

To the Editor: We read with interest the recent paper by AlSubait et al1 on the dermatoscopy of scalp cutaneous metastasis of sigmoid adenocarcinoma. We would like to report a similar case of a patient with scalp metastasis of gastric adenocarcinoma.
A 31-year–old man with a past medical history of gastric adenocarcinoma with C2 spinal metastasis underwent cervical tumor debulking surgery as well as radiotherapy to the cervical spine. Three months later, he developed an ulcerative nodule over the superior end of the surgical site (Fig 1). Positron emission tomography-computed tomography showed fluorodeoxyglucose-avid foci along the surgical incision (right side of the C3 vertebra). He was then referred to Dermatology for further assessment of this nodule. On examination, a 1.5 cm × 1.5 cm pink nodule with central ulceration and overlying serum crust was observed over the occiput.
Fig 1.

Ulcerative nodule at the superior edge of the incision site on the occiput.
Dermatoscopy (DermLite 4, 3 Gen, Heine, DELTAone) showed a crateriform nodule with central ulceration, filled with yellow keratin. The rim of the nodule showed hairpin vessels as well as comma-shaped vessels. Moreover, shiny white lines were observed at the rim of the nodule (Fig 2).
Fig 2.
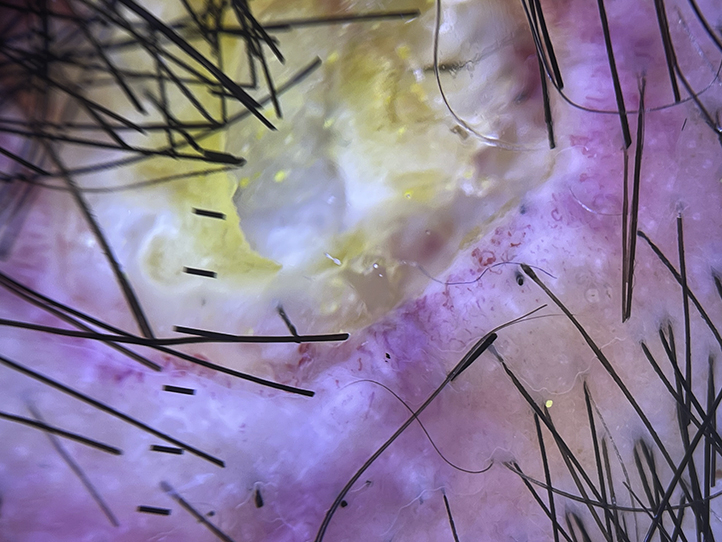
Dermatoscopy of the ulcerated nodule. Hairpin vessels, comma-shaped vessels and shiny white lines are seen at the rim of the ulcer. The central ulcer is filled with yellow keratin.
A skin biopsy was performed, and histopathology revealed adenocarcinoma characterized by diffuse infiltration of the carcinoma cells arranged as single cells and forming tubules and glands. Occasional signet ring cells were observed (Fig 3). On immunochemistry, the cells showed cytokeratin7 and cytokeratin20 positivity, along with weak, scattered caudal-type homeobox 2 positivity. Histopathology results showed positivity for adenocarcinoma, in keeping with the metastasis from the known primary upper gastrointestinal tract caricoma. He subsequently underwent radiotherapy for the metastatic nodule on his scalp.
Fig 3.

Skin biopsy of the ulcerated nodule. There was diffuse infiltration of carcinoma cells forming tubules, glands, and single cells. Occasional signet ring cells were seen. (Hematoxylin-eosin stain; original magnification: ×100.)
Previously reported dermatoscopic findings in cutaneous metastasis showed vascular patterns, of which serpentine, or linear, irregular vessels were the most common. The high prevalence of vascular structures in cutaneous metastasis supports the role of neovascularization in the pathogenesis of these skin lesions.2 Of note, the dermatoscopic features of hairpin vessels observed in our case have not been reported in previous studies. Similar to the case by AlSubait et al,1 the presence of shiny white lines in our case may represent the remodeling of new collagen in the dermis after neovascularization.
In summary, for patients with known malignancies, dermatoscopy can be a useful bedside tool to evaluate for new-onset cutaneous lesions. The presence of vascular structures as well as shiny white lines (or white structureless areas) can aid in the diagnosis of cutaneous metastasis.
Conflicts of interest
None disclosed.
Footnotes
Funding Sources: None.
IRB approval status: Not applicable.
Key words: cancer; cutaneous metasasis; dermoscopy; gastric cancer.
References
- 1.AlSubait N.A., BinJadeed H.F., AlSaleh M.R., AlFaifi F.S., AlSaif F.M., Arafah M.A. Dermoscopy of scalp cutaneous metastasis of sigmoid adenocarcinoma. JAAD Case Rep. 2021;14:116–119. doi: 10.1016/j.jdcr.2021.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chernoff K.A., Marghoob A.A., Lacouture M.E., Deng L., Busam K.J., Myskowski P.L. Dermoscopic findings in cutaneous metastases. JAMA Dermatol. 2014;150(4):429–433. doi: 10.1001/jamadermatol.2013.8502. [DOI] [PubMed] [Google Scholar]