2 compared strategies that have social components to those that do not among both Internal and External strategies and their relative correlation with self-reported physical activity. Of the 4108 women, 784 (19%) endorsed a social motivation strategy, and 673 (86%) of the social strategies were External strategies.
An ANCOVA of Social versus Non Social, controlling for age and education, on activity hours was a significant overall model F(4, 3318) = 31.9, p < 0.001, but only age, F(1, 3318) = 48.96, p < 0.001, and education, F(2, 3318) = 34.05, p < 0.001, had significant effects. Social, F(1, 3318) = 1.50, p = 0.221, had no significant effect. The same model, additionally controlling for region, on intensity, however, showed a significant model, F(7, 3339) = 23.06, p < 0.001, and significant effects of Social, F(1, 3339) = 6.37, p = 0.012, and age, F(1, 3339) = 119.89, p < 0.001, and education, F(2, 3339) = 9.90, p < 0.001. Region had no significant effect, F(3, 3339) = 1.99, p = 0.113. The mean (SE) walking METs for those who reported a social strategy was 5.8 (0.24), and those who did not was 5.1 (0.12). One speculation for this difference between the analyses on the amount and the intensity (walking METs) is that walking is among the physical activities most amenable to partners (e.g. walking buddies), and 196 (25%) of the social responses involved a dog, shown to increase walking (Cutt et al., 2008). Therefore, those who report walking more may be more likely to have a social strategy they use.
In sum, Approach Good and Manipulate were consistent correlates across both measures of physical activity per week. Capitalize was a less consistent correlate, as it only significantly correlated with intensity. Nothing Worked, or the absence of successful strategies, consistently correlated with fewer hours for both outcomes. Social strategies only correlated with intensity.
Discussion
Older adults have low activity levels and face a number of unique barriers to increasing activity levels. It is therefore critical to identify strategies that are effective in this age group. To address this issue, we asked a diverse group of older women about their physical activity strategies that got them moving the last time they did not feel like it.
The most common strategies fell into External: Manipulate (e.g. change the world around them in advance to facilitate the physical activity). Endorsing more strategies was associated with higher amounts and intensity of physical activity, with effects diminishing at four or more strategies. Use of Internal strategies correlated with the amount of physical activity, while External strategies were a consistent correlate of physical activity amount and intensity. Particularly well-associated subcategories of strategies were Approach Good (e.g. looking for future benefits of activity), Manipulate, and Capitalize (e.g. using something already in the world to help motivate movement). Social strategies did not correlate with amount, but notably did correlate with intensity as measured by walking METs, likely due to walking being an easily sociable task with either a walking buddy or a dog.
Theoretical implications
Our findings that External strategies may be more effective for motivating behavior initiation than Internal lends support to Duckworth et al.’s (2014) process model of self-control. The findings also extend the phenomena of distributed cognition to the motivation domain. People can offload cognitive demands into the environment. For example, people may leave their index finger on a portion of text as they look away. Their finger eliminates the need to use cognitive energy to keep in mind where they left off reading as they momentarily shift attention to something else (for a review, see Pea, 1993). Similarly, people can offload a high demand for motivational energy by putting components of the motivation into the environment (Oppezzo and Schwartz, 2013). The possibility of distributing motivational energy should be particularly useful for older populations, when physical barriers to exercise require greater motivation to overcome.
Practical and clinical implications
An implication from these findings is that helping people adopt multiple strategies, thus having more than one to choose from, may help motivate physical activity. An intervention to test causality might teach one group a single strategy to practice, and another three strategies to interchange, then compare subsequent physical activity.
There are also implications for physical activity messaging. The positive association with Approach Good and physical activity aligns with Notthoff and Carstensen (2014) where highlighting physical activity benefits (Approach Good) proved more effective than noting the sedentary behavior risks (Avoid Bad). Likewise, work by McArthur et al.(2014), and Holahan et al. (2020) found that anticipating positive emotions, an Approach Good strategy, has been shown to help to motivate women to engage in regular leisure-time physical activity. Practically, intervention messaging for older women might shift away from a common message of “move it or lose it” which focuses on the potential perils of being sedentary; instead, encouraging women to an equally catchy positive framing of “choose to move it” or “move towards a good mood” may have more success.
The relatively low frequency of “Just Do It” and willpower responses contradicts many exercise motivational statements and campaigns (Nayak, 2017). While Nike may try to motivate us to “Just Do It,” for an older adult population, forcing oneself was not a commonly reported successful motivational tool. Designing campaigns that focus on a more agentic, strategic approach to initiating physical activity may have more successful uptake.
The association between social component strategies and walking MET-hours supports other work demonstrating social support, and even dog ownership, affects walking (Cutt et al., 2007; Moudon et al., 2007). Interventions designed to increase walking in older women could suggest walking partners, or note health benefits of owning a dog beyond increased physical activity (e.g. perceived social support, heart health, decreased depression rates, decreased loneliness, Knight and Edwards, 2008).
The broadly classified External strategies appear useful for older women. Clinically, while the association for External strategies on intensity was small (for every External strategy there was a 0.08 increase in MET-hours, which is about 5 minutes), the biggest effect of physical activity for older adults is the difference between inactivity and any activity (Manson et al., 1999). Indeed, relatively small amounts of exercise can yield significant health benefits. The Nurse’s Health Study found only 1–1.9 hours of weekly moderate to vigorous exercise had an adjusted Risk Ratio of 0.82 (95% CI 0.76–0.89, Trolle-Lagerros et al., 2005). Further, Soares-Miranda et al. (2016) found heart disease risk reduction in older adults (HR 0.7, 95% CI 0.58–0.83) for walking as little as 6–12 blocks per week, or about a block a day. (Note: hazard ratio of 0.7 means those who walked had a 0.7% chance of getting heart disease as those who did not walk.) Therefore, even if the movement difference from using an External motivation strategy is small, it can still be clinically meaningful.
Strengths, limitations, and future directions
Notably, this study has a large and diverse sample of older women. We produced a reliable codebook for reducing over 4000 motivational strategies into manageable, mutually exclusive categories, useful to researchers in this space. Two broad categories of Internal and External captured 88.8% of the responses. Our cross-sectional study has laid the groundwork for future causal comparison of these classes of strategies.
Our findings are limited to the older women of this sample who returned the postcard, already active enough to request a belt for their pedometer, and were more active and younger than those who did not respond. The prompt was an optional add-in to regular mailing, but future work could integrate into regular WHISH surveys for a less biased sample. Considering limitations of self-report, more objective measures of activity with accelerometers is warranted. Finally, the prompt had several limitations. The short, singular prompt may have minimized participant burden, yet it only solicited successful strategies, not unsuccessful ones. Knowing what did not work can be equally useful for intervention design. Additionally, the prompt was retrospective, which limits directional inferences, though minimizing the risk of real-time tracking where one might change the behavior they are monitoring. Using ecological momentary assessments would instead allow participants to share in-the-moment strategies as they are used at various points throughout the day.
Future studies can use our coding scheme to classify strategies for their participants, simplifying the report of what works and when. An informative direction would be to identify physical and psychological conditions where each category or subcategory works best, and when they fail. For example, perhaps an Approach Good strategy works better than an Avoid Bad strategy when fatigue is high, but Avoid Bad may be more successful when one is experiencing acute physical pain. For activities like walking, Social and Manipulate strategies may work best, but for strength training, an Approach Good may be more effective. Finally, adding a prompt that asks about maintenance of physical activity once initiated (e.g. how do you keep yourself moving once you get going?) would explore differences between strategies that start activity and those that keep it going.
Knowing that having more than one motivational trick in the bag, utilizing the world for help, and positively framing physical activity may help overcome inertia is a great first step towards developing interventions to help older adults motivate their physical activity. Given that even small amounts of exercise conferring cardiovascular benefits and extending functional quality of life, every step counts (Fries, 2012; Paúl et al., 2012).
Supplementary Material
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially funded by National Heart, Lung, and Blood Institute of the National Institute of Health under Award Number K01HL136702. The Women’s Health Initiative (WHI) Strong and Healthy (WHISH) trial is funded by the National Heart, Lung, and Blood Institute (NHLBI), National Institutes of Health (NIH), U.S. Department of Health and Human Services (DHHS) through U01 HL122280-CCC and U01 HL122273-DCC. The WHI program is funded by NHLBI, NIH, US DHHS through contracts HHSN268201600018C, HHSN268201600001C, HH SN268201600002C, HHSN268201600003C, and HHSN268201600004C. These sponsors were not involved in any of the research or analyses.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
- Ainsworth BE, Haskell WL, Leon AS, et al. (1993) Compendium of physical activities: Classification of energy costs of human physical activities. Medicine and Science in Sports and Exercise 25(1): 71–80. [DOI] [PubMed] [Google Scholar]
- Bennett JA and Winters-Stone K (2011) Motivating older adults to exercise: What works? Age and Ageing 40(2): 148–149. [DOI] [PubMed] [Google Scholar]
- Brawley LR, Rejeski WJ and King AC (2003) Promoting physical activity for older adults: The challenges for changing behavior. American Journal of Preventive Medicine 25(3, Supplement 2): 172–183. [DOI] [PubMed] [Google Scholar]
- Campbell PG, MacAuley D, McCrum E, et al. (2001) Age differences in the motivating factors for exercise. Journal of Sport and Exercise Psychology 23(3): 191–199. [Google Scholar]
- Chase JAD (2015) Interventions to increase physical activity among older adults: A meta-analysis. The Gerontologist 55(4): 706–718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cousins SO (2000) “My Heart Couldn’t Take It”: Older women’s beliefs about exercise benefits and risks. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 55(5): P283–P294. [DOI] [PubMed] [Google Scholar]
- Cutt H, Giles-Corti B, Knuiman M, et al. (2007) Dog ownership, health and physical activity: A critical review of the literature. Health & Place 13(1): 261–272. [DOI] [PubMed] [Google Scholar]
- Cutt H, Giles-Corti B, Knuiman M, et al. (2008) Understanding dog owners’ increased levels of physical activity: Results from RESIDE. American Journal of Public Health 98(1): 66–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duckworth AL, Gendler TS and Gross JJ (2014) Self-control in school-age children. Educational Psychologist 49(3): 199–217. [Google Scholar]
- Duckworth AL, Gendler TS and Gross JJ (2016) Situational strategies for self-control. Perspectives on Psychological Science: A Journal of the Association for Psychological Science 11(1): 35–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duckworth AL, Milkman KL and Laibson D (2018) Beyond willpower: Strategies for reducing failures of self-control. Psychological Science in the Public Interest 19(3): 102–129. [DOI] [PubMed] [Google Scholar]
- Fleg Jerome L, Morrell Christopher H, Bos Angelo G, et al. (2005) Accelerated longitudinal decline of aerobic capacity in healthy older adults. Circulation 112(5): 674–682. [DOI] [PubMed] [Google Scholar]
- French DP, Olander EK, Chisholm A, et al. (2014) Which behaviour change techniques are most effective at increasing older adults’ self-efficacy and physical activity behaviour? A systematic review. Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine 48(2): 225–234. [DOI] [PubMed] [Google Scholar]
- Freund AM, Hennecke M and Riediger M (2010) Age-related differences in outcome and process goal focus. European Journal of Developmental Psychology 7(2): 198–222. [Google Scholar]
- Fries JF (2012) The theory and practice of active aging. Current Gerontology and Geriatrics Research 2012: 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grossman M and Stewart A (2003) “You aren’t going to get better by just sitting around”: Physical activity perceptions, motivations, and barriers in adults 75 years of age or older. The American Journal of Geriatric Cardiology 12: 33–37. [DOI] [PubMed] [Google Scholar]
- Holahan CK, Holahan CJ, Chen YT, et al. (2020) Leisure-time physical activity and affective experience in middle-aged and older women. Journal of Women & Aging 32(6): 1–12. [DOI] [PubMed] [Google Scholar]
- Katzmarzyk PT, Lee I-M, Martin CK, et al. (2017) Epidemiology of physical activity and exercise training in the United States. Progress in Cardiovascular Diseases 60(1): 3–10. [DOI] [PubMed] [Google Scholar]
- Knight S and Edwards V (2008) In the company of wolves: The physical, social, and psychological benefits of dog ownership. Journal of Aging and Health 20(4): 437–455. [DOI] [PubMed] [Google Scholar]
- Koeneman MA, Verheijden MW, Chinapaw MJM, et al. (2011) Determinants of physical activity and exercise in healthy older adults: A systematic review. The International Journal of Behavioral Nutrition and Physical Activity 8: 142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kohl HW 3rd, Craig CL, Lambert EV, et al. (2012) The pandemic of physical inactivity: Global action for public health. The Lancet 380(9838): 294–305. [DOI] [PubMed] [Google Scholar]
- Lees FD, Clark PG, Nigg CR, et al. (2005) Barriers to exercise behavior among older adults: A focus-group study. Journal of Aging and Physical Activity 13(1): 23–33. [DOI] [PubMed] [Google Scholar]
- Manson JE, Hu FB, Rich-Edwards JW, et al. (1999) A prospective study of walking as compared with vigorous exercise in the prevention of coronary heart disease in women. The New England Journal of Medicine 341(9): 650–658. [DOI] [PubMed] [Google Scholar]
- McArthur D, Dumas A, Woodend K, et al. (2014) Factors influencing adherence to regular exercise in middle-aged women: A qualitative study to inform clinical practice. BMC Women’s Health 14(1): 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moudon AV, Lee C, Cheadle AD, et al. (2007) Attributes of environments supporting walking. American Journal of Health Promotion 21(5): 448–459. [DOI] [PubMed] [Google Scholar]
- Nayak T (2017) “Just Do It”@Ad campaign: The case of Nike Inc. Globsyn Management Journal 11(1/2): 59–66. [Google Scholar]
- Notthoff N and Carstensen LL (2014) Positive messaging promotes walking in older adults. Psychology and Aging 29(2): 329–341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oppezzo M and Schwartz DL (2013) A behavior change perspective on self-regulated learning with teachable agents. In: International Handbook of Metacognition and Learning Technologies. Springer, pp.485–500. [Google Scholar]
- Paúl C, Ribeiro O and Teixeira L (2012) Active ageing: An empirical approach to the WHO model. Current Gerontology and Geriatrics Research 2012: 382972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pea RD (1993) Practices of distributed intelligence and designs for education. Distributed Cognitions: Psychological and Educational Considerations 11: 47–87. [Google Scholar]
- Powell KE, Paluch AE and Blair SN (2011) Physical activity for health: What kind? How much? How intense? On top of what? Annual Review of Public Health 32: 349–365. [DOI] [PubMed] [Google Scholar]
- Schrack JA, Knuth ND, Simonsick EM, et al. (2014) “IDEAL” aging is associated with lower resting metabolic rate: The Baltimore longitudinal study of aging. Journal of the American Geriatrics Society 62(4): 667–672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schrack JA, Simonsick EM and Ferrucci L (2010) The energetic pathway to mobility loss: An emerging new framework for longitudinal studies on aging. Journal of the American Geriatrics Society 58(s2): S329–S336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soares-Miranda L, Siscovick DS, Psaty BM, et al. (2016) Physical activity and risk of coronary heart disease and stroke in older adults: The cardiovascular health study. Circulation 133(2): 147–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stewart AL, Mills KM, King AC, et al. (2001) CHAMPS physical activity questionnaire for older adults: Outcomes for interventions. Medicine & Science in Sports & Exercise 33(7): 1126–1141. [DOI] [PubMed] [Google Scholar]
- Studenski S, Perera S, Patel K, et al. (2011) Gait speed and survival in older adults. JAMA 305(1): 50–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Women’s Health Initiative Study Group (1998) Design of the Women’s Health Initiative Clinical Trial and Observational Study. Controlled Clinical Trials 19(1): 61–109. [DOI] [PubMed] [Google Scholar]
- Trolle-Lagerros Y, Mucci LA, Kumle M, et al. (2005) Physical activity as a determinant of mortality in women. Epidemiology 16(6): 780–785. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services (2008) Physical Activity Guidelines for Americans. Washington, DC: U.S. Department of Health and Human Services. [Google Scholar]
- U.S. Department of Health and Human Services (2018) Physical Activity Guidelines for Americans, 2nd edn. Washington, DC: U.S. Department of Health and Human Services. [Google Scholar]
- Yardley L, Bishop FL, Beyer N, et al. (2006) Older people’s views of falls-prevention interventions in six European countries. The Gerontologist 46(5): 650–660. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.