

Abstract
Purpose:
Sugar-sweetened beverage (SSB) consumption is high among US adults and associated with obesity. Given that over 100 million Americans consume food or beverages at work daily, the worksite may be a venue for interventions to reduce SSB consumption. However, the level of support for these interventions is unknown. We examined associations between workday SSB intake and employees’ support for worksite wellness strategies (WWS).
Design:
Cross-sectional study conducted using data from web-based annual surveys that gathers information on health-related attitudes and behaviors.
Setting:
United States
Subjects:
Randomly selected 1,924 employed adults (≥18 years) using probability-based sampling.
Measures:
Self-reported independent variable was workday SSB intake (0, <1 or ≥1 times/day) and dependent variables were employees’ support (yes/no) for the following WWS: 1) Accessible Free Water, 2) Affordable Healthy Food/Drink, 3) Available Healthy Options, and 4) Less Available SSB.
Analysis:
Multivariable logistic regression was used to control for sociodemographic variables, employee size, and availability of cafeteria/VM.
Results:
About half of employees supported Accessible Free Water (54%), Affordable Healthy Food/Drink (49%), and Available Healthy Options (46%), but only 28% supported Less Available SSB. Compared to non-SSB consumers, daily SSB consumers were significantly less supportive of Accessible Free Water (adjusted odds ratio [OR]=0.67, p<0.05) or Less Available SSB (OR=0.49, p<0.05).
Conclusion:
Almost half of employees supported increasing healthy options within worksites, although daily workday SSB consumers were less supportive of certain strategies. Lack of support could be a potential barrier to the successful implementation of certain worksite interventions.
Keywords: Sugar-sweetened beverage, adults, worksite, intervention, wellness, Manuscript format: Research, Research purpose: Relationship testing, Study design: Cross-sectional, Outcome measure: Behavioral, Setting: Worksite, Health Focus: Nutrition, Target population age: Adults, Target population circumstances: Employed US Adults
INTRODUCTION
Worksites are an important setting to promote behaviors associated with improving adults’ dietary intake, which may also assist in preventing and controlling obesity.1–3 Approximately 111.5 million US adults are employed full-time and over 100 million Americans consume food or beverages at work daily.1 Of employed adults, a recent study found that approximately 3 of 10 employed adults were obese.4 The work environment has been shown to influence obesity-related behaviors due to a number of factors including sedentary work environment,5 worksite cafeterias,6 and vending machines.7 Obesity is associated with increased use and duration of sick leave and reductions in work productivity.8 In addition, obesity and other chronic diseases may lead to increasing and unsustainable health care costs for the worksites.8,9 For example, a morbidly obese employee (BMI >40 kg/m2) costs his or her employer $3,800 more per year in covered health care expenditures compared to a normal weight employee.9 Healthy lifestyle practices throughout the workday can assist in the maintenance of good health and a healthy weight, as well as prevention of chronic diseases.10
One obesity-related behavior of employees that may be affected by their worksite nutrition environment (e.g., vending machines and cafeterias at worksites) is consumption of sugar-sweetened beverages (SSBs), which has been associated with obesity/weight gain, diabetes, and cardiovascular disease.11 The 2010 Dietary Guidelines for Americans defined SSB as “liquids that are sweetened with various forms of sugars that add calories. These beverages include, but are not limited to, soda, fruit aides and fruit drinks, and sports and energy drinks.”12 SSBs are a large source of added sugars to American adults’ diet.13 In 2009‒2010, nearly half of American adults consumed SSBs on any given day, contributing on average 151 kcal per day.14 Worksites could be a venue for interventions to reduce employees’ SSB consumption.
Worksite wellness strategies (WWS) are employer-sponsored initiatives directed at improving the health and well-being of workers.15 One of several factors important to successful implementation of WWS is employee support.16 It is well-documented that employee health results from a complex interplay of intrapersonal, interpersonal, organizational, and cultural factors.17–20 According to an organization-level theory of the determinants of effective implementation of worksite health promotion programs, organizational readiness for change directly influences implementation policies and practices.21 Therefore, we conceptualized that employees’ support for WWS might influence organizational readiness for change and thus lead to implementation.
Food and beverage WWS, including point-of-purchase labeling, promotional materials, expanded availability of healthy foods, and targeted food placement, have shown to improve dietary quality among employees.22 The level of employees’ support for food and beverage WWS is unknown, despite the importance of the worksite nutrition environment for obesity and chronic disease prevention. In this study, we 1) describe the level of support for four WWS targeting food and beverage options and associated characteristics of employees, 2) describe SSB intake during the workday among employed US adults and characteristics associated with employees’ level of SSB intake during the workday, and 3) examine the relationship between employee support for WWS and SSB intake during the workday among employed US adults.
METHODS
Sample and survey administration
This cross-sectional study was conducted using data from the summer wave of Porter Novelli’s 2013 ConsumerStyles survey, which is a series of web-based annual surveys that gathers information from American consumers. Included in ConsumerStyles are questions on health-related attitudes and behaviors. The survey participants were randomly selected from the GfK’s Knowledge Panel® (a large-scale online panel based on a representative random sample of the US population), a pool of approximately 50,000 adults, using probability-based sampling which included respondents regardless of phone or internet access. Households without a computer or no access to internet were provided with a laptop computer and internet access. The analysis of this data was considered as exempt from the CDC Institutional Review Board, because de-identified data were provided to CDC.
In order to participate in the summer wave of ConsumerStyles survey, the respondent completed the spring wave of ConsumerStyles survey sent during April and May 2013. The spring wave of ConsumerStyles survey was sent out to 11,188 adults aged ≥18 years old and a response rate of 60.0% was achieved (n=6,717) (Figure 1). Subsequently, during June and July 2013, the summer wave of ConsumerStyles survey was sent to a random sample of 6,105 adults (4,497 panelists aged 18 or older plus a supplemental sample of 1,608 panelists with children aged 12–17 to collect adult-youth data) who previously completed the spring wave. A total of 4,033 of the summer wave of the ConsumerStyles survey were returned, yielding a response rate of 66.0%. The resulting data were weighted to match the US Current Population Survey proportions for sex, age, household income, race/ethnicity, household size, education level, census region, metro status, and whether or not a respondent had internet access prior to joining the survey panel.
Figure 1.
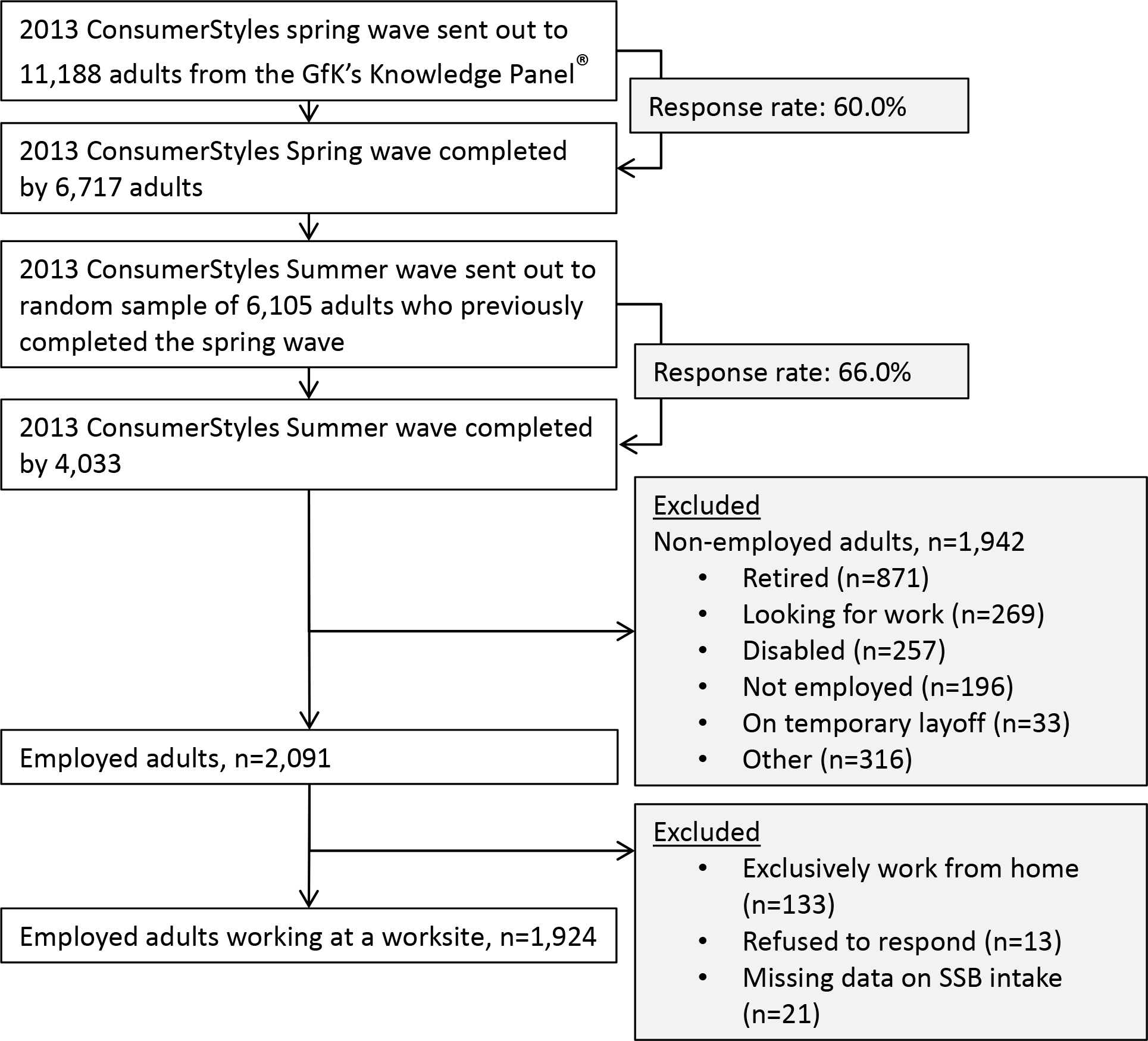
Analytic Sample flowchart
For the purpose of our study, we included adults aged ≥18 years old who were employed (n=2,091). We excluded a total of 164 participants (7.8%) from the study because they worked exclusively from home (n=133), refused to respond (n=13), or had missing data on SSB intake (n=21). The final analytic sample size was 1,924 adults (Figure 1).
Support for worksite wellness strategies
The outcome variables of interest were employees’ support for food and beverage WWS (three accessibility and one restrictive). To measure employees’ support for worksite food and beverage wellness strategies, respondents were asked “Which of the following do you think employers should do to make worksites healthier?” and to respond ‘yes’ or ‘no’ to the following four strategies that included three accessibility strategies: (1) ‘Provide employees ready access to free drinking water’ (Accessible Free Water); (2) ‘Make healthier foods and drinks more affordable in cafeterias/vending machines’ (Affordable Healthy Food/Drink); (3) ‘Provide employees with healthy cafeteria/vending options’ (Available Healthy Options); and one restrictive strategy (4) ‘Decrease the number of sugary drinks, such as sodas, in cafeterias/vending machines’ (Less Available SSB).
SSB intake
SSB intake was the main exposure variable and it was assessed using the following question: “During the last week, how many times during the workday did you drink sugary drinks such as sodas, sugar-sweetened ice tea, sports or energy drinks, and fruit drink? Do not count diet/low calorie versions”. Response choices were ‘I did not drink any sugary drinks at work’, ‘1 to 4 times last week’, ‘once a day’, or ‘more than once a day’. We created three mutually exclusive categories to reflect SSB intake during the workweek: none (no SSB intake at work), 1–4 times/workweek, or ≥1 time/workday.
Sociodemographic and employment variables
Sociodemographic variables were age (18–24, 25–44, 45–64, and ≥65 years), sex, race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, or non-Hispanic other races), education level (<high school, high school, some college, and college graduate), annual household income (<$35,000, $35,000–$74,999, $75,000–$99,999, or ≥$100,000), and geographic regions (Northeast, Midwest, South, and West based on the Census regions). Employment characteristic variables were the number of employees (1–49, 50–99, 100–499, and ≥500) and the availability of cafeteria/vending machine (VM) (A response of ‘yes” indicated that any of the following is available: food vending, drink vending, cafeteria, or snack bar; otherwise no).
Statistical Analysis
Chi-square tests were used to examine the relationship between four outcome variables and covariates. A p-value of <0.05 was used to define statistical significance. A series of independent multivariable logistic regression analyses was used to estimate adjusted odds ratios (AORs) and 95% confidence intervals (CI) for SSB intake (exposure variable) associated with employees’ support on WWS (outcome) after controlling for age, sex, race/ethnicity, education level, annual household income, geographic regions, number of employees, and any availability of cafeteria/VM. All statistical analyses were performed with the Statistical Analysis Software (SAS) (version 9.3, SAS Institute Inc, Cary, NC) and all analyses accounted for the sample weights.
RESULTS
Among the 1,924 employed adults included in the analytic sample, 56% of adults did not consume SSB during the workweek, 25% consumed SSB 1–4 times/work week, and 19% consumed SSB at least once per workday (Table 1). SSB intake significantly differed by age, sex, race/ethnicity, education level, annual household income, geographic region, and any availability of cafeteria/VM (χ2 tests, p<0.05). Within demographic groups with significant differences, the proportion of adults who consumed SSB at least once per workday was highest among adults aged 18‒44 years, males, Hispanics, those with <high school education, those with annual household income of ≤$74,999, and those living in the Midwest or South region (Table 1).
Table 1.
Characteristics of employed US adults and their sugar-sweetened beverage (SSB) intake during the workday (N=1,924)—Summer ConsumerStyles Survey, 2013
| Characteristics | All | SSB intake during the workweek | |||
|---|---|---|---|---|---|
| None | 1–4 times/workweek | ≥1 times/workday | P valueb | ||
| N (weighted %)a | % ± SE | % ± SE | % ± SE | ||
| Total sample | 1,924 (100) | 56.1 ± 1.6 | 24.7 ± 1.4 | 19.2 ± 1.3 | |
| Age | |||||
| 18–24 y | 108 (10.6) | 44.4 ±5.2 | 34.7 ± 5.0 | 20.9 ± 4.3 | <0.001 |
| 25–44 y | 731 (46.8) | 51.8 ± 2.5 | 27.5 ± 2.2 | 20.7 ± 2.1 | |
| 45–64 y | 989 (38.3) | 63.5 ± 2.2 | 18.4 ± 1.8 | 18.1 ± 1.8 | |
| ≥65 y | 96 (4.3) | 71.5 ± 6.2 | 19.3 ± 5.9 | 9.1 ± 3.2 | |
| Sex | |||||
| Male | 989 (54.7) | 50.2 ± 2.3 | 26.0 ±2.0 | 23.8 ± 2.0 | <0.0001 |
| Female | 935 (45.3) | 62.9 ± 2.2 | 23.2 ± 2.0 | 13.9 ± 1.7 | |
| Race/ethnicity | |||||
| NH white | 1476 (68.1) | 58.8 ± 1.8 | 22.3 ± 1.5 | 19.0 ± 1.5 | <0.001 |
| NH black | 164 (10.1) | 47.9 ± 5.3 | 32.9 ± 5.1 | 19.2 ± 4.1 | |
| Hispanic | 182 (14.8) | 42.9 ± 4.7 | 29.8 ± 4.6 | 27.4 ± 4.3 | |
| Other, non-Hispanic | 102 (7.1) | 69.1 ± 6.3 | 25.6 ± 6.0 | 5.3 ± 2.2 | |
| Education level | |||||
| <High school | 80 (8.0) | 39.5 ± 6.2 | 29.6 ± 6.4 | 30.9 ± 6.1 | <0.0001 |
| High school | 468 (28.1) | 51.3 ± 3.1 | 24.3 ± 2.7 | 24.4 ± 2.8 | |
| Some college | 592 (27.5) | 50.8 ± 2.9 | 28.5 ± 2.6 | 20.7 ± 2.4 | |
| College graduate | 784 (36.4) | 68.3 ± 2.5 | 20.8 ± 2.1 | 10.9 ± 1.7 | |
| Annual household income | |||||
| ≤$34,999 | 346 (17.5) | 48.5 ± 3.6 | 26.5 ± 3.3 | 25.0 ± 3.1 | <0.0001 |
| $35,000–$74,999 | 703 (36.7) | 49.0 ± 2.7 | 27.3 ± 2.4 | 23.6 ± 2.4 | |
| $75,000–$99,999 | 346 (17.0) | 60.7 ± 3.8 | 23.9 ± 3.3 | 15.4 ± 2.9 | |
| ≥$100,000 | 529 (28.8) | 67.1 ± 2.9 | 20.7 ± 2.5 | 12.3 ± 2.1 | |
| Geographic regions | |||||
| Northeast | 358 (19.1) | 65.4 ± 3.5 | 20.0 ± 3.0 | 14.6 ± 2.5 | 0.02 |
| Midwest | 522 (23.4) | 54.9 ± 3.3 | 22.6 ± 2.7 | 22.5 ± 2.9 | |
| South | 642 (36.9) | 50.1 ± 2.7 | 28.3 ± 2.5 | 21.6 ± 2.3 | |
| West | 402 (20.7) | 59.3 ± 3.5 | 25.0± 3.1 | 15.7± 2.8 | |
| Worksite characteristics | |||||
| No. of employees (n=1,911) c | |||||
| 1–49 | 766 (40.5) | 54.2 ± 2.7 | 24.2 ± 2.3 | 21.6 ± 2.3 | 0.15 |
| 50–99 | 264 (14.0) | 48.3 ± 4.5 | 29.3 ± 4.2 | 22.4 ± 4.2 | |
| 100–499 | 446 (23.2) | 56.4 ± 3.5 | 25.1 ± 3.1 | 18.5 ± 2.8 | |
| 500+ | 435 (22.4) | 64.5 ± 3.6 | 21.0 ± 30 | 14.5 ± 2.7 | |
| Any availability of cafeteria/vending machine d | |||||
| No | 694 (38.3) | 56.2 ± 2.8 | 20.9 ± 2.3 | 23.0 ± 2.5 | 0.05 |
| Yes | 1,230 (61.7) | 56.5 ± 2.1 | 26.4 ± 1.9 | 17.0 ± 1.6 | |
Weighted percentage may not add up to 100% because of rounding.
Chi-square tests were used to examine differences in SSB intake during the workweek across categories for each characteristic.
13 respondents refused to answer.
Any availability of food vending, drink vending, cafeteria or snack bar.
About half of our sample supported the accessibility strategies of Accessible Free Water (54%), Affordable Healthy Food/Drink (49%), Available Healthy Options (46%), while only 28% supported Less Available SSB strategy (Table 2). Support for all four WWS showed significant variation by certain demographic and employment characteristics (χ2 tests, P<0.05). Supports for all four WWS were highest among college graduates. Female employees and those with household income ≥$100,000 had the highest proportion of support for Accessible Free Water. Additionally, the proportion supporting Affordable Healthy Options was the highest among females. Support for Affordable Healthy Options and Available Healthy Options were higher in more populous worksites. Finally, the proportion of employees supportive of Less Available SSB was the highest among non-Hispanic other races and the South region (Table 2).
Table 2.
Support for food and beverage worksite wellness strategies by characteristics of employed US adults (N=1,924)—Summer ConsumerStyles Survey, 2013a
| Characteristics | Accessible Free Water | Affordable Healthy Food/Drink | Available Healthy Options | Less Available SSB |
|---|---|---|---|---|
| % ± SE | % ± SE | % ± SE | % ± SE | |
| Total sample | 54.3 ± 1.6 | 48.6 ± 1.6 | 45.8 ± 1.6 | 28.3 ± 1.5 |
| Age | ||||
| 18–24 y | 51.1 ± 5.2 | 50.2 ± 5.2 | 37.6± 5.0 | 28.9 ± 4.7 |
| 25–44 y | 53.7 ± 2.5 | 49.9 ± 2.5 | 46.7 ± 2.5 | 30.4 ± 2.3 |
| 45–64 y | 56.3 ± 2.3 | 47.5 ± 2.3 | 48.2 ± 2.3 | 27.1 ± 2.1 |
| ≥65 y | 53.3 ± 6.6 | 40.8 ± 6.5 | 40.5 ± 6.3 | 27.1 ± 5.5 |
| Sex | ||||
| Male | 51.8 ± 2.3b | 43.4 ± 2.2b | 43.6 ± 2.2 | 27.7 ± 2.0 |
| Female | 57.3 ± 2.3 | 54.7 ± 2.3 | 48.3 ± 2.3 | 30.1 ± 2.1 |
| Race/ethnicity | ||||
| NH White | 56.9 ± 1.8 | 46.9 ± 1.8b | 45.1 ± 1.8 | 24.1 ± 1.5b |
| NH Black | 45.9± 5.3 | 47.8 ± 5.3 | 50.6 ± 5.3 | 38.0 ± 5.3 |
| Hispanic | 46.8 ± 4.8 | 52.8 ± 4.8 | 41.0 ± 4.7 | 36.1 ± 4.6 |
| Other, non-Hispanic | 57.1± 7.1 | 58.3 ± 6.9 | 55.1 ± 7.0 | 44.8 ± 7.0 |
| Education level | ||||
| <High school | 35.1± 5.9b | 30.3 ± 5.6b | 39.6 ± 6.3b | 16.3 ± 4.4b |
| High school | 50.7 ± 3.1 | 42.7 ± 3.1 | 42.1 ± 3.0 | 23.3 ± 2.6 |
| Some college | 50.1 ± 2.9 | 51.3 ± 2.9 | 40.7 ± 2.8 | 28.1 ± 2.7 |
| College graduate | 65.4 ± 2.5 | 55.9 ± 2.6 | 54.6 ± 2.6 | 37.0 ± 2.6 |
| Annual household income | ||||
| ≤$34,999 | 48.9 ± 3.6 b | 45.9 ± 3.6 | 43.3 ± 3.6 | 26.1 ± 3.2 |
| $35,000–$74,999 | 47.9 ± 2.7 b | 48.8 ± 2.7 | 43.9 ± 2.7 | 26.4 ± 2.3 |
| $75,000–$99,999 | 53.3 ± 3.9 b | 46.0 ± 3.9 | 48.0 ± 3.9 | 32.2 ± 3.7 |
| ≥$100,000 | 61.3 ± 3.0 b | 51.8 ± 3.1 | 48.6 ± 3.1 | 31.6 ± 2.9 |
| Geographic regions | ||||
| Northeast | 52.4 ± 3.7 | 52.9 ± 3.7 | 50.0 ± 3.7 | 29.1 ± 3.3b |
| Midwest | 55.0 ± 3.2 | 41.9 ± 3.1 | 44.9 ± 3.2 | 20.2 ± 2.5 |
| South | 53.3± 2.7 | 48.7 ± 2.7 | 44.0 ± 2.7 | 33.0 ± 2.6 |
| West | 57.2 ± 3.6 | 52.3 ± 3.5 | 46.1 ± 3.5 | 31.1 ± 3.3 |
| Worksite characteristics | ||||
| No. of employees (n=1,911) c | ||||
| 1–49 | 51.5 ± 2.7 | 40.7 ± 2.6b | 39.5 ± 2.6b | 23.4 ± 2.2 |
| 50–99 | 53.0 ± 4.6 | 46.5 ± 4.5 | 40.9 ± 4.4 | 26.4 ± 4.0 |
| 100–499 | 58.9 ± 3.9 | 55.3 ± 3.4 | 51.7 ± 3.5 | 31.3 ± 3.3 |
| 500+ | 56.5 ± 3.7 | 58.3 ± 3.6 | 56.8 ± 3.7 | 31.8 ± 3.4 |
| Any availability of cafeteria/VM d | ||||
| No | 46.6 ± 2.8 | 40.3 ± 2.8 | 35.2 ± 2.7 | 20.9 ± 2.2 |
| Yes | 58.9 ± 2.1 | 53.9 ± 2.1 | 53.0 ± 2.1 | 31.5 ± 2.0 |
| SSB intake during the workweek | ||||
| None | 57.3 ± 2.2b | 49.0 ± 2.2 | 46.3 ± 2.2 | 29.6 ± 2.0b |
| 1–4 times/workweek | 56.6 ± 3.5 | 52.6 ± 3.5 | 49.3 ± 3.5 | 32.1 ± 3.3 |
| ≥ 1 time/workday | 42.2 ± 3.9 | 43.0 ±4.0 | 41.9 ± 4.0 | 15.2 ± 2.6 |
Weighted percentage may not add up to 100% because of rounding.
χ2 test was used for each variable to examine differences across categories, and p value was ≤0.05.
13 respondents refused to answer.
Any availability of food vending, drink vending, cafeteria or snack bar.
Based on multivariable logistic regression analyses (Table 3), daily SSB consumers were less supportive of Accessible Free Water (aOR=0.67; 95% CI=0.46–0.97) and decreasing the number of SSB in cafeterias/VM (aOR=0.49; 95% CI=0.31–0.79) compared with non-SSB consumers after controlling for covariates (sociodemographic characteristics, number of employees, and availability of cafeteria/VM). However, no significant associations were found for daily SSB consumers’ support of Available Healthy Options or Affordable Healthy Food/Drink.
Table 3.
Relationship between employee’s SSB intakea and their support for food and beverage worksite wellness strategies among employed US adults —Summer ConsumerStyles Survey, 2013
| Support for Food and Beverage Worksite Wellness Strategies | ||||
|---|---|---|---|---|
| Accessible Free Water | Affordable Healthy Food/Drink | Available Healthy Options | Less Available SSB | |
| AORb(95% CI) | AORb (95% CI) | AORb (95% CI) | AORb (95% CI) | |
|
| ||||
| SSB intakea | ||||
| None | Reference | Reference | Reference | Reference |
| 1−4 times/workweek | 1.09 (0.78, 1.53) | 1.22 (0.87, 1.71) | 1.27 (0.90, 1.78) | 1.08 (0.75, 1.56) |
| ≥1 time/workday | 0.67 (0.46, 0.97) | 1.01 (0.69, 1.47) | 1.06 (0.72, 1.56) | 0.49 (0.31, 0.79) |
“During the last week that you were at work, how many times during the workday did you drink sugary drinks such as soda pop, sugar sweetened ice tea, sports drinks, energy drinks, or fruit drinks? Do not count diet/low calorie versions.”
Adjusted odds ratio, calculated from logistic regression controlling for age, sex, race/ethnicity, education level, annual household income, geographic regions, number of employees, and any availability of worksite cafeteria/vending machines.
DISCUSSION
This study found that 19% of employed American adults drank a SSB at least once during the workday and 25% consumed them one or two times during a workweek. Consistent with our findings, previous studies reported higher SSB consumption among Hispanics,23 younger adults, males, and those with less education and income.7 Furthermore, the proportion of non-SSB consumers was similar with or without cafeteria/VM in the present study. Previous work found that SSB consumption was associated with the total number of regular sodas available in VM,7 which suggests that reducing the availability and access of SSB in worksites may be an opportunity to decrease SSB consumption. However, we found only 28% of employees supported this kind of restrictive WWS strategy of making SSB less available, while finding considerably stronger support for the accessibility strategies of increasing access to free water and affordable healthy foods and beverages. Support for strategies that increase access is consistent with previous research,24–27 such as over 80% of worksite cafeteria patrons supporting calorie labeling, which led to increased lower calorie side dishes and snacks purchases.27 Lower support for restrictive strategy is also in line with earlier research, such as only 23% supporting a soda and candy tax.28
Environmental and individual factors interrelate in many ways to shape human opportunities and actions.29 Environmental factors such as ease access to food and beverage influence behavior by providing options that may be selected consciously or unconsciously.30 Alternately, if no option is available, the individual is required to act intentionally and plan accordingly to meet needs. In other words, limited availability of SSB in worksites might decrease SSB consumption, because primarily only consumers who plan in advance to bring SSB to work would have access to SSB. More studies are needed to determine the combinations of environmental and individual approaches that are most effective and acceptable in worksite wellness programs after incorporating theories such as the theory of planned behavior and organization-level theory.
We also found daily SSB consumers at worksite being less supportive of free drinking water access and of decreasing SSB availability, although they were as likely as non-consumers to support healthy and affordable cafeteria/VM options. While potential underlying reasons for these findings are unclear, it may be partially due to a lack of knowledge about the negative health consequences of SSB consumption, which is associated with higher levels of SSB consumption,31,32 and knowledge influences individuals’ attitudes and behaviors.33 Thus, increasing SSB consumers’ support for some WWS may be achieved by providing health education at worksite.34
The mutual support by SSBs consumers and non-consumers for increasing healthy and affordable food/drink options provides a clear and actionable way forward. Employee support is an important factor for a strategy’s success and has benefits to employees and employers.24,35 It is also consistent with criteria, such as public support and political will, that policy makers use to determine when to implement policies.35 Employers can operationalize these strategies by integrating food and nutrition guidelines (e.g., the Health and Sustainability Guidelines for Federal Concessions and Vending Operations36) into food service agreements to make worksite food environment healthier. The food and nutrition guidelines can be edited to address barriers to improve worksite food environment, such as potential decline in revenue generated by cafeteria/VM, contracts with vendors and food/beverage companies, and ability to bring less healthful food/beverage from home.
This study has several limitations. First, the findings are potentially subject to selection bias due to sampling methodology, and might not be generalizable to the entire population of employed US adults. However, Summer ConsumerStyle data is population-based and weighted to represent the distribution of the US population, to minimize any potential distortion of results due to selection bias. Second, there is possible bias due to the potential differences between the characteristics of our analytic sample and those who were excluded from the study. Third, Summer ConsumerStyle contains self-reported information, and the reliability and validity of the instruments that were used to measure support for worksite wellness strategies and SSB intake are unknown. Fourth, SSB intake question was limited to workdays in the past week, which may not be representative of a typical week. Lastly, it is unknown where our study respondents obtained the SSB consumed during the workday.
CONCLUSIONS
Our study on employee’s opinion found that almost half supported positive WWS that employers should provide access to free drinking water but daily SSB consumers were less likely to support a healthier worksite beverage environment. Lack of support could be a potential barrier to the successful implementation of certain worksite interventions. Increasing worksite choices for healthy food/beverage is a potential health promotion approach for many adults. Further research could help identify why SSB consumers do not support food and beverage WWS and inform targeted interventions to increase their support.
SO WHAT?
What is already known on this topic?
Worksites are an important setting to promote behaviors associated with improving employee’s dietary intake, which may contribute preventing and controlling obesity, because the work environment has influence on obesity-related behaviors including sedentary work environment, worksite cafeterias, and vending machines.
What does this article add?
About 1 in 5 employed adults reported consuming SSB at least once per workday. Daily workday SSB consumers were less supportive of certain wellness strategies (Accessible free water and Less available SSB).
What are the implications for health promotion practice or research?
Lack of support could be a potential barrier to the successful implementation of certain worksite interventions. Employers might benefit from prioritizing worksite wellness strategies based on employees’ support. Further research could help identify why SSB consumers do not support food and beverage WWS and inform targeted interventions to increase their support.
ACKNOWLEDGEMENTS
Authors would like to thank Steve Onufrack for help developing questionnaires, and Carrie Dooyema, Lisa McGuire, and David Freedman for their kindness in reviewing early drafts and providing insights.
REFERENCES
- 1.Linnan L, Bowling M, Childress J, Lindsay G, Blakey C, Pronk S, et al. Results of the 2004 National Worksite Health Promotion survey. Am J Public Health. 2008;98(8):1503–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.French SA, Harnack LJ, Hannan PJ, Mitchell NR, Gerlach AF, Toomey TL. Worksite environment intervention to prevent obesity among metropolitan transit workers. Prev Med. 2010;50(4):180–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Neville BH, Merrill RM, Kumpfer KL. Longitudinal outcomes of a comprehensive, incentivized worksite wellness program. Eval Health Prof. 2011;34(1):103–23. [DOI] [PubMed] [Google Scholar]
- 4.Park S, Pan L, Lankford T. Relationship Between employment characteristics and obesity among employed U.S. adults. Am J Health Promot. 2013;28(6):389–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Choi B, Schnall PL, Yang H, Dobson M, Landsbergis P, Israel L, et al. Sedentary work, low physical job demand, and obesity in US workers. Am J Ind Med. 2010;53(11):1088–101. [DOI] [PubMed] [Google Scholar]
- 6.Jeffery RW, French SA, Raether C, Baxter JE. An environmental intervention to increase fruit and salad purchases in a cafeteria. Prev Med. 1994;23(6):788–92. [DOI] [PubMed] [Google Scholar]
- 7.Davy BM, You W, Almeida F, Wall S, Harden S, Comber DL, et al. Impact of individual and worksite environmental factors on water and sugar-sweetened beverage consumption among overweight employees. Prev Chronic Dis. 2014;11:E71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Robroek SJW, Van den Berg TIJ, Plat JF, Burdorf A. The role of obesity and lifestyle behaviours in a productive workforce. Occup Environ Med. 2011;68(2):134–9. [DOI] [PubMed] [Google Scholar]
- 9.Van Nuys K, Globe D, Ng-Mak D, Cheung H, Sullivan J, Goldman D. The association between employee obesity and employer costs: Evidence from a panel of U.S. employers. Am J Health Promot. 2014;28(5):277–85. [DOI] [PubMed] [Google Scholar]
- 10.Sorensen G, Landsbergis P, Hammer L, Amick BC, Linnan L, Yancey A, et al. Preventing chronic disease in the workplace: A workshop report and recommendations. Am J Public Health. 2011;101(S1):S196–S207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Malik VS, Popkin BM, Bray GA, Després J-P, Hu FB. Sugar-sweetened beverages, obesity, type 2 diabetes mellitus, and cardiovascular disease risk. Circulation. 2010;121(11):1356–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.US Department of Agriculture, US Department of Health and Human Services. Dietary guidelines for Americans, 2010. 7th edition. Washington, DC: US Government Printing Office; 2010. Available from: http://health.gov/dietaryguidelines/dga2010/dietaryguidelines2010.pdf. Accessed November 18, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Han E, Powell LM. Consumption patterns of sugar-sweetened beverages in the United States. J Acad Nutr Diet. 2013;113(1):43–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kit BK, Fakhouri TH, Park S, Nielsen SJ, Ogden CL. Trends in sugar-sweetened beverage consumption among youth and adults in the United States: 1999–2010. Am J Clin Nutr. 2013;98(1):180–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Goetzel RZ, Roemer EC, Liss-Levinson R, Samoly D. Workplace Health Promotion: Policy Recommendations that Encourage Employers to Support Health Improvement Programs for their Workers. Partnership for Prevention, 2008. Available at: https://www.prevent.org/data/files/initiatives/workplacehealtpromotion-policyrecommendations.pdf. Accessed April 8, 2015. [Google Scholar]
- 16.Orlandi MA. The diffusion and adoption of worksite health promotion innovations: An analysis of barriers. Prev Med. 1986;15(5):522–36. [DOI] [PubMed] [Google Scholar]
- 17.Linnan L, LaMontagne AD, Stoddard A, Emmons KM, Sorensen G. Norms and their relationship to behavior in worksite settings: an application of the Jackson Return Potential Model. Am J Health Behav. 2005;29(3):258–268. [DOI] [PubMed] [Google Scholar]
- 18.Peterson KE, Dubowitz T, Stoddard AM, Troped PH, Sorensen G, Emmons KM. Social context of physical activity and weight status in working-class populations. J Phys Act Health. 2007;4:381–396. [PubMed] [Google Scholar]
- 19.Sorensen G, Barbeau E, Hunt MK, Emmons K. Reducing social disparities in tobacco use: a social-contextual model for reducing tobacco use among blue-collar workers. Am J Public Health. 2004;94(2):230–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Biener L, Glanz K, McLerran D, Sorensen G, Thompson B, Basen-Engquist K, Linnan L, Varnes J. Impact of the Working Well Trial on the worksite smoking and nutrition environment. Health Educ Behav. 1999;26(4):478–494. [DOI] [PubMed] [Google Scholar]
- 21.Weiner BJ, Lewis MA, Linnan LA. Using organization theory to understand the determinants of effective implementation of worksite health promotion programs. Health Educ Res. 2009;24(2):292–305. [DOI] [PubMed] [Google Scholar]
- 22.Engbers LH, van Poppel MNM, Chin A Paw MJM, van Mechelen W. Worksite Health Promotion Programs with Environmental Changes: A Systematic Review. Am J Prev Med. 2005;29(1):61–70. [DOI] [PubMed] [Google Scholar]
- 23.Gase LN, Robles B, Barragan NC, Kuo T. Relationship between nutritional knowledge and the amount of sugar-sweetened beverages consumed in Los Angeles County. Health Educ Behav. 2014;41(4):431–9. [DOI] [PubMed] [Google Scholar]
- 24.Foltz JL, Harris DM, Blanck HM. Support among U.S. Adults for local and state policies to increase fruit and vegetable access. Am J Prev Med. 2012;43(3, Suppl 2):S102–S108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Handy S, Sallis JF, Weber D, Maibach E, Hollander M. Is support for traditionally designed communities growing? Evidence from two national surveys. J Am Plann Assoc. 2008;74(2):209–21. [Google Scholar]
- 26.Carlson SA, Guide R, Schmid TL, Moore LV, Barradas DT, Fulton JE. Public support for street-scale urban design practices and policies to increase physical activity. J Phys Act Health. 2011;8(Suppl 1):S125–34. [DOI] [PubMed] [Google Scholar]
- 27.Webb KL, Solomon LS, Sanders J, Akiyama C, Crawford PB. Menu labeling responsive to consumer concerns and shows promise for changing patron purchases. J Hunger Environ Nutr. 2011;6(2):166–78. [Google Scholar]
- 28.Norton A Most Americans Oppose Soda, Candy Taxes. HealthDay. Apr 25, 2013. Available at www.harrisinteractive.com/vault/HealthDay%20Harris%20Poll%20Candy%20Tax_042513.pdf. Accessed February 3, 2015. [Google Scholar]
- 29.Frerichs L, Brittin J, Sorensen D, Trowbridge MJ, Yaroch AL, Siahpush M, Tibbits M, Huang TTK. Influence of School Architecture and Design on Healthy Eating: A Review of the Evidence. Am J Public Health. 2015;105(4):e46–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Morsella E, Poehlman TA. The inevitable contrast: Conscious vs. unconscious processes in action control. Front Psychol. 2013;4:590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hattersley L, Irwin M, King L, Allman-Farinelli M. Determinants and patterns of soft drink consumption in young adults: a qualitative analysis. Public Health Nutr. 2009;12(10):1816–22. [DOI] [PubMed] [Google Scholar]
- 32.Park S, Onufrak S, Sherry B, Blanck HM. The Relationship between health-related knowledge and sugar-sweetened beverage intake among US adults. J Acad Nutr Diet. 2014;114(7):1059–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Madden TJ, Ellen PS, Ajzen I. A Comparison of the Theory of Planned Behavior and the Theory of Reasoned Action. Pers Soc Psychol Bull. 1992;18(1):3–9. [Google Scholar]
- 34.Hyland A, Higbee C, Borland R, Travers M, Hastings G, Fong GT, et al. Attitudes and beliefs about secondhand smoke and smoke-free policies in four countries: Findings from the international tobacco control four country survey. Nicotine Tob Res. 2009;11(6):642–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Greener J, Douglas F, van Teijlingen E. More of the same? Conflicting perspectives of obesity causation and intervention amongst overweight people, health professionals and policy makers. Soc Sci Med. 2010;70(7):1042–9. [DOI] [PubMed] [Google Scholar]
- 36.Centers for Disease Control and Prevention. Health and sustainability guidelines for federal concessions and vending operations. Available at www.cdc.gov/obesity/downloads/guidelines_for_federal_concessions_and_vending_operations.pdf. Accessed April 8, 2015.