

Abstract
Aims and Objectives
How health risks are communicated can have a substantial impact on medical judgments and choice. Here, we examine whether the language used to process health-related information systematically changes bilinguals’ perceptions and preferences.
Methodology
Chinese-English bilinguals were presented with ten medical scenarios in either their native language (Mandarin Chinese; N = 76) or a second language (American English; N = 84) and made judgments regarding their familiarity with the medical conditions and the perceived severity of the possible symptoms (incurability, emotional distress, physical pain, social harm). Participants then rated their agreement with statements pertaining to beliefs about medical decision-making (trust in the good intentions of doctors, acceptability of challenging doctors, importance of involving family, preference for standard treatments, preference for experimental treatments).
Data and Analysis
Linear mixed effects models were constructed for judgments of medical conditions and for beliefs regarding medical decision-making.
Findings and Conclusions
Medical conditions were perceived to be easier to cure, less physically painful, and less emotionally distressing when processed in the second language, English. Using English also increased endorsement of beliefs (such as challenging doctors’ opinions and accepting experimental treatments) that were more consistent with individualistic than collectivistic norms.
We propose that the activation of emotions and values is linked to language, with consequences for how individuals make decisions that impact their health and well-being.
Originality
The present study is among the first to systematically examine the interactive psychological impact of language context and experience on judgments and beliefs in an applied medical domain.
Keywords: language, bilingualism, medical judgment, medical beliefs, foreign language effect, cultural priming
Few decisions are more consequential, yet rife with uncertainty and bias, as the choices we make about our physical health. Even when medical professionals have reliable and relevant knowledge, the extent to which these translate to beneficial behaviors is largely contingent on how we, as decision-makers, interpret and respond to health-related information. Take, for instance, a parent’s decision to vaccinate their child. The perceived costs and benefits of vaccination can be influenced by real and fake statistics regarding potential risks, as well as more subjective factors, such as emotional reactions to the prospect of adverse effects and pre-existing beliefs about a topic or source of information (Broniatowski et al. 2018; Krishna & Thompson, 2019). A substantial body of research has been dedicated to understanding the conditions that promote or impede optimal decision-making in order to improve how we communicate and interpret information in a medical context (Kite, Foley, Grunseit, & Freeman, 2016; Wright, 2020). Unsurprisingly, the way that decision-makers respond to health-related messages is impacted by how these messages are communicated – patients can be nudged by a physician’s choice of words or a compelling testimonial (Finset et al., 2020; Gebbers, De Wit, & Appel, 2017). Here, we provide evidence that medical judgments and beliefs can be swayed not only by the content of a message, but also by the language of communication itself.
How individuals process and respond to a given language varies as a function of prior language experience. For instance, bilinguals often report feeling less emotional when using a foreign language compared to their native tongue. Even when the content of a message is fully understood, hearing “I love you” (Dewaele, 2008), receiving a reprimand (Harris, Aycicegi, & Gleason, 2003), discussing a distressing experience (Dewaele & Costa, 2013), or reading an emotional passage (Hsu, Jacobs, & Conrad, 2015) are likely to be more evocative in a native language. This is because when we learn the meaning of a word or a phrase, we do not merely associate a sequence of letters or sounds with its intended referent, but also with the events and emotions we experience in the process. For instance, when bilinguals are asked to describe a past experience in response to a word, they are more likely to retrieve memories that were encoded in the same language as the one currently being used (i.e. language-dependent memory; Marian & Neisser, 2000; see also Marian & Fausey, 2006; Marian & Kaushanskaya, 2007; Marsh, Kanaya, & Pezdek, 2015).
Because our experiences, values, norms, and beliefs are often encoded in a native-language context, they may not be as readily or vividly activated when making judgments in a non-native language. Indeed, research outside of the medical domain suggests that using a foreign language can reduce adherence to social norms (Geipel, Hadjichristidis, & Surian, 2015) and superstitious beliefs (Hadjichristidis, Geipel, & Surian, 2019), as well as attenuate the perceived negativity of aversive stimuli (Geipel, Hadjichristidis, & Klesse, 2018) and perceived risk of potential hazards (Hadjichristidis, Geipel, & Savadori, 2015). As a result, using a foreign language can even change people’s behaviors, for instance by reducing risk aversion when presented with financial gambles (e.g., Ascher et al., 2017; Besuglov & Crasselt, 2020; Costa et al., 2014; Geipel et al., 2018; Hayakawa et al., 2019; Keysar, Hayakawa, & An, 2012) and increasing utilitarianism when faced with moral dilemmas (Corey et al., 2017; Costa et al., 2014a; Hayakawa et al., 2017; Hayakawa & Keysar, 2018). Using a foreign language may similarly impact how people respond to difficult medical dilemmas by attenuating the perceived severity of potential adverse effects and reducing the salience of pre-existing beliefs.
While foreign language effects are, by definition, assumed to result from the use of a non-native language (one which is often less integrated with prior experiences compared to the native tongue), switching between two native or high-proficiency languages can also affect cognition and behavior by bringing different associations to mind (e.g., cultural accommodation, Akkermans, Harzing, Wsitteloostuijn, 2010; Ralston, Cunniff, & Gustafson, 1995; cultural frame-switching, Ramírez-Esparza et al., 2006; Ross, Xun, & Wilson, 2002; Verkuyten & Pouliasi, 2002). Priming bilinguals with linguistic cues can elicit thoughts and behaviors consistent with knowledge, scripts, and schemas of the associated culture – for instance, language has been shown to influence bilinguals’ social judgments and self-construal (Kemmelmeier & Cheng, 2004; Marian & Kaushanskaya, 2004; Ross et al., 2002; Trafimow, Silverman, Fan, & Law, 1997), implicit associations (Luna, Ringberg, & Perrachio, 2008), emotions (Marian & Kaushanskaya, 2004; Panayiotou, 2004), competitive vs. cooperative behaviors (Akkermans et al., 2010), and consumer decisions (Briley, Morris, & Simonson, 2005) in culturally-prescribed ways.
Applied to the medical domain, sociocultural norms, such as those associated with deference to authority (Deschepper et al., 2008; Hofstede, 1980; Meeuwesen, van den Brink-Muinen, & Hofstede, 2009), individual vs. group decision-making (Kim, Smith, & Yueguo, 1999), conformity to existing rules and common practices (Kim & Drolet, 2003; Markus & Kitayama, 1991; Triandis, 1995), and attitudes toward uncertainty (De Meulenaer, De Pelsmacker, & Dens, 2015, 2018; Deschepper et al., 2008; Hofstede, 1991; Huynh, 2020; Meeuwesen et al., 2009) could be differentially activated depending on the language context and subsequently modulate how bilinguals perceive and respond to health-related information.
Though foreign language effects and cultural priming have typically been investigated as distinct phenomena, they are likely to share some underlying mechanisms. In both cases, it has been proposed that language shapes cognition and behavior by selectively increasing the accessibility of associated concepts, memories, and modes of processing (e.g., Cultural Priming: Ramírez-Esparza et al., 2006; Verkuyten & Pouliasi, 2002; see Merunka, 2013 for review and Hong et al., 2000; Hong & Mallorie, 2004 for similar explanations with non-linguistic primes; Foreign Language Effects: Costa et al., 2014; Geipel, Hadjichristidis, & Surian, 2015; Hayakawa et al., 2017; Keysar, Hayakawa, & An, 2012; see Hayakawa, Costa, Foucart, & Keysar, 2016 for discussion).
One notable distinction, however, is that while cultural priming is proposed to result from the activation of different culture- and language-specific frames and experiences, foreign language effects are more often considered to stem from the reduced automaticity and accessibility of associations formed in a native language context (without necessarily activating a comparably rich network of meaning tied to the non-native language). In other words, elicitation of cultural priming vs. a foreign language effect is likely to vary as a function of prior language experience and the extent to which the language in use has been integrated with its associations. Here, we explore the impact of language in the medical domain by examining how the immediate language environment (Chinese vs. English) interacts with prior language experience (age of acquisition and proficiency) to shape bilinguals’ healthcare-related judgments and beliefs.
The Present Study
Chinese speakers with varying degrees of English experience (including foreign language learners and balanced bilinguals) were randomly assigned to read scenarios describing a medical condition and a preventative treatment in either Chinese or English. After each scenario, participants made a series of evaluations regarding the medical condition, including judgments of perceived severity (physical pain, emotional distress, curability, social harm) and familiarity. Following all judgments, participants were asked to indicate how much they agreed with beliefs and attitudes about medical decision-making, which aligned to varying degrees with cultural orientations associated with American English and Mandarin Chinese (trusting/challenging doctors’ opinions, considering family’s opinions, preference for standard/experimental treatments).
The two sets of evaluations (judgments of medical conditions and beliefs about medical decision-making) enabled us to examine whether effects of language context and experience are further moderated by the type of judgment to be made. Based on prior work demonstrating that information is often processed less emotionally and vividly in a non-native tongue (e.g., Geipel, Hadjichristidis, & Klesse, 2018; Harris, Aycicegi, & Gleason, 2003; Hayakawa & Keysar, 2018), we predicted that using a foreign language would elicit lower (i.e., less severe) ratings of medical conditions relative to using a native language. In other words, bilinguals using English as a foreign language were expected to perceive medical conditions as less physically painful, less emotionally distressing, less socially harmful, and easier to cure than those using native Chinese. If prior experiences with similar situations are additionally less accessible in a non-native tongue, bilinguals using a foreign language may perceive the medical conditions to be less familiar relative to those using their native language. Importantly, if such effects are attributable to differences in the richness or quantity of experientially-grounded associations tied to a native vs. foreign language, we would expect the impact of language context to decline with greater second language experience (e.g., earlier age of acquisition and higher proficiency).
On the other hand, if effects of language are attributable to the activation of distinct language- and culture-specific associations, we may expect language-dependent judgments to be greatest among individuals with significant experience with both languages. For instance, the degree to which using English (vs. Chinese) selectively enhances the accessibility of individualistic (vs. collectivistic) norms is likely to depend on how well each value system has been internalized, which may in turn determine the impact of language on medical judgments. Relative to the individualistic orientations characteristic of Western societies, East Asian cultures have traditionally been associated with greater deference to authority (i.e., higher power distance), accountability to family and community (i.e., greater collectivism), and adherence to established norms and practices (i.e., higher uncertainty avoidance; Hofstede, 1980). Extending the study of cultural orientations to the medical domain, Kim, Smith, and Yueguo (1999) found that individual differences in individualism and collectivism predicted Chinese patients’ preferences regarding the degree of collaboration between physicians and patients, as well as the involvement of family.
Here, we examine the possibility that effects of cultural orientation on medical judgments may also be observed within a single individual when culturally-prescribed norms and values are selectively activated by an associated language context. Specifically, we predicted that, relative to English, bilinguals using Chinese would exhibit (1) greater trust in doctors, (2) reduced willingness to challenge doctors, (3) greater consideration of family’s wishes when making medical decisions, (4) greater preference for commonly accepted courses of treatment, and (5) reduced willingness to undergo experimental treatments.
In sum, the aim of the present investigation is to examine how language context and language experience interact to shape bilinguals’ medical evaluations and beliefs. In particular, we explore the potential contributions of foreign language processing and cultural priming to the emergence of language-dependent judgment among individuals with varying degrees of bilingual language experience.
Methods
Participants
Participants were 165 Chinese-English bilinguals (54.4% female) residing in the United States at the time of the experiment. The majority of participants were either enrolled in or had graduated from a U.S. university1. The study took place online and interested volunteers were screened prior to participation to ensure that they were native Mandarin Chinese speakers who spoke English as a second language. Eligible participants indicated during the initial screening task that Chinese was their dominant language and that Chinese was acquired prior to English. More detailed language background information collected following the experiment showed that a subset of participants reported full fluency in both languages (8.75%) and/or that both languages were acquired in infancy (13.75%). The remaining participants reported higher proficiency in Chinese than English based on aggregated self-report measures of speaking, listening, and reading (each using 0–10 scales taken from the Language Experience and Proficiency Questionnaire; Marian, Blumenfeld & Kaushanskaya, 2007). English proficiency ranged from 4.3 to 10 and age of English acquisition ranged from infancy to 15 years old. Participants who passed the screening were randomly assigned to complete the experiment in either their native (L1 Chinese; n = 76) or second language (L2 English; n = 84) in a between-group design, and the two groups did not differ in age, gender, Chinese age of acquisition, English age of acquisition, or Chinese proficiency. Participants in the L1 Chinese condition did, however, report higher English proficiency relative to those in the L2 English condition (see Table 1).
Table 1.
Means (SDs) for demographic and language background measures by language condition
| L1 Chinese | L2 English | p-value | |
|---|---|---|---|
| Age | 25.93 (4.29) | 25.63 (3.55) | 0.63 |
| Gender | 52.6% Female | 55.9% Female | 0.79 |
| Chinese AoA | 0.77 (1.81) | 0.88 (1.87) | 0.72 |
| English AoA | 6.24 (3.65) | 6.00 (3.31) | 0.67 |
| Chinese Proficiency | 9.72 (0.70) | 9.58 (0.96) | 0.28 |
| English Proficiency | 8.21 (1.16) | 7.79 (1.17) | 0.03* |
Stimuli and Procedure
Following eligibility screening and consent, participants made a series of judgments in response to ten medical scenarios (see Supplemental Materials for all scenarios). The original English scenarios were translated into Chinese by a native Mandarin speaker and then back-translated into English by a second native Mandarin speaker (Brislin, 1970). The two English versions were then compared, and any discrepancies were resolved through consensus among the original two translators, a third Mandarin-English bilingual, and the authors. Mandarin-English bilinguals were additionally consulted to confirm that the medical conditions were not culturally biased. All scenarios followed the same structure – each began with a sentence introducing a medical condition (e.g., the flu), followed by two sentences describing five adverse effects that could result from the condition (e.g., sore throat, fever, pneumonia, severe body aches, difficulty breathing). Participants then read one sentence introducing a preventive treatment (e.g., a flu vaccine) and three sentences describing five potential side effects of the treatment (e.g., soreness at the injection site, weakness in the arms, difficulty performing normal tasks, allergic reactions, difficulty breathing). All scenarios were matched in structure and length. After reading each scenario, participants responded to the following five questions on 0–100 scales (italicized words varied depending on the scenario):
-
How familiar are you with the flu? [Familiarity]
Not familiar at all; Extremely familiar
-
How hard do you think it is to cure the flu? [Incurability]
Not hard at all; Extremely hard
-
How emotionally distressing do you think it is to have the flu? [Distress]
Not distressing at all; Extremely distressing
-
How physically painful do you think it is to have the flu? [Pain]
Not painful at all; Extremely painful
-
How harmful do you think having the flu will be for your social interactions with others? [Social]
Not harmful at all; Extremely harmful
In addition to ratings of overall familiarity, which were taken as a general metric of exposure to and/or knowledge of the medical condition, participants explicitly indicated whether or not they had personal experience with the medical condition (“Yes,” “No,” “Prefer not to answer”). This more objective measure of prior exposure was used to confirm that the two language groups did not differ in previous experience with the scenarios utilized in the study (p > .05). After providing their judgments for all ten medical conditions, participants were asked to indicate how strongly they agreed with the following beliefs about medical decision-making (0–100 scales ranging from “strongly disagree” to “strongly agree”):
Doctors always have my best interests in mind. [Doctor]
Patients should challenge their doctors when they have different opinions. [Challenge]
It is important to have my family members be part of my medical decision-making process. [Family]
If I am unsure about what medical decision to make, I will prefer the treatment that is most frequently chosen by other people. [Common]
I would prefer to accept an experimental treatment over a standard treatment if it may be more effective. [Experimental]
Analyses
The effect of language was evaluated separately for the five judgments of medical conditions (Familiarity, Incurability, Physical Pain, Emotional Distress, and Social Harm) and the five beliefs regarding medical decision-making (Involving Family, Trusting Doctor, Challenging Doctor, Preferring Common Treatments, and Preferring Experimental Treatments). Both analyses were conducted using linear mixed effect models with fixed effects of Language (contrast-coded and weighted by the number of participants; L1 Chinese: −0.525 vs. L2 English: +0.475), Judgment Measure or Belief Measure (deviation coded to compare each of the five levels against the mean of all levels), and interactions, plus a random intercept for participant. The model evaluating judgments of medical conditions additionally included a by-participant random slope for Judgment Measure (i.e., Familiarity, Incurability, Physical Pain, Emotional Distress, and Social Harm) and a random intercept for medical condition.
We followed up on the primary analyses by exploring whether the effects of language were moderated by participants’ age of acquisition and proficiency in each language. We began by calculating two continuous measures representing each participant’s relative age of acquisition (calculated as the age of L2 English acquisition minus the age of L1 Chinese acquisition) and relative reading proficiency (calculated as L1 reading proficiency minus L2 reading proficiency). The additional measures of listening and speaking proficiency were not included in the model due to the fact that the three proficiency measures were highly correlated (rs > 0.51, ps < .0001), which could introduce issues of multicollinearity. As all stimuli were presented visually and no production was required, reading proficiency was deemed to be the most relevant and precise measure of language ability for the present experiment2. Separate linear mixed-effects models were constructed for judgments of medical conditions and beliefs about medical decision-making, each with fixed effects of Language, Judgment/Belief Measure, Relative AoA, and Relative Proficiency, as well as all two- and three-way interactions between Language, Judgment/Belief Measure, and each language background variable. Both models included random intercepts for participant, and the model evaluating judgments of medical conditions additionally included a random intercept for medical condition.
Results
Judgments of Medical Conditions
Participants using the second language, English, provided significantly lower judgment ratings of the medical conditions (M = 55.92, SD = 29.63) relative to those using the native language, Chinese (M = 60.65, SD = 31.64; Estimate = −4.74, SE = 1.66, t(158.05) = −2.86, p = 0.005), suggesting that overall, medical conditions were perceived to be less severe when processed in English. Ratings additionally varied depending on the Judgment Measure (p < .001 for each Judgment Measure relative to the mean of all measures). Lastly, there was a significant interaction between Language and Judgment Measure (Estimate = −3.60, SE = 1.36, t(269.11) = −2.64, p = 0.009). Planned comparisons of L1 Chinese vs. L2 English for each of the judgment measures revealed that participants using English perceived the medical conditions to be significantly easier to cure (Estimate = −3.92, SE = 1.68, z = −2.33, p = 0.020), less physically painful (Estimate = −4.87, SE = 2.27, z = −2.14, p = 0.032), and less emotionally distressing (Estimate = −8.34, SE = 2.37, z = −3.52, p = 0.0004). The two language groups did not differ in familiarity with the medical condition (Estimate = −3.3, SE = 2.65, z = −1.25, p = 0.213) or perceived social harm (Estimate = −3.26, SE = 2.57, z = −1.27, p = 0.205; see Figure 1).
Figure 1.
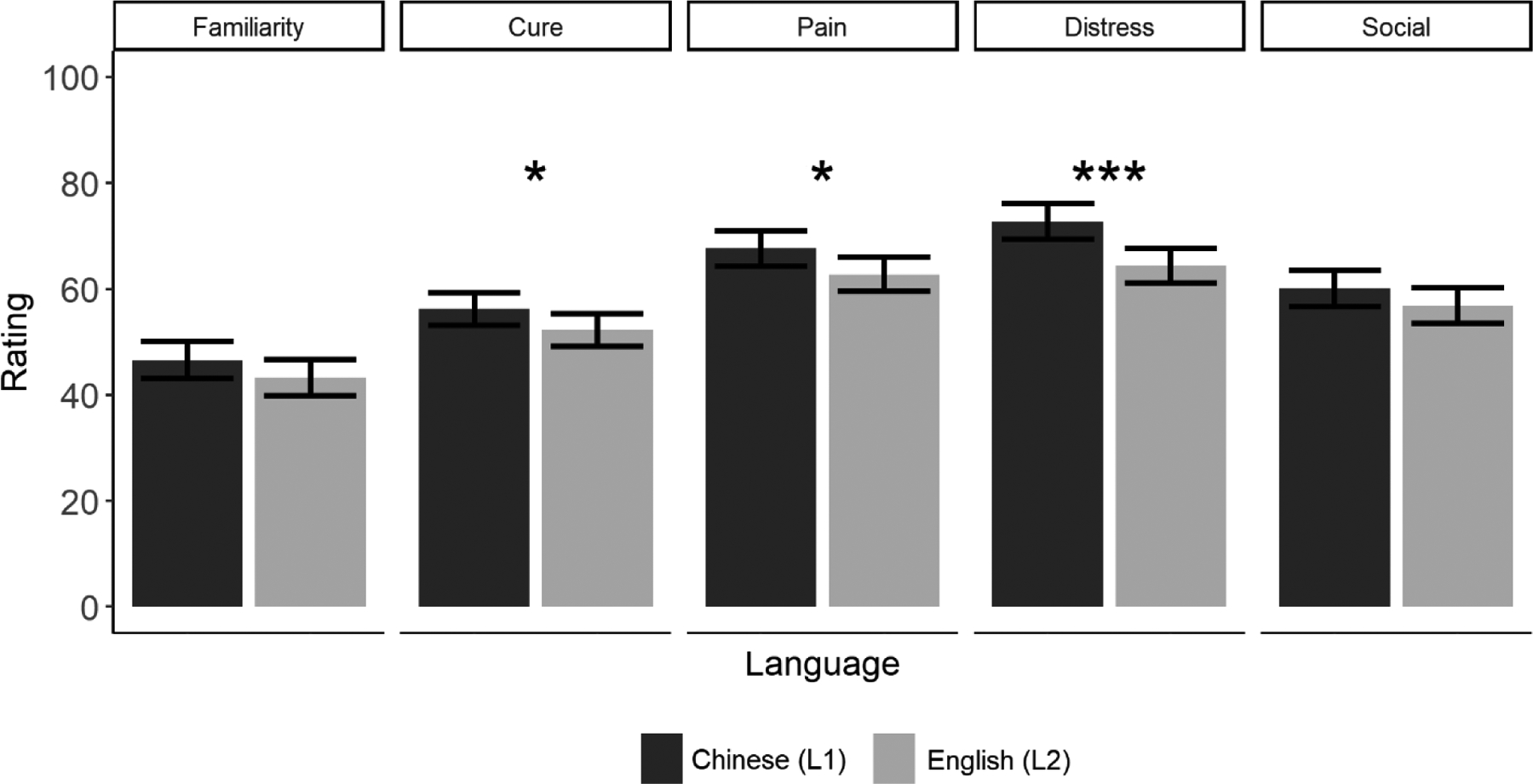
Effects of language on medical evaluations. Medical conditions were perceived to be easier to cure, less physically painful, and less emotionally distressing when judgments were made in the L2 (English). Error bars represent standard error. *p < .05, **p < .01, ***p < .001.
Beliefs about Medical Decision-Making
Overall, participants using English expressed stronger agreement with the beliefs about medical decision-making (M = 62.03, SD = 24.31) compared to those using Chinese (M = 56.67, SD = 29.63; Estimate = 5.36, SE = 1.91, t(158) = 2.8, p = 0.006). Participants also indicated different levels of agreement depending on the belief (p < .05 for each of the beliefs relative to the mean of all beliefs). Planned comparisons of Chinese vs. English for each of the beliefs revealed that those using English thought it was significantly more acceptable to challenge doctors’ opinions compared to those using Chinese (Estimate = 9.16, SE = 4.1, t = 2.23, p = 0.026), and were more open to accepting promising experimental treatments (Estimate = 9.39, SE = 4.1, t = 2.29, p = 0.022). The two language groups did not differ in the perceived importance of involving family in medical decisions (Estimate = 5.05, SE = 4.1, t = 1.23, p = 0.218), trust in doctors’ intentions (Estimate = 3.33, SE = 4.1, t = 0.81, p = 0.417), or preference for pursuing commonly accepted courses of treatment (Estimate = −0.13, SE = 4.1, t = −0.03, p = 0.975; see Figure 2).
Figure 2.

Effects of language on beliefs about medical decision-making. Using L2 English significantly increased the perceived acceptability of challenging doctors’ opinions, as well as the preference for promising experimental treatments. Error bars represent standard error. *p < .05
Effects of Age of Acquisition and Language Proficiency
Judgments of Medical Conditions
In addition to a significant main effect of Language (Estimate = −14.06, SE = 3.26, t(152) = −4.32, p < 0.001), there was a significant interaction between Language and Relative AoA (Estimate = 1.19, SE = 0.49, t(152) = 2.42, p = 0.017), as well as a marginal interaction between Language and Relative Proficiency (Estimate = 2.49, SE = 1.4, t(152) = 1.78, p = 0.077). In order to visualize these interactions, each language group was further divided into Simultaneous3 and Sequential bilinguals, as well as those with Balanced and Unbalanced bilingual proficiency based on the median L1:L2 difference scores of 5 and 1, respectively (see Tables 2 and 3 for language background measures for the age of acquisition and proficiency subgroups). The effects of language within each subgroup were assessed using separate linear mixed-effects models, with participants’ mean ratings for each of the five measures (aggregated across the ten scenarios) entered as the outcome variable. The models for the simultaneous and sequential acquisition groups included fixed effects of Language, Measure, Relative Reading Proficiency, and all interactions, as well as a random intercept for participant. The models for the balanced and unbalanced proficiency groups included fixed effects of Language, Measure, Relative Age of Acquisition, and all interactions, as well as a random intercept for participant.
Table 2.
Means (SDs) for background measures by acquisition group (L2 English – L1 Chinese)
| Simultaneous | Sequential | p-value | |
|---|---|---|---|
| Age | 25.11 (2.87) | 26.24 (4.43) | 0.051 |
| Gender | 54.5% Female | 54.3% Female | 0.769 |
| Chinese AoA | 0.69 (1.25) | 0.50 (0.94) | 0.314 |
| English AoA | 3.45 (3.00) | 7.98 (2.39) | <.001 |
| Relative AoA | 2.58 (2.40) | 7.48 (2.27) | <.001 |
| Chinese Reading Proficiency | 9.54 (1.08) | 9.79 (0.47) | .085 |
| English Reading Proficiency | 8.57 (1.38) | 8.32 (1.27) | .238 |
| Relative Reading Proficiency | 0.94 (1.16) | 1.48 (1.22) | .006 |
Table 3.
Means (SDs) for background measures by proficiency group (L1 Chinese – L2 English)
| Balanced | Unbalanced | p-value | |
|---|---|---|---|
| Age | 26.03 (4.22) | 25.30 (3.24) | 0.218 |
| Gender | 56.3% Female | 50.9% Female | 0.619 |
| Chinese AoA | 0.65 (1.18) | 0.49 (0.89) | 0.198 |
| English AoA | 5.64 (3.67) | 6.96 (2.91) | 0.013 |
| Relative AoA | 4.91 (3.46) | 6.53 (2.88) | 0.002 |
| Chinese Reading Proficiency | 9.62 (0.82) | 9.82 (0.71) | 0.110 |
| English Reading Proficiency | 9.06 (0.84) | 7.28 (1.29) | <.001 |
| Relative Reading Proficiency | 0.53 (0.52) | 2.54 (1.05) | <.001 |
As shown in Figure 3, the effect of Language was significant for the simultaneous (Estimate = −7.16, SE = 2.37, t(79) = −3.02, p = .003), but not sequential acquisition group (Estimate = −0.96, SE = 2.29, t(71) = −421, p = .675). Similarly, there was a significant effect of language for the balanced (Estimate = −7.12, SE = 2.13, t(97) = −3.34, p = .001), but not unbalanced reading proficiency group (Estimate = −0.99, SE = 2.57, t(53) = −0.38, p = .702).
Figure 3.

Effects of language on judgments of medical conditions for (a) simultaneous vs. sequential bilinguals and (b) bilinguals with balanced vs. unbalanced reading proficiency. Participants perceived medical conditions to be significantly more severe when using L1 Chinese compared to L2 English. This was particularly the case for simultaneous bilinguals and those who had balanced proficiency across their two languages. Error bars represent standard error. **p < .01
Tukey-adjusted tests of simple effects for each of the individual measures revealed a comparable pattern, with significant effects of language on evaluations of physical pain (p = .036), emotional distress (p < .001), and social harm (p = .033) for simultaneous, but not sequential bilinguals (ps > .05), as well as on evaluations of familiarity (p = .009), physical pain (p = .029), emotional distress (p < .001), and social harm (p = .044) for bilinguals with balanced, but not unbalanced reading proficiency (ps > .05; see Figure 4).
Figure 4.
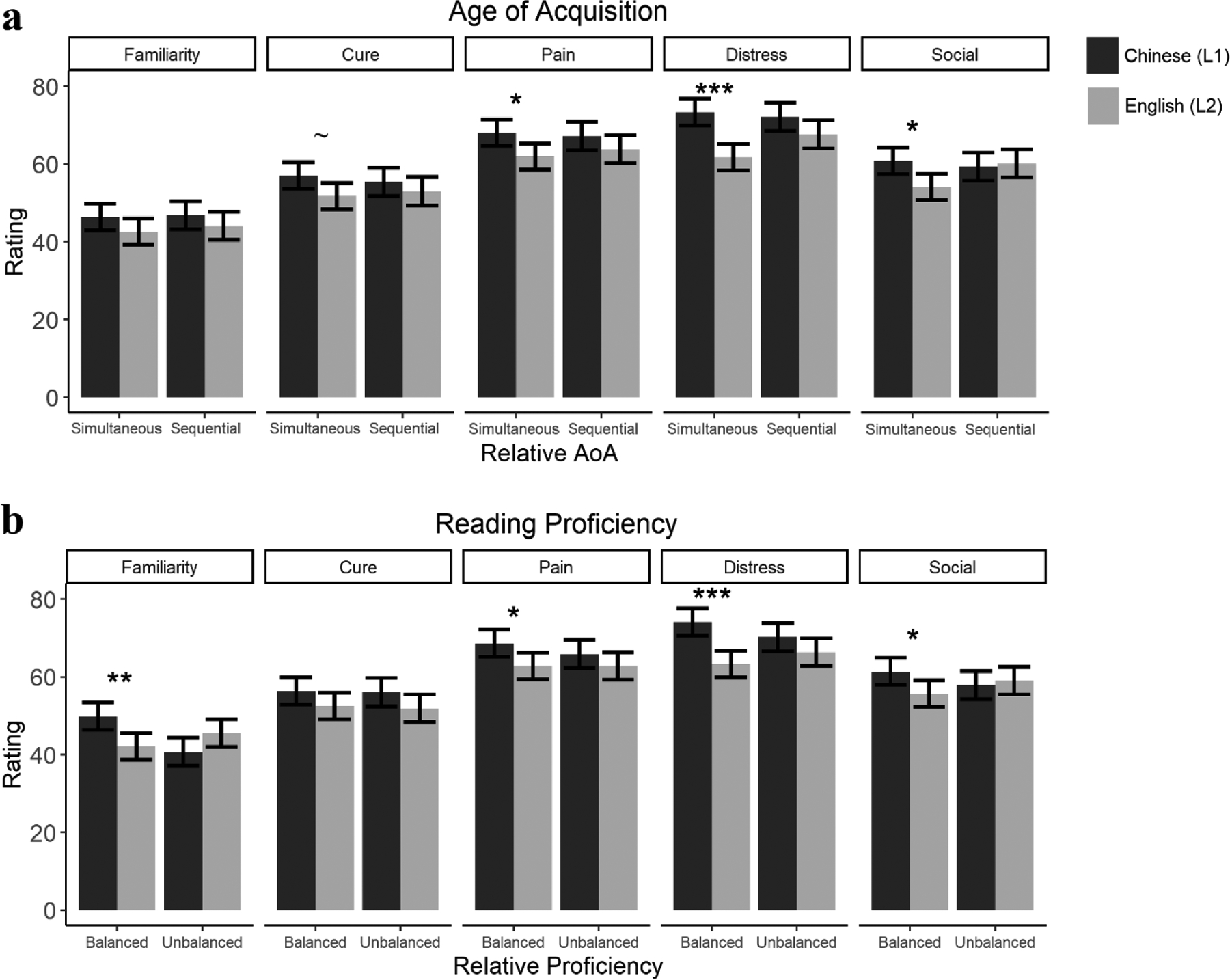
Effects of language on each of the judgment measures for (a) simultaneous vs. sequential bilinguals and (b) bilinguals with balanced vs. unbalanced reading proficiency. Using L2 English significantly increased the perceived severity of physical pain, emotional distress, and social harm for simultaneous bilinguals and those with balanced reading proficiency. Error bars represent standard error. ***p < .001, **p < .01, *p < .05
Beliefs about Medical Decision-Making
The two-way interactions between Language and Relative AoA, as well as between Language × Relative Proficiency were not significant (both p > .05). There was, however, a significant three-way interaction between Language, Relative Proficiency, and Measure (Estimate = 6.63, SE = 3.1, t(608) = 2.14, p = 0.033). As in the follow-up analyses for judgments of medical conditions, effects of language within each subgroup were assessed using separate linear mixed-effects models, with participants’ ratings for the five measures entered as the outcome variable. The models for the simultaneous and sequential acquisition groups included fixed effects of Language, Measure, Relative Proficiency, and all interactions, as well as a random intercept for participant. The models for the balanced and unbalanced proficiency groups included fixed effects of Language, Measure, Relative Age of Acquisition, and all interactions, as well as a random intercept for participant.
Tukey-adjusted tests for each of the individual measures revealed that, unlike the consistent effects of language background observed for judgments of medical conditions, the effects of AoA and proficiency were more complex for beliefs about medical decision-making. Specifically, the perceived acceptability of challenging doctors was significantly greater in L2 English for the simultaneous acquisition (p = 0.007) and unbalanced proficiency groups (p = .030), but not for the sequential acquisition or balanced proficiency groups (p > .05). The opposite pattern emerged for willingness to accept experimental treatments, where the effects of language were significant for the sequential acquisition (p = .006) and balanced proficiency groups (p = .011), but not for the simultaneous acquisition or unbalanced proficiency groups (ps > .05).
Discussion
The present study examined the effects of language context and experience on bilinguals’ medical judgments and beliefs. When making health-related decisions, such as whether or not to get vaccinated for a disease, people can be influenced by online affective responses to prospective outcomes (e.g., the perceived risk or negativity of adverse effects), as well as by prior beliefs or norms surrounding a given issue (e.g., believed reliability of an information source). How readily a particular outcome or schema comes to mind depends, to some extent, on how well incoming stimuli match information stored in our long-term memory (i.e., context-dependent memory; Jensen, Harris, & Anderson, 1971; Tulving & Thomson, 1973; see Davies & Thomson, 1988 and Smith & Vela, 2001 for reviews). For instance, an English-speaker seeing “COVID-19” is likely to activate sensory, affective, and semantic memory traces, which could then impact their judgments and decisions; notably, however, “COVID-19” is likely to be a more effective and evocative cue than “SARS-CoV-2.” Even if we know that two terms refer to similar concepts (e.g., the COVID-19 disease and the SARS-CoV-2 virus), more frequent exposure to one means that we have had more opportunities to connect its auditory and visual forms to our ever-growing network of associations. For multilinguals, entire languages may be more or less effective at connecting us to aspects of our past experience, with potential implications for future behavior.
In particular, the present study set out to explore distinct, but related mechanisms, whereby language may impact judgments and beliefs in the medical domain. Based on earlier work in non-medical contexts demonstrating that using a foreign language can elicit less emotional judgments and behaviors relative to a native tongue, we predicted that reading about adverse health effects in a non-native language would attenuate the perceived severity of medical conditions relative to using a native language. As expected, Chinese-English bilinguals perceived medical conditions to be easier to cure, less physically painful, and less emotionally distressing when reading about them in a second language (English) compared to a native language (Chinese). Notably, however, the influence of language was most robust for bilinguals who had relatively more balanced ages of acquisition and proficiency across their two languages. In other words, while the reduction in perceived severity elicited by English (relative to native Chinese) is generally consistent with what would be expected for a foreign language effect, the impact of language was greatest among bilinguals for whom English was a second, but not necessarily foreign language. To the extent that earlier AoA and higher proficiency in L2 facilitate connections between a second language and our memories, we may have expected bilinguals with more balanced AoA and proficiency to exhibit smaller (rather than larger) effects of language. One possibility is that while the psychological distance of a non-native tongue reduces the perceived negativity of adverse outcomes, the difficulty or anxiety associated with using a less proficient language exerts an opposing influence by increasing perceptions of severity and risk.
More likely, however, is that the relatively more robust effects observed for experienced bilinguals stemmed from the activation of different, and more strongly internalized, memories, concepts, and modes of processing associated with the two languages. Models of bilingual language representation such as the Conceptual Feature Model (Kroll & De Groot, 1997) posit that each word in a bilingual’s two languages activates a set of conceptual features, which can often differ even between translation equivalents. For instance, when informed that a symptom of a disease is a high fever, the English word “fever” and its Chinese translation “发烧” will activate some overlapping concepts (e.g., heat, illness), as well as associations that may be stronger in one language than the other due to differences in linguistic features (e.g., between fever and burning in Chinese via the shared character 烧) or linguistic contexts of exposure (e.g., between Saturday, night, and fever in English via the iconic English film title). Each conceptual feature can then go on to activate its own constellation of associations, potentially resulting in an increasingly distinct series of exemplars and ideas across languages that form the basis for subsequent judgments (see Luna, Ringberg, & Peracchio, 2008). Importantly, individuals with higher proficiency in a second language and a more balanced bilingual profile would be expected to activate a broader and more entrenched language network, yielding judgments that are especially sensitive to the linguistic context.
Given the close correspondence between language and culture, the patterns of language-dependent judgments observed in the present study could additionally stem from the selective activation of culture-specific norms and schemas. For instance, the use of English vs. Chinese could have modulated activation of culturally-prescribed display rules for expressing discomfort (Matsumoto, 1990; Panayiotou, 2004), as well as ways of conceptualizing emotions (Norasakkunkit, 2003; Norasakkunkit & Kalick, 2002) and even experiencing pain (Wang, Ma, & Han, 2014; i.e., a cultural priming effect). Stronger support for the specific role of culture comes from the effect of language on beliefs regarding medical decision-making, which were explicitly designed to map to dimensions that have been shown to vary across Eastern and Western societies. We had predicted that individuals using Chinese would be more likely to endorse beliefs that align with values such as deference for authority and family, as well as adherence to accepted practices compared to those using English. This prediction was partially confirmed, with those using English expressing greater willingness to challenge the authority of doctors and accept promising experimental treatments over standard treatments. As with the judgments of medical conditions, the effect of language on willingness to challenge doctors was greater among bilinguals who had acquired both Chinese and English at a younger age. To the extent that effects of language are driven by the activation of culture-specific norms and values, one might expect to see stronger language-dependent judgments among those who have been exposed to both languages and cultures from a young age. In other words, while simultaneous bilinguals may selectively activate American or Chinese norms when using English vs. Chinese, respectively, bilinguals who acquired English later in life may be more likely to access Chinese cultural schemas regardless of the language context. Unlike judgments of medical conditions, however, the effect of language on willingness to challenge doctors was weaker among bilinguals with balanced language proficiency. A similar dissociation between age of acquisition and proficiency was observed for willingness to accept experimental treatments (but in the opposite direction), such that the effect of language was greater among bilinguals with later ages of English acquisition, but more native-like proficiency. The influence of language context therefore appears to be moderated by both individual differences in bilinguals’ language experiences, as well as the nature of the task itself.
It should be noted that the foreign language effect, effects arising from the activation of distinct language networks, and cultural priming are not mutually exclusive. Language and culture are closely intertwined and language frequently functions as a vehicle for culture, with additional research needed to disentangle the relative contributions of each. For instance, it is possible that the activation of distinct, culture- and language-specific schemas had a more significant impact in the present study due to the fact that all participants had immersive English language experience. The degree of psychological distance prompted by the use of a native vs. non-native language may play a greater role among bilinguals with more formal contexts of L2 acquisition and use.
Additionally, while it was assumed that participants in the present study had full comprehension of the English stimuli (due to their residence and education in an English-speaking country), comprehension was not directly assessed. To the extent that lower-proficiency bilinguals had greater difficulty understanding the English scenarios, the impact of foreign language processing may have been underestimated. Follow-up studies, particularly those including lower-proficiency participants, would therefore benefit from including explicit tests of comprehension. Future research will also need to fully cross first and second language status (i.e., by testing bilinguals for whom English is the first and Chinese is the second language), as well as to recruit monolingual members of each cultural group for baseline comparisons, include more detailed measures of language and cultural experience, and test bilingual speakers of other languages. The present investigation serves as an initial step toward understanding the roles of language and culture during medical decision-making, showing that judgments and beliefs about physical health and medical treatments can be influenced by linguistic experience and context.
From immigrant families to foreign-born doctors, bilinguals all around the world make healthcare decisions using a wide array of native and non-native languages. Research in the medical domain has often focused on how language background can affect comprehension of semantic content, as well as how it can trigger stereotypes and biases of interlocutors. Here, we provide evidence that language experience and exposure can systematically alter how we interpret health-related information, with potential implications for the millions of healthcare practitioners and patients who make medical decisions every day in diverse linguistic contexts.
Supplementary Material
Figure 5.

Effects of language on each of the belief measures for (a) simultaneous vs. sequential bilinguals and (b) bilinguals with balanced vs. unbalanced reading proficiency. Using L2 English significantly increased willingness to challenge doctors for simultaneous bilinguals with unbalanced proficiency. Using L2 English significantly increased willingness to accept experimental treatments for sequential bilinguals with balanced proficiency. Error bars represent standard error. **p < .01, *p < .05
Significance.
With millions of practitioners and patients worldwide making medical decisions in a combination of native and non-native languages, the present findings highlight the need to account for language, including language use, context, and experience, in order to optimize health-related communication and judgments.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health [grant number R01HD059858] to Viorica Marian. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Declaration of Conflicting Interests
The authors declare no conflicts of interest.
The restriction to U.S. residents helped to ensure that participants had a requisite amount of English language ability and minimized possible variance in participants’ inferences regarding the prevalence and treatment of medical conditions in the United States vs. China.
Note that similar findings were obtained when reading proficiency was substituted with a composite measure of proficiency aggregated across reading, listening, and speaking proficiency.
Note that while individuals with more similar ages of L1 and L2 acquisition were labeled as “simultaneous” bilinguals (to differentiate them from those who acquired the L2 relatively later than the L1), in both groups, the average age of L1 Chinese acquisition was earlier than that of L2 English (see Table 2).
References
- Akkermans D, Harzing AW, & Van Witteloostuijn A (2010). Cultural accommodation and language priming. Management International Review, 50(5), 559–583. [Google Scholar]
- Ascher D, Polowczyk J, Wielicka-Regulska A, da Silva WV, & Souza A (2017, October). The Foreign Language Effect in risk decision-making: A cross-country review of Brazilians and Poles behavior in a loss aversion experiment. In Proceedings of the 8th International Conference on E-business, Management and Economics (pp. 42–45). [Google Scholar]
- Besuglov E, & Crasselt N (2020). The effect of readability and language choice in management accounting reports on risk-taking: an experimental study. Journal of Business Economics, 1–29. [Google Scholar]
- Bond MH (1983). How language variation affects inter-cultural differentiation of values by Hong Kong bilinguals. Journal of Language and Social Psychology, 2, 57–66. [Google Scholar]
- Briley DA, Morris MW, & Simonson I (2005). Cultural Chameleons: Biculturals, Conformity Motives, and Decision Making. Journal of Consumer Psychology, 15(4), 351–362. [Google Scholar]
- Brislin RW (1970). Back-translation for cross-cultural research. Journal of Cross-Cultural Psychology, 1(3), 185–216. [Google Scholar]
- Broniatowski DA, Jamison AM, Qi S, AlKulaib L, Chen T, Benton A, … & Dredze M (2018). Weaponized health communication: Twitter bots and Russian trolls amplify the vaccine debate. American Journal of Public Health, 108(10), 1378–1384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corey JD, Hayakawa S, Foucart A, Aparici M, Botella J, Costa A, & Keysar B (2017). Our moral choices are foreign to us. Journal of Experimental Psychology: Learning, Memory, and Cognition, 43(7), 1109–1128. [DOI] [PubMed] [Google Scholar]
- Costa A, Foucart A, Hayakawa S, Aparici M, Apesteguia J, Heafner J, & Keysar B (2014a). Your morals depend on language. PloS One, 9(4), e94842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costa A, Foucart A, Arnon I, Aparici M, & Apesteguia J (2014b). “Piensa” twice: On the foreign language effect in decision making. Cognition, 130(2), 236–254. [DOI] [PubMed] [Google Scholar]
- Davies GM, & Thomson DM (Eds.). (1988). Memory in context: Context in memory. Chichester, English: John Wiley & Sons. [Google Scholar]
- Dewaele JM (2008). The emotional weight of I love you in multilinguals’ languages. Journal of Pragmatics, 40(10), 1753–1780. [Google Scholar]
- Dewaele JM, & Costa B (2013). Multilingual clients’ experience of psychotherapy. Language and Psychoanalysis, 2(2), 31–50. [Google Scholar]
- De Meulenaer S, De Pelsmacker P, & Dens N (2015). Have no fear: How individuals differing in uncertainty avoidance, anxiety, and chance belief process health risk messages. Journal of Advertising, 44(2), 114–125. [Google Scholar]
- De Meulenaer S, De Pelsmacker P, & Dens N (2018). Power distance, uncertainty avoidance, and the effects of source credibility on health risk message compliance. Health communication, 33(3), 291–298. [DOI] [PubMed] [Google Scholar]
- Deschepper R, Grigoryan L, Lundborg CS, Hofstede G, Cohen J, Van Der Kelen G, … & Haaijer-Ruskamp FM (2008). Are cultural dimensions relevant for explaining cross-national differences in antibiotic use in Europe?. BMC Health Services Research, 8(1), 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finset A, Bosworth H, Butow P, Gulbrandsen P, Hulsman RL, Pieterse AH, … & van Weert J (2020). Effective health communication–a key factor in fighting the COVID-19 pandemic. Patient Education and Counseling, 103(5), 873–876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gebbers T, De Wit JB, & Appel M (2017). Health communication transportation into narrative worlds and the motivation to change health-related behavior. International Journal of Communication, 11, 4886–4906. [Google Scholar]
- Geipel J, Hadjichristidis C, & Klesse AK (2018). Barriers to sustainable consumption attenuated by foreign language use. Nature Sustainability, 1(1), 31–33. [Google Scholar]
- Geipel J, Hadjichristidis C, & Surian L (2015). The foreign language effect on moral judgment: The role of emotions and norms. PloS one, 10(7), e0131529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hadjichristidis C, Geipel J, & Savadori L (2015). The effect of foreign language in judgments of risk and benefit: The role of affect. Journal of Experimental Psychology: Applied, 21(2), 117–129. [DOI] [PubMed] [Google Scholar]
- Hadjichristidis C, Geipel J, & Surian L (2019). Breaking magic: Foreign language suppresses superstition. Quarterly Journal of Experimental Psychology, 72(1), 18–28. [DOI] [PubMed] [Google Scholar]
- Harris CL, Aycicegi A, & Gleason JB (2003). Taboo words and reprimands elicit greater autonomic reactivity in a first language than in a second language. Applied Psycholinguistics, 24(4), 561–579. [Google Scholar]
- Hayakawa S, Costa A, Foucart A, & Keysar B (2016). Using a foreign language changes our choices. Trends in Cognitive Sciences, 20(11), 791–793. [DOI] [PubMed] [Google Scholar]
- Hayakawa S, & Keysar B (2018). Using a foreign language reduces mental imagery. Cognition, 173, 8–15. [DOI] [PubMed] [Google Scholar]
- Hayakawa S, Lau BKY, Holtzmann S, Costa A, & Keysar B (2019). On the reliability of the foreign language effect on risk-taking. Quarterly Journal of Experimental Psychology, 72(1), 29–40. [DOI] [PubMed] [Google Scholar]
- Hayakawa S, Tannenbaum D, Costa A, Corey JD, & Keysar B (2017). Thinking more or feeling less? Explaining the foreign-language effect on moral judgment. Psychological Science, 28(10), 1387–1397. [DOI] [PubMed] [Google Scholar]
- Hofstede GH (1980). Culture’s consequences: International differences in work-related values. Beverly Hills, CA: Sage. [Google Scholar]
- Hofstede GH (1991). Cultures and organizations: Software of the mind. London, England: McGraw-Hill. [Google Scholar]
- Hong YY, & Mallorie LM (2004). A dynamic constructivist approach to culture: Lessons learned from personality psychology. Journal of Research in Personality, 38, 59–67. [Google Scholar]
- Huynh TLD (2020). Does culture matter social distancing under the COVID-19 pandemic?. Safety Science, 130, 104872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hsu CT, Jacobs AM, & Conrad M (2015). Can Harry Potter still put a spell on us in a second language? An fMRI study on reading emotion-laden literature in late bilinguals. Cortex, 63, 282–295. [DOI] [PubMed] [Google Scholar]
- Jensen LC, Harris K, & Anderson DC (1971). Retention following a change in ambient contextual stimuli for six age groups. Developmental Psychology, 4(3), 394–299. [Google Scholar]
- Kemmelmeier M, & Cheng BY-M (2004). Language and self-construal priming: A replication and extension in a Hong Kong sample. Journal of Cross-cultural Psychology, 35(6), 705–712. [Google Scholar]
- Keysar B, Hayakawa SL, & An SG (2012). The foreign-language effect: Thinking in a foreign tongue reduces decision biases. Psychological Science, 23(6), 661–668. [DOI] [PubMed] [Google Scholar]
- Kim HS, & Drolet A (2003). Choice and self-expression: A cultural analysis of variety-seeking. Journal of Personality and Social Psychology, 85, 373–382. [DOI] [PubMed] [Google Scholar]
- Kim MS, Smith DH, & Yueguo G (1999). Medical decision making and Chinese patients’ self-construals. Health Communication, 11(3), 249–260. [Google Scholar]
- Kite J, Foley BC, Grunseit AC, & Freeman B (2016). Please like me: Facebook and public health communication. PloS one, 11(9), e0162765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krishna A, & Thompson TL (2019). Misinformation about health: a review of health communication and misinformation scholarship. American Behavioral Scientist, 0002764219878223. [Google Scholar]
- Kroll JF & de Groot AM (1997). Lexical and conceptual memory in the bilingual: Mapping form to meaning in two languages,” in Tutorials in Bilingualism: Psycholinguistic Perspectives, ed. de Groot Annette and Kroll Judith F., Mahwah, NJ: Erlbaum, 169–99. [Google Scholar]
- Luna D, Ringberg T, & Perrachio LA (2008). One Individual, Two Identities: Frame Switching Among Biculturals. Journal of Consumer Research, 35(2), 279–293. [Google Scholar]
- Marian V, Blumenfeld HK, & Kaushanskaya M (2007). The Language Experience and Proficiency Questionnaire (LEAP-Q): Assessing language profiles in bilinguals and multilinguals. Journal of Speech, Language, and Hearing Research, 50(4), 940–967. [DOI] [PubMed] [Google Scholar]
- Marian V, & Fausey CM (2006). Language-dependent memory in bilingual learning. Applied Cognitive Psychology, 20(8), 1025–1047. [Google Scholar]
- Marian V, & Kaushanskaya M (2004). Self-Construal and Emotion in Bicultural Bilinguals. Journal of Memory and Language, 51(2), 190–201. [Google Scholar]
- Marian V, & Kaushanskaya M (2007). Language context guides memory content. Psychonomic Bulletin & Review, 14(5), 925–933. [DOI] [PubMed] [Google Scholar]
- Marian V, & Neisser U (2000). Language-dependent recall of autobiographical memories. Journal of Experimental Psychology: General, 129(3), 361–368. [DOI] [PubMed] [Google Scholar]
- Marsh BU, Kanaya T, & Pezdek K (2015). The language dependent recall effect influences the number of items recalled in autobiographical memory reports. Journal of Cognitive Psychology, 27(7), 829–843. [Google Scholar]
- Meeuwesen L, van den Brink-Muinen A, & Hofstede G (2009). Can dimensions of national culture predict cross-national differences in medical communication?. Patient Education and Counseling, 75(1), 58–66. [DOI] [PubMed] [Google Scholar]
- Merunka DR (2013). Reinterpreting cultural priming effects in cross-cultural consumer research. AMS Review, 3(4), 232–248. [Google Scholar]
- Panayiotou A (2004). Switching Codes, Switching Code: Bilinguals’ Emotional Responses in English and Greek. Journal of Multilingual and Multicultural Development, 25(2&3), 124–139. [Google Scholar]
- Ramírez-Esparza N, Gosling SD, Benet-Martínez V, Potter JP, & Pennebaker JW (2006). Do bilinguals have two personalities? A special case of cultural frame switching. Journal of Research in Personality, 40(2), 99–120. [Google Scholar]
- Ralston DA, Cunniff MK, & Gustafson DJ (1995). Cultural accommodation: The effect of language on the response of bilingual Hong Kong Chinese managers. Journal of Cross-Cultural Psychology, 26(6), 714–727. [Google Scholar]
- Ross M, Xun WE, & Wilson AE (2002). Language and the bicultural self. Personality and Social Psychology Bulletin, 28(8), 1040–1050. [Google Scholar]
- Smith SM, & Vela E (2001). Environmental context-dependent memory: A review and meta-analysis. Psychonomic Bulletin & Review, 8(2), 203–220. [DOI] [PubMed] [Google Scholar]
- Tulving E, & Thomson DM (1973). Encoding specificity and retrieval processes in episodic memory. Psychological Review, 80(5), 352–373. [Google Scholar]
- Verkuyten M, & Pouliasi K (2002). Biculturalism among older children: Cultural frame switching, attributions, self-identification, and attitudes. Journal of Cross-Cultural Psychology, 33(6), 596–609. [Google Scholar]
- Wang C, Ma Y, & Han S (2014). Self-construal priming modulates pain perception: event-related potential evidence. Cognitive Neuroscience, 5(1), 3–9. [DOI] [PubMed] [Google Scholar]
- Wright KB (2020). New technologies and health communication. The Handbook of Applied Communication Research, 863–878. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.