

Abstract
Objective
To evaluate the impact of the COVID‐19 lockdown on admissions to gynecological emergency departments (ED) of three Italian university hospitals with different rates of COVID‐19 incidence.
Methods
A retrospective study was conducted in the gynecological EDs of Modena (Emilia‐Romagna), Sassari and Cagliari (Sardinia) regarding all admissions to gynecological EDs during November 1 to 30, 2019, and March 11 to April 9, 2020 (lockdown period).
Results
A total of 691 women (mean age 38.3 ± 14.3 years) who were admitted to the gynecological EDs were included. The relative decrease in women evaluated from March 11 to April 9, 2020, was −56.6% (95% confidence interval [CI] 52.2–61.1). Time spent in the ED was also significantly shorter during this period (P=0.02) in comparison to November 1 to 30, 2019. The most evident decrease was observed for pelvic pain (−68.9% [95% CI 60.3–76.7]; −91 cases). The management of women suggests a more effective use of the ED, with higher rates of hospitalization (P=0.001) and recourse to emergent surgeries (P=0.005) and lower rates of discharge to home (P=0.03).
Conclusion
The COVID‐19 lockdown greatly reduced the rate of admission to gynecological EDs, but the real emergencies were filtered from the more deferrable ones.
Keywords: COVID‐19, Emergency, Emergency department, Emergency room, Gynecology, Pandemic, SARS‐CoV‐2, Urgency
Short abstract
The COVID‐19 lockdown greatly reduced the admission rate to gynecological emergency departments, particularly for pelvic pain; however, real emergencies were filtered from more deferrable cases.
1. INTRODUCTION
The first cases of a new pneumonia of unknown origin were found in Wuhan (China) on December 31, 2019. 1 The causative virus was identified from throat swab samples in the Chinese Centre of Disease Control and Prevention (CCDC) on January 7, 2020, and it was named severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). Subsequently, WHO renamed it COVID‐19. 2 The reproduction rate of COVID‐19 is very high, and the extent of the infection soon spread around the world. It has shown equal numbers of cases between men and women, but a lower mortality rate in women. 3 , 4
In Italy, COVID‐19 first manifested on January 31, 2020, when two tourists from China tested positive for the virus in Rome. 5 Subsequently, an outbreak of infection was identified on February 21, 2020, with 20 confirmed cases in Codogno (Lombardy). Within a few days, the virus had spread throughout the country. Since February 23, 2020, the Italian Council of Ministers has issued a series of restrictive measures to limit the spread of the contagion that has been progressively restricting, until the decree on March 8, 2020 (which was more narrowly extended on March 11, 2020) defined the beginning of the so‐called “lockdown” phase, resulting in the closure of all business and educational activities, as well as all restaurants, prohibiting the gathering of people in public places, that continued until May 4, 2020. Hospital activities have also been partially reorganized, suspending all outpatient activities (including non‐urgent and deferred visits) and freelance activities and permitting only urgent surgeries for oncological diseases or emergencies. 6 However, no restrictions were possible on a citizen’s basic right to seek medical attention in emergency departments (EDs) for urgent health problems. The aim of the present study was to evaluate the extent by which the lockdown, imposed by the government, has impacted the activity of admissions to the gynecological EDs of three Italian university hospitals with different COVID‐19 incidence rates.
2. MATERIALS AND METHODS
A retrospective observational study was conducted in the Department of Obstetrics and Gynecology of three different university hospitals with a similar catchment area: Modena (Emilia‐Romagna); Sassari (Sardinia); and Cagliari (Sardinia). The different provinces showed markedly different rates of incidence: lower rates in Cagliari (0.55 cases per 1000 individuals) and Sassari (1.70 cases per 1000 individuals) and higher in Modena (5.18 cases per 1000 individuals). 7 The present study analyzed all admissions to the Obstetrics and Gynecology (Ob/Gyn) EDs of the three hospitals during November 1 to 30, 2019, and from March 11 to April 9, 2020. Those periods were selected because November 2019 was the last entire month without the perception of the existence of COVID‐19 (30 days) and the narrowest national lockdown started on March 11, 2020 (the subsequent 30 days have been included). The study included only women who presented to the ED for gynecological reasons (not pregnancy) or for problems related to the first trimester of pregnancy (threatened miscarriage, ectopic pregnancy, and pregnancy of unknown location), excluding all admissions during the second and third trimesters of pregnancy and the puerperium, because pregnancy surveillance was always considered a non‐deferrable activity.
The two hospitals in Sardinia (Cagliari and Sassari) were contacted via email by an author (GG) on May 5, 2020, to verify the possibility of obtaining the same data as collected in Modena from their available databases. The two centers that were contacted then agreed to participate in the study.
The specific characteristics of individuals that accessed the different Ob/Gyn EDs were then obtained from the databases of local hospitals and sent anonymously to GG who analyzed the data. The following were evaluated: the age of patients; time in the ED (minutes from admission to final decision [self‐discharge, discharge to home, and hospitalization]); menopausal status; indication for admission; evaluation of actual genital bleeding performed by healthcare professional present at admission (doctor, midwife, or nurse) categorized as none, mild, intermediate, or heavy; management in the ED considering observation (yes/no); execution of blood test (yes/no); medical therapy and office surgery (yes/no); final disposition (self‐discharge, discharge to home, hospitalization, or hospitalization for emergent surgery); eventual suggestions for other outpatient services; and prescribed drugs at home.
No ethical approval was requested from the different Institutional Review Boards (IRBs) for a simple review of the medical records, since the collection of these data was performed during clinical practice.
Statistical analyses were performed using StatView, version 5.01.98 (SAS Institute Inc., Cary, NC, USA). Within‐group and intra‐group comparisons were performed using t tests for paired data. When necessary, prevalence was compared by contingency tables and the χ2 test. Binomial “exact” calculations were used to calculate the 95% confidence intervals (CIs) of proportions. For all analyses, the null hypothesis was rejected at a two‐tailed P value <0.05. Parametric results were expressed as the mean ± standard deviation (SD).
3. RESULTS
A total of 691 women (mean age 38.3 ± 14.3 years) who were admitted to the gynecological ED in the three university hospitals (n=268 in Modena, n=215 in Sassari, and n=208 in Cagliari) for the included reasons were evaluated in the study (n=209 from March 11 to April 9, 2020 and n=482 from November 1 to 30, 2019).
The basal features of women evaluated in November 2019 and in March to April 2020 are reported in Table 1. The age, menopausal status, and bleeding entity were similar between the different periods, while the time in the ED was significantly longer in November 2019 in comparison to the period in March to April 2020 (P=0.02). The general indications for admission were problems related to the first trimester of pregnancy (n=238, 34.4%), pelvic pain (n=173, 25.0%), bleeding during reproductive age (n=102, 14.8%), postmenopausal bleeding (n=55, 7.6%), vulvovaginitis (n=65, 9.4%) and other indications (n=58, 8.4%). The prevalence of women admitted for problems related to the first trimester of pregnancy was significantly higher (P<0.0001) in March to April 2020 in comparison to November 2019, while it was significantly lower for pelvic pain (P=0.03) during the same time period in comparison to November 2019.
Table 1.
General features of women admitted to the gynecological emergency department during November 1 to 30, 2019, and March 10 to April 9, 2020 (lockdown period) and their indication for admission. a
| November 2019 (n=482) | March–April 2020 (lockdown period) (n=209) | P | |
|---|---|---|---|
| Age (years) | 38.2 ± 14.8 | 38.6 ± 12.9 | 0.74 |
| Postmenopausal (yes) | 72 (16.2) | 23 (11.0) | 0.17 |
| Time in emergency room (min) | 108.9 ± 101.7 | 89.5 ± 94.9 | 0.02 |
| Bleeding entity | 0.53 | ||
| None | 295 (61.2) | 116 (55.5) | |
| Mild | 120 (24.9) | 57 (27.3) | |
| Intermediate | 58 (12.0) | 31 (14.8) | |
| Heavy | 9 (1.9) | 5 (2.4) | |
| Indication for admission | |||
| Problems of first trimester of pregnancy | 143 (29.7) | 95 (45.5) | <0.0001 |
| Pelvic pain | 132 (27.4) | 41 (19.6) | 0.03 |
| Bleeding during reproductive age | 76 (15.8) | 26 (12.4) | 0.26 |
| Postmenopausal bleeding | 39 (8.1) | 16 (7.7) | 0.81 |
| Vulvovaginitis | 49 (10.2) | 16 (7.7) | 0.27 |
| Others | 43 (8.9) | 15 (7.2) | 0.58 |
Values are given as number (percentage) or mean ± standard deviation.
The relative decrease in women evaluated in March to April 2020 in comparison to November 2019 was −56.6% (95% CI 52.2–61.1), which was similar between the hospitals in Modena (−62.5%, 95% CI 55.4–79.4) and Sassari (−65.6%, 95% CI 57.7–72.9) (P=0.68) and significantly milder, but still present, in Cagliari (−36.2%, 95% CI 27.9–45.2) (P=0.001).
In Figure 1, the percentage decrease (95% CI) in admissions to the ED by indication was reported, with the most evident decrease being observed for pelvic pain (−68.9%, 95% CI 60.3–76.7) and, in absolute terms (−91 cases) (Table 1), the mildest for problems related to the first trimester of pregnancy (−33.6%, 95% CI 25.9–41.9).
Figure 1.
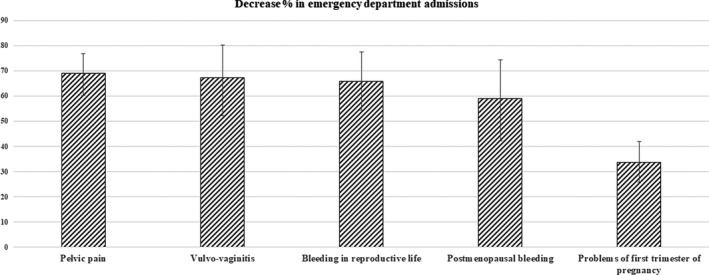
Percentage decrease (95% confidence interval) in admissions to the gynecological emergency department by indication between November 1–30, 2019, and March 10 to April 9, 2020 (lockdown period).
The management of women in EDs for the different periods is reported in Table 2. It suggests a more effective use of the ED by patients, with higher rates of hospitalization (P=0.001) and recourse to emergent surgeries (P=0.005) and lower rates of discharge to home (P=0.03) with a prevalence similar to other interventions in the ED (Table 2). Prescribed drugs after discharge to home were similar between the two periods that were considered (Table 2).
Table 2.
Management of women during admission to emergency department during November 1–30, 2019, and March 10 to April 9, 2020 (lockdown period) and prescribed drugs after discharge at home. a
| November 2019 | March–April 2020 (lockdown period) | P | |
|---|---|---|---|
| Observation | 105/482 (21.8) | 34/209 (16.3) | 0.10 |
| Blood test execution | 101/482 (20.9) | 53/209 (25.4) | 0.20 |
| Medical therapy | 59/482 (12.2) | 26/209 (12.4) | 0.94 |
| Office surgery | 19/482 (3.9) | 12/209 (5.7) | 0.29 |
| Hospitalization | 50/482 (10.4) | 41/209 (19.6) | 0.001 |
| Hospitalization for emergent surgery | 14/482 (2.9) | 16/209 (7.7) | 0.005 |
| Self‐discharge | 18/482 (3.7) | 3/209 (1.4) | 0.11 |
| Discharge at home | 407/482 (84.4) | 162/209 (77.5) | 0.03 |
| Sent to other outpatient services | 112/482 (23.2) | 45/209 (21.5) | 0.62 |
| Prescribed drugs at discharge | |||
| Antibiotics | 63/407 (15.5) | 18/162 (11.1) | 0.18 |
| Anti‐inflammatory drugs | 68/407 (16.7) | 22/162 (13.5) | 0.36 |
| Hormonal treatments | 71/407 (17.4) | 28/162 (17.3) | 0.96 |
| Anti‐hemorrhagic drugs | 27/407 (6.6) | 6/162 (3.7) | 0.18 |
| Others | 58/407 (14.2) | 19/162 (11.7) | 0.43 |
Values are given as number (percentage).
4. DISCUSSION
In the present multicenter Italian study, a significant reduction was found in the number of admissions and in the time spent by women in Ob/Gyn EDs of different hospitals after the Italian lockdown due to the COVID‐19 pandemic. This reduction proved to be greater than half (>50%), especially for indications such as pelvic pain (−68.9%), vulvovaginitis (−67.3%), and genital bleeding, both during reproductive age (−65.8%) and in the postmenopausal period (−59.0%), with a lower decrease in the indications related to the first trimester of pregnancy (−33.6%). This reduction was significant in all the hospitals included in the study and does not seem to depend on the actual incidence of COVID‐19 in the different Italian provinces but on the lockdown imposed by the Government. This occurred in the face of a non‐substantial drop in hospitalizations and emergent surgeries, resulting in a reduced rate of discharge to home. This suggests that COVID‐19 greatly reduced the rate of admission to gynecological EDs; however, the real emergencies were filtered from the more deferrable cases.
EDs are increasingly being utilized for non‐emergent medical care, especially during pregnancy. 8 Up to one‐third of patients seen in the ED have “non‐urgent” problems that could have potentially been addressed in an outpatient setting. 9 Use of the ED for non‐urgent conditions may lead to excessive healthcare spending, unnecessary testing and treatment, and weaker relationships between patients and primary care providers. 10 The results of the present study suggest that during the COVID‐19 lockdown, real emergencies have been filtered from more deferrable cases, increasing the number of hospitalized women, especially for emergent surgeries, and decreasing the number of women discharged from the ED. Furthermore, the COVID‐19 epidemic could have challenged the capability of healthcare systems to deal with emergencies. During the same period, admissions to hospital for acute myocardial infarction in Italy decreased, while the fatality rate and complications increased. 11 The data in the present study reassure that the number of hospitalizations (50 vs 41) and emergent gynecological surgeries (14 vs 16), which are potentially life‐saving, was not significantly different in the two time periods, suggesting that the system has withstood the emergency.
Many governments and directors of hospitals and other medical institutions decided to restrict the number of outpatient medical consultations, as well as non‐essential surgeries, because they face challenges providing health care to patients with COVID‐19 and also argue that these restrictions are to reduce the risk of contamination to both health providers and patients. 12 No restrictions were possible on the opportunity to seek medical attention in the ED for urgent health problems. However, a similar, although slightly lower, decrease (−42%) in admission to the ED during the COVID‐19 pandemic has recently been found in a general hospital in USA), 13 and this was unlikely to be attributable to declines in elective surgeries or incidence of disease. As in the present study, many patients may be avoiding hospitals to minimize the risk of COVID‐19 infection. The risk of exposing patients to COVID‐19 infection while in hospital to receive gynecological care was considered too high and sometimes not justified, but it must be weighed against the risks of protracted diagnostic and/or therapeutic delays. This is particularly true for symptoms that can mask an oncological disease, such as genital bleeding, especially in the postmenopausal period. The problem is less pressing with symptoms such as pelvic pain that can hide such chronic but not malignant diseases (i.e. endometriosis, adenomyosis, fibroids, etc.), and possibly even be treated in an outpatient setting. In the present study, pelvic pain was the symptom that had the greatest decline in absolute and relative terms in the EDs of the three hospitals, leading to new questions on how the pandemic may have changed patients’ perception of pain.
The present study has several limitations. The data may not be generalizable to other populations, because they were collected from only three hospitals in an Italian population. The comparative period (November 2019) may not be exactly optimal for seasonal influences. Furthermore, the clinical consequences of this decreased rate of admission remain unknown and warrant longer‐term studies. Being an observational study, a phenomenon was described and no demonstration of cause could be drawn from the results. However, the decline showed herein is pronounced and cannot be the result of randomness.
The COVID‐19 lockdown greatly reduced the rate of admission to gynecological EDs. This reduction suggests a more effective use of the ED by patients that may inspire future policies for the implementation of emergency services, trying to avoid the risks of diagnostic and/or therapeutic delays, which it is hoped were only marginally caused by the COVID‐19 pandemic.
AUTHOR CONTRIBUTIONS
GG: concept and design, data analysis, interpretation, manuscript draft, final approval. MCDS: study execution, manuscript revise, final approval. MC: study execution, final approval. GC: interpretation, study execution, manuscript revise, final approval. FD: manuscript revise, final approval. GT: study execution, manuscript revise, final approval. MP: interpretation, manuscript revise, final approval. CS: study execution, manuscript revise, final approval. AP: interpretation, study execution, manuscript revise, final approval. FF: concept and design, study execution, manuscript revise, final approval.
CONFLICTS OF INTEREST
The authors have no conflicts of interest.
REFERENCES
- 1. Lu H, Stratton CW, Tang Y. Outbreak of pneumonia of unknown etiology in Whuan China: The mistery and the miracle. J Med Virol. 2020;92:401–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. World Health Organization . WHO Director‐General’s Remarks at the Media Briefing on 2019‐nCoV on 11 February 2020.
- 3. Grandi G, Facchinetti F, Bitzer J. The gendered impact of coronavirus disease (COVID‐19): Do estrogens play a role? Eur J Contracept Reprod Health Care. 2020;25:233–234. [DOI] [PubMed] [Google Scholar]
- 4. Cagnacci A, Xholli A. Age‐related difference in the rate of COVID‐19 mortality in women versus men. Am J Obstet Gynecol. 2020; 10.1016/j.ajog.2020.05.039. Online ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Severgnini C. Coronavirus: Primi due casi in Italia, Corriere della Sera, 31st January 2020. Available at: https://www.corriere.it/cronache/20_gennaio_30/coronavirus‐italia‐corona‐9d6dc436‐4343‐11ea‐bdc8‐faf1f56f19b7.shtml.
- 6. CovidSurg Collaborative , Nepogodiev D, Bhangu A. Elective surgery cancellations due to the COVID‐19 pandemic: global predictive modelling to inform surgical recovery plans. Br J Surg. 2020; 10.1002/bjs.11746. Online ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Italian Civil Protection Department; Department of Health . Published online May 1, 2020. Available at: http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioNotizieNuovoCoronavirus.jsp. Accessed June 16, 2020.
- 8. Kilfoyle KA, Vrees R, Raker CA, Matteson KA. Nonurgent and urgent emergency department use during pregnancy: An observational study. Am J Obstet Gynecol. 2017;216:181.e1–181.e7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Uscher‐Pines L, Pines J, Kellermann A, Gillen E, Mehrotra A. Emergency department visits for nonurgent conditions: Systematic literature review. Am J Manag Care. 2013;19:47–59. [PMC free article] [PubMed] [Google Scholar]
- 10. Matteson KA, Weitzen SH, Lafontaine D, Phipps MG. Accessing care: Use of a specialized women's emergency care facility for nonemergent problems. J Womens Health (Larchmt). 2008;17:269–277. [DOI] [PubMed] [Google Scholar]
- 11. De Rosa S, Spaccarotella C, Basso C, et al. Società Italiana di Cardiologia and the CCU Academy investigators group. Reduction of hospitalizations for myocardial infarction in Italy in the COVID‐19 era. Eur Heart J. 2020;41:2083–2088. 10.1093/eurheartj/ehaa409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Bahamondes L, Makuch MY. Family planning: an essential health activity in the pandemic of SARS‐CoV‐2. Eur J Contracept Reprod Health Care. 2020;1–2. 10.1080/13625187.2020.1768368. Online ahead of print. [DOI] [PubMed] [Google Scholar]
- 13. Baum A, Schwartz MD. Admissions to Veterans Affairs Hospitals for emergency conditions during the COVID‐19 pandemic. JAMA. 2020; 10.1001/jama.2020.9972. Online ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]