

Abstract
Background:
Eagle’s syndrome is famous for one of the causes of internal carotid artery dissection. The treatment strategy for the illness, however, is not well established. Here, we report a case of internal carotid dissection due to an elongated styloid process successfully treated by carotid artery stenting (CAS).
Case Description:
A 72-year-old male with temporary dysarthria and consciousness disorder was diagnosed to suffer from multiple cerebral infarctions due to Eagle’s syndrome. A cerebral blood flow (CBF) study revealed decreased blood flow and a CAS was performed 15 days after admission to preserve antegrade blood flow, resulting in full recovery of the affected CBF.
Conclusion:
We reported a case of vascular Eagle’s syndrome in which the patient showed fluctuated neurological deficits successfully treated by CAS. Our experience suggests that cases of vascular Eagle’s syndrome due to hemodynamic stress can be treated by CAS.
Keywords: Carotid artery stenting, Carotid dissection, Eagle’s syndrome

INTRODUCTION
An elongated styloid process is one of the causes of ICA dissection[5,7] and the condition leading to ischemic stroke is well known as Eagle’s syndrome. The treatment strategies of Eagle’s syndrome include antithrombotic therapy, endovascular treatment, and surgical styloid process resection. However, there are few discussions regarding treatment choice in various clinical conditions. Here, the authors report a case of the left ICA dissection due to an elongated styloid process presenting unstable neurological symptoms treated by carotid artery stenting (CAS), further adding some literature reviews.
CASE PRESENTATION
A 72-year-old male was transferred to our institution presenting temporary dysarthria and consciousness disorder. Diffusion-weighted image (DWI) revealed several small infarctions [Figure 1a] and magnetic resonance angiography showed a decrease of flow signal of the right intracranial arteries [Figure 1b], which was due to partial disappearance of the high cervical portion of the left internal carotid artery (ICA) [Figure 1c]. Furthermore, a three-dimensional computed tomography angiogram (3D-CTA) revealed an elongated styloid process stenosing the nearby ICA [Figure 1d]. The arterial spin labeling study revealed a remarkable decrease in cerebral blood flow (CBF) [Figure 1e], with mural hematoma around the stenotic ICA on thin slice T1-weighted images. Angiogram examination again revealed severe stenosis of the left ICA [Figures 2a and b] at around the elongated styloid process. The final diagnosis was a case of carotid artery dissection due to the elongated styloid process (Eagle’s syndrome).
Figure 1:

Radiological images at initial symptom onset are presented. DWI showed multiple hyperintense lesions at the left hemisphere (a) and intracranial blood flow was impaired at the lesion side on magnetic resonance angiography (b: Red arrow). The blood flow signal was absent at the high cervical portion of the ICA (c: Red arrow). 3D-CTA revealed an enlarged styloid process, whose length was 32.3 mm (d), and a cerebral blood flow study by arterial spin labeling showed a remarkable CBF decrease at the affected side (e).
Figure 2:
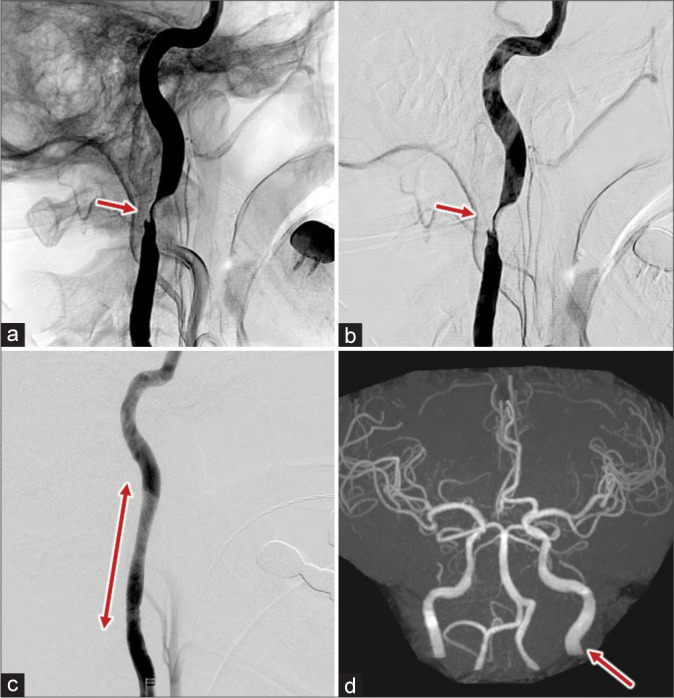
DSA at initial symptom onset (a) and 5 days later (b) are shown. The red arrows indicate the location of stenosis. Carotid artery stenting (CAS) was performed and a reasonable vascular reconstruction was achieved (c). The red arrowheads indicate the whole length of the placed stent. Magnetic resonance angiography after CAS showed recovered cerebral blood flow (d: red arrow).
As the patient’s neurological symptoms recovered during the initial assessment, medical treatment was chosen, and the patient was treated conservatively by aspirin (100 mg/body/day). Oral administration of clopidogrel (loading 150 mg/day, maintenance 75 mg/day) and intravenous infusion of argatroban were added later on, as the patient suffered from repeatedly appearing transient neurological deficits with no change in DWI. Systolic blood pressure was also maintained above 160 mmHg to counteract the cerebral hemodynamic stress. CAS was performed 15 days after admission. The procedure was performed under general anesthesia, and an eight French temporally occlusion balloon catheter (OPTIMO, Tokai Medical Products, Japan) was delivered proximal to the stenotic lesion. A micro-guidewire was passed through the lesion right after balloon inflation. The blood from the distal ICA was flowed out through to the femoral vein. After percutaneous transluminal angioplasty (PTA) for stenosis, A 6 to 8 mm tapered Carotid WALLSTENT (Boston Scientific, Boston, USA) was placed at the stenotic lesion after PTA [Figure 2c]. MRA 3d-tof improved the signal intensity compared to before CAS [Figure 2d]. Post stenting angiogram showed no distal embolization at the intracranial arteries and postoperative iodoamphetamine single-photon emission computed tomography (IMP-SPECT) showed recovered left CBF [Figure 3]. The blood pressure target was decreased to under 120 mmHg just after stent placement to prevent cerebral hyperperfusion syndrome, and the patient showed neither hyperperfusion nor ischemic symptoms. The patient was discharged to a rehabilitation hospital at a modified Rankin Scale of 2.
Figure 3:
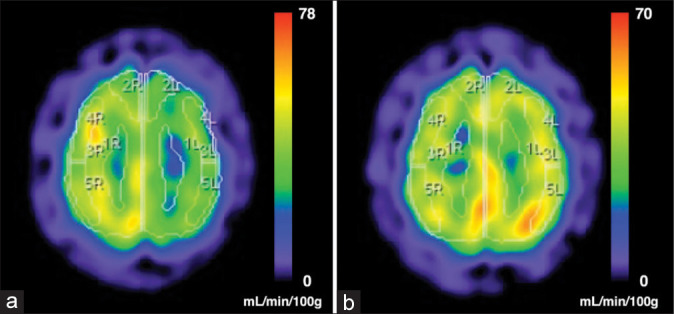
Iodoamphetamine single-photon emission computed tomography before (a) and after (b) carotid artery stenting (CAS) is shown. Cerebral blood flow of the anterior circulation decreased by 75–80% compared with that at the right side before the treatment. The decrease recovered after CAS.
DISCUSSION
The elongated styloid process is defined as that longer than 25– 30 mm[1,6,13] and it sometimes compresses the cervical nerves or arteries, leading to symptomatic conditions named Eagle’s syndrome. Although Eagle’s syndrome is famous for being one of the causes of ICA dissection, symptomatic vascular Eagle’s syndrome is rarely encountered.[2] Proposed treatments for vascular Eagle’s syndrome’s include antithrombotic therapy, endovascular revascularization, and styloid process resection. However, a gold standard treatment strategy is not established due to the small number of cases.[6,11] English-based papers on PubMed were searched and we found 17 cases referring to symptomatic ICA dissection caused by Eagle’s syndrome. Antithrombotic therapy, including antiplatelet drugs, anticoagulants, and tissue plasminogen activator, was chosen for nine cases[3,8-10,12,14] as first line treatment. On the other hand, endovascular treatment was chosen only for seven cases.[1,4-6,10,11,13] Styloid process resection was not chosen as the first-line treatment.
In our presented cases, the patient presented repeated transient neurological symptoms due to low CBF of the affected side with no change in DWI. This clinical course caused us some confusion to choose or not to choose surgical interventions. Some case reports describe worsening of neurological symptoms by trigger movements such as head flexion, tilt, and extension,[5,8] even if antithrombotic therapy was introduced. Furthermore, the choice of intervention is not well established, and there are reports treating the lesion by CAS and carotid endarterectomy.[6,7] The choice of the type of stent for CAS is another debate that should be mentioned. While open-cell stents with stronger radial force have the advantage to preserve the patency of the compressed ICA by the elongated styloid process, closed-cell stents have the advantage to prevent further embolic cerebral vascular events caused by the already injured carotid intima, as they fit the vasculature more gently than open-cell stents. In the presented case, the authors felt that the latter issue was more significant for the patient and chose a closed-cell stent.
Styloid process resection (styloidectomy) was sometimes carried out to prevent its ICA compression and we found five such cases.[3,4,6,10,11] In addition, there were two case reports where the elongated styloid process and calcified ligament compressed the stent resulting in its fracture.[4,13] Continuous compression of the carotid artery after CAS could cause intra-stent thrombosis and thromboembolism of the distal cerebral artery.[6] Thus, it might be necessary to subsequently resect the styloid process after CAS. As for the present case, although distal embolization and intra-stent thrombus were not observed, hemodynamic stress was quite strong. The authors consider that this particular case should undergo styloidectomy in the near future.
CONCLUSION
We experienced a symptomatic vascular Eagle’s syndrome with unstable neurological symptoms due to hemodynamic stress. Intervention by vascular reconstruction could be considered not only for cases suffering distal cerebral artery embolization caused by the syndrome but also for cases presenting fluctuation of neurological symptoms due to hemodynamic stress. The elongated styloid process could sometimes compress and damage the placed stent for treatment; thus, styloidectomy should be considered for most symptomatic vascular Eagle’s syndrome cases.
Footnotes
How to cite this article: Okada Y, Mitsui N, Ozaki H, Sanada T, Yamamoto S, Saito M, et al. Carotid artery dissection due to elongated styloid process treated by acute phase carotid artery stenting: A case report. Surg Neurol Int 2022;13:183.
Contributor Information
Yasuaki Okada, Email: yasu.vio04nagata@gmail.com.
Nobuyuki Mitsui, Email: nmichy0106@gmail.com.
Hirokazu Ozaki, Email: doublehorn.bass@gmail.com.
Takahiro Sanada, Email: kyokui100084@gmail.com.
Shota Yamamoto, Email: shota.ikao@gmail.com.
Masato Saito, Email: sight20.sight20.sight20@gmail.com.
Manabu Kinoshita, Email: mail@manabukinoshita.com.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Duarte-Celada WR, Jin D, Neves G, Windisch T. Bilateral carotid dissection due to Eagle syndrome in a young female. eNeurologicalsci. 2021;24:100353. doi: 10.1016/j.ensci.2021.100353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Eagle WW. Elongated styloid process: Further observations and a new syndrome. Archiv Otolaryngol. 1948;47:630–40. doi: 10.1001/archotol.1948.00690030654006. [DOI] [PubMed] [Google Scholar]
- 3.Faivre A, Abdelfettah Z, Rodriguez S, Nicoli F. Neurological picture. Bilateral internal carotid artery dissection due to elongated styloid processes and shaking dancing. J Neurology Neurosurg Psychiatry. 2009;80:1154–5. doi: 10.1136/jnnp.2008.159954. [DOI] [PubMed] [Google Scholar]
- 4.Hooker JD, Joyner DA, Farley EP, Khan M. Carotid stent fracture from stylocarotid syndrome. J Radiol Case Rep. 2016;10:1–8. doi: 10.3941/jrcr.v10i6.1618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Horio Y, Fukuda K, Miki K, Hirao N, Iwaasa M, Abe H, et al. Dynamic assessment of internal carotid artery and elongated styloid process in a case of bilateral carotid artery dissection. Surg Neurol Int. 2020;11:163. doi: 10.25259/SNI_42_2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ogura T, Mineharu Y, Todo K, Kohara N, Sakai N. Carotid artery dissection caused by an elongated styloid process: Three case reports and review of the literature. Nmc Case Rep J. 2015;2:21–5. doi: 10.2176/nmccrj.2014-0179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ohara N, Sakaguchi M, Okazaki S, Nagano K, Kitagawa K. Internal carotid artery dissection caused by an elongated styloid process: Usefulness of transoral ultrasonography. J Stroke Cerebrovasc Dis. 2012;21:918.e7.8. doi: 10.1016/j.jstrokecerebrovasdis.2012.05.014. [DOI] [PubMed] [Google Scholar]
- 8.Razak A, Short JL, Hussain SI. Carotid artery dissection due to elongated styloid process: A self-stabbing phenomenon. J Neuroimaging. 2014;24:298–301. doi: 10.1111/j.1552-6569.2012.00759.x. [DOI] [PubMed] [Google Scholar]
- 9.Soo OY, Chan YL, Wong KS. Carotid artery dissection after prolonged head tilting while holding a newborn baby to sleep. Neurology. 2004;62:1647–8. doi: 10.1212/01.wnl.0000123016.81648.b6. [DOI] [PubMed] [Google Scholar]
- 10.Sveinsson O, Kostulas N, Herrman L. Internal carotid dissection caused by an elongated styloid process (Eagle syndrome) BMJ Case Rep. 2013;2013:bcr2013009878. doi: 10.1136/bcr-2013-009878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Torikoshi S, Yamao Y, Ogino E, Taki W, Sunohara T, Nishimura M. A staged therapy for internal carotid artery dissection caused by vascular eagle syndrome. World Neurosurg. 2019;129:133–9. doi: 10.1016/j.wneu.2019.05.208. [DOI] [PubMed] [Google Scholar]
- 12.Yamamoto S, Todo K, Kawamoto M, Kohara N. Carotid artery dissection associated with an elongated styloid process. Intern Med. 2013;52:1005–6. doi: 10.2169/internalmedicine.52.0024. [DOI] [PubMed] [Google Scholar]
- 13.Yano T, Sasaki I, Kiyohara K, Kawanishi M. Carotid stent fracture due to eagle syndrome after endovascular stenting for the treatment of acute ischemic stroke caused by internal carotid artery dissection: Case report. J Neuroendovascular Ther. 2019;13:454–61. [Google Scholar]
- 14.Zuber M, Mender J, Mas J. Carotid artery dissection due to elongated styloid process. Neurology. 1999;53:1886–7. doi: 10.1212/wnl.53.8.1886. [DOI] [PubMed] [Google Scholar]