

Abstract
Vaccination is an important and cost‐effective disease prevention and control strategy. Over the years, milestone discoveries in vaccine research and development as well as vaccine delivery systems, have contributed to expanded immunisation coverage and reduction in morbidity and mortality associated with vaccine‐preventable diseases. While this outstanding development in vaccine delivery continues, there are considerable gaps in access to vaccines among populations living in fragile and conflict‐affected zones which appeared to be the fault line of limited vaccine coverage. Despite progress in coronavirus disease 2019 (COVID‐19) vaccine development, there are concerns about the feasibility of African countries affected by armed conflict and violence to effectively deliver COVID‐19 vaccines at the unprecedented level required to fight against the virus. In this article we discuss the feasibility of access to COVID‐19 vaccine among populations in conflict affected areas in Nigeria including methods that can be applied to reach and vaccinate populations in these settings.
Keywords: access, conflict, COVID‐19, insecurity, Nigeria, vaccine
Highlights
Conflict and violence exerts immediate impact on the determinants of health including access to essential health interventions.
People living in violent and conflict affected areas in Nigeria are disproportionately affected by limited immunisation coverage.
These populations risk been excluded from coronavirus disease 2019 (COVID‐19) vaccination framework.
There is need to develop refined approaches in order to ensure safe and effective COVID‐vaccine delivery to populations in conflict‐affected areas.
1.
The World Health Organisation (WHO) declared the novel coronavirus disease 2019 (COVID‐19) a global health pandemic of International concern on the 11th of March 2020. 1 Since then, the new virus has continued to spread across the globe with more than 432 million cases and more than 5.9 million deaths as of 24 February 2022. 2 Its rapid dissemination has prompted biopharmaceutical industries to begin the development of novel therapeutic interventions and vaccines in order to fight against the virus. 3 There have been unfamiliar collaborations between giant pharmaceutical industries and governments in the race for vaccine development. 4 In February 2020, the WHO highlighted that a vaccine against SARS‐CoV‐2 is not expected to be available in less than 18 months. 5
Global efforts to develop and distribute COVID‐19 vaccines have yielded accelerated development of multiple vaccines at an unprecedented level. The recent advancements in COVID‐19 vaccine discovery have offered hope in the discovery of tools required to combat the new global threat. While the WHO has outlined general guidelines for vaccine prioritisation, many countries have set a distribution plan that prioritises at‐risk populations including the elderly and health workers. 6 As of 13 February 2022%, 61.8% of the world population have been administered at least one dose of COVID‐19 vaccine, with 10.6% in low and middle income countries. 7
There is already an overt gap in vaccination programs in different continents across the globe. In February 2021, the arrival of COVID‐19 vaccine supply to African countries began under the COVID‐19 Vaccines Global Access (COVAX) programme (an initiative that ensures equitable access to vaccines especially in low‐income countries) including bilateral deals, and donations. By 18 March 2021, 38 countries have received COVID‐19 vaccine consignments and 30 have begun vaccination campaigns. As of 22 February 2022%, 12.77% of populations have received full dose of COVID‐19 vaccine while 4.98% have been partially vaccinated in Africa. 8 Percentages of people who have received at least one dose of COVID19 vaccine in 40 African Countries are shown in Figure 1.
FIGURE 1.
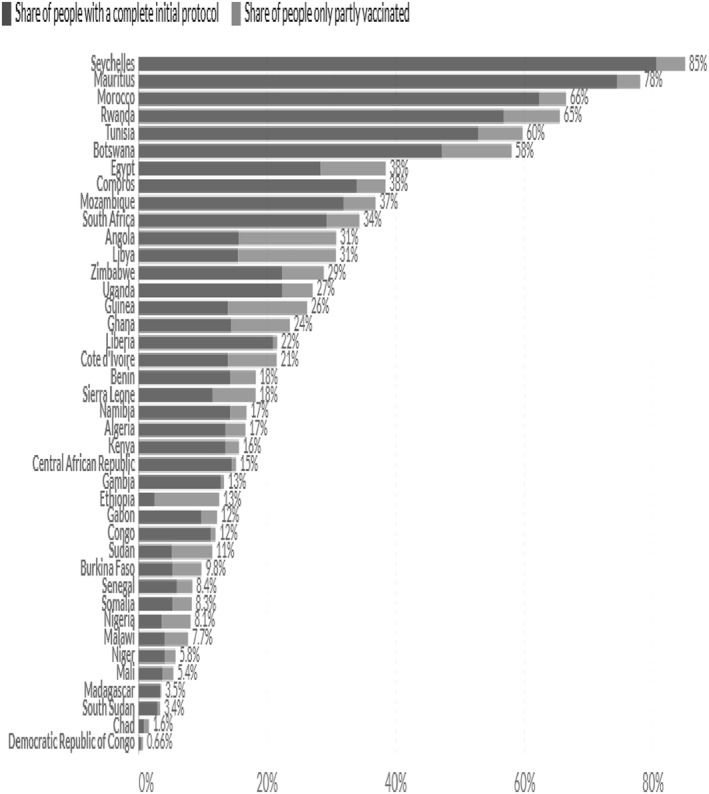
Showing percentage of people who have received at least one dose of COVID19 vaccine in 40 African Countries
Source: Our World in Data. Share of People Vaccinated against COVID‐19, 22 Feb, 2022. https://ourworldindata.org/explorers/coronavirus‐data‐explorer?facet=none&pickerSort=desc&pickerMetric=location&Metric=People+vaccinated+%28by+dose%29&Interval=7‐day+rolling+average&Relative+to+Population=true&Color+by+test+positivity=false&country=Africa. Accessed 22 February 2022
Africa has shown to be one of the most skilful continents in the fight against disease outbreaks. The region has successfully implemented an expanded vaccine distributions and vaccinations in rural and remote communities. 9 While these experiences will provide valuable insight into COVID19 vaccine deployment in the continent, there are concerns on the feasibility of mass vaccination campaigns in fragile and conflict‐affected zones. Conflict and violence exerts immediate impact on the determinants of health including access to essential health interventions. Inhabitants of conflicts affected areas are often faced with little or no access to lifesaving vaccines, making them more vulnerable to incidents and deaths due to vaccine‐preventable diseases (VPDs). 10 The eruption of violence and conflict has been correlated with shortfalls in terms of immunisation outcomes leading to epidemics of VPDs in Africa. 11 Typical examples are widespread insurgencies in the Horn of Africa; armed insurgency in Somalia contributed to higher unimmunised or under‐immunised populations resulting in widespread poliovirus infection following importation of the virus in the country, which spread to neighbouring countries (Ethiopia and Kenya) throughout 2013–2014. 12 , 13
The emergence of COVID‐19 has increased vulnerability and tension in the conflicted affected part of Nigeria. As of 24 February 2022, there are 254, 428 confirmed cases of COVID‐19 with 3142 deaths across Nigeria. 14 Although the arrival and distribution of COVID‐19 vaccine in Nigeria has offered hope in the fight against the deadly disease, populations living in conflict affected regions are at risk of being inaccessible with the life‐saving vaccines in a country with existing vaccination gaps. Over the years, Nigeria has undergone traumatising security issues in the form of insurgency, kidnapping and militancy. One of the most devastating violent crises in recent years is the activities of Boko Haram. Thousands of populations have been forced to flee their homes with many more being displaced, trapped or living behind enemy lines. This makes it difficult for health workers and humanitarian actors to reach vulnerable populations with basic healthcare and life‐saving vaccines. This situation has prevented vaccines from reaching targeted vaccine recipients, thereby creating immunity gaps across geographical locations in Nigeria. 15 This begs the question, will people in fragile and conflict‐affected zones in Nigeria have access to COVID‐19 vaccines?
2. ARMED CONFLICT AND VACCINATION IN NIGERIA
Globally in 2015, two‐third of the 20 million infants who are eligible for diphtheria, tetanus toxoids and pertussis (DTP) vaccines are from countries affected by armed conflicts. 16 Also, United Nations Children's Fund estimated in 2015 that six countries (Central African Republic, Equatorial Guinea, Somalia, Syrian Arab Republic, South Sudan, and Ukraine) that reported less than 50% coverage of the DTP vaccine were all experiencing conflicts or other humanitarian emergencies. 17 A similar pattern has been reported concerning the recent emergence of vaccine‐deprived poliovirus infection outbreaks in seven conflict‐affected settings in Africa including Nigeria. 18
Nigeria has experienced series of crisis (ethnic, religious and political violence) since independence, each leading to loss of lives and destruction of properties. The insecurity crisis in Nigeria include, among others, kidnapping, armed robbery, assassination, ritual killings in almost all parts of the country, and currently the activities of Boko Haram (a non‐state armed group that resists western education and modern science) in selected parts of the Northern region especially northeast. 19 In the past decades especially, there have been series of violent attacks linked to the activities of Boko Haram in the northern part of the country resulting in loss of lives and extensive damage to infrastructure, drawing further backwards the already slow development rate in the region. The frequent attacks have resulted in major loss of lives and extensive damage to infrastructure, causing devastating decline in health service delivery, decline in immunisation coverage and mass displacement of people from their homes.
Since 2009, the extended armed conflict in the North‐Eastern states (Borno, Adamawa, and Yobe) in Nigeria has deprived almost 5.6 million people of access to health services. 20 The ongoing conflict has led to an escalation of attacks on healthcare which has resulted in the depletion of humanitarian spaces available for relief societies. According to the WHO Surveillance System for Attacks on Healthcare, more than 40 attacks on healthcare have been reported since 2019. 21 This is complicated by the shortage of skilled health workers in rural communities leading to further deterioration in access to healthcare by those most in need. Despite the important role of healthcare support in conflict‐affected regions, healthcare workers face constant risk of being attacked, abducted, abused, and criminalised including death in some instances.
In 2017, an estimated 600,000 people (with 100,000 children aged 9–59 months) were reported living in 200 internaly displaced person camps across 18 Local Government Areas in Borno state. These children were not covered during routine vaccination and were continually omitted during immunisation programs, resulting to increase in population of children susceptible to VPDs. 22 In addition, significantly low vaccination coverage has been observed in North‐eastern Nigeria compared to other regions of the country. According to the National immunisation Coverage Study carried out in 2016 and 2017 in Nigeria, 42% of children in the northeast have in no occasion received any vaccine compared to only 8% of children in the southeast. 15 This issue has had substantial impact on vaccine distribution with significant population of children who are not reached with routine vaccinations, leading to epidemics of VPDs. 22
3. ACCESS TO CORONAVIRUS DISEASE 2019 VACCINE
Nigeria received 3.94 million doses of AstraZeneca‐Oxford vaccine manufactured by the Serum Institute of India through the COVAX facility on 2 March 2021. On 7 March 2021, the National Primary Health Care Development Agency in partnership with the Federal Ministry of Health officially commenced a nationwide immunisation campaign against COVID‐19. 23 The vaccination plan was rolled out in phases, starting with the most priority groups such as healthcare workers who are at the frontline of beating the pandemic. According to the Secretary to the Government of the Federation and Chairman, Presidential Task Force on COVID‐19, the vaccination campaign will reach every eligible Nigeria by the end of 2022 when 70% of the population is expected to have been vaccinated and achieved herd immunity. 23 As of 21 February 2022, only 8.3% of eligible populations have received the first dose of COVID‐19 vaccine while just 3.7% have been fully vaccinated across the 36 states in Nigeria. 8 Number of people who have been partially and fully vaccinated in Nigeria is shown in Figure 2.
FIGURE 2.
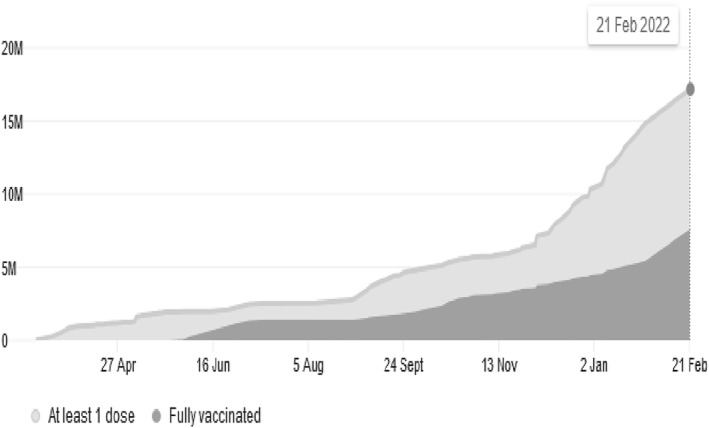
Showing number of people who have been partially and fully vaccinated in Nigeria
Source: Our World in Data. https://ourworldindata.org/covid‐vaccinations?country=NGA. Accessed 23 February 2022.
Although Nigeria has joined the rest of the world to mobilise support towards rapid, fair and equitable access to COVID‐19 vaccines, there are concerns among experts that people in conflict affected regions of the country may not have access to the life‐saving vaccine (ICRC, 2022). Populations in these regions are at risk of being excluded from COVID‐19 immunisation coverage for several reasons. First, prevailing factors such as poor health capacities (shortage of skilled health personnel, weakened infrastructure) and disputed borders due to frequent attacks in these settings can compromise the COVID‐19 vaccination campaign, thereby creating a subpopulation of unimmunised or under‐immunised persons prone to potential disease outbreak since no one is safe until everyone is safe. Second, according to the United Nations Commission on Human Rights, over 2.9 million people have been displaced by conflict and violence in the north‐eastern part of Nigeria. 24 This large‐scale displacement occasioned by the decimation of towns since the onset of insurgency in the north‐eastern part of Nigeria can make it difficult to reach communities and settlements controlled by the non‐state armed group during COVID‐19 vaccine immunisation rollout. Finally, difficulty in keeping COVID‐19 vaccines cold enough until they can be administered can pose a major logistical challenge in areas affected by armed conflict and violence in Nigeria. The organisation of the cold chain in Nigeria involves five stages of distribution; the National Strategic Cold Store (NSCS) which is the main vaccines storage site, six zonal stores each representing six geopolitical zones receives vaccines supply from the NSCS, state vaccine stores receive vaccine delivery from the zonal stores, Local Government Area (LGA) store receives supply from state storage and Primary Health Care centres receives supply from LGA stores. 25 Achieving effective delivery of quality vaccines requires a cold chain that meets specific temperature requirements which can be difficult to maintain in under‐resourced settings. Fragile and conflict‐affected areas in Nigeria are often faced with infrastructural challenges, specifically electricity, which is crucial for maintaining vaccine storage at the specified temperature. Although there are quite an efficient vaccine organisation from primary storage facilities to the stores, there are numerous logistic disruptions from local cold stores to endpoints. All of these factors combine to inflict risk of impaired access to COVID‐19 vaccine by populations in areas controlled by armed groups, thereby increasing the risk of COVID‐19 spread in vulnerable populations and risk of disease spread across national borders.
4. RECOMMENDATIONS
People living in conflict‐affected regions in Africa who have endured the double burden of conflict and COVID‐19 deserve the right to access COVID‐19 vaccines as do other vulnerable populations. It is crucial to consider and ensure the inclusion of this population in the COVID‐19 national vaccination framework. The government in Nigeria must develop refined approaches in order to ensure safe and effective COVID‐vaccine delivery to populations in conflict‐affected areas. Based on available evidences and best practices, the following strategies can be adopted.
5. ENGAGING MILITARY WORKFORCE TO DELIVER CORONAVIRUS DISEASE 2019 VACCINE
Military involvement in vaccination programs has offered valuable insight to the delivery of vaccines to populations in security‐inaccessible areas in Nigeria. For example, in an attempt to reach populations at‐risk of polio virus in conflict affected areas during polio outbreak in Borno state in 2016, the government engaged the military to support delivery of oral polio vaccines to inaccessible areas. This approach led to 47% increase in LGAs covered by oral polio vaccination programs between May 2016 and July 2016. 26
In line with this approach, the Nigerian government should ensure safe and effective COVID‐19 vaccine delivery through collaboration with the military and other security personnel as well as integration of vaccination protocols into existing and ongoing humanitarian response activities. In addition, enlisted military personnel should be trained across military parastatals on instructional and practical training on COVID‐19 vaccination efforts. This will allow qualified medical personnel to deliver and administer COVID‐19 vaccines to civilians in security‐inaccessible communities across Nigeria.
6. INTEGRATING LOCATION INTELLIGENCE IN CORONAVIRUS DISEASE 2019 VACCINE DISTRIBUTION
Location intelligence helps immunisation programs to understand risk profiles of communities where they operate. The Government should evaluate the current security status in conflict affected regions as well as develop geographic intelligent assessments in areas affected by armed conflict. This will provide additional security to health workers based on current intelligence assessment and ensure effective planning and safe implementation of field COVID‐19 vaccination activities. Application of geographic assessment tools can assist in development of maps for local testing and to quantify at‐risk populations in hard‐to‐reach communities that have been prioritised to receive COVID‐19 vaccines. This approach will help to predestinate COVID‐19 vaccines at selected relatively safe locations with effective storage facilities before mapping redistribution routes for the vaccine delivery in security inaccessible areas. In addition, integration of vaccine distribution information database and geospatial data system will help inform vaccination activities across communities as well as track locations of populations that have been vaccinated.
7. ENGAGING THE COMMUNITY
Developing community engagement strategies is pivotal in ensuring an effective COVID‐19 vaccine delivery in conflict and humanitarian emergency locations. The Volunteer Community Mobiliser programme, an initiative that recruited and trained local community women as vaccinators has been observed to improve participation in house‐to‐house routine immunisation programs in security‐inaccessible communities in northern Nigeria. Engaging traditional and religious leaders in local communities, training of local residents as vaccinators and building community mobilisation networks will help improve access to COVID‐19 vaccines. This will bring to light the key community engagement components that addresses issues associated with access to COVID‐19 vaccines.
8. EXPANSION OF VACCINE STORAGE CAPACITY
Vaccine delivery must be kept safe and at the right temperature requirement. Maintaining vaccine cold chain logistics is often difficult in areas affected by conflict and violence due to the break down and sometimes deliberates destruction of vital health services. There is need for the government to strengthen collaborations with local and international stakeholders in order to expand COVID‐19 vaccine storage in conflict regions. This collaboration will foster instalment of solar‐powered vaccine storage equipments at predestinated locations that are less vulnerable to attacks. This will allow mapping of redistribution routes for COVID‐19 vaccine delivery to health facilities in security compromised areas. Delivery of potent COVID‐19 vaccines to health facilities in security inaccessible sites can be conducted through the use of cooling vans and mobile cooling devices conditioned to specific storage temperature requirement for the vaccine storage.
9. CONCLUSION
People living in regions affected by conflict and violence in Africa often face little or no access to basic health services. These populations are equally vulnerable to COVID‐19 and have the right to be protected from the deadly infectious disease. It is important for the government in Nigeria to develop refined approaches towards inclusion and coverage of people in security compromised regions in COVID‐19 vaccination framework.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
ETHICS STATEMENT
Not applicable.
AUTHORS’ CONTRIBUTIONS
Amos Abimbola Oladunni and Usman Abubakar Harun developed the concept of the manuscript. Amos Abimbola Oladunni, Usman Abubakar Harun, Lawrence Gregory Ijafu and Don Eliseo Lucero‐Prisno draughted and prepared the manuscript. DELP assisted with article interpretation and language edit. All authors read and approved the final manuscript.
ACKNOWLEDGEMENT
Not applicable. No funding sources available.
Oladunni AA, Haruna UA, Ijafu LG, Lucero‐Prisno DE III. Will people in conflict affected zones in Africa have access to COVID‐19 vaccine? A case of Nigeria. Int J Health Plann Mgmt. 2022;37(4):1918‐1925. 10.1002/hpm.3474
DATA AVAILABILITY STATEMENT
No data are available.
REFERENCES
- 1. WHOa. WHO Ramps up Preparedness for Novel Coronavirus in the African Region: WHO Regional Office for Africa; 2020. https://www.afro.who.int/news/who‐rampspreparedness‐novel‐coronavirus‐african‐region.Accessed23March2021 [Google Scholar]
- 2. Worldometer. 2022. Accessed 15 February 2022. https://www.worldometers.info/coronavirus/ [Google Scholar]
- 3. Le TT, Cramer JP, Chen R, Mayhew S. Evolution of the COVID‐19 vaccine development landscape. Nat Rev Drug Discov. 2020;19(10):667‐668. 10.1038/d41573-020-00151 [DOI] [PubMed] [Google Scholar]
- 4. Biopharmaceutical Innovators Lead the Charge in the Fight against Coronavirus. Accessed 23, March 2021. https://www.bio.org/policy/human‐health/vaccines‐biodefense/coronavirus [Google Scholar]
- 5. Grenfell R, Drew T. Here’s Why the WHO Says a Coronavirus Vaccine Is 18 Months Away. Accessed 25 March 2021. https://theconversation.cm/heres‐why‐the‐who‐says‐a‐coronavirus‐vaccine‐is‐18‐months‐away‐131213 [Google Scholar]
- 6. Beaumont P. COVID‐19 Vaccine: Who Are Countries Prioritizing for First Doses?. Accessed March 23, 2021. https://www.theguardian.com/world/2020/nov/18/covid‐19‐vaccine [Google Scholar]
- 7. Mathieu E, Ritchie H, Ortiz‐Ospina E, et al. A Global Database of COVID‐19 Vaccinations; 2022. Accessed February 13, 2022. https://ourworldindata.org/covid‐vaccinations [Google Scholar]
- 8. Our World in Data . Share of People Vaccinated against COVID‐19, Feb. 22, 2022. Accessed 22 February 2022. https://ourworldindata.org/explorers/coronavirus‐data‐explorer?facet=none&pickerSort=desc&pickerMetric=location&Metric=People+vaccinated+%28by+dose%29&Interval=7‐day+rolling+average&Relative+to+Population=true&Color+by+test+positivity=false&country=Africa [Google Scholar]
- 9. Uwagbale EE. African Countries Have an Advantage in Rolling Out COVID‐19 Vaccines; 2021. Accessed February 13, 2022. https://qz.com/africa/1974325/decades‐of‐vaccine‐programs‐will‐help‐africa‐with‐covid‐19/ [Google Scholar]
- 10. Nnadi C, Etsano A, Uba B, et al. Approaches to vaccination among populations in areas of conflict. J Infect Dis. 2017;216:S368‐S372. 10.1093/infdis/jix175 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Grundy J, Biggs BA. The impact of conflict on immunisation coverage in 16 countries. Int J Heal Policy Manag. 2019:211‐221. 10.15171/ijhpm.2018.127 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Kamadjeu R, Mahamud A, Webeck J, et al. Polio outbreak investigation and response in Somalia. J Infect Dis. 2014;210(Suppl 1):S181‐S186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Walker AT, Sodha S, Warren WC, et al. Forewarning of poliovirus outbreaks in the Horn of Africa: an assessment of acute flaccid paralysis surveillance and routine immunization systems in Kenya. J Infect Dis. 2014;210(Suppl 1):S85‐S90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. NCDC . COVID‐19 Nigeria. Accessed March 24, 2021. https://covid19.ncdc.gov.ng [Google Scholar]
- 15. Ryoko Sato. Effect of armed conflict on vaccination: evidence from the Boko haram insurgency in north‐eastern Nigeria. Confl Health. 2019;13:49. 10.1186/s13031-019-0235-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. UNICEFa . Two‐third of Unimmunized Children Lives in Conflict‐Affected Countries; 2016. Accessed 4, April 2021. https://www.unicef.org/media/media_09087.html [Google Scholar]
- 17. UNICEFb . Immunization: Current Status and Progress. 2016; 2016. Accessed April 4, 2021. https://data.unicef.org/topic/child‐health/immunization/# [Google Scholar]
- 18. Morales M, Nnadi CD, Tangermann RH, Wassilak SG. Note from the field: circulating vaccine‐deprived poliovirus outbreaks‐five countries. 2014‐2015. MMWR Morb Mortal Wkly Rep. 2016;65:128‐129. March 2021. [DOI] [PubMed] [Google Scholar]
- 19. Udeh SC, Okoroafor EC, Ihezie UR. Insecurity and National economic development implications for Nigeria’s vision 20: 2020. Int J Dev Man Rev. 2013;8:1. [Google Scholar]
- 20. WHOc. How Community Engagement Prevents and Protects Health Care from Attacks in North‐East Nigeria. Accessed March 29, 2021. https://www.who.int/news‐room/feature‐stories/detail/howPage11of12JohnWiley&Sonscommunity‐engagement‐prevents‐and‐protects‐health‐care‐from‐attacks‐in‐north‐eastnigeria [Google Scholar]
- 21. WHOd. Surveillance System for Attacks on Health Care (SSA). Accessed March12 29, 2021. https://ssa.who.int [Google Scholar]
- 22. Ibrahim BS, Mohammed Y, Usman R, Abubakar A, Nguku P. Five Year Review Case‐Base Surveillance Data; 2018:2‐3.Burden and trend of measles in Nigeria. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. NPHCDA. COVID‐19 Vaccination Update in 36 States and the FCT. Accessed January 24, 2022. https://nphcda.gov.ng/covid‐19‐vaccination‐update‐in‐36‐states‐and‐the‐fct/ [Google Scholar]
- 24. UNCHR . Nigeria Emergency. Accessed 29 March 2021. https://www.unchr.org/nigeria‐emergency.html [Google Scholar]
- 25. Sarley D, Mahmud M, Idris J, et al. Transforming vaccines supply chains in Nigeria. Vaccines. 2017;35(17):2167‐2174. [DOI] [PubMed] [Google Scholar]
- 26. Nkwogu L, Shuaib F, Braka F, et al. Impact of engaging security personnel on access and polio immunization outcomes in security‐inaccessible areas in Borno state, Nigeria. BMC Publ Health;18:1311. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
No data are available.