

Abstract
Background:
The optimal management of unruptured cerebral aneurysms is widely debated in the medical field. Rapid technology advances, evolving understanding of underlying pathophysiology, and shifting practice patterns have made the cerebrovascular field particularly dynamic in recent years. Despite progress, there remains a dearth of large randomized studies to help guide the management of these controversial patients.
Methods:
We review the existing literature on the natural history of unruptured cerebral aneurysms and highlight ongoing research aimed at improving our ability to stratify risk in these patients.
Results:
Landmark natural history studies demonstrated the significance of size, location, and other risk factors for aneurysm rupture, but prior studies have significant limitations. We have begun to understand the underlying pathophysiology behind aneurysm formation and rupture and are now applying new tools such as flow dynamics simulations and machine learning to individualize rupture risk stratification.
Conclusion:
Prior studies have identified several key risk factors for aneurysmal rupture, but have limitations. New technology and research methods have enabled us to better understanding individual rupture risk for patients with unruptured cerebral aneurysms.
Keywords: Aneurysm, Cerebrovascular, Computational flow dynamics, Endovascular, Machine learning, Open vascular neurosurgery, Subarachnoid hemorrhage

BACKGROUND
Cerebral aneurysms [Figure 1] are relatively common in the general population. Several autopsy and radiographic studies have investigated the prevalence of these lesions, with estimates ranging between 2% and 5%[15,30,64] and exceeding 19% in high-risk populations.[9] Aneurysmal rupture can be a catastrophic event. Mortality after aneurysmal subarachnoid hemorrhage (aSAH) is as high 10–12% within the first 24 h,[28,59] 19–45% at 1 week,[2,60] and 25–60% at 3 months.[2,81]
Figure 1:
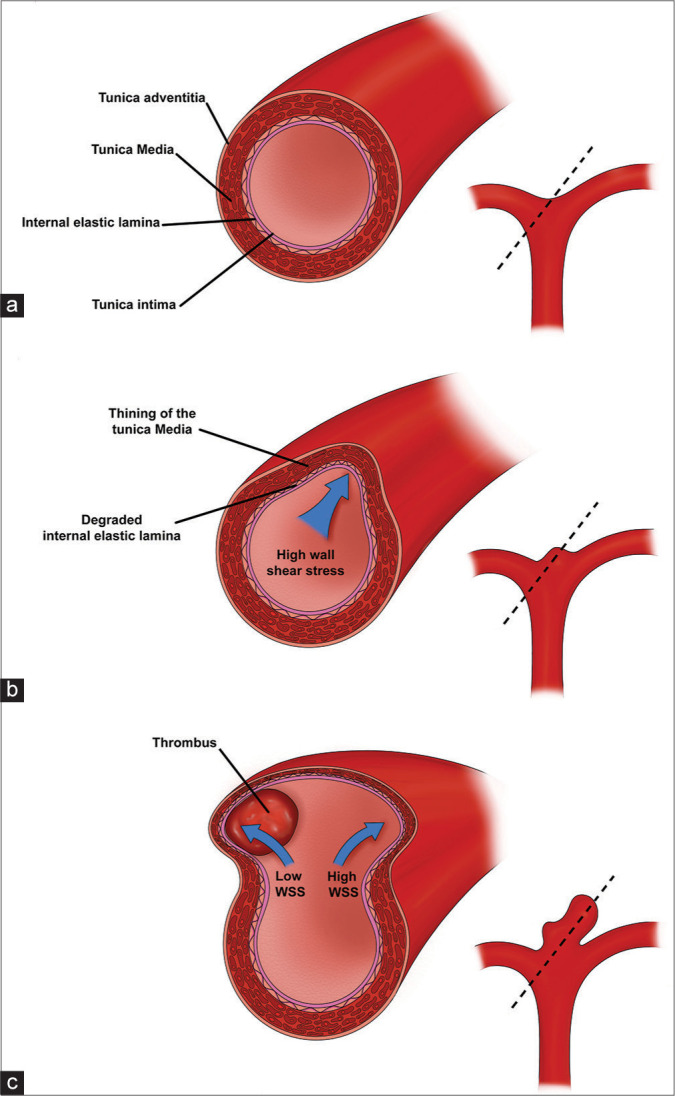
Aneurysm wall pathophysiology and progression. (a) The normal arterial vessel wall consists of an inner endothelial layer (tunica intima) followed by the two strength layers: internal elastic lamina and the smooth-muscle of the tunica media. Dotted line represents the region of the cross-sectional image displayed on the left (b) Regions of high WSS (blue arrow) (e.g., vessel bifurcations and outer wall of curved vessels) trigger an inflammatory cascade, increased protease activity, and breakdown of the tunica media and internal elastic lamina. Loss of integrity of the strength layers of the vessel wall cause outpouching of the vessel wall and formation of an early aneurysm bulge. (c) Enlargement of the aneurysm sac alters the flow dynamics, leading to areas of low WSS and high WSS (blue arrows). Areas of low WSS can develop thrombus, which trigger further inflammation and wall breakdown. Areas of persistent high WSS continue to experience protease activity and inflammation leading to continues degradation of the tunica media and internal elastic lamina.
The rate of repeat hemorrhage after aSAH rises steadily for the first 7 days and then tapers at 3 weeks.[24] For those who survive, rates of disability are extremely high, with only one-third of patients achieving favorable outcome (modified Rankin scale 1–3) at 1-year.[79] At long-term follow-up, just 62% of previously employed patients return to work,[72] and only half of elderly patients with aSAH return to living at home.[88] The social and economic repercussions of aSAH are particularly problematic since patients tend to be young and healthy. Indeed, aSAH accounts for just 4.4% of stroke mortality, but 27.3% of years of life lost due to stroke.[35] Given the extremely poor natural history of aSAH, it is important to treat unruptured aneurysms that are at high risk for rupture while balancing rupture risk with the risk of aneurysm treatment. Identifying which aneurysms are high risk is challenging and actively debated.
NATURAL HISTORY OF UNRUPTURED INTRACRANIAL ANEURYSMS
A series of landmark studies describe the natural history of unruptured cerebral aneurysms. The best-known of these studies is the International Study of Unruptured Intracranial Aneurysms (ISUIA) which was published in several phases throughout the late 1990s and early 2000s.
The ISUIA I study was a hybrid retrospective and prospective study published in 1998. In the retrospective portion, 1449 patients with 1937 unruptured cerebral aneurysms with a mean duration of follow-up of 8.3 years were analyzed. The study described a 0.05% annual risk of rupture for aneurysms <10 mm (727 patients), which rose to 0.5% among patients with a prior history of ruptured aneurysm (722 patients). Rupture risk increased with aneurysm diameter, with aneurysms larger than 25 mm carrying a 6% annual risk of rupture.[31] In the prospective portion of the study, treatment related morbidity and mortality in 1172 patients with unruptured aneurysms was found to be 15.7% at 1 year. The authors concluded that the risks of surgery outweighed the annual risk of rupture for aneurysms <10 mm. However, the study is limited by short follow-up and is unable to capture the lifetime rupture risk that is saved by treatment, thus underestimating the full benefits of surgery. Although controversial, this study was an early demonstration of the importance of aneurysm size, personal history of aSAH, and age in estimating aneurysm rupture risk and the role of treatment.
The ISUIA 2 study assessed 4060 patients (1692 managed conservatively, 1917 with open surgery, 451 endovascular treatment) with unruptured aneurysms. Importantly, ISUIA investigated the impact of both size and location on 5-year cumulative rupture risk. The results corroborated earlier findings that larger size was associated with increased rupture risk, concluding that anterior circulation aneurysms <7 mm had a 0% rupture risk over 5 years. In contrast, posterior circulation and posterior communicating artery aneurysms of at least 25 mm had a 50% 5-year cumulative rupture rate.[91] However, patient selection and drop out are key limitations of this study. For instance, a significant number of patients were excluded from the study if their perceived risk of treatment was low (i.e., young healthy patients) or if their perceived rupture risk was high (because they were treated and excluded from analysis).[16,80] The high rate of crossover, with over 500 patients excluded from analysis because they received treatment for their aneurysm, may have excluded high risk lesions from the final analysis, as it is not made clear why these aneurysms were treated.[63] In addition, selection bias may have favored lower risk aneurysms, as there were significant differences between the conservatively-managed cohort and the intervention cohort in aneurysm size, location, patient age, and presenting symptoms. An older patient population is particularly problematic because it leads to shorter follow-up times.[63] Despite these limitations, ISUIA was an important step toward a better understanding of the natural history of unruptured aneurysms.
Natural history studies out of Finland (Juvela et al., 2000) and Japan (Unruptured Cerebral Aneurysm Study of Japan [UCAS], 2012) reported similar findings with additional nuances. Juvela et al. followed 2575 patients over nearly 20 years.[38] Their retrospective cohort consisted of mostly unruptured MCA (45%) and ICA (44%) aneurysms diagnosed before 1979 with follow-up. They found an overall annual rupture rate of 1.3%. Importantly, this study consisted predominantly of patients with a previously treated ruptured aneurysm and another unruptured aneurysm that was managed conservatively. Whether aneurysm multiplicity influences rupture risk of individual aneurysms remains to be elucidated,[43,52,65] but personal history of subarachnoid hemorrhage is associated with increased rupture risk[25] and calls to question the generalizability of their study. Compared to ISUIA, patients in the Finnish series were younger, had smaller aneurysms (mean 5 mm), and were followed for a longer period of time with fewer excluded patients. Even in their cohort of small aneurysms in young patients, larger aneurysm size was significantly associated with rupture. In several follow-up studies from Juvela et al., they have demonstrated the association between smoking, young age, and aneurysm growth with rupture.[40] In one analysis of 111 aneurysms followed for over 20 years, all aneurysms that went on to rupture had increased in size by at least 1mm on preceding follow-up.[42] Like ISUIA, aneurysm size of 7 mm or greater was an independent predictor of rupture.[37,40] Female sex and smoking were associated with aneurysm growth and rupture, even when adjusting for other variables.[39,40]
The UCAS study was a prospective natural history study from Japan.[32] In their cohort of 5720 patients, they found an average 0.95% annual rupture risk that varied significantly with size, location, and morphology. Their location subgroup analysis differed from ISUIA in that they isolated posterior communicating artery (pcomm) aneurysms and anterior communicating artery (acomm) aneurysms as being most strongly associated with increased rupture risk. In contrast, ISUIA classified pcomm aneurysms as posterior circulation and acomm as anterior circulation. Importantly, UCAS was the first large natural history study to find a significant association between aneurysm morphology and rupture risk, concluding that specifically presence of a daughter sac was associated with rupture. Interestingly, UCAS found that the previous SAH from another aneurysm, smoking, and family history were not a risk factor for rupture. Similar to other natural history studies, the UCAS study cohort may not represent the general population because patients who are deemed either low risk for rupture and/or high risk for treatment were followed over time.[80] Indeed, patients in the UCAS study were older (40% over the age of 70) and less likely to be smokers (15%). Moreover, many aneurysms (48% of initially included patients) were treated during the study and excluded from the final analysis. These higher-risk lesions excluded from analysis represents selection bias, likely underestimating overall rupture risk.
To consolidate these findings Greving et al. performed a meta-analysis from 6 prospective natural history studies[32,33,38,78,90,91] and developed the PHASES aneurysm risk score, which attributes points to variables associated with aneurysmal rupture.[25] Their pooled analysis of over 8000 patients determined the following factors to be predictive of rupture risk: Age over 70, hypertension, aneurysm size, prior subarachnoid hemorrhage, location (anterior cerebral artery, pcomm, or posterior circulation as highest risk), and Finnish or Japanese background. The PHASES score has been validated in several retrospective and prospective studies[4,7,21] and may also be correlated with poor functional outcome after aSAH.[21] However, some studies have found that the majority of aSAH patients present with a low PHASES score, suggesting that the score may not fully capture rupture risk.[21,66]
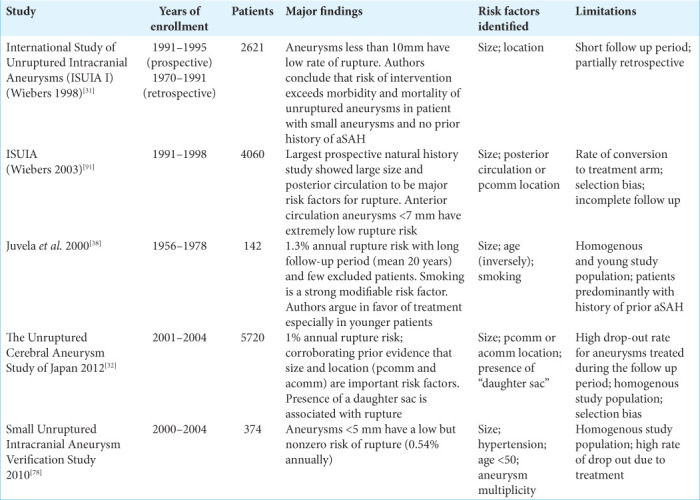
A summary of the major natural history studies of unruptured cerebral aneurysms is shown in [Table 1].
Table 1:
Summary of major natural history studies.
ANEURYSM SIZE
The debate over the importance of aneurysm size in predicting rupture risk is ongoing. The natural history studies reviewed above consistently show that increased aneurysm size is a risk factor for rupture. ISUIA, which reported a 0% rate of rupture for aneurysms <7 mm in the anterior circulation,[91] is commonly cited as evidence against treatment of small anterior circulation aneurysms. However, 70% of the aneurysms that subsequently ruptured in the Finnish study were <6 mm,[38] and 72% of aneurysms in a large meta-analysis of 56,304 patients were <6 mm.[64] Median size of ruptured aneurysms in a large series of nearly 2000 patients was 7 mm.[45]
Reconciling this data is the subject of ongoing debate. It has been proposed that post-rupture aneurysm size may not represent the size of an aneurysm at the time of rupture, suggesting that perhaps the small ruptured aneurysms we see were actually larger at the time of rupture. However, Rahman et al. evaluated imaging of 13 patients who had pre- and post-rupture imaging and found that none had significantly decreased in size and in fact 53.8% increased in size after rupture.[61] Other studies have also demonstrated that aneurysms do not seem to shrink (and may even increase in size) after rupture.[93,94] Current evidence suggests that post-rupture size is similar to pre-rupture size.
The constancy of aneurysm growth has also been called to question. Aneurysm growth has been shown to be associated with rupture.[40,87] However, aneurysms may experience periods of growth followed by periods of stagnancy, and their rupture risk may depend on their growth phase.[44,55,69] Aneurysms that have been stable over time carry a different risk profile than newly discovered lesions.[47] A subset of small aneurysms grow with time,[10] and it has also been proposed that small aneurysms may be at highest risk of rupture shortly after formation.[47,55,69] Importantly, these lesions would not have been captured in most of the natural history studies because small symptomatic or growing aneurysms were typically treated. Moreover, these irregular growth patterns highlight the limitations of natural history studies with short follow-up periods, which may underestimate the lifetime rupture risk. Indeed, when aneurysms are followed for many years, lifetime rupture risk reaches nearly 30%.[46]
Moreover, it is impossible to know the true denominator when estimating the risk of rupture of small aneurysms. Autopsy studies, radiographic surveys, and meta-analyses have consistently shown a high percentage of small aneurysms. Dr. Housepian’s autopsy data from the 1910s to 1950s found that 45% of the aneurysms found among his nearly 6000 brain autopsies were <6 mm.[30] More recent studies have corroborated his findings, showing that 50– 72% of aneurysms are <6 mm.[1,64] Even if the rupture risk of small aneurysms is exceedingly low, with a large enough denominator there will inevitably be a reasonable number of small aneurysms that present ruptured.
The Small Unruptured Intracranial Aneurysm Verification Study out of Japan in 2010 sought to address this very issue. This prospective study of 374 patients with aneurysms <5 mm found a 0.5% overall annual rupture risk, further demonstrating the nonzero risk of rupture for small aneurysms.[78] Size remained an important risk factor in their study; size >4 mm was associated with increased rupture risk. Hypertension, young age, and aneurysm multiplicity were also identified as risk factors.[78]
In summary, the literature on small aneurysms suggests that they may have a very low rupture risk. However, given the high morbidity and mortality associated with rupture in combination with the high prevalence of small aneurysms (likely over 50%), further studies are necessary to weigh the risks and benefits of treatment versus observation.
HERITABILITY AND FAMILY HISTORY
As many as, 10–20% of patients with aSAH have a positive family history of aneurysmal rupture.[70,95] In addition, familial aneurysms (i.e., in patients with at least one direct relative with a ruptured aneurysm) have a higher rate of rupture compared to matched sporadic aneurysms.[8] Syndromic cases of intracranial aneurysms from, for example, autosomal dominant polycystic kidney disease (APCKD), have been well described. Patients with APCKD are more likely to develop aneurysms and tend to rupture earlier than patients with non-syndromic aneurysms.[23] Ehlers-Danlos syndrome and other connective tissue disorders have been proposed to be associated with increased risk of intracranial aneurysms; however, more research is needed to investigate the genetic basis of these associations.[29]
MODIFIABLE RISK FACTORS
Hypertension and smoking have been demonstrated by several studies to be associated with increased risk of aneurysmal rupture.[14,19,25,82] A large prospective study out of Norway with over 20 years of follow-up showed that systolic and diastolic blood pressure has a positive correlation with aneurysmal rupture risk.[68] Their data also demonstrated a strong association between current or former smoking and rupture risk. In fact, current smoking carried a higher risk of rupture compared to former smoking,[68] suggesting that this risk factor is modifiable with lifestyle changes. Epidemiologic studies suggest that these results are generalizable to broader populations; both smoking and hypertension have been consistently shown to be risk factors for aSAH.[14,19,25,82] Smoking is associated with both aneurysmal growth and rupture.[41] In patients with both cigarette smoking and hypertension, the size at which aneurysm rupture occurs is smaller than in those without these risk factors.[18] Indeed, the American Heart Association and American Stroke Association recommend treatment of hypertension and decreased smoking to reduce the risk of aSAH.[14]
LOCATION
The major natural history studies vary in their classification of aneurysm location, thus their cumulative results leave room for interpretation. ISUIA found that pcomm and posterior circulation aneurysms (as a group) had a higher rate of rupture than anterior circulation (which included acomm, MCA, and noncavernous ICA aneurysms).[91] UCAS, on the other hand, separated pcomm and acomm aneurysms from other locations and found a significantly higher rate of rupture at these two locations.[32] The link between aneurysm location and rupture risk begs the question of whether flow dynamics and wall stress play a role in determining rupture risk, which are discussed later in this review. The size of an aneurysm relative to its parent artery may be more important than the absolute size, which may explain why pcomm and acomm aneurysms have a higher rupture risk than similarly sized aneurysms of the larger ICA or MCA. Indeed, it has been shown that higher size ratio (i.e., the ratio of aneurysm sac diameter to parent artery diameter) is associated with higher rupture risk.[62]
MORPHOLOGY
The only major natural history study to find a significant association between a morphologic feature and aneurysm rupture risk is UCAS, which found that specifically the presence of a daughter sac in the aneurysm was high risk [Figures 2a and 2b].[32]
Figure 2:
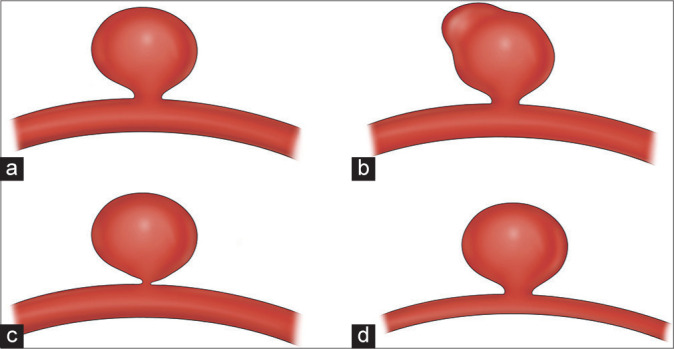
High-risk aneurysm morphologies. (a) Standard saccular aneurysm morphology. (b) Aneurysm with daughter sac. (c) Aneurysm with high aspect ratio. (d) Aneurysm with high size ratio.
Certain morphologies have been associated with aneurysm growth, which we know is associated with aneurysmal rupture.[87] The ELAPSS study, which investigated risk factors for aneurysm growth and consolidated this data into a scoring system, found that three features were associated with rupture risk: blebs, wall protrusions, and multiple lobes.[3]
A recent study from China found that aneurysm sac irregularity (lobulation or blebs) and higher aspect ratio was associated with rupture.[89] Like many studies that assess aneurysm morphology, the authors compared pre-rupture to post-rupture morphology, and they acknowledge the limitations of making such a comparison. It is important to keep in mind that post-rupture morphology may not be fully representative of pre-rupture morphology, thus studies that draw conclusions about morphology based on post-rupture imaging may not fully capture the relationship. A prospective analysis from Juvela et al. demonstrated that post-rupture morphology differs significantly from pre-rupture morphology and thus cannot be used as a proxy.[37] Aneurysm volume and ratio of volume to neck size were independent predictors of aneurysm rupture in aneurysms that were imaged and subsequently ruptured.[37]
It has also been proposed that aneurysm size and morphology may be linked in that large aneurysms are more likely to develop blebs and other high-risk morphologies compared to small aneurysms, which become more regular with growth.[48] These findings suggest that perhaps the association between size and rupture risk may be related to evolution in morphology as an aneurysm grows.
FLOW DYNAMICS
Research has increasingly focused on flow dynamics as a possible explanation for why some aneurysms are more likely to rupture than others. Several parameters have been highlighted in the literature as important. In a matched case– control study, Skodvin et al. identified a straighter inflow angle as significantly associated with ruptured cases.[77] This is one of the few studies comparing pre-rupture morphology between aneurysms that did or did not go on to rupture, thus is of particular importance.
Higher aspect ratio [i.e., the ratio of aneurysm dome diameter to neck width, Figure 2c] has also been associated with increased risk of rupture.[85] In a study by Ujiie et al. 80% of ruptured aneurysms had an aspect ratio >1.6, compared to only 10% of unruptured aneurysms.[85] A major limitation of this study, however, is that it compares unruptured to ruptured morphology which, as discussed earlier, may not be reliable.
Higher size ratio [i.e., the ratio of the maximum diameter of the aneurysm sac to the diameter of the parent vessel, Figure 2d] is associated with high-risk flow dynamics.[62] The study also found an association with rupture status, but comparing unruptured to ruptured morphology may not be reliable. Complex flow patterns with vortices and areas of low wall shear stress (WSS) have been observed in aneurysms with higher size ratios.[83] Thus, absolute aneurysm size may not fully capture the rupture potential, and small aneurysms with higher size ratios may behave more like large aneurysms.
WSS is an important concept that is now being applied to aneurysm modeling to better understand rupture risk. WSS represents the frictional force on the wall per unit area and is dependent on blood viscosity and velocity.[22] Areas of high WSS occur at the apex of vessel bifurcations, regions of vessel stenosis, and the outer wall of curved vessel segments.[22] This concept correlates with areas of cerebral vasculature where we commonly see aneurysms develop, and intuitively makes sense when thinking of which vessel regions experience trauma and subsequently are more prone to aneurysm formation. WSS may additionally help predict which areas of the aneurysm are most at risk of rupturing.[53]
A similar concept called oscillatory shear index (OSI) measures the change in the vector of blood flow throughout the cardiac cycle, a more physiologic measure of WSS in the vasculature.[11,58] Oscillatory shear stress promotes endothelial changes and triggers inflammatory pathways.[53] Unsurprisingly, higher OSI has been observed in ruptured aneurysms compare to unruptured aneurysms when matched by location and geometry.[58] The increased capability and wider use of computer simulations to model flow dynamics through different aneurysm positions, sizes, and morphologies have greatly facilitated our understanding of these parameters and their impact on rupture risk.[75]
ANEURYSM PATHOGENESIS
Cerebral arteries consist of several layers that are critical for understanding the pathophysiology of aneurysm formation. The innermost layer, the tunica intima, consists of endothelium, and basement membrane. The tunica intima is surrounded by an internal elastic lamina, which serves as a strength layer to withstand the repeated stretch forces from each cardiac cycle. This is followed by a thick tunica media of smooth muscle and then the thin adventitia (which is present in the proximal cerebral vessels but not distally); there is no external elastic lamina [Figure 1].[6] True aneurysms maintain all three layers of the vessel wall, unlike dissections or pseudoaneurysms which separate one or more layers of the vessel wall and are beyond the scope of this review. The key feature of true aneurysm development is the thinning of the tunica media and the internal elastic lamina, the two strength layers of the vessel.[53]
In vivo animal models and human histologic studies have facilitated our understanding of this process. Meng et al. used an in vivo dog model to surgically create artificial vessel bifurcations and subsequently measured hemodynamics, WSS, and histologic changes over time.[54] High WSS on the vessel wall was found to promote cellular hyperplasia in response.[53,54] Destructive remodeling ensues, whereby protease activity increases, and inflammatory cascades are triggered, leading to breakdown of the smooth muscle cells in the tunica media and degradation of the internal elastic lamina.[53] Macrophages, lymphocytes, and other inflammatory cells infiltrate the vessel wall, disrupting tight junction and producing reactive oxygen species which further increase vessel wall permeability.[73] Collagen and elastin in the vessel wall are degraded by proteases and replaced with more flexible type I collagen.[22] The now weakened vessel wall cannot tolerate the forces of arterial blood flow and a bleb is formed.
Once an early aneurysm sac has appeared, flow dynamics change dramatically [Figure 1]. Aneurysm sac growth is driven by two processes: high WSS and low WSS cascades. Areas of low flow within the aneurysm sac promote thrombus formation, which is highly inflammatory. This inflammation propagates a vicious cycle of vessel wall breakdown, weakening of the wall, aneurysm sac growth, and further thrombus formation.[22] Other regions of the aneurysm sac may experience persistent high WSS, which further traumatizes the weakened vessel wall, promotes protease activity, damages the endothelium, thins the tunica media, and promotes aneurysm sac growth.[53] Aneurysm sac growth increases wall tension (a product of pressure, radius, and wall thickness) until the intramural stress reaches the point of failure and the aneurysm ruptures.[22]
RADIOGRAPHIC PREDICTION
MRI is increasingly being used to detect aneurysms at higher risk of rupture. It has been shown that gadolinium enhancement of the aneurysm wall on MRI is associated with areas of low WSS.[92] Given the results of prior studies showing the relationship between low WSS and aneurysm growth and rupture,[22] MRI enhancement may be a useful tool to identify high risk aneurysms. In fact, a prospective study by Vergouwen et al. found that 21% of aneurysms with gadolinium enhancement on MRI grew or ruptured over their follow up period (mean = 27 months), whereas 0% of non-enhancing aneurysms grew or ruptured.[86] Understanding that aneurysm growth is associated with higher risk of rupture,[87] one can conclude that MRI enhancement may be predictive of future rupture.
More advanced imaging modalities have shown promise in identifying unstable aneurysms and predicting future rupture. Given the known role of inflammation in the development of the aneurysm sac,[13,73] it is thought that inflammation in the aneurysm wall may indicated instability and is thus the target of new imaging technology.[84] 7T MRI has been shown to identify thinning of the aneurysm wall where WSS and thus rupture risk might be highest.[5] Similarly, high resolution quantitative susceptibility mapping has been used to identify micro hemorrhages from sentinel bleeding that may predict future hemorrhage.[56]
Ferumoxytol is an FDA-approved iron oxide used for iron deficiency anemia, which appears hyperintense on T1 and hypointense on T2 gradient echo sequences. It is cleared by macrophages and is, therefore, useful for identifying regions of active inflammation.[12] Early uptake of the molecule in the aneurysm wall on ferumoxytol-enhanced MRI has been associated with aneurysm instability and increased risk of rupture.[27]
MACHINE LEARNING (ML)
Due to the complexity of risk stratification for aSAH, some groups have turned to novel data analytics tools to better understand aneurysm rupture risk. ML algorithms, of which there are many types, have revolutionized high throughput data analysis because of their ability to detect patterns in data that traditional statistics may not.[36] ML algorithms are fed either labeled or unlabeled data and iteratively test the algorithm on new input data. ML can be supervised (i.e., trained on labeled input and output data to optimize the algorithm to predict the output of new data) or unsupervised (i.e., trained on unlabeled input data to allow the algorithm to detect new patterns or associations).[51] The model is trained and optimized on a training data set until the parameters that achieve the best performance are determined. The algorithm is validated on external data and can then be easily applied to new data. The iterative nature of ML algorithm training allows for the simulation of large quantities of input data which would otherwise be difficult to achieve with traditional statistics.[51] Furthermore, the unsupervised or partially supervised nature of many algorithms allows ML to detect novel associations without being explicitly programmed with a particular hypothesis in mind.[36,57]
ML is increasingly used throughout medicine, neurosurgery, and has even integrated itself into many aspects of our daily life.[36,71] After being trained on one dataset, it can be applied to new data, making implementation of ML algorithms straightforward and easily scaled. ML algorithms have been shown to identify features associated with rupture that closely match the findings of the landmark natural history studies.[76] Similar to ISUIA and UCAS, random forest and support vector machine models highlighted pcomm, acomm, and posterior circulation aneurysms as most strongly associated with rupture, and also found size to be a clear risk factor.[76] The consistency of these results supports the validity of ML as a reliable tool for analyzing big data. Other studies have shown that ML can predict rupture status based on hemodynamic, clinical, and morphologic parameters[74] and even identify aneurysms on digital subtraction angiography.[26] Additional research is needed to identify a clinical role for ML in the management of patients with unruptured aneurysms.
CONCLUSION
Our understanding of unruptured cerebral aneurysms and their risk of rupture has improved over the past several decades. However, it remains challenging to identify aneurysms at high risk for rupture and to individualize risk stratification for unruptured aneurysms. Natural history data tells us that size, location, and family history, among other variables, are important for estimating rupture risk. Newer tools such as flow dynamics analysis, in vivo aneurysm models, and ML have improved our ability to predict which aneurysms are at higher risk of rupture. Despite significant progress, there remains uncertainty and debate regarding the natural history of unruptured cerebral aneurysms, even among cerebrovascular specialists.[17]
As the cerebrovascular field continues to evolve, we will continue to see the expansion of endovascular treatment options[50,67] and aneurysm treatment availability.[20] For both open and endovascular treatment of aneurysms, complications rates and length of stay have steadily decreased over the past two decades.[34,49] Nonetheless, it is important that we continue to hone our ability to identify which patients warrant treatment in the context of the natural history of unruptured aneurysms and taking into account the new tools that are being developed to stratify risk in these patients.
Footnotes
How to cite this article: Silva MA, Chen S, Starke RM. Unruptured cerebral aneurysm risk stratification: Background, current research, and future directions in aneurysm assessment. Surg Neurol Int 2022;13:182.
Contributor Information
Michael A. Silva, Email: michael.silva@jhsmiami.org.
Stephanie Chen, Email: stephanie.chen@jhsmiami.org.
Robert M. Starke, Email: rstarke@med.miami.edu.
Disclosures
RMS research is supported by the NREF, Joe Niekro Foundation, Brain Aneurysm Foundation, Bee Foundation, and by National Institute of Health (R01NS111119-01A1) and (UL1TR002736, KL2TR002737) through the Miami Clinical and Translational Science Institute, from the National Center for Advancing Translational Sciences and the National Institute on Minority Health and Health Disparities. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. RMS has an unrestricted research grant from Medtronic and has consulting and teaching agreements with Penumbra, Abbott, Medtronic, InNeuroCo and Cerenovus.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Agarwal N, Gala NB, Choudhry OJ, Assina R, Prestigiacomo CJ, Duffis EJ, et al. Prevalence of asymptomatic incidental aneurysms: A review of 2,685 computed tomographic angiograms. World Neurosurg. 2014;82:1086–90. doi: 10.1016/j.wneu.2013.01.082. [DOI] [PubMed] [Google Scholar]
- 2.Alvord EC, Jr, Loeser JD, Bailey WL, Copass MK. Subarachnoid hemorrhage due to ruptured aneurysms. A simple method of estimating prognosis. Arch Neurol. 1972;27:273–84. doi: 10.1001/archneur.1972.00490160001001. [DOI] [PubMed] [Google Scholar]
- 3.Backes D, Rinkel GJ, Greving JP, Velthuis BK, Murayama Y, Takao H, et al. ELAPSS score for prediction of risk of growth of unruptured intracranial aneurysms. Neurology. 2017;88:1600–6. doi: 10.1212/WNL.0000000000003865. [DOI] [PubMed] [Google Scholar]
- 4.Bijlenga P, Gondar R, Schilling S, Morel S, Hirsch S, Cuony J, et al. PHASES score for the management of intracranial aneurysm: A cross-sectional population-based retrospective study. Stroke. 2017;48:2105–12. doi: 10.1161/STROKEAHA.117.017391. [DOI] [PubMed] [Google Scholar]
- 5.Blankena R, Kleinloog R, Verweij BH, van Ooij P, Ten Haken B, Luijten PR, et al. Thinner regions of intracranial aneurysm wall correlate with regions of higher wall shear stress: A 7T MRI study. AJNR Am J Neuroradiol. 2016;37:1310–7. doi: 10.3174/ajnr.A4734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bond KM, Krings T, Lanzino G, Brinjikji W. Intracranial dissections: A pictorial review of pathophysiology, imaging features, and natural history. J Neuroradiol. 2021;48:176–88. doi: 10.1016/j.neurad.2020.03.007. [DOI] [PubMed] [Google Scholar]
- 7.Brinjikji W, Pereira VM, Khumtong R, Kostensky A, Tymianski M, Krings T, et al. PHASES and ELAPSS scores are associated with aneurysm growth: A study of 431 unruptured intracranial aneurysms. World Neurosurg. 2018;114:e425–32. doi: 10.1016/j.wneu.2018.03.003. [DOI] [PubMed] [Google Scholar]
- 8.Broderick JP, Brown RD, Jr, Sauerbeck L, Hornung R, Huston J, 3rd, Woo D, et al. Greater rupture risk for familial as compared to sporadic unruptured intracranial aneurysms. Stroke. 2009;40:1952–7. doi: 10.1161/STROKEAHA.108.542571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brown RD, Jr, Huston J, Hornung R, Foroud T, Kallmes DF, Kleindorfer D, et al. Screening for brain aneurysm in the Familial Intracranial Aneurysm study: Frequency and predictors of lesion detection. J Neurosurg. 2008;108:1132–8. doi: 10.3171/JNS/2008/108/6/1132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Burns JD, Huston J, 3rd, Layton KF, Piepgras DG, Brown RD., Jr Intracranial aneurysm enlargement on serial magnetic resonance angiography: Frequency and risk factors. Stroke. 2009;40:406–11. doi: 10.1161/STROKEAHA.108.519165. [DOI] [PubMed] [Google Scholar]
- 11.Casa LD, Deaton DH, Ku DN. Role of high shear rate in thrombosis. J Vasc Surg. 2015;61:1068–80. doi: 10.1016/j.jvs.2014.12.050. [DOI] [PubMed] [Google Scholar]
- 12.Chalouhi N, Jabbour P, Magnotta V, Hasan D. The emerging role of ferumoxytol-enhanced MRI in the management of cerebrovascular lesions. Molecules. 2013;18:9670–83. doi: 10.3390/molecules18089670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chyatte D, Bruno G, Desai S, Todor DR. Inflammation and intracranial aneurysms. Neurosurgery. 1999;45:1137–46. doi: 10.1097/00006123-199911000-00024. discussion 1146-37. [DOI] [PubMed] [Google Scholar]
- 14.Connolly ES, Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the American Heart Association/ american Stroke Association. Stroke. 2012;43:1711–37. doi: 10.1161/STR.0b013e3182587839. [DOI] [PubMed] [Google Scholar]
- 15.Dell S. Asymptomatic cerebral aneurysm: Assessment of its risk of rupture. Neurosurgery. 1982;10:162–6. [PubMed] [Google Scholar]
- 16.Dumont AS, Lanzino G, Kassell NF. Unruptured aneurysms. J Neurosurg. 2002;96:52–6. doi: 10.3171/jns.2002.96.1.0052. discussion 58-60. [DOI] [PubMed] [Google Scholar]
- 17.Etminan N, Beseoglu K, Barrow DL, Bederson J, Brown RD, Jr, Connolly ES, Jr, et al. Multidisciplinary consensus on assessment of unruptured intracranial aneurysms: Proposal of an international research group. Stroke. 2014;45:1523–30. doi: 10.1161/STROKEAHA.114.004519. [DOI] [PubMed] [Google Scholar]
- 18.Etminan N, Beseoglu K, Steiger HJ, Hanggi D. The impact of hypertension and nicotine on the size of ruptured intracranial aneurysms. J Neurol Neurosurg Psychiatry. 2011;82:4–7. doi: 10.1136/jnnp.2009.199661. [DOI] [PubMed] [Google Scholar]
- 19.Feigin VL, Rinkel GJ, Lawes CM, Algra A, Bennett DA, van Gijn J, et al. Risk factors for subarachnoid hemorrhage: An updated systematic review of epidemiological studies. Stroke. 2005;36:2773–80. doi: 10.1161/01.STR.0000190838.02954.e8. [DOI] [PubMed] [Google Scholar]
- 20.Fennell VS, Martirosyan NL, Palejwala SK, Lemole GM, Jr, Dumont TM. Morbidity and mortality of patients with endovascularly treated intracerebral aneurysms: Does physician specialty matter? J Neurosurg. 2016;124:13–7. doi: 10.3171/2014.11.JNS141030. [DOI] [PubMed] [Google Scholar]
- 21.Foreman PM, Hendrix P, Harrigan MR, Fisher WS, 3rd, Vyas NA, Lipsky RH, et al. PHASES score applied to a prospective cohort of aneurysmal subarachnoid hemorrhage patients. J Clin Neurosci. 2018;53:69–73. doi: 10.1016/j.jocn.2018.04.014. [DOI] [PubMed] [Google Scholar]
- 22.Frosen J, Cebral J, Robertson AM, Aoki T. Flow-induced, inflammation-mediated arterial wall remodeling in the formation and progression of intracranial aneurysms. Neurosurg Focus. 2019;47:E21. doi: 10.3171/2019.5.FOCUS19234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gieteling EW, Rinkel GJ. Characteristics of intracranial aneurysms and subarachnoid haemorrhage in patients with polycystic kidney disease. J Neurol. 2003;250:418–23. doi: 10.1007/s00415-003-0997-0. [DOI] [PubMed] [Google Scholar]
- 24.Graf CJ. Prognosis for patients with nonsurgically-treated aneurysms. Analysis of the cooperative study of intracranial aneurysms and subarachnoid hemorrhage. J Neurosurg. 1971;35:438–43. doi: 10.3171/jns.1971.35.4.0438. [DOI] [PubMed] [Google Scholar]
- 25.Greving JP, Wermer MJ, Brown RD, Jr, Morita A, Juvela S, Yonekura M, et al. Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms: A pooled analysis of six prospective cohort studies. Lancet Neurol. 2014;13:59–66. doi: 10.1016/S1474-4422(13)70263-1. [DOI] [PubMed] [Google Scholar]
- 26.Hainc N, Mannil M, Anagnostakou V, Alkadhi H, Bluthgen C, Wacht L, et al. Deep learning based detection of intracranial aneurysms on digital subtraction angiography: A feasibility study. Neuroradiol J. 2020;33:311–7. doi: 10.1177/1971400920937647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hasan D, Chalouhi N, Jabbour P, Dumont AS, Kung DK, Magnotta VA, et al. Early change in ferumoxytol-enhanced magnetic resonance imaging signal suggests unstable human cerebral aneurysm: A pilot study. Stroke. 2012;43:3258–65. doi: 10.1161/STROKEAHA.112.673400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hijdra A, Braakman R, van Gijn J, Vermeulen M, van Crevel H. Aneurysmal subarachnoid hemorrhage. Complications and outcome in a hospital population. Stroke. 1987;18:1061–7. doi: 10.1161/01.str.18.6.1061. [DOI] [PubMed] [Google Scholar]
- 29.Hitchcock E, Gibson WT. A review of the genetics of intracranial berry aneurysms and implications for genetic counseling. J Genet Couns. 2017;26:21–31. doi: 10.1007/s10897-016-0029-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Housepian EM, Pool JL. A systematic analysis of intracranial aneurysms from the autopsy file of the Presbyterian Hospital, 1914 to 1956. J Neuropathol Exp Neurol. 1958;17:409–23. doi: 10.1097/00005072-195807000-00001. [DOI] [PubMed] [Google Scholar]
- 31.International Study of Unruptured Intracranial Aneurysms Investigators Unruptured intracranial aneurysms--risk of rupture and risks of surgical intervention. N Engl J Med. 1998;339:1725–33. doi: 10.1056/NEJM199812103392401. [DOI] [PubMed] [Google Scholar]
- 32.Investigators UJ, Morita A, Kirino T, Hashi K, Aoki N, Fukuhara S, et al. The natural course of unruptured cerebral aneurysms in a Japanese cohort. N Engl J Med. 2012;366:2474–82. doi: 10.1056/NEJMoa1113260. [DOI] [PubMed] [Google Scholar]
- 33.Ishibashi T, Murayama Y, Urashima M, Saguchi T, Ebara M, Arakawa H, et al. Unruptured intracranial aneurysms: Incidence of rupture and risk factors. Stroke. 2009;40:313–6. doi: 10.1161/STROKEAHA.108.521674. [DOI] [PubMed] [Google Scholar]
- 34.Jalbert JJ, Isaacs AJ, Kamel H, Sedrakyan A. Clipping and coiling of unruptured intracranial aneurysms among medicare beneficiaries, 2000 to 2010. Stroke. 2015;46:2452–7. doi: 10.1161/STROKEAHA.115.009777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Johnston SC, Selvin S, Gress DR. The burden, trends, and demographics of mortality from subarachnoid hemorrhage. Neurology. 1998;50:1413–8. doi: 10.1212/wnl.50.5.1413. [DOI] [PubMed] [Google Scholar]
- 36.Jordan MI, Mitchell TM. Machine learning: Trends, perspectives, and prospects. Science. 2015;349:255–60. doi: 10.1126/science.aaa8415. [DOI] [PubMed] [Google Scholar]
- 37.Juvela S, Korja M. Intracranial aneurysm parameters for predicting a future subarachnoid hemorrhage: A long-term follow-up study. Neurosurgery. 2017;81:432–40. doi: 10.1093/neuros/nyw049. [DOI] [PubMed] [Google Scholar]
- 38.Juvela S, Porras M, Poussa K. Natural history of unruptured intracranial aneurysms: Probability of and risk factors for aneurysm rupture. J Neurosurg. 2000;93:379–87. doi: 10.3171/jns.2000.93.3.0379. [DOI] [PubMed] [Google Scholar]
- 39.Juvela S, Porras M, Poussa K. Natural history of unruptured intracranial aneurysms: Probability of and risk factors for aneurysm rupture. J Neurosurg. 2008;108:1052–60. doi: 10.3171/JNS/2008/108/5/1052. [DOI] [PubMed] [Google Scholar]
- 40.Juvela S, Poussa K, Lehto H, Porras M. Natural history of unruptured intracranial aneurysms: A long-term follow-up study. Stroke. 2013;44:2414–21. doi: 10.1161/STROKEAHA.113.001838. [DOI] [PubMed] [Google Scholar]
- 41.Juvela S, Poussa K, Porras M. Factors affecting formation and growth of intracranial aneurysms: A long-term follow-up study. Stroke. 2001;32:485–91. doi: 10.1161/01.str.32.2.485. [DOI] [PubMed] [Google Scholar]
- 42.Juvela S. Growth and rupture of unruptured intracranial aneurysms. J Neurosurg. 2018;131:843–51. doi: 10.3171/2018.4.JNS18687. [DOI] [PubMed] [Google Scholar]
- 43.Juvela S. Risk factors for multiple intracranial aneurysms. Stroke. 2000;31:392–7. doi: 10.1161/01.str.31.2.392. [DOI] [PubMed] [Google Scholar]
- 44.Koffijberg H, Buskens E, Algra A, Wermer MJ, Rinkel GJ. Growth rates of intracranial aneurysms: Exploring constancy. J Neurosurg. 2008;109:176–85. doi: 10.3171/JNS/2008/109/8/0176. [DOI] [PubMed] [Google Scholar]
- 45.Korja M, Kivisaari R, Jahromi BR, Lehto H. Size and location of ruptured intracranial aneurysms: Consecutive series of 1993 hospital-admitted patients. J Neurosurg. 2017;127:748–53. doi: 10.3171/2016.9.JNS161085. [DOI] [PubMed] [Google Scholar]
- 46.Korja M, Lehto H, Juvela S. Lifelong rupture risk of intracranial aneurysms depends on risk factors: A prospective Finnish cohort study. Stroke. 2014;45:1958–63. doi: 10.1161/STROKEAHA.114.005318. [DOI] [PubMed] [Google Scholar]
- 47.Lanzino G, Brown RD., Jr Natural history of unruptured intracranial aneurysms. J Neurosurg. 2012;117:50–1. doi: 10.3171/2012.1.JNS129. discussion 51-2. [DOI] [PubMed] [Google Scholar]
- 48.Leemans EL, Cornelissen BM, Said M, van den Berg R, Slump CH, Marquering HA, et al. Intracranial aneurysm growth: Consistency of morphological changes. Neurosurg Focus. 2019;47:E5. doi: 10.3171/2019.4.FOCUS1987. [DOI] [PubMed] [Google Scholar]
- 49.Luther E, McCarthy DJ, Brunet MC, Sur S, Chen SH, Sheinberg D, et al. Treatment and diagnosis of cerebral aneurysms in the post-international subarachnoid aneurysm trial (ISAT) era: Trends and outcomes. J Neurointerv Surg. 2020;12:682–7. doi: 10.1136/neurintsurg-2019-015418. [DOI] [PubMed] [Google Scholar]
- 50.Majidi SM, Mehta A, De Leacy R, Mocco J, Fifi J. Trend in mortality and morbidity after treatment of unruptured intracranial aneurysm in the United States 2006-2016. J Neurointerv Surg. 2020 O-007. [Google Scholar]
- 51.Maleki F, Ovens K, Najafian K, Forghani B, Reinhold C, Forghani R. Overview of machine learning part 1: Fundamentals and classic approaches. Neuroimaging Clin N Am. 2020;30:e17–32. doi: 10.1016/j.nic.2020.08.007. [DOI] [PubMed] [Google Scholar]
- 52.McDowell MM, Zhao Y, Kellner CP, Barton SM, Sussman E, Claassen J, et al. Demographic and clinical predictors of multiple intracranial aneurysms in patients with subarachnoid hemorrhage. J Neurosurg. 2018;128:961–8. doi: 10.3171/2017.1.JNS162785. [DOI] [PubMed] [Google Scholar]
- 53.Meng H, Tutino VM, Xiang J, Siddiqui A. High WSS or low WSS? Complex interactions of hemodynamics with intracranial aneurysm initiation, growth, and rupture: Toward a unifying hypothesis. AJNR Am J Neuroradiol. 2014;35:1254–62. doi: 10.3174/ajnr.A3558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Meng H, Wang Z, Hoi Y, Gao L, Metaxa E, Swartz DD, et al. Complex hemodynamics at the apex of an arterial bifurcation induces vascular remodeling resembling cerebral aneurysm initiation. Stroke. 2007;38:1924–31. doi: 10.1161/STROKEAHA.106.481234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Mitchell P, Jakubowski J. Estimate of the maximum time interval between formation of cerebral aneurysm and rupture. J Neurol Neurosurg Psychiatry. 2000;69:760–7. doi: 10.1136/jnnp.69.6.760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Nakagawa D, Cushing C, Nagahama Y, Allan L, Hasan D. Quantitative susceptibility mapping as a possible tool to radiographically diagnose sentinel headache associated with intracranial aneurysm: Case report. World Neurosurg. 2017;103:954.e1–4. doi: 10.1016/j.wneu.2017.04.151. [DOI] [PubMed] [Google Scholar]
- 57.Noble WS. What is a support vector machine? Nat Biotechnol. 2006;24:1565–7. doi: 10.1038/nbt1206-1565. [DOI] [PubMed] [Google Scholar]
- 58.Perera R, Isoda H, Ishiguro K, Mizuno T, Takehara Y, Terada M, et al. Assessing the risk of intracranial aneurysm rupture using morphological and hemodynamic biomarkers evaluated from magnetic resonance fluid dynamics and computational fluid dynamics. Magn Reson Med Sci. 2020;19:333–44. doi: 10.2463/mrms.mp.2019-0107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Phillips LH, 2nd, Whisnant JP, O’Fallon WM, Sundt TM., Jr The unchanging pattern of subarachnoid hemorrhage in a community. Neurology. 1980;30:1034–40. doi: 10.1212/wnl.30.10.1034. [DOI] [PubMed] [Google Scholar]
- 60.Post KD, Flamm ES, Goodgold A, Ransohoff J. Ruptured intracranial aneurysms. Case morbidity and mortality. J Neurosurg. 1977;46:290–5. doi: 10.3171/jns.1977.46.3.0290. [DOI] [PubMed] [Google Scholar]
- 61.Rahman M, Ogilvy CS, Zipfel GJ, Derdeyn CP, Siddiqui AH, Bulsara KR, et al. Unruptured cerebral aneurysms do not shrink when they rupture: Multicenter collaborative aneurysm study group. Neurosurgery. 2011;68:155–60. doi: 10.1227/NEU.0b013e3181ff357c. discussion 160-51. [DOI] [PubMed] [Google Scholar]
- 62.Rahman M, Smietana J, Hauck E, Hoh B, Hopkins N, Siddiqui A, et al. Size ratio correlates with intracranial aneurysm rupture status: A prospective study. Stroke. 2010;41:916–20. doi: 10.1161/STROKEAHA.109.574244. [DOI] [PubMed] [Google Scholar]
- 63.Raymond J, Guillemin F, Proust F, Molyneux AJ, Fox AJ, Claiborne JS, et al. A critical review of the international study of unruptured intracranial aneurysms (ISUIA) and of appropriate methods to address the clinical problem. Interv Neuroradiol. 2008;14:85–96. doi: 10.1177/159101990801400111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Rinkel GJ, Djibuti M, Algra A, van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: A systematic review. Stroke. 1998;29:251–6. doi: 10.1161/01.str.29.1.251. [DOI] [PubMed] [Google Scholar]
- 65.Roethlisberger M, Achermann R, Bawarjan S, Stienen MN, Fung C, D’Alonzo D, et al. Predictors of occurrence and anatomic distribution of multiple aneurysms in patients with aneurysmal subarachnoid hemorrhage. World Neurosurg. 2018;111:e199–205. doi: 10.1016/j.wneu.2017.12.046. [DOI] [PubMed] [Google Scholar]
- 66.Rutledge C, Jonzzon S, Winkler EA, Raper D, Lawton MT, Abla AA. Small aneurysms with low PHASES scores account for most subarachnoid hemorrhage cases. World Neurosurg. 2020;139:e580–4. doi: 10.1016/j.wneu.2020.04.074. [DOI] [PubMed] [Google Scholar]
- 67.Salahuddin H, Siddiqui NS, Castonguay AC, Johnson M, Zaidi SF, Jumaa MA. Recent trends in electively treated unruptured intracranial aneurysms. J Stroke Cerebrovasc Dis. 2019;28:2011–7. doi: 10.1016/j.jstrokecerebrovasdis.2019.03.010. [DOI] [PubMed] [Google Scholar]
- 68.Sandvei MS, Romundstad PR, Muller TB, Vatten L, Vik A. Risk factors for aneurysmal subarachnoid hemorrhage in a prospective population study: The HUNT study in Norway. Stroke. 2009;40:1958–62. doi: 10.1161/STROKEAHA.108.539544. [DOI] [PubMed] [Google Scholar]
- 69.Sato K, Yoshimoto Y. Risk profile of intracranial aneurysms: Rupture rate is not constant after formation. Stroke. 2011;42:3376–81. doi: 10.1161/STROKEAHA.111.625871. [DOI] [PubMed] [Google Scholar]
- 70.Schievink WI, Schaid DJ, Michels VV, Piepgras DG. Familial aneurysmal subarachnoid hemorrhage: A community-based study. J Neurosurg. 1995;83:426–9. doi: 10.3171/jns.1995.83.3.0426. [DOI] [PubMed] [Google Scholar]
- 71.Senders JT, Staples PC, Karhade AV, Zaki MM, Gormley WB, Broekman ML, et al. Machine learning and neurosurgical outcome prediction: A systematic review. World Neurosurg. 2018;109:476–86.e1. doi: 10.1016/j.wneu.2017.09.149. [DOI] [PubMed] [Google Scholar]
- 72.Seule M, Oswald D, Muroi C, Brandi G, Keller E. Outcome, return to work and health-related costs after aneurysmal subarachnoid hemorrhage. Neurocrit Care. 2020;33:49–57. doi: 10.1007/s12028-019-00905-2. [DOI] [PubMed] [Google Scholar]
- 73.Sheinberg DL, McCarthy DJ, Elwardany O, Bryant JP, Luther E, Chen SH, et al. Endothelial dysfunction in cerebral aneurysms. Neurosurg Focus. 2019;47:E3. doi: 10.3171/2019.4.FOCUS19221. [DOI] [PubMed] [Google Scholar]
- 74.Shi Z, Chen GZ, Mao L, Li XL, Zhou CS, Xia S, et al. Machine learning-based prediction of small intracranial aneurysm rupture status using CTA-derived hemodynamics: A multicenter study. AJNR Am J Neuroradiol. 2021;42:648–54. doi: 10.3174/ajnr.A7034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Shishir SS, Karim A, Islam AK, Hasan AB. Blood flow dynamics in cerebral aneurysm. Proc Eng. 2015;105:919–27. [Google Scholar]
- 76.Silva MA, Patel J, Kavouridis V, Gallerani T, Beers A, Chang K, et al. Machine learning models can detect aneurysm rupture and identify clinical features associated with rupture. World Neurosurg. 2019;131:e46–51. doi: 10.1016/j.wneu.2019.06.231. [DOI] [PubMed] [Google Scholar]
- 77.Skodvin TO, Evju O, Sorteberg A, Isaksen JG. Prerupture intracranial aneurysm morphology in predicting risk of rupture: A matched case-control study. Neurosurgery. 2019;84:132–40. doi: 10.1093/neuros/nyy010. [DOI] [PubMed] [Google Scholar]
- 78.Sonobe M, Yamazaki T, Yonekura M, Kikuchi H. Small unruptured intracranial aneurysm verification study: SUAVe study, Japan. Stroke. 2010;41:1969–77. doi: 10.1161/STROKEAHA.110.585059. [DOI] [PubMed] [Google Scholar]
- 79.Starke RM, Komotar RJ, Otten ML, Schmidt JM, Fernandez LD, Rincon F, et al. Predicting long-term outcome in poor grade aneurysmal subarachnoid haemorrhage patients utilising the glasgow coma scale. J Clin Neurosci. 2009;16:26–31. doi: 10.1016/j.jocn.2008.02.010. [DOI] [PubMed] [Google Scholar]
- 80.Starke RM. Small cerebral aneurysms: Can we identify patients at risk for rupture? Ann Intern Med. 2017;167:59–60. doi: 10.7326/M17-1215. [DOI] [PubMed] [Google Scholar]
- 81.Sundt TM, Jr, Whisnant JP. Subarachnoid hemorrhage from intracranial aneurysms. Surgical management and natural history of disease. N Engl J Med. 1978;299:116–22. doi: 10.1056/NEJM197807202990303. [DOI] [PubMed] [Google Scholar]
- 82.Teunissen LL, Rinkel GJ, Algra A, van Gijn J. Risk factors for subarachnoid hemorrhage: A systematic review. Stroke. 1996;27:544–9. doi: 10.1161/01.str.27.3.544. [DOI] [PubMed] [Google Scholar]
- 83.Tremmel M, Dhar S, Levy EI, Mocco J, Meng H. Influence of intracranial aneurysm-to-parent vessel size ratio on hemodynamics and implication for rupture: Results from a virtual experimental study. Neurosurgery. 2009;64:622–30. doi: 10.1227/01.NEU.0000341529.11231.69. discussion 630-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Turan N, Heider RA, Roy AK, Miller BA, Mullins ME, Barrow DL, et al. Current perspectives in imaging modalities for the assessment of unruptured intracranial aneurysms: A comparative analysis and review. World Neurosurg. 2018;113:280–92. doi: 10.1016/j.wneu.2018.01.054. [DOI] [PubMed] [Google Scholar]
- 85.Ujiie H, Tamano Y, Sasaki K, Hori T. Is the aspect ratio a reliable index for predicting the rupture of a saccular aneurysm? Neurosurgery. 2001;48:495–502. doi: 10.1097/00006123-200103000-00007. discussion 502-3. [DOI] [PubMed] [Google Scholar]
- 86.Vergouwen MD, Backes D, van der Schaaf IC, Hendrikse J, Kleinloog R, Algra A, et al. Gadolinium enhancement of the aneurysm wall in unruptured intracranial aneurysms is associated with an increased risk of aneurysm instability: A follow-up study. AJNR Am J Neuroradiol. 2019;40:1112–6. doi: 10.3174/ajnr.A6105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Villablanca JP, Duckwiler GR, Jahan R, Tateshima S, Martin NA, Frazee J, et al. Natural history of asymptomatic unruptured cerebral aneurysms evaluated at CT angiography: Growth and rupture incidence and correlation with epidemiologic risk factors. Radiology. 2013;269:258–65. doi: 10.1148/radiol.13121188. [DOI] [PubMed] [Google Scholar]
- 88.Virta JJ, Satopaa J, Luostarinen T, Raj R. One-year outcome after aneurysmal subarachnoid hemorrhage in elderly patients. World Neurosurg. 2020;143:e334–43. doi: 10.1016/j.wneu.2020.07.127. [DOI] [PubMed] [Google Scholar]
- 89.Wang Y, Cheng M, Liu S, Xie G, Liu L, Wu X, et al. Shape related features of intracranial aneurysm are associated with rupture status in a large Chinese cohort. J Neurointerv Surg. 2022;14:252–6. doi: 10.1136/neurintsurg-2021-017452. [DOI] [PubMed] [Google Scholar]
- 90.Wermer MJ, van der Schaaf IC, Algra A, Rinkel GJ. Risk of rupture of unruptured intracranial aneurysms in relation to patient and aneurysm characteristics: An updated meta-analysis. Stroke. 2007;38:1404–10. doi: 10.1161/01.STR.0000260955.51401.cd. [DOI] [PubMed] [Google Scholar]
- 91.Wiebers DO, Whisnant JP, Huston J, 3rd, Meissner I, Brown RD, Jr, Piepgras DG, et al. Unruptured intracranial aneurysms: Natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003;362:103–10. doi: 10.1016/s0140-6736(03)13860-3. [DOI] [PubMed] [Google Scholar]
- 92.Xiao W, Qi T, He S, Li Z, Ou S, Zhang G, et al. Low wall shear stress is associated with local aneurysm wall enhancement on high-resolution MR vessel wall imaging. AJNR Am J Neuroradiol. 2018;39:2082–7. doi: 10.3174/ajnr.A5806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Yasui N, Magarisawa S, Suzuki A, Nishimura H, Okudera T, Abe T. Subarachnoid hemorrhage caused by previously diagnosed, previously unruptured intracranial aneurysms: A retrospective analysis of 25 cases. Neurosurgery. 1996;39:1096–100. doi: 10.1097/00006123-199612000-00004. discussion 1100-91. [DOI] [PubMed] [Google Scholar]
- 94.Yi J, Zielinski D, Chen M. Cerebral aneurysm size before and after rupture: Case series and literature review. J Stroke Cerebrovasc Dis. 2016;25:1244–8. doi: 10.1016/j.jstrokecerebrovasdis.2016.01.031. [DOI] [PubMed] [Google Scholar]
- 95.Zhou S, Dion PA, Rouleau GA. Genetics of intracranial aneurysms. Stroke. 2018;49:780–7. doi: 10.1161/STROKEAHA.117.018152. [DOI] [PubMed] [Google Scholar]