

Abstract
Introduction
Alzheimer's disease (AD) represents a global health crisis. Treatments are needed to prevent, delay the onset, slow the progression, improve cognition, and reduce behavioral disturbances of AD. We review the current clinical trials and drugs in development for the treatment of AD.
Methods
We searched the governmental website clinicaltrials.gov where are all clinical trials conducted in the United States must be registered. We used artificial intelligence (AI) and machine learning (ML) approaches to ensure comprehensive detection and characterization of trials and drugs in development. We use the Common Alzheimer's Disease Research Ontology (CADRO) to classify drug targets and mechanisms of action of drugs in the pipeline.
Results
As of January 25, 2022 (index date for this study) there were 143 agents in 172 clinical trials for AD. The pipeline included 31 agents in 47 trials in Phase 3, 82 agents in 94 trials in Phase 2, and 30 agents in 31 trials in Phase 1. Disease‐modifying therapies represent 83.2% of the total number of agents in trials; symptomatic cognitive enhancing treatments represent 9.8% of agents in trials; and drugs for the treatment of neuropsychiatric symptoms comprise 6.9%. There is a diverse array of drug targets represented by agents in trials including nearly all CADRO categories. Thirty‐seven percent of the candidate agents in the pipeline are repurposed drugs approved for other indications. A total of 50,575 participants are needed to fulfill recruitment requirements for all currently active clinical trials.
Discussion
The AD drug development pipeline has agents representing a substantial array of treatment mechanisms and targets. Advances in drug design, outcome measures, use of biomarkers, and trial conduct promise to accelerate the delivery of new and better treatments for patients with AD.
Highlights
There are 143 drugs in the current Alzheimer's disease (AD) drug development pipeline.
Disease‐modifying therapies represent 83.2% of the candidate treatments.
Current trials require 50,575 participants who will donate 3,878,843 participant‐weeks to clinical trials.
The biopharmaceutical industry sponsors 50% of all clinical trials including 68% of Phase 3 trials.
Sixty‐three percent of Phase 3 trials and 46% of Phase 2 trials include non–North American clinical trial site locations indicating the global ecosystem required for AD drug development.
Keywords: aducanumab, Alzheimer's disease, amyloid, biomarkers, clinical trials, Common Alzheimer's Disease Research Ontology (CADRO), donanemab, drug development, inflammation, lecanemab, pharmaceutical companies, repurposed drugs, tau
1. INTRODUCTION
Alzheimer's disease (AD) is increasing as the size of the aged population grows. 1 In the United States there are currently 6.2 million individuals with AD dementia and the number will reach 12.7 million by 2050. In addition to those with AD in the dementia stages, there are ≈10 million individuals in the United States with mild cognitive impairment (MCI), half of whom (5 million) have MCI due to AD. The total number of persons in the United States with symptomatic forms of AD—MCI due to AD and AD dementia—is 11.2 million. 1 The estimated 2021 cost of caring for those with Alzheimer's disease and related dementias (ADRD) was $355 billion. The world‐wide prevalence of AD dementia will triple from its current 50 to 150 million by 2050 with most of those affected living in low‐ and middle‐income countries. 2
The need for therapy to prevent, delay the onset, slow the progression, and improve the symptoms of AD is compelled by the rising number of those with AD and the growing public health crisis posed by the disease. Advances in therapy are being achieved; aducanumab, the first disease‐modifying therapy (DMT) to be approved for AD, became available on the market for those with MCI due to AD and mild AD dementia in 2021. Aducanumab is an anti‐amyloid monoclonal antibody, and two more monoclonal antibodies (donanemab and lecanemab) are under review by the US Food and Drug Administration (FDA). 3 , 4 , 5 Additional new treatments for AD may become available in the foreseeable future.
We review the drugs in current clinical trials for AD. We present data from analyses of the clinicaltrials.gov registry, noting agents in Phase 1, 2, and 3; we describe their mechanism of action (MoA) and major trial characteristics. Our goal is to provide an update on agents being developed for AD and to present information on progress in the field of AD therapeutic development. The report follows the strategy developed in previous annual reviews of the AD pipeline. 6 , 7 , 8 , 9 , 10 , 11 The current report used more advanced analytic tools than previously applied including artificial intelligence (AI) and machine learning (ML) to automate our interrogation of clinicaltrials.gov.
2. METHODS
We used the US National Library of Medicine of the National Institutes of Health (NIH) clinical research registry, clinicaltrials.gov, as the source of information for this review. Beginning in 2007 the “Common Rule” governing clinicaltrials.gov required registration for studies that meet the definition of an “applicable clinical trial” (ACT). ACTs include controlled clinical investigations of any FDA‐regulated drugs, biological therapies, or devices for any disease or condition. 12 Review of studies of clinicaltrials.gov indicate that compliance with the common rule is high and most ACTs are registered appropriately. 13 , 14 The United States has more clinical trials than any other country, and clinicaltrials.gov includes most but not all therapies currently in clinical trials for AD globally. 10 A recent review showed that this registry includes far more trials than any other of the 18 registries reviewed. 15 Based on this information, the current review can be regarded as a comprehensive but not exhaustive analysis of clinical trials of therapies for AD.
RESEARCH IN CONTEXT
Systematic Review: We searched clinicaltrials.gov to identify all drugs currently being tested in Alzheimer's disease (AD) clinical trials. There are 143 agents being assessed in 172 trials. Most of the drugs being assessed are disease‐modifying agents addressing a wide variety of biological processes involved in AD. We used artificial intelligence (AI) and machine learning (ML) to enhance our registry search techniques.
Interpretation: AD drug development is progressing despite temporary slowing of clinical trial activity during the COVID pandemic. The first disease‐modifying therapy for AD (aducanumab) has been approved by the US Food and Drug Administration (FDA) and other disease‐modifying therapies are advancing in clinical trials. There is progress in clinical trial outcome measures, biomarkers indicative of drug efficacy and safety, and clinical trial designs that provide the foundation for development of new and better therapies for patients with AD.
Future Directions: Improved understanding of the biology of AD and better approaches to drug discovery are providing improved candidates for clinical trials. Biomarkers are now used to confirm the presence of AD‐type pathology in clinical trial participants. Biomarkers are playing a greater role as outcomes of disease‐modifying therapy trials and amyloid plaque lowering on a biomarker (amyloid positron emission tomography) was the basis for accelerated approval of aducanumab. Improvements in drug candidates and trial methodologies increase confidence in the future development of new therapies for AD.
The index date for this review is January 25, 2022, and the tables and text apply to the information available on that date. We include all trials of agents in Phases 1, 2, and 3. We collect information on the trial agent; trial title; trial number assigned on clinicaltrials.gov; start date; projected end date; actual end date, if completed or terminated; primary completion date; calculated trial duration; duration of treatment exposure; calculated recruitment period; number of subjects planned for enrollment; number of arms of the study (usually a placebo arm and one or more treatment arms with different doses); whether a biomarker was described as an entry criterion or an outcome; whether the agent was repurposed; subject characteristics (e.g., allowable Mini‐Mental State Examination [MMSE] range); and sponsorship (a biopharmaceutical company, NIH with academic medical centers, public–private partnership, or “other”). We included trials labeled as recruiting, active but not recruiting (e.g., trials that have completed recruitment and are continuing with the exposure portion of the trial), enrolling by invitation (e.g., open‐label extensions of trials), and not yet recruiting. We do not comment on trials listed as terminated, suspended, unknown, or withdrawn unless the specific reasons for their status were publicly revealed. We do not include trials of non‐pharmacologic therapeutic approaches such as cognitive‐behavior therapies, caregiver interventions, supplements, medical foods, or devices. We do not include trials of biomarkers; we note whether biomarkers were used in the trials for inclusion or as outcome measures. We include stem cell therapies among the interventions reviewed (they are not integrated into Figure 1).
FIGURE 1.

Agents in clinical trials for treatment of Alzheimer's disease in 2021 (from clinicaltrials.gov as of the index date of January 5, 2021). The inner ring shows Phase 3 agents; the middle ring comprises Phase 2 agents; the outer ring presents Phase 1 therapies; agents in green areas are biologics; agents in purple are disease‐modifying small molecules; agents in orange areas are symptomatic agents addressing cognitive enhancement or behavioral and neuropsychiatric symptoms; the shape of the icon shows the population of the trial; the icon color shows the Common Alzheimer's Disease Research Ontology (CADRO)‐based class of the agent (“Other” category includes CADRO classes that have three or fewer agents in trials). Agents underlined are new to the pipeline since 2020. (Figure © J Cummings; M de la Flor, PhD, Illustrator)
We use the National Institute on Aging and the Alzheimer's Association, International Alzheimer's and Related Dementias Research Portfolio (IADRP) approach to the MoA of agents in the pipeline (iadrp.nia.nih.gov). The IADRP catalogue of AD research is the Common Alzheimer's Disease Research Ontology (CADRO). The Translational Research and Clinical Interventions category of CADRO lists potential targets for AD and ADRD therapeutics from early therapeutic discovery through late‐stage preclinical development and all stages of clinical testing. These targets were used to classify the MoA of the agents in the pipeline. The targets include amyloid; tau; apolipoprotein E (APOE)/lipids, and lipoprotein receptors; neurotransmitter receptors; neurogenesis; inflammation; oxidative stress; cell death; proteostasis/proteinopathies; metabolism and bioenergetics; vasculature; growth factors and hormones; synaptic plasticity/neuroprotection; gut‐brain axis; circadian rhythm; epigenetic regulators; multi‐target; unknown target, and other. Some agents may have more than one MoA and, for these we reviewed the available literature to identify the putative predominant mechanism. “Symptomatic” was used for treatments whose purpose was cognitive enhancement or control of neuropsychiatric symptoms without claiming to impact the underlying biological causes of AD. “Disease‐modifying” was used for treatments intended to change the biology of AD and produce neuroprotection (often through a variety of intermediate mechanisms such as effects on amyloid or tau). 16 We used the features of the trials (e.g., clinical outcomes, trial duration, use of biomarkers, and number of participants) to determine whether a trial was attempting to demonstrate disease modification or symptomatic benefit. We recognize that these definitions are arbitrary, and many therapies may have symptomatic and disease‐modifying effects. We divided DMTs into biologics (e.g., monoclonal antibodies, vaccines, antisense oligonucleotides [ASOs], and gene therapy) and small molecules (drugs typically taken orally and < 500 Daltons in molecular weight). We note if the trials are prevention studies of asymptomatic individuals or treatment trials of participants with MCI due to AD or AD dementia. Prevention trials include participants with normal cognition and biological evidence of AD pathology; trials of participants with prodromal AD comprise individuals manifesting MCI who have biomarker evidence indicative of AD pathology; and trials of AD dementia include participants with mild, moderate, or severe dementia.
We used AI and ML to facilitate our analyses. AI strategies were used to assist reading text and ML techniques were used to extract information automatically. We used supervised natural language processing classification approaches to categorize text describing a drug's MoA into two categories: small molecules and DMTs. We used term frequency‐inverse document frequency (TF‐IDF) to generate the words’ matrix representation of the text and trained several ML models including XGBoost, random forest, logistic regression, decision tree, and support vector machine. The decision tree model achieved the highest accuracy (95%) in classifying the drugs’ MoA texts. 17 Human supervision verified the results and solved any unresolved identifications. In addition to ML models, we used multiple pattern extraction methods to extract information regarding biomarkers and other trials features from the trial's text description.
To generate the tables and data used in the pipeline, we designed a sentinel system to collect the needed data automatically from clinicaltrials.gov and store it in a relational database system. In this system, charts and graphs can be generated to provide insight into the data and illustrate trends. The sentinel system automatically updates daily to capture any changes posted on clinicaltrials.gov of any relevant trial as defined by our search parameters. The system generates an e‐mail notification as new data are identified and imported into the database.
3. RESULTS
3.1. Overview
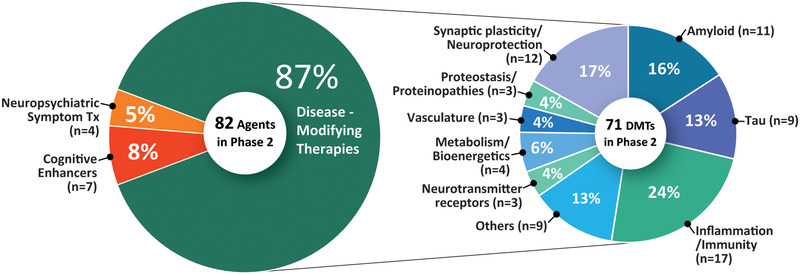
We identified 143 agents in 172 trials of treatments for AD (as of the index date of January 25, 2022). There were 31 agents in 47 Phase 3 trials; 82 agents in 94 Phase 2 trials; and 30 agents in 31 Phase 1 trials. Figure 1 shows all pharmacologic compounds (biologics and small molecules) currently in clinical trials for AD. The most common agents being studied are DMTs (119 agents; 83.2% of the total number of agents in trials); 24 (16.8%) are symptomatic agents including 14 (9.8% of all agents in trials) targeting cognitive enhancement and 10 (6.9% of all agents in trials) intending to treat neuropsychiatric and behavioral symptoms. Of the DMTs, 40 (33.6% of DMTs) are biologics and 79 (66.4% of DMTs) are small molecules. Twenty (16.8%) DMTs have amyloid, 13 (10.9%) have tau, 23 (19.3%) have inflammation, and 19 (16%) have synaptic plasticity/neuroprotection as their primary mechanistic targets. Considering DMTs only, 21 (67.8%) of Phase 3 agents are DMTs; 71 (86.6%) Phase 2 drugs are DMTs; and 27 (90%) Phase 1 agents are DMTs. There are 53 repurposed agents in the pipeline comprising 37.1% of the candidate therapies (all phases combined).
3.2. Phase 3
There are 31 agents in 47 Phase 3 trials (Figures 1 and 2, Table 1). Twenty‐one (67.8%) agents in Phase 3 trials are DMTs including five (16.1% of the Phase 3 agents) biologics and 16 (51.6%) small molecules. There are five (16.1% of Phase 3 agents) putative cognitive enhancing agents and five (16.1%) drugs targeting behavioral symptoms. CADRO mechanisms represented among Phase 3 DMTs include amyloid (6 agents; 28.6% of DMTs); synaptic plasticity/neuroprotection (4; 19%); oxidative stress (3; 14.3%); metabolism and bioenergetics (3; 14.3%); tau (1; 4.8%); inflammation (1; 4.8%); proteostasis/proteinopathies (1; 4.8%); vasculature (1; 4.8%); and gut‐brain axis (1; 4.8%). Figure 2 shows the CADRO‐based MOAs of agents in Phase 3. Thirteen (42%) of the Phase 3 agent are repurposed treatments approved for use in another indication (8 = DMT; 2 = cognitive enhancer; 3 = treatment for neuropsychiatric symptoms). In the past year (2021), four trials have been completed or terminated.
FIGURE 2.

Mechanisms of action of agents in Phase 3 (as classified using the Common Alzheimer's Disease Research Ontology [CADRO] approach) (Figure © J Cummings; M de la Flor, PhD, Illustrator)
TABLE 1.
Agents in Phase 3 of Alzheimer's disease drug development (clinicaltrials.gov accessed January 25, 2022)
| Agent | CADRO mechanism class | Mechanism of action | Therapeutic purpose | Status (CT.gov ID) | Sponsor | Start date | Estimated end date |
|---|---|---|---|---|---|---|---|
| Aducanumab | Amyloid | Monoclonal antibody directed at Aβ plaques and oligomers | DMT | Active, not recruiting (NCT04241068) | Biogen | Mar 2020 | Oct 2023 |
| AGB101 (low‐dose levetiracetam) | Synaptic Plasticity/Neuroprotection | SV2A modulator; to reduce Aβ‐induced neuronal hyperactivity | DMT | Active, not recruiting a (NCT03486938) | AgeneBio, NIA | Jan 2019 | Dec 2022 |
| Atuzaginstat (COR388) | Synaptic Plasticity/Neuroprotection | Bacterial protease inhibitor targeting gingipain produced by P. gingivalis to reduce neuroinflammation and hippocampal degeneration | DMT | Active, not recruiting a (NCT03823404) | Cortexyme | Mar 2019 | Dec 2022 |
| AVP‐786 | Neurotransmitter receptors | Sigma 1 receptor agonist; NMDA receptor antagonist | Neuropsychiatric symptoms agent (agitation) | Recruiting (NCT03393 520) | Avanir | Oct 2017 | Jul 2022 |
| Recruiting, extension study (NCT02446132) | Avanir | Dec 2015 | Oct 2023 | ||||
| Recruiting (NCT04464564) | Avanir | Sep 2020 | Dec 2024 | ||||
| Recruiting, extension study (NCT04408755) | Avanir | Jul 2020 | Dec 2024 | ||||
| AXS‐05 | Neurotransmitter receptors | NMDA receptor antagonist; combination of dextromethorphan and bupropion | Neuropsychiatric symptoms agent (agitation) | Recruiting (NCT04797715) | Axsome therapeutics | Dec 2020 | Dec 2022 |
| Recruiting, extension study (NCT04947553) | Axsome therapeutics | Jun 2021 | Jun 2023 | ||||
| Blarcamesine (ANAVEX2‐73) | Synaptic plasticity/neuroprotection | Sigma‐1 receptor agonist, M2 autoreceptor antagonist; to ameliorate oxidative stress, protein misfolding, mitochondrial dysfunction, and inflammation | DMT | Active, not recruiting a (NCT03790709) | Anavex life sciences | Jul 2018 | Jun 2022 |
| Recruiting a (NCT04314934) | Anavex life sciences | Oct 2019 | Jun 2024 | ||||
| BPDO‐1603 | Undisclosed | Undisclosed | Cognitive enhancer | Recruiting (NCT04229927) | Hyundai pharmaceutical | Feb 2020 | Mar 2023 |
| Brexpiprazole | Neurotransmitter receptors | Atypical antipsychotic; D2 receptor partial agonist; serotonin‐dopamine modulator | Neuropsychiatric symptoms agent (agitation) | Recruiting a (NCT03620981) | Otsuka | Aug 2018 | Aug 2022 |
| Recruiting, extension study (NCT03594123) | Otsuka | Oct 2018 | Jul 2022 | ||||
| Recruiting (NCT03548584) | Otsuka | May 2018 | Apr 2022 | ||||
| Caffeine | Neurotransmitter receptors | Adenosine antagonist; non‐specific phosphodiesterase inhibitor | Cognitive enhancer | Not yet recruiting (NCT04570085) | University Hospital, Lille | Nov 2021 | Nov 2024 |
| Donanemab | Amyloid | Monoclonal antibody specific for pyroglutamate form of Aβ | DMT | Active, not recruiting (NCT04437511) | Eli Lilly | Jun 2020 | Aug 2025 |
| Recruiting (NCT05026866) | Eli Lilly | Aug 2021 | Nov 2027 | ||||
| Donanemab & Aducanumab | Amyloid | Monoclonal antibody specific for pyroglutamate form of Aβ (donanemab); monoclonal antibody directed at plaques and oligomers (aducanumab); given in separate arms of the trial | DMT | Recruiting (NCT05108922) | Eli Lilly | Nov 2021 | Jun 2023 |
| Donepezil | Neurotransmitter receptors | Acetylcholinesterase inhibitor | Cognitive enhancer | Not yet recruiting (NCT04661280) | Assistance Publique – Hôpitaux de Paris | Jan 2022 | Jul 2024 |
| Escitalopram | Neurotransmitter receptors | Selective serotonin reuptake inhibitor | Neuropsychiatric symptoms agent (agitation) | Recruiting (NCT03108846) | Johns Hopkins University, NIA | Jan 2018 | Aug 2022 |
| Gantenerumab | Amyloid | Monoclonal antibody directed at Aβ plaques and oligomers | DMT | Recruiting (NCT03444870) | Roche | Jun 2018 | Oct 2026 |
| Active, not recruiting (NCT03443973) | Roche | Aug 2018 | Aug 2023 | ||||
| Active, not recruiting, extension study; (NCT04339413) | Roche | May 2020 | Apr 2023 | ||||
| Recruiting, extension study; (NCT04374253) | Roche | Feb 2021 | Dec 2024 | ||||
| Gantenerumab & Solanezumab | Amyloid | Monoclonal antibody directed at Aβ plaques and oligomers (gantenerumab); Monoclonal antibody directed at Aβ monomers (solanezumab); given in separate arms of the trial | DMT | Recruiting a ; (NCT01760005) | Washington University, Eli Lilly, Roche, NIA, Alzheimer's Association | Dec 2012 | Jul 2022 |
| Guanfacine | Neurotransmitter receptors | Alpha‐2 adrenergic agonist | Cognitive enhancer | Recruiting; (NCT03116126) | Imperial College London, UK National Institute of Health Research | Jan 2019 | Dec 2022 |
| GV‐971 | Gut‐brain axis | Algae‐derived acidic oligosaccharides; changes microbiome to reduce peripheral and central inflammation | DMT | Recruiting; (NCT04520412) | Shanghai Greenvalley | Oct 2020 | Oct 2026 |
| Hydralazine | Oxidative stress | Free radical scavenger | DMT | Recruiting; (NCT04842552) | Shahid Sadoughi University, Iran | Jun 2021 | Dec 2023 |
| Icosapent ethyl (IPE) | Oxidative stress | Purified form of the omega‐3 fatty acid EPA; to improve synaptic function and reduce inflammation | DMT | Active, not recruiting a ; (NCT02719327) | VA Office of Research and Development, University of Wisconsin, Madison | Jun 2017 | Jan 2023 |
| Lecanemab (BAN2401) | Amyloid | Monoclonal antibody directed at Aβ protofibrils | DMT | Active, not recruiting; (NCT03887455) | Eisai, Biogen | Mar 2019 | Aug 2024 |
| Recruiting; (NCT04468659) | Eisai, Biogen, ACTC, NIA | Jul 2020 | Oct 2027 | ||||
| Losartan & Amlodipine & Atorvastatin + exercise | Vasculature | Angiotensin II receptor blocker (losartan), calcium channel blocker (amlodipine), cholesterol agent (atorvastatin) | DMT | Active, not recruiting a ; (NCT02913664) | University of Texas Southwestern | Feb 2017 | Jan 2022 |
| Metformin | Metabolism and bioenergetics | Insulin sensitizer to improve CNS glucose metabolism | DMT | Recruiting a ; (NCT04098666) | Columbia University, NIA | Apr 2021 | Apr 2025 |
| Nabilone | Neurotransmitter receptors | Synthetic cannabinoid | Neuropsychiatric symptoms agent (agitation) | Recruiting (NCT04516057) | Sunnybrook Health Sciences Center, ADDF | Feb 2021 | Oct 2025 |
| NE3107 | Inflammation | MAPK‐1/3 inhibitor; reduces proinflammatory NFκB activation | DMT | Recruiting; (NCT04669028) | Neurmedix | Aug 2021 | Jan 2023 |
| Nilotinib BE | Proteostasis/Proteinopathies | Tyrosine kinase inhibitor; autophagy enhancer; promotes clearance of Aβ and tau | DMT | Not yet recruiting; (NCT05143528) | KeifeRx | Feb 2022 | Jun 2026 |
| Octohydro‐aminoacridine Succinate | Neurotransmitter receptors | Acetylcholinesterase inhibitor | Cognitive enhancer | Recruiting; (NCT03283059) | Shanghai Mental Health Center | Aug 2017 | Feb 2021 |
| Omega‐3 (DHA+EPA) | Oxidative stress | Antioxidant | DMT | Recruiting; (NCT03691519) | University Hospital, Toulouse | Apr 2018 | Dec 2023 |
| Semaglutide | Metabolism and bioenergetics | GLP‐1 agonist; reduces neuroinflammation and improves insulin signaling in the brain | DMT | Recruiting; (NCT04777396) | Novo Nordisk | May 2021 | Apr 2026 |
| Recruiting; (NCT04777409) | Novo Nordisk | May 2021 | Apr 2026 | ||||
| Simufilam (PTI‐125) | Synaptic Plasticity/Neuroprotection | Filamin A protein inhibitor; stabilizes amyloid‐alpha‐7 nicotinic receptor interaction | DMT | Recruiting; (NCT04994483) | Cassava sciences | Nov 2021 | Oct 2023 |
| Recruiting; (NCT05026177) | Cassava sciences | Dec 2021 | Jun 2024 | ||||
| Solanezumab | Amyloid | Monoclonal antibody directed at Aβ monomers | DMT | Active, not recruiting; (NCT02008357) | Eli Lilly, ATRI | Feb 2014 | Jun 2023 |
| Tricaprilin | Metabolism and bioenergetics | Caprylic triglyceride; induces ketosis and improves mitochondrial and neuronal function | DMT | Not yet recruiting; (NCT04187547) | Cerecin | Jun 2022 | Feb 2024 |
| TRx0237 | Tau | Tau protein aggregation inhibitor | DMT | Active, not recruiting; (NCT03446001) | TauRx Therapeutics | Jan 2018 | Mar 2023 |
| Valiltramiprosate (ALZ‐801) | Amyloid | Prodrug of tramiprosate; inhibits Aβ aggregation into toxic oligomers | DMT | Recruiting; (NCT04770220) | Alzheon, NIA | May 2021 | May 2024 |
NOTE. Thirty‐one agents in 47 Phase 3 clinical trials currently ongoing as of January 25, 2022 according to clinicaltrials.gov.
Abbreviations: Aβ, amyloid beta; ACTC, Alzheimer's Clinical Trial Consortium; ADDF, Alzheimer's Drug Discovery Foundation; ATRI, Alzheimer's Therapeutic Research Institute; BE, bioequivalent; CADRO, Common Alzheimer's Disease and Related Disorders Research Ontology; DMT, disease‐modifying therapy; EPA, eicosapentaenoic acid; GLP‐1, glucagon‐like peptide‐1; MAPK, mitogen activated protein kinase; NFκB, Nuclear Factor Kappa B; NIA, National Institute on Aging; NMDA, N‐methyl‐D‐aspartate; SV2A, synaptic vesicle protein 2A.
Phase 2/3 trials.
Six of the trials in Phase 3 are prevention trials enrolling cognitively normal participants known to be at risk for AD (preclinical AD); one trial enrolling both preclinical participants and participants with MCI to mild AD dementia (DIAN‐TU trial); 17 trials enrolling early AD defined as prodromal AD and mild AD dementia; 11 trials including participants with mild to moderate AD dementia; and 12 trials of participants with mild‐to‐severe AD dementia.
Trials in Phase 3 included a mean of 791 participants per trial (range 112 to 3300) and a total of 37,184 participants were needed for enrollment in all currently active Phase 3 trials. DMT prevention trials included a mean of 1058 participants (range 150 to 3300) and had a mean duration of 362 weeks (range 256 to 500 weeks, including the recruitment and the treatment period). DMT trials focusing on prodromal AD or prodromal AD/mild AD dementia had a mean of 991 participants (range 116 to 2032) and a mean duration of 243 weeks (range 83 to 500 weeks, including the recruitment and the treatment period). Trials of DMTs enrolling mild to moderate AD dementia participants included an average of 776 participants (range 316 to 2046) and a mean duration of 162 weeks (range 73 to 309 weeks, including the recruitment and the treatment period).
The mean treatment exposure period was 159 weeks (range 80 to 240 weeks) for prevention trials, 105 weeks (range 48 to 208 weeks) for prodromal AD or prodromal AD/mild AD dementia trials, and 48 weeks (range 20 to 76 weeks) for mild to moderate AD dementia trials. Calculated recruitment periods (calculated as the total projected time until the primary completion date minus the treatment period) for DMT trials were: prevention (183 weeks), prodromal AD and prodromal AD/mild AD dementia (93 weeks), and mild to moderate AD dementia (91 weeks).
The mean duration of cognitive enhancer trials was 167 weeks (range 130 to 208 weeks) including 24 treatment weeks (range 12 to 30 weeks), and they intended to recruit an average of 392 participants (range 160 to 712). The mean duration of trials of treatments for neuropsychiatric symptoms was 218 weeks (range 100 to 408 weeks) including 18 treatment weeks (range 8 to 52 weeks), and they included an average of 478 participants (range 112 to 1200).
3.3. Phase 2
There are 82 agents in 94 Phase 2 trials (Figures 1 and 3, Table 2). Seventy‐one (86.6%) of the agents in Phase 2 trials are DMTs including 26 (31.7% of the Phase 2 agents) biologics and 45 (54.8%) small molecules. There are seven (8.5% of Phase 2 agents) putative cognitive enhancing agents and four (4.9%) drugs targeting behavioral symptoms. CADRO mechanisms represented among Phase 2 DMT therapies include inflammation (17 agents; 24% of DMTs); synaptic plasticity/neuroprotection (12; 16.9%); amyloid (11; 15.5%); tau (9; 12.7%); metabolism and bioenergetics (4; 5.6%); neurotransmitter receptors (3; 4.2%); proteostasis/proteinopathies (3; 4.2%); vasculature (3; 4.2%); neurogenesis (2; 2.8%); growth factors and hormones (2; 2.8%); epigenetic regulators (2; 2.8%); ApoE, lipids, and lipoprotein receptors (1; 1.4%); oxidative stress (1; 1.4%); and cell death (1; 1.4%). Figure 3 shows the CADRO‐based MoAs of agents in Phase 2. Thirty‐one (37.8%) of the Phase 2 agents are repurposed from another indication (27 = DMT; 1 = cognitive enhancer; 3 = treatment for neuropsychiatric symptoms). In the past year (2021), 23 Phase 2 trials have been completed or terminated.
FIGURE 3.
Mechanisms of action of agents in Phase 2 (Figure © J Cummings; M de la Flor, PhD, Illustrator)
TABLE 2.
Agents in Phase 2 of Alzheimer's disease drug development (clinicaltrials.gov accessed January 25, 2022)
| Agent | CADRO mechanism class | Mechanism of action | Therapeutic purpose | Status (CT.gov ID) | Sponsor | Start date | Estimated end date |
|---|---|---|---|---|---|---|---|
| ABvac40 | Amyloid | Active immunotherapy to remove Aβ | DMT | Active, not recruiting; (NCT03461276) | Araclon Biotech | Feb 2018 | Dec 2022 |
| ACI‐35 | Tau | Active immunotherapy targeting tau | DMT | Recruiting a ; (NCT04445831) | AC Immune, Janssen | Jul 2019 | Oct 2023 |
| AD‐35 | Neurotransmitter receptors | Acetylcholinesterase inhibitor | Cognitive enhancer | Active, not recruiting; (NCT03625401) | Zhejiang Hisun Pharmaceutical | Oct 2018 | Dec 2020 |
| AL002 | Inflammation | Monoclonal antibody targeting TREM2 receptors to promote microglial clearance of Aβ | DMT | Recruiting; (NCT04592874) | Alector, AbbVie | Jan 2021 | Aug 2023 |
| Allopregnanolone | Neurogenesis | Allosteric modulator of GABA‐A receptors | DMT | Not yet recruiting; (NCT04838301) | University of Arizona, NIA | Nov 2021 | Jun 2024 |
| APH‐1105 | Amyloid | Alpha‐secretase modulator to reduce Aβ production | DMT | Not yet recruiting; (NCT03806478) | Aphios | Jun 2023 | Dec 2024 |
| Baricitinib | Inflammation | Janus kinase inhibitor; reduces neuroinflammation | DMT | Not yet recruiting a ; (NCT05189106) | Massachusetts General Hospital | Feb 2022 | Oct 2023 |
| Bepranemab | Tau | Anti‐tau monoclonal antibody | DMT | Recruiting; (NCT04867616) | UCB Biopharma | Jun 2021 | Nov 2025 |
| BCG vaccine | Inflammation/Immunity | Immunomodulator | DMT | Not yet recruiting; (NCT05004688) | Massachusetts General Hospital | Dec 2021 | Oct 2023 |
| BPN14770 | Synaptic plasticity/neuroprotection | PDE‐4 inhibitor; prolongs cAMP activity and improves neuronal plasticity | DMT | Active, not recruiting; (NCT03817684) | Tetra discovery partners | Apr 2019 | Feb 2020 |
| Bromocriptine | Neurotransmitter receptors | Dopamine agonist with anti‐Aβ effects | DMT | Active, not recruiting a ; (NCT04413344) | Kyoto University | Jun 2020 | Mar 2022 |
| Bryostatin 1 | Synaptic plasticity/neuroprotection | Protein Kinase C inhibitor; facilitates synaptogenesis | DMT | Recruiting; (NCT04538066) | Neurotrope Bioscience, NIH, NIA | Aug 2020 | Nov 2022 |
| BXCL‐501 | Neurotransmitter receptors | Sublingual dexmedetomidine; selective α2‐adrenergic receptor agonist | Neuropsychiatric symptoms agent (agitation) | Recruiting; (NCT04251910) | BioXcel therapeutics | Dec 2020 | Sep 2021 |
| Canakinumab | Inflammation | Anti‐IL‐1β monoclonal antibody | DMT | Recruiting; (NCT04795466) | Novartis | Oct 2021 | Jan 2024 |
| CORT108297 | Hormones | Selective glucocorticoid receptor antagonist; reduce neuroendocrine stress responses | Cognitive enhancer | Recruiting; (NCT04601038) | Johns Hopkins University | Jun 2021 | Jan 2024 |
| Crenezumab | Amyloid | Monoclonal antibody targeting soluble Aβ oligomers | DMT | Active, not recruiting; (NCT01998841) | Genentech, NIA Banner Alzheimer's Institute | Dec 2013 | Dec 2022 |
| CST‐2032 | Neurotransmitter receptors | Noradrenergic agonist | Cognitive enhancer | Not yet recruiting; (NCT05104463) | CuraSen Therapeutics | Jan 2022 | Oct 2022 |
| Curcumin + aerobic yoga | Inflammation | Herb with antioxidant and anti‐inflammatory properties | DMT | Active, not recruiting; (NCT01811381) | VA Office of Research and Development | Jan 2014 | Dec 2020 |
| CY6463 | Synaptic Plasticity/Neuroprotection | Guanylate cyclase positive allosteric modulator | DMT | Recruiting; (NCT04798989) | Cyclerion therapeutics | Jun 2021 | Jul 2022 |
| DAOIB | Neurotransmitter receptors | NMDA receptor antagonist to augment the effect of tDCS | Cognitive enhancer | NCT05006781 | Chang Gung Memorial Hospital | Mar 2022 | Aug 2025 |
| Dapagliflozin | Metabolism and bioenergetics | SGLT2 inhibitor; to improve insulin sensitivity and CNS glucose metabolism | DMT | Recruiting a ; (NCT03801642) | University of Kansas | Jan 2019 | Oct 2022 |
| Daratumumab | Inflammation/immunity | Monoclonal antibody targeting CD38; regulates microglial activity | DMT | Recruiting; (NCT04070378) | Northwell Health, Janssen | Nov 2019 | Jun 2023 |
| Dasatinib + Quercetin | Inflammation/immunity | Tyrosine kinase inhibitor (dasatinib) and flavonoid (quercetin); senolytic therapy approach to reduce senescent cells and tau aggregation | DMT | Recruiting a ; (NCT04063124) | The University of Texas at San Antonio, Mayo Clinic | Feb 2020 | Aug 2023 |
| Recruiting; (NCT04685590) | Wake Forest University, The University of Texas at San Antonio | Jan 2022 | Jan 2032 | ||||
| Recruiting a ; (NCT04785300) | Mayo Clinic | Oct 2021 | Jun 2023 | ||||
| Deferiprone | Cell death | Iron chelating agent; reduce damaging reactive oxygen species | DMT | Active, not recruiting; (NCT03234686) | Neuroscience Trials Australia | Jan 2018 | Sep 2023 |
| DHA | Oxidative stress | Omega 3 fatty acid; improve synaptic function; antioxidant | DMT | Recruiting; (NCT03613844) | University of Southern California, NIA, ADDF | Jul 2018 | Dec 2024 |
| Donanemab (LY3002813) | Amyloid | Monoclonal antibody specific for pyroglutamate Aβ | DMT | Active, not recruiting; (NCT03367403) | Eli Lilly | Dec 2017 | Nov 2021 |
| Recruiting; (NCT04640077) | Eli Lilly | Nov 2020 | Oct 2023 | ||||
| Dronabinol | Neurotransmitter receptors | CB1 and CB2 endocannabinoid receptor partial agonist | Neuropsychiatric symptoms agent (agitation) | Recruiting; (NCT02792257) | Mclean Hospital, Johns Hopkins University | Mar 2017 | May 2023 |
| E2814 | Tau | Anti‐tau monoclonal antibody | DMT | Recruiting a ; (NCT04971733) | Eisai | Jun 2021 | Apr 2024 |
| Edonerpic (T‐817MA) | Synaptic plasticity/neuroprotection | Neurotrophic agent; activates sigma receptors to preserve synaptic plasticity; protect against Aβ toxicity | DMT | Active, not recruiting; (NCT04191486) | Toyama Chemical | Dec 2019 | Mar 2023 |
| Elayta (CT1812) | Synaptic plasticity/neuroprotection | Sigma‐2 receptor antagonist; competes with oligomeric Aβ binding; protect against Aβ‐induced synaptic toxicity | DMT | Recruiting; (NCT03507790) | Cognition therapeutics | Oct 2018 | Oct 2023 |
| Recruiting; (NCT04735536) | Cognition therapeutics | Jul 2020 | Jul 2022 | ||||
| ExPlas (exercised plasma) | Synaptic plasticity/neuroprotection | Plasma transfusion from exercise‐trained donors | DMT | Recruiting; (NCT05068830) | Norwegian University, St. Olavs Hospital | Sep 2021 | Sep 2025 |
| Fosgonimeton (ATH‐1017) | Synaptic plasticity/neuroprotection | Activates signaling via the hepatocyte growth factor system to regenerate neurons and enhance synaptic plasticity | DMT | Recruiting; (NCT04488419) | Athira Pharma | Sep 2020 | Oct 2022 |
| Active, not recruiting; (NCT04491006) | Athira Pharma | Nov 2020 | May 2022 | ||||
| Recruiting, extension study; (NCT04886063) | Athira Pharma | Jun 2021 | May 2023 | ||||
| Gantenerumab | Amyloid | Monoclonal antibody directed at Aβ plaques and oligomers | DMT | Active, not recruiting; (NCT04592341) | Roche | Nov 2020 | Nov 2023 |
| Brain Shuttle Gantenerumab (RO7126209) | Amyloid | Anti‐Aβ monoclonal antibody (gantenerumab) with enhanced blood‐brain barrier penetration | DMT | Recruiting a ; (NCT04639050) | Roche | Mar 2021 | Oct 2024 |
| GB301 | Inflammation/immunity | Regulatory T cells; reduce neuroinflammation | DMT | Not yet recruiting a ; (NCT03865017) | GMP BIO, BHT Lifescience Australia | Dec 2019 | Dec 2021 |
| Grapeseed extract | Proteostasis/proteinopathies | Polyphenolic compound; antioxidant; prevent aggregation of Aβ and tau | DMT | Active, not recruiting; (NCT02033941) | Mount Sinai School of Medicine, NCCIH | Nov 2014 | Dec 2021 |
| GV1001 | Epigenetic | hTERT peptide vaccine; mimics extra‐telomeric functions to inhibit neurotoxicity, apoptosis, and reactive oxygen species | DMT | Not yet recruiting; (NCT03959553) | GemVax & Kael | Sep 2019 | Feb 2022 |
| Not yet recruiting; (NCT05189210) | GemVax & Kael | May 2022 | Sep 2024 | ||||
| Intranasal insulin | Metabolism and bioenergetics | Decrease glucose resistance and increase insulin signaling in the brain | DMT | Not yet recruiting; (NCT05006599) | Wake Forest University | Oct 2021 | Oct 2025 |
| Intranasal insulin + Empagliflozin | Metabolism and bioenergetics | SGLT2 inhibitor (empagliflozin) and insulin combination therapy; decrease glucose resistance and increase insulin signaling in the brain | DMT | Not yet recruiting; (NCT05081219) | Wake Forest University | Nov 2021 | Nov 2028 |
| IONIS MAPTRx (BIIB080) | Tau | Antisense oligonucleotide targeting tau expression; MAPT RNA inhibitor | DMT | Active, not recruiting a ; (NCT03186989) | Ionis Pharmaceuticals | Jun 2017 | May 2022 |
| JNJ‐63733657 | Tau | Monoclonal antibody targeting soluble tau | DMT | Recruiting; (NCT04619420) | Janssen | Jan 2021 | Nov 2025 |
| Lamivudine (3TC) | Epigenetic | Nucleoside reverse transcriptase inhibitor; reduces genetic rearrangements | DMT | Recruiting a ; (NCT04552795) | University of Texas Health Science Center at San Antonio | Feb 2021 | Jun 2022 |
| Lecanemab (BAN2401) | Amyloid | Monoclonal antibody directed at protofibrils | DMT | Active, not recruiting; (NCT01767311) | Eisai | Dec 2012 | Feb 2025 |
| Lenalidomide | Inflammation/immunity | Reduce inflammatory cytokines; modulate innate and adaptive immune responses | DMT | Recruiting; (NCT04032626) | Cleveland Clinic, NIA | Jul 2020 | Sep 2024 |
| Levetiracetam | Synaptic plasticity/neuroprotection | SV2A modulator; improve synaptic function; reduce Aβ‐induced neuronal hyperactivity | DMT | Active, not recruiting; (NCT02002819) | University of California, San Francisco | Jun 2014 | Dec 2021 |
| Active, not recruiting; (NCT03489044) | UCB Pharma, University of Oxford, NHS Foundation Trust | Oct 2018 | Dec 2022 | ||||
| Recruiting; (NCT03875638) | Beth Israel Deaconess Medical Center | Aug 2019 | Nov 2023 | ||||
| L‐Serine | Inflammation | Dietary amino acid; reduce brain inflammation and preserve nerve cells | DMT | Active, not recruiting; (NCT03062449) | Dartmouth‐Hitchcock Medical Center | Mar 2017 | Dec 2022 |
| Lupron (leuprolide acetate depot) | Growth factors and hormones | GnRH receptor agonist; reduce effects of elevated GnRH and gonadotropins on the brain | DMT | Recruiting; (NCT03649724) | New York University | Nov 2020 | Feb 2026 |
| LY3372689 | Tau | O‐GlycNAcase inhibitor; promote tau glycosylation, prevent tau aggregation | DMT | Recruiting; (NCT05063539) | Eli Lilly | Sep 2021 | Jun 2024 |
| Memantine | Neurotransmitter receptors | NMDA receptor antagonist | DMT | Recruiting; (NCT05063851) | University of Virginia | Oct 2021 | Oct 2024 |
| Metabolic cofactor supplementation | Metabolism and bioenergetics | Mixture of N‐acetylcysteine, L‐carnitine tartrate, nicotinamide roboside, and serine to increase mitochondrial activity | Cognitive enhancer | Recruiting; (NCT04044131) | Istanbul Medipol University Hospital, ScandiBio therapeutics | Dec 2019 | Sep 2020 |
| MIB‐626 | Amyloid | Sirtuin‐nicotinamide adenine dinucleotide stimulator to enhance alpha‐secretase | DMT | Not yet recruiting a ; (NCT05040321) | Brigham and Women's Hospital | Dec 2021 | Dec 2024 |
| Montelukast | Inflammation | Cysteinyl leukotriene type 1 (cysLT‐1) receptor antagonist; effects on inflammatory processes, neuronal injury, blood‐brain‐barrier integrity, and Aβ protein accumulation | DMT | Recruiting; (NCT03402503) –buccal film | IntelGenx Corp. | Nov 2018 | Jul 2021 |
| Active, not recruiting; (NCT03991988) – tablet | Emory University | Sep 2019 | Oct 2022 | ||||
| MW150 | Synaptic plasticity/neuroprotection | p38 MAPK‐α inhibitor | DMT | Not yet recruiting; (NCT05194163) | Neurokine Therapeutics, Columbia University, NIA | Feb 2022 | Jan 2025 |
| Neflamapimod (VX‐745) | Synaptic plasticity/neuroprotection | p38 MAPK‐α inhibitor; enhance endolysosomal function to reduce synaptic dysfunction | DMT | Recruiting; (NCT03435861) | EIP Pharma | Oct 2018 | Jun 2021 |
| Nicotinamide | Tau | HDAC inhibitor; to reduce tau‐induced microtubule depolymerization and tau phosphorylation | DMT | Recruiting; (NCT03061474) | University of California, Irvine | Jul 2017 | Jul 2022 |
| Nicotine transdermal patch | Neurotransmitter receptors | Nicotinic acetylcholine receptor agonist | Cognitive enhancer | Recruiting; (NCT02720445) | University of Southern California, NIA, ATRI, Vanderbilt University | Jan 2017 | Jul 2023 |
| Obicetrapib | Lipids and lipoprotein receptors | Cholesteryl ester transfer protein (CETP) inhibitor | DMT | Not yet recruitin; (NCT05161715) | NewAmsterdam Pharma | Dec 2021 | Mar 2023 |
| Omega‐3 PUFA | Vasculature | Polyunsaturated fatty acid; reduce damage to small blood vessels | DMT | Active, not recruiting; (NCT01953705) | Oregon Health and Science University, NIA | May 2014 | Jun 2021 |
| Pepinemab (VX15) | Inflammation | Monoclonal antibody directed at semaphorin 4D to reduce inflammation | DMT | Recruiting a ; (NCT04381468) | Vaccinex, ADDF, Alzheimer's Association | Jul 2021 | Jan 2023 |
| Posiphen | Proteostasis/proteinopathies | Inhibitor of APP and α‐synuclein | DMT | Active, not recruiting a ; (NCT02925650) | QR Pharma, ADCS | Mar 2017 | Feb 2022 |
| Active, not recruiting a ; (NCT04524351) | Annovis Bio, Parexel | Aug 2020 | Mar 2022 | ||||
| Prazosin | Neurotransmitter receptors | Alpha‐1 adrenoreceptor antagonist | Neuropsychiatric symptoms agent (agitation) | Active, not recruiting; (NCT03710642) | ADCS, NIA | Oct 2018 | Feb 2022 |
| PU‐AD | Tau | Heat shock protein 90 inhibitor; to prevent aggregation and hyperphosphorylation of tau | DMT | Active, not recruiting; (NCT04311515) | Samus therapeutics | Jun 2020 | Dec 2022 |
| Rapamycin (sirolimus) | Proteostasis/proteinopathies | mTOR inhibitor; ameliorate metabolic and vascular effects of aging | DMT | Recruiting; (NCT04629495) | The University of Texas Health Science Center at San Antonio | Aug 2021 | Aug 2024 |
| Sargramostim | Inflammation/immunity | Granulocyte macrophage colony stimulating factor | DMT | Not yet recruiting; (NCT04902703) | University of Colorado, NIA, Alzheimer's association, partner therapeutics | Dec 2021 | Jul 2024 |
| Semorinemab (RO7105705) | Tau | Monoclonal antibody to remove extracellular tau | DMT | Active, not recruiting; (NCT03828747) | Genentech | Jan 2019 | Jun 2023 |
| Senicapoc | Inflammation | Calcium‐activated potassium channel blocker | DMT | Not yet recruiting; (NCT04804241) | University of California, Davis | Jan 2022 | Jun 2023 |
| Sovateltide (PMZ‐1620) | Neurogenesis | Endothelin B receptor agonist; augments activity of neuronal progenitor cells | DMT | Recruiting; (NCT04052737) | Pharmazz | Mar 2018 | Oct 2022 |
| Simufilam (PTI‐125) | Synaptic plasticity/neuroprotection | Filamin A protein inhibitor; stabilizes the interaction of soluble Aβ and the alpha7 nicotinic acetylcholine receptor, reducing Aβ and synaptic dysfunction | DMT | Active, not recruiting; (NCT04388254) | Cassava Sciences, NIA | Mar 2020 | Jul 2023 |
| Suvorexant | Neurotransmitter receptors | Dual Orexin receptor antagonist; improved sleep with effects on CSF Aβ | DMT | Not yet recruiting; (NCT04629547) | Washington University School of Medicine | Nov 2021 | Jan 2025 |
| T3D‐959 | Metabolism and bioenergetics | Dual agonist of PPARδ/γ; reduce glucose and lipid metabolism | DMT | Recruiting; (NCT04251182) | T3D Therapeutics, Alzheimer's Association, NIA | Mar 2021 | Jul 2022 |
| TB006 | Inflammation | Monoclonal antibody targeting galactin 3 | DMT | Recruiting a ; (NCT05074498) | TrueBinding, Inc. | Oct 2021 | Oct 2022 |
| Telmisartan & perindopril | Vasculature | Angiotensin II receptor blocker (telmisartan); angiotensin converting enzyme inhibitor (perindopril) | DMT | Recruiting; (NCT02085265) | Sunnybrook Health Sciences Centre, ADDF | Mar 2014 | Mar 2022 |
| Tdap vaccine | Inflammation and immunity | Immune reaction to diphtheria, pertussis, tetanus vaccine | DMT | Not yet recruiting a ; (NCT05183516) | Mindful diagnostics and therapeutics | May 2022 | Mar 2023 |
| THC‐free CBD oil | Neurotransmitter receptors | Cannabinoid with effects on cannabinoid receptors | Neuropsychiatric symptoms agent (agitation) | Recruiting; (NCT04436081) | Eastern Virginia Medical School, Ananda Hemp | Feb 2021 | Jun 2022 |
| Thiethylperazine (TEP) | Amyloid | Activates transport protein ABCC1 to remove Aβ | DMT | Active, not recruiting; (NCT03417986) | Immungenetics AG | Nov 2017 | Dec 2021 |
| Troriluzole (BHV4157) | Synaptic plasticity/neuroprotection | Glutamate modulator; prodrug of riluzole; improve synaptic function | DMT | Active, not recruiting; (NCT03605667) | Biohaven Pharma, ADCS | Jul 2018 | Jan 2022 |
| Valacyclovir | Infection/immunity | Antiviral against HSV‐1 and ‐2 infection; to prevent Aβ aggregation and plaque deposition | DMT | Recruiting; (NCT03282916) | New York State Psychiatric Institute, NIH, NIA | Feb 2018 | Dec 2023 |
| Valiltramiprosate (ALZ‐801) | Amyloid | Prodrug of tramiprosate; inhibits Aβ aggregation into toxic oligomers | DMT | Active, note recruiting; (NCT04693520) | Alzheon | Sep 2020 | Aug 2023 |
| Varoglutamstat (PQ912) | Amyloid | Glutaminyl cyclase (QC) enzyme inhibitor to reduce pyroglutamate Aβ production | DMT | Recruiting; (NCT03919162) | Vivoryon Therapeutics AG, ADCS, NIA | Nov 2021 | May 2023 |
| Recruiting; (NCT04498650) | Vivoryon Therapeutics AG, ADCS, NIA | Jul 2020 | Jul 2023 | ||||
| VGH‐AD1 | Undisclosed | Traditional Chinese herbal medicine | Cognitive enhancer | Not yet recruiting; (NCT04249869) a | Taipei Veterans General Hospital, Taiwan | Feb 2020 | Dec 2020 |
| Xanamem | Growth factors and hormones | 11‐beta‐hydroxysteroid dehydrogenase type 1 inhibitor | DMT | Active, not recruiting a (NCT04983368) | Actinogen Medical | Jun 2021 | Jun 2022 |
| Yangxue Qingnao pills | Vasculature | Cerebral blood flow enhancer | DMT | Recruiting(NCT04780399) | Dongzhimen Hospital, Beijing | Nov 2021 | Dec 2024 |
NOTE. Eighty‐two agents in 94 Phase 2 clinical trials currently ongoing as of January 25, 2022 according to clinicaltrials.gov.
Abbreviations: Aβ, amyloid beta; ADCS, Alzheimer's Disease Cooperative Study; ADDF, Alzheimer's Drug Discovery Foundation; APP, amyloid precursor protein; CADRO, Common Alzheimer's Disease and Related Disorders Research Ontology; cAMP, cycling adenosine monophosphate; CB, cannabinoid; DMT, disease‐modifying therapy; GnRH, gonadotropin‐releasing hormone; HSV, herpes simplex virus; hTERT, human telomerase reverse transcriptase; MAPK, mitogen‐activated protein kinase; mTOR, mammalian target of rapamycin; NCCIH, National Center for Complementary and Integrative Health; NIA, National Institute on Aging; NMDA, N‐methyl‐D‐aspartate; PDE, phosphodiesterase; PPARδ/γ, peroxisome proliferator nuclear receptor δ/γ; PUFA, polyunsaturated fatty acids; SGLT2, sodium glucose transporter 2; SV2A, synaptic vesicle protein 2A; tDCS, transcranial direct current stimulation; TREM2, Triggering Receptor Expressed On Myeloid Cells 2.
Phase 1/2 trials.
There are five trials in Phase 2 involving cell therapies (Table 3).
TABLE 3.
Agents in Phase 1 of Alzheimer's disease drug development (clinicaltrials.gov accessed January 25, 2022)
| Agent | CADRO mechanism class | Mechanism of action | Therapeutic purpose | Status (CT.gov ID) | Sponsor | Start date | Estimated end date |
|---|---|---|---|---|---|---|---|
| AAV‐Htert | Epigenetic | Extending telomeres may benefit AD; reduce Aβ‐induced neurotoxicity; effects on multiple cellular pathways | DMT | Recruiting; (NCT04133454) | Libella Gene Therapeutics | Oct 2019 | Jan 2021 |
| ACU193 | Amyloid | Monoclonal antibody targeting soluble Aβ | DMT | Recruiting; (NCT04931459) | Acumen Pharmaceuticals, NIA | Jun 2021 | Dec 2022 |
| Allopregnanolone | Neurogenesis | GABA‐A receptor modulator; promote neurogenesis and reduce inflammation | DMT | Active, not recruiting; (NCT03748303) | University of Southern California, University of Arizona, Alzheimer's Association | Oct 2019 | Oct 2022 |
| ASN51 | Tau | O‐GlycNAcase Inhibitor | DMT | Recruiting; (NCT04759365) | Asceneuron | Jun 2021 | Jan 2022 |
| BEY2153 | Proteostasis/proteinopathies | Aβ and tau aggregation inhibitor; inhibits neuronal death | DMT | Recruiting; (NCT04476303) | BeyondBio | Aug 2020 | Oct 2021 |
| BMS‐984923 | Synaptic plasticity/neuroprotection | mGluR5 allosteric modulator | DMT | Recruiting; (NCT04805983) | Yale University, NIA | Mar 2021 | Oct 2021 |
| BDPP (bioactive dietary polyphenol preparation) | Proteostasis/proteinopathies | Prevents Aβ and tau aggregation | DMT | Recruiting; (NCT02502253) | Johns Hopkins University, Mount Sinai School of Medicine | Jun 2015 | Jun 2022 |
| Contraloid acetate | Proteostasis/proteinopathies | Aggregation inhibitor | DMT | Recruiting; (NCT04711486) | Charite University, Berlin, Germany | Dec 2020 | Nov 2021 |
| COR588 | Synaptic plasticity/neuroprotection | Lysine‐gingipain inhibitor | DMT | Recruiting; (NCT04920903) | Cortexyme | Aug 2021 | May 2022 |
| Dabigatran | Vasculature | Direct thrombin inhibitor; reduce neurovascular damage | DMT | Not yet recruiting; (NCT03752294) | University of Rhode Island, ADDF, Boehringer Ingelheim | Nov 2018 | Dec 2021 |
| Donepezil | Neurotransmitter receptors | Cholinesterase inhibitor | Cognitive enhancer | Recruiting; (NCT04730635) | Merck | Mar 2021 | Aug 2022 |
| Edicotinib (JNJ‐40346527) | Inflammation | CSF‐1R antagonist; attenuates microglial proliferation and neurodegeneration | DMT | Not yet recruiting; (NCT04121208) | Janssen, University of Oxford | Nov 2020 | Dec 2021 |
| Efavirenz | Epigenetics | NNRTI; promote cholesterol removal; enhance amyloid reduction. | DMT | Active, not recruiting; (NCT03706885) | Case Western Reserve University, Cleveland Medical Center, Massachusetts General Hospital | May 2018 | Dec 2022 |
| Emtricitabine | Inflammation | NRTI; reduce neuroinflammation | DMT | Recruiting; (NCT04500847) | Butler Hospital, Alzheimer's Association, Brown University | Dec 2021 | Aug 2023 |
| IGC AD1 | Neurotransmitter receptors | Tetrahydrocannabinol that binds to the CB1 receptor | Neuropsychiatric symptoms agent (agitation) | Recruiting; (NCT04749563) | IGC Pharma | Jan 2021 | Jul 2021 |
| Lu AF87908 | Tau | Monoclonal antibody to reduce tau | DMT | Recruiting; (NCT04149860) | Lundbeck | Sep 2019 | Jul 2022 |
| LX1001 | Epigenetic | 10hAPOE2, serotype rh. Ten AAV gene transfer vector expressing the cDNA coding for human APOE ε2, directly to the CNS/CSF of APOE ε4 homozygotes with AD | DMT | Recruiting; (NCT03634007) | Cornell University | Nov 2019 | Jan 2024 |
| LY3372993 | Amyloid | Monoclonal antibody to reduce Aβ | DMT | Recruiting; (NCT04451408) | Eli Lilly | Jul 2020 | Sep 2023 |
| MK‐1942 + donepezil | Neurotransmitter receptors | Undisclosed (MK‐1942) | Cognitive enhancer | Recruiting; (NCT04308304) | Merck | Feb 2021 | May 2022 |
| NNI‐362 | Neurogenesis | Enhance neurogenesis; activates progenitor cells | DMT | Recruiting; (NCT04074837) | Neuronascent, NIA | Aug 2019 | Dec 2020 |
| REM0046127 | Synaptic Plasticity/Neuroprotection | Regulates calcium dyshomeostasis; tau and Aβ reduction | DMT | Recruiting; (NCT04672135) | reMYND, NeuroScios GmbH | Nov 2020 | May 2022 |
| Salsalate | Inflammation | Non‐steroidal anti‐inflammatory to reduce inflammation | DMT | Active, not recruiting; (NCT03277573) | University of California, San Francisco | Jul 2017 | Dec 2021 |
| SHR‐1707 | Amyloid | Anti‐amyloid monoclonal antibody | DMT | Recruiting; (NCT04973189) | Shanghai Hengrui Pharmaceutical | May 2021 | Nov 2021 |
| Recruiting; (NCT04745104) | Atridia Pty Ltd. | Feb 2021 | May 2022 | ||||
| TB006 | Tau | Anti‐tau monoclonal antibody | DMT | Recruiting; (NCT04920786) | TrueBinding, Inc. | Jun 2021 | Jan 2023 |
| Telmisartan | Vasculature | Angiotensin II receptor blocker | DMT | Recruiting; (NCT02471833) | Emory University | Apr 2015 | Feb 2022 |
| Trehalose | Cell death | Induces autophagy and promotes clearance of aggregated proteins | DMT | Recruiting; (NCT04663854) | Mashhad University of Medical Sciences | Aug 2020 | Aug 2022 |
| Tricaprilin (AC‐1202) | Metabolism and bioenergetics | Caprylic triglyceride | DMT | Recruiting; (NCT05028114) | Cerecin | Aug 2021 | Dec 2022 |
| Vorinostat | Epigenetics | Histone deacetylase (HDAC) inhibitor; enhanced synaptic plasticity | DMT | Recruiting; (NCT03056495) | German Center for Neurodegenerative Diseases, University Hospital, Bonn, University of Gottingen | Sep 2017 | Mar 2022 |
| VT301 | Inflammation | Regulatory T cells | DMT | Recruiting; (NCT05016427) | VTBIO Co. | Nov 2020 | Apr 2022 |
| XPro1595 | Inflammation | TNF inhibitor; reduce neuroinflammation | DMT | Recruiting; (NCT03943264) | Immune Bio, Alzheimer's Association | Nov 2019 | Dec 2020 |
NOTE. Thirty agents in 31 Phase 1 clinical trial currently ongoing as of January 25, 2022 according to clinicaltrials.gov.
Abbreviations: Aβ, amyloid beta; AAV, adeno‐associated virus; ADDF, Alzheimer's Drug Discovery Foundation; ApoE, apolipoprotein E; CADRO, Common Alzheimer's Disease and Related Disorders Research Ontology; CSF, cerebrospinal fluid; CSF‐1R, colony‐stimulating factor 1 receptor; DMT, disease‐modifying therapy; GABA, gamma‐aminobutyric acid; hTERT, human telomerase reverse transcriptase; NIA, National Institute on Aging; NNRTI, non‐nucleoside reverse transcriptase inhibitors; NRTI, nucleoside reverse transcriptase inhibitors; TNF, tumor necrosis factor.
Four (4%) of the trials in Phase 2 are prevention trials enrolling cognitively normal participants known to be at risk for AD (preclinical AD); three (3%) trials enroll both preclinical participants and participants with MCI to mild AD dementia; 49 (52%) trials enroll early AD defined as prodromal AD and mild AD dementia; 34 (36%) trials are with participants with mild to moderate AD dementia; two (2%) trials include participants with mild‐to‐severe AD dementia; and two (2%) trials enroll healthy volunteers.
Trials in Phase 2 included a mean of 127 participants per trial (range 5 to 856) and a total of 11,938 participants were needed for enrollment in all currently active Phase 2 trials. DMT prevention trials included a mean of 151 participants (range 32 to 320) and had a mean duration of 284 weeks (range 155 to 471 weeks, including the recruitment and the treatment period). DMT trials focusing on prodromal AD or prodromal AD/mild AD dementia had a mean of 138 participants (range 5 to 856) and a mean duration of 198 weeks (range 40 to 635 weeks, including the recruitment and the treatment period). Trials of DMTs enrolling mild to moderate AD dementia participants included an average of 107 participants (range 8 to 350) and a mean duration of 172 weeks (range 70 to 417 weeks, including the recruitment and the treatment period).
The mean treatment exposure period was 97 weeks (range 3 to 260 weeks) for prevention trials, 53 weeks (range 3 to 260 weeks) for prodromal AD or prodromal AD/mild AD dementia trials, and 31 weeks (range 8 to 108 weeks) for mild to moderate AD dementia trials. Recruitment periods (calculated as the total projected time until the primary completion date minus the treatment period) for DMT trials were prevention (145 weeks), prodromal AD and prodromal AD/mild AD dementia (117 weeks), and mild to moderate AD dementia (118 weeks).
The mean duration of Phase 2 cognitive enhancer trials was 127 weeks (range 39 to 337 weeks) including 27 treatment weeks (range 2 to 104 weeks), and they included an average of 105 participants (range 28 to 300). The mean duration of Phase 2 trials of treatments for neuropsychiatric symptoms was 150 weeks (range 39 to 321 weeks) including eight treatment weeks (range 1 to 15 weeks), and they included an average of 122 participants (range 40 to 186).
3.4. Phase 1
There are 30 agents in 31 Phase 1 trials (Figure 1, Table 4). There are 27 DMTs (90% of Phase 1 agents) in Phase 1 trials including nine (30% of the Phase 1 agents) biologics and 18 (60%) small molecules. There are two (6.7% of Phase 1 agents) putative cognitive enhancing agents and one (3.3%) drug intended to target behavioral symptoms. CADRO mechanisms represented among Phase 1 DMT therapies include inflammation (5 agents; 18.5% of DMTs); epigenetic regulators (4; 14.8%); amyloid (3; 11.1%); tau (3; 11.1%); proteostasis/proteinopathies (3; 11.1%); synaptic plasticity/neuroprotection (3; 11.1%); neurogenesis (2; 7.4%); vasculature (2; 7.4%); cell death (1; 3.7%); and metabolism and bioenergetics (1; 3.7%). Nine (30%) of the Phase 1 agents are repurposed treatments approved for use in another indication (eight DMTs; one cognitive enhancer). There are two trials in Phase 1 involving stem cell therapies.
TABLE 4.
Stem cell therapy in clinical trials for Alzheimer's disease (ClinicalTrials.gov accessed January 25, 2022)
| Agent | Phase | Status (CT.gov ID) | Sponsor | Subject characteristics | Amyloid evidence at entry |
|---|---|---|---|---|---|
| Allogeneic human MSCs | 1 | Active, not recruiting; (NCT04040348) | University of Miami | Mild to moderate AD with MMSE of 20 to 26 | Amyloid PET or CSF |
| SNK01 (autologous natural killer cell) | 1 | Recruiting; (NCT04678453) | NKMax America | MCI or AD | Not required |
| Allogenic adipose MSC‐Exosomes | 1/2 | Recruiting; (NCT04388982) | Ruijin Hospital, Cellular Biomedicine Group | Mild to moderate AD with MMSE of 10 to 24 | Not required |
| CB‐AC‐02 (placenta derived MSCs) | 1/2 | Recruiting; (NCT02899091) | CHABiotech Co. | Mild to moderate AD with KMMSE of 10 to 26 | Amyloid PET |
| Human umbilical cord blood‐derived MSCs (NEUROSTEM) | 1/2 | Recruiting, extension study; (NCT03172117) | Medipost | Probable AD with KMMSE of 18 to 26 | Amyloid PET |
| Allogeneic human MSCs | 2 | Recruiting; (NCT02833792) | Stemedica | Mild to moderate AD with MMSE of 12 to 24 | Amyloid PET |
| AstroStem (autologous adipose‐derived MSCs) | 2 | Not yet recruiting; (NCT04482413) | Nature Cell Co. | Mild AD with MMSE of 20 to 24 | CSF amyloid |
Abbreviations: AD, Alzheimer's disease; KMMSE, Korea Mini‐Mental State Examination; MMSE, Mini‐Mental State Examination; MSC, mesenchymal stem cell; PET, positron emission tomography.
Phase 1 trials have an average duration of 115 weeks (range 24 to 365 weeks) (recruitment and treatment period) and include a mean of 47 participants (range 5 to 120) in each trial. Phase 1 trials include both single ascending dose and multiple ascending dose studies.
3.5. Biomarkers
Table 5 shows the biomarkers used as entry criteria or as outcome measures in current Phase 3 and Phase 2 AD clinical trials of DMTs as described on clinicaltrials.gov; these data may be incomplete as not all trial descriptions note if biomarkers are included in the trial.
TABLE 5.
Biomarkers as outcome measures or as entry criteria in Phase 2 and Phase 3 DMT trials (clinicaltrials.gov accessed January 25, 2025)
| N of trials (%) | ||
|---|---|---|
| Biomarker role in trial | Phase 3 DMTs | Phase 2 DMTs |
| Biomarker as an entry criterion a | ||
| Amyloid PET | 6 (19%) | 12 (14%) |
| CSF amyloid | 0 | 5 (6%) |
| Amyloid PET or CSF amyloid | 6 (19%) | 12 (14%) |
| CSF Aβ/tau ratio | 0 | 6 (7%) |
| CSF Aβ/tau ratio or amyloid PET | 5 (16%) | 4 (5%) |
| Tau PET | 0 | 3 (4%) |
| Amyloid PET or CSF tau | 0 | 1 (1%) |
| Plasma tau | 1 (3%) | 0 |
| Biomarker as an outcome measure a | ||
| CSF amyloid | 8 (26%) | 20 (24%) |
| CSF tau | 8 (26%) | 24 (29%) |
| FDG‐PET | 2 (6%) | 7 (8%) |
| vMRI | 9 (29%) | 15 (18%) |
| Plasma amyloid | 4 (13%) | 13 (16%) |
| Plasma tau | 6 (19%) | 9 (11%) |
| Amyloid PET | 10 (32%) | 11 (13%) |
| Tau PET | 7 (23%) | 10 (12%) |
Abbreviations: CSF, cerebrospinal fluid; DMT, disease‐modifying therapy; FDG, fluorodeoxyglucose; PET, positron emission tomography; vMRI, volumetric magnetic resonance imaging.
Percentages refer to the percent of trials that used any biomarker as an outcome or the percent that used biomarkers as an entry criterion.
Of the 31 Phase 3 DMT trials, six trials (19%) used amyloid positron emission tomography (PET) as an entry criterion and six (19%) used either amyloid PET or cerebrospinal fluid (CSF) amyloid measures. Five (16%) of the Phase 3 DMT trials used either CSF‐amyloid/tau ratio or amyloid PET as an entry criterion, and one trial used plasma phosphorylated tau (p‐tau) 217. Thirteen (42%) of Phase 3 DMT trials did not use biomarkers as study entry criteria. One Phase 3 trial of a cognitive enhancer used CSF amyloid or CSF tau for entry.
In Phase 2, 12 (14%) DMT trials used amyloid PET as an entry criterion, five (6%) used CSF amyloid or amyloid ratios, and 12 (14%) used either amyloid PET or CSF amyloid assessments. Six (7%) of the Phase 2 DMT trials used CSF‐amyloid/tau ratio as an entry criterion, four (5%) used either CSF‐amyloid/tau ratio or amyloid PET, three (4%) used tau PET, and one trial (1%) used either amyloid PET or CSF‐tau. Thirty‐nine (47%) of Phase 2 trials did not require biomarker‐based diagnostic confirmation for study entry.
Of Phase 3 DMT trials, 19 (61%) used biomarkers as supportive outcomes. Ten (32%) used amyloid PET and seven (23%) used tau PET in support of clinical outcomes. In Phase 2, 46 DMT trials (55%) have biomarkers as supportive outcomes (11 amyloid PET; 10 tau PET).
3.6. Trial participants
Including all currently active trials, the total number of participants needed is 50,575. Of these, 37,184 are required for Phase 3 trials; 11,938 for Phase 2 trials; and 1453 for Phase 1 trials. Table 6 shows the major types of trials, the average duration in weeks of treatment exposure for each type of trial, and the number of participants required for each type of trial. This demonstrates that across all active trials, 3,878,843 participant‐weeks will be devoted to clinical trials. This total is an underestimate as it does not include time devoted to screening prior to randomization or the time consumed in screen fails of individuals who do not progress to randomization. Nearly all trials (except Phase 1 trials) require a research partner that devotes an equal number of weeks to the trials making the total investment of time by participants and families ≈7,757,686 weeks or 148,777 years.
TABLE 6.
Total person weeks contributed by participants for each type of trial (clinicaltrials.gov accessed January 25, 2022)
| Phase | Type of trial | Average duration of treatment (weeks) | Total number of participants | Total participant weeks devoted to clinical trials |
|---|---|---|---|---|
| Phase 3 | Prevention (preclinical AD) | 159 | 7403 | 1,177,077 |
| DMT (not prevention) | 87 | 23,050 | 2,005,350 | |
| Cognitive enhancing | 24 | 1960 | 47,040 | |
| Psychotropic | 18 | 5261 | 94,698 | |
| Phase 2 | DMT | 49 | 10,717 | 525,133 |
| Cognitive enhancing | 27 | 735 | 19,845 | |
| Psychotropic | 8 | 486 | 3888 | |
| Phase 1 | All | 4 | 1453 | 5812 |
| Total | 3,878,843 weeks | |||
Abbreviations: AD, Alzheimer's disease; DMT, disease‐modifying therapy.
Recruitment of participants remains a major challenge and a key reason for the long duration of trials. Using the treatment period as a comparison, Phase 3 prevention and prodromal/mild AD dementia trials have approximately equal treatment and recruitment periods. Phase 3 mild‐moderate AD dementia trials take 1.8 times longer to recruit participants than to assess treatment effects. In Phase 2, recruitment periods are consistently longer than exposure periods: 1.5 times longer for prevention trials, 2.2 times longer for prodromal/mild AD dementia trials, and 3.8 times longer for mild‐moderate AD dementia.
3.7. Trial sponsors
Across all trials, 50% are sponsored by the biopharma industry, 28% by academic medical centers (usually with funding from NIH), 17% are funded through public–private partnerships, and 5% are funded by other entities. In Phase 3, 68% of trials are sponsored by the biopharma industry, 15% by academic medical centers/NIH, 11% are public–private partnerships, and 6% are sponsored by others. In Phase 2, 41% of trials are sponsored by the biopharma industry, 36% by academic medical centers/NIH, 19% are public–private partnerships, and 3% are funded by others. Table 7 shows the sponsor of agents in each phase of development. Repurposed agents are more likely to have academic medical center/NIH sponsors (56%) and less likely to have industry sponsors (21%; Table 7).
TABLE 7.
Trial sponsor for each phase of AD drug development and the number of trials of repurposed agents supported by each entity (clinicaltrials.gov accessed January 25, 2022)
| N of trials (%) | |||||
|---|---|---|---|---|---|
| Sponsor type | Phase 3 | Phase 2 | Phase 1 | All phases | Repurposed agents |
| Biopharma Industry | 32 (68%) | 39 (41%) | 15 (48%) | 86 (50%) | 13 (21%) |
| Academic medical centers/NIH | 7 (15%) | 34 (36%) | 8 (26%) | 49 (28%) | 34 (56%) |
| Public‐private partnerships (PPP) | 5 (11%) | 18 (19%) | 6 (19%) | 29 (17%) | 7 (11%) |
| Others | 3 (6%) | 3 (3%) | 2 (6%) | 8 (5%) | 7 (11%) |
Abbreviations: AD, Alzheimer's disease; NIH, National Institutes of Health.
3.8. Global distribution of trials
Table 8 shows the global distribution of trials. We divided trials into those performed only in North America (United States and Canada); those conduced only outside of North America (excluding United States and Canada); and those conducted globally including North American and non‐North American sites combined. Thirty‐six percent of Phase 3 trials involved only North America and 40% included North American and non‐North American countries (76% of trials include North American sites with or without sites in other global regions). Phase 2 trials are more often conducted only in North America (54%); North America is included as a trial location in 64% of trials (trials done in North America only plus those conducted in North American and non‐North American sites together). Some Phase 1 trials conducted outside the United States may not be registered on clinicaltrials.gov and may have gone undetected in this review. Across all phases, 48% of trials are conducted only in North America; 33% are conducted only outside of North America; and 20% are conducted with both North American and non‐North American sites participating. North America participates in 67% of all trials registered on clinicaltrials.gov.
TABLE 8.
Global distribution of trials (clinicaltrials.gov accessed January 25, 2022)
| N of trials (%) | |||
|---|---|---|---|
| Phase 3 | Phase 2 | Phase 1 | |
| North America (United States & Canada) only | 17 (36%) | 51 (54%) | 14 (45%) |
| Non‐North America only | 11 (23%) | 30 (32%) | 15 (48%) |
| North America and Non‐North America | 19 (40%) | 13 (14%) | 2 (6%) |
4. DISCUSSION
Development of new therapies for diseases of the nervous system is challenging with high failure rates and long development times forcing some major pharmaceutical companies to stop investing in this area of drug development. 18 Of the 49 novel drugs approved by the FDA in 2021, seven were for treatment of disorders of the central nervous system (CNS) and two were for the peripheral nervous system disorders (Duchenne muscular dystrophy, myasthenia gravis; fda.gov). 19 The CNS disorders with new treatments were migraine, von Hippel‐Lindau disease (including CNS hemangioblastomas), schizophrenia, relapsing multiple sclerosis, attention deficit‐hyperactivity disorders (two drugs approved), and AD. The AD drug approval is the first in the United States since 2003.
The AD drug development pipeline comprises 143 agents in 172 trials (Figure 1). There are 31 agents in Phase 3, 82 in Phase 2, and 31 in Phase 1. DMTs are the agents most included in the pipeline. One hundred nineteen putative DMTs are being assessed (21 in Phase 3, 71 in Phase 2, 27 in Phase 1). DMTs represent 83.2% of the pipeline of agents. There are 14 cognitive enhancers and 10 drugs targeting neuropsychiatric symptoms in the pipeline. The 143 agents in the pipeline compares to 126 in the pipeline in 2021; 10 , 11 this apparent increase may be partially attributable to our improved search techniques.
Aducanumab is the first DMT approved by the US FDA for the treatment of AD. It is the second DMT approved in the United States for any neurodegenerative disease, the other is edaravone used in the treatment of amyotrophic lateral sclerosis. 20 The approval of aducanumab used an accelerated regulatory mechanism based on demonstration of amyloid plaque lowering considered reasonably likely to predict clinical benefit. 21 The accelerated pathway may be used for other anti‐amyloid plaque‐lowering antibodies currently under review by the FDA (donanemab and lecanemab). 3 , 4 , 5 The trials of gantenerumab will be completed in 2022 and may lead to a request for marketing approval based on conventional clinical outcomes. 22 , 23 Other biomarkers may eventually be qualified as surrogate outcomes predictive of clinical benefit. Surrogate outcomes facilitate drug development. 24
MCI due to AD and mild AD dementia comprise the most common population included in current clinical trials accounting for 36% of Phase 3 trials and 52% of Phase 2 trials. 25 These trials may be most impacted by the approval of aducanumab for this same population. Trial patients eligible for aducanumab may wish to begin active therapy rather than remain in a placebo‐controlled trial that will last many months; patients appropriate for treatment with aducanumab and eligible for trial participation may prefer active treatment to trial enrollment; or patients on aducanumab may wish to continue this treatment and be included in trials of potential new AD therapies in addition to their ongoing treatment. Trial design will require reconsideration to account for the presence of aducanumab in the market. 26 Among the trial design options are to exclude patients on aducanumab from participation in a trial assessing a new therapy as is currently done in some AD trials that exclude cholinesterase inhibitors or memantine. Another option is to allow aducanumab as background therapy with stratification, analytic adjustment, and recalculation of sample sizes required to show a treatment effect. Trials comparing a novel agent to aducanumab may be conducted with superiority or a non‐inferiority design with clinical efficacy, biomarker effects, or safety as primary or key secondary outcomes. AD therapeutic research can build on lessons learned from multiple sclerosis where multiple DMTs have been approved using a variety of assessment strategies. 27
The CADRO classification of targets reveals a proliferation of mechanistic treatment approaches to AD including agents directed at amyloid (20 agents), tau (13 agents), inflammation (23 agents), and synaptic plasticity (19 agents). Altogether 15 of the 17 categories (excluding “unknown” and “other”) are represented by drugs in the pipeline (Figure 4).
FIGURE 4.
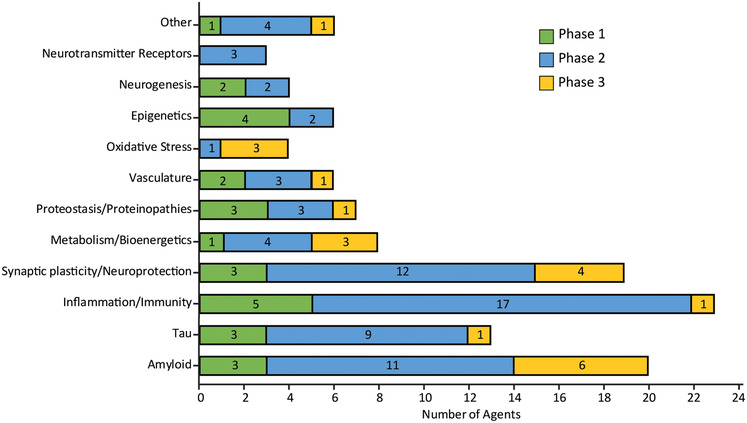
Mechanisms of action of disease modifying agents in all phases of clinical trials grouped according to the Common Alzheimer's Disease Research Ontology (CADRO) (Figure © J Cummings; M de la Flor, PhD, Illustrator)
Seven monoclonal antibodies, one active vaccine, one ASO, and four small molecules directed at aspects of the biology of the tau protein and neurofibrillary tangle formation are currently in AD clinical trials. The antibodies are directed primarily at extracellular tau that is transferred from cell to cell in a prion‐like manner. Several tau monoclonal antibodies have failed to establish a drug–placebo difference in recent AD trials including semorinemab, zagotenemab, gosuranemab, and ABBV‐8E12. 28 , 29
Targets for monoclonal antibodies in the current AD pipeline other than the canonical amyloid and tau proteins include antibodies directed at TREM2, CD38, semaphorin 4D, and galactin 3.
The SARS‐CoV‐2 virus and ensuing pandemic have challenged trial sites and temporarily slowed drug development. Many COVID‐related issues affected trial sites including temporary or permanent site closure; delayed recruitment; participant reluctance to visit sites for clinical assessments and laboratory tests; patient and care partner decisions to stop trial participation; difficulty providing drugs to participants not visiting sites; the change of on‐site testing stemming from masks, shields, and COVID testing procedures; the need to develop unanticipated strategies for remote data collection and laboratory testing; the requirement to adjust procedures to obtain or renew informed consent remotely; illness and death of trial participants; and illness, death, and resignation of trial site staff. 30 The FDA provided guidance of Good Clinical Practice of trial conduct during the pandemic. 31 , 32 The FDA also provided guidance on statistical and analytic considerations for data from trials affected by the COVID pandemic. 31 Many AD trial outcomes were successfully administered using telemedicine without compromise of data reliability. 33 Statistical modeling and trial simulation of AD trials indicated that stopping trials usually resulted in substantial loss of power and prolonging or enlarging trials were strategies to preserve trial integrity. 34 Despite the many challenges posed by the SARS‐CoV‐2 pandemic, the AD trial ecosystem proved to be resilient with few trials stopped during the pandemic and a substantial number of new trials initiated.
The increased use of composite outcomes is apparent in this review. This trend is especially evident in trials in early AD (MCI due to AD and mild AD dementia) in which a significant drug–placebo difference on a single primary outcome measure may be the basis for regulatory approval. Many trials in this stage of the disease use the Clinical Dementia Rating–Sum of Boxes (CDR‐SB) as the primary outcome. 35 Phase 2 trials have used a greater diversity of primary clinical outcomes. The Phase 2 trial of lecanemab used the Alzheimer's Disease Composite Score (ADCOMS)—an analytic approach using the all items of the CDR and elements of the MMSE and Alzheimer's Disease Assessment Scale–Cognitive subscale (ADAS‐Cog)—as an outcome and as a guide to dose decisions in the Bayesian dose‐finding portion of the study. 5 , 36 The Phase 2 trial of donanemab used the integrated Alzheimer's Disease Rating Scale (iADRS) comprising the ADAS‐Cog‐13 and the Alzheimer's Disease Cooperative Study (ADCS) instrumental Activities of Daily Living (iADL) scale as the primary clinical outcome measure. Composite endpoints, when appropriately constructed and interpreted, provide greater measurement efficiency and can facilitate efficacy conclusions with smaller sample sizes. 37
Biomarkers play increasingly informative roles in AD trials. The Phase 2 trial of donenemab used tau PET to define the population, requiring the presence of tau but without a high level of tau abundance suggesting advanced disease. 4 Nearly all the participants meeting the tau PET criteria had positive amyloid imaging; the discordance was 0.9% of individuals who met the tau PET criteria and not the amyloid PET criteria. This supports the observation that the presence of moderate levels of tau are highly predictive of the amyloid plaque burden. 38 , 39 Plasma p‐tau is highly correlated with amyloid PET 40 , 41 and is being used to identify participants for some AD trials (e.g., Trailblazer 3). If confirmed, use of p‐tau to identify individuals for AD trials is anticipated to simplify and accelerate AD trial recruitment.
Other notable observations from this pipeline review include the large number of participants needed for all ongoing trials (50,757) and the tremendous amount of participant time devoted to trials (3,878,843 weeks spent in trials). The long periods required for participant recruitment are documented in this review; many trials have recruitment periods that exceed the treatment period by 2‐fold. The key role played by the biopharmaceutical industry in drug development is highlighted by the observation that industry sponsors 68% of all Phase 3 trials and 41 percent of all Phase 2 trials. The NIH and academic medical centers play a large role in Phase 2 proof‐of‐concept studies (36% of trials) and a smaller role in late‐stage drug development (15% of Phase 3 trials). Repurposed agents have a greater role in proof‐of‐concept and are more likely to be funded by NIH (56%) than biopharmaceutical sponsors (21%). 42 Global participation in drug development is evident in this review. Sixty‐three percent of Phase 3 trials and 46% of Phase 2 trials include non‐North American sites.
This review is based on data from the clinical trials registry, clinicaltrials.gov. Recent studies support the use of this data source. Venugopal and Saberwal showed that clinicaltrials.gov is more comprehensive than any other of the 18 worldwide registries they reviewed. 15 The FDA Amendments Act of 2007 requires reporting of trial results within 1 year of trial completion and the FDA and NIH are increasingly vigilant about enforcement of this mandate, further strengthening the data available from the registry. 43 The registry and our search strategies are imperfect, and some agents may have been omitted in this review.
5. SUMMARY
Clinical trials for AD target a robust array of biological processes including most of those identified in the CADRO classification. Amyloid therapies have shown progress with approval of the monoclonal antibody aducanumab. Other amyloid approaches as well as treatments for tau abnormalities, inflammation, and synaptic dysfunction are well represented in the AD drug development pipeline. The number of clinical trials has increased somewhat despite challenges created by the current pandemic. Biomarkers are increasingly used to inform clinical trials including their use in diagnosis and as outcomes. New clinical outcome measures, especially composite scale and scores, provide greater sensitivity to treatment response. Drug development for AD depends on robust alliances with participants and their families given the large time sacrifices they make in trial involvement. The distribution of sites in trials demonstrates the global ecosystem that supports AD drug development. Progress in target identification, drug discovery, and clinical trial methodology increases confidence that more and better treatments will emerge from the AD drug development pipeline.
CONFLICTS OF INTEREST
Jeffrey Cummings has provided consultation to Acadia, Alkahest, AlphaCognition, AriBio, Avanir, Axsome, Behren Therapeutics, Biogen, Biohaven, Cassava, Cerecin, Cortexyme, Diadem, EIP Pharma, Eisai, GemVax, Genentech, Green Valley, Grifols, Janssen, LSP, Merck, NervGen, Novo Nordisk, Oligomerix, Ono, Otsuka, PRODEO, ReMYND, Renew, Resverlogix, Roche, Signant Health, Suven, United Neuroscience, and Unlearn AI pharmaceutical, assessment, and investment companies. Jeffrey Cummings owns the copyright of the Neuropsychiatric Inventory. Garam Lee is a full‐time employee of Biogen. Kate Zhong provides consultation to Green Valley Pharmaceuticals. Pouyan Nahed has no disclosures. Mina Esmail Zadeh Nojoo Kambar has no disclosures. Jorge Fonseca has no disclosures. Kate Zhong has no disclosures.
ACKNOWLEDGMENTS
Jeffrey Cummings is supported by NIGMS grant P20GM109025; NINDS grant U01NS093334; NIA grant R01AG053798; NIA grant P20AG068053; NIA grant R35AG71476; and the Alzheimer's Disease Drug Discovery Foundation (ADDF).
Cummings J, Lee G, Nahed P, et al. Alzheimer's disease drug development pipeline: 2022. Alzheimer's Dement. 2022;8:e12295. 10.1002/trc2.12295
REFERENCES
- 1. Alzheimer's Association . 2021 Alzheimer's disease facts and figures. Alzheimer's Dement. 2021;17:327‐406. [DOI] [PubMed] [Google Scholar]
- 2. Scheltens P, De Strooper B, Kivipelto M, et al. Alzheimer's disease. Lancet. 2021;397:1577‐1590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Rabinovici GD. Controversy and progress in Alzheimer's disease—FDA approval of aducanumab. N Engl J Med. 2021;385:771‐774. [DOI] [PubMed] [Google Scholar]
- 4. Mintun MA, Lo AC, Duggan Evans C, et al. Donanemab in early Alzheimer's disease. N Engl J Med. 2021;384:1691‐1704. [DOI] [PubMed] [Google Scholar]
- 5. Swanson CJ, Zhang Y, Dhadda S, et al. A randomized, double‐blind, phase 2b proof‐of‐concept clinical trial in early Alzheimer's disease with lecanemab, an anti‐Abeta protofibril antibody. Alzheimers Res Ther. 2021;13:80‐94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Cummings J, Morstorf T, Lee G. Alzheimer's drug‐development pipeline: 2016. Alzheimers Dement (N Y). 2016;2:222‐232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Cummings J, Lee G, Mortsdorf T, et al. Alzheimer's disease drug development pipeline: 2017. Alzheimers Dement (N Y). 2017;3:367‐384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Cummings J, Lee G, Ritter A, et al. Alzheimer's disease drug development pipeline: 2018. Alzheimers Dement (N Y). 2018;4:195‐214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Cummings J, Lee G, Ritter A, et al. Alzheimer's disease drug development pipeline: 2019. Alzheimers Dement (N Y). 2019;5:272‐293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Cummings J, Lee G, Ritter A, et al. Alzheimer's disease drug development pipeline: 2020. Alzheimer's Dementi. 2020;6:e12050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Cummings J, Lee G, Zhong K, et al. Alzheimer's disease drug development pipeline: 2021. Alzheimers Dement (N Y). 2021;7:e12179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. H.R.3580 – Food and Drug Administration Amendments Act of 2007 110th Congress (2007‐2008). 2007–2008.
- 13. Lassman SM, Shopshear OM, Jazic I, et al. Clinical trial transparency: a reassessment of industry compliance with clinical trial registration and reporting requirements in the United States. BMJ Open. 2017;7:e015110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Phillips AT, Desai NR, Krumholz HM, et al. Association of the FDA Amendment Act with trial registration, publication, and outcome reporting. Trials. 2017;18:333‐343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Venugopal N, Saberwal G. A comparative analysis of important public clinical trial registries, and a proposal for an interim ideal one. PLoS One. 2021;16:e0251191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Cummings J, Fox N. Defining disease modifying therapy for Alzheimer's disease. J Prev Alzheimers Dis. 2017;4:109‐115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Kambar MEZN, Nahed P, Cacho JRF, et al. Clinical text classification of Alzheimer's drugs’ mechanism of action In: Yang XS., Sherratt S., Dey N., Joshi A. (eds) Proceedings of Sixth International Congress on Information and Communication Technology. Lecture Notes in Networks and Systems, vol 235. Springer, Singapore. 10.1007/978-981-16-2377-6_48.2022. [DOI] [Google Scholar]
- 18. Gribkoff VK, Kaczmarek LK. The need for new approaches in CNS drug discovery: why drugs have failed, and what can be done to improve outcomes. Neuropharmacology. 2017;120:11‐19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. U.S. Food & Drug Administration fda.gov . Novel drug approvals for 2021. https://www.fda.gov/
- 20. Yoshino H. Edaravone for the treatment of amyotrophic lateral sclerosis. Expert Rev Neurother. 2019;19:185‐193. [DOI] [PubMed] [Google Scholar]
- 21. Dunn B, Stein P, Cavazzoni P. Approval of aducanumab for Alzheimer disease‐the FDA's perspective. JAMA Intern Med. 2021;181:1276‐1278. [DOI] [PubMed] [Google Scholar]
- 22. Ostrowitzki S, Lasser RA, Dorflinger E, et al. A phase III randomized trial of gantenerumab in prodromal Alzheimer's disease. Alzheimers Res Ther. 2017;9:95‐110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Klein G, Delmar P, Kerchner GA, et al. Thirty‐six‐month amyloid positron emission tomography results show continued reduction in amyloid burden with subcutaneous gantenerumab. J Prev Alzheimers Dis. 2021;8:3‐6. [DOI] [PubMed] [Google Scholar]
- 24. Cummings J. The role of biomarkers in Alzheimer's disease drug development. Adv Exp Med Biol. 2019;1118:29‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Weiner MW, Aisen PS, Beckett LA, et al. Editorial: How will aducanumab approval impact AD research? J Prev Alzheimers Dis. 2021;8:391‐392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Grill JD, Karlawish J. Implications of FDA approval of a first disease‐modifying therapy for a neurodegenerative disease on the design of subsequent clinical trials. Neurology. 2021;97:496‐500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Grzegorski T, Losy J. Multiple sclerosis—The remarkable story of a baffling disease. Rev Neurosci. 2019;30:511‐526. [DOI] [PubMed] [Google Scholar]
- 28. Mulnard A. Anti‐tau antibody failures stack up. Nat Rev Drug Discov. 2021;20:888. [DOI] [PubMed] [Google Scholar]
- 29. Mulnard A. Failure of first anti‐tau antibody in Alzheimer disease highlights risks of history repeating Nat Rev Drug Discov 2021;20:3‐5. [DOI] [PubMed] [Google Scholar]
- 30. Mitchell EJ, Ahmed K, Breeman S, et al. It is unprecedented: trial management during the COVID‐19 pandemic and beyond. Trials. 2020;21:784‐791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Food and Drug Administration . Statistical Considerations for Clinical Trials during the COVID‐19 Public Health Emergency: Guidance for Industry. U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluation and Research (CBER), Center for Devices and Radiological Health (CDRH), Center for Veterinary Medicine (CVM). Washington DC: Food and Drug Administration; 2020. [Google Scholar]
- 32. Food and Drug Administration . Conduct of Clinical Trials of Medical Products during the COVID‐19 Public Health Emergency: Guidance for Industry, Investigators, and Institutional Review Boards. Food and Drug Administration; 2020. Updated on August 30, 2021. U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluation and Research (CBER), Center for Devices and Radiological Health (CDRH) Oncology Center of Excellence (OCE), Office of Good Clinical Practice (OGCP). Washington, DC: Food and Drug Administration; 2020. Updated August 2021. 2021. [Google Scholar]
- 33. Geddes MR, O'Connell ME, Fisk JD, et al. Remote cognitive and behavioral assessment: report of the Alzheimer Society of Canada Task Force on dementia care best practices for COVID‐19. Alzheimers Dement (Amst). 2020;12:e12111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Schneider LS, Qiu Y, Thomas RG, et al. Impact of potential modifications to Alzheimer's disease clinical trials in response to disruption by COVID‐19: a Simulation Study. Alzheimers Res Ther. 2021;13:201‐214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. McDougall F, Edgar C, Mertes M, et al. Psychometric properties of the Clinical Dementia Rating—Sum of Boxes and other cognitive and functional outcomes in a prodromal Alzheimer's disease population. J Prev Alzheimers Dis. 2021;8:151‐160. [DOI] [PubMed] [Google Scholar]
- 36. Wang J, Logovinsky V, Hendrix SB, et al. ADCOMS: a composite clinical outcome for prodromal Alzheimer's disease trials. J Neurol Neurosurg Psychiatry. 2016;87:993‐999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Sankoh AJ, Li H, D'Agostino RB, Sr. . Use of composite endpoints in clinical trials. Stat Med. 2014;33:4709‐4714. [DOI] [PubMed] [Google Scholar]
- 38. Pontecorvo MJ, Devous MD, Sr. , Navitsky M, et al. Relationships between flortaucipir PET tau binding and amyloid burden, clinical diagnosis, age and cognition. Brain. 2017;140:748‐763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Brier MR, Gordon B, Friedrichsen K, et al. Tau and Abeta imaging, CSF measures, and cognition in Alzheimer's disease. Sci Transl Med. 2016;8:338ra366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Barthelemy NR, Horie K, Sato C, et al. Blood plasma phosphorylated‐tau isoforms track CNS change in Alzheimer's disease. J Exp Med. 2020;217:e20200861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Mattsson‐Carlgren N, Janelidze S, Bateman RJ, et al. Soluble P‐tau217 reflects amyloid and tau pathology and mediates the association of amyloid with tau. EMBO Mol Med. 2021;13:e14022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Cummings J, Bauzon J, Lee G. Who funds Alzheimer's disease drug development? Alzheimers Dement (N Y). 2021;7:e12185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Ramachandran R, Morten CJ, Ross JS. Strengthening the FDA's enforcement of ClinicalTrials.gov reporting requirements. JAMA. 2021;326:2131‐2132. [DOI] [PubMed] [Google Scholar]